la appendage closure devices,final (2)
TRANSCRIPT

LA APPENDAGE CLOSURE DEVICESSHYAM SASIDHARAN

FEATURING…• Background and Rationale.
• Anatomy and physiology of LAA.
• Current status- various devices.
• WATCHMAN/AMPLATZER CARDIAC PLUG/LARIAT.
• Major Trials/Recommendations.

BACKGROUND


CHALLENGES IN AF TREATMENT

MAJOR BLEEDING RATES
EuroIntervention 2014;10:497-504
Left atrial appendage closure for stroke prevention in non-valvular atrial fibrillation: rationale,
devices in clinical development and insights into implantation techniques

Rationale of LAA closure • Stroke risk closely related to bleeding risk.
• In non-valvular AF, over 90 % of stroke-causing clots formed in LA from LAA.
• Given the important role played by LAA in the pathogenesis of embolic stroke, early attempts to reduce the risk by surgical removal or more recently ligation during the cardiac surgery were made.
• Data on surgical LAA closure showed that such procedure is feasible and safe . LAAOS (Left Atrial Appendage Occlusion Study)
• LIMITATIONS : need for major surgical procedure and a high rate of incomplete occlusion of the LAA orifice which might contribute to a high residual risk of stroke.
• Because of this a less invasive approach of percutaneous LAA closure was translated from animal models into the clinical setting and a growing body of evidence has shown its safety and feasibility.

ANATOMY OF LAA

ANATOMY OF LAA…

Distribution of number of lobes (1 to 4) of left atrial appendage
Fifty-four percent of LAAs had two lobes, and the number ranged between one and four lobes . There were no age or sex differencesVeinot J et al. Circulation
1997;96:3112-3115

4 MORPHOLOGICAL TYPESCACTUS CHICKEN WING
BROCCOLI WINDSOCK

PHYSIOLOGY AND PATHOLOGY IN AF
• LAA cardiocytes have high concentrations of ANP but < RAA.
• LAA function measured by means of echocardiographic Emptying fraction,peaksystolic strain and flow velocity.
• In AF ,LAA undergoes remodelling,sizeincreases – endocardial elastosis – depress LAA function.

PREDICTORS OF THROMBOEMBOLISM
• Risk is 6 times higher in non-chicken wing LAA compared to chicken wing type.
• Increase in chamber dimensions and LAA volume.
• Smaller ostial size
• Shorter LAA length.
• LAA dysfunction- peak systolic strain<21%
Emptying fraction <21%
LAA velocity<20cm/s

DEVICES
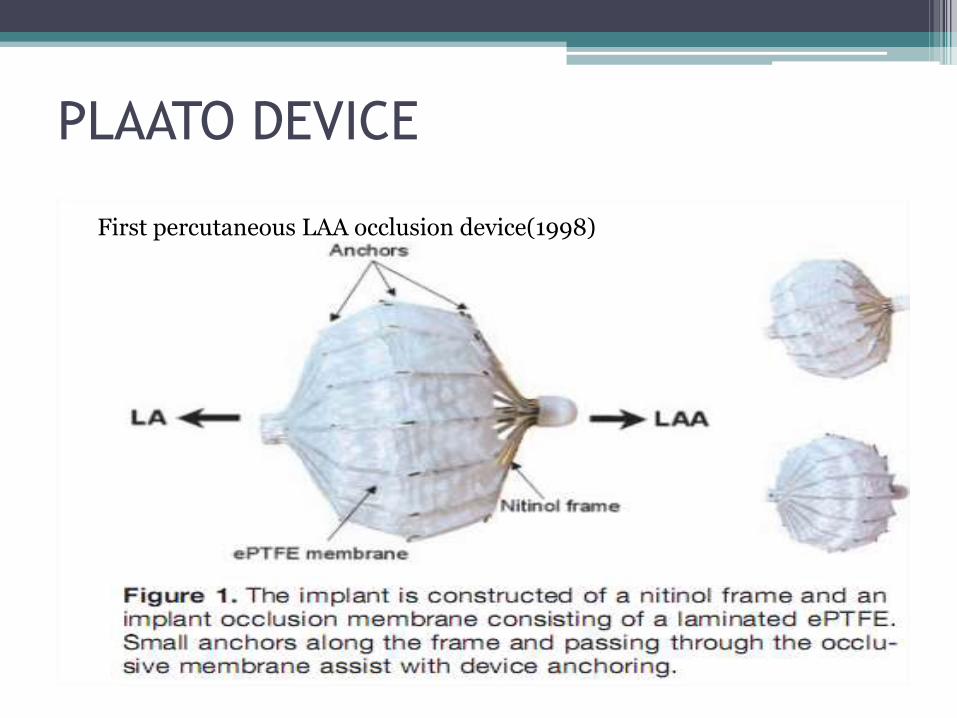
PLAATO DEVICE
First percutaneous LAA occlusion device(1998)

• The PLAATO system (Appriva Medical), consists of an implant and a delivery catheter.
• The implant ( is a self-expanding nitinol cage (range of from 15 to 32 mm) covered with an occlusive expanded polytetrafluoroethylene (ePTFE) membrane,which is laminated directly to the frame structure so that the perimeter has intimate contact with the inner wall of the appendage.
• The purpose of the membrane is both to occlude the orifice of the LAA and to allow tissue incorporation into the device.
• Small anchors along the struts and passing through the occlusivemembrane assist with device anchoring and encourage healing response.
• The device is delivered through a custom 14 Fr transseptalsheath curved to point at the LAA

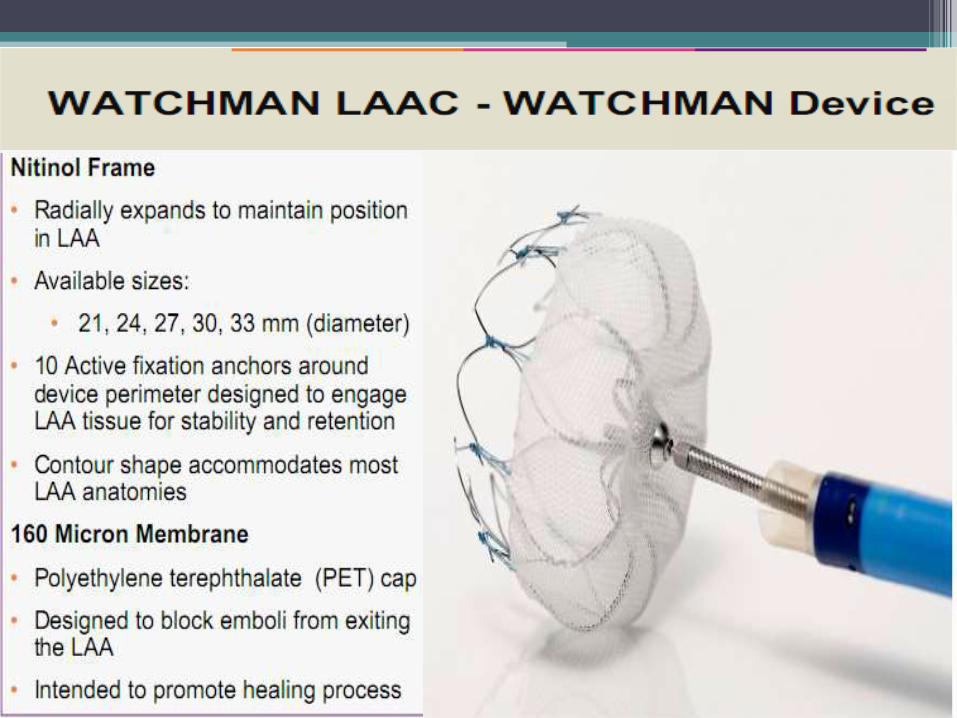
WATCHMAN LAAC
DEVICE
• Developed by Atritech medical in 2003.• Largest published clinical data to date.• PROTECT AF - seminal trial proving both the
efficacy of the device and concept of LAA closure.
• CE mark in 2005.• CAP registry (2010) and PREVAIL trial• ASAP and EVOLVE trials.• FDA approval for warfarin eligible patients
pending.

PROCEDURE
• Selecting appropriate size, according to TEE guided measurement of ostial diameter.(0 & 135)
• GA/Consciuos sedation- fluoroscopic and TEE.
• Trans septal puncture and introduction of Access sheath.
• Access into LAA with a pigtail catheter.
• Device loading of Access sheath.
• Device deployment and release.

DEVICE RELEASE CRITERIA
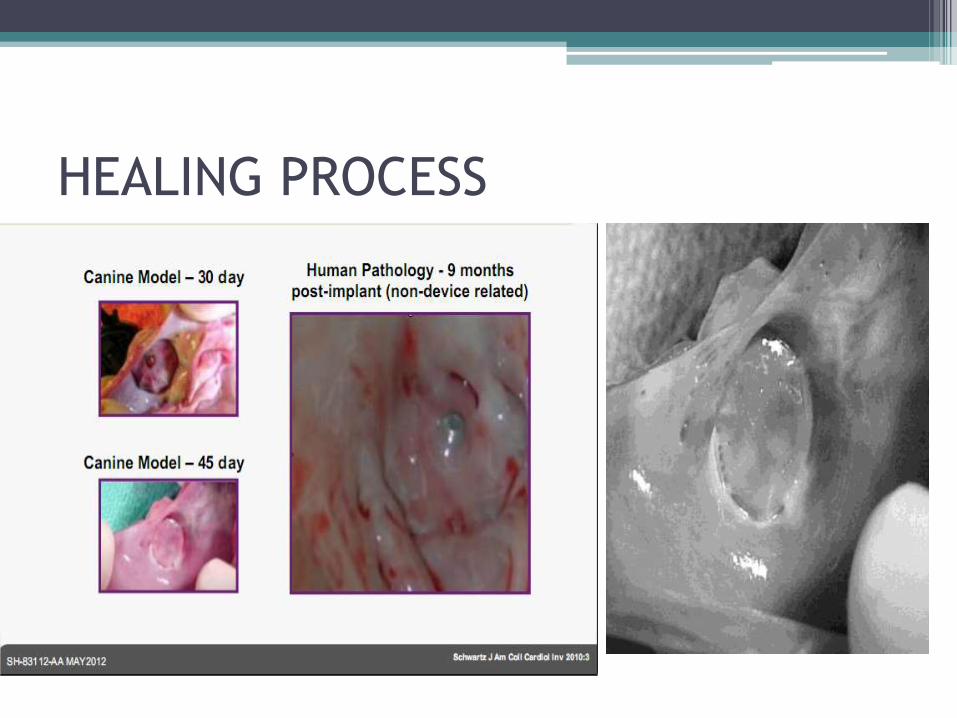
HEALING PROCESS

WATCHMAN - COMPLICATIONS
• Pericardial effusion – 4.8%
• Air embolism – 1.1%
• Cardiac perforation – 1.6%
• Device embolisation – 0.6%


AMPLATZER CARDIAC PLUG• Amplatzer Cardiac Plug is a self-
expanding device made from nitinol& dacron consisting of 3 parts namely lobe, disk, & the middle segment.
• 1ST human experience with this device was published by Park et al in 2010 in Europe
• LAA closure in 132 of 137 (96.4 %) pts,& development of serious complications (ischemic stroke in 3, device embolization in 2, and clinically significant PE in 5 cases) in 10 (7.3 %) pts was reported
• Doesnot require anticoagulation.

COHEREX WAVECREST LAA OCCLUDER
• Made of e-PTFE
• Anchored with 20 microtinesdistributed circumferentially at the distal device margin.
• Ideal for shallow LAA
• WAVECREST I trial
• CE approval in 2013.
• US pivotal WAVECREST II trial started in 2014.

LARIAT DEVICE
• Endo-epicardial procedure
• Pericardial and transseptalaccess.
• Placement of 2 magnet tipped guidewires
• Connection of epicardial and endocardial guidewires.
• Snare capture of the LAA and release of the pretied suture for LAA ligation.
• Serious pericardial effusion and major bleeding.


EMERGING TECHNOL0GIES
• OCCLUTECH LAA OCCLUDER
• LIFETECH LAA OCCLUDER : Lambre
• CARDIA ULTRASEPT LAA OCCLUDER
• AEGIS –ECG guided LAA capture and ligation system
• EPITEK- Fibreoptic endoscope mediated.


ACC/AHA/HRS 2014 AF GUIDELINES
• Class IIb - Surgical excision of the LAA may be considered in patients undergoing cardiac surgery. (Level of Evidence: C)
• WATCHMAN device and ACP device may be used in patients with high risk of stroke and contraindiactions for OACs.

TAKE HOME MESSAGE
• Device occlusion of LAA – impressive results.
• Currently recommended only for those patients with high risk for stroke and contraindications for OACs
• Further improvement expected with operator experience and newer generation devices.
• Likely to be approved for use in warfarin eligible patients in near future.

Thank you…