l-carnitine : effect on morbidities and risk factors important to patients on dialysis brian...
TRANSCRIPT

L-Carnitine : Effect on L-Carnitine : Effect on Morbidities and Risk Morbidities and Risk Factors Important to Factors Important to Patients on DialysisPatients on Dialysis
Brian Schreiber,M.D.Brian Schreiber,M.D.Assistant Clinical Professor, Department of Assistant Clinical Professor, Department of
Medicine,Medicine,Division of NephrologyDivision of Nephrology
Medical College of Wisconsin, Milwaukee, Medical College of Wisconsin, Milwaukee, WisconsinWisconsin

Effect of CHF on SurvivalEffect of CHF on Survivalin Dialysis in Dialysis
Harnett 1995Harnett 1995
Time (Months)Time (Months)
00 1212 2424 3636 4848 6060
Cu
mu
lati
ve S
urv
ival
Cu
mu
lati
ve S
urv
ival
00
0.20.2
0.40.4
0.60.6
0.80.8
1.01.0
No CHFNo CHF
CHFCHF
7272

Five Year Survival Five Year Survival RatesRates
H.D with C.H.FH.D with C.H.F 15% 15% Stage IIIA nsc lung CaStage IIIA nsc lung Ca 15% 15% COPD, FEV-1 20-30%COPD, FEV-1 20-30% 30% 30% Stage IIA nsc lung Ca Stage IIA nsc lung Ca 39% 39% Dukes C2 colon CaDukes C2 colon Ca 48% 48%
Mean survival metastatic breast cancer is 18 to Mean survival metastatic breast cancer is 18 to 24 months. H.D. with CHF mean survival is 32 24 months. H.D. with CHF mean survival is 32 months.months.
OutlineOutline
Cardiac Substrate Utilization in Cardiac Substrate Utilization in normal and pathological disease normal and pathological disease statesstates
Effect of Carnitine on Cardiac Effect of Carnitine on Cardiac Substrate UtilizationSubstrate Utilization
Carnitine in Ischemia and CHF non-Carnitine in Ischemia and CHF non-dialysisdialysis
Carnitine and CHF and LVH in Carnitine and CHF and LVH in Dialysis patientsDialysis patients

Cardiac Substrate Preference and Effect of Carnitine
Preferred Cardiac Preferred Cardiac SubstrateSubstrate
GlucoseGlucose IntrauterineIntrauterine Left Ventricular Left Ventricular
HypertrophyHypertrophy Compensated Compensated
CardiomyopathyCardiomyopathy Pre-dialysis Renal Pre-dialysis Renal
InsufficientcyInsufficientcy
Fatty AcidsFatty Acids extrauterine normalsextrauterine normals Insulin resistant Insulin resistant
cardiomyopathycardiomyopathy Decompensated Decompensated
cardiomyopathycardiomyopathy DialysisDialysis
Insulin Resistant Insulin Resistant CardiomyopathyCardiomyopathy


Insulin Resistance Insulin Resistance Independently Predicts Independently Predicts
CardiomyopathyCardiomyopathy
Ingelsson E 2005

Insulin resistance Insulin resistance predicts Cardiac events predicts Cardiac events
in HD Patientsin HD Patients
Takaneka 2007Homa IR > 1.6;69% diabetic HD pts
27% non-diabetic HD pts

Enhanced Cardiac Glucose Enhanced Cardiac Glucose Metabolism As compensation Metabolism As compensation
for Ischemiafor Ischemia

Mechanisms For Diabetic Mechanisms For Diabetic CardiomyopathyCardiomyopathy
Boudina S. 2007

Deleterious Effects of Excess Long Deleterious Effects of Excess Long Chain Acyl-CoA on Cardiac Chain Acyl-CoA on Cardiac
MyocytesMyocytes
1)Mitochondrial Permeability Defects
2)Increase Protein Kinase C Beta activity
3)Decreased calcium re-uptake into sarcolemma
4)Decreased glut 4 receptor activity-insulin resistance

Carnitine: Metabolic FunctionsCarnitine: Metabolic Functions CYTOSOL
MITOCHONDRIAL MATRIX
Fatty Acids
Fatty ACYL Coa
Carnitine CPT-1
Fatty ACYL Carnitine
Fatty ACYL Carnitine
Carnitine
CarnitineFatty ACYL
Coa
ACETYL Coa
CAT
CAT
CPT II
PYRUVATEGLUCOSE
CAT
Carnitine
PDH
Acetylcarnitine Acetylcarnitine
β-oxidation
CO2
Carnitine
Citric Acid Cycle
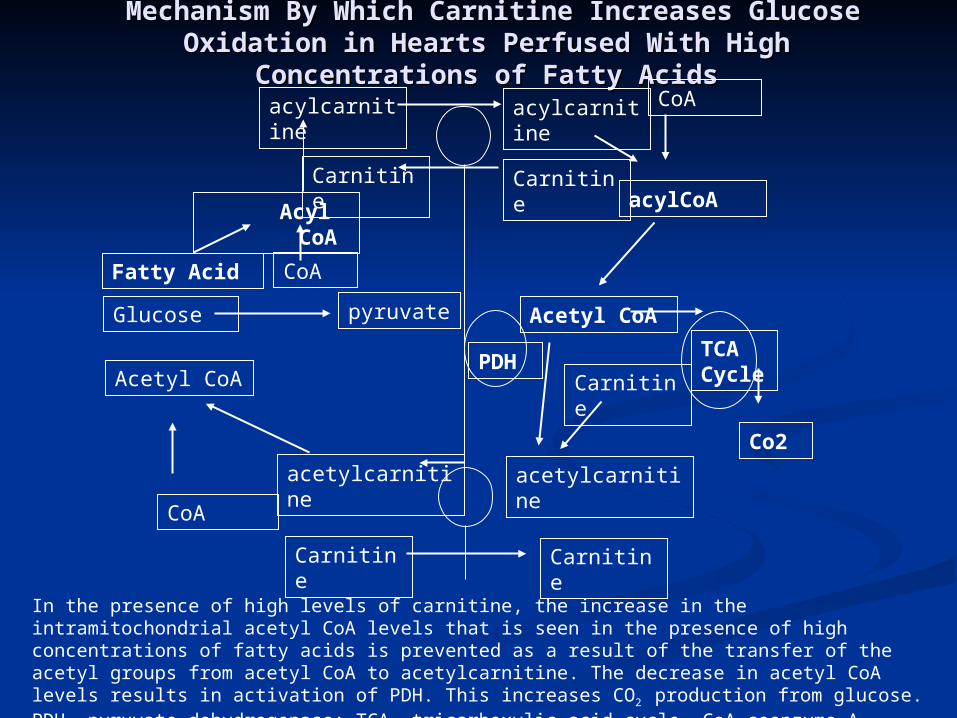
Mechanism By Which Carnitine Increases Glucose Mechanism By Which Carnitine Increases Glucose Oxidation in Hearts Perfused With High Oxidation in Hearts Perfused With High
Concentrations of Fatty AcidsConcentrations of Fatty Acids
acylCoA
acylcarnitine
CoA
TCACycle
CarnitineCarnitine
acylcarnitine
Acetyl CoA
Carnitine
acetylcarnitineacetylcarnitine
Carnitine Carnitine
PDH
pyruvateGlucose
CoAFatty Acid
AcylCoA
CoA
Acetyl CoA
Co2
In the presence of high levels of carnitine, the increase in the intramitochondrial acetyl CoA levels that is seen in the presence of high concentrations of fatty acids is prevented as a result of the transfer of the acetyl groups from acetyl CoA to acetylcarnitine. The decrease in acetyl CoA levels results in activation of PDH. This increases CO2 production from glucose. PDH, pyruvate dehydrogenase: TCA, tricarboxylic acid cycle, CoA coenzyme A.
Sauer 2008
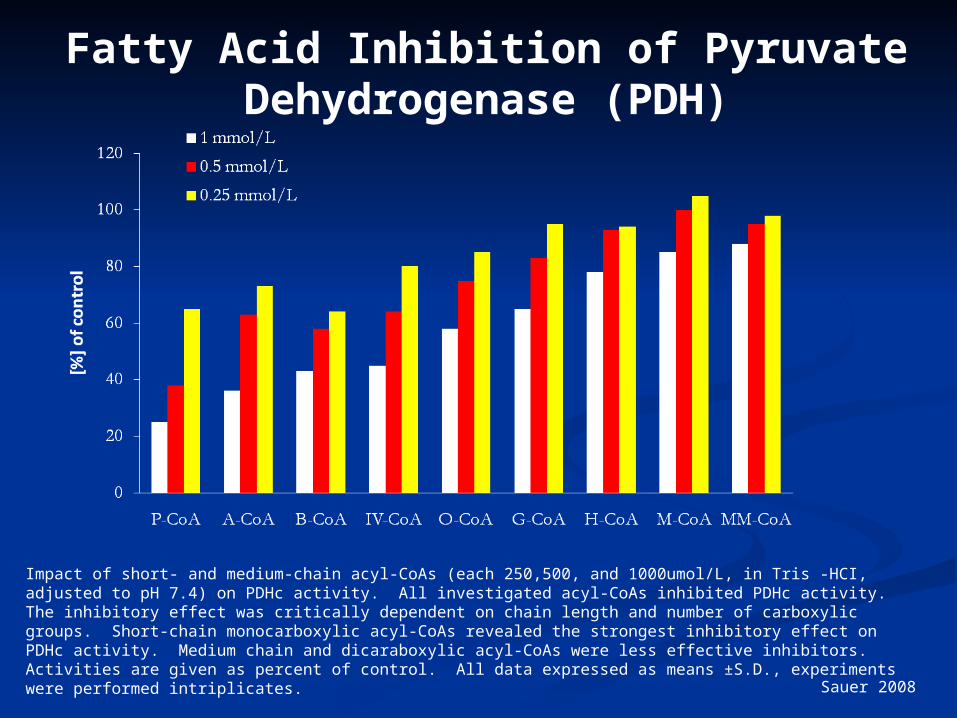
Impact of short- and medium-chain acyl-CoAs (each 250,500, and 1000umol/L, in Tris -HCI, adjusted to pH 7.4) on PDHc activity. All investigated acyl-CoAs inhibited PDHc activity. The inhibitory effect was critically dependent on chain length and number of carboxylic groups. Short-chain monocarboxylic acyl-CoAs revealed the strongest inhibitory effect on PDHc activity. Medium chain and dicaraboxylic acyl-CoAs were less effective inhibitors. Activities are given as percent of control. All data expressed as means ±S.D., experiments were performed intriplicates.
Fatty Acid Inhibition of Pyruvate Dehydrogenase (PDH)

Ischemia Effects on Acyl-Ischemia Effects on Acyl-CoACoA
Long-chain CoA
0
5
10
15
20
25
Cyto Mito
nm
ol/
g
Cellular distribution of CoA in the heart. All values are expressed as nmol of wet tissue, and represented as mean ± SEM (n=8). *P<0.01 vs no ischemia. Cyto, cytosolic compartment; Mito, mitochondrial compartment.
Kobayashi A, Fujisawa S. J Mol Cell Cardiol. 1994;26:499-508.
*
*
* *
*

Carnitine EffectCarnitine Effect
*P<0.01 vs nontreated group (control).Effect of L-carnitine on the cellular distribution of CoA esters in the ischemic heart.All values represent mean ± SEM (n=8).Homo, homogenate (cytosol + mitochondria); Cyto, cytosolic compartment; Mito, mitochondrial compartment.
Kobayashi A, Fujisawa S. J Mol Cell Cardiol. 1994;26:499-508.
Control 30 mg/kg carnitine
100 mg/kg carnitine
*
*
* *
*
* *
*
*
*
**
**
*
Carnitine and Cardiac Substrate Metabolism

Figure 2 Effect of L-carnitine on glucose oxidation rates in control and diabetic rat heart Figure 2 Effect of L-carnitine on glucose oxidation rates in control and diabetic rat heart hearts before and after ischaemia. Values are the means of 7 untreated control, 8 L-hearts before and after ischaemia. Values are the means of 7 untreated control, 8 L-carnitine treated control, 8 untreated diabetic and 8 L-carnitine treated diabetic rat hearts. carnitine treated control, 8 untreated diabetic and 8 L-carnitine treated diabetic rat hearts. Error bars = SEM. Glucose oxidation rates were determined as described in Methods.Error bars = SEM. Glucose oxidation rates were determined as described in Methods. *P <0.05 v L-carnitine treated hearts. *P <0.05 v L-carnitine treated hearts. Broderick 1995
Aerobic Reperfusion following ischaemia
L-Carnitine and Glucose Oxidation in Ischemia-Reperfusion

Lupaschuk 1994
Effects of L-carnitine on Glycolysis & Effects of L-carnitine on Glycolysis & Glucose Oxidation in Isolated Glucose Oxidation in Isolated
Working Hearts Perfused with Fatty Working Hearts Perfused with Fatty AcidsAcids
Perfusion
Conditions
Glycolysis (nmol 3H- glucose/g dry
wt- min)
Glucose Oxidation (nmol 14C-
glucose/g dry wt- min)
No addition (n=9) 291 0.23 158.4 21.4
Carnitine loaded 4.63 0.46* 454.1 85.3*
* Significantly different from those in hearts perfused in the absence of fat
Data are the mean S.E.M. of a number of hearts indicated in brackets. Carnitine-loaded hearts were pre-perfused in the working mode for 1 hour with 10 mM carnitine. Glycolysis and glucose oxidation was measured by perfusing hearts with 11 mM (2-3H/U-14C) glucose and 1.2 mM palmitate. Glycolytic rates were determined by measuring ¼ CO2 production.
Lopashuk 1992

Carnitine and Cardiac Disease: Non-dialysis

Selected Studies of Carnitine Selected Studies of Carnitine Treatment in Ischemic Heart Treatment in Ischemic Heart
Disease in HumansDisease in Humans
Author # Patients Results
Bohles et al, 1987 40 undergoing coronary artery bypass graft surgery
Pre CABG administration, increased, myocardial ATP decreased lactateand decrease inotropic medication requirement in post operative period
Iliceto et al, 1995Double-blind placebo controlled
472 with acute MI Decreased LV dilatation and decrease death from CHF in carnitine group
Cacciatore et al, 1991Randomized
200 with stable angina
Increased exercise capacity
Rizzon et al, 1989Double-blind placebo controlled
56 with acute MI Significant reduction in ventricular arrhythmias in carnitine treated group

Singh 1996Singh 1996
Randomized, double blind, placebo Randomized, double blind, placebo controlled trial lasting 28 dayscontrolled trial lasting 28 days
101 total patients: 51 carnitine, 50 101 total patients: 51 carnitine, 50 controlscontrols
Inclusion Criteria:Inclusion Criteria:Likely myocardial infarction within 24 hoursLikely myocardial infarction within 24 hours
Patients unable to give consent or with Patients unable to give consent or with symptoms of MI longer than 24 hours were symptoms of MI longer than 24 hours were
excludedexcluded

InterventionIntervention
Treatment group: L-carnitine 660 mg Treatment group: L-carnitine 660 mg PO TIDPO TID
Placebo group: aluminum hydroxide Placebo group: aluminum hydroxide 100 mg PO TID100 mg PO TID
Nitrates and aspirin used in 94% of Nitrates and aspirin used in 94% of carnitine and 100% of placebo patientscarnitine and 100% of placebo patients
Similar use of beta blocker and calcium Similar use of beta blocker and calcium blocker in both groups(40-50%)blocker in both groups(40-50%)
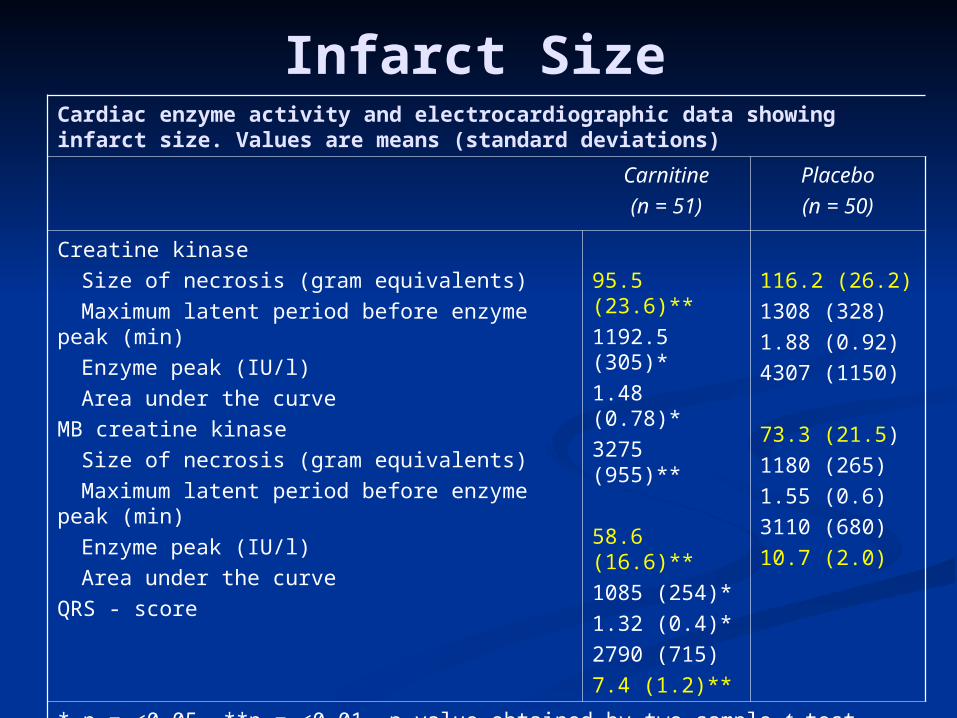
Infarct SizeCardiac enzyme activity and electrocardiographic data showing infarct size. Values are means (standard deviations)
Carnitine
(n = 51)
Placebo
(n = 50)
Creatine kinase
Size of necrosis (gram equivalents)
Maximum latent period before enzyme peak (min)
Enzyme peak (IU/l)
Area under the curve
MB creatine kinase
Size of necrosis (gram equivalents)
Maximum latent period before enzyme peak (min)
Enzyme peak (IU/l)
Area under the curve
QRS - score
95.5 (23.6)**
1192.5 (305)*
1.48 (0.78)*
3275 (955)**
58.6 (16.6)**
1085 (254)*
1.32 (0.4)*
2790 (715)
7.4 (1.2)**
116.2 (26.2)
1308 (328)
1.88 (0.92)
4307 (1150)
73.3 (21.5)
1180 (265)
1.55 (0.6)
3110 (680)
10.7 (2.0)
* p = <0.05, **p = <0.01. p-value obtained by two-sample t-test comparing carnitine and placebo groups.
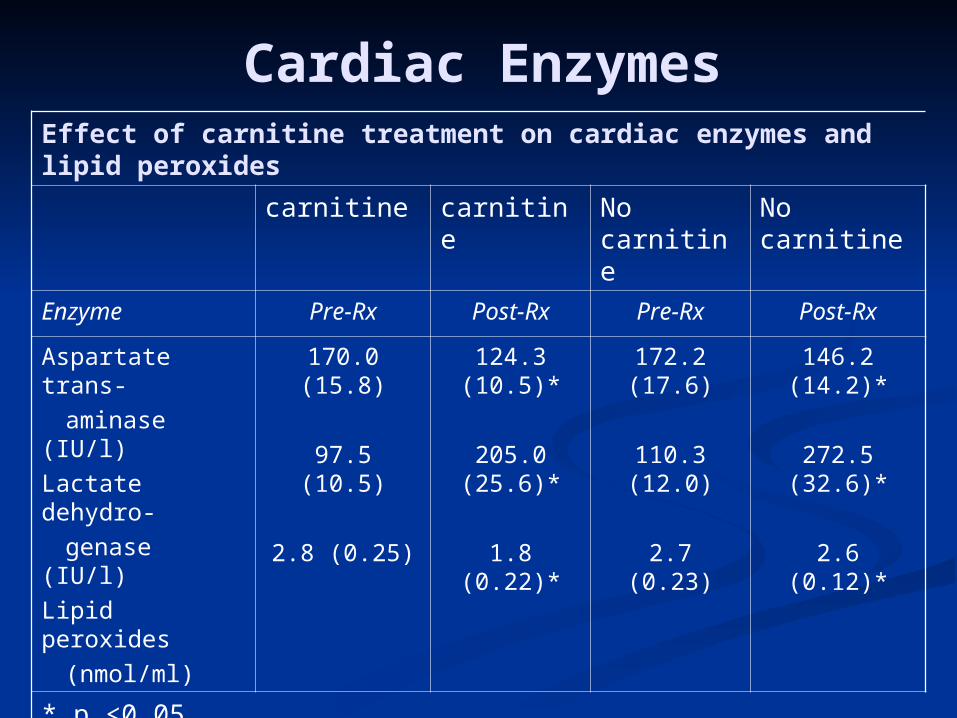
Cardiac EnzymesEffect of carnitine treatment on cardiac enzymes and lipid peroxides
carnitine carnitine No carnitine
No carnitine
Enzyme Pre-Rx Post-Rx Pre-Rx Post-Rx
Aspartate trans-
aminase (IU/l)
Lactate dehydro-
genase (IU/l)
Lipid peroxides
(nmol/ml)
170.0 (15.8)
97.5 (10.5)
2.8 (0.25)
124.3 (10.5)*
205.0 (25.6)*
1.8 (0.22)*
172.2 (17.6)
110.3 (12.0)
2.7 (0.23)
146.2 (14.2)*
272.5 (32.6)*
2.6 (0.12)*
* p <0.05

ComplicationsComplications at 28 days of follow-up. Values are numbers (percentages)
Complications
Carnitine(n = 51)
Placebo(n = 50)
Relative risk(95) CL)
Angina pectoris
NYHA Class III and IVheart failure
Left ventricular enlargement
Total cases with poor leftventricular function
Ventricular ectopics (>8/min)
Ventricular ectopics(>3 consecutively)
Total arrhythmias
Hypotension (systolic <90 mmHg)
Cardiac end points:total cardiac deaths
nonfatal reinfarction
total cardiac events
9 (17.6)*
4 (7.8)
8 (15.6)
12 (23.4)*
6 (11.7)
1 (1.9)
7 (13.7)*
1 (1.9)
4 (7.8)
4 (7.8)*
8 (15.6)*
18 (36.0)
7 (14.0)
11 (22.0)
18 (36.0)
11 (22.0)
3 (6.0)
14 (28.0)
3 (6.0)
6 (12.0)
7 (14.0)
13 (26.0)
0.49(0.98, 0.24)0.56(1.86, 0.17)0.71(1.61, 0.31)0.65(1.24, 0.35)0.54(1.32, 0.24)0.31(2.79, 0.03)0.491.11, 0.21)0.31(2.79, 0.03)
0.65(1.88, 0.22)0.56(1.86, 0.17)0.60(1.62, 0.27)
* p = <0.05; p-value significant by Z score test for proportions by comparison of carnitine group with placebo. CL = confidence limits; NYHA = New York Heart Association.

Levocarnitine Treatment in Levocarnitine Treatment in CHF in Humans-NondialysisCHF in Humans-Nondialysis
Author Patients Results
Ferrari, et al double blind, randomized placebo controlled
574NYHA Class II-III
EF<40%
Carnitine group: exercise tolerance improved, non-improvement in mortality or hospital admission
Kobayashi, et al intent to treat analysis
40Improvement to lower NYHA class, in 55% of patients receiving carnitine
Rizos, et al, 2000double blind, randomized placebo controlled
80NYHA Class III-IV
Carnitine group had lower mortality rate (P<0.04). Statistically significant improvement in VO2 Max, Weber Class, cardiac output and lower rate of arrhythmias

Carnitine & Muscle Apoptosis in CHF
0
50
100
150
200
250O
D 4
05 n
m (
% o
f co
ntr
ol)
*
*#
#
*P < 0.01; #P < 0.05 Vescovo 2002

Carnitine and Cardiac Disease: Dialysis

Cardiac Substrate Uptake in Cardiac Substrate Uptake in Predialysis CKD,Normal Predialysis CKD,Normal
Patients, and CHFPatients, and CHF
Mean Myocardial Glucose UptakeNormal=27.6 µmol/min/100gCKD Non-dialysis=68.9µmol/min/100gDilated Cardiomyopathy=12.3µmol/min/1006
Fink 2010

Increased NEFA in Hemodialysis Increased NEFA in Hemodialysis
PatientsPatients
0
250
500
750
1000
1250
[NE
FA
] (µ
mo
l.L -
1)
healthy control CKD, non-dialysis
PD HD prior to treatment
HD post treatment
Gillett M Saudi Med J 2004 25(11)1611-1616

Fatty acid oxidation control = 1487 ± 267 dpm/mg
Fatty acid oxidation hemodialysis patients = 638 ± 285 dpm/mg (p < 0.003 control vs HD)
(Savica 1983)
Abnormality of Skeletal Abnormality of Skeletal Fatty Acid Metabolism in Fatty Acid Metabolism in
DialysisDialysis

Myocardial Fatty Acid Metabolism in Myocardial Fatty Acid Metabolism in Uremic Patients Measured With BMIPP Uremic Patients Measured With BMIPP
ScintigraphyScintigraphy H/M Ratio WOR %H/M Ratio WOR %
Chronic HD-Carn 1.91+/-.19 * 17.%+/-Chronic HD-Carn 1.91+/-.19 * 17.%+/-6.0 *6.0 *
Chronic HD+carn 1.89+/-2.0 * 21.9+/-6.6 Chronic HD+carn 1.89+/-2.0 * 21.9+/-6.6 ** **
Non HD control 1.52+/-.24 22.8+/-4.2Non HD control 1.52+/-.24 22.8+/-4.2
* p<.05 vs.non HD **p<.001 vs.-Carn* p<.05 vs.non HD **p<.001 vs.-Carn
Sakurabayashi Am J Nephrol 1999:19:480-484

20
25
30
35
40
45
50
55
60
0 0.2 0.4 0.6 0.8 1
Time on dialysis (yr)
Pla
sma C
on
c (
nm
ol/
ml)
normal range
L-carnitine Plasma Concentrations in ESRD patients During the First Year of Dialysis Treatment
Evans AM, et al. Kidney Int. 2004;66:1527-1534.

Decreased Plasma Free Decreased Plasma Free CarnitineCarnitine
Levels in Hemodialysis Levels in Hemodialysis PatientsPatients Value prior to Hemodialysis Value prior to Hemodialysis
(maximum value for HD patients)(maximum value for HD patients)
19.2 ± 6.5 μmol/liter 19.2 ± 6.5 μmol/liter (Sakurabayashi 1999)(Sakurabayashi 1999) (a/f=.87)(a/f=.87) 24.8 ± 7.9 μmol/liter 24.8 ± 7.9 μmol/liter (Suzuki 1982)(Suzuki 1982) 21.5 ± 7 μmol/liter 21.5 ± 7 μmol/liter (van Es 1992)(van Es 1992) (a/f=.98)(a/f=.98) 28 ± 6.0 μmol/liter 28 ± 6.0 μmol/liter (Bellinghieri 1983)(Bellinghieri 1983) 24.4 ± 8.524.4 ± 8.528.2 ± 6.5 μmol/liter 28.2 ± 6.5 μmol/liter (Sakurabayashi 1999)(Sakurabayashi 1999) 19.5 ± 5.6 μmol/liter 19.5 ± 5.6 μmol/liter (Evans 2000)(Evans 2000) (a/f=.77) (a/f=.77) 25.9 μmol/liter 25.9 μmol/liter (Lennon 1986)(Lennon 1986) (a/f=.96)(a/f=.96) 32.4 μmol/liter 32.4 μmol/liter (Rossle 1985)(Rossle 1985) 30.4 μmol/liter 30.4 μmol/liter (Savica 1983)(Savica 1983) (Normal control value 40 (Normal control value 40 50 μmol/liter) 50 μmol/liter) (a/f<.4)(a/f<.4)

Reason for Dialysis Related Reason for Dialysis Related Carnitine deficiencyCarnitine deficiency
70% of plasma carnitine removed with each dialysis
decreased dietary intake
decreased synthetic capacity
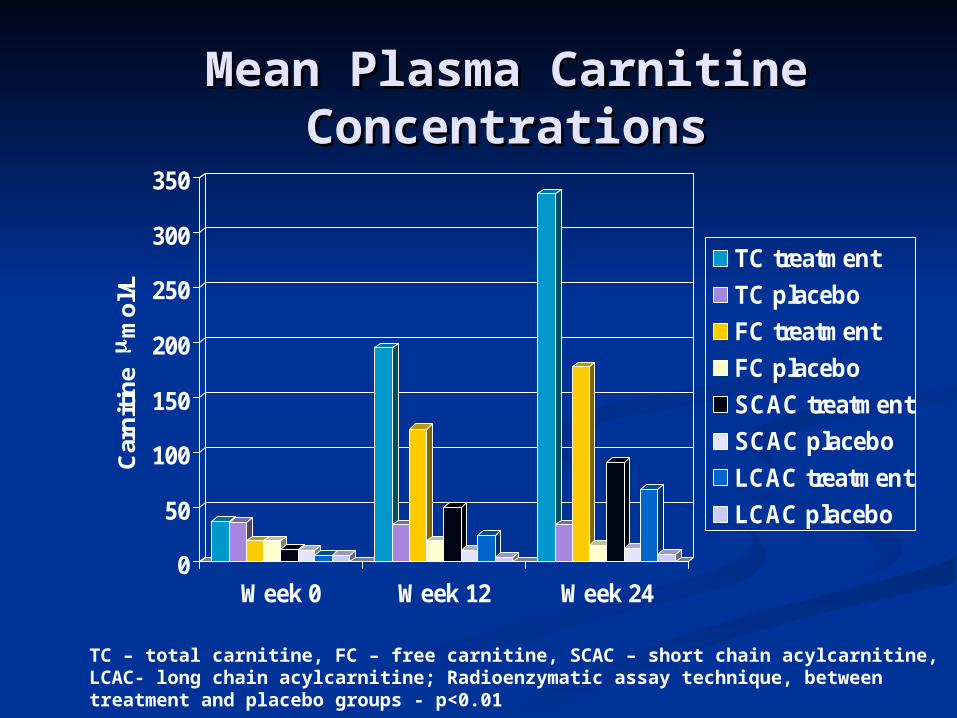
Mean Plasma Carnitine Mean Plasma Carnitine ConcentrationsConcentrations
0
50
100
150
200
250
300
350
Car
nit
ine
mm
ol/L
Week 0 Week 12 Week 24
TC treatment
TC placebo
FC treatment
FC placebo
SCAC treatment
SCAC placebo
LCAC treatment
LCAC placebo
TC – total carnitine, FC – free carnitine, SCAC – short chain acylcarnitine, LCAC- long chain acylcarnitine; Radioenzymatic assay technique, between treatment and placebo groups - p<0.01

Mean C8-C14 AcylcarnitineMean C8-C14 Acylcarnitine
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0 12 24
mm
ole
/L
C8 4methyl of C9 C10 C12 C14
Baseline to 12 weeks and baseline to 24 weeks, p<0.01Except C14 = p<0.05, n=13
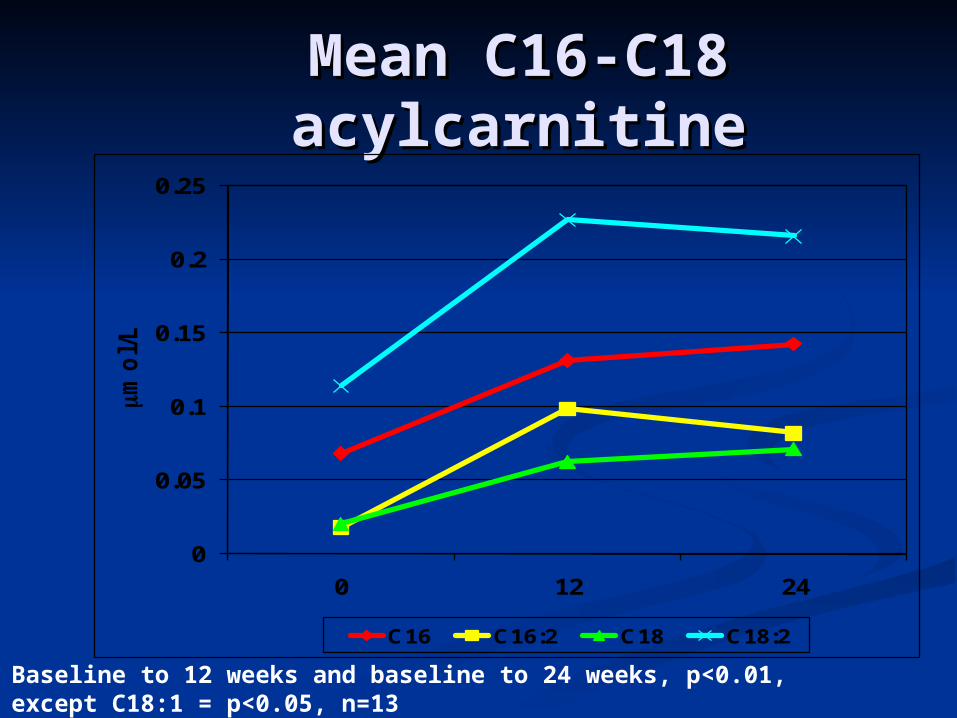
Mean C16-C18 Mean C16-C18 acylcarnitineacylcarnitine
0
0.05
0.1
0.15
0.2
0.25
0 12 24
mmo
l/L
C16 C16:2 C18 C18:2
Baseline to 12 weeks and baseline to 24 weeks, p<0.01, except C18:1 = p<0.05, n=13

Mean C16-C18 Mean C16-C18 acylcarnitineacylcarnitine
0
0.05
0.1
0.15
0.2
0.25
0 12 24
mmo
l/L
C16 C16:2 C18 C18:2
Baseline to 12 weeks and baseline to 24 weeks, p<0.01, except C18:1 = p<0.05, n=13

Changes in AcetylcarnitineChanges in Acetylcarnitine
0
10
20
30
40
50
60
70
80
Baseline 12 Weeks 24 Weeks
Acety
lcarn
itin
e (
mm
ol/L)
Baseline to 12 weeks and baseline to 24 weeks, p<0.01, n=13

Decrease in CRP in Patients with High Baseline
0
1
2
3
4
5
0 1 2 3 4 5 6
Follow-up (months)
CR
P (
mg
/dl)
Placebo Carnitine Placebo Carnitine
Savica V Journal of Renal Nutrition 2005 15(2) 225-230

L-carnitine and Markers of Free L-carnitine and Markers of Free Radical Metabolism in HDRadical Metabolism in HD
Parameter baseline 3 mos 6 mos 9 mosSOD u/g/hgb
1.044 1.034 1.043 983
GSH perox 38.4 40.8 45.8* 38.4‡GSHmmol/l 1.65 1.90* 2.23** 1.67‡Antiox cap 1.65 1.67 2.06* 1.52‡Sel mcg/l 54 38.2* 49.5 59.5MDA µmol/l 4.18 3.48* 3.07*** 2.82Tot Prot g/l 65.6 73.5* 71.8** 66.7†
Alb g/l 34.8 40.8 46.0* 43.2
Vesela 2001

Carnitine and Plasma Glucose Carnitine and Plasma Glucose Disappearance in HD Patients in HD Patients
Placebo (n=6)
L-Carnitine (n=7)
Before After P Before After P
Fasting glucose
(mmol/L)5.1 ± 0.2 4.94 ± 0.4 NS 5.19 ± 0.2 4.84 ± 0.1 NS
C-peptide (µg/L) 4.90 ± 0.9 5.01 ± 0.1 NS 5.98 ± 0.9 7.35 ± 2.3 NS
Insulin (µmol/L) 36.9 ± 7.6 38.1 ± 8.2 NS 40.60 ± 5.4 32.80 ± 4.0 NS
Kitt (%/min)* 3.30 ± .4 3.37 ± 0.4 NS 2.99 ± 0.3 3.54 ± 0.2 <0.03
Gunal A.Journal of Nephrology Vol 12 no.1 1999 38-40
*Kitt: rate constant for plasma glucose disappearance

Systolic Dysfunction Systolic Dysfunction Development of CHF Development of CHF
Harnett 1995Time (Months)
1.01.0
0.80.8
0.60.6
0.40.4
0.20.2
00
00 2424 36361212 4848 6060 7272
NormalNormal
Systolic Systolic DysfunctionDysfunction
ConcentricConcentric LVHLVH
LV DilationLV Dilation

van Es et al. 1992van Es et al. 1992
Three monthsThree months Symptomatic (n=7) Asymptomatic Symptomatic (n=7) Asymptomatic
(n=9)(n=9) 1 g levocarnitine intravenously after 1 g levocarnitine intravenously after
each dialysis sessioneach dialysis session
van Es A, et al. In Guarnieri G, Panzetta G, Toigo G (eds.): Metabolic and Nutritional Abnormalities in Kidney Disease. Contrib Nephrol. Basal, Karger 1992; 98:28-35.

FCFC(µmol(µmol
TC,TC, (µmol/l(µmol/l
CarnitineCarnitine(% free)(% free)
EF beforeEF beforeL-carnitineL-carnitine
EF after 3 mos.EF after 3 mos.of L-carnitine, of L-carnitine,
(%)(%)
SymptomaticSymptomaticpatientspatients(n=7(n=7
Effect of L-Carnitine Therapy on Effect of L-Carnitine Therapy on Left Ventricular Ejection FractionLeft Ventricular Ejection Fraction
A.van ES et al Contrib Nephrol, A.van ES et al Contrib Nephrol, 19921992

Romagnoli GF, Noso A, Carraro G, et al. Beneficial Effects of L-Carnitine in Dialysis Patients with Impaired Left Ventricular Function: an Observational Study. Curr Med Res Opin 18(3):1-4, 2002
Romagnoli et al. 2001
Changes in Left Ventricular Ejection Fraction During Carnitine Therapy
0
5
10
15
20
25
30
35
40
45
LV
EF
%
Baseline 2 Mo. 4 Mo. 6 Mo. 8 Mo.
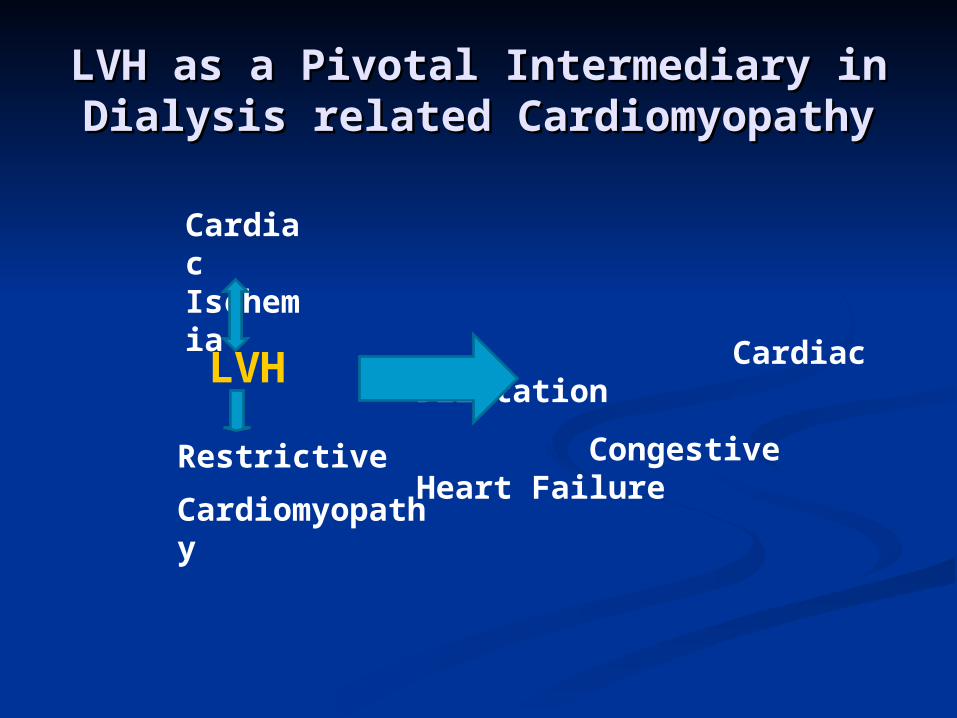
LVH as a Pivotal Intermediary in LVH as a Pivotal Intermediary in Dialysis related CardiomyopathyDialysis related Cardiomyopathy
LVH
Cardiac Ischemia
Restrictive
Cardiomyopathy
Cardiac Dilatation
Congestive Heart Failure

Change in LVH and Event Free Change in LVH and Event Free SurvivalSurvival
Zoccali C 2004

Causes of LVH in ESRD Causes of LVH in ESRD PatientsPatients
AnemiaAnemia HypertensionHypertension Volume overloadVolume overload Increased growth factor levelsIncreased growth factor levels Abnormal glucose and fatty Abnormal glucose and fatty
acid metabolismacid metabolism

Hyperinsulinemia Promotes Left Ventricular Hypertrophy
Sharma N 2007

Carnitine and LVH-Carnitine and LVH-Sakurabayashi 2008Sakurabayashi 2008
10 patients given 10mg/kg L 10 patients given 10mg/kg L carnitine 3x/week post dialysis for carnitine 3x/week post dialysis for one yearone year
10 untreated controls10 untreated controls Primary endpoints-Primary endpoints-
Echocardiographic change in indices Echocardiographic change in indices of LVHof LVH

Carnitine No Carnitine
NumberM/FAge (years)Duration of HD (years)Primary renal disease
Chronic glomerulonephritisDiabetes mellitus
AntihypertensivesCalcium antagonistsACE inhibitorsARBβ-blockers
r-HuEPO
109/1
45.7±13.712.2±4.5
91665227
109/1
46.0±7.812.5±4.2
82865216
Data are mean±SD.HD, hemodialysis; Antihypertensives, number of patients taking antihypertensive medication; ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blockers; r-HuEPO, number of patients taking recombinant human erythropoietin medication.
Carnitine and LVH-DialysisCarnitine and LVH-Dialysis
Sakurabayashi T 2008 Circ J 72:926-931

Beginning End
Carnitine No Carnitine Carnitine No Carnitine
LVEDD (cm)LVESD (cm)IVS (cm)LVPW (cm)IVS + LVPW (cm)LVFS (%)LVM (g)LVMI (g/m2)
5.03±0.653.35±0.431.04±0.171.15±0.222.19±0.3533.2±5.3
243.0±34.7151.8±21.2
5.29±0.843.39±0.721.40±0.171.05±0.152.09±0.3136.2±5.0
247.8±40.2153.3±28.2
5.00±0.373.31±0.391.00±0.111.02±0.12*2.02±0.2233.9±4.7
217.1±36.8**134.0±16.0**
5.28±0.903.38±0.801.14±0.341.08±0.172.22±0.4836.6±6.2
270.6±65.9167.1±43.1
*p<0.05, **p<0.01 within the group. Data are mean±SD.LVEDD, left ventricular end-diastolic dimension; LVESD, left ventricular end-systolic dimension; IVS, interventricular septal end-diastolic thickness; LVPW, left ventricular posterior wall end-diastolic thickness; LVFS, left ventricular fractional shortening; LVM, left ventricular mass; LVMI, left ventricular mass index.
Change in Cardiac Dimensions Change in Cardiac Dimensions and Mass with L-Carnitine in and Mass with L-Carnitine in
ESRDESRD
Sakurabayashi T 2008 Circ J 72:926-931

Carnitine and Diastolic Dysfunction in Pediatric
Hemodialysis
24 Children on chronic hemodialysis 24 Children on chronic hemodialysis treated with L-carnitine 50mg/kg treated with L-carnitine 50mg/kg orally after each hemodialysis for two orally after each hemodialysis for two monthsmonths
24 healthy children of similar age and 24 healthy children of similar age and socioeconomic status as controlssocioeconomic status as controls
Age range 8-19 yearsAge range 8-19 years Mean number of months on Mean number of months on
hemodialysis=19hemodialysis=19El-Metwally et al 2003

Carnitine and Diastolic Function ESRDCarnitine and Diastolic Function ESRD
El-Metwally 2003
Reduced E/A ratio pre-carnitine
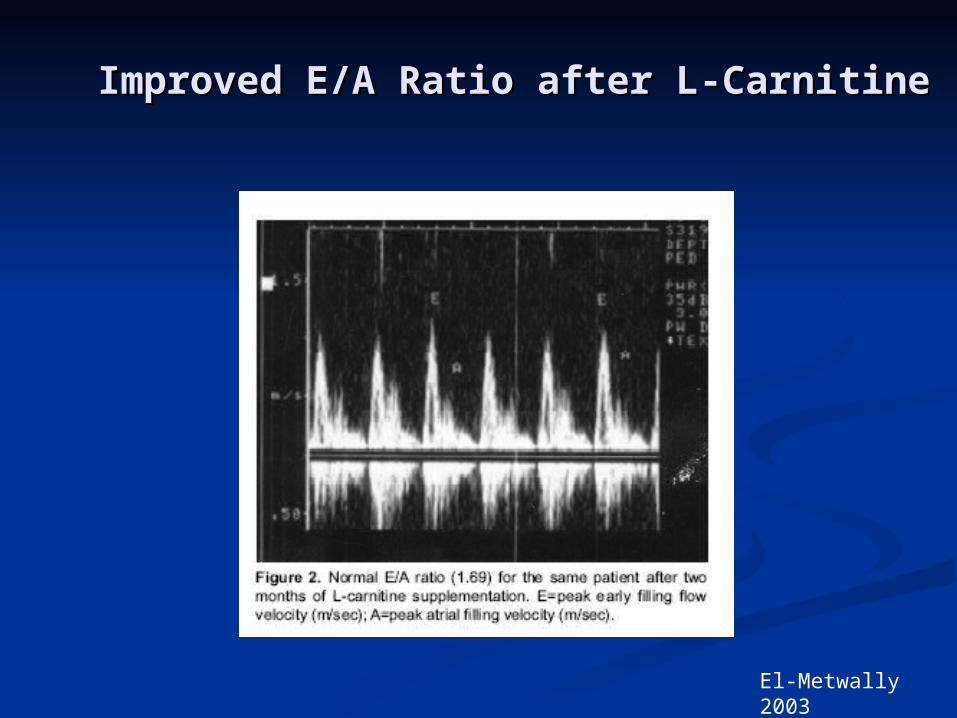
Improved E/A Ratio after L-CarnitineImproved E/A Ratio after L-Carnitine
El-Metwally 2003

Importance of Red Cell Importance of Red Cell DeformabilityDeformability
in Microcirculation in Microcirculation
Baskurt O Meiselman H (2003). Blood rheology and hemomdynamics. Seminars in Thrombosis and Hemostasis 29 (5) 435-450.

Decrease in Cerebral Blood Flow Decrease in Cerebral Blood Flow in HD Patients with Normalization in HD Patients with Normalization
of Hematocritof Hematocrit
Metry et al J Am Soc Nephrol 10:854-863 1999

Deformability of RBC In Hemodialysis Patients Before Deformability of RBC In Hemodialysis Patients Before and After the Dialysis Session, as Well as in Normal and After the Dialysis Session, as Well as in Normal
ControlsControls Before HDBefore HD
nn Before HD Before HD After HD After HD (after LC)(after LC)
1 17.99 27.92 10.4
2 15.68 16.44 14.53
3 11.90 21.25 11.02
4 15.78 24.11 14.62
5 10.08 19.29 10.03
6 11.80 22.81 11.02
7 15.78 34.67 10.00
8 12.34 19.73 11.90
9 15.27 16.33 15.44
10 19.71 20.01 10.29
11 13.19 13.49 9.50
12 20.58 22.63 10.40
13 17.77 25.65 11.76
14 13.88 25.00 6.60
15 13.12 16.71 14.70Mean ± SD 15.0 ± 3.1 21.7 ± 5.4
11.5 ± 2.4(before HO vs normal controls p < 0.00001),
(before HD vs after HD p < 0.00001),
(before HD vs before HD after 3 months LC supplementation, p < 0.004),
(before HD after 3 months LC supplementation vs normal control, p < 0.02).
Sotirakopoulos, Nikolaos
Renal Failure, 22(1), 73-80(2000)
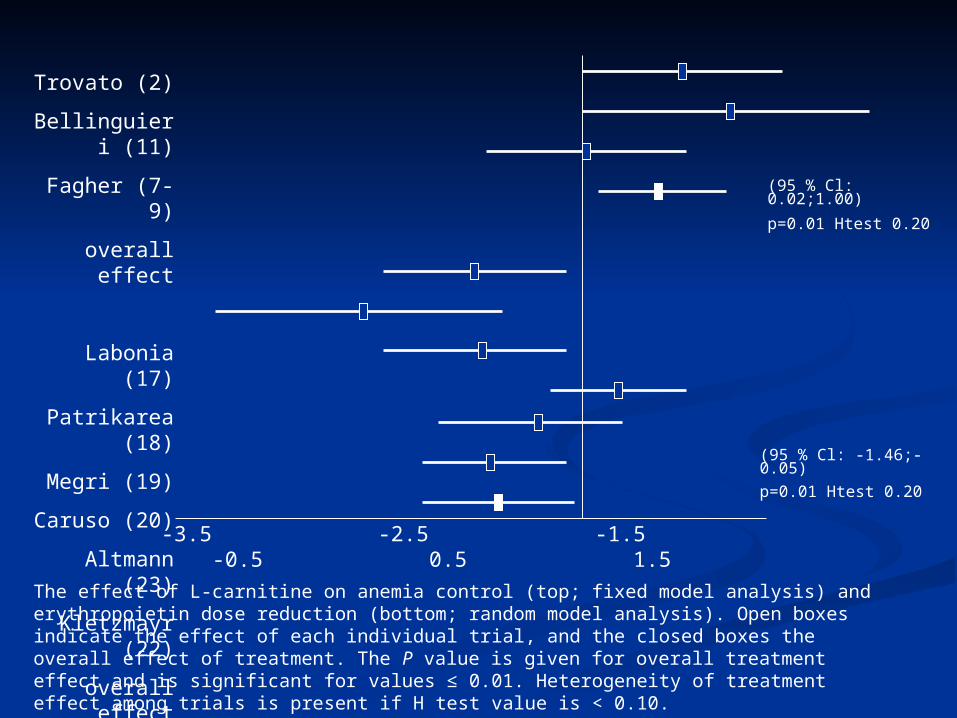
Trovato (2)
Bellinguieri (11)
Fagher (7-9)
overall effect
Labonia (17)
Patrikarea (18)
Megri (19)
Caruso (20)
Altmann (23)
Kletzmayr (22)
overall effect
-3.5 -2.5 -1.5 -0.5 0.5 1.5
The effect of L-carnitine on anemia control (top; fixed model analysis) and erythropoietin dose reduction (bottom; random model analysis). Open boxes indicate the effect of each individual trial, and the closed boxes the overall effect of treatment. The P value is given for overall treatment effect and is significant for values ≤ 0.01. Heterogeneity of treatment effect among trials is present if H test value is < 0.10.
(95 % Cl: 0.02;1.00)
p=0.01 Htest 0.20
(95 % Cl: -1.46;-0.05)
p=0.01 Htest 0.20

Decrease in Hospitalization With Levocarnitine Therapy-
Kazmi et al 2005
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
Months before and after initiation of carnitine therapy
Rel
ativ
e R
isk
of
Ho
spit
aliz
atio
n Non cardiac
Cardiac History
Kazmi WH, et al. Am J Nephrol. 2005;25:106-115.

USRDS Data 1998-2003USRDS Data 1998-2003
Weinhandl 2007

Peritoneal DialysisPeritoneal Dialysis Free carnitine level below normal but not as low Free carnitine level below normal but not as low
as hemodialysisas hemodialysis
Elevated acyl/free carnitine ratio indicative of Elevated acyl/free carnitine ratio indicative of fatty acid metabolic abnormalityfatty acid metabolic abnormality
Serum free carnitine falls as effluent volumes Serum free carnitine falls as effluent volumes and adequacy increaseand adequacy increase
Limited clinical data for improvement in muscle Limited clinical data for improvement in muscle biochemistry and EPO resistancebiochemistry and EPO resistance

Constantin –Teodosiu Constantin –Teodosiu 19961996
Plasma free carnitine concentration Plasma free carnitine concentration 28.5µmol/liter,significantly lower than 28.5µmol/liter,significantly lower than controlcontrol
Daily loss of free carnitine in CAPD Daily loss of free carnitine in CAPD significantly greater than healthy controlssignificantly greater than healthy controls
Total/free carnitine ratio greater in plasma Total/free carnitine ratio greater in plasma than controlsthan controls
““These ratio differences suggests that These ratio differences suggests that an alteration in acyl group metabolism is an alteration in acyl group metabolism is occurring in CAPD patientsoccurring in CAPD patients
Constantin-Teodosiu et al Kidney Int.1996 49 (1):158-Constantin-Teodosiu et al Kidney Int.1996 49 (1):158-162162

Sotirakopoulos 2002Sotirakopoulos 2002
12 adult patients on CAPD > 6 months12 adult patients on CAPD > 6 months 2 grams L-carnitine per os x 3 months2 grams L-carnitine per os x 3 months Hct ↑ 35.4 →38.1 (p<.03)Hct ↑ 35.4 →38.1 (p<.03) Hb ↑ 11.0 →11.9 (p<.01)Hb ↑ 11.0 →11.9 (p<.01) rHuEPO dose ↓3833 →1292+/- (p<.01)rHuEPO dose ↓3833 →1292+/- (p<.01)
● ● RBC IR(index de regidite)↓16.6→13.0 RBC IR(index de regidite)↓16.6→13.0 (p<.03)(p<.03)
Sotirakopoulos N et al Renal Failure 2002 24(4) 505-Sotirakopoulos N et al Renal Failure 2002 24(4) 505-
510510

SummarySummary Cardiac substrate metabolism is an important Cardiac substrate metabolism is an important
predictor of cardiac physiologypredictor of cardiac physiology Prior to starting dialysis,CKD patients are in a Prior to starting dialysis,CKD patients are in a
state where increased cardiac glucose metabolism state where increased cardiac glucose metabolism is a partial compensation for cardiac diseaseis a partial compensation for cardiac disease
Dialysis patients, almost always carnitine Dialysis patients, almost always carnitine deficient,have excess myocardial unmetabolized deficient,have excess myocardial unmetabolized fatty acidsfatty acids
The excess fatty acids have major harmful effects The excess fatty acids have major harmful effects on myocardial cells including inhibition of glucose on myocardial cells including inhibition of glucose metabolismmetabolism
Administration of L-carnitine to dialysis patients Administration of L-carnitine to dialysis patients has been associated with improved cardiac has been associated with improved cardiac function in CHF and a reduction of LVHfunction in CHF and a reduction of LVH