labor & delivery akmal abbasi, m.d.. prenatal care prenatal care includes: 1. complete history...
TRANSCRIPT

LABOR & DELIVERY
Akmal Abbasi, M.D.

Prenatal Care
• Prenatal care includes:1. Complete history (medical, obstetrical, psychosocial)2. Complete physical exam3. Complete pelvic exam & assessment4. Nutritional assessment and counseling5. Lab work; standard prenatal screen is recommended:
• Complete blood count (CBC) with differential• ABO type & Rh factor

Prenatal Care
• Rubella
• Rapid plasma reagin (RPR) or veneral disease research laboratory (VDRL)
• Hepatitis B surface antigen
• Antibody screen
• Urinalysis (UA) culture & sensitivity
Other lab work when appropriate which may include:
• Glucose testing• Alpha fetal protein• Amniocentesis• Ultrasound• Sickle cell• HIV• Gonorrhea
• Chlamydia• Toxoplasmosis• Group B Strep (GBS)
culture• Platelet &
differential• Pap smear

Return visits
• Frequency:
• Every 4 weeks, up to 28 weeks LMP;
• Every 2 weeks, from 28 weeks to 36 weeks;
• Weekly from 36 weeks until the birth.
• Visits more frequent as needed.

• Second trimester– Organ systems increase in complexity
• Third trimester– Many organ systems become fully functional– Fetus undergoes largest weight change– At end of gestation fetus and uterus push maternal
organs out of position
Second and Third Trimesters

The Second and Third Trimesters
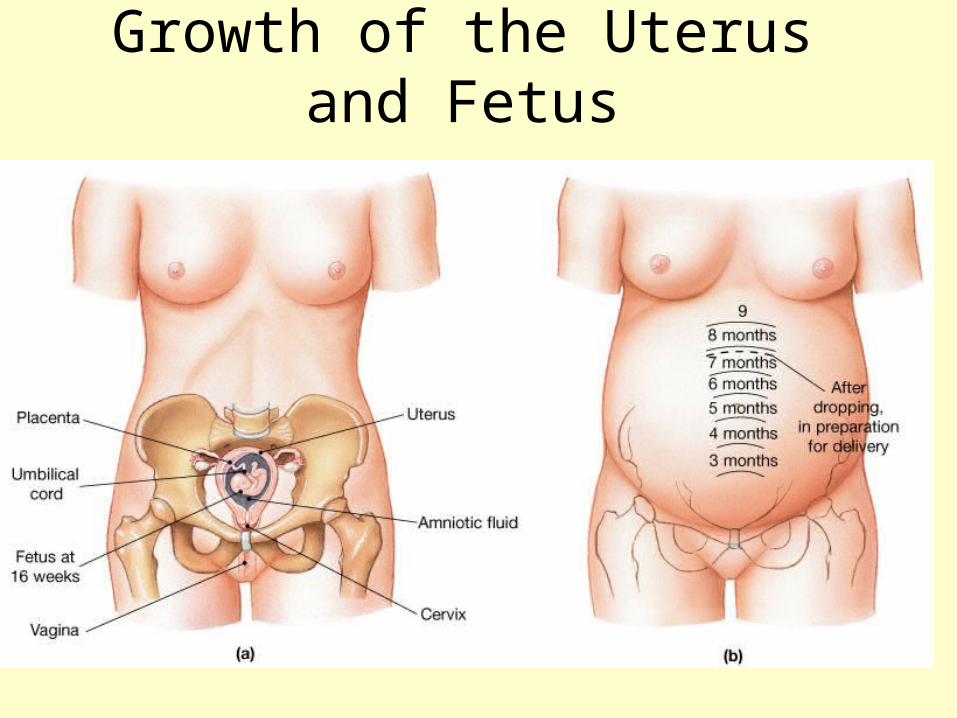
Growth of the Uterus and Fetus

Growth of the Uterus and Fetus

Developing fetus totally dependent on maternal organs
• Maternal adaptations include increased– Respiratory rate– Tidal volume– Blood volume– Nutrient and vitamin uptake– Glomerular filtration rate

Structural and Functional Changes in the Uterus
• Progesterone inhibits uterine muscle contraction – Opposed by estrogens, oxytocin and
prostaglandins
• Multiple factors interact to produce labor contractions in uterine wall

Structural and Functional Changes in the Uterus
• Passage– pelvimetry - measurement of dimension of bony
pelvis– pelvic cavity and inlet– are they wide enough?
• Passenger– fetal head - largest part, compressible– biparietal diameter - most important measurement– fetal attitude - head facing where?– fetal lie– fetal presentation

Passenger & Passage = fetopelvic relationships
• Station - level of the presenting part in relation to ischial spines– -5 to +4– 0 = ischial spines
• Lie-relation of long axis of fetus to long axis of mother– longitudinal– transverse

Presentation
• Presentation- part of the fetus that enters the pelvis first– breech
– cephalic
• Attitude - degree of flexion,extension of head– vertex
– military
– brow
– face

Position
• Position - relationship of a particular reference point on presenting part of fetus to pelvis– breech=sacrum– cephalic=occiput

Labor• Physiology - unknown
• Premontory signs of labor– lightening (engagement)
• leg cramps, frequency, edema
– Braxton-hicks– cervical changes (ripening)– bloody show (mucous plug, 24 – 48 hours)– ROM (24 hours)

Factors Involved in the Initiation of Labor and Delivery

Parturition: Initiation of Labor
• Estrogen reaches a peak during the last weeks of pregnancy causing myometrial weakness and irritability
• Weak Braxton Hicks contractions may take place• As birth nears, oxytocin and prostaglandins cause
uterine contractions• Emotional and physical stress:
– Activates the hypothalamus – Sets up a positive feedback mechanism, releasing more
oxytocin
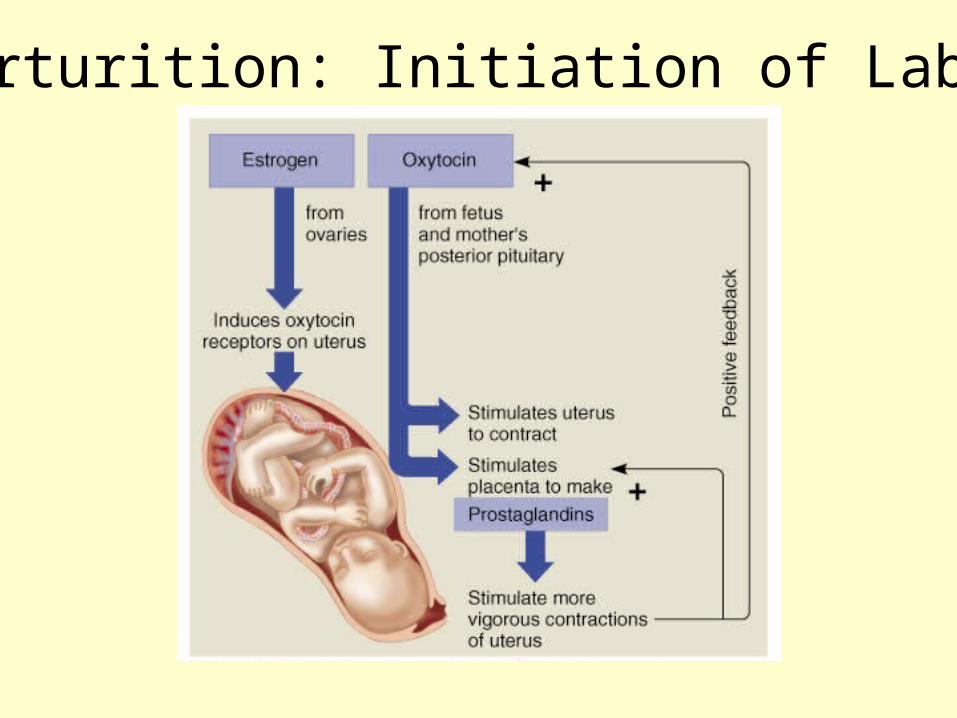
Parturition: Initiation of Labor

Fetal Monitoring
• Track the baby’s heart rate during labor.
• Safe procedure that has saved the lives of many babies in high-risk situations.

Problems with Fetal Monitors
• Critics think fetal monitors falsely identify babies as being in danger.
• Fetal monitoring is linked to an increase in the number of emergency cesarean deliveries.
• Many women complain that the monitors are uncomfortable and restrictive.

Labor & Delivery
• Normally, labor and subsequent delivery occurs from 38 to 41 weeks after the start of the last normal menstrual period.
• If labor occurs before 37 weeks of pregnancy, it is considered premature, and after 42 weeks, is termed postmature (post-term) labor.
• Labor can be divided into three stages (plus a fourth stage that begins immediately after the placenta is delivered):

Labor & Delivery
• The first stage is from the earliest contractions up to the time of the birth.
• It is generally the longest and hardest and involves the effacement (thinning out) and dilation (opening up) of the cervix to 10 centimeters (5 fingerbreadths) or slightly more in a large baby or a breech birth.
• Stage one has 3 phases. • The second stage of labor involves the baby's
birth and lasts an average of about 1 to 3 hours.

Labor & Delivery
• The third stage of labor consists of the expulsion of the afterbirth (placenta) and takes about 30 minutes, sometimes a little longer.
• There is also considered a fourth stage, which consists of the immediate postpartum phase in which the uterus continues to contract into a hard, grapefruit sized ball to prevent excessive bleeding.

Stages of Labor
• Stage 1 of Labor
• Phase 1 (Early or Latent Phase)
• Phase 2 (Active Phase)
• Phase 3 (Transitional Phase)
• Stage 2 of Labor
• Stage 3 of Labor & Birth
• Stage 4 of Labor & Birth


Labor and Delivery Medication
• Analgesics are pain-relieving drugs that help the mother relax.
• Anesthetics are stronger painkillers that block sensation.
Induced Labor
• Labor is started artificially by breaking the amnion and giving the mother medications to stimulates contractions.
• Used when continuing the pregnancy threatens the well-being of mother or baby.
• Contractions often longer, harder, and closer together.

STAGE 1 OF LABOR--First phase
(latent phase). • This early labor of stage 1 take about 8 to 12
hours (average) if the woman has had one or more children (multipara) and about 16 to 18 hours in a woman expecting her first child (primipara).
• This part of labor can last much longer in some births and still be considered normal.
• Some women will experience start and stop labor over a period of several days before true labor finally starts and continues until the baby is born.

STAGE 1 OF LABOR--First phase (latent phase).
• The cervix begins to efface and dilate up to 3 centimeters.
• True contractions begin. • The contractions are rhythmic, squeezing
muscular activity that affects the walls of the uterus during labor.
• These contractions last 15 to 30 seconds, up to 45 seconds each and occur every 10 to 30 minutes and may be almost imperceptible and come on an irregular basis.

STAGE 1 OF LABOR--First phase (latent phase).
• They become regular as time passes. • The amniotic sac may or may not break
at this early stage. • The passing of the thick, blood-tinged
plug of mucus (bloody show) that protects the mouth of the uterus during pregnancy will most likely occur at this point.

STAGE 1 OF LABOR--- Phase 2
(Active Phase): • Contractions grow stronger and start coming
every 3 to 5 minutes and for a duration of 45 to 60 seconds each.
• The cervix dilates from 3 to 8 centimeters and is effaced close to 100%.
• The woman's breathing needs to stay as relaxed as possible during this phase, but she will, most likely, have to focus more on the contractions as they come and go.

STAGE 1 OF LABOR--- Phase 2 (Active Phase):
• Observations should be made regarding the frequency, duration and intensity of the contractions as well as the mother's ability to cope with the contractions.
• An initial exam is made to determine how far the cervix had dilated and effaced, the extent of the engagement into the pelvis and position of the baby's head and its placement upon the cervix.
• Notation is made about the "bloody show".

STAGE 1 OF LABOR--- Phase 2 (Active Phase):
• The abdomen will be palpated to confirm the baby's body position and degree of engagement into the pelvis.
• The baby's heart rate will be monitored using a fetoscope or by using a doppler.
• When the amniotic sac breaks, note the color and amount of amniotic fluid.
• Green or brown fluid indicates the presence of meconium (fetal bowel contents) and its consistency.

STAGE 1 OF LABOR--- Phase 2 (Active Phase):
• If meconium is present, extreme caution is taken during the birth to prevent the baby from aspirating it into the lungs.
• Assess the mother by taking her blood pressure, pulse and respirations.
• Ask questions about her last bowel movement, urination (which needs to be done every few hours since a full bladder may inhibit contractions and slow labor) and last oral intake.
• An IV may be started on the mother in the event a cesarean delivery needs to be done.

STAGE 1 OF LABOR--- Phase 2 (Active Phase):
• Drugs (analgesic or a regional anesthetic) may be administered by an anesthesiologist.
• If the labor slows down or stalls (most often either due to drug administration or inability to move about, or both), then pitocin (synthetic oxytocin) will be given to speed the labor up again.
• Oral food and fluid intake is usually discouraged and prohibited in the event that a cesarean surgery and a general anesthesia is to be used.
STAGE 1 OF LABOR-- Phase 3
(Transition Phase): • The cervix becomes fully dilated (10 cm). • Contractions switch from the type that open the
cervix to the "pushing-down" type meant to expel the baby.
• Other symptoms may occur -- nausea, vomiting, shivers and irritability.
• This is the time when a woman may have some feelings of self-doubt and feels that she cannot go on through the labor. A good supportive birthing team can aid in overcoming these feelings.
STAGE 1 OF LABOR-- Phase 3 (Transition Phase):
• Focusing, relaxation, encouragement and support are reinforced.
• The woman may be encouraged to continue with slow breathing patterns as long as she is able to do so and use the panting (rapid breathing) only if she feels the urge to push (pushing should be done only after complete dilation is achieved and the cervix has slipped over the baby's head... pushing to soon can cause the cervix to swell and the dilation to regress, slowing down the labor and birth process).

STAGE 2 OF LABOR
• This stage of labor begins at complete dilation and ends with the birth of the baby.
• It may last from a few minutes to 3 hours. • The uterus becomes longer as the cervix dilates,
with contractions lasting longer and becoming more intense.
• The baby continues to descend into the pelvis. • Contractions continue about every 2 to 5
minutes and last for 60 to 90 seconds.

STAGE 2 OF LABOR
• Pushing down is done during contractions.
• The baby is moving down through the birth canal aided by the mother's desire to push with her abdominal muscle force combined with the uterine contractions.
• The baby's head flexes and rotates as it descends through the birth canal.

STAGE 2 OF LABOR
• An episiotomy may be made in the perineum (area between the vagina and the rectum) to widen the birth opening.
• This is often done to aid in forceps and vacuum extraction placement for instrument assisted births.
• This procedure may require a local analgesic or other anesthetic option such as a spinal, epidural, pudendal, paracervical, or local in the perineum.

STAGE 2 OF LABOR
• Toward the end of this stage, the perineum begins to bulge with the baby's head pushing against it and then appears at the vaginal opening (crowning).
• The baby's head emerges and then rotates either to the left or to the right maternal leg.
• At this time, the shoulders emerge and the rest of the body follows quickly.
• The baby is placed upon the mother's abdomen.

STAGE 2 OF LABOR
• The cord is clamped and cut right away.
• The baby is removed from the mother's abdomen, suctioned (usually with an electrical suction unit) and examined.

STAGE 3 LABOR
• After a brief time (usually 15 to 45 minutes after the birth of the baby), mild contractions begin again.
• As the uterus contracts, the placenta separates from the uterine wall and is expelled during this phase.
• Initiating breast-feeding at birth releases the hormone oxytocin, which stimulates the contractions of the uterus.
• Uterine involution begins.

STAGE 3 LABOR
• Placental expulsion may be accompanied by a sudden gush of blood.
• If the uterus doesn't contract and remain firm, hemorrhaging may occur.
• A final examination is conducted to be sure the entire placenta is out.
• Examinations of both the maternal and the fetal side of the placenta are done and note any abnormalities.
• The mother is examined after the placenta has been expelled for tears in the vagina or cervix.

STAGE 3 LABOR
• If an episiotomy has been done, it is repaired at this time (with or without local anesthesia).
• Continuing assessments are made on both the mother and infant.
• Both are cleaned up and made warm and comfortable.
• Breast-feeding, if not initiated before the expulsion of the placenta, is now usually encouraged.
• This helps the uterus to remain firm and contracted preventing excess bleeding.
STAGE 4 OF LABOR & BIRTH
• This encompasses the first hour after the placental expulsion.
• The mother's risk of hemorrhaging, urinary retention and hypotension increases.
• This is also the time necessary for family bonding to occur.
• If the woman has received drugs during her labor and birth, observe both the mother and the infant for anesthetic side effects and complications.

Instrument DeliveryForceps
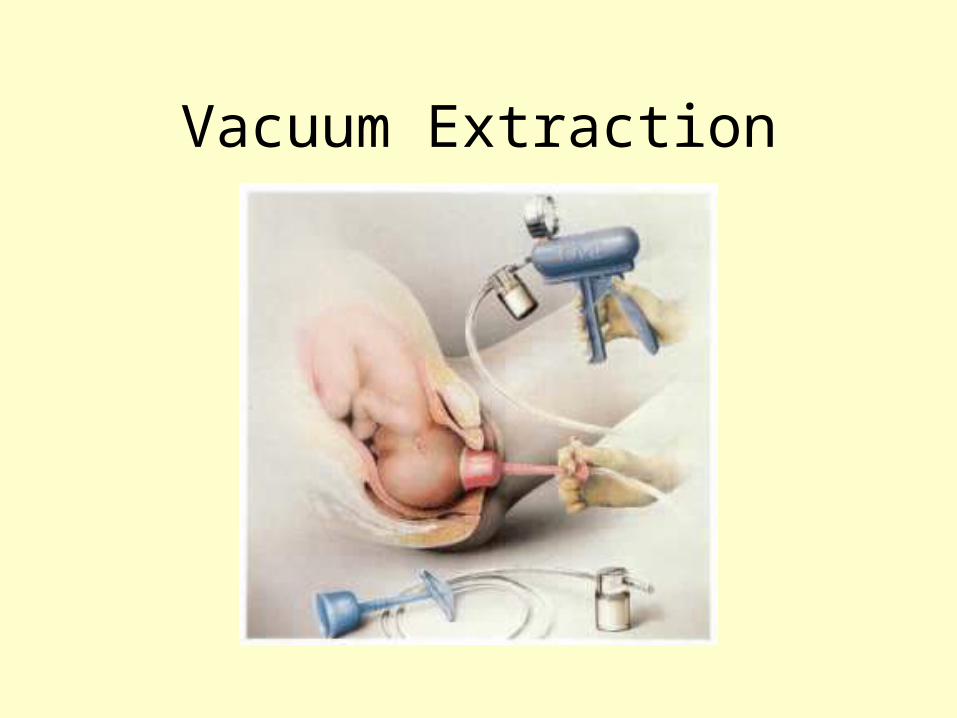
Vacuum Extraction


The Baby’s Adaptation to
Labor and Delivery
Newborn’s appearance

The Apgar Score

BIRTH COMPLICATIONS
Anoxia: Inadequate oxygen supply during labor/delivery
Caused by– Squeezing of umbilical cord– Abruptio Placenta: premature separation of the
placenta– Placenta Previa: placenta covers the cervical
opening

Other labor and delivery situations
• Premature labor – True labor begins before fetus has completed normal
development (< 37 weeks gestational age).
• Difficult deliveries – When the fetus faces the pubis rather than the sacrum – The legs or buttocks enter the vaginal canal first
(breech births)
• Multiple births – Twins, triplets, etc.
• Dizygotic or monozygotic situations