kewei li nih public access qian wang thuy pham, and...
TRANSCRIPT

Quantification of Structural Compliance of Aged Human andPorcine Aortic Root Tissues
Kewei Li, Qian Wang, Thuy Pham, and Wei SunTissue Mechanics Laboratory Biomedical Engineering Program and Department of MechanicalEngineering University of Connecticut, Storrs, CT 06269
Abstract
The structural compliance of the aortic root has a significant implication for valve procedures such
as transcatheter aortic valve implantation and valve-sparing aortic root replacement. However, a
detailed quantification of human aortic roots structural compliance, particularly in different
regions has been incomplete. In this study, the structural properties of human aortic roots (81 ±
8.74 years, n=10) were characterized and compared with those of porcine ones (6–9 months,
n=10) using a vessel pressure-inflation test. The test involves tracking three-dimensional
deformation of the markers affixed on the different surface regions of the aortic roots, including
the three sinuses: the non-coronary sinus (NCS), the left coronary sinus (LCS) and the right
coronary sinus (RCS), and at three regions along the longitudinal direction of each sinus: the
upper sinus (US), the middle sinus (MS) and the lower sinus (LS), and the ascending aorta (AA)
region above the NCS. We found that tissue stiffness at a physiological pressure range was similar
among the three human sinuses. The regional structural stiffness of human aorta was observed. In
the circumferential direction, the LS regions were the stiffest in the LCS and RCS sinuses, while
NCS had relatively uniform stiffness. In the longitudinal direction, the human AA regions were
more compliant than all sinuses. There was a significant difference in tissue stiffness between
human and porcine aortic tissues, suggesting that the mechanical properties of porcine may not be
analogous to aged human ones.
Keywords
Heart valve mechanics; Aortic root compliance; Inflation test; Surface deformation; Direct lineartransformation
INTRODUCTION
Aortic root is defined as the portion of the left ventricular outflow tract which supports the
leaflets of the aortic valve, delineated by the sinotubular ridge superiorly and bases of the
valve leaflets inferiorly [1]. It comprises the sinuses, the aortic valve leaflets, the
commissures, and the interleaflet triangles. The sinuses are expanded portions of the aortic
root which are confined proximally by the attachments of the valve leaflets and distally by
For correspondence: Wei Sun, Ph.D. Biomedical Engineering 207 Bronwell Building University of Connecticut Storrs, CT06269-3247 Phone: (860) 486-0369 Fax: (860) 486-5088 [email protected].
NIH Public AccessAuthor ManuscriptJ Biomed Mater Res A. Author manuscript; available in PMC 2015 July 01.
Published in final edited form as:J Biomed Mater Res A. 2014 July ; 102(7): 2365–2374. doi:10.1002/jbm.a.34884.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript

the sinotubular junction. Common forms of aortic root diseases include aortic stenosis and
aortic aneurysms. Surgical and transcatheter approaches have been used to treat these
diseases with the purpose of restoring the normal function of the aortic root. Hence, the
knowledge of both normal anatomy and physiological function of the human aortic root is
critical to the clinical success of these operations [2]. Moreover, since aortic root diseases
primarily affect patients with advanced age, there is a dire need for a complete
understanding of biomechanical responses of aged human aortic tissues. However, the
knowledge of structural compliance and regional variation of aged human aortic root tissue
remains very limited.
The extensibility of the aortic root in the circumferential (CIRC) and longitudinal (LONG)
directions was studied by several research groups [2–5] using pressure inflation tests with
radiopaque markers or sonomicrometric crystals using either in vitro or in vivo animal
models. The results were, however, limited to the overall dimensional changes of the whole
aortic root, not specific to each of the sinuses. Studies using either planar biaxial tests [6–11]
or uniaxial tests [12, 13] quantified the aortic root material properties at a specific location.
Since the aortic root is heterogeneous, the overall aortic root structural compliance may not
be accurately derived using such localized material testing data.
Much of our knowledge on human aortic root properties is derived from these studies of
porcine and ovine aortic roots, partly due to the limited access of human tissues. With the
advent of transcatheter valve intervention, new devices and approaches are being
extensively tested using porcine and ovine animal models. Indeed, in recent years, there
have been approximately 40 journal articles published on animal trials of various
transcatheter valve interventions, with about 500 porcine, ovine, bovine animals used [14–
24]. The number could be much higher considering those unpublished animal experiments.
Although significant experience has been gained through animal and human clinical trials,
disparity between the results of animal trials and those of human trials often exists. It should
be noted that these animals were often young and healthy at the time of implantation. For
instance, juvenile swine with weight of 35–46 kg [25] and 45–55 kg [26] was used to
evaluate transcatheter aortic valve (TAV) device and delivery system. Wendt et al. [27]
recently reported feasibility and safety of the transapical ACURATE TA ™ (Symetis SA,
Ecublens, Switzerland) TAV implantation using healthy porcine (57 – 71 kg) and ovine (36
– 52 kg) models. Although doubts always exist regarding the validity of animal models and
their applicability to human ones, there is clearly a lack of scientific evidence and
engineering quantification of the discrepancy between animal and human trials. Therefore,
the current assumption taken for TAV pre-clinical trials - porcine and ovine animal models
are similar to those of aged humans – is still prevailing.
In this study, human aortic roots were characterized and compared to young porcine ones.
Structural compliance of both human and porcine aortic roots was analyzed at different
regions, including the three sinuses: the non-coronary sinus (NCS), the left coronary sinus
(LCS) and the right coronary sinus (RCS), and at three regions along the LONG direction of
each sinus: the upper sinus (US), the middle sinus (MS) and the lower sinus (LS) near the
aortic annulus, and the ascending aorta (AA) above the NCS.
Li et al. Page 2
J Biomed Mater Res A. Author manuscript; available in PMC 2015 July 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript

MATERIALS AND METHODS
Tissue Preparation
Ten human cadaver hearts (age of 81.00 ± 8.74 years and weight of 563.50 ± 218.35g)
without any valvular heart disease were obtained from the National Disease Research
Interchange (NDRI, Philadelphia, PA). The use of human tissues was approved by the
Institutional Review Board at the University of Connecticut. The characteristics of human
specimens were listed in Table 1. All human hearts were fresh frozen within a post-mortem
recovery interval (15.32 ± 6.51 hours) and remained frozen until delivery on the next day.
All hearts were stored in −80°C freezer prior to testing. Ten fresh frozen porcine hearts with
ascending aortas (6 – 9 months old and weight of 600.09 ± 75.46 g) were obtained from the
Animal Technologies, Inc. (Tyler, TX) and stored in −80°C freezer. Prior to testing, each
heart was submerged in a 37°C water bath until totally defrosted. Both human and porcine
hearts were frozen and thawed using the same procedure. The aortic root including
ascending aorta was carefully separated from the left ventricle and surrounding tissues. All
adherent connective and fatty tissues on the surface of the aortic root were carefully
removed from the specimens. The coronary arteries were occluded with sutures to prevent
leakage during pressurization of the aortic root.
Experiment Setup
Each aortic root was cannulated at the AA using a plastic fitting, mounted vertically to a
laboratory stand via a plastic ring clamp, and submerged in 0.9% saline solution. Fig. 1
shows the setup of the inflation test system. The plastic fitting was connected to a pressure
transducer (model BLPR2, World Precision Instruments, Sarasota, FL) and a 100 mL
surgical syringe through plastic barb fittings and flexible tubing. The syringe filled with
saline solution was used to pressurize the aortic root. A hand-held pressure gauge with a
range up to 300 mmHg was connected to the tubing for calibration of the pressure
transducer. The pressure transducer and hand-held pressure gauge were positioned at the
same height level as the aortic root in order to minimize the pressure difference. The
pressure transducer was calibrated up to 200 mmHg against the pressure gauge with error
less than 1 mmHg. After 10 cycles of preconditioning, the aortic root was inflated from 0 to
200 mmHg by smoothly injecting saline solution to the root. An inflation pressure of 200
mmHg was chosen because the aortic root may bear high loads during procedures such as
TAV implantation. Two CCD cameras (model XC-ST50, Sony Corporation of America,
Park Ridge, NJ), positioned approximately 30 degree apart from each other, were utilized to
capture the motion of the markers on the specimen at 30 frames per second. An in-house
LabVIEW (National Instruments, Austin TX) program was developed to simultaneously
acquire videos from the two cameras and pressure data from the pressure transducer.
Surface Strain Computation
The marker layout on the aortic root is shown in Fig. 2a. The markers were used to calculate
the mechanical responses of each sinus and at three regions along the LONG direction—
US, MS and LS, as well as AA. To minimize the effect of coronary arteries on the strain
measurement of RCS and LCS, the markers were affixed 3–5 mm away from coronary
arterial ostia. The marker pattern on the specimen was arranged so that each region consists
Li et al. Page 3
J Biomed Mater Res A. Author manuscript; available in PMC 2015 July 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript
of 7 markers (Fig. 2b). Three dimensional (3D) spatial coordinates of the markers were
reconstructed from the 2D images using the direct linear transformation method [28–30].
The 3D coordinates of all markers were captured at all frames to calculate the displacement
gradients and the regional in-plane Green strain.
To compute the in-plane Green strain within each region, shell-based 2D isoparametric finite
element shape functions [31] were used to fit the surface geometry of each region.
Following the surface fitting methods reported by Sacks et al. 2002 [32], the local surface of
aortic sinus, in the region delimited by the 7 markers, was approximated by a seven-node
C0-continuity quadratic Lagrangian element. The surface fitting of the initial state (Pressure
= 0 mmHg) yields the reference configuration of the region. To determine the strain field at
each frame, the displacements of each marker were computed as the difference between the
reference and the deformed spatial marker positions. The displacement component was
fitted separately using the same shape functions. This fitting was completed for each region
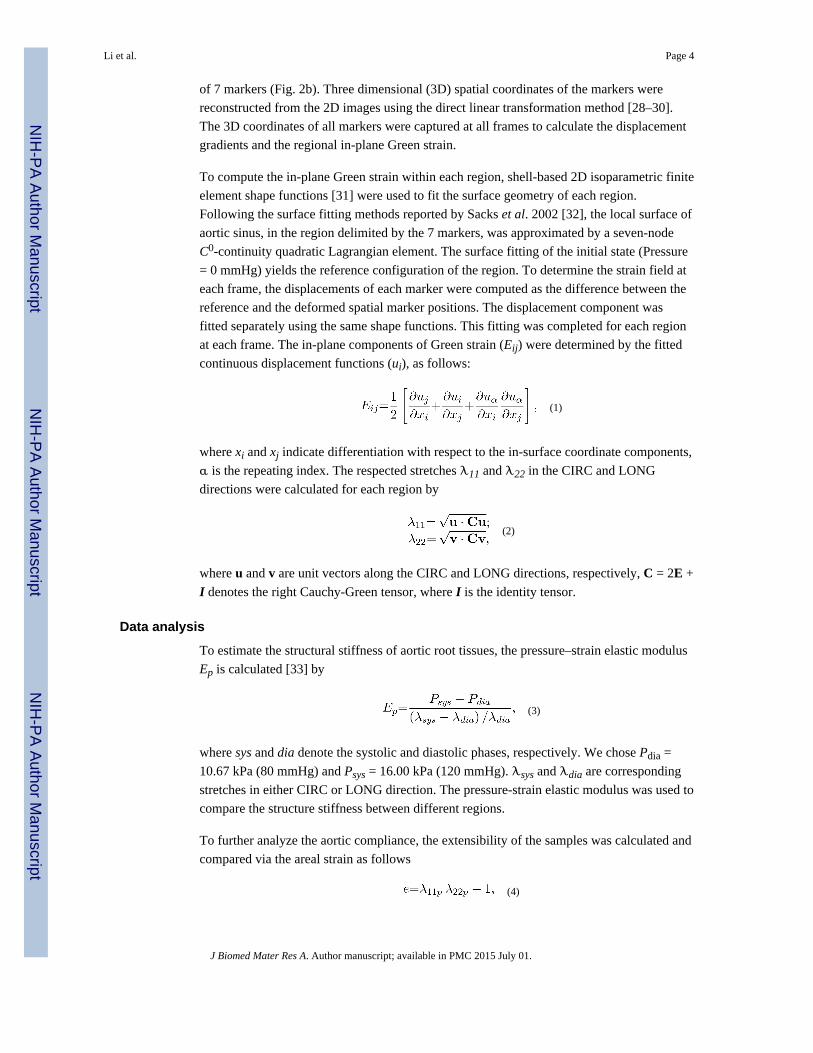
at each frame. The in-plane components of Green strain (Eij) were determined by the fitted
continuous displacement functions (ui), as follows:
(1)
where xi and xj indicate differentiation with respect to the in-surface coordinate components,
α is the repeating index. The respected stretches λ11 and λ22 in the CIRC and LONG
directions were calculated for each region by
(2)
where u and v are unit vectors along the CIRC and LONG directions, respectively, C = 2E +
I denotes the right Cauchy-Green tensor, where I is the identity tensor.
Data analysis
To estimate the structural stiffness of aortic root tissues, the pressure–strain elastic modulus
Ep is calculated [33] by
(3)
where sys and dia denote the systolic and diastolic phases, respectively. We chose Pdia =
10.67 kPa (80 mmHg) and Psys = 16.00 kPa (120 mmHg). λsys and λdia are corresponding
stretches in either CIRC or LONG direction. The pressure-strain elastic modulus was used to
compare the structure stiffness between different regions.
To further analyze the aortic compliance, the extensibility of the samples was calculated and
compared via the areal strain as follows
(4)
Li et al. Page 4
J Biomed Mater Res A. Author manuscript; available in PMC 2015 July 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript
where λ11p and λ22p are the CIRC and LONG stretch values, respectively, at three pressure
levels of p =10, 15, and 25 kPa. A pressure of 25 kPa was chosen to represent a hypertensive
condition. Patients' characterization including age, gender, hypertension (HTN) or
normotensive (NTN) were related to the biomechanical parameters to determine any
correlation.
Statistical Analysis
Statistical analyses were evaluated using SigmaPlot (V11.0, Systat Software Inc., San Jose,
CA). Both one-way and two-way Repeated Measures ANOVA tests were used to compare
the difference among the three sinuses and the regions along the LONG direction. The
Tukey pairwise multiple comparison procedures were performed to identify which group is
different, with p < 0.05 was considered a statistically significant difference and p < 0.001
indicates highly statistical significance. The Student's t-test was used to determine
significant differences between the parameters between human and porcine tissues.
RESULTS
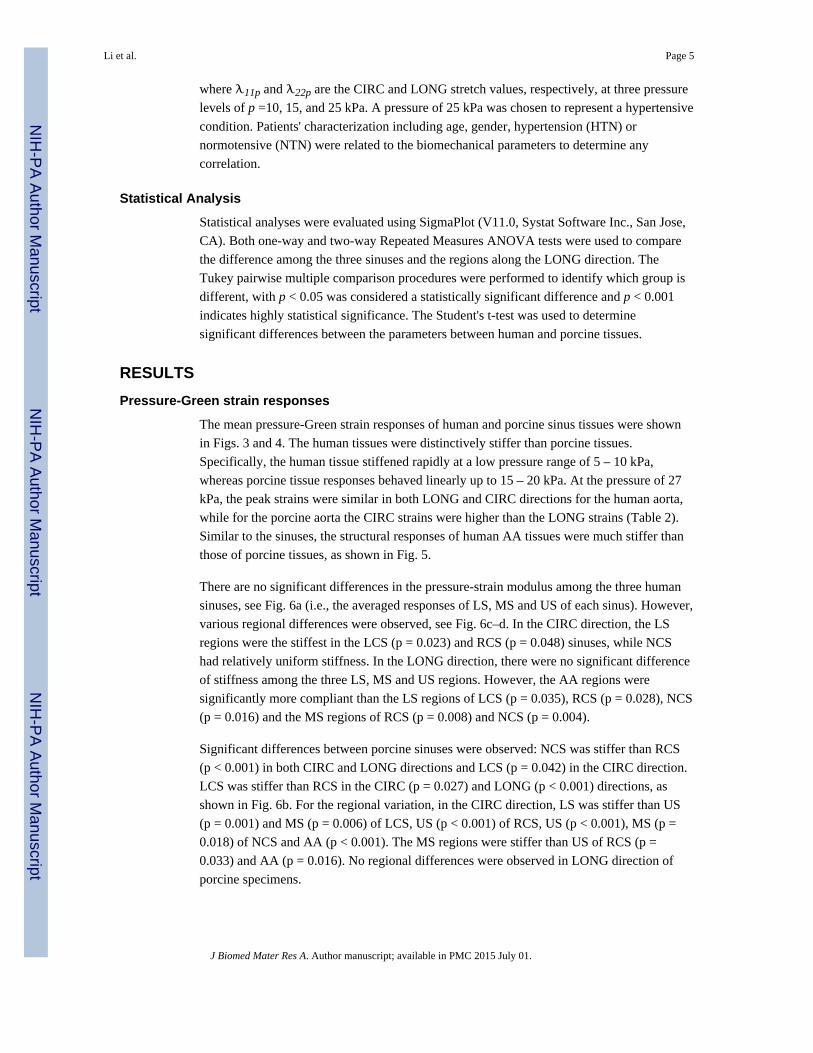
Pressure-Green strain responses
The mean pressure-Green strain responses of human and porcine sinus tissues were shown
in Figs. 3 and 4. The human tissues were distinctively stiffer than porcine tissues.
Specifically, the human tissue stiffened rapidly at a low pressure range of 5 – 10 kPa,
whereas porcine tissue responses behaved linearly up to 15 – 20 kPa. At the pressure of 27
kPa, the peak strains were similar in both LONG and CIRC directions for the human aorta,
while for the porcine aorta the CIRC strains were higher than the LONG strains (Table 2).
Similar to the sinuses, the structural responses of human AA tissues were much stiffer than
those of porcine tissues, as shown in Fig. 5.
There are no significant differences in the pressure-strain modulus among the three human
sinuses, see Fig. 6a (i.e., the averaged responses of LS, MS and US of each sinus). However,
various regional differences were observed, see Fig. 6c–d. In the CIRC direction, the LS
regions were the stiffest in the LCS (p = 0.023) and RCS (p = 0.048) sinuses, while NCS
had relatively uniform stiffness. In the LONG direction, there were no significant difference
of stiffness among the three LS, MS and US regions. However, the AA regions were
significantly more compliant than the LS regions of LCS (p = 0.035), RCS (p = 0.028), NCS
(p = 0.016) and the MS regions of RCS (p = 0.008) and NCS (p = 0.004).
Significant differences between porcine sinuses were observed: NCS was stiffer than RCS
(p < 0.001) in both CIRC and LONG directions and LCS (p = 0.042) in the CIRC direction.
LCS was stiffer than RCS in the CIRC (p = 0.027) and LONG (p < 0.001) directions, as
shown in Fig. 6b. For the regional variation, in the CIRC direction, LS was stiffer than US
(p = 0.001) and MS (p = 0.006) of LCS, US (p < 0.001) of RCS, US (p < 0.001), MS (p =
0.018) of NCS and AA (p < 0.001). The MS regions were stiffer than US of RCS (p =
0.033) and AA (p = 0.016). No regional differences were observed in LONG direction of
porcine specimens.
Li et al. Page 5
J Biomed Mater Res A. Author manuscript; available in PMC 2015 July 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript
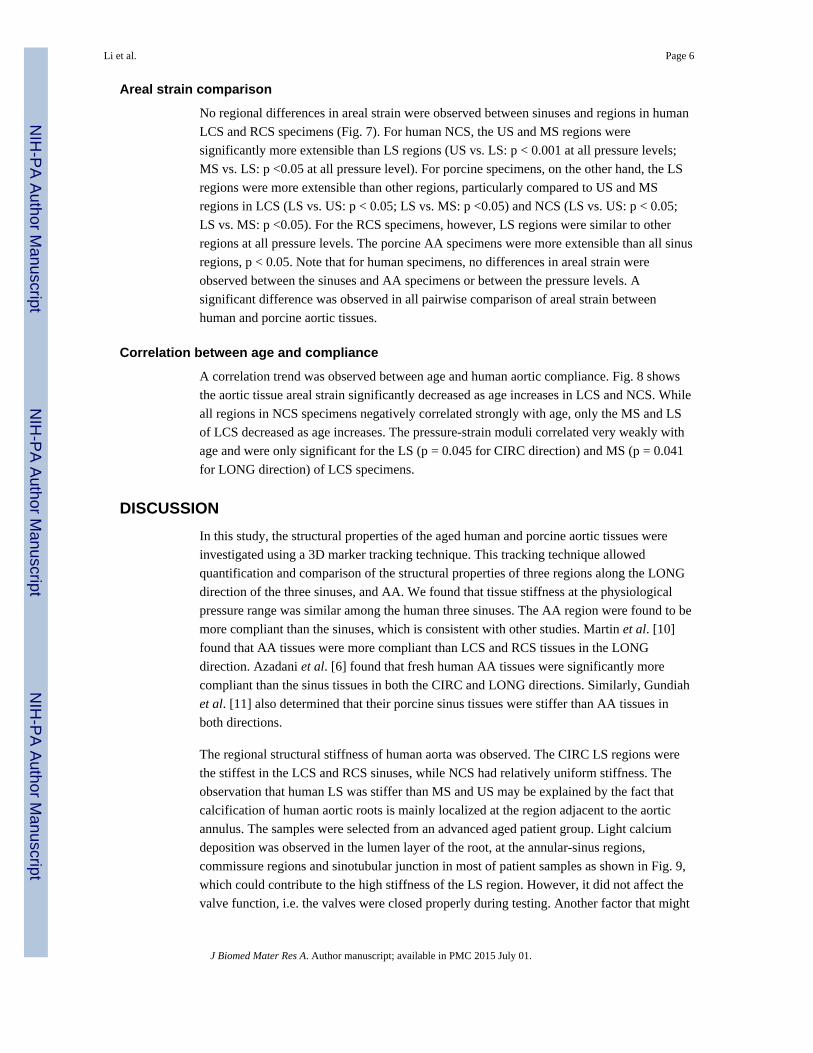
Areal strain comparison
No regional differences in areal strain were observed between sinuses and regions in human
LCS and RCS specimens (Fig. 7). For human NCS, the US and MS regions were
significantly more extensible than LS regions (US vs. LS: p < 0.001 at all pressure levels;
MS vs. LS: p <0.05 at all pressure level). For porcine specimens, on the other hand, the LS
regions were more extensible than other regions, particularly compared to US and MS
regions in LCS (LS vs. US: p < 0.05; LS vs. MS: p <0.05) and NCS (LS vs. US: p < 0.05;
LS vs. MS: p <0.05). For the RCS specimens, however, LS regions were similar to other
regions at all pressure levels. The porcine AA specimens were more extensible than all sinus
regions, p < 0.05. Note that for human specimens, no differences in areal strain were
observed between the sinuses and AA specimens or between the pressure levels. A
significant difference was observed in all pairwise comparison of areal strain between
human and porcine aortic tissues.
Correlation between age and compliance
A correlation trend was observed between age and human aortic compliance. Fig. 8 shows
the aortic tissue areal strain significantly decreased as age increases in LCS and NCS. While
all regions in NCS specimens negatively correlated strongly with age, only the MS and LS
of LCS decreased as age increases. The pressure-strain moduli correlated very weakly with
age and were only significant for the LS (p = 0.045 for CIRC direction) and MS (p = 0.041
for LONG direction) of LCS specimens.
DISCUSSION
In this study, the structural properties of the aged human and porcine aortic tissues were
investigated using a 3D marker tracking technique. This tracking technique allowed
quantification and comparison of the structural properties of three regions along the LONG
direction of the three sinuses, and AA. We found that tissue stiffness at the physiological
pressure range was similar among the human three sinuses. The AA region were found to be
more compliant than the sinuses, which is consistent with other studies. Martin et al. [10]
found that AA tissues were more compliant than LCS and RCS tissues in the LONG
direction. Azadani et al. [6] found that fresh human AA tissues were significantly more
compliant than the sinus tissues in both the CIRC and LONG directions. Similarly, Gundiah
et al. [11] also determined that their porcine sinus tissues were stiffer than AA tissues in
both directions.
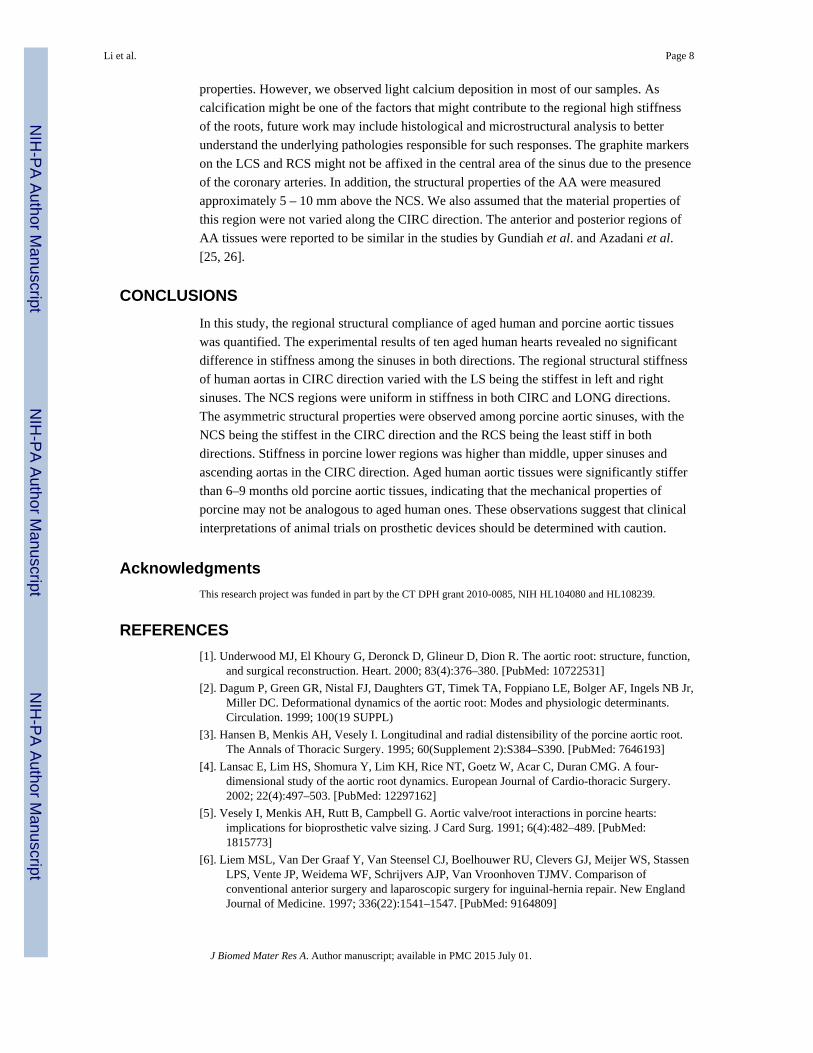
The regional structural stiffness of human aorta was observed. The CIRC LS regions were
the stiffest in the LCS and RCS sinuses, while NCS had relatively uniform stiffness. The
observation that human LS was stiffer than MS and US may be explained by the fact that
calcification of human aortic roots is mainly localized at the region adjacent to the aortic
annulus. The samples were selected from an advanced aged patient group. Light calcium
deposition was observed in the lumen layer of the root, at the annular-sinus regions,
commissure regions and sinotubular junction in most of patient samples as shown in Fig. 9,
which could contribute to the high stiffness of the LS region. However, it did not affect the
valve function, i.e. the valves were closed properly during testing. Another factor that might
Li et al. Page 6
J Biomed Mater Res A. Author manuscript; available in PMC 2015 July 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript

have caused a high stiffness in structural tissue properties is hypertension. Hypertension is a
significant risk factor for many diseases and is well known to induce changes in the
mechanical properties of the cardiovascular [34] and other arteries [35]. A total of six out of
ten patients had a record of systematic hypertension. We observed that these three out of six
patients exhibited a higher physiological stiffness than the group mean in the LS region. Our
observation suggests a trend towards an increase in physiological stiffness with either or
both calcification and hypertension. In addition, a negative correlation between age and
human tissue compliance was observed. The microstructural components such as elastin and
collagen play an important role in tissue compliance. Studies have shown that the decrease
in elastin functionality [36] and the increase in collagen fiber recruitments with aging [37,
38] might greatly impact the mechanical properties of aortic tissues, resulting in higher
stiffness and lower areal strain. A future study on the changes of the microstructure in aging
aorta in relation to changes in the structural properties as a result of the hemodynamic
alternation is needed to elucidate an increase in stiffness of aged human aortic tissues.
Statistical significant differences in stiffness and areal strain between human and porcine
aortic root tissues were found in this study, which is similar to a previous study [10]
comparing the planar biaxial mechanical properties of human and porcine aortic tissues. One
reason is that human specimens used in this study were obtained from older patients with
mean age of 81 ± 8.74 years, which could result in an overall higher stiffness of human
aortic tissues. As shown in Fig. 7, for human samples, there was no significant increase in
the areal strain when pressure increased from 10 to 25 kPa. However, for porcine specimens,
there was a significant increase in the areal strain as pressure increases. These differences
indicate that porcine aortic tissues might not be analogous to human. As this phenomenon
has been previously reported in aortic tissues [10] and other cardiovascular tissue studies
[39], it is important to know the discrepancy between the animal and human models to avoid
erroneous assumption when one attempts to apply animal data to human study, particularly
in the pre-clinical animal study of prosthetic devices. Computational modeling has also been
employed as a predictive tool to study the biomechanics of the aortic root and to better
understand the complex interactions between prostheses and host tissues. To date, due to the
lack of experimental data, many computational studies assumed homogeneity [40] of aortic
root and of different locations on the root. The aortic root has been characterized as either
linear elastic (isotropic or anisotropic) [41–45] and nonlinear hyperelastic [46–49]. The
current experimental data provide a detailed quantification of regional aortic responses
which could be used to derive tissue material responses using inverse finite element analysis
[50] as well as to validate the simulation results.
Limitations
Several assumptions and simplifications were made in the present study. Both human and
porcine tissues were frozen prior to testing. Therefore, the structural properties obtained
might be different from those of fresh tissues. Due to the limited sample size, we were not
able to identify any correlation between structural properties and age, gender and disease
states such as aortic hypertension. Because our samples were collected from a subset of
individuals with no-valvular disease in the medical record, we could not correlate aortic
pathologies (e.g. aortic wall/root dilation and wall degenerative changes) with structural
Li et al. Page 7
J Biomed Mater Res A. Author manuscript; available in PMC 2015 July 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript
properties. However, we observed light calcium deposition in most of our samples. As
calcification might be one of the factors that might contribute to the regional high stiffness
of the roots, future work may include histological and microstructural analysis to better
understand the underlying pathologies responsible for such responses. The graphite markers
on the LCS and RCS might not be affixed in the central area of the sinus due to the presence
of the coronary arteries. In addition, the structural properties of the AA were measured
approximately 5 – 10 mm above the NCS. We also assumed that the material properties of
this region were not varied along the CIRC direction. The anterior and posterior regions of
AA tissues were reported to be similar in the studies by Gundiah et al. and Azadani et al.
[25, 26].
CONCLUSIONS
In this study, the regional structural compliance of aged human and porcine aortic tissues
was quantified. The experimental results of ten aged human hearts revealed no significant
difference in stiffness among the sinuses in both directions. The regional structural stiffness
of human aortas in CIRC direction varied with the LS being the stiffest in left and right
sinuses. The NCS regions were uniform in stiffness in both CIRC and LONG directions.
The asymmetric structural properties were observed among porcine aortic sinuses, with the
NCS being the stiffest in the CIRC direction and the RCS being the least stiff in both
directions. Stiffness in porcine lower regions was higher than middle, upper sinuses and
ascending aortas in the CIRC direction. Aged human aortic tissues were significantly stiffer
than 6–9 months old porcine aortic tissues, indicating that the mechanical properties of
porcine may not be analogous to aged human ones. These observations suggest that clinical
interpretations of animal trials on prosthetic devices should be determined with caution.
Acknowledgments
This research project was funded in part by the CT DPH grant 2010-0085, NIH HL104080 and HL108239.
REFERENCES
[1]. Underwood MJ, El Khoury G, Deronck D, Glineur D, Dion R. The aortic root: structure, function,and surgical reconstruction. Heart. 2000; 83(4):376–380. [PubMed: 10722531]
[2]. Dagum P, Green GR, Nistal FJ, Daughters GT, Timek TA, Foppiano LE, Bolger AF, Ingels NB Jr,Miller DC. Deformational dynamics of the aortic root: Modes and physiologic determinants.Circulation. 1999; 100(19 SUPPL)
[3]. Hansen B, Menkis AH, Vesely I. Longitudinal and radial distensibility of the porcine aortic root.The Annals of Thoracic Surgery. 1995; 60(Supplement 2):S384–S390. [PubMed: 7646193]
[4]. Lansac E, Lim HS, Shomura Y, Lim KH, Rice NT, Goetz W, Acar C, Duran CMG. A four-dimensional study of the aortic root dynamics. European Journal of Cardio-thoracic Surgery.2002; 22(4):497–503. [PubMed: 12297162]
[5]. Vesely I, Menkis AH, Rutt B, Campbell G. Aortic valve/root interactions in porcine hearts:implications for bioprosthetic valve sizing. J Card Surg. 1991; 6(4):482–489. [PubMed:1815773]
[6]. Liem MSL, Van Der Graaf Y, Van Steensel CJ, Boelhouwer RU, Clevers GJ, Meijer WS, StassenLPS, Vente JP, Weidema WF, Schrijvers AJP, Van Vroonhoven TJMV. Comparison ofconventional anterior surgery and laparoscopic surgery for inguinal-hernia repair. New EnglandJournal of Medicine. 1997; 336(22):1541–1547. [PubMed: 9164809]
Li et al. Page 8
J Biomed Mater Res A. Author manuscript; available in PMC 2015 July 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript

[7]. Gundiah N, Kam K, Matthews PB, Guccione J, Dwyer HA, Saloner D, Chuter TAM, Guy TS,Ratcliffe MB, Tseng EE. Asymmetric Mechanical Properties of Porcine Aortic Sinuses. Annalsof Thoracic Surgery. 2008; 85(5):1631–1638. [PubMed: 18442553]
[8]. Nicosia MA, Kasalko JS, Cochran RP, Einstein DR, Kunzelman KS. Biaxial mechanicalproperties of porcine ascending aortic wall tissue. Journal of Heart Valve Disease. 2002; 11(5):680–687. [PubMed: 12358405]
[9]. Matthews PB, Azadani AN, Jhun C-S, Ge L, Guy TS, Guccione JM, Tseng EE. Comparison ofPorcine Pulmonary and Aortic Root Material Properties. The Annals of Thoracic Surgery. 2010;89(6):1981–1988. [PubMed: 20494060]
[10]. Lake GJ, Yeoh OH. MEASUREMENT OF RUBBER CUTTING RESISTANCE IN THEABSENCE OF FRICTION. Rubber Chemistry and Technology. 1980; 53(1):210–227.
[11]. Gundiah N, Matthews PB, Karimi R, Azadani A, Guccione J, Guy TS, Saloner D, Tseng EE.Significant material property differences between the porcine ascending aorta and aortic sinuses.The Journal of heart valve disease. 2008; 17(6):606–613. [PubMed: 19137790]
[12]. Ferraresi C, Manuelo Bertetto A, Maffiodo D, Franco W, Mazza L. One-dimensionalexperimental mechanical characterisation of porcine aortic root wall. Medical and BiologicalEngineering and Computing. 1999; 37(2):202–207. [PubMed: 10396824]
[13]. Satava RM. Accomplishments and challenges of surgical simulation: Dawning of the next-generation surgical education. Surgical Endoscopy. 2001; 15(3):232–241. [PubMed: 11344421]
[14]. Boudjemline Y, Agnoletti G, Bonnet D, Behr L, Borenstein N, Sidi D, Bonhoeffer P. StepsToward the Percutaneous Replacement of Atrioventricular Valves: An Experimental Study.Journal of the American College of Cardiology. 2005; 46(2):360–365. [PubMed: 16022968]
[15]. Lauten A, Ferrari M, Petri A, Ensminger SM, Gummert JF, Boudjemline Y, Schubert H,Schumm J, Hekmat K, Schlosser M, Figulla HR. Experimental evaluation of the JenaCliptranscatheter aortic valve. Catheterization and Cardiovascular Interventions. 2009; 74(3):514–519. [PubMed: 19434747]
[16]. Lutter G, Kuklinski D, Berg G, Von Samson P, Martin J, Handke M, Uhrmeister P, Beyersdorf F.Percutaneous aortic valve replacement: An experimental study. I. Studies on implantation.Journal of Thoracic and Cardiovascular Surgery. 2002; 123(4):768–776. [PubMed: 11986605]
[17]. Pavcnik D, Wright KC, Wallace S. Development and initial experimental evaluation of aprosthetic aortic valve for transcatheter placement: Work in progress. Radiology. 1992; 183(1):151–154. [PubMed: 1549662]
[18]. Walther T, Dewey T, Wimmer-Greinecker G, Doss M, Hambrecht R, Schuler G, Mohr FW,Mack M. Transapical approach for sutureless stent-fixed aortic valve implantation: experimentalresults. European Journal of Cardio-thoracic Surgery. 2006; 29(5):703–708. [PubMed:16600616]
[19]. Cribier A, Eltchaninoff H, Borenstein N. Trans-catheter implantation of a baloon-expandableprosthetic heart valves: Early results in an animal model. Circulation. 2001; 11(Suppl. 11):11–552.
[20]. Dewey TM, Walther T, Doss M, Brown D, Ryan WH, Svensson L, Mihaljevic T, Hambrecht R,Schuler G, Wimmer-Greinecker G, Mohr FW, Mack MJ. Transapical Aortic Valve Implantation:An Animal Feasibility Study. Annals of Thoracic Surgery. 2006; 82(1):110–116. [PubMed:16798200]
[21]. Garay F, Cao Q-L, Olin J, Hijazi ZM. The Cribier-Edwards percutaneous heart valve in thepulmonic position: initial animal experience. EuroIntervention Supplements. 2006; 1(SupplementA):A32–A35.
[22]. Naqvi TZ, Buchbinder M, Zarbatany D, Logan J, Molloy M, Balke G, Ainsworth R, Webb JG,Alfieri O, Maisano F. Beating-heart percutaneous mitral valve repair using a transcatheterendovascular suturing device in an animal model. Catheterization and CardiovascularInterventions. 2007; 69(4):525–531. [PubMed: 17323355]
[23]. Pedersen WR, Block P, Leon M, Kramer P, Kapadia S, Babaliaros V, Kodali S, Tuzcu EM,Feldman T. iCoapsys mitral valve repair system: Percutaneous implantation in an animal model.Catheterization and Cardiovascular Interventions. 2008; 72(1):125–131. [PubMed: 18561162]
Li et al. Page 9
J Biomed Mater Res A. Author manuscript; available in PMC 2015 July 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript
[24]. Zong GJ, Bai Y, Jiang HB, Li WP, Wu H, Zhao XX, Qin YW. Use of a novel valve stent fortranscatheter pulmonary valve replacement: An animal study. Journal of Thoracic andCardiovascular Surgery. 2009; 137(6):1363–1369. [PubMed: 19464449]
[25]. Dewey TM, Walther T, Doss M, Brown D, Ryan WH, Svensson L, Mihaljevic T, Hambrecht R,Schuler G, Wimmer-Greinecker G, Mohr FW, Mack MJ. Transapical aortic valve implantation:an animal feasibility study. Ann Thorac Surg. 2006; 82(1):110–116. [PubMed: 16798200]
[26]. Kappetein AP, Piazza N, Laborde JC, de Jaegere PP, Serruys PW. Transapical implantation of aself-expanding aortic valve bioprosthesis--animal feasibility study. Eur J Cardiothorac Surg.2009; 36(5):813–817. [PubMed: 19682918]
[27]. Wendt D, Pasa S, Kahlert P, Delaloye S, Al-Rashid F, Price V, J ⊢ínosi RA, Borenstein N, BehrL, Konorza T, Erbel R, Jakob H, Thielmann M. A New self-expandable transcatheter aortic valvefor transapical implantation: Feasibility in acute and chronic animal experiments. ScandinavianCardiovascular Journal. 2013; 47(3):145–153. [PubMed: 23098267]
[28]. Marzan GT, KH. A Computer Program for Direct Linear Transformation Solution of theCollinearity Condition and some Applications of it; Proceedings of the Symposium on Close-Range Photogrammetric Systems; 1975. p. 420-476.
[29]. Iyengar AKS, Sugimoto H, Smith DB, Sacks MS. Dynamic in vitro quantification ofbioprosthetic heart valve leaflet motion using structured light projection. Annals of BiomedicalEngineering. 2001; 29(11):963–973. [PubMed: 11791679]
[30]. Sun W, Abad A, Sacks MS. Simulated Bioprosthetic Heart Valve Deformation under Quasi-Static Loading. Journal of Biomechanical Engineering. 2005; 127(6):905–914. [PubMed:16438226]
[31]. Section 11.5 Surface-based fluid modeling, ABAQUS Analysis Manual. 2012. ABAQUS_6.11
[32]. Sacks MS, He Z, Baijens L, Wanant S, Shah P, Sugimoto H, Yoganathan AP. Surface strains inthe anterior leaflet of the functioning mitral valve. Annals of Biomedical Engineering. 2002;30(10):1281–1290. [PubMed: 12540204]
[33]. Lill S, Rantala A, Vahlberg T, Grönroos JM. Elective laparoscopic cholecystectomy: The effectof age on conversions, complications and long-term results. Digestive Surgery. 2011; 28(3):205–209. [PubMed: 21540608]
[34]. Matsumoto T, Hayashi K. Stress and strain distribution in hypertensive and normotensive rataorta considering residual strain. J Biomech Eng. 1996; 118(1):62–73. [PubMed: 8833076]
[35]. Hajdu MA, Baumbach GL. Mechanics of large and small cerebral arteries in chronichypertension. Am J Physiol. 1994; 266(3 Pt 2):H1027–1033. [PubMed: 8160806]
[36]. Fonck E, Feigl GG, Fasel J, Sage D, Unser M, Rufenacht DA, Stergiopulos N. Effect of aging onelastin functionality in human cerebral arteries. Stroke. 2009; 40(7):2552–2556. [PubMed:19478233]
[37]. Garcia M, Kassab GS. Right coronary artery becomes stiffer with increase in elastin and collagenin right ventricular hypertrophy. J Appl Physiol. 2009; 106(4):1338–1346. [PubMed: 19179652]
[38]. Wuyts FL, Vanhuyse VJ, Langewouters GJ, Decraemer WF, Raman ER, Buyle S. Elasticproperties of human aortas in relation to age and atherosclerosis: a structural model. Physics inMedicine and Biology. 1995; 40(10):1577. [PubMed: 8532741]
[39]. Pham T, Sun W. Comparison of biaxial mechanical properties of coronary sinus tissues fromporcine, ovine and aged human species. J Mech Behav Biomed Mater. 2012; 6:21–29. [PubMed:22301170]
[40]. Liu A, Tendick F, Cleary K, Kaufmann C. A Survey of Surgical Simulation: Applications,Technology, and Education. Presence: Teleoperators and Virtual Environments. 2003; 12(6):599–614.
[41]. Conti CA, Votta E, Della Corte A, Del Viscovo L, Bancone C, Cotrufo M, Redaelli A. Dynamicfinite element analysis of the aortic root from MRI-derived parameters. Medical Engineering &Physics. 2010; 32(2):212–221. [PubMed: 20060766]
[42]. Soncini M, Votta E, Zinicchino S, Burrone V, Mangini A, Lemma M, Antona C, Redaelli A.Aortic root performance after valve sparing procedure: A comparative finite element analysis.Medical Engineering & Physics. 2009; 31(2):234–243. [PubMed: 18786848]
Li et al. Page 10
J Biomed Mater Res A. Author manuscript; available in PMC 2015 July 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript

[43]. Nicosia MA, Cochran RP, Einstein DR, Rutland CJ, Kunzelman KS. A coupled fluid-structurefinite element model of the aortic valve and root. Journal of Heart Valve Disease. 2003; 12(6):781–789. [PubMed: 14658821]
[44]. Chanthasopeephan T, Desai J. p. Lau A, C. Modeling soft-tissue deformation prior to cutting forsurgical simulation: Finite element analysis and study of cutting parameters. IEEE Trans onBiomed. Eng. 2007; 54(3):349–359.
[45]. Valdastri P, Tognarelli S, Menciassi A, Drio P. A scalable platform for biomechanical studies oftissue cutting forces. Meas. Sci. Technol. 2009; 20
[46]. Chanthasopeephan T, Desai J. p. Lau A, C. Measuring forces in liver cutting: new equipment andexperimental results. Ann Biomed Eng. 2003; 31:1372–1378. [PubMed: 14758928]
[47]. Ranga A, Mongrain R, Mendes Galaz R, Biadillah Y, Cartier R. Large-displacement 3Dstructural analysis of an aortic valve model with nonlinear material properties. Journal of MedicalEngineering and Technology. 2004; 28(3):95–103. [PubMed: 15204613]
[48]. Mohsen Mahvash, a. V. H. “Haptic rendering of cutting: A fracture mechanics approach,”Haptics-e. The Electronic Journal of Haptics Research. 2001; 2(3)
[49]. Mohsen Mahvash LMV, Kim Diana, Jeung Kristin, Wainer Joshua, Okamura Allison M.Modeling the force of cutting with scissors. Biomedical Engineering. 2008; 55(3):848–856.
[50]. Bischoff JE, Drexler ES, Slifka AJ, McCowan CN. Quantifying nonlinear anisotropic elasticmaterial properties of biological tissue by use of membrane inflation. Computer Methods inBiomechanics and Biomedical Engineering. 2009; 12(3):353–369. [PubMed: 19396729]
Li et al. Page 11
J Biomed Mater Res A. Author manuscript; available in PMC 2015 July 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript

Figure 1.Schematic of the primary components in the inflation test system, including a specimen
chamber, an inflation test system consisting of a pressure transducer, pressure gauge, syringe
and two digital cameras.
Li et al. Page 12
J Biomed Mater Res A. Author manuscript; available in PMC 2015 July 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript
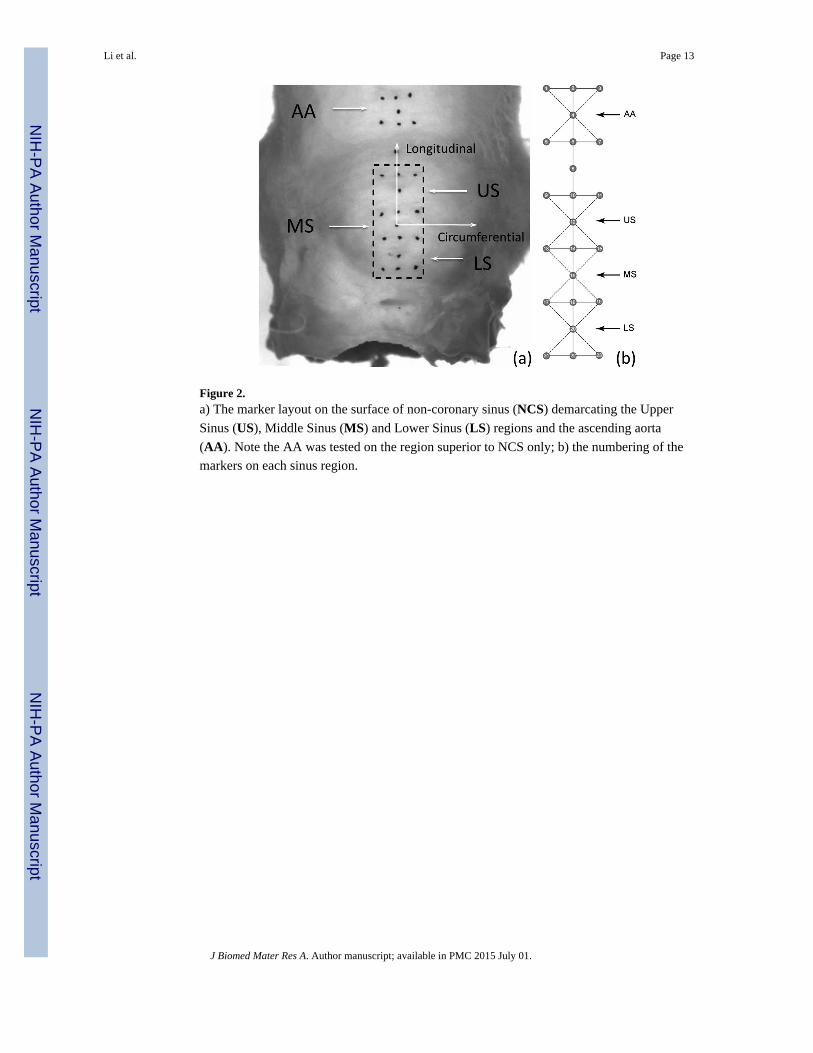
Figure 2.a) The marker layout on the surface of non-coronary sinus (NCS) demarcating the Upper
Sinus (US), Middle Sinus (MS) and Lower Sinus (LS) regions and the ascending aorta
(AA). Note the AA was tested on the region superior to NCS only; b) the numbering of the
markers on each sinus region.
Li et al. Page 13
J Biomed Mater Res A. Author manuscript; available in PMC 2015 July 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript

Figure 3.The pressure-Green strain curves (mean and standard error) in the circumferential (CIRC)
direction of human (HH) and porcine (PH) aortic root tissues. LCS – Left Coronary Sinus,
RCS – Right Coronary Sinus, NCS – Non-coronary sinus, US – Upper Sinus, MS – Middle
Sinus, and LS – Lower Sinus.
Li et al. Page 14
J Biomed Mater Res A. Author manuscript; available in PMC 2015 July 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript

Figure 4.The pressure-Green strain curves (mean and standard error) in the longitudinal (LONG)
direction of human (HH) and porcine (PH) aortic root tissues. LCS – Left Coronary Sinus,
RCS – Right Coronary Sinus, NCS – Non-coronary sinus, US – Upper Sinus, MS – Middle
Sinus, and LS – Lower Sinus.
Li et al. Page 15
J Biomed Mater Res A. Author manuscript; available in PMC 2015 July 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript
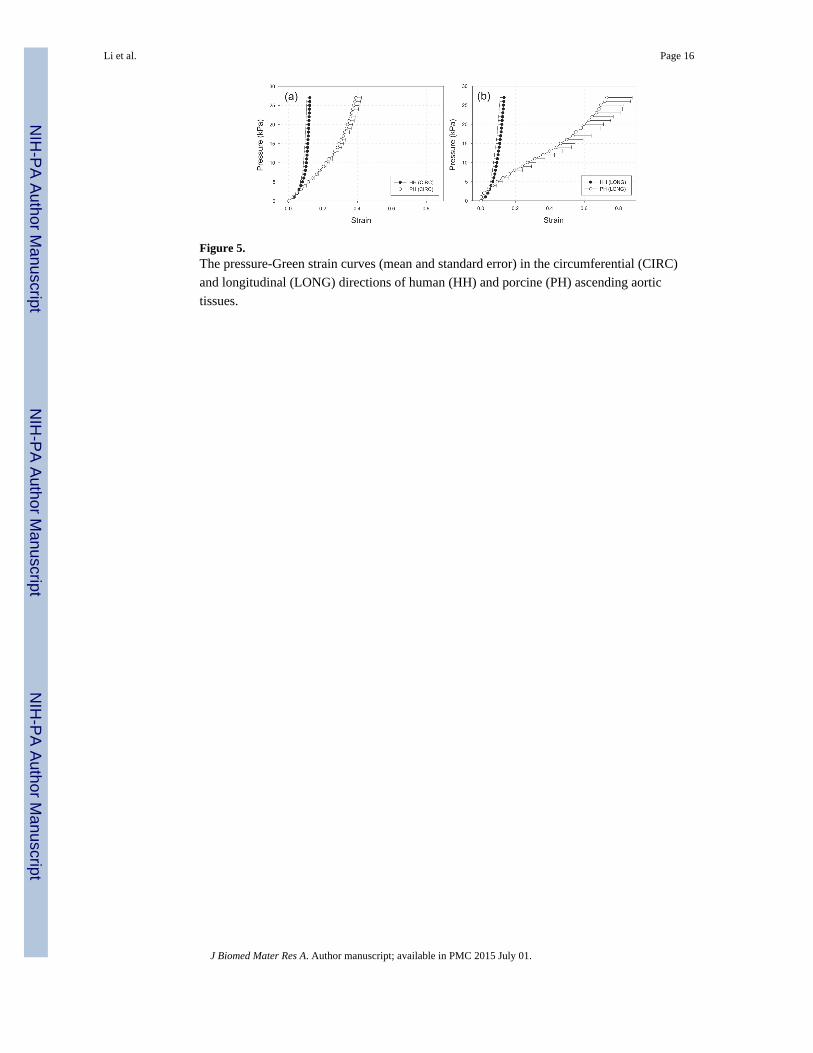
Figure 5.The pressure-Green strain curves (mean and standard error) in the circumferential (CIRC)
and longitudinal (LONG) directions of human (HH) and porcine (PH) ascending aortic
tissues.
Li et al. Page 16
J Biomed Mater Res A. Author manuscript; available in PMC 2015 July 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript
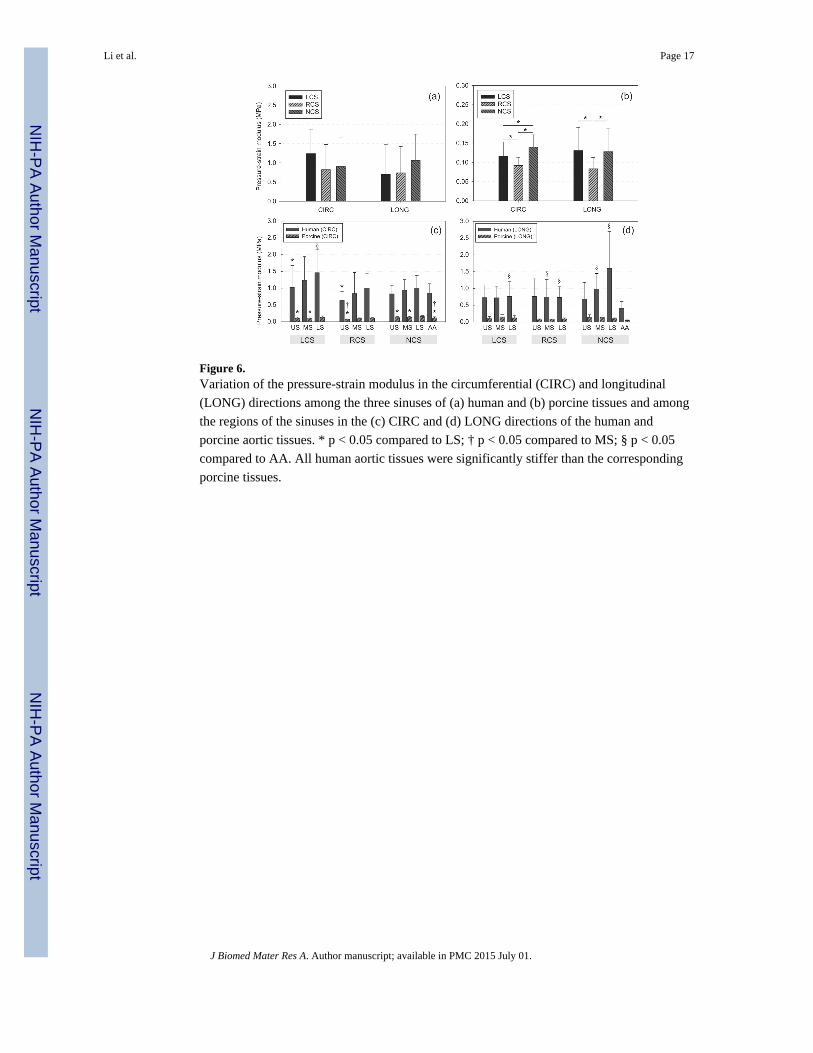
Figure 6.Variation of the pressure-strain modulus in the circumferential (CIRC) and longitudinal
(LONG) directions among the three sinuses of (a) human and (b) porcine tissues and among
the regions of the sinuses in the (c) CIRC and (d) LONG directions of the human and
porcine aortic tissues. * p < 0.05 compared to LS; † p < 0.05 compared to MS; § p < 0.05
compared to AA. All human aortic tissues were significantly stiffer than the corresponding
porcine tissues.
Li et al. Page 17
J Biomed Mater Res A. Author manuscript; available in PMC 2015 July 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript

Figure 7.Variation in (a) circumferential (CIRC) and (b) longitudinal (LONG) pressure-strain
modulus of the human and porcine aortic tissues. * p < 0.05 compared to LS; § p < 0.05
compared to AA. Difference between stress levels within sinus and regions are all
significant for porcine, but not human tissues. All human aortic tissues were significantly
stiffer than the corresponding porcine tissues.
Li et al. Page 18
J Biomed Mater Res A. Author manuscript; available in PMC 2015 July 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript

Figure 8.Correlations between age and areal strain for (a) LCS and (b) NCS specimens. Table shows
the correlation coefficient, R, and p-values. Solid lines are the linear fits to the datasets.
Li et al. Page 19
J Biomed Mater Res A. Author manuscript; available in PMC 2015 July 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript
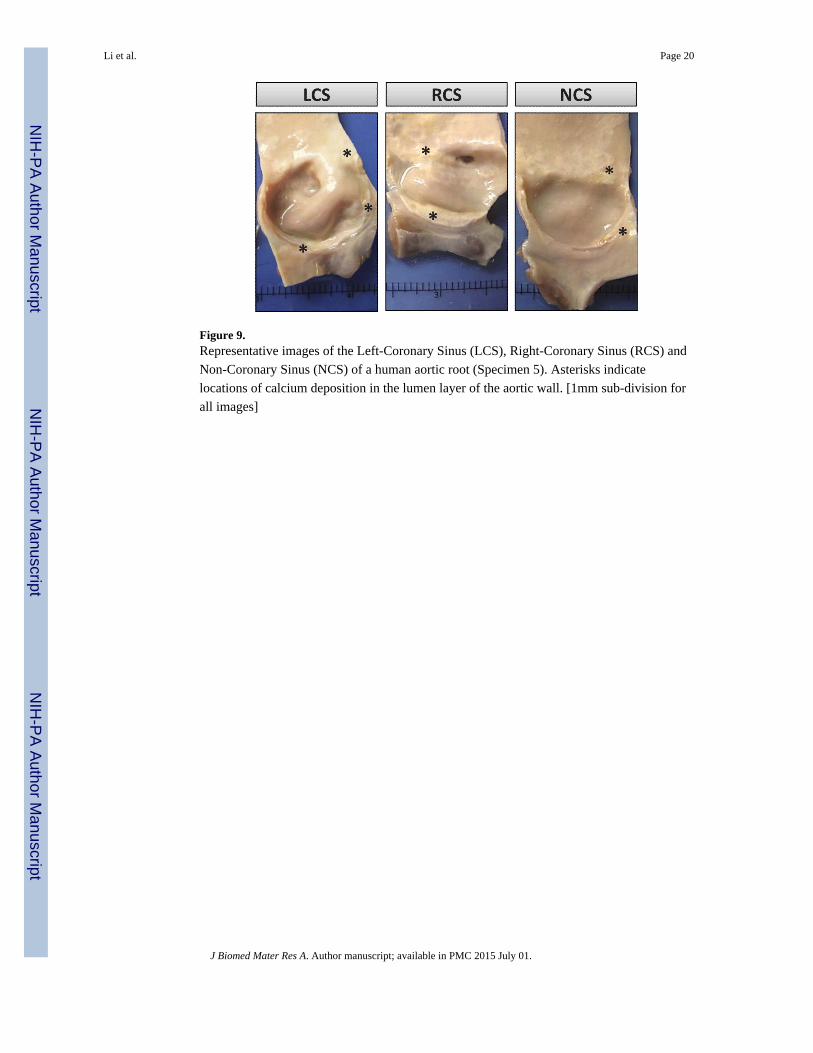
Figure 9.Representative images of the Left-Coronary Sinus (LCS), Right-Coronary Sinus (RCS) and
Non-Coronary Sinus (NCS) of a human aortic root (Specimen 5). Asterisks indicate
locations of calcium deposition in the lumen layer of the aortic wall. [1mm sub-division for
all images]
Li et al. Page 20
J Biomed Mater Res A. Author manuscript; available in PMC 2015 July 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript

NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript
Li et al. Page 21
Tab
le 1
Patie
nts'
clin
ical
info
rmat
ion
Spec
imen
12
34
56
78
910
Age
8196
8275
6375
8283
8786
Sex
FF
MM
MF
MM
FF
Cau
se o
f de
ath
AL
ZC
PAC
OPD
CA
UN
KN
CPA
CPA
VD
UN
KN
UN
KN
Ris
k fa
ctor
s
H
yper
tens
ion
NN
YN
YY
YY
NY
D
iabe
tes
NU
NK
NY
NN
NN
NN
N
A
sthm
aN
NN
NN
NN
NY
N
P
neum
onia
YN
NN
NN
NN
NN
D
emen
tia
YN
NN
NN
NY
YY
H
CL
NN
NN
YY
YN
NY
E
mph
ysem
aN
NN
NN
NN
NY
N
AL
Z: A
lzhe
imer
's d
isea
se, C
A: c
ardi
ac a
rres
t, C
HF:
con
gest
ive
hear
t fai
lure
, CO
PD: c
hron
ic o
bstr
uctiv
e pu
lmon
ary
diso
rder
, CPA
: chr
onic
pul
mon
ary
aspe
rgill
osis
, HC
L: H
yper
chol
este
role
mia
(hi
ghch
oles
tero
l lev
els)
, HT
N: h
yper
tens
ion,
RA
: res
pira
tory
arr
est,
UN
KN
: unk
now
n, V
D: V
ascu
lar
Dem
entia
.
J Biomed Mater Res A. Author manuscript; available in PMC 2015 July 01.

NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript
Li et al. Page 22
Tab
le 2
Max
imum
str
ains
at a
max
imum
str
ess
of 2
7 kP
a fo
r bo
th h
uman
and
por
cine
aor
tas.
Hum
anP
orci
ne
CIR
CL
ON
GC
IRC
LO
NG
LC
S
US
0.15
± 0
.08
0.13
± 0
.07
0.41
± 0
.08
0.29
± 0
.09
MS
0.12
± 0
.07
0.16
± 0
.09
0.42
± 0
.10
0.28
± 0
.12
LS
0.10
± 0
.08
0.15
± 0
.10
0.45
± 0
.07
0.45
± 0
.13
RC
S
US
0.12
± 0
.06
0.12
± 0
.04
0.56
± 0
.09
0.47
± 0
.18
MS
0.11
± 0
.05
0.12
± 0
.08
0.51
± 0
.11
0.41
± 0
.17
LS
0.10
± 0
.05
0.10
± 0
.04
0.45
± 0
.09
0.44
± 0
.10
NC
S
US
0.12
± 0
.06
0.15
± 0
.07
0.40
± 0
.08
0.28
± 0
.14
MS
0.10
± 0
.05
0.12
± 0
.08
0.38
± 0
.05
0.24
± 0
.10
LS
0.08
± 0
.05
0.05
± 0
.04
0.42
± 0
.05
0.44
± 0
.13
AA
0.12
± 0
.05
0.13
± 0
.08
0.39
± 0
.09
0.73
± 0
.42
J Biomed Mater Res A. Author manuscript; available in PMC 2015 July 01.