kidney inflammation and ckd-mbd regulatory molecules ... · alberto ortiz, madrid, spain ... if...
TRANSCRIPT

Kidney inflammation and CKD-MBD regulatory molecules Alberto Ortiz, Madrid, Spain
Chairs: Bengt Lindholm, Stockholm, Sweden Alberto Ortiz, Madrid, Spain
Prof. Alberto Ortiz Nephrology and Hypertension Department
Instituto de Investigación Sanitaria de la Fundación Jiménez Díaz and Universidad Autónoma de Madrid
Madrid, Spain
Slide 1
Slide 2

Good morning, I'm glad to be here to be able to discuss some of the issues we are addressing and thatwe're currently interested in in our lab relating to inflammation and CKD-MBD regulatory molecules.
Slide 3
The connection between inflammation and vascular calcification in both diseases has long been known. Infact, this paper, one of the original descriptions of calciphylaxis in 1961 already indicated that for calciphylaxisto occur you needed some sensitization agent like overdose of vitamin D or PTH. Then certain challengersand after that you got calcification followed by inflammation. So the connection between soft tissuecalcification and inflammation has long been known although the exact mechanisms are not.
Slide 4

This is the problem we face every day in our clinical practice. The vertical axis represents mortality, thehorizontal axis age and
Slide 5
we can see that for a dialysis patient aged 30 the mortality is similar to that for a general population individual

aged 35.
Slide 6
So, we have accelerated ageing in CKD patients and perhaps by exploring the mechanisms linking CKD withinflammation and CKD-MBD we can better treat our patients. So, this is our nightmare; accelerating ageing ofour patients.
Slide 7

200 years ago there was another man having nightmares this was the famous Spanish painter Francisco DeGoya. Francisco de Goya was the last of the old masters and the first of the modern.
Slide 8
At the end of his life he bought
Slide 9

a small house near the Manzanares river in Madrid and he started painting in the walls of the house. Thatwas the collection of paintings known as 'black paintings' because they were depressing paintings.
Slide 10
One of the subjects of his nightmares that he painted on the upper floor of his house
Slide 11

next to the Fight with Cudgels was
Slide 12
this representation of the Fates, the Greek goddesses. He emphasised Atropos.
Slide 13

So who were the Fates? The Fates were three great goddesses: Klotho who started to spin the thread of lifeand Atropos cut it. In his nightmares in his later years, his depressive years Goya emphasized Atropos but forus nephrologists the interest lies in Klotho.
Slide 14
Why is Klotho interesting for nephrologists? Well, this is a gene, which is mainly expressed in the kidney sothe kidney is the main site of klotho expression.
Slide 15

What do we know about klotho? In a series of papers coming from Japan, the main literature being fromMakoto Kuro-o, he showed first that klotho was a hormone like erythropoietin, a kidney-secreted hormone.Second that klotho could suppress ageing. That's the problem of our CKD patients, they have acceleratedageing. So this graph represents life span in days and cumulative survival. Normal mice can live up to 3years.
Slide 16

If they are klotho deficient, mice that are genetically klotho deficient, our CKD patients are also klotho deficientbut that's acquired klotho deficient. Mice that are genetically klotho deficient die of old age at age 3 months.Accelerated ageing, early death.
Slide 17

By contrast, when you overexpress klotho, these are the pink and blue lines,
Slide 18
you can have an expansion of life, an extension of lifespan. So, klotho is a kidney-secreted hormone, whichregulates ageing and lifespan.
Slide 19
How do these mice lacking klotho look? So they are smaller than their counterparts, they have bone disease

like kidney patients, they have loss of calcium and phosphate from the bone and where does this calciumand phosphate that are missing from the bone go? They deposit in the vascular wall. Mice deficient in klothoalso have high serum phosphate. So we have klotho, a hormone secreted by the kidney, it is lost in CKD.CKD patients have bone disease and vascular calcification and high phosphate. Mice lacking klotho havealso bone disease, vascular calcification and high phosphate. So we may learn from these mice in order tounderstand what's going on in our patients.
Slide 20
What are klotho functions? So two main groups of klotho functions have been described. First klothopromotes phosphaturia, it promotes phosphate excretion by the kidneys, both are FGF23 dependent and thishas already been commented on this morning here and also through FGF23 independent actions. Besidesthis, in addition to this phosphaturic effect, klotho has another set of effects, of actions that are thought to berelated to its glycosidase activity. Klotho has been shown to be anti-oxidant, anti-inflammatory, anti-fibrotic, sohere we're having a kidney-secreted hormone that may link inflammation with bone mineral disorders.
Slide 21

In fact, this anti-inflammatory, anti-fibrosis effects of klotho have been studied and studies so far suggest thatperhaps klotho can be used therapeutically to limit kidney injury in particular to limit kidney fibrosis. A renalpaper was published and we commented upon it last month in JASN. Therapeutic effect of klotho in kidneyinjury.
Slide 22
However, the best-known action of klotho is regulation of phosphate levels. Klotho is a receptor for FGF23 inproximal tubular cells, binding of FGF23 to klotho transduces signals that decrease calcitriol synthesis,decreases vitamin D synthesis. This is important to protect us from phosphate because when calcitrioldecreases, we absorb less phosphate from the gut. However, we should also remember that calcitriol hasvitamin D, has anti-inflammatory actions, so when we have an excess of phosphate and the organism needsto activate the FGF23 klotho low calcitriol synthesis to get rid and protect us from the excess of phosphate, wemay be impairing our anti-inflammatory defences. The second main action of klotho in these cells is toincrease phosphate excretion. It prevents tubular cells from reabsorbing, from internalising phosphate intothe lumen, in the glomerular ultrafiltrate. In addition to this action of klotho, which is membrane-based klotho

Slide 23
there are also actions of secreted klotho and these are the hormonal multi-actions that are based on itsglycosylase activity.
Slide 24

So how important are the different actions of klotho for survival? It has anti-inflammatory effects; it also has aphosphaturic effect. Ohnishi and Razzaque made a series of experiments that shed light on this. So here wehave a wild type mouse, a healthy mouse, this is a klotho deficient mouse, this is smaller, has vascularcalcification.
Slide 25

What they did is they took these klotho deficient mice and they deleted the phosphate transporter thatreabsorbs phosphate from the tubular lumen. So they made a double knockout. These mice don't haveklotho, so they should be smaller but they also have very high phosphaturia because they cannot recoverphosphate from the glomerular ultrafiltrate. When these klotho mice are made phosphaturic, they looknormal. Then they took these normal looking double knockout mice that lack klotho
Slide 26
and have phosphaturia and expose them to a very high phosphate diet. These mice lack klotho, this is adouble knockout just like the big mouse here. They excrete lots of phosphate but they eat even morephosphate, so they were made hyperphosphatemic again. Klotho knockout are hyperphosphatemic, doubleknockout are also hyperphosphatemic.
Slide 27

What happens to survival?
Slide 28
So these are the survivors that are normal mice.
Slide 29

This is the survival of klotho deficient mice. They accelerate ageing and early death. When these klothodeficient mice became hyperphosphaturic, serum phosphate was normalized
Slide 30
they lived longer like normal mice. When these same blue mice were subjected to a very high phosphatediet,
Slide 31

they developed accelerated ageing again. So the function of klotho protecting us from excess phosphate isvery important for its overall protective actions. So maybe what we should do is control serum phosphate inour patients but that may be hard to do. We have daily experience that it is hard to control serum phosphate inour patients.
Slide 32
So what is the alternative? We know and this Slide has already been shown here that with progression ofCKD there is a derangement of a series of parameters of bone mineral disorders.
Slide 33

But the earliest of them is decreased klotho. As you see here in the Slide, you have decreased klotho in stage1 CKD. What does stage 1 CKD mean? It means that GFR is normal, so why would a CKD-MBD parameterchange when GFR is normal? You can excrete all the phosphate you want,
Slide 34
why would that change? So we were thinking about this question, why when GFR is normal, klotho is already

decreased?
Slide 35
In order to try to understand it we put some pictures in front of us because sometimes that helps tounderstand things. So this is a normal kidney, it is much bigger than an ESRD kidney. A normal kidney isalso full of renal cells, glomerular cells and tubular cells. An ESRD kidney has lost many of the cells,
Slide 36

there is atrophy, there is cell death, there are no more glomerular cells, you have only fibrosis stained here inblue.
Slide 37
However, if this were a stage 1 CKD kidney, you already have some alterations what's that? Inflammation, instage 1 CKD you have normal function but there is something wrong, usually what's wrong is that you haveproteinuria and proteinuria is known to promote inflammation, the excess protein in the tubular lumen willactivate inflammation in proximal tubular cells.
Slide 38

So we tried to think, is maybe inflammation the factor driving the decrease in klotho? If that is so, could weintervene therapeutically to prevent our patients from losing their klotho in their kidneys?
Slide 39
We performed a series of experiments that I've summarized here. I would like to introduce you to NFkB. NFkBis a transcription factor, a transcription factor is a key to the genome. Transcription factors will open thegenome in order to allow it to express certain genes. Most of the genes that are targets of NFkB are known tobe involved in inflammation. So when NFkB is activated through the canonical pathway, you have this bluething here that is NFkB. It is usually inactive, kept inactive in the cytosol by IkB by inhibitory proteins. Whenthere is activation of the pathway, these inhibitory proteins will get degraded and NFkB itself will be able tomigrate to the nucleus and upregulate the expression of pro-inflammatory genes. This is how the pathwayworks.
Slide 40

So what's the relationship with klotho? We set up to study this relationship and we showed that NFkBactivation promotes klotho down regulation. How did we reach this conclusion? We performed experimentsbased on siRNA, inhibitory RNA that prevented the production of these inhibitory proteins IkB. So we got rid ofthese inhibitory proteins that activated the pathway.
Slide 41

When calcium cells inactivated NFkB pathway, independent from the stimuli just activation of the NFkBpathway the production of klotho decreased.
Slide 42

Furthermore, we activated the pathway with some inflammatory cytokines. Then in some cells in someexperiments, we prevented NFkB activation by the use of this compound, Parthenolide. Parthenolide willprotect the inhibitory proteins from degradation. The inhibitory proteins will keep NFkB in the cytosol inactiveand when we did this, in cultured cells we observed this,
Slide 43
these are normal cells, this is the normal expression of klotho, these are tubular cells, kidney cells, when weexposed the cells to inflammatory
Slide 44

cytokines such as TWEAK or TNF-α, klotho expression decreased. When we prevented NFkB activation,
Slide 45
we also prevented the loss of klotho.
Slide 46

This could also be of help in animals so these are mice, we injected them with TWEAK, with thisproinflammatory cytokine
Slide 47
and klotho expression went down at the miRNA and also at the protein level. We also treated the animalswith an inhibitor of NFkB
Slide 48
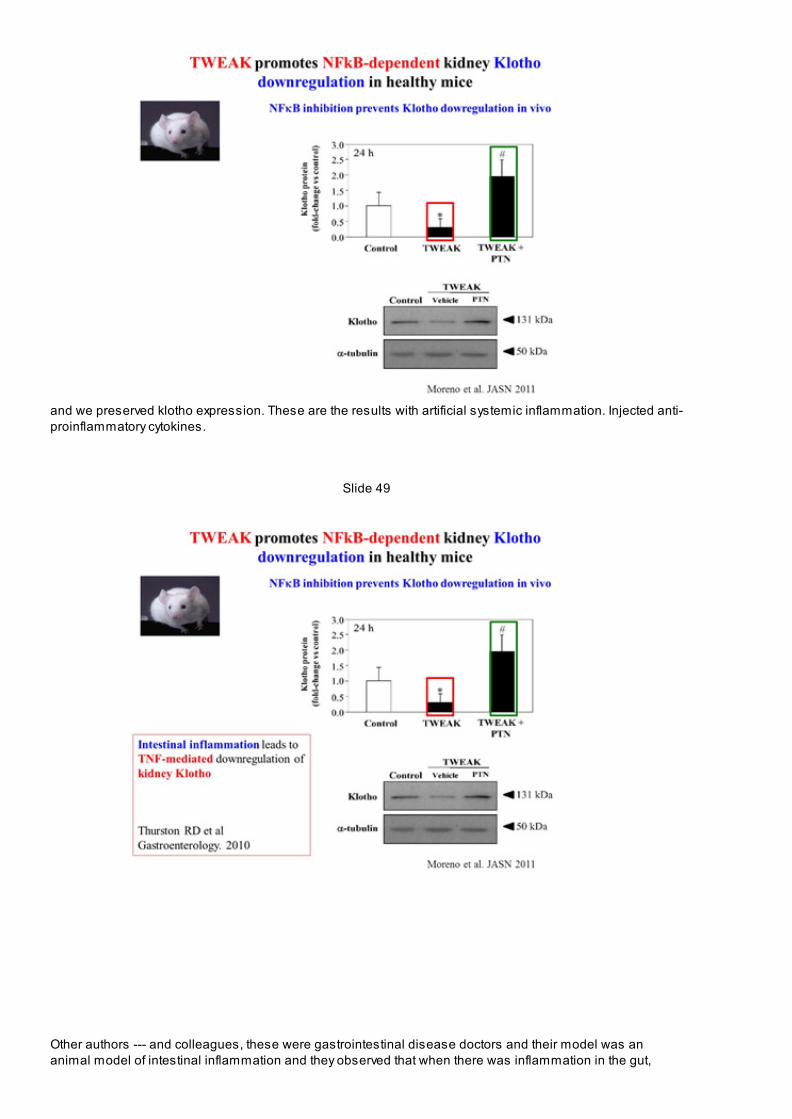
and we preserved klotho expression. These are the results with artificial systemic inflammation. Injected anti-proinflammatory cytokines.
Slide 49
Other authors --- and colleagues, these were gastrointestinal disease doctors and their model was ananimal model of intestinal inflammation and they observed that when there was inflammation in the gut,

kidney klotho went down. So systemic inflammation will be able to reduce kidney klotho and that the mediatorin this case was TNF. So systemic inflammation in the gut led to increased TNF levels and circulating TNFwould decrease kidney klotho. So there is evidence that inflammation decreases klotho and we have beentalking today about evidence that inflammation is increased in CKD patients.
Slide 50
So we have to update the function of NFkB, it will upregulate inflammatory genes but it also down regulatesklotho and that will impact both on inflammation because klotho has an anti-inflammatory effect and also onCKD-MBD.
Slide 51

Moreover, there are studies on vascular cells by Lim et al. published in Circulation a very highly regardedjournal. They observed that in healthy subjects there is klotho in the vascular wall that is lost in CKD. Whenthey tried to address why klotho is lost from the vascular wall in these patients
Slide 52
the cultured vascular smooth muscle cells in the presence of TNF inflammation again. In the vascular wallinflammation also decreases klotho expression. Vascular wall klotho expression is thought to be importantto prevent vascular calcification. There were also other stimuli that would decrease the klotho.
Slide 53

One of them was high phosphate levels. Again, the link between inflammation CKD-MBD and vascular injuryin CKD patients.
Slide 54
So we have known for a long time that inflammation is associated with accelerated ageing at least withdiseases associated with ageing and
Slide 55

we propose that inflammation will decrease in the klotho, perhaps in other organs and that either bypreventing the anti-inflammatory effect of klotho or by increasing the – phosphate may contribute to bothaccelerated ageing and further inflammation.
Slide 56

So this is the take home message I've tried to convey. There is an increasingly recognised link betweeninflammation and CKD-MBD and both professor Carrero and professor Gilmath have provided clinicalevidence for this. We don't know yet what the connection is what is the chicken and the egg as professorCarrero said. There is evidence that inflammation may favour CKD-MBD and there is also evidence of thecontrary that CKD-MBD may favour inflammation. However, we have observed that inflammation relates a keyregulator of both inflammation and CKD-MBD, which is klotho in the kidney and vessels and this, offers thepossibility for therapeutic intervention. Thank you very much for your attention.