la gestione delle trasfusioni a domicilio - reteoncologica.it · la gestione delle trasfusioni a...
TRANSCRIPT

ONCOEMATOLOGIA E SERVIZI TERRITORIALI26 aprile 2018
La gestione delle trasfusioni a domicilio
Dottssa Renata MarinelloSC U Geriatria e MMO
Servizio di Ospedalizzazione a Domcilio
Numero di condizioni patologiche croniche per gruppo drsquoetagrave
E Tragni Giornale italiano di farmacoeconomia 2014
Elevato rischiodi complicanze
Elevata instabilitagraveclinica
Stabilizzazione ritardata
Recupero incompleto
Ripetuteospedalizzazioni
Altamortalitagrave
PAZIENTE ANZIANOCOMPLESSO
OSPEDALE
IATROSI AMBIENTALE
MODELLI DI OSPEDALIZZAZIONE A DOMICILIO NEL MONDO
bull Israeli Home Hospital - ISRAELE
bull Hopkins Home Hospital di Baltimora - USA
bull Peterborough Hospital at Home
bull Gloucester Hospital at Home
bull Leicester Hospital at Home scheme
bull Verdun Hospital in the Home - CANADA
bull Hospital-in-the-home program at Royal Melbourne Hospital
bull Hospital-in-the-home program at Prince of Wales Hospital-Sidney
bull Hospitalizacioacuten a domicilio di Valencia Madrid Barcellona - SPAGNA
GB
AUSTRALIA
bull Etagrave avanzata della popolazione
bull Aumento delle malattie croniche e le loro
riacutizzazioni
bull Progressi tecnologici
bull Elevata spesa sanitaria
bull Necessitagrave di contenere la spesa
OSPEDALIZZAZIONE A DOMICILIO
Lrsquo ospedalizzazione domiciliare egrave definita
come la modalitagrave attraverso cui le strutture
ospedaliere in considerazione di specifiche
valutazioni seguono con il proprio
personale direttamente a domicilio pazienti
che necessitano di prestazioni con
particolare complessitagrave tali da richiedere un
processo assistenziale di livello ospedaliero
Piano Sanitario Nazionale 2002-2004
REGIONE PIEMONTE - BOLLETTINO UFFICIALE N 14 DEL 080410Deliberazione della Giunta Regionale 16 marzo 2010 n 85-13580Attivita di continuita assistenziale organizzazione e remunerazione delle attivitadi assistenza specialistica di ospedalizzazione domiciliare
Attivitagrave di ospedalizzazione presso il domicilioSi definisce attivitagrave di ospedalizzazione presso il domicilio lrsquoorganizzazione di attivitagrave assistenziali di tipo sanitario che assicurano la cura di pazienti in fase ancora acuta in una fase di continuitagrave assistenziale trattabili presso la residenza con supporto infermieristico e medico specialistico e la presa in carico da parte di unitagrave operativa di presidio ospedaliero Si tratta ad esempio di pazienti da trattare con scompenso cardiaco in fase acuta riacutizzazione di broncopneumopatie croniche ostruttive ictus ischemici non complicati infezioni respiratorie eo urinarie scompensi glicometabolici o per altre patologie di analoga complessitagrave assistenziale Tale presa in carico comporta lrsquoassunzione della responsabilitagrave clinica del paziente nel periodo in trattamento da parte dellrsquounitagrave operativa ospedaliera che dovragrave garantire oltre che lrsquoassistenza infermieristica giornaliera anche lrsquoassistenza medica specialistica necessaria e la contattabilitagrave dello specialista presso il presidio durante tutto lrsquoarco della settimana
Ospedalizzazione a Domicilio di Torino
ATTIVITArsquo ANNO 2015
482 ricoveri
9424 visite infermieristiche
5969 visite mediche
Etagrave media dei pazienti 8407 anni (range 19-104 anni)
Durata media del ricovero 1527 giorni
Numero medio di pazienti seguiti giornalmente 198
Peso medio del ricovero 157
PROVENIENZA
-Pronto Soccorso 462 - Reparti e DH 417 -Territorio 121
ESITO RICOVERO
- Dimessi rimanendo al proprio domicilio 811
- Deceduti al domicilio 108
- Trasferiti in ospedale 81
Per circa il 10 di questi pz egrave stata concordata con il medico di Medicina Generale la prosecuzione delle cure in Assistenza Domiciliare Integrata (ADI)
Ospedalizzazione a Domicilio
Principali patologie
Patologia bronco-polmonare 219
bullPatologia cardiaca 197
bullPatologie neurologiche 152
bullPatologie ematologiche 142
bullPatologie oncologiche 68
Ospedalizzazione a Domicilio di Torino
COSTI PER GIORNATA DI RICOVERO
AOU Cittagrave della Salute e della Scienza
Terapia intensiva 1500 euro
Ematologia 1086 euro
Medicina drsquourgenza 850 euro
Medicina 400 euro
Ospedalizzazione a domicilio 155 euro
LAVORO DI SQUADRA
PRINCIPALI COLLABORAZIONI
DEA e Med UrgenzaSC U CardiologiaSC EmatologiaSC Pneumologia
THE RAD-HOME PROJECT
Da Giugno 2008
Ospedalizzazione a Domicilio di Torino
Posizionamento di cateteri venosi centrali e periferici con ecoguida
Trasfusioni a domicilio percheacute
Vantaggi per il servizio sanitario
Riduzione dei costi
Riduzione di errori
Vantaggi per i pazienti
Miglioramento dellrsquoautonomia
Miglioramento del comfort
Riduzione del rischio infettivo
Guidelines for home transfusion Nova Scotia 2014
Sempre sicure Quali rischi
Il rischio principale egrave rappresentato dalla mancanza di una immediata disponibilitagrave di
assistenza medica intensiva in caso di evento avverso correlato alla trasfusione
Fridey 2013
Transfusions at home in patients with myelodysplasticsyndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
bull Inclusion criteria patient and disease
Caregiver
Home environment
bull Exclusion criteria patient and disease
caregiver
home environment
211 MDS patients transfusion dependent 7766 trasfusions 4980 domiciliary transfusionsHome Care program 5-years period (2006-2010)
Inclusion criteria
bull Patient living in Rome or in the near urban area covered by our HC service
bull Disease-related anemia refractory to all conventional measures
bull Physical limitations andor compromised clinical and personal status
bull Family and social problems resulting in the impossibility to travel to the hospital and to attend clinical visits and transfusion
bull Stable medical conditions
bull Adequate venous access
bull Informed and written consent
bull Responsible capable and collaborating adult suitable at home Other than a family member caregiver would be also a friend or a home-aid assistant
bull Deemed adequate and suitable for HC program In particular the home shouldbe deemed easily accessible clear comfortable and safe to perform the transfusion
bull Avalability of a functioning telephone
Patientanddisease
Caregiver
Home environment
Niscola P et al Leukemia Research 36 (2012) 684-688
Exclusion criteria
bull Patientrsquos refusalbull Urgent trasfusion in emergent clinical situationsbull Inadequate vascular accessbull Sepsisbull Anemia due to underlying causes (hemolysis active bleeding iron and
vitamins deficiency and so on) potentially resolvable by othermeasures whenever applicable
bull Positive indirect antiglobulin test and no antigen-negative donorsRBCs units (both for autoantibodies and alloantibodies)
bull Unresolved andor undiagnosed fever cardiovascular instabilityandor others active clinical illnesses
bull History of previous severe transfusion-related adverse reactions
bull Patient living alone no capable and responsible adult suitable ascaregiver
bull Poor home condidions home deemed unsafe and unsiutable fortransfusion
PatientAnddisease
Caregiver
Homeenvironment
Niscola P et al Leukemia Research 36 (2012) 684-688
Home transfusion (4980) clinical complications
Transfusions at home in patients with myelodysplastic syndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
Extravasationsvascular accessrelated hematoma 6(00012)
Fever (gt 38deg C) 2(00004)
Cardiorespiratory symptoms(fluid overload and other complications) 2(00004
Skin rash 1(00002)
Nausea and vomiting 1(00002)
Total 12(00024)
bullA maximum of 2 red blood cell units have been administred for each transfusion
bull All adverse reactions were managed at home a rapid resolution and an uncomplicated outcome wereobserved in all cases
Avantages of transfusion at home compared to hospital
bull Logistic no need to travel to the hospital no long waits for visits
bull Psychological less distressing and more comfortable in the patientrsquos ownhome environment
bull Medical less patientrsquos discomfort and energy expenditure decreasedinfections
bull QoL potential for better QoL
bull Safety and liability Higher attention and better monitoring to single patient at home potential for fewer transfusion errors and adversereactions
bull Cost free for patients and families The cost have been covered by the Public Health Care System and by a non profit organization
bull Social and economic potential for fewer days lost from work for family members
Niscola P et al Leukemia Research 36 (2012) 684-688
Disavantages of transfusion at home comparedto hospital
bull Logistic and organizational time expensive for the team
bull Medical distance from advanced medical service full reanimation measures not immediately available in anemergent situation
bull Safety and liability greater risk due to increased distancefrom hospital care and emergency services
bull Regulatory and legal concerns national and local laws and regulations should be considered before to providing the transfusion service at home
bull Costs more expensive for the health care agency
Niscola P et al Leukemia Research 36 (2012) 684-688
The hospital-at-home service (HHS) could be considered as an alternative to the traditional ward for elderly patients We aimed at evaluating the home management of elderly people requiring transfusions The ever-increasing demand on acute hospital services requires alternative methods of delivering all aspects of health care HHS demonstrated to be as efficacious as a traditional ward for elderly and functionally compromised patients The method was a retrospective descriptive study enrolling patients needing an hospital admission from 1st January 2007 to 31st December 2007 and reporting an hematological discharges diagnosis as primary or secondary diagnosis A total of 54 patients were evaluated in this study Of them 34 (629) needed a hemocomponent transfusion for a total volume of 112 blood units and 49 platelet pools Patients requiring at least one blood or platelet transfusion were more functionally compromised and presented a higher level of acute physiology and chronic health evaluation compared to the non-transfused ones The conclusion was that hematological subjects mainly the frail ones and functionally highly compromised with acute illnesses could be treated at home as an alternative of the traditional medical ward This could be the starting point for future studies that will be able to increase the power of hospital-at-home service for this type of patients
Home management of hematological patients requiring hospital admissionIsaia G1 Tibaldi V Astengo M Ladetto M Marinello R Bo M Michelis G Ruatta F Ricauda NA
Arch Gerontol Geriatr 2010 Nov-Dec51(3)309-11
The client may be appropriate for home transfusion if (CCNS 2008) bullThere is at least one previous history of transfusion in hospital without a serious adverse reaction Clients who have never had a transfusion may be considered when the physician determines the benefits of home transfusion outweigh the risks bullThere is a history of adverse transfusion reactions that are of a controllable nature (ie fever controlled with medication) bullThere are physical limitations that would require ambulance transport to hospital for transfusion or hospital admission for transfusionbullThe client is alert cooperative and able to respond appropriately to body symptoms unless otherwise determined appropriate by the physician (particularly nursing home patients and pediatrics) bullThe client has a predictable stable medical condition without significant cardiovascular compromise (unstable angina CHF) bullThe client has adequate venous accessbullThere is a history of clinically significant red cell antibodies (reactive or not) provided antibody specificities are clearly identified There should be no unresolved serological findings
Giudelines for home transfusion 2014
CLINICAL ASSESSMENT
VARESETrasfusione di sangue a domicilio grazie allrsquoinfermiere di famigliaA pochi giorni dallapprovazione della riforma della sanitagrave a Varese avviene la prima trasfusione a casa di una paziente anziana allettata Levento possibile grazie alla collaborazione del medico di base
Pubblicato il 10 agosto 2015
Consegnata dallAIL oggi lunedigrave 2 dicembre la Fiat Panda in comodato duso gratuito per le attivitagrave di terapia trasfusionale domiciliare La Spezia
MARCHE SANITA TRASFUSIONI SANGUE A DOMICILIOAncona 17 ott (Adnkronos) - La Giunta della Regione Marche ha approvato il protocollo operativo sulla terapia trasfusionale domiciliare che prevede che i pazienti affetti da gravi malattie possano effettuare le trasfusioni nella propria abitazioni anziche in ospedale Lobiettivo -ha detto lassessore regionale alla Sanita Augusto Melappioni- e quello di venire incontro alle esigenze personali e terapeutiche dei malati che si trovano in precarie condizioni di salute riducendo allo stesso tempo i costi della prestazione
Trasfusione domiciliare premio nazionale allrsquoAsp di Ragusa4 ottobre 2016Per un progetto sulla sicurezza presentato da Giovanni Garozzo direttore della UOC di Medicina Trasfusionale ed Ematologia
0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient

Numero di condizioni patologiche croniche per gruppo drsquoetagrave
E Tragni Giornale italiano di farmacoeconomia 2014
Elevato rischiodi complicanze
Elevata instabilitagraveclinica
Stabilizzazione ritardata
Recupero incompleto
Ripetuteospedalizzazioni
Altamortalitagrave
PAZIENTE ANZIANOCOMPLESSO
OSPEDALE
IATROSI AMBIENTALE
MODELLI DI OSPEDALIZZAZIONE A DOMICILIO NEL MONDO
bull Israeli Home Hospital - ISRAELE
bull Hopkins Home Hospital di Baltimora - USA
bull Peterborough Hospital at Home
bull Gloucester Hospital at Home
bull Leicester Hospital at Home scheme
bull Verdun Hospital in the Home - CANADA
bull Hospital-in-the-home program at Royal Melbourne Hospital
bull Hospital-in-the-home program at Prince of Wales Hospital-Sidney
bull Hospitalizacioacuten a domicilio di Valencia Madrid Barcellona - SPAGNA
GB
AUSTRALIA
bull Etagrave avanzata della popolazione
bull Aumento delle malattie croniche e le loro
riacutizzazioni
bull Progressi tecnologici
bull Elevata spesa sanitaria
bull Necessitagrave di contenere la spesa
OSPEDALIZZAZIONE A DOMICILIO
Lrsquo ospedalizzazione domiciliare egrave definita
come la modalitagrave attraverso cui le strutture
ospedaliere in considerazione di specifiche
valutazioni seguono con il proprio
personale direttamente a domicilio pazienti
che necessitano di prestazioni con
particolare complessitagrave tali da richiedere un
processo assistenziale di livello ospedaliero
Piano Sanitario Nazionale 2002-2004
REGIONE PIEMONTE - BOLLETTINO UFFICIALE N 14 DEL 080410Deliberazione della Giunta Regionale 16 marzo 2010 n 85-13580Attivita di continuita assistenziale organizzazione e remunerazione delle attivitadi assistenza specialistica di ospedalizzazione domiciliare
Attivitagrave di ospedalizzazione presso il domicilioSi definisce attivitagrave di ospedalizzazione presso il domicilio lrsquoorganizzazione di attivitagrave assistenziali di tipo sanitario che assicurano la cura di pazienti in fase ancora acuta in una fase di continuitagrave assistenziale trattabili presso la residenza con supporto infermieristico e medico specialistico e la presa in carico da parte di unitagrave operativa di presidio ospedaliero Si tratta ad esempio di pazienti da trattare con scompenso cardiaco in fase acuta riacutizzazione di broncopneumopatie croniche ostruttive ictus ischemici non complicati infezioni respiratorie eo urinarie scompensi glicometabolici o per altre patologie di analoga complessitagrave assistenziale Tale presa in carico comporta lrsquoassunzione della responsabilitagrave clinica del paziente nel periodo in trattamento da parte dellrsquounitagrave operativa ospedaliera che dovragrave garantire oltre che lrsquoassistenza infermieristica giornaliera anche lrsquoassistenza medica specialistica necessaria e la contattabilitagrave dello specialista presso il presidio durante tutto lrsquoarco della settimana
Ospedalizzazione a Domicilio di Torino
ATTIVITArsquo ANNO 2015
482 ricoveri
9424 visite infermieristiche
5969 visite mediche
Etagrave media dei pazienti 8407 anni (range 19-104 anni)
Durata media del ricovero 1527 giorni
Numero medio di pazienti seguiti giornalmente 198
Peso medio del ricovero 157
PROVENIENZA
-Pronto Soccorso 462 - Reparti e DH 417 -Territorio 121
ESITO RICOVERO
- Dimessi rimanendo al proprio domicilio 811
- Deceduti al domicilio 108
- Trasferiti in ospedale 81
Per circa il 10 di questi pz egrave stata concordata con il medico di Medicina Generale la prosecuzione delle cure in Assistenza Domiciliare Integrata (ADI)
Ospedalizzazione a Domicilio
Principali patologie
Patologia bronco-polmonare 219
bullPatologia cardiaca 197
bullPatologie neurologiche 152
bullPatologie ematologiche 142
bullPatologie oncologiche 68
Ospedalizzazione a Domicilio di Torino
COSTI PER GIORNATA DI RICOVERO
AOU Cittagrave della Salute e della Scienza
Terapia intensiva 1500 euro
Ematologia 1086 euro
Medicina drsquourgenza 850 euro
Medicina 400 euro
Ospedalizzazione a domicilio 155 euro
LAVORO DI SQUADRA
PRINCIPALI COLLABORAZIONI
DEA e Med UrgenzaSC U CardiologiaSC EmatologiaSC Pneumologia
THE RAD-HOME PROJECT
Da Giugno 2008
Ospedalizzazione a Domicilio di Torino
Posizionamento di cateteri venosi centrali e periferici con ecoguida
Trasfusioni a domicilio percheacute
Vantaggi per il servizio sanitario
Riduzione dei costi
Riduzione di errori
Vantaggi per i pazienti
Miglioramento dellrsquoautonomia
Miglioramento del comfort
Riduzione del rischio infettivo
Guidelines for home transfusion Nova Scotia 2014
Sempre sicure Quali rischi
Il rischio principale egrave rappresentato dalla mancanza di una immediata disponibilitagrave di
assistenza medica intensiva in caso di evento avverso correlato alla trasfusione
Fridey 2013
Transfusions at home in patients with myelodysplasticsyndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
bull Inclusion criteria patient and disease
Caregiver
Home environment
bull Exclusion criteria patient and disease
caregiver
home environment
211 MDS patients transfusion dependent 7766 trasfusions 4980 domiciliary transfusionsHome Care program 5-years period (2006-2010)
Inclusion criteria
bull Patient living in Rome or in the near urban area covered by our HC service
bull Disease-related anemia refractory to all conventional measures
bull Physical limitations andor compromised clinical and personal status
bull Family and social problems resulting in the impossibility to travel to the hospital and to attend clinical visits and transfusion
bull Stable medical conditions
bull Adequate venous access
bull Informed and written consent
bull Responsible capable and collaborating adult suitable at home Other than a family member caregiver would be also a friend or a home-aid assistant
bull Deemed adequate and suitable for HC program In particular the home shouldbe deemed easily accessible clear comfortable and safe to perform the transfusion
bull Avalability of a functioning telephone
Patientanddisease
Caregiver
Home environment
Niscola P et al Leukemia Research 36 (2012) 684-688
Exclusion criteria
bull Patientrsquos refusalbull Urgent trasfusion in emergent clinical situationsbull Inadequate vascular accessbull Sepsisbull Anemia due to underlying causes (hemolysis active bleeding iron and
vitamins deficiency and so on) potentially resolvable by othermeasures whenever applicable
bull Positive indirect antiglobulin test and no antigen-negative donorsRBCs units (both for autoantibodies and alloantibodies)
bull Unresolved andor undiagnosed fever cardiovascular instabilityandor others active clinical illnesses
bull History of previous severe transfusion-related adverse reactions
bull Patient living alone no capable and responsible adult suitable ascaregiver
bull Poor home condidions home deemed unsafe and unsiutable fortransfusion
PatientAnddisease
Caregiver
Homeenvironment
Niscola P et al Leukemia Research 36 (2012) 684-688
Home transfusion (4980) clinical complications
Transfusions at home in patients with myelodysplastic syndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
Extravasationsvascular accessrelated hematoma 6(00012)
Fever (gt 38deg C) 2(00004)
Cardiorespiratory symptoms(fluid overload and other complications) 2(00004
Skin rash 1(00002)
Nausea and vomiting 1(00002)
Total 12(00024)
bullA maximum of 2 red blood cell units have been administred for each transfusion
bull All adverse reactions were managed at home a rapid resolution and an uncomplicated outcome wereobserved in all cases
Avantages of transfusion at home compared to hospital
bull Logistic no need to travel to the hospital no long waits for visits
bull Psychological less distressing and more comfortable in the patientrsquos ownhome environment
bull Medical less patientrsquos discomfort and energy expenditure decreasedinfections
bull QoL potential for better QoL
bull Safety and liability Higher attention and better monitoring to single patient at home potential for fewer transfusion errors and adversereactions
bull Cost free for patients and families The cost have been covered by the Public Health Care System and by a non profit organization
bull Social and economic potential for fewer days lost from work for family members
Niscola P et al Leukemia Research 36 (2012) 684-688
Disavantages of transfusion at home comparedto hospital
bull Logistic and organizational time expensive for the team
bull Medical distance from advanced medical service full reanimation measures not immediately available in anemergent situation
bull Safety and liability greater risk due to increased distancefrom hospital care and emergency services
bull Regulatory and legal concerns national and local laws and regulations should be considered before to providing the transfusion service at home
bull Costs more expensive for the health care agency
Niscola P et al Leukemia Research 36 (2012) 684-688
The hospital-at-home service (HHS) could be considered as an alternative to the traditional ward for elderly patients We aimed at evaluating the home management of elderly people requiring transfusions The ever-increasing demand on acute hospital services requires alternative methods of delivering all aspects of health care HHS demonstrated to be as efficacious as a traditional ward for elderly and functionally compromised patients The method was a retrospective descriptive study enrolling patients needing an hospital admission from 1st January 2007 to 31st December 2007 and reporting an hematological discharges diagnosis as primary or secondary diagnosis A total of 54 patients were evaluated in this study Of them 34 (629) needed a hemocomponent transfusion for a total volume of 112 blood units and 49 platelet pools Patients requiring at least one blood or platelet transfusion were more functionally compromised and presented a higher level of acute physiology and chronic health evaluation compared to the non-transfused ones The conclusion was that hematological subjects mainly the frail ones and functionally highly compromised with acute illnesses could be treated at home as an alternative of the traditional medical ward This could be the starting point for future studies that will be able to increase the power of hospital-at-home service for this type of patients
Home management of hematological patients requiring hospital admissionIsaia G1 Tibaldi V Astengo M Ladetto M Marinello R Bo M Michelis G Ruatta F Ricauda NA
Arch Gerontol Geriatr 2010 Nov-Dec51(3)309-11
The client may be appropriate for home transfusion if (CCNS 2008) bullThere is at least one previous history of transfusion in hospital without a serious adverse reaction Clients who have never had a transfusion may be considered when the physician determines the benefits of home transfusion outweigh the risks bullThere is a history of adverse transfusion reactions that are of a controllable nature (ie fever controlled with medication) bullThere are physical limitations that would require ambulance transport to hospital for transfusion or hospital admission for transfusionbullThe client is alert cooperative and able to respond appropriately to body symptoms unless otherwise determined appropriate by the physician (particularly nursing home patients and pediatrics) bullThe client has a predictable stable medical condition without significant cardiovascular compromise (unstable angina CHF) bullThe client has adequate venous accessbullThere is a history of clinically significant red cell antibodies (reactive or not) provided antibody specificities are clearly identified There should be no unresolved serological findings
Giudelines for home transfusion 2014
CLINICAL ASSESSMENT
VARESETrasfusione di sangue a domicilio grazie allrsquoinfermiere di famigliaA pochi giorni dallapprovazione della riforma della sanitagrave a Varese avviene la prima trasfusione a casa di una paziente anziana allettata Levento possibile grazie alla collaborazione del medico di base
Pubblicato il 10 agosto 2015
Consegnata dallAIL oggi lunedigrave 2 dicembre la Fiat Panda in comodato duso gratuito per le attivitagrave di terapia trasfusionale domiciliare La Spezia
MARCHE SANITA TRASFUSIONI SANGUE A DOMICILIOAncona 17 ott (Adnkronos) - La Giunta della Regione Marche ha approvato il protocollo operativo sulla terapia trasfusionale domiciliare che prevede che i pazienti affetti da gravi malattie possano effettuare le trasfusioni nella propria abitazioni anziche in ospedale Lobiettivo -ha detto lassessore regionale alla Sanita Augusto Melappioni- e quello di venire incontro alle esigenze personali e terapeutiche dei malati che si trovano in precarie condizioni di salute riducendo allo stesso tempo i costi della prestazione
Trasfusione domiciliare premio nazionale allrsquoAsp di Ragusa4 ottobre 2016Per un progetto sulla sicurezza presentato da Giovanni Garozzo direttore della UOC di Medicina Trasfusionale ed Ematologia
0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient

Elevato rischiodi complicanze
Elevata instabilitagraveclinica
Stabilizzazione ritardata
Recupero incompleto
Ripetuteospedalizzazioni
Altamortalitagrave
PAZIENTE ANZIANOCOMPLESSO
OSPEDALE
IATROSI AMBIENTALE
MODELLI DI OSPEDALIZZAZIONE A DOMICILIO NEL MONDO
bull Israeli Home Hospital - ISRAELE
bull Hopkins Home Hospital di Baltimora - USA
bull Peterborough Hospital at Home
bull Gloucester Hospital at Home
bull Leicester Hospital at Home scheme
bull Verdun Hospital in the Home - CANADA
bull Hospital-in-the-home program at Royal Melbourne Hospital
bull Hospital-in-the-home program at Prince of Wales Hospital-Sidney
bull Hospitalizacioacuten a domicilio di Valencia Madrid Barcellona - SPAGNA
GB
AUSTRALIA
bull Etagrave avanzata della popolazione
bull Aumento delle malattie croniche e le loro
riacutizzazioni
bull Progressi tecnologici
bull Elevata spesa sanitaria
bull Necessitagrave di contenere la spesa
OSPEDALIZZAZIONE A DOMICILIO
Lrsquo ospedalizzazione domiciliare egrave definita
come la modalitagrave attraverso cui le strutture
ospedaliere in considerazione di specifiche
valutazioni seguono con il proprio
personale direttamente a domicilio pazienti
che necessitano di prestazioni con
particolare complessitagrave tali da richiedere un
processo assistenziale di livello ospedaliero
Piano Sanitario Nazionale 2002-2004
REGIONE PIEMONTE - BOLLETTINO UFFICIALE N 14 DEL 080410Deliberazione della Giunta Regionale 16 marzo 2010 n 85-13580Attivita di continuita assistenziale organizzazione e remunerazione delle attivitadi assistenza specialistica di ospedalizzazione domiciliare
Attivitagrave di ospedalizzazione presso il domicilioSi definisce attivitagrave di ospedalizzazione presso il domicilio lrsquoorganizzazione di attivitagrave assistenziali di tipo sanitario che assicurano la cura di pazienti in fase ancora acuta in una fase di continuitagrave assistenziale trattabili presso la residenza con supporto infermieristico e medico specialistico e la presa in carico da parte di unitagrave operativa di presidio ospedaliero Si tratta ad esempio di pazienti da trattare con scompenso cardiaco in fase acuta riacutizzazione di broncopneumopatie croniche ostruttive ictus ischemici non complicati infezioni respiratorie eo urinarie scompensi glicometabolici o per altre patologie di analoga complessitagrave assistenziale Tale presa in carico comporta lrsquoassunzione della responsabilitagrave clinica del paziente nel periodo in trattamento da parte dellrsquounitagrave operativa ospedaliera che dovragrave garantire oltre che lrsquoassistenza infermieristica giornaliera anche lrsquoassistenza medica specialistica necessaria e la contattabilitagrave dello specialista presso il presidio durante tutto lrsquoarco della settimana
Ospedalizzazione a Domicilio di Torino
ATTIVITArsquo ANNO 2015
482 ricoveri
9424 visite infermieristiche
5969 visite mediche
Etagrave media dei pazienti 8407 anni (range 19-104 anni)
Durata media del ricovero 1527 giorni
Numero medio di pazienti seguiti giornalmente 198
Peso medio del ricovero 157
PROVENIENZA
-Pronto Soccorso 462 - Reparti e DH 417 -Territorio 121
ESITO RICOVERO
- Dimessi rimanendo al proprio domicilio 811
- Deceduti al domicilio 108
- Trasferiti in ospedale 81
Per circa il 10 di questi pz egrave stata concordata con il medico di Medicina Generale la prosecuzione delle cure in Assistenza Domiciliare Integrata (ADI)
Ospedalizzazione a Domicilio
Principali patologie
Patologia bronco-polmonare 219
bullPatologia cardiaca 197
bullPatologie neurologiche 152
bullPatologie ematologiche 142
bullPatologie oncologiche 68
Ospedalizzazione a Domicilio di Torino
COSTI PER GIORNATA DI RICOVERO
AOU Cittagrave della Salute e della Scienza
Terapia intensiva 1500 euro
Ematologia 1086 euro
Medicina drsquourgenza 850 euro
Medicina 400 euro
Ospedalizzazione a domicilio 155 euro
LAVORO DI SQUADRA
PRINCIPALI COLLABORAZIONI
DEA e Med UrgenzaSC U CardiologiaSC EmatologiaSC Pneumologia
THE RAD-HOME PROJECT
Da Giugno 2008
Ospedalizzazione a Domicilio di Torino
Posizionamento di cateteri venosi centrali e periferici con ecoguida
Trasfusioni a domicilio percheacute
Vantaggi per il servizio sanitario
Riduzione dei costi
Riduzione di errori
Vantaggi per i pazienti
Miglioramento dellrsquoautonomia
Miglioramento del comfort
Riduzione del rischio infettivo
Guidelines for home transfusion Nova Scotia 2014
Sempre sicure Quali rischi
Il rischio principale egrave rappresentato dalla mancanza di una immediata disponibilitagrave di
assistenza medica intensiva in caso di evento avverso correlato alla trasfusione
Fridey 2013
Transfusions at home in patients with myelodysplasticsyndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
bull Inclusion criteria patient and disease
Caregiver
Home environment
bull Exclusion criteria patient and disease
caregiver
home environment
211 MDS patients transfusion dependent 7766 trasfusions 4980 domiciliary transfusionsHome Care program 5-years period (2006-2010)
Inclusion criteria
bull Patient living in Rome or in the near urban area covered by our HC service
bull Disease-related anemia refractory to all conventional measures
bull Physical limitations andor compromised clinical and personal status
bull Family and social problems resulting in the impossibility to travel to the hospital and to attend clinical visits and transfusion
bull Stable medical conditions
bull Adequate venous access
bull Informed and written consent
bull Responsible capable and collaborating adult suitable at home Other than a family member caregiver would be also a friend or a home-aid assistant
bull Deemed adequate and suitable for HC program In particular the home shouldbe deemed easily accessible clear comfortable and safe to perform the transfusion
bull Avalability of a functioning telephone
Patientanddisease
Caregiver
Home environment
Niscola P et al Leukemia Research 36 (2012) 684-688
Exclusion criteria
bull Patientrsquos refusalbull Urgent trasfusion in emergent clinical situationsbull Inadequate vascular accessbull Sepsisbull Anemia due to underlying causes (hemolysis active bleeding iron and
vitamins deficiency and so on) potentially resolvable by othermeasures whenever applicable
bull Positive indirect antiglobulin test and no antigen-negative donorsRBCs units (both for autoantibodies and alloantibodies)
bull Unresolved andor undiagnosed fever cardiovascular instabilityandor others active clinical illnesses
bull History of previous severe transfusion-related adverse reactions
bull Patient living alone no capable and responsible adult suitable ascaregiver
bull Poor home condidions home deemed unsafe and unsiutable fortransfusion
PatientAnddisease
Caregiver
Homeenvironment
Niscola P et al Leukemia Research 36 (2012) 684-688
Home transfusion (4980) clinical complications
Transfusions at home in patients with myelodysplastic syndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
Extravasationsvascular accessrelated hematoma 6(00012)
Fever (gt 38deg C) 2(00004)
Cardiorespiratory symptoms(fluid overload and other complications) 2(00004
Skin rash 1(00002)
Nausea and vomiting 1(00002)
Total 12(00024)
bullA maximum of 2 red blood cell units have been administred for each transfusion
bull All adverse reactions were managed at home a rapid resolution and an uncomplicated outcome wereobserved in all cases
Avantages of transfusion at home compared to hospital
bull Logistic no need to travel to the hospital no long waits for visits
bull Psychological less distressing and more comfortable in the patientrsquos ownhome environment
bull Medical less patientrsquos discomfort and energy expenditure decreasedinfections
bull QoL potential for better QoL
bull Safety and liability Higher attention and better monitoring to single patient at home potential for fewer transfusion errors and adversereactions
bull Cost free for patients and families The cost have been covered by the Public Health Care System and by a non profit organization
bull Social and economic potential for fewer days lost from work for family members
Niscola P et al Leukemia Research 36 (2012) 684-688
Disavantages of transfusion at home comparedto hospital
bull Logistic and organizational time expensive for the team
bull Medical distance from advanced medical service full reanimation measures not immediately available in anemergent situation
bull Safety and liability greater risk due to increased distancefrom hospital care and emergency services
bull Regulatory and legal concerns national and local laws and regulations should be considered before to providing the transfusion service at home
bull Costs more expensive for the health care agency
Niscola P et al Leukemia Research 36 (2012) 684-688
The hospital-at-home service (HHS) could be considered as an alternative to the traditional ward for elderly patients We aimed at evaluating the home management of elderly people requiring transfusions The ever-increasing demand on acute hospital services requires alternative methods of delivering all aspects of health care HHS demonstrated to be as efficacious as a traditional ward for elderly and functionally compromised patients The method was a retrospective descriptive study enrolling patients needing an hospital admission from 1st January 2007 to 31st December 2007 and reporting an hematological discharges diagnosis as primary or secondary diagnosis A total of 54 patients were evaluated in this study Of them 34 (629) needed a hemocomponent transfusion for a total volume of 112 blood units and 49 platelet pools Patients requiring at least one blood or platelet transfusion were more functionally compromised and presented a higher level of acute physiology and chronic health evaluation compared to the non-transfused ones The conclusion was that hematological subjects mainly the frail ones and functionally highly compromised with acute illnesses could be treated at home as an alternative of the traditional medical ward This could be the starting point for future studies that will be able to increase the power of hospital-at-home service for this type of patients
Home management of hematological patients requiring hospital admissionIsaia G1 Tibaldi V Astengo M Ladetto M Marinello R Bo M Michelis G Ruatta F Ricauda NA
Arch Gerontol Geriatr 2010 Nov-Dec51(3)309-11
The client may be appropriate for home transfusion if (CCNS 2008) bullThere is at least one previous history of transfusion in hospital without a serious adverse reaction Clients who have never had a transfusion may be considered when the physician determines the benefits of home transfusion outweigh the risks bullThere is a history of adverse transfusion reactions that are of a controllable nature (ie fever controlled with medication) bullThere are physical limitations that would require ambulance transport to hospital for transfusion or hospital admission for transfusionbullThe client is alert cooperative and able to respond appropriately to body symptoms unless otherwise determined appropriate by the physician (particularly nursing home patients and pediatrics) bullThe client has a predictable stable medical condition without significant cardiovascular compromise (unstable angina CHF) bullThe client has adequate venous accessbullThere is a history of clinically significant red cell antibodies (reactive or not) provided antibody specificities are clearly identified There should be no unresolved serological findings
Giudelines for home transfusion 2014
CLINICAL ASSESSMENT
VARESETrasfusione di sangue a domicilio grazie allrsquoinfermiere di famigliaA pochi giorni dallapprovazione della riforma della sanitagrave a Varese avviene la prima trasfusione a casa di una paziente anziana allettata Levento possibile grazie alla collaborazione del medico di base
Pubblicato il 10 agosto 2015
Consegnata dallAIL oggi lunedigrave 2 dicembre la Fiat Panda in comodato duso gratuito per le attivitagrave di terapia trasfusionale domiciliare La Spezia
MARCHE SANITA TRASFUSIONI SANGUE A DOMICILIOAncona 17 ott (Adnkronos) - La Giunta della Regione Marche ha approvato il protocollo operativo sulla terapia trasfusionale domiciliare che prevede che i pazienti affetti da gravi malattie possano effettuare le trasfusioni nella propria abitazioni anziche in ospedale Lobiettivo -ha detto lassessore regionale alla Sanita Augusto Melappioni- e quello di venire incontro alle esigenze personali e terapeutiche dei malati che si trovano in precarie condizioni di salute riducendo allo stesso tempo i costi della prestazione
Trasfusione domiciliare premio nazionale allrsquoAsp di Ragusa4 ottobre 2016Per un progetto sulla sicurezza presentato da Giovanni Garozzo direttore della UOC di Medicina Trasfusionale ed Ematologia
0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient

MODELLI DI OSPEDALIZZAZIONE A DOMICILIO NEL MONDO
bull Israeli Home Hospital - ISRAELE
bull Hopkins Home Hospital di Baltimora - USA
bull Peterborough Hospital at Home
bull Gloucester Hospital at Home
bull Leicester Hospital at Home scheme
bull Verdun Hospital in the Home - CANADA
bull Hospital-in-the-home program at Royal Melbourne Hospital
bull Hospital-in-the-home program at Prince of Wales Hospital-Sidney
bull Hospitalizacioacuten a domicilio di Valencia Madrid Barcellona - SPAGNA
GB
AUSTRALIA
bull Etagrave avanzata della popolazione
bull Aumento delle malattie croniche e le loro
riacutizzazioni
bull Progressi tecnologici
bull Elevata spesa sanitaria
bull Necessitagrave di contenere la spesa
OSPEDALIZZAZIONE A DOMICILIO
Lrsquo ospedalizzazione domiciliare egrave definita
come la modalitagrave attraverso cui le strutture
ospedaliere in considerazione di specifiche
valutazioni seguono con il proprio
personale direttamente a domicilio pazienti
che necessitano di prestazioni con
particolare complessitagrave tali da richiedere un
processo assistenziale di livello ospedaliero
Piano Sanitario Nazionale 2002-2004
REGIONE PIEMONTE - BOLLETTINO UFFICIALE N 14 DEL 080410Deliberazione della Giunta Regionale 16 marzo 2010 n 85-13580Attivita di continuita assistenziale organizzazione e remunerazione delle attivitadi assistenza specialistica di ospedalizzazione domiciliare
Attivitagrave di ospedalizzazione presso il domicilioSi definisce attivitagrave di ospedalizzazione presso il domicilio lrsquoorganizzazione di attivitagrave assistenziali di tipo sanitario che assicurano la cura di pazienti in fase ancora acuta in una fase di continuitagrave assistenziale trattabili presso la residenza con supporto infermieristico e medico specialistico e la presa in carico da parte di unitagrave operativa di presidio ospedaliero Si tratta ad esempio di pazienti da trattare con scompenso cardiaco in fase acuta riacutizzazione di broncopneumopatie croniche ostruttive ictus ischemici non complicati infezioni respiratorie eo urinarie scompensi glicometabolici o per altre patologie di analoga complessitagrave assistenziale Tale presa in carico comporta lrsquoassunzione della responsabilitagrave clinica del paziente nel periodo in trattamento da parte dellrsquounitagrave operativa ospedaliera che dovragrave garantire oltre che lrsquoassistenza infermieristica giornaliera anche lrsquoassistenza medica specialistica necessaria e la contattabilitagrave dello specialista presso il presidio durante tutto lrsquoarco della settimana
Ospedalizzazione a Domicilio di Torino
ATTIVITArsquo ANNO 2015
482 ricoveri
9424 visite infermieristiche
5969 visite mediche
Etagrave media dei pazienti 8407 anni (range 19-104 anni)
Durata media del ricovero 1527 giorni
Numero medio di pazienti seguiti giornalmente 198
Peso medio del ricovero 157
PROVENIENZA
-Pronto Soccorso 462 - Reparti e DH 417 -Territorio 121
ESITO RICOVERO
- Dimessi rimanendo al proprio domicilio 811
- Deceduti al domicilio 108
- Trasferiti in ospedale 81
Per circa il 10 di questi pz egrave stata concordata con il medico di Medicina Generale la prosecuzione delle cure in Assistenza Domiciliare Integrata (ADI)
Ospedalizzazione a Domicilio
Principali patologie
Patologia bronco-polmonare 219
bullPatologia cardiaca 197
bullPatologie neurologiche 152
bullPatologie ematologiche 142
bullPatologie oncologiche 68
Ospedalizzazione a Domicilio di Torino
COSTI PER GIORNATA DI RICOVERO
AOU Cittagrave della Salute e della Scienza
Terapia intensiva 1500 euro
Ematologia 1086 euro
Medicina drsquourgenza 850 euro
Medicina 400 euro
Ospedalizzazione a domicilio 155 euro
LAVORO DI SQUADRA
PRINCIPALI COLLABORAZIONI
DEA e Med UrgenzaSC U CardiologiaSC EmatologiaSC Pneumologia
THE RAD-HOME PROJECT
Da Giugno 2008
Ospedalizzazione a Domicilio di Torino
Posizionamento di cateteri venosi centrali e periferici con ecoguida
Trasfusioni a domicilio percheacute
Vantaggi per il servizio sanitario
Riduzione dei costi
Riduzione di errori
Vantaggi per i pazienti
Miglioramento dellrsquoautonomia
Miglioramento del comfort
Riduzione del rischio infettivo
Guidelines for home transfusion Nova Scotia 2014
Sempre sicure Quali rischi
Il rischio principale egrave rappresentato dalla mancanza di una immediata disponibilitagrave di
assistenza medica intensiva in caso di evento avverso correlato alla trasfusione
Fridey 2013
Transfusions at home in patients with myelodysplasticsyndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
bull Inclusion criteria patient and disease
Caregiver
Home environment
bull Exclusion criteria patient and disease
caregiver
home environment
211 MDS patients transfusion dependent 7766 trasfusions 4980 domiciliary transfusionsHome Care program 5-years period (2006-2010)
Inclusion criteria
bull Patient living in Rome or in the near urban area covered by our HC service
bull Disease-related anemia refractory to all conventional measures
bull Physical limitations andor compromised clinical and personal status
bull Family and social problems resulting in the impossibility to travel to the hospital and to attend clinical visits and transfusion
bull Stable medical conditions
bull Adequate venous access
bull Informed and written consent
bull Responsible capable and collaborating adult suitable at home Other than a family member caregiver would be also a friend or a home-aid assistant
bull Deemed adequate and suitable for HC program In particular the home shouldbe deemed easily accessible clear comfortable and safe to perform the transfusion
bull Avalability of a functioning telephone
Patientanddisease
Caregiver
Home environment
Niscola P et al Leukemia Research 36 (2012) 684-688
Exclusion criteria
bull Patientrsquos refusalbull Urgent trasfusion in emergent clinical situationsbull Inadequate vascular accessbull Sepsisbull Anemia due to underlying causes (hemolysis active bleeding iron and
vitamins deficiency and so on) potentially resolvable by othermeasures whenever applicable
bull Positive indirect antiglobulin test and no antigen-negative donorsRBCs units (both for autoantibodies and alloantibodies)
bull Unresolved andor undiagnosed fever cardiovascular instabilityandor others active clinical illnesses
bull History of previous severe transfusion-related adverse reactions
bull Patient living alone no capable and responsible adult suitable ascaregiver
bull Poor home condidions home deemed unsafe and unsiutable fortransfusion
PatientAnddisease
Caregiver
Homeenvironment
Niscola P et al Leukemia Research 36 (2012) 684-688
Home transfusion (4980) clinical complications
Transfusions at home in patients with myelodysplastic syndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
Extravasationsvascular accessrelated hematoma 6(00012)
Fever (gt 38deg C) 2(00004)
Cardiorespiratory symptoms(fluid overload and other complications) 2(00004
Skin rash 1(00002)
Nausea and vomiting 1(00002)
Total 12(00024)
bullA maximum of 2 red blood cell units have been administred for each transfusion
bull All adverse reactions were managed at home a rapid resolution and an uncomplicated outcome wereobserved in all cases
Avantages of transfusion at home compared to hospital
bull Logistic no need to travel to the hospital no long waits for visits
bull Psychological less distressing and more comfortable in the patientrsquos ownhome environment
bull Medical less patientrsquos discomfort and energy expenditure decreasedinfections
bull QoL potential for better QoL
bull Safety and liability Higher attention and better monitoring to single patient at home potential for fewer transfusion errors and adversereactions
bull Cost free for patients and families The cost have been covered by the Public Health Care System and by a non profit organization
bull Social and economic potential for fewer days lost from work for family members
Niscola P et al Leukemia Research 36 (2012) 684-688
Disavantages of transfusion at home comparedto hospital
bull Logistic and organizational time expensive for the team
bull Medical distance from advanced medical service full reanimation measures not immediately available in anemergent situation
bull Safety and liability greater risk due to increased distancefrom hospital care and emergency services
bull Regulatory and legal concerns national and local laws and regulations should be considered before to providing the transfusion service at home
bull Costs more expensive for the health care agency
Niscola P et al Leukemia Research 36 (2012) 684-688
The hospital-at-home service (HHS) could be considered as an alternative to the traditional ward for elderly patients We aimed at evaluating the home management of elderly people requiring transfusions The ever-increasing demand on acute hospital services requires alternative methods of delivering all aspects of health care HHS demonstrated to be as efficacious as a traditional ward for elderly and functionally compromised patients The method was a retrospective descriptive study enrolling patients needing an hospital admission from 1st January 2007 to 31st December 2007 and reporting an hematological discharges diagnosis as primary or secondary diagnosis A total of 54 patients were evaluated in this study Of them 34 (629) needed a hemocomponent transfusion for a total volume of 112 blood units and 49 platelet pools Patients requiring at least one blood or platelet transfusion were more functionally compromised and presented a higher level of acute physiology and chronic health evaluation compared to the non-transfused ones The conclusion was that hematological subjects mainly the frail ones and functionally highly compromised with acute illnesses could be treated at home as an alternative of the traditional medical ward This could be the starting point for future studies that will be able to increase the power of hospital-at-home service for this type of patients
Home management of hematological patients requiring hospital admissionIsaia G1 Tibaldi V Astengo M Ladetto M Marinello R Bo M Michelis G Ruatta F Ricauda NA
Arch Gerontol Geriatr 2010 Nov-Dec51(3)309-11
The client may be appropriate for home transfusion if (CCNS 2008) bullThere is at least one previous history of transfusion in hospital without a serious adverse reaction Clients who have never had a transfusion may be considered when the physician determines the benefits of home transfusion outweigh the risks bullThere is a history of adverse transfusion reactions that are of a controllable nature (ie fever controlled with medication) bullThere are physical limitations that would require ambulance transport to hospital for transfusion or hospital admission for transfusionbullThe client is alert cooperative and able to respond appropriately to body symptoms unless otherwise determined appropriate by the physician (particularly nursing home patients and pediatrics) bullThe client has a predictable stable medical condition without significant cardiovascular compromise (unstable angina CHF) bullThe client has adequate venous accessbullThere is a history of clinically significant red cell antibodies (reactive or not) provided antibody specificities are clearly identified There should be no unresolved serological findings
Giudelines for home transfusion 2014
CLINICAL ASSESSMENT
VARESETrasfusione di sangue a domicilio grazie allrsquoinfermiere di famigliaA pochi giorni dallapprovazione della riforma della sanitagrave a Varese avviene la prima trasfusione a casa di una paziente anziana allettata Levento possibile grazie alla collaborazione del medico di base
Pubblicato il 10 agosto 2015
Consegnata dallAIL oggi lunedigrave 2 dicembre la Fiat Panda in comodato duso gratuito per le attivitagrave di terapia trasfusionale domiciliare La Spezia
MARCHE SANITA TRASFUSIONI SANGUE A DOMICILIOAncona 17 ott (Adnkronos) - La Giunta della Regione Marche ha approvato il protocollo operativo sulla terapia trasfusionale domiciliare che prevede che i pazienti affetti da gravi malattie possano effettuare le trasfusioni nella propria abitazioni anziche in ospedale Lobiettivo -ha detto lassessore regionale alla Sanita Augusto Melappioni- e quello di venire incontro alle esigenze personali e terapeutiche dei malati che si trovano in precarie condizioni di salute riducendo allo stesso tempo i costi della prestazione
Trasfusione domiciliare premio nazionale allrsquoAsp di Ragusa4 ottobre 2016Per un progetto sulla sicurezza presentato da Giovanni Garozzo direttore della UOC di Medicina Trasfusionale ed Ematologia
0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient
bull Etagrave avanzata della popolazione
bull Aumento delle malattie croniche e le loro
riacutizzazioni
bull Progressi tecnologici
bull Elevata spesa sanitaria
bull Necessitagrave di contenere la spesa
OSPEDALIZZAZIONE A DOMICILIO
Lrsquo ospedalizzazione domiciliare egrave definita
come la modalitagrave attraverso cui le strutture
ospedaliere in considerazione di specifiche
valutazioni seguono con il proprio
personale direttamente a domicilio pazienti
che necessitano di prestazioni con
particolare complessitagrave tali da richiedere un
processo assistenziale di livello ospedaliero
Piano Sanitario Nazionale 2002-2004
REGIONE PIEMONTE - BOLLETTINO UFFICIALE N 14 DEL 080410Deliberazione della Giunta Regionale 16 marzo 2010 n 85-13580Attivita di continuita assistenziale organizzazione e remunerazione delle attivitadi assistenza specialistica di ospedalizzazione domiciliare
Attivitagrave di ospedalizzazione presso il domicilioSi definisce attivitagrave di ospedalizzazione presso il domicilio lrsquoorganizzazione di attivitagrave assistenziali di tipo sanitario che assicurano la cura di pazienti in fase ancora acuta in una fase di continuitagrave assistenziale trattabili presso la residenza con supporto infermieristico e medico specialistico e la presa in carico da parte di unitagrave operativa di presidio ospedaliero Si tratta ad esempio di pazienti da trattare con scompenso cardiaco in fase acuta riacutizzazione di broncopneumopatie croniche ostruttive ictus ischemici non complicati infezioni respiratorie eo urinarie scompensi glicometabolici o per altre patologie di analoga complessitagrave assistenziale Tale presa in carico comporta lrsquoassunzione della responsabilitagrave clinica del paziente nel periodo in trattamento da parte dellrsquounitagrave operativa ospedaliera che dovragrave garantire oltre che lrsquoassistenza infermieristica giornaliera anche lrsquoassistenza medica specialistica necessaria e la contattabilitagrave dello specialista presso il presidio durante tutto lrsquoarco della settimana
Ospedalizzazione a Domicilio di Torino
ATTIVITArsquo ANNO 2015
482 ricoveri
9424 visite infermieristiche
5969 visite mediche
Etagrave media dei pazienti 8407 anni (range 19-104 anni)
Durata media del ricovero 1527 giorni
Numero medio di pazienti seguiti giornalmente 198
Peso medio del ricovero 157
PROVENIENZA
-Pronto Soccorso 462 - Reparti e DH 417 -Territorio 121
ESITO RICOVERO
- Dimessi rimanendo al proprio domicilio 811
- Deceduti al domicilio 108
- Trasferiti in ospedale 81
Per circa il 10 di questi pz egrave stata concordata con il medico di Medicina Generale la prosecuzione delle cure in Assistenza Domiciliare Integrata (ADI)
Ospedalizzazione a Domicilio
Principali patologie
Patologia bronco-polmonare 219
bullPatologia cardiaca 197
bullPatologie neurologiche 152
bullPatologie ematologiche 142
bullPatologie oncologiche 68
Ospedalizzazione a Domicilio di Torino
COSTI PER GIORNATA DI RICOVERO
AOU Cittagrave della Salute e della Scienza
Terapia intensiva 1500 euro
Ematologia 1086 euro
Medicina drsquourgenza 850 euro
Medicina 400 euro
Ospedalizzazione a domicilio 155 euro
LAVORO DI SQUADRA
PRINCIPALI COLLABORAZIONI
DEA e Med UrgenzaSC U CardiologiaSC EmatologiaSC Pneumologia
THE RAD-HOME PROJECT
Da Giugno 2008
Ospedalizzazione a Domicilio di Torino
Posizionamento di cateteri venosi centrali e periferici con ecoguida
Trasfusioni a domicilio percheacute
Vantaggi per il servizio sanitario
Riduzione dei costi
Riduzione di errori
Vantaggi per i pazienti
Miglioramento dellrsquoautonomia
Miglioramento del comfort
Riduzione del rischio infettivo
Guidelines for home transfusion Nova Scotia 2014
Sempre sicure Quali rischi
Il rischio principale egrave rappresentato dalla mancanza di una immediata disponibilitagrave di
assistenza medica intensiva in caso di evento avverso correlato alla trasfusione
Fridey 2013
Transfusions at home in patients with myelodysplasticsyndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
bull Inclusion criteria patient and disease
Caregiver
Home environment
bull Exclusion criteria patient and disease
caregiver
home environment
211 MDS patients transfusion dependent 7766 trasfusions 4980 domiciliary transfusionsHome Care program 5-years period (2006-2010)
Inclusion criteria
bull Patient living in Rome or in the near urban area covered by our HC service
bull Disease-related anemia refractory to all conventional measures
bull Physical limitations andor compromised clinical and personal status
bull Family and social problems resulting in the impossibility to travel to the hospital and to attend clinical visits and transfusion
bull Stable medical conditions
bull Adequate venous access
bull Informed and written consent
bull Responsible capable and collaborating adult suitable at home Other than a family member caregiver would be also a friend or a home-aid assistant
bull Deemed adequate and suitable for HC program In particular the home shouldbe deemed easily accessible clear comfortable and safe to perform the transfusion
bull Avalability of a functioning telephone
Patientanddisease
Caregiver
Home environment
Niscola P et al Leukemia Research 36 (2012) 684-688
Exclusion criteria
bull Patientrsquos refusalbull Urgent trasfusion in emergent clinical situationsbull Inadequate vascular accessbull Sepsisbull Anemia due to underlying causes (hemolysis active bleeding iron and
vitamins deficiency and so on) potentially resolvable by othermeasures whenever applicable
bull Positive indirect antiglobulin test and no antigen-negative donorsRBCs units (both for autoantibodies and alloantibodies)
bull Unresolved andor undiagnosed fever cardiovascular instabilityandor others active clinical illnesses
bull History of previous severe transfusion-related adverse reactions
bull Patient living alone no capable and responsible adult suitable ascaregiver
bull Poor home condidions home deemed unsafe and unsiutable fortransfusion
PatientAnddisease
Caregiver
Homeenvironment
Niscola P et al Leukemia Research 36 (2012) 684-688
Home transfusion (4980) clinical complications
Transfusions at home in patients with myelodysplastic syndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
Extravasationsvascular accessrelated hematoma 6(00012)
Fever (gt 38deg C) 2(00004)
Cardiorespiratory symptoms(fluid overload and other complications) 2(00004
Skin rash 1(00002)
Nausea and vomiting 1(00002)
Total 12(00024)
bullA maximum of 2 red blood cell units have been administred for each transfusion
bull All adverse reactions were managed at home a rapid resolution and an uncomplicated outcome wereobserved in all cases
Avantages of transfusion at home compared to hospital
bull Logistic no need to travel to the hospital no long waits for visits
bull Psychological less distressing and more comfortable in the patientrsquos ownhome environment
bull Medical less patientrsquos discomfort and energy expenditure decreasedinfections
bull QoL potential for better QoL
bull Safety and liability Higher attention and better monitoring to single patient at home potential for fewer transfusion errors and adversereactions
bull Cost free for patients and families The cost have been covered by the Public Health Care System and by a non profit organization
bull Social and economic potential for fewer days lost from work for family members
Niscola P et al Leukemia Research 36 (2012) 684-688
Disavantages of transfusion at home comparedto hospital
bull Logistic and organizational time expensive for the team
bull Medical distance from advanced medical service full reanimation measures not immediately available in anemergent situation
bull Safety and liability greater risk due to increased distancefrom hospital care and emergency services
bull Regulatory and legal concerns national and local laws and regulations should be considered before to providing the transfusion service at home
bull Costs more expensive for the health care agency
Niscola P et al Leukemia Research 36 (2012) 684-688
The hospital-at-home service (HHS) could be considered as an alternative to the traditional ward for elderly patients We aimed at evaluating the home management of elderly people requiring transfusions The ever-increasing demand on acute hospital services requires alternative methods of delivering all aspects of health care HHS demonstrated to be as efficacious as a traditional ward for elderly and functionally compromised patients The method was a retrospective descriptive study enrolling patients needing an hospital admission from 1st January 2007 to 31st December 2007 and reporting an hematological discharges diagnosis as primary or secondary diagnosis A total of 54 patients were evaluated in this study Of them 34 (629) needed a hemocomponent transfusion for a total volume of 112 blood units and 49 platelet pools Patients requiring at least one blood or platelet transfusion were more functionally compromised and presented a higher level of acute physiology and chronic health evaluation compared to the non-transfused ones The conclusion was that hematological subjects mainly the frail ones and functionally highly compromised with acute illnesses could be treated at home as an alternative of the traditional medical ward This could be the starting point for future studies that will be able to increase the power of hospital-at-home service for this type of patients
Home management of hematological patients requiring hospital admissionIsaia G1 Tibaldi V Astengo M Ladetto M Marinello R Bo M Michelis G Ruatta F Ricauda NA
Arch Gerontol Geriatr 2010 Nov-Dec51(3)309-11
The client may be appropriate for home transfusion if (CCNS 2008) bullThere is at least one previous history of transfusion in hospital without a serious adverse reaction Clients who have never had a transfusion may be considered when the physician determines the benefits of home transfusion outweigh the risks bullThere is a history of adverse transfusion reactions that are of a controllable nature (ie fever controlled with medication) bullThere are physical limitations that would require ambulance transport to hospital for transfusion or hospital admission for transfusionbullThe client is alert cooperative and able to respond appropriately to body symptoms unless otherwise determined appropriate by the physician (particularly nursing home patients and pediatrics) bullThe client has a predictable stable medical condition without significant cardiovascular compromise (unstable angina CHF) bullThe client has adequate venous accessbullThere is a history of clinically significant red cell antibodies (reactive or not) provided antibody specificities are clearly identified There should be no unresolved serological findings
Giudelines for home transfusion 2014
CLINICAL ASSESSMENT
VARESETrasfusione di sangue a domicilio grazie allrsquoinfermiere di famigliaA pochi giorni dallapprovazione della riforma della sanitagrave a Varese avviene la prima trasfusione a casa di una paziente anziana allettata Levento possibile grazie alla collaborazione del medico di base
Pubblicato il 10 agosto 2015
Consegnata dallAIL oggi lunedigrave 2 dicembre la Fiat Panda in comodato duso gratuito per le attivitagrave di terapia trasfusionale domiciliare La Spezia
MARCHE SANITA TRASFUSIONI SANGUE A DOMICILIOAncona 17 ott (Adnkronos) - La Giunta della Regione Marche ha approvato il protocollo operativo sulla terapia trasfusionale domiciliare che prevede che i pazienti affetti da gravi malattie possano effettuare le trasfusioni nella propria abitazioni anziche in ospedale Lobiettivo -ha detto lassessore regionale alla Sanita Augusto Melappioni- e quello di venire incontro alle esigenze personali e terapeutiche dei malati che si trovano in precarie condizioni di salute riducendo allo stesso tempo i costi della prestazione
Trasfusione domiciliare premio nazionale allrsquoAsp di Ragusa4 ottobre 2016Per un progetto sulla sicurezza presentato da Giovanni Garozzo direttore della UOC di Medicina Trasfusionale ed Ematologia
0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient

OSPEDALIZZAZIONE A DOMICILIO
Lrsquo ospedalizzazione domiciliare egrave definita
come la modalitagrave attraverso cui le strutture
ospedaliere in considerazione di specifiche
valutazioni seguono con il proprio
personale direttamente a domicilio pazienti
che necessitano di prestazioni con
particolare complessitagrave tali da richiedere un
processo assistenziale di livello ospedaliero
Piano Sanitario Nazionale 2002-2004
REGIONE PIEMONTE - BOLLETTINO UFFICIALE N 14 DEL 080410Deliberazione della Giunta Regionale 16 marzo 2010 n 85-13580Attivita di continuita assistenziale organizzazione e remunerazione delle attivitadi assistenza specialistica di ospedalizzazione domiciliare
Attivitagrave di ospedalizzazione presso il domicilioSi definisce attivitagrave di ospedalizzazione presso il domicilio lrsquoorganizzazione di attivitagrave assistenziali di tipo sanitario che assicurano la cura di pazienti in fase ancora acuta in una fase di continuitagrave assistenziale trattabili presso la residenza con supporto infermieristico e medico specialistico e la presa in carico da parte di unitagrave operativa di presidio ospedaliero Si tratta ad esempio di pazienti da trattare con scompenso cardiaco in fase acuta riacutizzazione di broncopneumopatie croniche ostruttive ictus ischemici non complicati infezioni respiratorie eo urinarie scompensi glicometabolici o per altre patologie di analoga complessitagrave assistenziale Tale presa in carico comporta lrsquoassunzione della responsabilitagrave clinica del paziente nel periodo in trattamento da parte dellrsquounitagrave operativa ospedaliera che dovragrave garantire oltre che lrsquoassistenza infermieristica giornaliera anche lrsquoassistenza medica specialistica necessaria e la contattabilitagrave dello specialista presso il presidio durante tutto lrsquoarco della settimana
Ospedalizzazione a Domicilio di Torino
ATTIVITArsquo ANNO 2015
482 ricoveri
9424 visite infermieristiche
5969 visite mediche
Etagrave media dei pazienti 8407 anni (range 19-104 anni)
Durata media del ricovero 1527 giorni
Numero medio di pazienti seguiti giornalmente 198
Peso medio del ricovero 157
PROVENIENZA
-Pronto Soccorso 462 - Reparti e DH 417 -Territorio 121
ESITO RICOVERO
- Dimessi rimanendo al proprio domicilio 811
- Deceduti al domicilio 108
- Trasferiti in ospedale 81
Per circa il 10 di questi pz egrave stata concordata con il medico di Medicina Generale la prosecuzione delle cure in Assistenza Domiciliare Integrata (ADI)
Ospedalizzazione a Domicilio
Principali patologie
Patologia bronco-polmonare 219
bullPatologia cardiaca 197
bullPatologie neurologiche 152
bullPatologie ematologiche 142
bullPatologie oncologiche 68
Ospedalizzazione a Domicilio di Torino
COSTI PER GIORNATA DI RICOVERO
AOU Cittagrave della Salute e della Scienza
Terapia intensiva 1500 euro
Ematologia 1086 euro
Medicina drsquourgenza 850 euro
Medicina 400 euro
Ospedalizzazione a domicilio 155 euro
LAVORO DI SQUADRA
PRINCIPALI COLLABORAZIONI
DEA e Med UrgenzaSC U CardiologiaSC EmatologiaSC Pneumologia
THE RAD-HOME PROJECT
Da Giugno 2008
Ospedalizzazione a Domicilio di Torino
Posizionamento di cateteri venosi centrali e periferici con ecoguida
Trasfusioni a domicilio percheacute
Vantaggi per il servizio sanitario
Riduzione dei costi
Riduzione di errori
Vantaggi per i pazienti
Miglioramento dellrsquoautonomia
Miglioramento del comfort
Riduzione del rischio infettivo
Guidelines for home transfusion Nova Scotia 2014
Sempre sicure Quali rischi
Il rischio principale egrave rappresentato dalla mancanza di una immediata disponibilitagrave di
assistenza medica intensiva in caso di evento avverso correlato alla trasfusione
Fridey 2013
Transfusions at home in patients with myelodysplasticsyndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
bull Inclusion criteria patient and disease
Caregiver
Home environment
bull Exclusion criteria patient and disease
caregiver
home environment
211 MDS patients transfusion dependent 7766 trasfusions 4980 domiciliary transfusionsHome Care program 5-years period (2006-2010)
Inclusion criteria
bull Patient living in Rome or in the near urban area covered by our HC service
bull Disease-related anemia refractory to all conventional measures
bull Physical limitations andor compromised clinical and personal status
bull Family and social problems resulting in the impossibility to travel to the hospital and to attend clinical visits and transfusion
bull Stable medical conditions
bull Adequate venous access
bull Informed and written consent
bull Responsible capable and collaborating adult suitable at home Other than a family member caregiver would be also a friend or a home-aid assistant
bull Deemed adequate and suitable for HC program In particular the home shouldbe deemed easily accessible clear comfortable and safe to perform the transfusion
bull Avalability of a functioning telephone
Patientanddisease
Caregiver
Home environment
Niscola P et al Leukemia Research 36 (2012) 684-688
Exclusion criteria
bull Patientrsquos refusalbull Urgent trasfusion in emergent clinical situationsbull Inadequate vascular accessbull Sepsisbull Anemia due to underlying causes (hemolysis active bleeding iron and
vitamins deficiency and so on) potentially resolvable by othermeasures whenever applicable
bull Positive indirect antiglobulin test and no antigen-negative donorsRBCs units (both for autoantibodies and alloantibodies)
bull Unresolved andor undiagnosed fever cardiovascular instabilityandor others active clinical illnesses
bull History of previous severe transfusion-related adverse reactions
bull Patient living alone no capable and responsible adult suitable ascaregiver
bull Poor home condidions home deemed unsafe and unsiutable fortransfusion
PatientAnddisease
Caregiver
Homeenvironment
Niscola P et al Leukemia Research 36 (2012) 684-688
Home transfusion (4980) clinical complications
Transfusions at home in patients with myelodysplastic syndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
Extravasationsvascular accessrelated hematoma 6(00012)
Fever (gt 38deg C) 2(00004)
Cardiorespiratory symptoms(fluid overload and other complications) 2(00004
Skin rash 1(00002)
Nausea and vomiting 1(00002)
Total 12(00024)
bullA maximum of 2 red blood cell units have been administred for each transfusion
bull All adverse reactions were managed at home a rapid resolution and an uncomplicated outcome wereobserved in all cases
Avantages of transfusion at home compared to hospital
bull Logistic no need to travel to the hospital no long waits for visits
bull Psychological less distressing and more comfortable in the patientrsquos ownhome environment
bull Medical less patientrsquos discomfort and energy expenditure decreasedinfections
bull QoL potential for better QoL
bull Safety and liability Higher attention and better monitoring to single patient at home potential for fewer transfusion errors and adversereactions
bull Cost free for patients and families The cost have been covered by the Public Health Care System and by a non profit organization
bull Social and economic potential for fewer days lost from work for family members
Niscola P et al Leukemia Research 36 (2012) 684-688
Disavantages of transfusion at home comparedto hospital
bull Logistic and organizational time expensive for the team
bull Medical distance from advanced medical service full reanimation measures not immediately available in anemergent situation
bull Safety and liability greater risk due to increased distancefrom hospital care and emergency services
bull Regulatory and legal concerns national and local laws and regulations should be considered before to providing the transfusion service at home
bull Costs more expensive for the health care agency
Niscola P et al Leukemia Research 36 (2012) 684-688
The hospital-at-home service (HHS) could be considered as an alternative to the traditional ward for elderly patients We aimed at evaluating the home management of elderly people requiring transfusions The ever-increasing demand on acute hospital services requires alternative methods of delivering all aspects of health care HHS demonstrated to be as efficacious as a traditional ward for elderly and functionally compromised patients The method was a retrospective descriptive study enrolling patients needing an hospital admission from 1st January 2007 to 31st December 2007 and reporting an hematological discharges diagnosis as primary or secondary diagnosis A total of 54 patients were evaluated in this study Of them 34 (629) needed a hemocomponent transfusion for a total volume of 112 blood units and 49 platelet pools Patients requiring at least one blood or platelet transfusion were more functionally compromised and presented a higher level of acute physiology and chronic health evaluation compared to the non-transfused ones The conclusion was that hematological subjects mainly the frail ones and functionally highly compromised with acute illnesses could be treated at home as an alternative of the traditional medical ward This could be the starting point for future studies that will be able to increase the power of hospital-at-home service for this type of patients
Home management of hematological patients requiring hospital admissionIsaia G1 Tibaldi V Astengo M Ladetto M Marinello R Bo M Michelis G Ruatta F Ricauda NA
Arch Gerontol Geriatr 2010 Nov-Dec51(3)309-11
The client may be appropriate for home transfusion if (CCNS 2008) bullThere is at least one previous history of transfusion in hospital without a serious adverse reaction Clients who have never had a transfusion may be considered when the physician determines the benefits of home transfusion outweigh the risks bullThere is a history of adverse transfusion reactions that are of a controllable nature (ie fever controlled with medication) bullThere are physical limitations that would require ambulance transport to hospital for transfusion or hospital admission for transfusionbullThe client is alert cooperative and able to respond appropriately to body symptoms unless otherwise determined appropriate by the physician (particularly nursing home patients and pediatrics) bullThe client has a predictable stable medical condition without significant cardiovascular compromise (unstable angina CHF) bullThe client has adequate venous accessbullThere is a history of clinically significant red cell antibodies (reactive or not) provided antibody specificities are clearly identified There should be no unresolved serological findings
Giudelines for home transfusion 2014
CLINICAL ASSESSMENT
VARESETrasfusione di sangue a domicilio grazie allrsquoinfermiere di famigliaA pochi giorni dallapprovazione della riforma della sanitagrave a Varese avviene la prima trasfusione a casa di una paziente anziana allettata Levento possibile grazie alla collaborazione del medico di base
Pubblicato il 10 agosto 2015
Consegnata dallAIL oggi lunedigrave 2 dicembre la Fiat Panda in comodato duso gratuito per le attivitagrave di terapia trasfusionale domiciliare La Spezia
MARCHE SANITA TRASFUSIONI SANGUE A DOMICILIOAncona 17 ott (Adnkronos) - La Giunta della Regione Marche ha approvato il protocollo operativo sulla terapia trasfusionale domiciliare che prevede che i pazienti affetti da gravi malattie possano effettuare le trasfusioni nella propria abitazioni anziche in ospedale Lobiettivo -ha detto lassessore regionale alla Sanita Augusto Melappioni- e quello di venire incontro alle esigenze personali e terapeutiche dei malati che si trovano in precarie condizioni di salute riducendo allo stesso tempo i costi della prestazione
Trasfusione domiciliare premio nazionale allrsquoAsp di Ragusa4 ottobre 2016Per un progetto sulla sicurezza presentato da Giovanni Garozzo direttore della UOC di Medicina Trasfusionale ed Ematologia
0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient

REGIONE PIEMONTE - BOLLETTINO UFFICIALE N 14 DEL 080410Deliberazione della Giunta Regionale 16 marzo 2010 n 85-13580Attivita di continuita assistenziale organizzazione e remunerazione delle attivitadi assistenza specialistica di ospedalizzazione domiciliare
Attivitagrave di ospedalizzazione presso il domicilioSi definisce attivitagrave di ospedalizzazione presso il domicilio lrsquoorganizzazione di attivitagrave assistenziali di tipo sanitario che assicurano la cura di pazienti in fase ancora acuta in una fase di continuitagrave assistenziale trattabili presso la residenza con supporto infermieristico e medico specialistico e la presa in carico da parte di unitagrave operativa di presidio ospedaliero Si tratta ad esempio di pazienti da trattare con scompenso cardiaco in fase acuta riacutizzazione di broncopneumopatie croniche ostruttive ictus ischemici non complicati infezioni respiratorie eo urinarie scompensi glicometabolici o per altre patologie di analoga complessitagrave assistenziale Tale presa in carico comporta lrsquoassunzione della responsabilitagrave clinica del paziente nel periodo in trattamento da parte dellrsquounitagrave operativa ospedaliera che dovragrave garantire oltre che lrsquoassistenza infermieristica giornaliera anche lrsquoassistenza medica specialistica necessaria e la contattabilitagrave dello specialista presso il presidio durante tutto lrsquoarco della settimana
Ospedalizzazione a Domicilio di Torino
ATTIVITArsquo ANNO 2015
482 ricoveri
9424 visite infermieristiche
5969 visite mediche
Etagrave media dei pazienti 8407 anni (range 19-104 anni)
Durata media del ricovero 1527 giorni
Numero medio di pazienti seguiti giornalmente 198
Peso medio del ricovero 157
PROVENIENZA
-Pronto Soccorso 462 - Reparti e DH 417 -Territorio 121
ESITO RICOVERO
- Dimessi rimanendo al proprio domicilio 811
- Deceduti al domicilio 108
- Trasferiti in ospedale 81
Per circa il 10 di questi pz egrave stata concordata con il medico di Medicina Generale la prosecuzione delle cure in Assistenza Domiciliare Integrata (ADI)
Ospedalizzazione a Domicilio
Principali patologie
Patologia bronco-polmonare 219
bullPatologia cardiaca 197
bullPatologie neurologiche 152
bullPatologie ematologiche 142
bullPatologie oncologiche 68
Ospedalizzazione a Domicilio di Torino
COSTI PER GIORNATA DI RICOVERO
AOU Cittagrave della Salute e della Scienza
Terapia intensiva 1500 euro
Ematologia 1086 euro
Medicina drsquourgenza 850 euro
Medicina 400 euro
Ospedalizzazione a domicilio 155 euro
LAVORO DI SQUADRA
PRINCIPALI COLLABORAZIONI
DEA e Med UrgenzaSC U CardiologiaSC EmatologiaSC Pneumologia
THE RAD-HOME PROJECT
Da Giugno 2008
Ospedalizzazione a Domicilio di Torino
Posizionamento di cateteri venosi centrali e periferici con ecoguida
Trasfusioni a domicilio percheacute
Vantaggi per il servizio sanitario
Riduzione dei costi
Riduzione di errori
Vantaggi per i pazienti
Miglioramento dellrsquoautonomia
Miglioramento del comfort
Riduzione del rischio infettivo
Guidelines for home transfusion Nova Scotia 2014
Sempre sicure Quali rischi
Il rischio principale egrave rappresentato dalla mancanza di una immediata disponibilitagrave di
assistenza medica intensiva in caso di evento avverso correlato alla trasfusione
Fridey 2013
Transfusions at home in patients with myelodysplasticsyndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
bull Inclusion criteria patient and disease
Caregiver
Home environment
bull Exclusion criteria patient and disease
caregiver
home environment
211 MDS patients transfusion dependent 7766 trasfusions 4980 domiciliary transfusionsHome Care program 5-years period (2006-2010)
Inclusion criteria
bull Patient living in Rome or in the near urban area covered by our HC service
bull Disease-related anemia refractory to all conventional measures
bull Physical limitations andor compromised clinical and personal status
bull Family and social problems resulting in the impossibility to travel to the hospital and to attend clinical visits and transfusion
bull Stable medical conditions
bull Adequate venous access
bull Informed and written consent
bull Responsible capable and collaborating adult suitable at home Other than a family member caregiver would be also a friend or a home-aid assistant
bull Deemed adequate and suitable for HC program In particular the home shouldbe deemed easily accessible clear comfortable and safe to perform the transfusion
bull Avalability of a functioning telephone
Patientanddisease
Caregiver
Home environment
Niscola P et al Leukemia Research 36 (2012) 684-688
Exclusion criteria
bull Patientrsquos refusalbull Urgent trasfusion in emergent clinical situationsbull Inadequate vascular accessbull Sepsisbull Anemia due to underlying causes (hemolysis active bleeding iron and
vitamins deficiency and so on) potentially resolvable by othermeasures whenever applicable
bull Positive indirect antiglobulin test and no antigen-negative donorsRBCs units (both for autoantibodies and alloantibodies)
bull Unresolved andor undiagnosed fever cardiovascular instabilityandor others active clinical illnesses
bull History of previous severe transfusion-related adverse reactions
bull Patient living alone no capable and responsible adult suitable ascaregiver
bull Poor home condidions home deemed unsafe and unsiutable fortransfusion
PatientAnddisease
Caregiver
Homeenvironment
Niscola P et al Leukemia Research 36 (2012) 684-688
Home transfusion (4980) clinical complications
Transfusions at home in patients with myelodysplastic syndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
Extravasationsvascular accessrelated hematoma 6(00012)
Fever (gt 38deg C) 2(00004)
Cardiorespiratory symptoms(fluid overload and other complications) 2(00004
Skin rash 1(00002)
Nausea and vomiting 1(00002)
Total 12(00024)
bullA maximum of 2 red blood cell units have been administred for each transfusion
bull All adverse reactions were managed at home a rapid resolution and an uncomplicated outcome wereobserved in all cases
Avantages of transfusion at home compared to hospital
bull Logistic no need to travel to the hospital no long waits for visits
bull Psychological less distressing and more comfortable in the patientrsquos ownhome environment
bull Medical less patientrsquos discomfort and energy expenditure decreasedinfections
bull QoL potential for better QoL
bull Safety and liability Higher attention and better monitoring to single patient at home potential for fewer transfusion errors and adversereactions
bull Cost free for patients and families The cost have been covered by the Public Health Care System and by a non profit organization
bull Social and economic potential for fewer days lost from work for family members
Niscola P et al Leukemia Research 36 (2012) 684-688
Disavantages of transfusion at home comparedto hospital
bull Logistic and organizational time expensive for the team
bull Medical distance from advanced medical service full reanimation measures not immediately available in anemergent situation
bull Safety and liability greater risk due to increased distancefrom hospital care and emergency services
bull Regulatory and legal concerns national and local laws and regulations should be considered before to providing the transfusion service at home
bull Costs more expensive for the health care agency
Niscola P et al Leukemia Research 36 (2012) 684-688
The hospital-at-home service (HHS) could be considered as an alternative to the traditional ward for elderly patients We aimed at evaluating the home management of elderly people requiring transfusions The ever-increasing demand on acute hospital services requires alternative methods of delivering all aspects of health care HHS demonstrated to be as efficacious as a traditional ward for elderly and functionally compromised patients The method was a retrospective descriptive study enrolling patients needing an hospital admission from 1st January 2007 to 31st December 2007 and reporting an hematological discharges diagnosis as primary or secondary diagnosis A total of 54 patients were evaluated in this study Of them 34 (629) needed a hemocomponent transfusion for a total volume of 112 blood units and 49 platelet pools Patients requiring at least one blood or platelet transfusion were more functionally compromised and presented a higher level of acute physiology and chronic health evaluation compared to the non-transfused ones The conclusion was that hematological subjects mainly the frail ones and functionally highly compromised with acute illnesses could be treated at home as an alternative of the traditional medical ward This could be the starting point for future studies that will be able to increase the power of hospital-at-home service for this type of patients
Home management of hematological patients requiring hospital admissionIsaia G1 Tibaldi V Astengo M Ladetto M Marinello R Bo M Michelis G Ruatta F Ricauda NA
Arch Gerontol Geriatr 2010 Nov-Dec51(3)309-11
The client may be appropriate for home transfusion if (CCNS 2008) bullThere is at least one previous history of transfusion in hospital without a serious adverse reaction Clients who have never had a transfusion may be considered when the physician determines the benefits of home transfusion outweigh the risks bullThere is a history of adverse transfusion reactions that are of a controllable nature (ie fever controlled with medication) bullThere are physical limitations that would require ambulance transport to hospital for transfusion or hospital admission for transfusionbullThe client is alert cooperative and able to respond appropriately to body symptoms unless otherwise determined appropriate by the physician (particularly nursing home patients and pediatrics) bullThe client has a predictable stable medical condition without significant cardiovascular compromise (unstable angina CHF) bullThe client has adequate venous accessbullThere is a history of clinically significant red cell antibodies (reactive or not) provided antibody specificities are clearly identified There should be no unresolved serological findings
Giudelines for home transfusion 2014
CLINICAL ASSESSMENT
VARESETrasfusione di sangue a domicilio grazie allrsquoinfermiere di famigliaA pochi giorni dallapprovazione della riforma della sanitagrave a Varese avviene la prima trasfusione a casa di una paziente anziana allettata Levento possibile grazie alla collaborazione del medico di base
Pubblicato il 10 agosto 2015
Consegnata dallAIL oggi lunedigrave 2 dicembre la Fiat Panda in comodato duso gratuito per le attivitagrave di terapia trasfusionale domiciliare La Spezia
MARCHE SANITA TRASFUSIONI SANGUE A DOMICILIOAncona 17 ott (Adnkronos) - La Giunta della Regione Marche ha approvato il protocollo operativo sulla terapia trasfusionale domiciliare che prevede che i pazienti affetti da gravi malattie possano effettuare le trasfusioni nella propria abitazioni anziche in ospedale Lobiettivo -ha detto lassessore regionale alla Sanita Augusto Melappioni- e quello di venire incontro alle esigenze personali e terapeutiche dei malati che si trovano in precarie condizioni di salute riducendo allo stesso tempo i costi della prestazione
Trasfusione domiciliare premio nazionale allrsquoAsp di Ragusa4 ottobre 2016Per un progetto sulla sicurezza presentato da Giovanni Garozzo direttore della UOC di Medicina Trasfusionale ed Ematologia
0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient

Ospedalizzazione a Domicilio di Torino
ATTIVITArsquo ANNO 2015
482 ricoveri
9424 visite infermieristiche
5969 visite mediche
Etagrave media dei pazienti 8407 anni (range 19-104 anni)
Durata media del ricovero 1527 giorni
Numero medio di pazienti seguiti giornalmente 198
Peso medio del ricovero 157
PROVENIENZA
-Pronto Soccorso 462 - Reparti e DH 417 -Territorio 121
ESITO RICOVERO
- Dimessi rimanendo al proprio domicilio 811
- Deceduti al domicilio 108
- Trasferiti in ospedale 81
Per circa il 10 di questi pz egrave stata concordata con il medico di Medicina Generale la prosecuzione delle cure in Assistenza Domiciliare Integrata (ADI)
Ospedalizzazione a Domicilio
Principali patologie
Patologia bronco-polmonare 219
bullPatologia cardiaca 197
bullPatologie neurologiche 152
bullPatologie ematologiche 142
bullPatologie oncologiche 68
Ospedalizzazione a Domicilio di Torino
COSTI PER GIORNATA DI RICOVERO
AOU Cittagrave della Salute e della Scienza
Terapia intensiva 1500 euro
Ematologia 1086 euro
Medicina drsquourgenza 850 euro
Medicina 400 euro
Ospedalizzazione a domicilio 155 euro
LAVORO DI SQUADRA
PRINCIPALI COLLABORAZIONI
DEA e Med UrgenzaSC U CardiologiaSC EmatologiaSC Pneumologia
THE RAD-HOME PROJECT
Da Giugno 2008
Ospedalizzazione a Domicilio di Torino
Posizionamento di cateteri venosi centrali e periferici con ecoguida
Trasfusioni a domicilio percheacute
Vantaggi per il servizio sanitario
Riduzione dei costi
Riduzione di errori
Vantaggi per i pazienti
Miglioramento dellrsquoautonomia
Miglioramento del comfort
Riduzione del rischio infettivo
Guidelines for home transfusion Nova Scotia 2014
Sempre sicure Quali rischi
Il rischio principale egrave rappresentato dalla mancanza di una immediata disponibilitagrave di
assistenza medica intensiva in caso di evento avverso correlato alla trasfusione
Fridey 2013
Transfusions at home in patients with myelodysplasticsyndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
bull Inclusion criteria patient and disease
Caregiver
Home environment
bull Exclusion criteria patient and disease
caregiver
home environment
211 MDS patients transfusion dependent 7766 trasfusions 4980 domiciliary transfusionsHome Care program 5-years period (2006-2010)
Inclusion criteria
bull Patient living in Rome or in the near urban area covered by our HC service
bull Disease-related anemia refractory to all conventional measures
bull Physical limitations andor compromised clinical and personal status
bull Family and social problems resulting in the impossibility to travel to the hospital and to attend clinical visits and transfusion
bull Stable medical conditions
bull Adequate venous access
bull Informed and written consent
bull Responsible capable and collaborating adult suitable at home Other than a family member caregiver would be also a friend or a home-aid assistant
bull Deemed adequate and suitable for HC program In particular the home shouldbe deemed easily accessible clear comfortable and safe to perform the transfusion
bull Avalability of a functioning telephone
Patientanddisease
Caregiver
Home environment
Niscola P et al Leukemia Research 36 (2012) 684-688
Exclusion criteria
bull Patientrsquos refusalbull Urgent trasfusion in emergent clinical situationsbull Inadequate vascular accessbull Sepsisbull Anemia due to underlying causes (hemolysis active bleeding iron and
vitamins deficiency and so on) potentially resolvable by othermeasures whenever applicable
bull Positive indirect antiglobulin test and no antigen-negative donorsRBCs units (both for autoantibodies and alloantibodies)
bull Unresolved andor undiagnosed fever cardiovascular instabilityandor others active clinical illnesses
bull History of previous severe transfusion-related adverse reactions
bull Patient living alone no capable and responsible adult suitable ascaregiver
bull Poor home condidions home deemed unsafe and unsiutable fortransfusion
PatientAnddisease
Caregiver
Homeenvironment
Niscola P et al Leukemia Research 36 (2012) 684-688
Home transfusion (4980) clinical complications
Transfusions at home in patients with myelodysplastic syndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
Extravasationsvascular accessrelated hematoma 6(00012)
Fever (gt 38deg C) 2(00004)
Cardiorespiratory symptoms(fluid overload and other complications) 2(00004
Skin rash 1(00002)
Nausea and vomiting 1(00002)
Total 12(00024)
bullA maximum of 2 red blood cell units have been administred for each transfusion
bull All adverse reactions were managed at home a rapid resolution and an uncomplicated outcome wereobserved in all cases
Avantages of transfusion at home compared to hospital
bull Logistic no need to travel to the hospital no long waits for visits
bull Psychological less distressing and more comfortable in the patientrsquos ownhome environment
bull Medical less patientrsquos discomfort and energy expenditure decreasedinfections
bull QoL potential for better QoL
bull Safety and liability Higher attention and better monitoring to single patient at home potential for fewer transfusion errors and adversereactions
bull Cost free for patients and families The cost have been covered by the Public Health Care System and by a non profit organization
bull Social and economic potential for fewer days lost from work for family members
Niscola P et al Leukemia Research 36 (2012) 684-688
Disavantages of transfusion at home comparedto hospital
bull Logistic and organizational time expensive for the team
bull Medical distance from advanced medical service full reanimation measures not immediately available in anemergent situation
bull Safety and liability greater risk due to increased distancefrom hospital care and emergency services
bull Regulatory and legal concerns national and local laws and regulations should be considered before to providing the transfusion service at home
bull Costs more expensive for the health care agency
Niscola P et al Leukemia Research 36 (2012) 684-688
The hospital-at-home service (HHS) could be considered as an alternative to the traditional ward for elderly patients We aimed at evaluating the home management of elderly people requiring transfusions The ever-increasing demand on acute hospital services requires alternative methods of delivering all aspects of health care HHS demonstrated to be as efficacious as a traditional ward for elderly and functionally compromised patients The method was a retrospective descriptive study enrolling patients needing an hospital admission from 1st January 2007 to 31st December 2007 and reporting an hematological discharges diagnosis as primary or secondary diagnosis A total of 54 patients were evaluated in this study Of them 34 (629) needed a hemocomponent transfusion for a total volume of 112 blood units and 49 platelet pools Patients requiring at least one blood or platelet transfusion were more functionally compromised and presented a higher level of acute physiology and chronic health evaluation compared to the non-transfused ones The conclusion was that hematological subjects mainly the frail ones and functionally highly compromised with acute illnesses could be treated at home as an alternative of the traditional medical ward This could be the starting point for future studies that will be able to increase the power of hospital-at-home service for this type of patients
Home management of hematological patients requiring hospital admissionIsaia G1 Tibaldi V Astengo M Ladetto M Marinello R Bo M Michelis G Ruatta F Ricauda NA
Arch Gerontol Geriatr 2010 Nov-Dec51(3)309-11
The client may be appropriate for home transfusion if (CCNS 2008) bullThere is at least one previous history of transfusion in hospital without a serious adverse reaction Clients who have never had a transfusion may be considered when the physician determines the benefits of home transfusion outweigh the risks bullThere is a history of adverse transfusion reactions that are of a controllable nature (ie fever controlled with medication) bullThere are physical limitations that would require ambulance transport to hospital for transfusion or hospital admission for transfusionbullThe client is alert cooperative and able to respond appropriately to body symptoms unless otherwise determined appropriate by the physician (particularly nursing home patients and pediatrics) bullThe client has a predictable stable medical condition without significant cardiovascular compromise (unstable angina CHF) bullThe client has adequate venous accessbullThere is a history of clinically significant red cell antibodies (reactive or not) provided antibody specificities are clearly identified There should be no unresolved serological findings
Giudelines for home transfusion 2014
CLINICAL ASSESSMENT
VARESETrasfusione di sangue a domicilio grazie allrsquoinfermiere di famigliaA pochi giorni dallapprovazione della riforma della sanitagrave a Varese avviene la prima trasfusione a casa di una paziente anziana allettata Levento possibile grazie alla collaborazione del medico di base
Pubblicato il 10 agosto 2015
Consegnata dallAIL oggi lunedigrave 2 dicembre la Fiat Panda in comodato duso gratuito per le attivitagrave di terapia trasfusionale domiciliare La Spezia
MARCHE SANITA TRASFUSIONI SANGUE A DOMICILIOAncona 17 ott (Adnkronos) - La Giunta della Regione Marche ha approvato il protocollo operativo sulla terapia trasfusionale domiciliare che prevede che i pazienti affetti da gravi malattie possano effettuare le trasfusioni nella propria abitazioni anziche in ospedale Lobiettivo -ha detto lassessore regionale alla Sanita Augusto Melappioni- e quello di venire incontro alle esigenze personali e terapeutiche dei malati che si trovano in precarie condizioni di salute riducendo allo stesso tempo i costi della prestazione
Trasfusione domiciliare premio nazionale allrsquoAsp di Ragusa4 ottobre 2016Per un progetto sulla sicurezza presentato da Giovanni Garozzo direttore della UOC di Medicina Trasfusionale ed Ematologia
0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient

Ospedalizzazione a Domicilio
Principali patologie
Patologia bronco-polmonare 219
bullPatologia cardiaca 197
bullPatologie neurologiche 152
bullPatologie ematologiche 142
bullPatologie oncologiche 68
Ospedalizzazione a Domicilio di Torino
COSTI PER GIORNATA DI RICOVERO
AOU Cittagrave della Salute e della Scienza
Terapia intensiva 1500 euro
Ematologia 1086 euro
Medicina drsquourgenza 850 euro
Medicina 400 euro
Ospedalizzazione a domicilio 155 euro
LAVORO DI SQUADRA
PRINCIPALI COLLABORAZIONI
DEA e Med UrgenzaSC U CardiologiaSC EmatologiaSC Pneumologia
THE RAD-HOME PROJECT
Da Giugno 2008
Ospedalizzazione a Domicilio di Torino
Posizionamento di cateteri venosi centrali e periferici con ecoguida
Trasfusioni a domicilio percheacute
Vantaggi per il servizio sanitario
Riduzione dei costi
Riduzione di errori
Vantaggi per i pazienti
Miglioramento dellrsquoautonomia
Miglioramento del comfort
Riduzione del rischio infettivo
Guidelines for home transfusion Nova Scotia 2014
Sempre sicure Quali rischi
Il rischio principale egrave rappresentato dalla mancanza di una immediata disponibilitagrave di
assistenza medica intensiva in caso di evento avverso correlato alla trasfusione
Fridey 2013
Transfusions at home in patients with myelodysplasticsyndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
bull Inclusion criteria patient and disease
Caregiver
Home environment
bull Exclusion criteria patient and disease
caregiver
home environment
211 MDS patients transfusion dependent 7766 trasfusions 4980 domiciliary transfusionsHome Care program 5-years period (2006-2010)
Inclusion criteria
bull Patient living in Rome or in the near urban area covered by our HC service
bull Disease-related anemia refractory to all conventional measures
bull Physical limitations andor compromised clinical and personal status
bull Family and social problems resulting in the impossibility to travel to the hospital and to attend clinical visits and transfusion
bull Stable medical conditions
bull Adequate venous access
bull Informed and written consent
bull Responsible capable and collaborating adult suitable at home Other than a family member caregiver would be also a friend or a home-aid assistant
bull Deemed adequate and suitable for HC program In particular the home shouldbe deemed easily accessible clear comfortable and safe to perform the transfusion
bull Avalability of a functioning telephone
Patientanddisease
Caregiver
Home environment
Niscola P et al Leukemia Research 36 (2012) 684-688
Exclusion criteria
bull Patientrsquos refusalbull Urgent trasfusion in emergent clinical situationsbull Inadequate vascular accessbull Sepsisbull Anemia due to underlying causes (hemolysis active bleeding iron and
vitamins deficiency and so on) potentially resolvable by othermeasures whenever applicable
bull Positive indirect antiglobulin test and no antigen-negative donorsRBCs units (both for autoantibodies and alloantibodies)
bull Unresolved andor undiagnosed fever cardiovascular instabilityandor others active clinical illnesses
bull History of previous severe transfusion-related adverse reactions
bull Patient living alone no capable and responsible adult suitable ascaregiver
bull Poor home condidions home deemed unsafe and unsiutable fortransfusion
PatientAnddisease
Caregiver
Homeenvironment
Niscola P et al Leukemia Research 36 (2012) 684-688
Home transfusion (4980) clinical complications
Transfusions at home in patients with myelodysplastic syndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
Extravasationsvascular accessrelated hematoma 6(00012)
Fever (gt 38deg C) 2(00004)
Cardiorespiratory symptoms(fluid overload and other complications) 2(00004
Skin rash 1(00002)
Nausea and vomiting 1(00002)
Total 12(00024)
bullA maximum of 2 red blood cell units have been administred for each transfusion
bull All adverse reactions were managed at home a rapid resolution and an uncomplicated outcome wereobserved in all cases
Avantages of transfusion at home compared to hospital
bull Logistic no need to travel to the hospital no long waits for visits
bull Psychological less distressing and more comfortable in the patientrsquos ownhome environment
bull Medical less patientrsquos discomfort and energy expenditure decreasedinfections
bull QoL potential for better QoL
bull Safety and liability Higher attention and better monitoring to single patient at home potential for fewer transfusion errors and adversereactions
bull Cost free for patients and families The cost have been covered by the Public Health Care System and by a non profit organization
bull Social and economic potential for fewer days lost from work for family members
Niscola P et al Leukemia Research 36 (2012) 684-688
Disavantages of transfusion at home comparedto hospital
bull Logistic and organizational time expensive for the team
bull Medical distance from advanced medical service full reanimation measures not immediately available in anemergent situation
bull Safety and liability greater risk due to increased distancefrom hospital care and emergency services
bull Regulatory and legal concerns national and local laws and regulations should be considered before to providing the transfusion service at home
bull Costs more expensive for the health care agency
Niscola P et al Leukemia Research 36 (2012) 684-688
The hospital-at-home service (HHS) could be considered as an alternative to the traditional ward for elderly patients We aimed at evaluating the home management of elderly people requiring transfusions The ever-increasing demand on acute hospital services requires alternative methods of delivering all aspects of health care HHS demonstrated to be as efficacious as a traditional ward for elderly and functionally compromised patients The method was a retrospective descriptive study enrolling patients needing an hospital admission from 1st January 2007 to 31st December 2007 and reporting an hematological discharges diagnosis as primary or secondary diagnosis A total of 54 patients were evaluated in this study Of them 34 (629) needed a hemocomponent transfusion for a total volume of 112 blood units and 49 platelet pools Patients requiring at least one blood or platelet transfusion were more functionally compromised and presented a higher level of acute physiology and chronic health evaluation compared to the non-transfused ones The conclusion was that hematological subjects mainly the frail ones and functionally highly compromised with acute illnesses could be treated at home as an alternative of the traditional medical ward This could be the starting point for future studies that will be able to increase the power of hospital-at-home service for this type of patients
Home management of hematological patients requiring hospital admissionIsaia G1 Tibaldi V Astengo M Ladetto M Marinello R Bo M Michelis G Ruatta F Ricauda NA
Arch Gerontol Geriatr 2010 Nov-Dec51(3)309-11
The client may be appropriate for home transfusion if (CCNS 2008) bullThere is at least one previous history of transfusion in hospital without a serious adverse reaction Clients who have never had a transfusion may be considered when the physician determines the benefits of home transfusion outweigh the risks bullThere is a history of adverse transfusion reactions that are of a controllable nature (ie fever controlled with medication) bullThere are physical limitations that would require ambulance transport to hospital for transfusion or hospital admission for transfusionbullThe client is alert cooperative and able to respond appropriately to body symptoms unless otherwise determined appropriate by the physician (particularly nursing home patients and pediatrics) bullThe client has a predictable stable medical condition without significant cardiovascular compromise (unstable angina CHF) bullThe client has adequate venous accessbullThere is a history of clinically significant red cell antibodies (reactive or not) provided antibody specificities are clearly identified There should be no unresolved serological findings
Giudelines for home transfusion 2014
CLINICAL ASSESSMENT
VARESETrasfusione di sangue a domicilio grazie allrsquoinfermiere di famigliaA pochi giorni dallapprovazione della riforma della sanitagrave a Varese avviene la prima trasfusione a casa di una paziente anziana allettata Levento possibile grazie alla collaborazione del medico di base
Pubblicato il 10 agosto 2015
Consegnata dallAIL oggi lunedigrave 2 dicembre la Fiat Panda in comodato duso gratuito per le attivitagrave di terapia trasfusionale domiciliare La Spezia
MARCHE SANITA TRASFUSIONI SANGUE A DOMICILIOAncona 17 ott (Adnkronos) - La Giunta della Regione Marche ha approvato il protocollo operativo sulla terapia trasfusionale domiciliare che prevede che i pazienti affetti da gravi malattie possano effettuare le trasfusioni nella propria abitazioni anziche in ospedale Lobiettivo -ha detto lassessore regionale alla Sanita Augusto Melappioni- e quello di venire incontro alle esigenze personali e terapeutiche dei malati che si trovano in precarie condizioni di salute riducendo allo stesso tempo i costi della prestazione
Trasfusione domiciliare premio nazionale allrsquoAsp di Ragusa4 ottobre 2016Per un progetto sulla sicurezza presentato da Giovanni Garozzo direttore della UOC di Medicina Trasfusionale ed Ematologia
0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient

Ospedalizzazione a Domicilio di Torino
COSTI PER GIORNATA DI RICOVERO
AOU Cittagrave della Salute e della Scienza
Terapia intensiva 1500 euro
Ematologia 1086 euro
Medicina drsquourgenza 850 euro
Medicina 400 euro
Ospedalizzazione a domicilio 155 euro
LAVORO DI SQUADRA
PRINCIPALI COLLABORAZIONI
DEA e Med UrgenzaSC U CardiologiaSC EmatologiaSC Pneumologia
THE RAD-HOME PROJECT
Da Giugno 2008
Ospedalizzazione a Domicilio di Torino
Posizionamento di cateteri venosi centrali e periferici con ecoguida
Trasfusioni a domicilio percheacute
Vantaggi per il servizio sanitario
Riduzione dei costi
Riduzione di errori
Vantaggi per i pazienti
Miglioramento dellrsquoautonomia
Miglioramento del comfort
Riduzione del rischio infettivo
Guidelines for home transfusion Nova Scotia 2014
Sempre sicure Quali rischi
Il rischio principale egrave rappresentato dalla mancanza di una immediata disponibilitagrave di
assistenza medica intensiva in caso di evento avverso correlato alla trasfusione
Fridey 2013
Transfusions at home in patients with myelodysplasticsyndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
bull Inclusion criteria patient and disease
Caregiver
Home environment
bull Exclusion criteria patient and disease
caregiver
home environment
211 MDS patients transfusion dependent 7766 trasfusions 4980 domiciliary transfusionsHome Care program 5-years period (2006-2010)
Inclusion criteria
bull Patient living in Rome or in the near urban area covered by our HC service
bull Disease-related anemia refractory to all conventional measures
bull Physical limitations andor compromised clinical and personal status
bull Family and social problems resulting in the impossibility to travel to the hospital and to attend clinical visits and transfusion
bull Stable medical conditions
bull Adequate venous access
bull Informed and written consent
bull Responsible capable and collaborating adult suitable at home Other than a family member caregiver would be also a friend or a home-aid assistant
bull Deemed adequate and suitable for HC program In particular the home shouldbe deemed easily accessible clear comfortable and safe to perform the transfusion
bull Avalability of a functioning telephone
Patientanddisease
Caregiver
Home environment
Niscola P et al Leukemia Research 36 (2012) 684-688
Exclusion criteria
bull Patientrsquos refusalbull Urgent trasfusion in emergent clinical situationsbull Inadequate vascular accessbull Sepsisbull Anemia due to underlying causes (hemolysis active bleeding iron and
vitamins deficiency and so on) potentially resolvable by othermeasures whenever applicable
bull Positive indirect antiglobulin test and no antigen-negative donorsRBCs units (both for autoantibodies and alloantibodies)
bull Unresolved andor undiagnosed fever cardiovascular instabilityandor others active clinical illnesses
bull History of previous severe transfusion-related adverse reactions
bull Patient living alone no capable and responsible adult suitable ascaregiver
bull Poor home condidions home deemed unsafe and unsiutable fortransfusion
PatientAnddisease
Caregiver
Homeenvironment
Niscola P et al Leukemia Research 36 (2012) 684-688
Home transfusion (4980) clinical complications
Transfusions at home in patients with myelodysplastic syndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
Extravasationsvascular accessrelated hematoma 6(00012)
Fever (gt 38deg C) 2(00004)
Cardiorespiratory symptoms(fluid overload and other complications) 2(00004
Skin rash 1(00002)
Nausea and vomiting 1(00002)
Total 12(00024)
bullA maximum of 2 red blood cell units have been administred for each transfusion
bull All adverse reactions were managed at home a rapid resolution and an uncomplicated outcome wereobserved in all cases
Avantages of transfusion at home compared to hospital
bull Logistic no need to travel to the hospital no long waits for visits
bull Psychological less distressing and more comfortable in the patientrsquos ownhome environment
bull Medical less patientrsquos discomfort and energy expenditure decreasedinfections
bull QoL potential for better QoL
bull Safety and liability Higher attention and better monitoring to single patient at home potential for fewer transfusion errors and adversereactions
bull Cost free for patients and families The cost have been covered by the Public Health Care System and by a non profit organization
bull Social and economic potential for fewer days lost from work for family members
Niscola P et al Leukemia Research 36 (2012) 684-688
Disavantages of transfusion at home comparedto hospital
bull Logistic and organizational time expensive for the team
bull Medical distance from advanced medical service full reanimation measures not immediately available in anemergent situation
bull Safety and liability greater risk due to increased distancefrom hospital care and emergency services
bull Regulatory and legal concerns national and local laws and regulations should be considered before to providing the transfusion service at home
bull Costs more expensive for the health care agency
Niscola P et al Leukemia Research 36 (2012) 684-688
The hospital-at-home service (HHS) could be considered as an alternative to the traditional ward for elderly patients We aimed at evaluating the home management of elderly people requiring transfusions The ever-increasing demand on acute hospital services requires alternative methods of delivering all aspects of health care HHS demonstrated to be as efficacious as a traditional ward for elderly and functionally compromised patients The method was a retrospective descriptive study enrolling patients needing an hospital admission from 1st January 2007 to 31st December 2007 and reporting an hematological discharges diagnosis as primary or secondary diagnosis A total of 54 patients were evaluated in this study Of them 34 (629) needed a hemocomponent transfusion for a total volume of 112 blood units and 49 platelet pools Patients requiring at least one blood or platelet transfusion were more functionally compromised and presented a higher level of acute physiology and chronic health evaluation compared to the non-transfused ones The conclusion was that hematological subjects mainly the frail ones and functionally highly compromised with acute illnesses could be treated at home as an alternative of the traditional medical ward This could be the starting point for future studies that will be able to increase the power of hospital-at-home service for this type of patients
Home management of hematological patients requiring hospital admissionIsaia G1 Tibaldi V Astengo M Ladetto M Marinello R Bo M Michelis G Ruatta F Ricauda NA
Arch Gerontol Geriatr 2010 Nov-Dec51(3)309-11
The client may be appropriate for home transfusion if (CCNS 2008) bullThere is at least one previous history of transfusion in hospital without a serious adverse reaction Clients who have never had a transfusion may be considered when the physician determines the benefits of home transfusion outweigh the risks bullThere is a history of adverse transfusion reactions that are of a controllable nature (ie fever controlled with medication) bullThere are physical limitations that would require ambulance transport to hospital for transfusion or hospital admission for transfusionbullThe client is alert cooperative and able to respond appropriately to body symptoms unless otherwise determined appropriate by the physician (particularly nursing home patients and pediatrics) bullThe client has a predictable stable medical condition without significant cardiovascular compromise (unstable angina CHF) bullThe client has adequate venous accessbullThere is a history of clinically significant red cell antibodies (reactive or not) provided antibody specificities are clearly identified There should be no unresolved serological findings
Giudelines for home transfusion 2014
CLINICAL ASSESSMENT
VARESETrasfusione di sangue a domicilio grazie allrsquoinfermiere di famigliaA pochi giorni dallapprovazione della riforma della sanitagrave a Varese avviene la prima trasfusione a casa di una paziente anziana allettata Levento possibile grazie alla collaborazione del medico di base
Pubblicato il 10 agosto 2015
Consegnata dallAIL oggi lunedigrave 2 dicembre la Fiat Panda in comodato duso gratuito per le attivitagrave di terapia trasfusionale domiciliare La Spezia
MARCHE SANITA TRASFUSIONI SANGUE A DOMICILIOAncona 17 ott (Adnkronos) - La Giunta della Regione Marche ha approvato il protocollo operativo sulla terapia trasfusionale domiciliare che prevede che i pazienti affetti da gravi malattie possano effettuare le trasfusioni nella propria abitazioni anziche in ospedale Lobiettivo -ha detto lassessore regionale alla Sanita Augusto Melappioni- e quello di venire incontro alle esigenze personali e terapeutiche dei malati che si trovano in precarie condizioni di salute riducendo allo stesso tempo i costi della prestazione
Trasfusione domiciliare premio nazionale allrsquoAsp di Ragusa4 ottobre 2016Per un progetto sulla sicurezza presentato da Giovanni Garozzo direttore della UOC di Medicina Trasfusionale ed Ematologia
0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient

LAVORO DI SQUADRA
PRINCIPALI COLLABORAZIONI
DEA e Med UrgenzaSC U CardiologiaSC EmatologiaSC Pneumologia
THE RAD-HOME PROJECT
Da Giugno 2008
Ospedalizzazione a Domicilio di Torino
Posizionamento di cateteri venosi centrali e periferici con ecoguida
Trasfusioni a domicilio percheacute
Vantaggi per il servizio sanitario
Riduzione dei costi
Riduzione di errori
Vantaggi per i pazienti
Miglioramento dellrsquoautonomia
Miglioramento del comfort
Riduzione del rischio infettivo
Guidelines for home transfusion Nova Scotia 2014
Sempre sicure Quali rischi
Il rischio principale egrave rappresentato dalla mancanza di una immediata disponibilitagrave di
assistenza medica intensiva in caso di evento avverso correlato alla trasfusione
Fridey 2013
Transfusions at home in patients with myelodysplasticsyndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
bull Inclusion criteria patient and disease
Caregiver
Home environment
bull Exclusion criteria patient and disease
caregiver
home environment
211 MDS patients transfusion dependent 7766 trasfusions 4980 domiciliary transfusionsHome Care program 5-years period (2006-2010)
Inclusion criteria
bull Patient living in Rome or in the near urban area covered by our HC service
bull Disease-related anemia refractory to all conventional measures
bull Physical limitations andor compromised clinical and personal status
bull Family and social problems resulting in the impossibility to travel to the hospital and to attend clinical visits and transfusion
bull Stable medical conditions
bull Adequate venous access
bull Informed and written consent
bull Responsible capable and collaborating adult suitable at home Other than a family member caregiver would be also a friend or a home-aid assistant
bull Deemed adequate and suitable for HC program In particular the home shouldbe deemed easily accessible clear comfortable and safe to perform the transfusion
bull Avalability of a functioning telephone
Patientanddisease
Caregiver
Home environment
Niscola P et al Leukemia Research 36 (2012) 684-688
Exclusion criteria
bull Patientrsquos refusalbull Urgent trasfusion in emergent clinical situationsbull Inadequate vascular accessbull Sepsisbull Anemia due to underlying causes (hemolysis active bleeding iron and
vitamins deficiency and so on) potentially resolvable by othermeasures whenever applicable
bull Positive indirect antiglobulin test and no antigen-negative donorsRBCs units (both for autoantibodies and alloantibodies)
bull Unresolved andor undiagnosed fever cardiovascular instabilityandor others active clinical illnesses
bull History of previous severe transfusion-related adverse reactions
bull Patient living alone no capable and responsible adult suitable ascaregiver
bull Poor home condidions home deemed unsafe and unsiutable fortransfusion
PatientAnddisease
Caregiver
Homeenvironment
Niscola P et al Leukemia Research 36 (2012) 684-688
Home transfusion (4980) clinical complications
Transfusions at home in patients with myelodysplastic syndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
Extravasationsvascular accessrelated hematoma 6(00012)
Fever (gt 38deg C) 2(00004)
Cardiorespiratory symptoms(fluid overload and other complications) 2(00004
Skin rash 1(00002)
Nausea and vomiting 1(00002)
Total 12(00024)
bullA maximum of 2 red blood cell units have been administred for each transfusion
bull All adverse reactions were managed at home a rapid resolution and an uncomplicated outcome wereobserved in all cases
Avantages of transfusion at home compared to hospital
bull Logistic no need to travel to the hospital no long waits for visits
bull Psychological less distressing and more comfortable in the patientrsquos ownhome environment
bull Medical less patientrsquos discomfort and energy expenditure decreasedinfections
bull QoL potential for better QoL
bull Safety and liability Higher attention and better monitoring to single patient at home potential for fewer transfusion errors and adversereactions
bull Cost free for patients and families The cost have been covered by the Public Health Care System and by a non profit organization
bull Social and economic potential for fewer days lost from work for family members
Niscola P et al Leukemia Research 36 (2012) 684-688
Disavantages of transfusion at home comparedto hospital
bull Logistic and organizational time expensive for the team
bull Medical distance from advanced medical service full reanimation measures not immediately available in anemergent situation
bull Safety and liability greater risk due to increased distancefrom hospital care and emergency services
bull Regulatory and legal concerns national and local laws and regulations should be considered before to providing the transfusion service at home
bull Costs more expensive for the health care agency
Niscola P et al Leukemia Research 36 (2012) 684-688
The hospital-at-home service (HHS) could be considered as an alternative to the traditional ward for elderly patients We aimed at evaluating the home management of elderly people requiring transfusions The ever-increasing demand on acute hospital services requires alternative methods of delivering all aspects of health care HHS demonstrated to be as efficacious as a traditional ward for elderly and functionally compromised patients The method was a retrospective descriptive study enrolling patients needing an hospital admission from 1st January 2007 to 31st December 2007 and reporting an hematological discharges diagnosis as primary or secondary diagnosis A total of 54 patients were evaluated in this study Of them 34 (629) needed a hemocomponent transfusion for a total volume of 112 blood units and 49 platelet pools Patients requiring at least one blood or platelet transfusion were more functionally compromised and presented a higher level of acute physiology and chronic health evaluation compared to the non-transfused ones The conclusion was that hematological subjects mainly the frail ones and functionally highly compromised with acute illnesses could be treated at home as an alternative of the traditional medical ward This could be the starting point for future studies that will be able to increase the power of hospital-at-home service for this type of patients
Home management of hematological patients requiring hospital admissionIsaia G1 Tibaldi V Astengo M Ladetto M Marinello R Bo M Michelis G Ruatta F Ricauda NA
Arch Gerontol Geriatr 2010 Nov-Dec51(3)309-11
The client may be appropriate for home transfusion if (CCNS 2008) bullThere is at least one previous history of transfusion in hospital without a serious adverse reaction Clients who have never had a transfusion may be considered when the physician determines the benefits of home transfusion outweigh the risks bullThere is a history of adverse transfusion reactions that are of a controllable nature (ie fever controlled with medication) bullThere are physical limitations that would require ambulance transport to hospital for transfusion or hospital admission for transfusionbullThe client is alert cooperative and able to respond appropriately to body symptoms unless otherwise determined appropriate by the physician (particularly nursing home patients and pediatrics) bullThe client has a predictable stable medical condition without significant cardiovascular compromise (unstable angina CHF) bullThe client has adequate venous accessbullThere is a history of clinically significant red cell antibodies (reactive or not) provided antibody specificities are clearly identified There should be no unresolved serological findings
Giudelines for home transfusion 2014
CLINICAL ASSESSMENT
VARESETrasfusione di sangue a domicilio grazie allrsquoinfermiere di famigliaA pochi giorni dallapprovazione della riforma della sanitagrave a Varese avviene la prima trasfusione a casa di una paziente anziana allettata Levento possibile grazie alla collaborazione del medico di base
Pubblicato il 10 agosto 2015
Consegnata dallAIL oggi lunedigrave 2 dicembre la Fiat Panda in comodato duso gratuito per le attivitagrave di terapia trasfusionale domiciliare La Spezia
MARCHE SANITA TRASFUSIONI SANGUE A DOMICILIOAncona 17 ott (Adnkronos) - La Giunta della Regione Marche ha approvato il protocollo operativo sulla terapia trasfusionale domiciliare che prevede che i pazienti affetti da gravi malattie possano effettuare le trasfusioni nella propria abitazioni anziche in ospedale Lobiettivo -ha detto lassessore regionale alla Sanita Augusto Melappioni- e quello di venire incontro alle esigenze personali e terapeutiche dei malati che si trovano in precarie condizioni di salute riducendo allo stesso tempo i costi della prestazione
Trasfusione domiciliare premio nazionale allrsquoAsp di Ragusa4 ottobre 2016Per un progetto sulla sicurezza presentato da Giovanni Garozzo direttore della UOC di Medicina Trasfusionale ed Ematologia
0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient

THE RAD-HOME PROJECT
Da Giugno 2008
Ospedalizzazione a Domicilio di Torino
Posizionamento di cateteri venosi centrali e periferici con ecoguida
Trasfusioni a domicilio percheacute
Vantaggi per il servizio sanitario
Riduzione dei costi
Riduzione di errori
Vantaggi per i pazienti
Miglioramento dellrsquoautonomia
Miglioramento del comfort
Riduzione del rischio infettivo
Guidelines for home transfusion Nova Scotia 2014
Sempre sicure Quali rischi
Il rischio principale egrave rappresentato dalla mancanza di una immediata disponibilitagrave di
assistenza medica intensiva in caso di evento avverso correlato alla trasfusione
Fridey 2013
Transfusions at home in patients with myelodysplasticsyndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
bull Inclusion criteria patient and disease
Caregiver
Home environment
bull Exclusion criteria patient and disease
caregiver
home environment
211 MDS patients transfusion dependent 7766 trasfusions 4980 domiciliary transfusionsHome Care program 5-years period (2006-2010)
Inclusion criteria
bull Patient living in Rome or in the near urban area covered by our HC service
bull Disease-related anemia refractory to all conventional measures
bull Physical limitations andor compromised clinical and personal status
bull Family and social problems resulting in the impossibility to travel to the hospital and to attend clinical visits and transfusion
bull Stable medical conditions
bull Adequate venous access
bull Informed and written consent
bull Responsible capable and collaborating adult suitable at home Other than a family member caregiver would be also a friend or a home-aid assistant
bull Deemed adequate and suitable for HC program In particular the home shouldbe deemed easily accessible clear comfortable and safe to perform the transfusion
bull Avalability of a functioning telephone
Patientanddisease
Caregiver
Home environment
Niscola P et al Leukemia Research 36 (2012) 684-688
Exclusion criteria
bull Patientrsquos refusalbull Urgent trasfusion in emergent clinical situationsbull Inadequate vascular accessbull Sepsisbull Anemia due to underlying causes (hemolysis active bleeding iron and
vitamins deficiency and so on) potentially resolvable by othermeasures whenever applicable
bull Positive indirect antiglobulin test and no antigen-negative donorsRBCs units (both for autoantibodies and alloantibodies)
bull Unresolved andor undiagnosed fever cardiovascular instabilityandor others active clinical illnesses
bull History of previous severe transfusion-related adverse reactions
bull Patient living alone no capable and responsible adult suitable ascaregiver
bull Poor home condidions home deemed unsafe and unsiutable fortransfusion
PatientAnddisease
Caregiver
Homeenvironment
Niscola P et al Leukemia Research 36 (2012) 684-688
Home transfusion (4980) clinical complications
Transfusions at home in patients with myelodysplastic syndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
Extravasationsvascular accessrelated hematoma 6(00012)
Fever (gt 38deg C) 2(00004)
Cardiorespiratory symptoms(fluid overload and other complications) 2(00004
Skin rash 1(00002)
Nausea and vomiting 1(00002)
Total 12(00024)
bullA maximum of 2 red blood cell units have been administred for each transfusion
bull All adverse reactions were managed at home a rapid resolution and an uncomplicated outcome wereobserved in all cases
Avantages of transfusion at home compared to hospital
bull Logistic no need to travel to the hospital no long waits for visits
bull Psychological less distressing and more comfortable in the patientrsquos ownhome environment
bull Medical less patientrsquos discomfort and energy expenditure decreasedinfections
bull QoL potential for better QoL
bull Safety and liability Higher attention and better monitoring to single patient at home potential for fewer transfusion errors and adversereactions
bull Cost free for patients and families The cost have been covered by the Public Health Care System and by a non profit organization
bull Social and economic potential for fewer days lost from work for family members
Niscola P et al Leukemia Research 36 (2012) 684-688
Disavantages of transfusion at home comparedto hospital
bull Logistic and organizational time expensive for the team
bull Medical distance from advanced medical service full reanimation measures not immediately available in anemergent situation
bull Safety and liability greater risk due to increased distancefrom hospital care and emergency services
bull Regulatory and legal concerns national and local laws and regulations should be considered before to providing the transfusion service at home
bull Costs more expensive for the health care agency
Niscola P et al Leukemia Research 36 (2012) 684-688
The hospital-at-home service (HHS) could be considered as an alternative to the traditional ward for elderly patients We aimed at evaluating the home management of elderly people requiring transfusions The ever-increasing demand on acute hospital services requires alternative methods of delivering all aspects of health care HHS demonstrated to be as efficacious as a traditional ward for elderly and functionally compromised patients The method was a retrospective descriptive study enrolling patients needing an hospital admission from 1st January 2007 to 31st December 2007 and reporting an hematological discharges diagnosis as primary or secondary diagnosis A total of 54 patients were evaluated in this study Of them 34 (629) needed a hemocomponent transfusion for a total volume of 112 blood units and 49 platelet pools Patients requiring at least one blood or platelet transfusion were more functionally compromised and presented a higher level of acute physiology and chronic health evaluation compared to the non-transfused ones The conclusion was that hematological subjects mainly the frail ones and functionally highly compromised with acute illnesses could be treated at home as an alternative of the traditional medical ward This could be the starting point for future studies that will be able to increase the power of hospital-at-home service for this type of patients
Home management of hematological patients requiring hospital admissionIsaia G1 Tibaldi V Astengo M Ladetto M Marinello R Bo M Michelis G Ruatta F Ricauda NA
Arch Gerontol Geriatr 2010 Nov-Dec51(3)309-11
The client may be appropriate for home transfusion if (CCNS 2008) bullThere is at least one previous history of transfusion in hospital without a serious adverse reaction Clients who have never had a transfusion may be considered when the physician determines the benefits of home transfusion outweigh the risks bullThere is a history of adverse transfusion reactions that are of a controllable nature (ie fever controlled with medication) bullThere are physical limitations that would require ambulance transport to hospital for transfusion or hospital admission for transfusionbullThe client is alert cooperative and able to respond appropriately to body symptoms unless otherwise determined appropriate by the physician (particularly nursing home patients and pediatrics) bullThe client has a predictable stable medical condition without significant cardiovascular compromise (unstable angina CHF) bullThe client has adequate venous accessbullThere is a history of clinically significant red cell antibodies (reactive or not) provided antibody specificities are clearly identified There should be no unresolved serological findings
Giudelines for home transfusion 2014
CLINICAL ASSESSMENT
VARESETrasfusione di sangue a domicilio grazie allrsquoinfermiere di famigliaA pochi giorni dallapprovazione della riforma della sanitagrave a Varese avviene la prima trasfusione a casa di una paziente anziana allettata Levento possibile grazie alla collaborazione del medico di base
Pubblicato il 10 agosto 2015
Consegnata dallAIL oggi lunedigrave 2 dicembre la Fiat Panda in comodato duso gratuito per le attivitagrave di terapia trasfusionale domiciliare La Spezia
MARCHE SANITA TRASFUSIONI SANGUE A DOMICILIOAncona 17 ott (Adnkronos) - La Giunta della Regione Marche ha approvato il protocollo operativo sulla terapia trasfusionale domiciliare che prevede che i pazienti affetti da gravi malattie possano effettuare le trasfusioni nella propria abitazioni anziche in ospedale Lobiettivo -ha detto lassessore regionale alla Sanita Augusto Melappioni- e quello di venire incontro alle esigenze personali e terapeutiche dei malati che si trovano in precarie condizioni di salute riducendo allo stesso tempo i costi della prestazione
Trasfusione domiciliare premio nazionale allrsquoAsp di Ragusa4 ottobre 2016Per un progetto sulla sicurezza presentato da Giovanni Garozzo direttore della UOC di Medicina Trasfusionale ed Ematologia
0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient

Ospedalizzazione a Domicilio di Torino
Posizionamento di cateteri venosi centrali e periferici con ecoguida
Trasfusioni a domicilio percheacute
Vantaggi per il servizio sanitario
Riduzione dei costi
Riduzione di errori
Vantaggi per i pazienti
Miglioramento dellrsquoautonomia
Miglioramento del comfort
Riduzione del rischio infettivo
Guidelines for home transfusion Nova Scotia 2014
Sempre sicure Quali rischi
Il rischio principale egrave rappresentato dalla mancanza di una immediata disponibilitagrave di
assistenza medica intensiva in caso di evento avverso correlato alla trasfusione
Fridey 2013
Transfusions at home in patients with myelodysplasticsyndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
bull Inclusion criteria patient and disease
Caregiver
Home environment
bull Exclusion criteria patient and disease
caregiver
home environment
211 MDS patients transfusion dependent 7766 trasfusions 4980 domiciliary transfusionsHome Care program 5-years period (2006-2010)
Inclusion criteria
bull Patient living in Rome or in the near urban area covered by our HC service
bull Disease-related anemia refractory to all conventional measures
bull Physical limitations andor compromised clinical and personal status
bull Family and social problems resulting in the impossibility to travel to the hospital and to attend clinical visits and transfusion
bull Stable medical conditions
bull Adequate venous access
bull Informed and written consent
bull Responsible capable and collaborating adult suitable at home Other than a family member caregiver would be also a friend or a home-aid assistant
bull Deemed adequate and suitable for HC program In particular the home shouldbe deemed easily accessible clear comfortable and safe to perform the transfusion
bull Avalability of a functioning telephone
Patientanddisease
Caregiver
Home environment
Niscola P et al Leukemia Research 36 (2012) 684-688
Exclusion criteria
bull Patientrsquos refusalbull Urgent trasfusion in emergent clinical situationsbull Inadequate vascular accessbull Sepsisbull Anemia due to underlying causes (hemolysis active bleeding iron and
vitamins deficiency and so on) potentially resolvable by othermeasures whenever applicable
bull Positive indirect antiglobulin test and no antigen-negative donorsRBCs units (both for autoantibodies and alloantibodies)
bull Unresolved andor undiagnosed fever cardiovascular instabilityandor others active clinical illnesses
bull History of previous severe transfusion-related adverse reactions
bull Patient living alone no capable and responsible adult suitable ascaregiver
bull Poor home condidions home deemed unsafe and unsiutable fortransfusion
PatientAnddisease
Caregiver
Homeenvironment
Niscola P et al Leukemia Research 36 (2012) 684-688
Home transfusion (4980) clinical complications
Transfusions at home in patients with myelodysplastic syndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
Extravasationsvascular accessrelated hematoma 6(00012)
Fever (gt 38deg C) 2(00004)
Cardiorespiratory symptoms(fluid overload and other complications) 2(00004
Skin rash 1(00002)
Nausea and vomiting 1(00002)
Total 12(00024)
bullA maximum of 2 red blood cell units have been administred for each transfusion
bull All adverse reactions were managed at home a rapid resolution and an uncomplicated outcome wereobserved in all cases
Avantages of transfusion at home compared to hospital
bull Logistic no need to travel to the hospital no long waits for visits
bull Psychological less distressing and more comfortable in the patientrsquos ownhome environment
bull Medical less patientrsquos discomfort and energy expenditure decreasedinfections
bull QoL potential for better QoL
bull Safety and liability Higher attention and better monitoring to single patient at home potential for fewer transfusion errors and adversereactions
bull Cost free for patients and families The cost have been covered by the Public Health Care System and by a non profit organization
bull Social and economic potential for fewer days lost from work for family members
Niscola P et al Leukemia Research 36 (2012) 684-688
Disavantages of transfusion at home comparedto hospital
bull Logistic and organizational time expensive for the team
bull Medical distance from advanced medical service full reanimation measures not immediately available in anemergent situation
bull Safety and liability greater risk due to increased distancefrom hospital care and emergency services
bull Regulatory and legal concerns national and local laws and regulations should be considered before to providing the transfusion service at home
bull Costs more expensive for the health care agency
Niscola P et al Leukemia Research 36 (2012) 684-688
The hospital-at-home service (HHS) could be considered as an alternative to the traditional ward for elderly patients We aimed at evaluating the home management of elderly people requiring transfusions The ever-increasing demand on acute hospital services requires alternative methods of delivering all aspects of health care HHS demonstrated to be as efficacious as a traditional ward for elderly and functionally compromised patients The method was a retrospective descriptive study enrolling patients needing an hospital admission from 1st January 2007 to 31st December 2007 and reporting an hematological discharges diagnosis as primary or secondary diagnosis A total of 54 patients were evaluated in this study Of them 34 (629) needed a hemocomponent transfusion for a total volume of 112 blood units and 49 platelet pools Patients requiring at least one blood or platelet transfusion were more functionally compromised and presented a higher level of acute physiology and chronic health evaluation compared to the non-transfused ones The conclusion was that hematological subjects mainly the frail ones and functionally highly compromised with acute illnesses could be treated at home as an alternative of the traditional medical ward This could be the starting point for future studies that will be able to increase the power of hospital-at-home service for this type of patients
Home management of hematological patients requiring hospital admissionIsaia G1 Tibaldi V Astengo M Ladetto M Marinello R Bo M Michelis G Ruatta F Ricauda NA
Arch Gerontol Geriatr 2010 Nov-Dec51(3)309-11
The client may be appropriate for home transfusion if (CCNS 2008) bullThere is at least one previous history of transfusion in hospital without a serious adverse reaction Clients who have never had a transfusion may be considered when the physician determines the benefits of home transfusion outweigh the risks bullThere is a history of adverse transfusion reactions that are of a controllable nature (ie fever controlled with medication) bullThere are physical limitations that would require ambulance transport to hospital for transfusion or hospital admission for transfusionbullThe client is alert cooperative and able to respond appropriately to body symptoms unless otherwise determined appropriate by the physician (particularly nursing home patients and pediatrics) bullThe client has a predictable stable medical condition without significant cardiovascular compromise (unstable angina CHF) bullThe client has adequate venous accessbullThere is a history of clinically significant red cell antibodies (reactive or not) provided antibody specificities are clearly identified There should be no unresolved serological findings
Giudelines for home transfusion 2014
CLINICAL ASSESSMENT
VARESETrasfusione di sangue a domicilio grazie allrsquoinfermiere di famigliaA pochi giorni dallapprovazione della riforma della sanitagrave a Varese avviene la prima trasfusione a casa di una paziente anziana allettata Levento possibile grazie alla collaborazione del medico di base
Pubblicato il 10 agosto 2015
Consegnata dallAIL oggi lunedigrave 2 dicembre la Fiat Panda in comodato duso gratuito per le attivitagrave di terapia trasfusionale domiciliare La Spezia
MARCHE SANITA TRASFUSIONI SANGUE A DOMICILIOAncona 17 ott (Adnkronos) - La Giunta della Regione Marche ha approvato il protocollo operativo sulla terapia trasfusionale domiciliare che prevede che i pazienti affetti da gravi malattie possano effettuare le trasfusioni nella propria abitazioni anziche in ospedale Lobiettivo -ha detto lassessore regionale alla Sanita Augusto Melappioni- e quello di venire incontro alle esigenze personali e terapeutiche dei malati che si trovano in precarie condizioni di salute riducendo allo stesso tempo i costi della prestazione
Trasfusione domiciliare premio nazionale allrsquoAsp di Ragusa4 ottobre 2016Per un progetto sulla sicurezza presentato da Giovanni Garozzo direttore della UOC di Medicina Trasfusionale ed Ematologia
0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient

Trasfusioni a domicilio percheacute
Vantaggi per il servizio sanitario
Riduzione dei costi
Riduzione di errori
Vantaggi per i pazienti
Miglioramento dellrsquoautonomia
Miglioramento del comfort
Riduzione del rischio infettivo
Guidelines for home transfusion Nova Scotia 2014
Sempre sicure Quali rischi
Il rischio principale egrave rappresentato dalla mancanza di una immediata disponibilitagrave di
assistenza medica intensiva in caso di evento avverso correlato alla trasfusione
Fridey 2013
Transfusions at home in patients with myelodysplasticsyndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
bull Inclusion criteria patient and disease
Caregiver
Home environment
bull Exclusion criteria patient and disease
caregiver
home environment
211 MDS patients transfusion dependent 7766 trasfusions 4980 domiciliary transfusionsHome Care program 5-years period (2006-2010)
Inclusion criteria
bull Patient living in Rome or in the near urban area covered by our HC service
bull Disease-related anemia refractory to all conventional measures
bull Physical limitations andor compromised clinical and personal status
bull Family and social problems resulting in the impossibility to travel to the hospital and to attend clinical visits and transfusion
bull Stable medical conditions
bull Adequate venous access
bull Informed and written consent
bull Responsible capable and collaborating adult suitable at home Other than a family member caregiver would be also a friend or a home-aid assistant
bull Deemed adequate and suitable for HC program In particular the home shouldbe deemed easily accessible clear comfortable and safe to perform the transfusion
bull Avalability of a functioning telephone
Patientanddisease
Caregiver
Home environment
Niscola P et al Leukemia Research 36 (2012) 684-688
Exclusion criteria
bull Patientrsquos refusalbull Urgent trasfusion in emergent clinical situationsbull Inadequate vascular accessbull Sepsisbull Anemia due to underlying causes (hemolysis active bleeding iron and
vitamins deficiency and so on) potentially resolvable by othermeasures whenever applicable
bull Positive indirect antiglobulin test and no antigen-negative donorsRBCs units (both for autoantibodies and alloantibodies)
bull Unresolved andor undiagnosed fever cardiovascular instabilityandor others active clinical illnesses
bull History of previous severe transfusion-related adverse reactions
bull Patient living alone no capable and responsible adult suitable ascaregiver
bull Poor home condidions home deemed unsafe and unsiutable fortransfusion
PatientAnddisease
Caregiver
Homeenvironment
Niscola P et al Leukemia Research 36 (2012) 684-688
Home transfusion (4980) clinical complications
Transfusions at home in patients with myelodysplastic syndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
Extravasationsvascular accessrelated hematoma 6(00012)
Fever (gt 38deg C) 2(00004)
Cardiorespiratory symptoms(fluid overload and other complications) 2(00004
Skin rash 1(00002)
Nausea and vomiting 1(00002)
Total 12(00024)
bullA maximum of 2 red blood cell units have been administred for each transfusion
bull All adverse reactions were managed at home a rapid resolution and an uncomplicated outcome wereobserved in all cases
Avantages of transfusion at home compared to hospital
bull Logistic no need to travel to the hospital no long waits for visits
bull Psychological less distressing and more comfortable in the patientrsquos ownhome environment
bull Medical less patientrsquos discomfort and energy expenditure decreasedinfections
bull QoL potential for better QoL
bull Safety and liability Higher attention and better monitoring to single patient at home potential for fewer transfusion errors and adversereactions
bull Cost free for patients and families The cost have been covered by the Public Health Care System and by a non profit organization
bull Social and economic potential for fewer days lost from work for family members
Niscola P et al Leukemia Research 36 (2012) 684-688
Disavantages of transfusion at home comparedto hospital
bull Logistic and organizational time expensive for the team
bull Medical distance from advanced medical service full reanimation measures not immediately available in anemergent situation
bull Safety and liability greater risk due to increased distancefrom hospital care and emergency services
bull Regulatory and legal concerns national and local laws and regulations should be considered before to providing the transfusion service at home
bull Costs more expensive for the health care agency
Niscola P et al Leukemia Research 36 (2012) 684-688
The hospital-at-home service (HHS) could be considered as an alternative to the traditional ward for elderly patients We aimed at evaluating the home management of elderly people requiring transfusions The ever-increasing demand on acute hospital services requires alternative methods of delivering all aspects of health care HHS demonstrated to be as efficacious as a traditional ward for elderly and functionally compromised patients The method was a retrospective descriptive study enrolling patients needing an hospital admission from 1st January 2007 to 31st December 2007 and reporting an hematological discharges diagnosis as primary or secondary diagnosis A total of 54 patients were evaluated in this study Of them 34 (629) needed a hemocomponent transfusion for a total volume of 112 blood units and 49 platelet pools Patients requiring at least one blood or platelet transfusion were more functionally compromised and presented a higher level of acute physiology and chronic health evaluation compared to the non-transfused ones The conclusion was that hematological subjects mainly the frail ones and functionally highly compromised with acute illnesses could be treated at home as an alternative of the traditional medical ward This could be the starting point for future studies that will be able to increase the power of hospital-at-home service for this type of patients
Home management of hematological patients requiring hospital admissionIsaia G1 Tibaldi V Astengo M Ladetto M Marinello R Bo M Michelis G Ruatta F Ricauda NA
Arch Gerontol Geriatr 2010 Nov-Dec51(3)309-11
The client may be appropriate for home transfusion if (CCNS 2008) bullThere is at least one previous history of transfusion in hospital without a serious adverse reaction Clients who have never had a transfusion may be considered when the physician determines the benefits of home transfusion outweigh the risks bullThere is a history of adverse transfusion reactions that are of a controllable nature (ie fever controlled with medication) bullThere are physical limitations that would require ambulance transport to hospital for transfusion or hospital admission for transfusionbullThe client is alert cooperative and able to respond appropriately to body symptoms unless otherwise determined appropriate by the physician (particularly nursing home patients and pediatrics) bullThe client has a predictable stable medical condition without significant cardiovascular compromise (unstable angina CHF) bullThe client has adequate venous accessbullThere is a history of clinically significant red cell antibodies (reactive or not) provided antibody specificities are clearly identified There should be no unresolved serological findings
Giudelines for home transfusion 2014
CLINICAL ASSESSMENT
VARESETrasfusione di sangue a domicilio grazie allrsquoinfermiere di famigliaA pochi giorni dallapprovazione della riforma della sanitagrave a Varese avviene la prima trasfusione a casa di una paziente anziana allettata Levento possibile grazie alla collaborazione del medico di base
Pubblicato il 10 agosto 2015
Consegnata dallAIL oggi lunedigrave 2 dicembre la Fiat Panda in comodato duso gratuito per le attivitagrave di terapia trasfusionale domiciliare La Spezia
MARCHE SANITA TRASFUSIONI SANGUE A DOMICILIOAncona 17 ott (Adnkronos) - La Giunta della Regione Marche ha approvato il protocollo operativo sulla terapia trasfusionale domiciliare che prevede che i pazienti affetti da gravi malattie possano effettuare le trasfusioni nella propria abitazioni anziche in ospedale Lobiettivo -ha detto lassessore regionale alla Sanita Augusto Melappioni- e quello di venire incontro alle esigenze personali e terapeutiche dei malati che si trovano in precarie condizioni di salute riducendo allo stesso tempo i costi della prestazione
Trasfusione domiciliare premio nazionale allrsquoAsp di Ragusa4 ottobre 2016Per un progetto sulla sicurezza presentato da Giovanni Garozzo direttore della UOC di Medicina Trasfusionale ed Ematologia
0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient

Sempre sicure Quali rischi
Il rischio principale egrave rappresentato dalla mancanza di una immediata disponibilitagrave di
assistenza medica intensiva in caso di evento avverso correlato alla trasfusione
Fridey 2013
Transfusions at home in patients with myelodysplasticsyndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
bull Inclusion criteria patient and disease
Caregiver
Home environment
bull Exclusion criteria patient and disease
caregiver
home environment
211 MDS patients transfusion dependent 7766 trasfusions 4980 domiciliary transfusionsHome Care program 5-years period (2006-2010)
Inclusion criteria
bull Patient living in Rome or in the near urban area covered by our HC service
bull Disease-related anemia refractory to all conventional measures
bull Physical limitations andor compromised clinical and personal status
bull Family and social problems resulting in the impossibility to travel to the hospital and to attend clinical visits and transfusion
bull Stable medical conditions
bull Adequate venous access
bull Informed and written consent
bull Responsible capable and collaborating adult suitable at home Other than a family member caregiver would be also a friend or a home-aid assistant
bull Deemed adequate and suitable for HC program In particular the home shouldbe deemed easily accessible clear comfortable and safe to perform the transfusion
bull Avalability of a functioning telephone
Patientanddisease
Caregiver
Home environment
Niscola P et al Leukemia Research 36 (2012) 684-688
Exclusion criteria
bull Patientrsquos refusalbull Urgent trasfusion in emergent clinical situationsbull Inadequate vascular accessbull Sepsisbull Anemia due to underlying causes (hemolysis active bleeding iron and
vitamins deficiency and so on) potentially resolvable by othermeasures whenever applicable
bull Positive indirect antiglobulin test and no antigen-negative donorsRBCs units (both for autoantibodies and alloantibodies)
bull Unresolved andor undiagnosed fever cardiovascular instabilityandor others active clinical illnesses
bull History of previous severe transfusion-related adverse reactions
bull Patient living alone no capable and responsible adult suitable ascaregiver
bull Poor home condidions home deemed unsafe and unsiutable fortransfusion
PatientAnddisease
Caregiver
Homeenvironment
Niscola P et al Leukemia Research 36 (2012) 684-688
Home transfusion (4980) clinical complications
Transfusions at home in patients with myelodysplastic syndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
Extravasationsvascular accessrelated hematoma 6(00012)
Fever (gt 38deg C) 2(00004)
Cardiorespiratory symptoms(fluid overload and other complications) 2(00004
Skin rash 1(00002)
Nausea and vomiting 1(00002)
Total 12(00024)
bullA maximum of 2 red blood cell units have been administred for each transfusion
bull All adverse reactions were managed at home a rapid resolution and an uncomplicated outcome wereobserved in all cases
Avantages of transfusion at home compared to hospital
bull Logistic no need to travel to the hospital no long waits for visits
bull Psychological less distressing and more comfortable in the patientrsquos ownhome environment
bull Medical less patientrsquos discomfort and energy expenditure decreasedinfections
bull QoL potential for better QoL
bull Safety and liability Higher attention and better monitoring to single patient at home potential for fewer transfusion errors and adversereactions
bull Cost free for patients and families The cost have been covered by the Public Health Care System and by a non profit organization
bull Social and economic potential for fewer days lost from work for family members
Niscola P et al Leukemia Research 36 (2012) 684-688
Disavantages of transfusion at home comparedto hospital
bull Logistic and organizational time expensive for the team
bull Medical distance from advanced medical service full reanimation measures not immediately available in anemergent situation
bull Safety and liability greater risk due to increased distancefrom hospital care and emergency services
bull Regulatory and legal concerns national and local laws and regulations should be considered before to providing the transfusion service at home
bull Costs more expensive for the health care agency
Niscola P et al Leukemia Research 36 (2012) 684-688
The hospital-at-home service (HHS) could be considered as an alternative to the traditional ward for elderly patients We aimed at evaluating the home management of elderly people requiring transfusions The ever-increasing demand on acute hospital services requires alternative methods of delivering all aspects of health care HHS demonstrated to be as efficacious as a traditional ward for elderly and functionally compromised patients The method was a retrospective descriptive study enrolling patients needing an hospital admission from 1st January 2007 to 31st December 2007 and reporting an hematological discharges diagnosis as primary or secondary diagnosis A total of 54 patients were evaluated in this study Of them 34 (629) needed a hemocomponent transfusion for a total volume of 112 blood units and 49 platelet pools Patients requiring at least one blood or platelet transfusion were more functionally compromised and presented a higher level of acute physiology and chronic health evaluation compared to the non-transfused ones The conclusion was that hematological subjects mainly the frail ones and functionally highly compromised with acute illnesses could be treated at home as an alternative of the traditional medical ward This could be the starting point for future studies that will be able to increase the power of hospital-at-home service for this type of patients
Home management of hematological patients requiring hospital admissionIsaia G1 Tibaldi V Astengo M Ladetto M Marinello R Bo M Michelis G Ruatta F Ricauda NA
Arch Gerontol Geriatr 2010 Nov-Dec51(3)309-11
The client may be appropriate for home transfusion if (CCNS 2008) bullThere is at least one previous history of transfusion in hospital without a serious adverse reaction Clients who have never had a transfusion may be considered when the physician determines the benefits of home transfusion outweigh the risks bullThere is a history of adverse transfusion reactions that are of a controllable nature (ie fever controlled with medication) bullThere are physical limitations that would require ambulance transport to hospital for transfusion or hospital admission for transfusionbullThe client is alert cooperative and able to respond appropriately to body symptoms unless otherwise determined appropriate by the physician (particularly nursing home patients and pediatrics) bullThe client has a predictable stable medical condition without significant cardiovascular compromise (unstable angina CHF) bullThe client has adequate venous accessbullThere is a history of clinically significant red cell antibodies (reactive or not) provided antibody specificities are clearly identified There should be no unresolved serological findings
Giudelines for home transfusion 2014
CLINICAL ASSESSMENT
VARESETrasfusione di sangue a domicilio grazie allrsquoinfermiere di famigliaA pochi giorni dallapprovazione della riforma della sanitagrave a Varese avviene la prima trasfusione a casa di una paziente anziana allettata Levento possibile grazie alla collaborazione del medico di base
Pubblicato il 10 agosto 2015
Consegnata dallAIL oggi lunedigrave 2 dicembre la Fiat Panda in comodato duso gratuito per le attivitagrave di terapia trasfusionale domiciliare La Spezia
MARCHE SANITA TRASFUSIONI SANGUE A DOMICILIOAncona 17 ott (Adnkronos) - La Giunta della Regione Marche ha approvato il protocollo operativo sulla terapia trasfusionale domiciliare che prevede che i pazienti affetti da gravi malattie possano effettuare le trasfusioni nella propria abitazioni anziche in ospedale Lobiettivo -ha detto lassessore regionale alla Sanita Augusto Melappioni- e quello di venire incontro alle esigenze personali e terapeutiche dei malati che si trovano in precarie condizioni di salute riducendo allo stesso tempo i costi della prestazione
Trasfusione domiciliare premio nazionale allrsquoAsp di Ragusa4 ottobre 2016Per un progetto sulla sicurezza presentato da Giovanni Garozzo direttore della UOC di Medicina Trasfusionale ed Ematologia
0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient

Transfusions at home in patients with myelodysplasticsyndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
bull Inclusion criteria patient and disease
Caregiver
Home environment
bull Exclusion criteria patient and disease
caregiver
home environment
211 MDS patients transfusion dependent 7766 trasfusions 4980 domiciliary transfusionsHome Care program 5-years period (2006-2010)
Inclusion criteria
bull Patient living in Rome or in the near urban area covered by our HC service
bull Disease-related anemia refractory to all conventional measures
bull Physical limitations andor compromised clinical and personal status
bull Family and social problems resulting in the impossibility to travel to the hospital and to attend clinical visits and transfusion
bull Stable medical conditions
bull Adequate venous access
bull Informed and written consent
bull Responsible capable and collaborating adult suitable at home Other than a family member caregiver would be also a friend or a home-aid assistant
bull Deemed adequate and suitable for HC program In particular the home shouldbe deemed easily accessible clear comfortable and safe to perform the transfusion
bull Avalability of a functioning telephone
Patientanddisease
Caregiver
Home environment
Niscola P et al Leukemia Research 36 (2012) 684-688
Exclusion criteria
bull Patientrsquos refusalbull Urgent trasfusion in emergent clinical situationsbull Inadequate vascular accessbull Sepsisbull Anemia due to underlying causes (hemolysis active bleeding iron and
vitamins deficiency and so on) potentially resolvable by othermeasures whenever applicable
bull Positive indirect antiglobulin test and no antigen-negative donorsRBCs units (both for autoantibodies and alloantibodies)
bull Unresolved andor undiagnosed fever cardiovascular instabilityandor others active clinical illnesses
bull History of previous severe transfusion-related adverse reactions
bull Patient living alone no capable and responsible adult suitable ascaregiver
bull Poor home condidions home deemed unsafe and unsiutable fortransfusion
PatientAnddisease
Caregiver
Homeenvironment
Niscola P et al Leukemia Research 36 (2012) 684-688
Home transfusion (4980) clinical complications
Transfusions at home in patients with myelodysplastic syndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
Extravasationsvascular accessrelated hematoma 6(00012)
Fever (gt 38deg C) 2(00004)
Cardiorespiratory symptoms(fluid overload and other complications) 2(00004
Skin rash 1(00002)
Nausea and vomiting 1(00002)
Total 12(00024)
bullA maximum of 2 red blood cell units have been administred for each transfusion
bull All adverse reactions were managed at home a rapid resolution and an uncomplicated outcome wereobserved in all cases
Avantages of transfusion at home compared to hospital
bull Logistic no need to travel to the hospital no long waits for visits
bull Psychological less distressing and more comfortable in the patientrsquos ownhome environment
bull Medical less patientrsquos discomfort and energy expenditure decreasedinfections
bull QoL potential for better QoL
bull Safety and liability Higher attention and better monitoring to single patient at home potential for fewer transfusion errors and adversereactions
bull Cost free for patients and families The cost have been covered by the Public Health Care System and by a non profit organization
bull Social and economic potential for fewer days lost from work for family members
Niscola P et al Leukemia Research 36 (2012) 684-688
Disavantages of transfusion at home comparedto hospital
bull Logistic and organizational time expensive for the team
bull Medical distance from advanced medical service full reanimation measures not immediately available in anemergent situation
bull Safety and liability greater risk due to increased distancefrom hospital care and emergency services
bull Regulatory and legal concerns national and local laws and regulations should be considered before to providing the transfusion service at home
bull Costs more expensive for the health care agency
Niscola P et al Leukemia Research 36 (2012) 684-688
The hospital-at-home service (HHS) could be considered as an alternative to the traditional ward for elderly patients We aimed at evaluating the home management of elderly people requiring transfusions The ever-increasing demand on acute hospital services requires alternative methods of delivering all aspects of health care HHS demonstrated to be as efficacious as a traditional ward for elderly and functionally compromised patients The method was a retrospective descriptive study enrolling patients needing an hospital admission from 1st January 2007 to 31st December 2007 and reporting an hematological discharges diagnosis as primary or secondary diagnosis A total of 54 patients were evaluated in this study Of them 34 (629) needed a hemocomponent transfusion for a total volume of 112 blood units and 49 platelet pools Patients requiring at least one blood or platelet transfusion were more functionally compromised and presented a higher level of acute physiology and chronic health evaluation compared to the non-transfused ones The conclusion was that hematological subjects mainly the frail ones and functionally highly compromised with acute illnesses could be treated at home as an alternative of the traditional medical ward This could be the starting point for future studies that will be able to increase the power of hospital-at-home service for this type of patients
Home management of hematological patients requiring hospital admissionIsaia G1 Tibaldi V Astengo M Ladetto M Marinello R Bo M Michelis G Ruatta F Ricauda NA
Arch Gerontol Geriatr 2010 Nov-Dec51(3)309-11
The client may be appropriate for home transfusion if (CCNS 2008) bullThere is at least one previous history of transfusion in hospital without a serious adverse reaction Clients who have never had a transfusion may be considered when the physician determines the benefits of home transfusion outweigh the risks bullThere is a history of adverse transfusion reactions that are of a controllable nature (ie fever controlled with medication) bullThere are physical limitations that would require ambulance transport to hospital for transfusion or hospital admission for transfusionbullThe client is alert cooperative and able to respond appropriately to body symptoms unless otherwise determined appropriate by the physician (particularly nursing home patients and pediatrics) bullThe client has a predictable stable medical condition without significant cardiovascular compromise (unstable angina CHF) bullThe client has adequate venous accessbullThere is a history of clinically significant red cell antibodies (reactive or not) provided antibody specificities are clearly identified There should be no unresolved serological findings
Giudelines for home transfusion 2014
CLINICAL ASSESSMENT
VARESETrasfusione di sangue a domicilio grazie allrsquoinfermiere di famigliaA pochi giorni dallapprovazione della riforma della sanitagrave a Varese avviene la prima trasfusione a casa di una paziente anziana allettata Levento possibile grazie alla collaborazione del medico di base
Pubblicato il 10 agosto 2015
Consegnata dallAIL oggi lunedigrave 2 dicembre la Fiat Panda in comodato duso gratuito per le attivitagrave di terapia trasfusionale domiciliare La Spezia
MARCHE SANITA TRASFUSIONI SANGUE A DOMICILIOAncona 17 ott (Adnkronos) - La Giunta della Regione Marche ha approvato il protocollo operativo sulla terapia trasfusionale domiciliare che prevede che i pazienti affetti da gravi malattie possano effettuare le trasfusioni nella propria abitazioni anziche in ospedale Lobiettivo -ha detto lassessore regionale alla Sanita Augusto Melappioni- e quello di venire incontro alle esigenze personali e terapeutiche dei malati che si trovano in precarie condizioni di salute riducendo allo stesso tempo i costi della prestazione
Trasfusione domiciliare premio nazionale allrsquoAsp di Ragusa4 ottobre 2016Per un progetto sulla sicurezza presentato da Giovanni Garozzo direttore della UOC di Medicina Trasfusionale ed Ematologia
0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient
Inclusion criteria
bull Patient living in Rome or in the near urban area covered by our HC service
bull Disease-related anemia refractory to all conventional measures
bull Physical limitations andor compromised clinical and personal status
bull Family and social problems resulting in the impossibility to travel to the hospital and to attend clinical visits and transfusion
bull Stable medical conditions
bull Adequate venous access
bull Informed and written consent
bull Responsible capable and collaborating adult suitable at home Other than a family member caregiver would be also a friend or a home-aid assistant
bull Deemed adequate and suitable for HC program In particular the home shouldbe deemed easily accessible clear comfortable and safe to perform the transfusion
bull Avalability of a functioning telephone
Patientanddisease
Caregiver
Home environment
Niscola P et al Leukemia Research 36 (2012) 684-688
Exclusion criteria
bull Patientrsquos refusalbull Urgent trasfusion in emergent clinical situationsbull Inadequate vascular accessbull Sepsisbull Anemia due to underlying causes (hemolysis active bleeding iron and
vitamins deficiency and so on) potentially resolvable by othermeasures whenever applicable
bull Positive indirect antiglobulin test and no antigen-negative donorsRBCs units (both for autoantibodies and alloantibodies)
bull Unresolved andor undiagnosed fever cardiovascular instabilityandor others active clinical illnesses
bull History of previous severe transfusion-related adverse reactions
bull Patient living alone no capable and responsible adult suitable ascaregiver
bull Poor home condidions home deemed unsafe and unsiutable fortransfusion
PatientAnddisease
Caregiver
Homeenvironment
Niscola P et al Leukemia Research 36 (2012) 684-688
Home transfusion (4980) clinical complications
Transfusions at home in patients with myelodysplastic syndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
Extravasationsvascular accessrelated hematoma 6(00012)
Fever (gt 38deg C) 2(00004)
Cardiorespiratory symptoms(fluid overload and other complications) 2(00004
Skin rash 1(00002)
Nausea and vomiting 1(00002)
Total 12(00024)
bullA maximum of 2 red blood cell units have been administred for each transfusion
bull All adverse reactions were managed at home a rapid resolution and an uncomplicated outcome wereobserved in all cases
Avantages of transfusion at home compared to hospital
bull Logistic no need to travel to the hospital no long waits for visits
bull Psychological less distressing and more comfortable in the patientrsquos ownhome environment
bull Medical less patientrsquos discomfort and energy expenditure decreasedinfections
bull QoL potential for better QoL
bull Safety and liability Higher attention and better monitoring to single patient at home potential for fewer transfusion errors and adversereactions
bull Cost free for patients and families The cost have been covered by the Public Health Care System and by a non profit organization
bull Social and economic potential for fewer days lost from work for family members
Niscola P et al Leukemia Research 36 (2012) 684-688
Disavantages of transfusion at home comparedto hospital
bull Logistic and organizational time expensive for the team
bull Medical distance from advanced medical service full reanimation measures not immediately available in anemergent situation
bull Safety and liability greater risk due to increased distancefrom hospital care and emergency services
bull Regulatory and legal concerns national and local laws and regulations should be considered before to providing the transfusion service at home
bull Costs more expensive for the health care agency
Niscola P et al Leukemia Research 36 (2012) 684-688
The hospital-at-home service (HHS) could be considered as an alternative to the traditional ward for elderly patients We aimed at evaluating the home management of elderly people requiring transfusions The ever-increasing demand on acute hospital services requires alternative methods of delivering all aspects of health care HHS demonstrated to be as efficacious as a traditional ward for elderly and functionally compromised patients The method was a retrospective descriptive study enrolling patients needing an hospital admission from 1st January 2007 to 31st December 2007 and reporting an hematological discharges diagnosis as primary or secondary diagnosis A total of 54 patients were evaluated in this study Of them 34 (629) needed a hemocomponent transfusion for a total volume of 112 blood units and 49 platelet pools Patients requiring at least one blood or platelet transfusion were more functionally compromised and presented a higher level of acute physiology and chronic health evaluation compared to the non-transfused ones The conclusion was that hematological subjects mainly the frail ones and functionally highly compromised with acute illnesses could be treated at home as an alternative of the traditional medical ward This could be the starting point for future studies that will be able to increase the power of hospital-at-home service for this type of patients
Home management of hematological patients requiring hospital admissionIsaia G1 Tibaldi V Astengo M Ladetto M Marinello R Bo M Michelis G Ruatta F Ricauda NA
Arch Gerontol Geriatr 2010 Nov-Dec51(3)309-11
The client may be appropriate for home transfusion if (CCNS 2008) bullThere is at least one previous history of transfusion in hospital without a serious adverse reaction Clients who have never had a transfusion may be considered when the physician determines the benefits of home transfusion outweigh the risks bullThere is a history of adverse transfusion reactions that are of a controllable nature (ie fever controlled with medication) bullThere are physical limitations that would require ambulance transport to hospital for transfusion or hospital admission for transfusionbullThe client is alert cooperative and able to respond appropriately to body symptoms unless otherwise determined appropriate by the physician (particularly nursing home patients and pediatrics) bullThe client has a predictable stable medical condition without significant cardiovascular compromise (unstable angina CHF) bullThe client has adequate venous accessbullThere is a history of clinically significant red cell antibodies (reactive or not) provided antibody specificities are clearly identified There should be no unresolved serological findings
Giudelines for home transfusion 2014
CLINICAL ASSESSMENT
VARESETrasfusione di sangue a domicilio grazie allrsquoinfermiere di famigliaA pochi giorni dallapprovazione della riforma della sanitagrave a Varese avviene la prima trasfusione a casa di una paziente anziana allettata Levento possibile grazie alla collaborazione del medico di base
Pubblicato il 10 agosto 2015
Consegnata dallAIL oggi lunedigrave 2 dicembre la Fiat Panda in comodato duso gratuito per le attivitagrave di terapia trasfusionale domiciliare La Spezia
MARCHE SANITA TRASFUSIONI SANGUE A DOMICILIOAncona 17 ott (Adnkronos) - La Giunta della Regione Marche ha approvato il protocollo operativo sulla terapia trasfusionale domiciliare che prevede che i pazienti affetti da gravi malattie possano effettuare le trasfusioni nella propria abitazioni anziche in ospedale Lobiettivo -ha detto lassessore regionale alla Sanita Augusto Melappioni- e quello di venire incontro alle esigenze personali e terapeutiche dei malati che si trovano in precarie condizioni di salute riducendo allo stesso tempo i costi della prestazione
Trasfusione domiciliare premio nazionale allrsquoAsp di Ragusa4 ottobre 2016Per un progetto sulla sicurezza presentato da Giovanni Garozzo direttore della UOC di Medicina Trasfusionale ed Ematologia
0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient

Exclusion criteria
bull Patientrsquos refusalbull Urgent trasfusion in emergent clinical situationsbull Inadequate vascular accessbull Sepsisbull Anemia due to underlying causes (hemolysis active bleeding iron and
vitamins deficiency and so on) potentially resolvable by othermeasures whenever applicable
bull Positive indirect antiglobulin test and no antigen-negative donorsRBCs units (both for autoantibodies and alloantibodies)
bull Unresolved andor undiagnosed fever cardiovascular instabilityandor others active clinical illnesses
bull History of previous severe transfusion-related adverse reactions
bull Patient living alone no capable and responsible adult suitable ascaregiver
bull Poor home condidions home deemed unsafe and unsiutable fortransfusion
PatientAnddisease
Caregiver
Homeenvironment
Niscola P et al Leukemia Research 36 (2012) 684-688
Home transfusion (4980) clinical complications
Transfusions at home in patients with myelodysplastic syndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
Extravasationsvascular accessrelated hematoma 6(00012)
Fever (gt 38deg C) 2(00004)
Cardiorespiratory symptoms(fluid overload and other complications) 2(00004
Skin rash 1(00002)
Nausea and vomiting 1(00002)
Total 12(00024)
bullA maximum of 2 red blood cell units have been administred for each transfusion
bull All adverse reactions were managed at home a rapid resolution and an uncomplicated outcome wereobserved in all cases
Avantages of transfusion at home compared to hospital
bull Logistic no need to travel to the hospital no long waits for visits
bull Psychological less distressing and more comfortable in the patientrsquos ownhome environment
bull Medical less patientrsquos discomfort and energy expenditure decreasedinfections
bull QoL potential for better QoL
bull Safety and liability Higher attention and better monitoring to single patient at home potential for fewer transfusion errors and adversereactions
bull Cost free for patients and families The cost have been covered by the Public Health Care System and by a non profit organization
bull Social and economic potential for fewer days lost from work for family members
Niscola P et al Leukemia Research 36 (2012) 684-688
Disavantages of transfusion at home comparedto hospital
bull Logistic and organizational time expensive for the team
bull Medical distance from advanced medical service full reanimation measures not immediately available in anemergent situation
bull Safety and liability greater risk due to increased distancefrom hospital care and emergency services
bull Regulatory and legal concerns national and local laws and regulations should be considered before to providing the transfusion service at home
bull Costs more expensive for the health care agency
Niscola P et al Leukemia Research 36 (2012) 684-688
The hospital-at-home service (HHS) could be considered as an alternative to the traditional ward for elderly patients We aimed at evaluating the home management of elderly people requiring transfusions The ever-increasing demand on acute hospital services requires alternative methods of delivering all aspects of health care HHS demonstrated to be as efficacious as a traditional ward for elderly and functionally compromised patients The method was a retrospective descriptive study enrolling patients needing an hospital admission from 1st January 2007 to 31st December 2007 and reporting an hematological discharges diagnosis as primary or secondary diagnosis A total of 54 patients were evaluated in this study Of them 34 (629) needed a hemocomponent transfusion for a total volume of 112 blood units and 49 platelet pools Patients requiring at least one blood or platelet transfusion were more functionally compromised and presented a higher level of acute physiology and chronic health evaluation compared to the non-transfused ones The conclusion was that hematological subjects mainly the frail ones and functionally highly compromised with acute illnesses could be treated at home as an alternative of the traditional medical ward This could be the starting point for future studies that will be able to increase the power of hospital-at-home service for this type of patients
Home management of hematological patients requiring hospital admissionIsaia G1 Tibaldi V Astengo M Ladetto M Marinello R Bo M Michelis G Ruatta F Ricauda NA
Arch Gerontol Geriatr 2010 Nov-Dec51(3)309-11
The client may be appropriate for home transfusion if (CCNS 2008) bullThere is at least one previous history of transfusion in hospital without a serious adverse reaction Clients who have never had a transfusion may be considered when the physician determines the benefits of home transfusion outweigh the risks bullThere is a history of adverse transfusion reactions that are of a controllable nature (ie fever controlled with medication) bullThere are physical limitations that would require ambulance transport to hospital for transfusion or hospital admission for transfusionbullThe client is alert cooperative and able to respond appropriately to body symptoms unless otherwise determined appropriate by the physician (particularly nursing home patients and pediatrics) bullThe client has a predictable stable medical condition without significant cardiovascular compromise (unstable angina CHF) bullThe client has adequate venous accessbullThere is a history of clinically significant red cell antibodies (reactive or not) provided antibody specificities are clearly identified There should be no unresolved serological findings
Giudelines for home transfusion 2014
CLINICAL ASSESSMENT
VARESETrasfusione di sangue a domicilio grazie allrsquoinfermiere di famigliaA pochi giorni dallapprovazione della riforma della sanitagrave a Varese avviene la prima trasfusione a casa di una paziente anziana allettata Levento possibile grazie alla collaborazione del medico di base
Pubblicato il 10 agosto 2015
Consegnata dallAIL oggi lunedigrave 2 dicembre la Fiat Panda in comodato duso gratuito per le attivitagrave di terapia trasfusionale domiciliare La Spezia
MARCHE SANITA TRASFUSIONI SANGUE A DOMICILIOAncona 17 ott (Adnkronos) - La Giunta della Regione Marche ha approvato il protocollo operativo sulla terapia trasfusionale domiciliare che prevede che i pazienti affetti da gravi malattie possano effettuare le trasfusioni nella propria abitazioni anziche in ospedale Lobiettivo -ha detto lassessore regionale alla Sanita Augusto Melappioni- e quello di venire incontro alle esigenze personali e terapeutiche dei malati che si trovano in precarie condizioni di salute riducendo allo stesso tempo i costi della prestazione
Trasfusione domiciliare premio nazionale allrsquoAsp di Ragusa4 ottobre 2016Per un progetto sulla sicurezza presentato da Giovanni Garozzo direttore della UOC di Medicina Trasfusionale ed Ematologia
0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient

Home transfusion (4980) clinical complications
Transfusions at home in patients with myelodysplastic syndromesNiscola P et al Leukemia Research 36 (2012) 684-688Hematology Unit S Eugenio Hospital Rome Italy
Extravasationsvascular accessrelated hematoma 6(00012)
Fever (gt 38deg C) 2(00004)
Cardiorespiratory symptoms(fluid overload and other complications) 2(00004
Skin rash 1(00002)
Nausea and vomiting 1(00002)
Total 12(00024)
bullA maximum of 2 red blood cell units have been administred for each transfusion
bull All adverse reactions were managed at home a rapid resolution and an uncomplicated outcome wereobserved in all cases
Avantages of transfusion at home compared to hospital
bull Logistic no need to travel to the hospital no long waits for visits
bull Psychological less distressing and more comfortable in the patientrsquos ownhome environment
bull Medical less patientrsquos discomfort and energy expenditure decreasedinfections
bull QoL potential for better QoL
bull Safety and liability Higher attention and better monitoring to single patient at home potential for fewer transfusion errors and adversereactions
bull Cost free for patients and families The cost have been covered by the Public Health Care System and by a non profit organization
bull Social and economic potential for fewer days lost from work for family members
Niscola P et al Leukemia Research 36 (2012) 684-688
Disavantages of transfusion at home comparedto hospital
bull Logistic and organizational time expensive for the team
bull Medical distance from advanced medical service full reanimation measures not immediately available in anemergent situation
bull Safety and liability greater risk due to increased distancefrom hospital care and emergency services
bull Regulatory and legal concerns national and local laws and regulations should be considered before to providing the transfusion service at home
bull Costs more expensive for the health care agency
Niscola P et al Leukemia Research 36 (2012) 684-688
The hospital-at-home service (HHS) could be considered as an alternative to the traditional ward for elderly patients We aimed at evaluating the home management of elderly people requiring transfusions The ever-increasing demand on acute hospital services requires alternative methods of delivering all aspects of health care HHS demonstrated to be as efficacious as a traditional ward for elderly and functionally compromised patients The method was a retrospective descriptive study enrolling patients needing an hospital admission from 1st January 2007 to 31st December 2007 and reporting an hematological discharges diagnosis as primary or secondary diagnosis A total of 54 patients were evaluated in this study Of them 34 (629) needed a hemocomponent transfusion for a total volume of 112 blood units and 49 platelet pools Patients requiring at least one blood or platelet transfusion were more functionally compromised and presented a higher level of acute physiology and chronic health evaluation compared to the non-transfused ones The conclusion was that hematological subjects mainly the frail ones and functionally highly compromised with acute illnesses could be treated at home as an alternative of the traditional medical ward This could be the starting point for future studies that will be able to increase the power of hospital-at-home service for this type of patients
Home management of hematological patients requiring hospital admissionIsaia G1 Tibaldi V Astengo M Ladetto M Marinello R Bo M Michelis G Ruatta F Ricauda NA
Arch Gerontol Geriatr 2010 Nov-Dec51(3)309-11
The client may be appropriate for home transfusion if (CCNS 2008) bullThere is at least one previous history of transfusion in hospital without a serious adverse reaction Clients who have never had a transfusion may be considered when the physician determines the benefits of home transfusion outweigh the risks bullThere is a history of adverse transfusion reactions that are of a controllable nature (ie fever controlled with medication) bullThere are physical limitations that would require ambulance transport to hospital for transfusion or hospital admission for transfusionbullThe client is alert cooperative and able to respond appropriately to body symptoms unless otherwise determined appropriate by the physician (particularly nursing home patients and pediatrics) bullThe client has a predictable stable medical condition without significant cardiovascular compromise (unstable angina CHF) bullThe client has adequate venous accessbullThere is a history of clinically significant red cell antibodies (reactive or not) provided antibody specificities are clearly identified There should be no unresolved serological findings
Giudelines for home transfusion 2014
CLINICAL ASSESSMENT
VARESETrasfusione di sangue a domicilio grazie allrsquoinfermiere di famigliaA pochi giorni dallapprovazione della riforma della sanitagrave a Varese avviene la prima trasfusione a casa di una paziente anziana allettata Levento possibile grazie alla collaborazione del medico di base
Pubblicato il 10 agosto 2015
Consegnata dallAIL oggi lunedigrave 2 dicembre la Fiat Panda in comodato duso gratuito per le attivitagrave di terapia trasfusionale domiciliare La Spezia
MARCHE SANITA TRASFUSIONI SANGUE A DOMICILIOAncona 17 ott (Adnkronos) - La Giunta della Regione Marche ha approvato il protocollo operativo sulla terapia trasfusionale domiciliare che prevede che i pazienti affetti da gravi malattie possano effettuare le trasfusioni nella propria abitazioni anziche in ospedale Lobiettivo -ha detto lassessore regionale alla Sanita Augusto Melappioni- e quello di venire incontro alle esigenze personali e terapeutiche dei malati che si trovano in precarie condizioni di salute riducendo allo stesso tempo i costi della prestazione
Trasfusione domiciliare premio nazionale allrsquoAsp di Ragusa4 ottobre 2016Per un progetto sulla sicurezza presentato da Giovanni Garozzo direttore della UOC di Medicina Trasfusionale ed Ematologia
0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient

Avantages of transfusion at home compared to hospital
bull Logistic no need to travel to the hospital no long waits for visits
bull Psychological less distressing and more comfortable in the patientrsquos ownhome environment
bull Medical less patientrsquos discomfort and energy expenditure decreasedinfections
bull QoL potential for better QoL
bull Safety and liability Higher attention and better monitoring to single patient at home potential for fewer transfusion errors and adversereactions
bull Cost free for patients and families The cost have been covered by the Public Health Care System and by a non profit organization
bull Social and economic potential for fewer days lost from work for family members
Niscola P et al Leukemia Research 36 (2012) 684-688
Disavantages of transfusion at home comparedto hospital
bull Logistic and organizational time expensive for the team
bull Medical distance from advanced medical service full reanimation measures not immediately available in anemergent situation
bull Safety and liability greater risk due to increased distancefrom hospital care and emergency services
bull Regulatory and legal concerns national and local laws and regulations should be considered before to providing the transfusion service at home
bull Costs more expensive for the health care agency
Niscola P et al Leukemia Research 36 (2012) 684-688
The hospital-at-home service (HHS) could be considered as an alternative to the traditional ward for elderly patients We aimed at evaluating the home management of elderly people requiring transfusions The ever-increasing demand on acute hospital services requires alternative methods of delivering all aspects of health care HHS demonstrated to be as efficacious as a traditional ward for elderly and functionally compromised patients The method was a retrospective descriptive study enrolling patients needing an hospital admission from 1st January 2007 to 31st December 2007 and reporting an hematological discharges diagnosis as primary or secondary diagnosis A total of 54 patients were evaluated in this study Of them 34 (629) needed a hemocomponent transfusion for a total volume of 112 blood units and 49 platelet pools Patients requiring at least one blood or platelet transfusion were more functionally compromised and presented a higher level of acute physiology and chronic health evaluation compared to the non-transfused ones The conclusion was that hematological subjects mainly the frail ones and functionally highly compromised with acute illnesses could be treated at home as an alternative of the traditional medical ward This could be the starting point for future studies that will be able to increase the power of hospital-at-home service for this type of patients
Home management of hematological patients requiring hospital admissionIsaia G1 Tibaldi V Astengo M Ladetto M Marinello R Bo M Michelis G Ruatta F Ricauda NA
Arch Gerontol Geriatr 2010 Nov-Dec51(3)309-11
The client may be appropriate for home transfusion if (CCNS 2008) bullThere is at least one previous history of transfusion in hospital without a serious adverse reaction Clients who have never had a transfusion may be considered when the physician determines the benefits of home transfusion outweigh the risks bullThere is a history of adverse transfusion reactions that are of a controllable nature (ie fever controlled with medication) bullThere are physical limitations that would require ambulance transport to hospital for transfusion or hospital admission for transfusionbullThe client is alert cooperative and able to respond appropriately to body symptoms unless otherwise determined appropriate by the physician (particularly nursing home patients and pediatrics) bullThe client has a predictable stable medical condition without significant cardiovascular compromise (unstable angina CHF) bullThe client has adequate venous accessbullThere is a history of clinically significant red cell antibodies (reactive or not) provided antibody specificities are clearly identified There should be no unresolved serological findings
Giudelines for home transfusion 2014
CLINICAL ASSESSMENT
VARESETrasfusione di sangue a domicilio grazie allrsquoinfermiere di famigliaA pochi giorni dallapprovazione della riforma della sanitagrave a Varese avviene la prima trasfusione a casa di una paziente anziana allettata Levento possibile grazie alla collaborazione del medico di base
Pubblicato il 10 agosto 2015
Consegnata dallAIL oggi lunedigrave 2 dicembre la Fiat Panda in comodato duso gratuito per le attivitagrave di terapia trasfusionale domiciliare La Spezia
MARCHE SANITA TRASFUSIONI SANGUE A DOMICILIOAncona 17 ott (Adnkronos) - La Giunta della Regione Marche ha approvato il protocollo operativo sulla terapia trasfusionale domiciliare che prevede che i pazienti affetti da gravi malattie possano effettuare le trasfusioni nella propria abitazioni anziche in ospedale Lobiettivo -ha detto lassessore regionale alla Sanita Augusto Melappioni- e quello di venire incontro alle esigenze personali e terapeutiche dei malati che si trovano in precarie condizioni di salute riducendo allo stesso tempo i costi della prestazione
Trasfusione domiciliare premio nazionale allrsquoAsp di Ragusa4 ottobre 2016Per un progetto sulla sicurezza presentato da Giovanni Garozzo direttore della UOC di Medicina Trasfusionale ed Ematologia
0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient

Disavantages of transfusion at home comparedto hospital
bull Logistic and organizational time expensive for the team
bull Medical distance from advanced medical service full reanimation measures not immediately available in anemergent situation
bull Safety and liability greater risk due to increased distancefrom hospital care and emergency services
bull Regulatory and legal concerns national and local laws and regulations should be considered before to providing the transfusion service at home
bull Costs more expensive for the health care agency
Niscola P et al Leukemia Research 36 (2012) 684-688
The hospital-at-home service (HHS) could be considered as an alternative to the traditional ward for elderly patients We aimed at evaluating the home management of elderly people requiring transfusions The ever-increasing demand on acute hospital services requires alternative methods of delivering all aspects of health care HHS demonstrated to be as efficacious as a traditional ward for elderly and functionally compromised patients The method was a retrospective descriptive study enrolling patients needing an hospital admission from 1st January 2007 to 31st December 2007 and reporting an hematological discharges diagnosis as primary or secondary diagnosis A total of 54 patients were evaluated in this study Of them 34 (629) needed a hemocomponent transfusion for a total volume of 112 blood units and 49 platelet pools Patients requiring at least one blood or platelet transfusion were more functionally compromised and presented a higher level of acute physiology and chronic health evaluation compared to the non-transfused ones The conclusion was that hematological subjects mainly the frail ones and functionally highly compromised with acute illnesses could be treated at home as an alternative of the traditional medical ward This could be the starting point for future studies that will be able to increase the power of hospital-at-home service for this type of patients
Home management of hematological patients requiring hospital admissionIsaia G1 Tibaldi V Astengo M Ladetto M Marinello R Bo M Michelis G Ruatta F Ricauda NA
Arch Gerontol Geriatr 2010 Nov-Dec51(3)309-11
The client may be appropriate for home transfusion if (CCNS 2008) bullThere is at least one previous history of transfusion in hospital without a serious adverse reaction Clients who have never had a transfusion may be considered when the physician determines the benefits of home transfusion outweigh the risks bullThere is a history of adverse transfusion reactions that are of a controllable nature (ie fever controlled with medication) bullThere are physical limitations that would require ambulance transport to hospital for transfusion or hospital admission for transfusionbullThe client is alert cooperative and able to respond appropriately to body symptoms unless otherwise determined appropriate by the physician (particularly nursing home patients and pediatrics) bullThe client has a predictable stable medical condition without significant cardiovascular compromise (unstable angina CHF) bullThe client has adequate venous accessbullThere is a history of clinically significant red cell antibodies (reactive or not) provided antibody specificities are clearly identified There should be no unresolved serological findings
Giudelines for home transfusion 2014
CLINICAL ASSESSMENT
VARESETrasfusione di sangue a domicilio grazie allrsquoinfermiere di famigliaA pochi giorni dallapprovazione della riforma della sanitagrave a Varese avviene la prima trasfusione a casa di una paziente anziana allettata Levento possibile grazie alla collaborazione del medico di base
Pubblicato il 10 agosto 2015
Consegnata dallAIL oggi lunedigrave 2 dicembre la Fiat Panda in comodato duso gratuito per le attivitagrave di terapia trasfusionale domiciliare La Spezia
MARCHE SANITA TRASFUSIONI SANGUE A DOMICILIOAncona 17 ott (Adnkronos) - La Giunta della Regione Marche ha approvato il protocollo operativo sulla terapia trasfusionale domiciliare che prevede che i pazienti affetti da gravi malattie possano effettuare le trasfusioni nella propria abitazioni anziche in ospedale Lobiettivo -ha detto lassessore regionale alla Sanita Augusto Melappioni- e quello di venire incontro alle esigenze personali e terapeutiche dei malati che si trovano in precarie condizioni di salute riducendo allo stesso tempo i costi della prestazione
Trasfusione domiciliare premio nazionale allrsquoAsp di Ragusa4 ottobre 2016Per un progetto sulla sicurezza presentato da Giovanni Garozzo direttore della UOC di Medicina Trasfusionale ed Ematologia
0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient
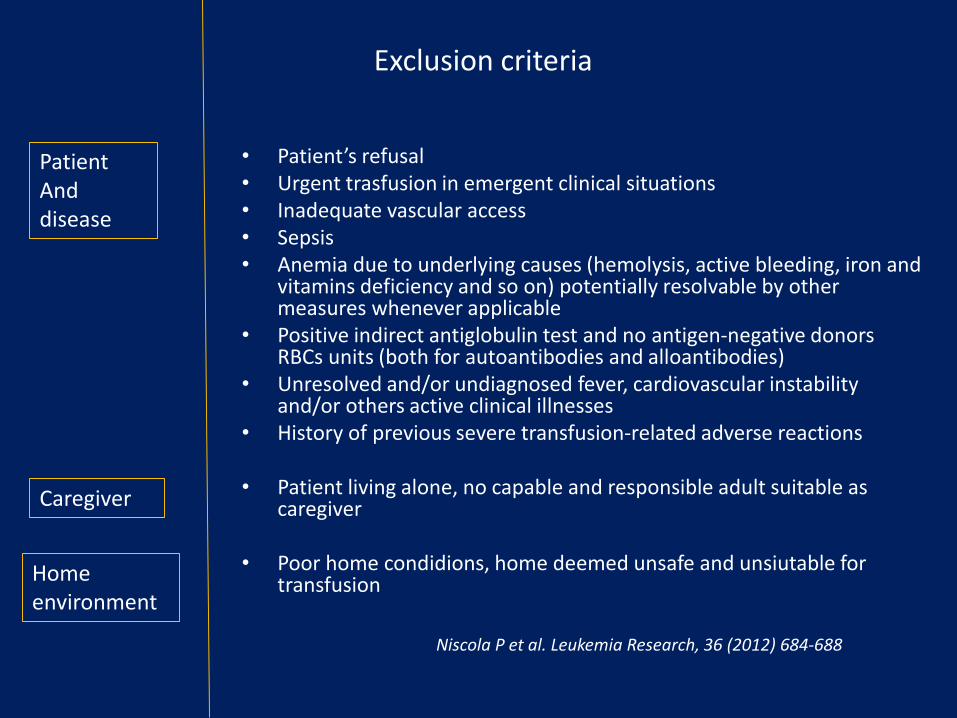
The hospital-at-home service (HHS) could be considered as an alternative to the traditional ward for elderly patients We aimed at evaluating the home management of elderly people requiring transfusions The ever-increasing demand on acute hospital services requires alternative methods of delivering all aspects of health care HHS demonstrated to be as efficacious as a traditional ward for elderly and functionally compromised patients The method was a retrospective descriptive study enrolling patients needing an hospital admission from 1st January 2007 to 31st December 2007 and reporting an hematological discharges diagnosis as primary or secondary diagnosis A total of 54 patients were evaluated in this study Of them 34 (629) needed a hemocomponent transfusion for a total volume of 112 blood units and 49 platelet pools Patients requiring at least one blood or platelet transfusion were more functionally compromised and presented a higher level of acute physiology and chronic health evaluation compared to the non-transfused ones The conclusion was that hematological subjects mainly the frail ones and functionally highly compromised with acute illnesses could be treated at home as an alternative of the traditional medical ward This could be the starting point for future studies that will be able to increase the power of hospital-at-home service for this type of patients
Home management of hematological patients requiring hospital admissionIsaia G1 Tibaldi V Astengo M Ladetto M Marinello R Bo M Michelis G Ruatta F Ricauda NA
Arch Gerontol Geriatr 2010 Nov-Dec51(3)309-11
The client may be appropriate for home transfusion if (CCNS 2008) bullThere is at least one previous history of transfusion in hospital without a serious adverse reaction Clients who have never had a transfusion may be considered when the physician determines the benefits of home transfusion outweigh the risks bullThere is a history of adverse transfusion reactions that are of a controllable nature (ie fever controlled with medication) bullThere are physical limitations that would require ambulance transport to hospital for transfusion or hospital admission for transfusionbullThe client is alert cooperative and able to respond appropriately to body symptoms unless otherwise determined appropriate by the physician (particularly nursing home patients and pediatrics) bullThe client has a predictable stable medical condition without significant cardiovascular compromise (unstable angina CHF) bullThe client has adequate venous accessbullThere is a history of clinically significant red cell antibodies (reactive or not) provided antibody specificities are clearly identified There should be no unresolved serological findings
Giudelines for home transfusion 2014
CLINICAL ASSESSMENT
VARESETrasfusione di sangue a domicilio grazie allrsquoinfermiere di famigliaA pochi giorni dallapprovazione della riforma della sanitagrave a Varese avviene la prima trasfusione a casa di una paziente anziana allettata Levento possibile grazie alla collaborazione del medico di base
Pubblicato il 10 agosto 2015
Consegnata dallAIL oggi lunedigrave 2 dicembre la Fiat Panda in comodato duso gratuito per le attivitagrave di terapia trasfusionale domiciliare La Spezia
MARCHE SANITA TRASFUSIONI SANGUE A DOMICILIOAncona 17 ott (Adnkronos) - La Giunta della Regione Marche ha approvato il protocollo operativo sulla terapia trasfusionale domiciliare che prevede che i pazienti affetti da gravi malattie possano effettuare le trasfusioni nella propria abitazioni anziche in ospedale Lobiettivo -ha detto lassessore regionale alla Sanita Augusto Melappioni- e quello di venire incontro alle esigenze personali e terapeutiche dei malati che si trovano in precarie condizioni di salute riducendo allo stesso tempo i costi della prestazione
Trasfusione domiciliare premio nazionale allrsquoAsp di Ragusa4 ottobre 2016Per un progetto sulla sicurezza presentato da Giovanni Garozzo direttore della UOC di Medicina Trasfusionale ed Ematologia
0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient

The client may be appropriate for home transfusion if (CCNS 2008) bullThere is at least one previous history of transfusion in hospital without a serious adverse reaction Clients who have never had a transfusion may be considered when the physician determines the benefits of home transfusion outweigh the risks bullThere is a history of adverse transfusion reactions that are of a controllable nature (ie fever controlled with medication) bullThere are physical limitations that would require ambulance transport to hospital for transfusion or hospital admission for transfusionbullThe client is alert cooperative and able to respond appropriately to body symptoms unless otherwise determined appropriate by the physician (particularly nursing home patients and pediatrics) bullThe client has a predictable stable medical condition without significant cardiovascular compromise (unstable angina CHF) bullThe client has adequate venous accessbullThere is a history of clinically significant red cell antibodies (reactive or not) provided antibody specificities are clearly identified There should be no unresolved serological findings
Giudelines for home transfusion 2014
CLINICAL ASSESSMENT
VARESETrasfusione di sangue a domicilio grazie allrsquoinfermiere di famigliaA pochi giorni dallapprovazione della riforma della sanitagrave a Varese avviene la prima trasfusione a casa di una paziente anziana allettata Levento possibile grazie alla collaborazione del medico di base
Pubblicato il 10 agosto 2015
Consegnata dallAIL oggi lunedigrave 2 dicembre la Fiat Panda in comodato duso gratuito per le attivitagrave di terapia trasfusionale domiciliare La Spezia
MARCHE SANITA TRASFUSIONI SANGUE A DOMICILIOAncona 17 ott (Adnkronos) - La Giunta della Regione Marche ha approvato il protocollo operativo sulla terapia trasfusionale domiciliare che prevede che i pazienti affetti da gravi malattie possano effettuare le trasfusioni nella propria abitazioni anziche in ospedale Lobiettivo -ha detto lassessore regionale alla Sanita Augusto Melappioni- e quello di venire incontro alle esigenze personali e terapeutiche dei malati che si trovano in precarie condizioni di salute riducendo allo stesso tempo i costi della prestazione
Trasfusione domiciliare premio nazionale allrsquoAsp di Ragusa4 ottobre 2016Per un progetto sulla sicurezza presentato da Giovanni Garozzo direttore della UOC di Medicina Trasfusionale ed Ematologia
0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient

VARESETrasfusione di sangue a domicilio grazie allrsquoinfermiere di famigliaA pochi giorni dallapprovazione della riforma della sanitagrave a Varese avviene la prima trasfusione a casa di una paziente anziana allettata Levento possibile grazie alla collaborazione del medico di base
Pubblicato il 10 agosto 2015
Consegnata dallAIL oggi lunedigrave 2 dicembre la Fiat Panda in comodato duso gratuito per le attivitagrave di terapia trasfusionale domiciliare La Spezia
MARCHE SANITA TRASFUSIONI SANGUE A DOMICILIOAncona 17 ott (Adnkronos) - La Giunta della Regione Marche ha approvato il protocollo operativo sulla terapia trasfusionale domiciliare che prevede che i pazienti affetti da gravi malattie possano effettuare le trasfusioni nella propria abitazioni anziche in ospedale Lobiettivo -ha detto lassessore regionale alla Sanita Augusto Melappioni- e quello di venire incontro alle esigenze personali e terapeutiche dei malati che si trovano in precarie condizioni di salute riducendo allo stesso tempo i costi della prestazione
Trasfusione domiciliare premio nazionale allrsquoAsp di Ragusa4 ottobre 2016Per un progetto sulla sicurezza presentato da Giovanni Garozzo direttore della UOC di Medicina Trasfusionale ed Ematologia
0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient

0
100
200
300
400
500
600
Emotrasfusioni
2011
2012
2013
2014
2015
2016
Trasfusioni in Ospedalizzazione a Domicilio
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient
ALLEGATO 2Materiale e farmaci che devono essere disponibili durante la trasfusione a domicilio
In caso di emotrasfusione a domicilio si deve prevedere la disponibilitagrave al domicilio del seguente materiale n 2 aghi cannula (18-20) n 1 unitagrave di soluzione fisiologica da 250 ml n 2 unitagrave di soluzione fisiologica da 100 ml n 2 fiale di soluzione fisiologica da 10 ml n 2 siringhe da 10 ml n 2 siringhe da 20 mln 1 scatola di Adrenalina da 1 mg fiale (da conservare in frigorifero)una confezione Urbason 20 mg Solu-Medrol 40 mg Solu-Medrol 125 mg n 2 fl Flebocortid1 gr (Solucortef 1gr) n 1 confezione di Furosemide fiale 20 mgn 1 confezione Diazepam fiale 10 mg n 1 confezione Trimeton fiale 10 mgn 1 confezione Broncovaleasn 1 flacone di paracetamolo 1000 mgAntibiotici ad ampio spettro
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient
Conclusioni
bull Norme esistenti
bull Selezione del paziente per patologia stato funzionale caregiver condizioni ambientali
bull Modello organizzativo
bull Collaborazione tra i diversi servizi coinvolti
bull Analisi dei costi
Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient

Forse egrave necessario buttare il cuore oltre lrsquoostacolo e non ritenere sicure solo le mura ospedaliere
Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient

Out-patient management of aplasia induced
by curatively intended consolidation
chemotherapy in patients with acute myeloid
leukemia
Study coordinators
Stefano DrsquoArdia MD Section of Hematology Department of Oncology and Hematology AOU Cittagrave
della Salute e della Scienza Hospital Turin Italy
Marinello Renata MD Home Hospitalization Service Department of Medical and Surgical
Science Section of Gerontology AOU Cittagrave della Salute e della Scienza Hospital Turin Italy
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient
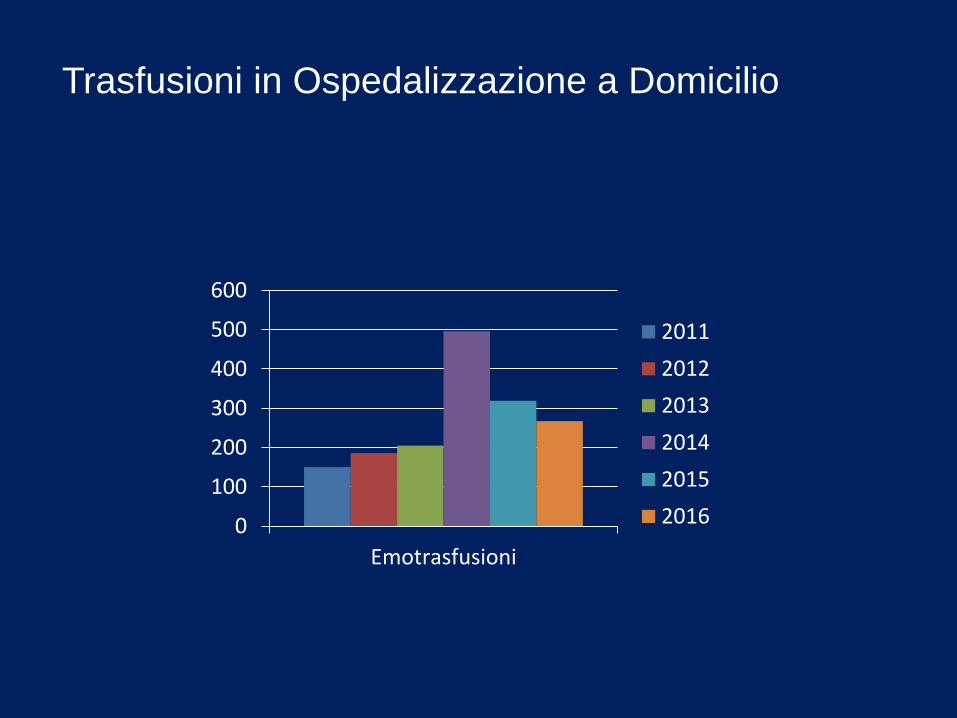
Disegno dello studio trial clinico non randomizzato
Obiettivo dello studio fattibilitagrave e sicurezza della gestione della fase di neutropenia indotta da chemioterapia di consolidamento in pazienti affetti da Leucemia Mieloide Acuta in regime di Ospedalizzazione a Domicilio (OAD)
Co-Primary endpointa) probabilitagrave di reingresso per i pazienti trattati in OADb) complicanze infettive nei diversi setting di curac) durata delle complicanzed) fabbisogno trasfusionalee) qualitagrave della vita durante la fase di aplasiaf) qualitagrave della vita dei caregiversg) valutazione dei costi nei diversi setting di cura
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient
55 Diagnostic steps in case of fever (gt380 C) in aplasiaaccording to ECIL3 IDSA SIE and NCCN guidelines
- In case of fever immediate contact with the on duty call service with following immediate access to patients home (lt45min) and initiation of diagnostic and therapeutic procedures- Peripheral blood cultures (2 sets) - Clinical examination with the determination of the National Early Warning Score (NEWS Table 14)24
- Chest X-ray - Further diagnostic tests according to the clinical symptoms of the patient
