kenneth s. serota, dds, mmsc - endoexperience · diagnosis • nowhere near enough endodontics is...
TRANSCRIPT

Kenneth S. Serota, DDS, MMScKenneth S. Serota, DDS, MMSc
You are hereYou are here

Genesis, Exodus,Leviticus, Numbers, Deuteronomy
Genesis, Exodus,Leviticus, Numbers, Deuteronomy
Treatment Outcomes, Diagnosis, Anaesthesia, Access,Ultrasonics, Irrigation, Instrumentation, Obturation, MTA
Treatment Outcomes, Diagnosis, Treatment Outcomes, Diagnosis, AnaesthesiaAnaesthesia, Access,, Access,UltrasonicsUltrasonics, Irrigation, Instrumentation, , Irrigation, Instrumentation, ObturationObturation, MTA, MTA

Diagnosis - EPTDiagnosis - EPT

DiagnosisDiagnosis
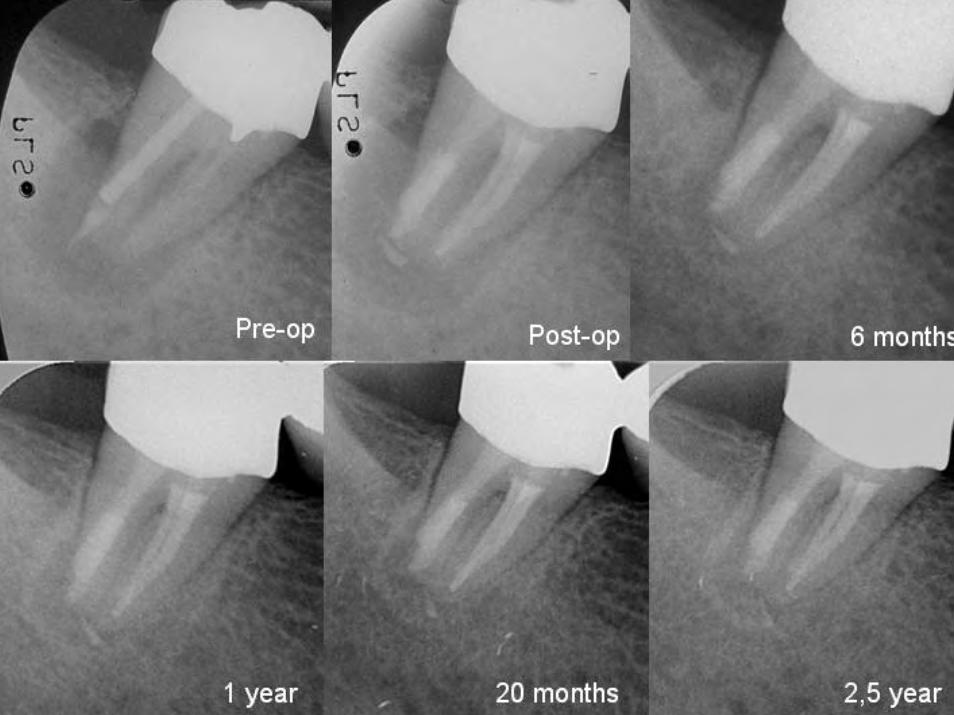
Current radiographs – – serial radiographs
• central / mesial / distal• be temporal and systematic – guide the conversation
• chief complaint –P A I N• history, stimulus, severity, frequency, duration,
location, spontaneity• onset, duration
recreate the complaint• Article - Warning signs of Pulpal Insult.pdf
Current radiographs – – serial radiographs
• central / mesial / distal• be temporal and systematic – guide the conversation
• chief complaint –P A I N• history, stimulus, severity, frequency, duration,
location, spontaneity• onset, duration
recreate the complaint• Article - Warning signs of Pulpal Insult.pdf
DiagnosisDiagnosis
• nowhere near enough endodontics is done• major missing piece in diagnosis –
Restorative History• analyze and extrapolate• tooth function and location affects diagnosis
STRESSED PULP
• nowhere near enough endodontics is done• major missing piece in diagnosis –
Restorative History• analyze and extrapolate• tooth function and location affects diagnosis
STRESSED PULP



Treatment OutcomesTreatment Outcomes
Retrospective studies have shown that the success rate of teeth without apical periodontitis remaining free of disease after initial treatment or those with orthograde retreatment is 92 to 98 percent. The chance of teeth with apical periodontitis to completely heal after initial treatment or retreatment is 74 to 86 percent, and their functionality over time determined to be 91 to 97 percent.
The difference in outcome between initial treatment and orthograde retreatment
does not appear to be significant.
Retrospective studies have shown that the success rate of teeth without apical periodontitis remaining free of disease after initial treatment or those with orthograde retreatment is 92 to 98 percent. The chance of teeth with apical periodontitis to completely heal after initial treatment or retreatment is 74 to 86 percent, and their functionality over time determined to be 91 to 97 percent.
The difference in outcome between initial treatment and orthograde retreatment
does not appear to be significant.

Effects of 4 Ni-Ti preparation techniques on root canal geometry
[assessed by micro-computed tomography]
Effects of 4 NiEffects of 4 Ni--Ti preparation techniques Ti preparation techniques on root canal geometryon root canal geometry
[assessed by micro[assessed by micro--computed tomography]computed tomography]
Peters OA, Schonenberger K, Laib A. Int Endod J. 2001Peters OA, Schonenberger K, Laib A. Int Endod J. 2001Peters OA, Schonenberger K, Laib A. Int Endod J. 2001
Maxillary molars ....all instrumentation techniques left 35% or more of the canals' surface area unchanged. ….a strong impact of variations of canal anatomywas demonstrated..
Maxillary molars ....all ....all instrumentation techniques instrumentation techniques left 35% or more of the canals' left 35% or more of the canals' surface area surface area unchangedunchanged. . …….a strong impact of .a strong impact of variations of variations of canal anatomycanal anatomywas demonstrated..was demonstrated..


Pulpal and Periapical DiseasePulpal and Periapical Disease
physicalchemical
microbiological
• caries• trauma
• microleakageabfraction/fractures• dentinal exposure
physicalchemical
microbiological
• caries• trauma
• microleakageabfraction/fractures• dentinal exposure
Irritation of the pulpIrritation of the pulp
microbiologicalmicrobiological

Endodonticsis
Endodonticsis
The Prevention & Treatment
of
Apical Periodontitis
The Prevention & Treatment
of
Apical Periodontitis

Pulpal and Periapical DiseasePulpal and Periapical Disease
Oral microorganismsOral microorganisms

Debridement & DisinfectionDebridement & Disinfection
‘cleaning and shaping’the root canal system
‘cleaning and shaping’the root canal system
IS MUCH MORE THANIS MUCH MORE THAN

Canal Anatomy - ComplexCanal Anatomy - Complex

Root Canal TherapyRoot Canal Therapy
MechanicalInstrumentation
MechanicalInstrumentation IrrigationIrrigation
Intra-canal medicationIntra-canal medication
R.C. FillingR.C. Filling
Microbial Control PhaseMicrobial Control Phase

Control of Endodontic InfectionControl of Endodontic Infection
1. Mech. preparation1. Mech. preparation
Apical Apical ApertureAperture PreparationPreparation
Volu
me
of
Volu
me
of
Mic
robi
al C
onte
nts
Mic
robi
al C
onte
nts #25
#30
#35
#40
Card et al. JOE 2002Sjøgren U et al. IEJ 1997 Ørstavik D et al. IEJ 1991Bystrøm et al. EDT 1987Kerekes et al. JOE 1979
Card Card et al. JOE 2002et al. JOE 2002SjSjøøgren U et al. IEJ 1997 gren U et al. IEJ 1997 ØØrstavik rstavik D et al. IEJ 1991D et al. IEJ 1991BystrBystrøøm m et al. EDT 1987et al. EDT 1987Kerekes Kerekes et al. JOE 1979et al. JOE 1979
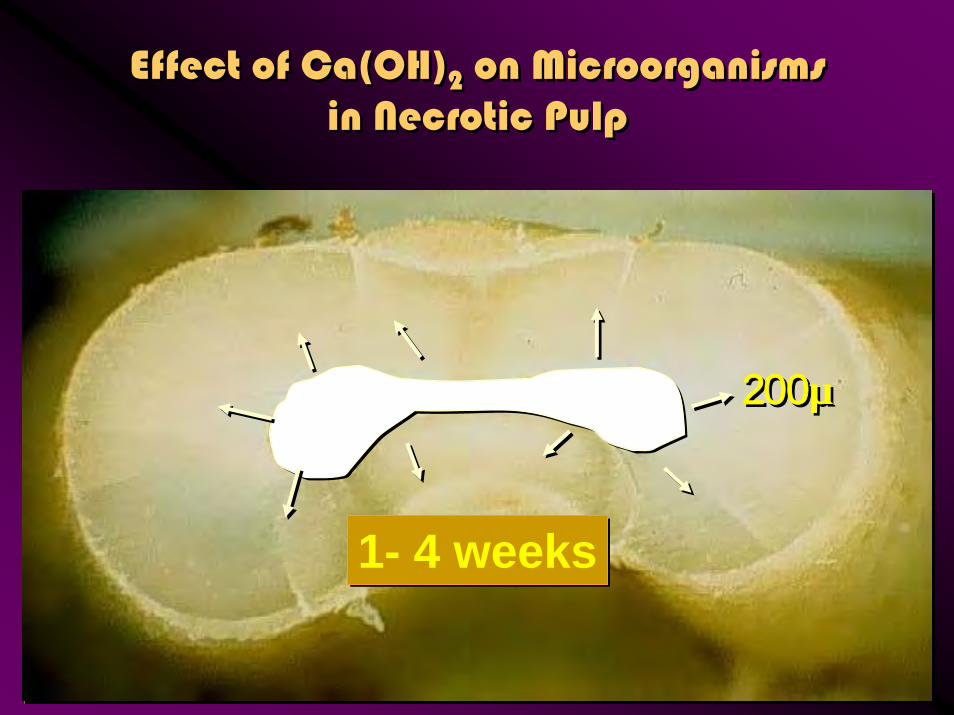
Effect of Ca(OH)2 on Microorganismsin Necrotic Pulp
Effect of Ca(OH)2 on Microorganismsin Necrotic Pulp
1- 4 weeks1- 4 weeks
200µ200µ



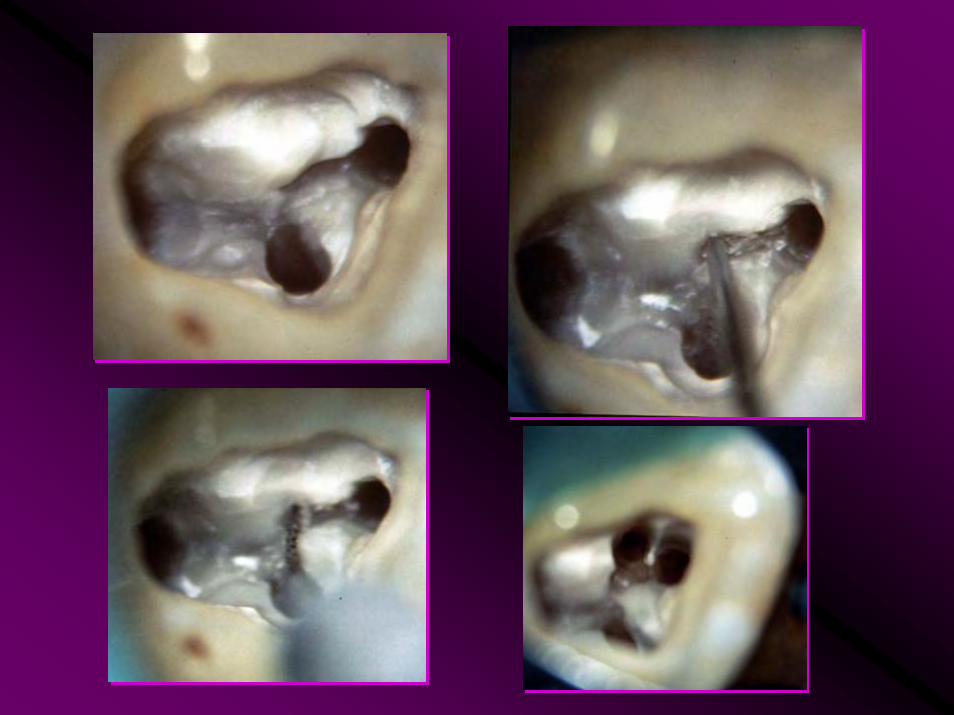
Endo is not little round holesEndo is not little round holes
Thermafil condenser removed from palatal canal
• floor is not clean nor sealed• debridement not achieved with
instruments nor irrigation protocol• neither straight line nor coronal
access adequate
Thermafil condenser removed from palatal canal
• floor is not clean nor sealed• debridement not achieved with
instruments nor irrigation protocol• neither straight line nor coronal
access adequate

Reasons for Shape/DesignReasons for Shape/Design
Convenience form• minimize overpreparation• gg’s - #1, #2, maybe #3• NiTi rotary systems
Resistance form• taper
Retention form• avoid apical displacement• Apical Control Zone
Convenience form• minimize overpreparation• gg’s - #1, #2, maybe #3• NiTi rotary systems
Resistance form• taper
Retention form• avoid apical displacement• Apical Control Zone


Goals and ObjectivesGoals and ObjectivesA substantial reduction in post treatment symptoms occurs when
using a crown down approach with rotary instruments as they are designed to remove debris coronally
A substantial reduction in post treatment symptoms occurs when using a crown down approach with rotary instruments
as they are designed to remove debris coronally

Goals and ObjectivesGoals and Objectives
“State of The Art”Gutta-Percha + Sealer?
“State of The Art”Gutta-Percha + Sealer?
• entomb existing bacteria• prevent coronal and apical
leakage• strengthen the root
• entomb existing bacteria• prevent coronal and apical
leakage• strengthen the root

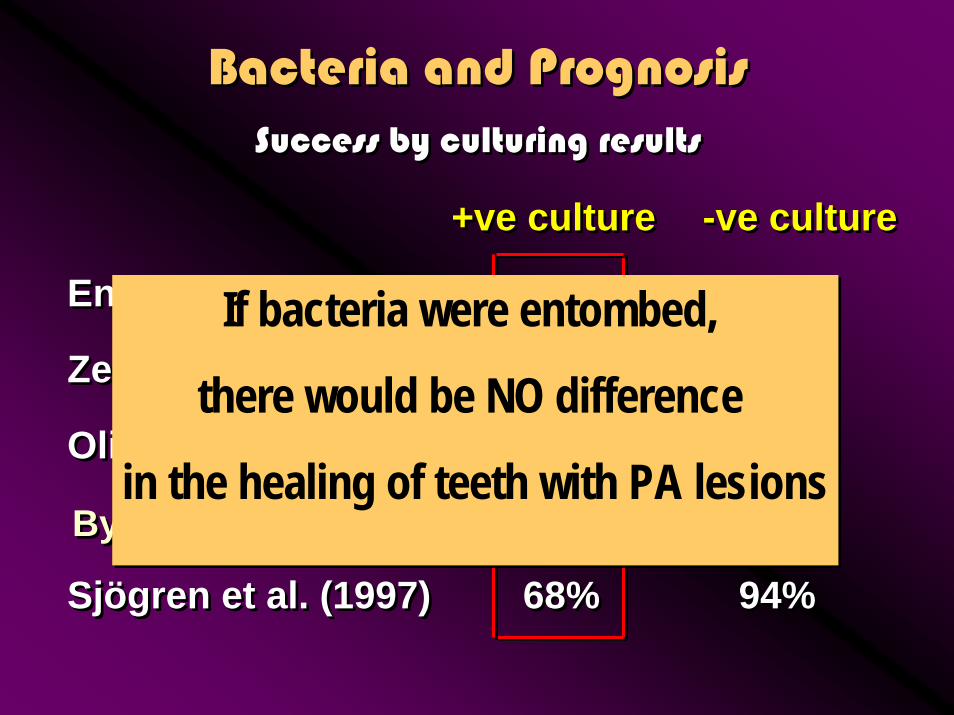
Bacteria and PrognosisBacteria and PrognosisSuccess by culturing resultsSuccess by culturing results
+ve culture+ve culture -ve culture-ve culture
Engstrom et al (1964)Engstrom et al (1964) 76%76% 89%89%
Zeldkow & Ingle (1963)Zeldkow & Ingle (1963) 83%83% 93%93%
Oliet & Sorin (1969)Oliet & Sorin (1969) 80%80% 91%91%
Sjögren et al. (1997)Sjögren et al. (1997) 68%68% 94%94%
Bystrom et al (1987)Bystrom et al (1987) 95%95%
Bacteria and PrognosisBacteria and PrognosisSuccess by culturing resultsSuccess by culturing results
+ve culture+ve culture -ve culture-ve culture
Engstrom et al (1964)Engstrom et al (1964) 76%76% 89%89%
Zeldkow & Ingle (1963)Zeldkow & Ingle (1963) 83%83% 93%93%
Oliet & Sorin (1969)Oliet & Sorin (1969) 80%80% 91%91%
Sjögren et al. (1997)Sjögren et al. (1997) 68%68% 94%94%
Bystrom et al (1987)Bystrom et al (1987) 95%95%
If bacteria were entombed,
there would be NO difference
in the healing of teeth with PA lesions
If bacteria were entombed,
there would be NO difference
in the healing of teeth with PA lesions

“State of The Art”Gutta-Percha + Sealer?
“State of The Art”Gutta-Percha + Sealer?
• entomb existing bacteria • prevent coronal and apical
leakage• strengthen the root
• entomb existing bacteria • prevent coronal and apical
leakage• strengthen the root

October / 05 JOEOctober / 05 JOESusceptibility of a Polycaprolactone-Based Root CanalFilling Material to Degradation. II. Gravimetric Evaluationof Enzymatic Hydrolysis…..Tay et al
Susceptibility of a Polycaprolactone-Based Root CanalFilling Material to Degradation. II. Gravimetric Evaluationof Enzymatic Hydrolysis…..Tay et al
Polycaprolactone is susceptible to enzymatic biodegradation via ester bond cleavage. This study examined the susceptibility of Resilon, a polycaprolactone-based root filling material to enzymatic hydrolysis. Resilon, gutta-percha, and polycaprolactone disks, prepared bycompression molding, were incubated in phosphatebuffered saline, lipase PS or cholesterol esterase at 37°C for 96 h. They were retrieved at different time intervals for gravimetric analysis and scanning electron microscopy. The materials exhibited slight weight gains when incubated in phosphate-buffered saline that can be attributed to water sorption. Gutta-percha showed similar weight gains in
the two enzymes. Conversely, Resilon and polycaprolactone exhibited extensive surface thinning and weight losses after incubation inlipase PS and cholesterol esterase. Glass filler particles in Resilonwere exposed following surface dissolution of the polymer matrix, creating rough surface topography. Biodegradation of Resilon by bacterial and salivary enzymes warrants further investigation oftheir activities using cultures of endodontically relevant microbes and human saliva extracts.
Polycaprolactone is susceptible to enzymatic biodegradation via ester bond cleavage. This study examined the susceptibility of Resilon, a polycaprolactone-based root filling material to enzymatic hydrolysis. Resilon, gutta-percha, and polycaprolactone disks, prepared bycompression molding, were incubated in phosphatebuffered saline, lipase PS or cholesterol esterase at 37°C for 96 h. They were retrieved at different time intervals for gravimetric analysis and scanning electron microscopy. The materials exhibited slight weight gains when incubated in phosphate-buffered saline that can be attributed to water sorption. Gutta-percha showed similar weight gains in
the two enzymes. Conversely, Resilon and polycaprolactone exhibited extensive surface thinning and weight losses after incubation inlipase PS and cholesterol esterase. Glass filler particles in Resilonwere exposed following surface dissolution of the polymer matrix, creating rough surface topography. Biodegradation of Resilon by bacterial and salivary enzymes warrants further investigation oftheir activities using cultures of endodontically relevant microbes and human saliva extracts.

Swanson et al. 1987 - Dye leakage to apex
Torabinejad et al. 1990 - Bacteria to apex
Khayat et al. 1993 - Bacteria to apex
Trope et al. 1994 – Endotoxins to apex
Swanson Swanson et al. 1987 et al. 1987 -- Dye Dye leakage leakage to to apexapex
Torabinejad Torabinejad et al. 1990 et al. 1990 -- Bacteria Bacteria to to apexapex
Khayat Khayat et al. 1993 et al. 1993 -- Bacteria Bacteria to to apexapex
Trope et al. 1994 Trope et al. 1994 –– Endotoxins Endotoxins to to apexapex
Coronal LeakageCoronal Leakage

Permaflo PurplePermaflo Purple

CLPCLPCLP
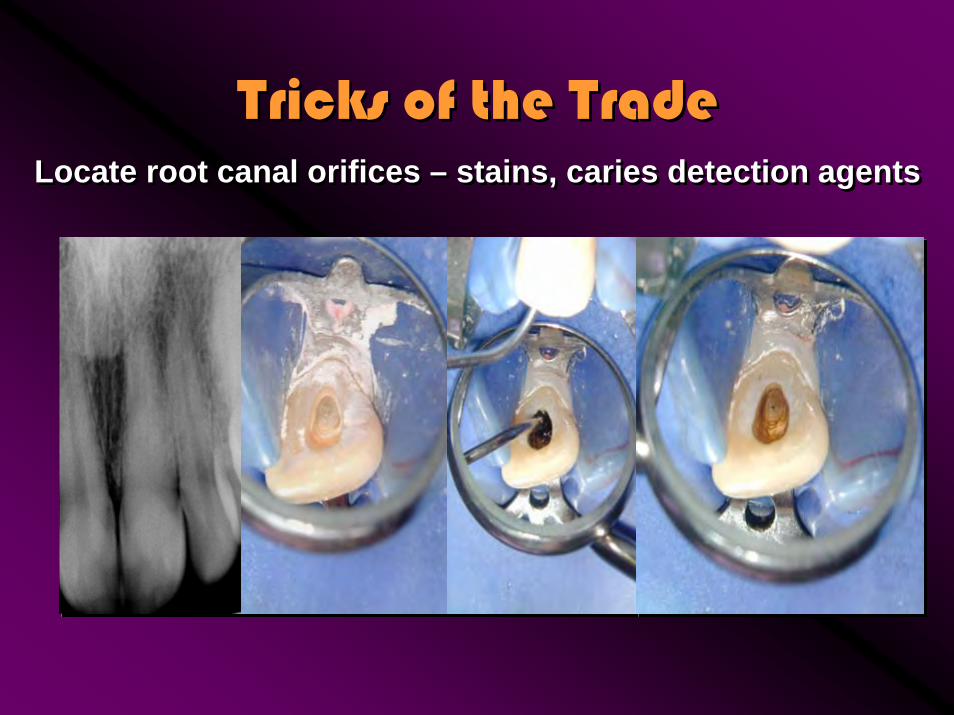
Tricks of the TradeTricks of the TradeLocate root canal orifices – stains, caries detection agentsLocate root canal orifices – stains, caries detection agents


Tricks of the TradeTricks of the Trade
Dentin of floor is darker than axial dentinAssess wet, never dry
Dentin of floor is darker than axial dentinAssess wet, never dry
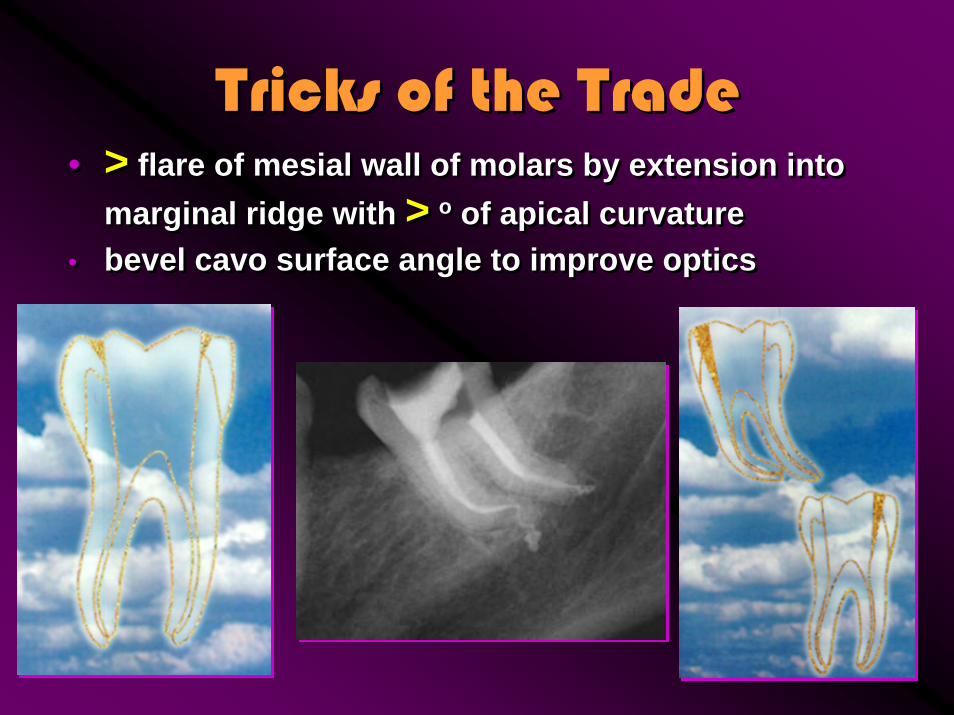
Tricks of the TradeTricks of the Trade• > flare of mesial wall of molars by extension into
marginal ridge with > o of apical curvature• bevel cavo surface angle to improve optics
• > flare of mesial wall of molars by extension into marginal ridge with > o of apical curvature
• bevel cavo surface angle to improve optics

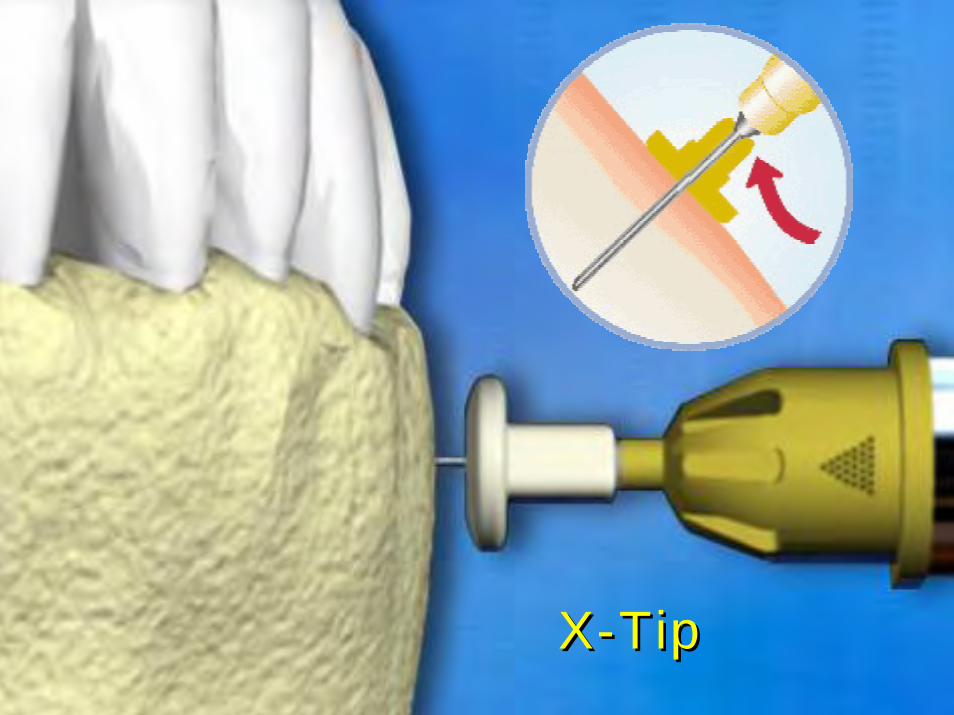
X-TipX-Tip

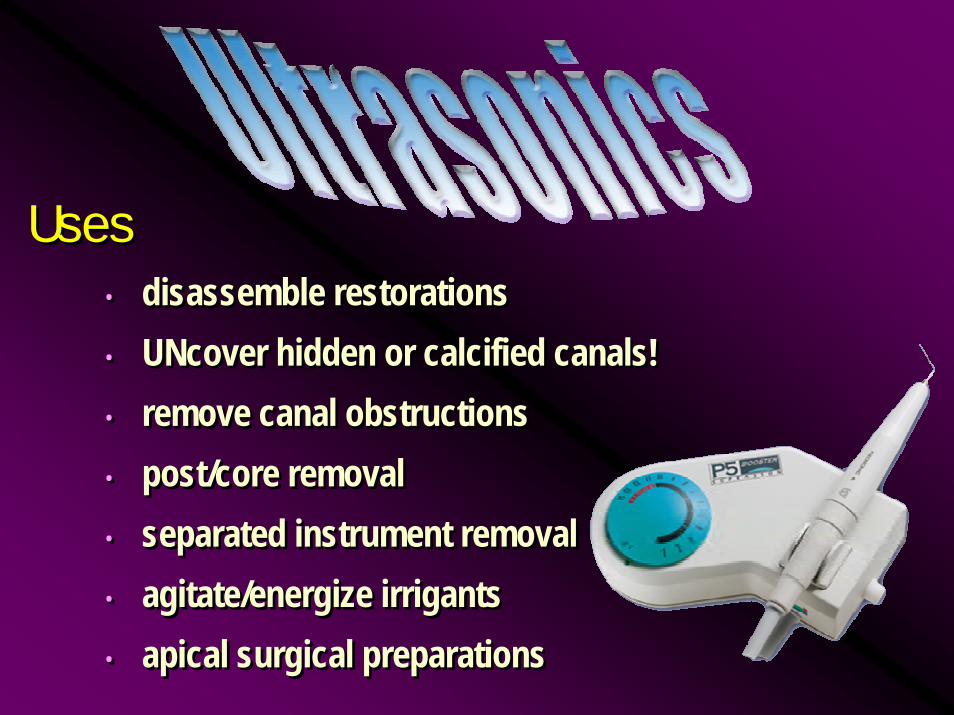
Uses• disassemble restorations • UNcover hidden or calcified canals!• remove canal obstructions• post/core removal• separated instrument removal• agitate/energize irrigants• apical surgical preparations
Uses• disassemble restorations • UNcover hidden or calcified canals!• remove canal obstructions• post/core removal• separated instrument removal• agitate/energize irrigants• apical surgical preparations
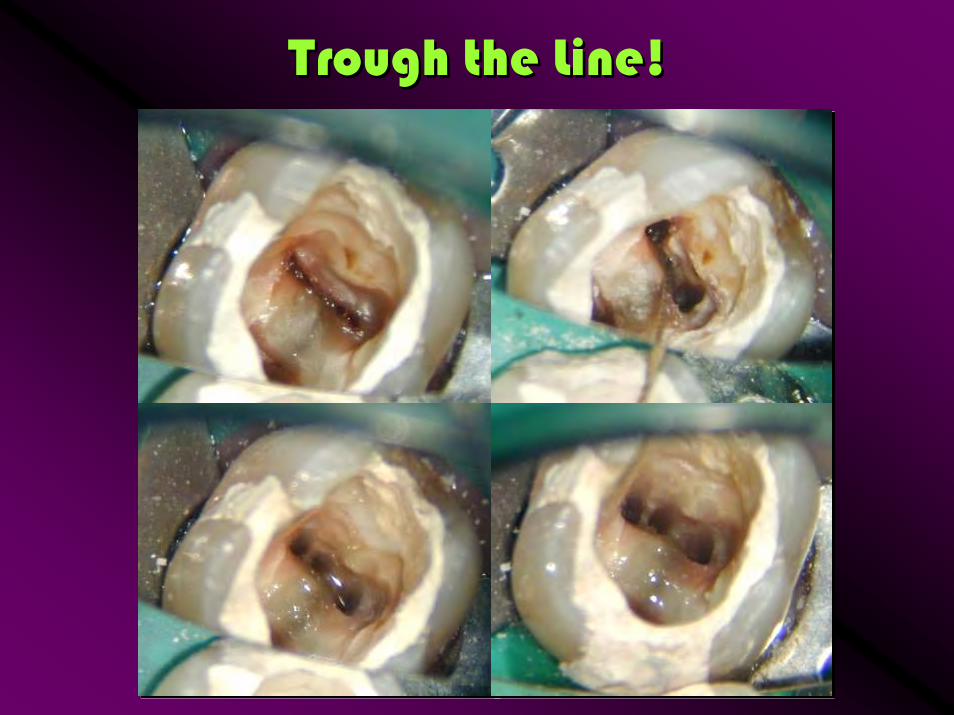
Trough the Line!Trough the Line!







Think ZThink Z
Even the world spins on an axisEven the world spins on an axis

Root Canal SYSTEMRoot Canal SYSTEM

Three Dimensions X, Y, ZThree Dimensions X, Y, Z
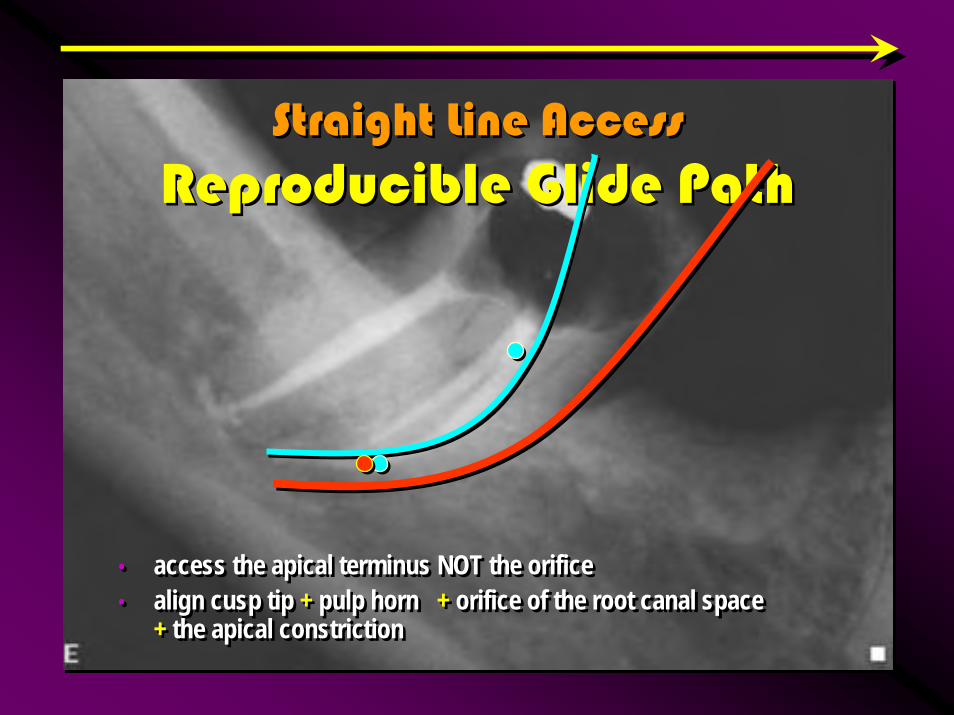
• access the apical terminus NOT the orifice• align cusp tip + pulp horn + orifice of the root canal space
+ the apical constriction
• access the apical terminus NOT the orifice• align cusp tip + pulp horn + orifice of the root canal space
+ the apical constriction
Straight Line AccessReproducible Glide Path
Straight Line AccessReproducible Glide Path
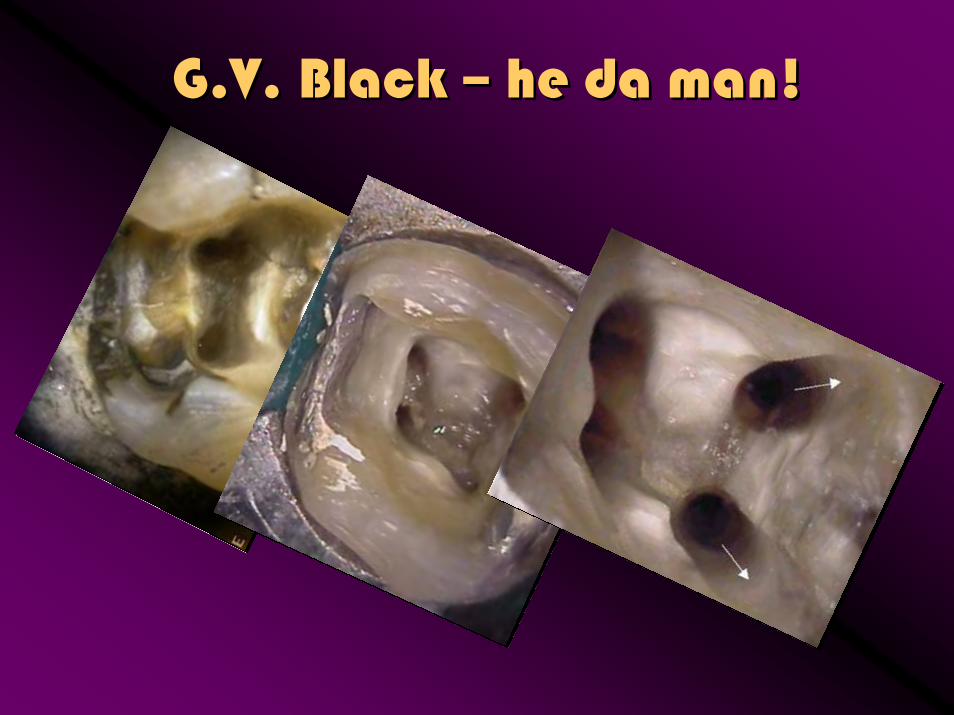
G.V. Black – he da man!G.V. Black – he da man!

Maxillary Anterior TeethMaxillary Anterior Teeth
• extension into incisal edge minimizes apical misadventure and maximizes debridement
• extension into incisal edge minimizes apical misadventure and maximizes debridement
Lingual TriangleLingual Triangle
Initial PenetrationInitial Penetration
Incisal TriangleIncisal Triangle

Maxillary Anterior TeethMaxillary Anterior Teeth

Mandibular Anterior TeethMandibular Anterior Teeth

Mandibular Incisor TeethMandibular Incisor Teeth
• must prepare access into incisal edge
• will miss lingual canal if straight line access not developed
• must prepare access into incisal edge
• will miss lingual canal if straight line access not developed
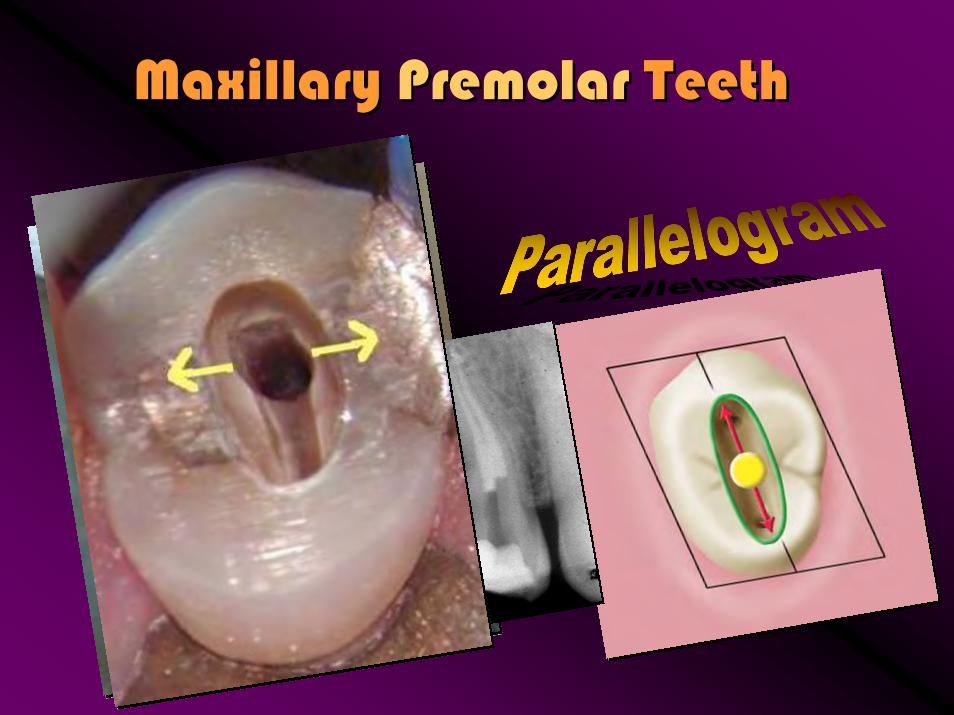
Maxillary Premolar TeethMaxillary Premolar Teeth

Maxillary Premolar TeethMaxillary Premolar Teeth

Maxillary Premolar TeethMaxillary Premolar Teeth

Mandibular Premolar TeethMandibular Premolar Teeth

Mandibular Premolar TeethMandibular Premolar Teeth

Mandibular Premolar TeethMandibular Premolar Teeth

Chromatic TopographyChromatic Topography
A road map exists, floor of the pulp chamber – dentin is darker than axial walls, fusion lines map the location of the orifices……..hypochlorite soak, etch, caries detection agents…..a road map exists beneath the layers
A road map exists, floor of the pulp chamber – dentin is darker than axial walls, fusion lines map the location of the orifices……..hypochlorite soak, etch, caries detection agents…..a road map exists beneath the layers
Maxillary Molar TeethMaxillary Molar Teeth
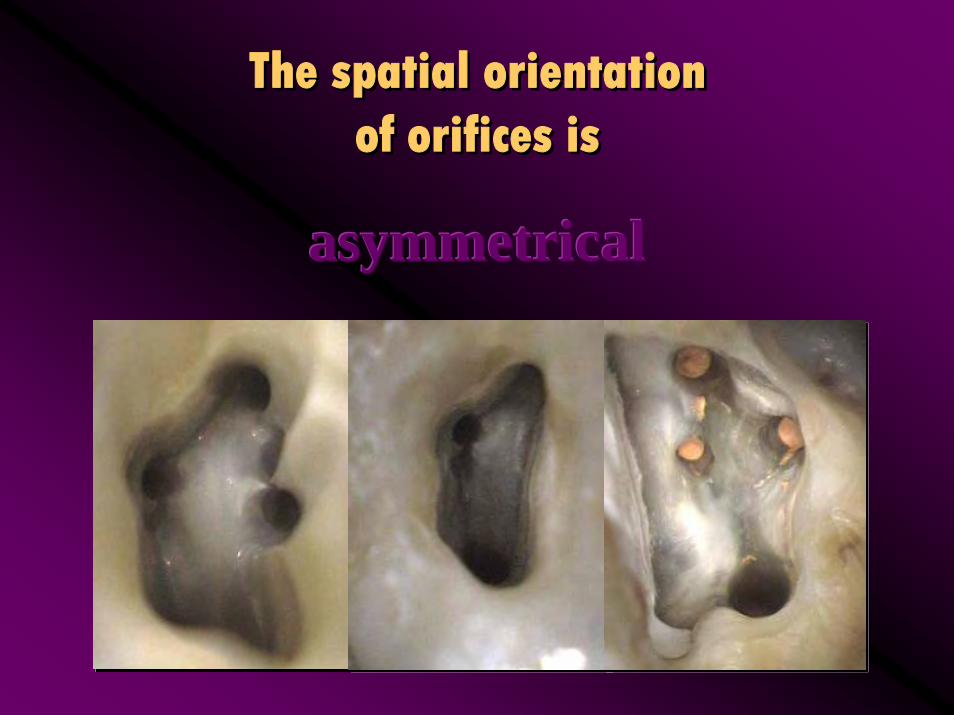
The spatial orientation of orifices is
The spatial orientation of orifices is
asymmetricalasymmetricalasymmetrical

Relocation of the canal orificesRelocation of the canal orifices




Mandibular Molar TeethMandibular Molar Teeth

Mandibular Molar TeethMandibular Molar Teeth
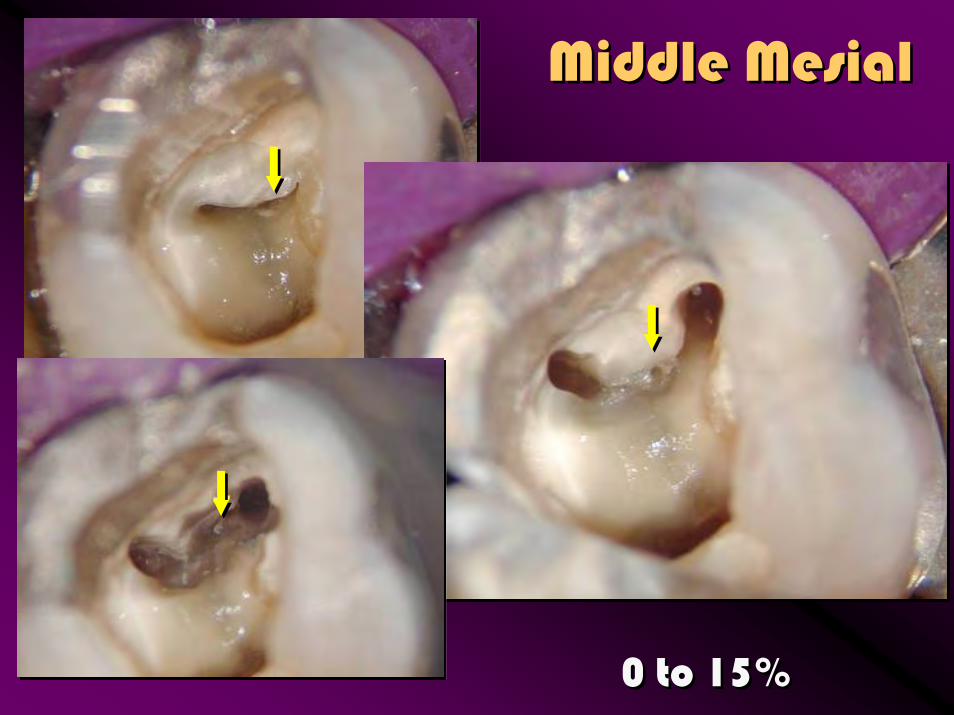
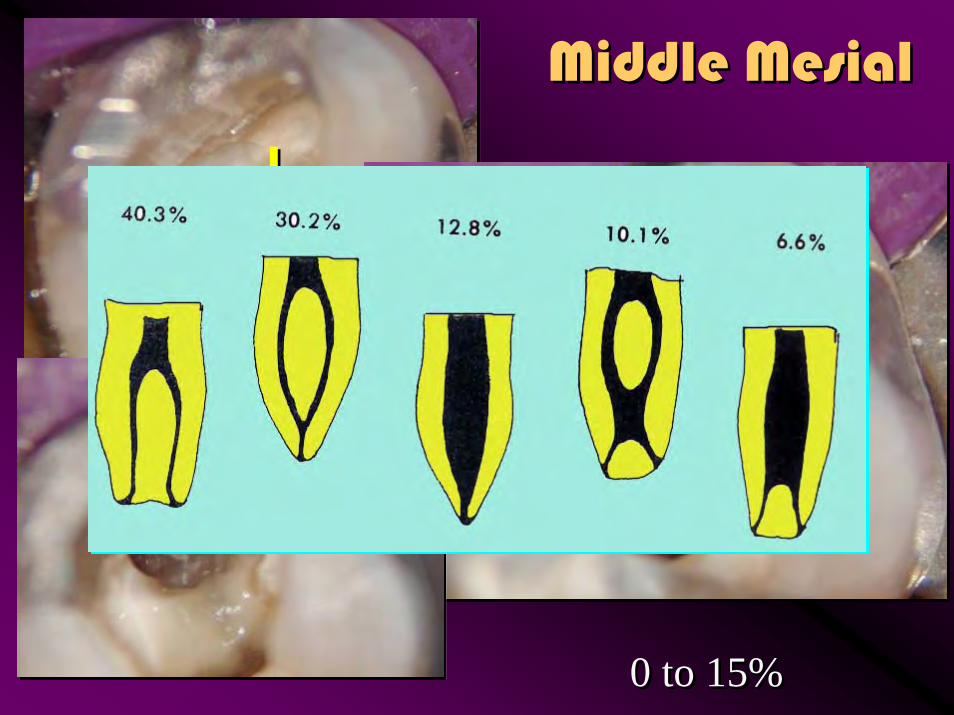
Middle MesialMiddle Mesial
0 to 15%0 to 15%
Middle MesialMiddle Mesial
0 to 15%0 to 15%



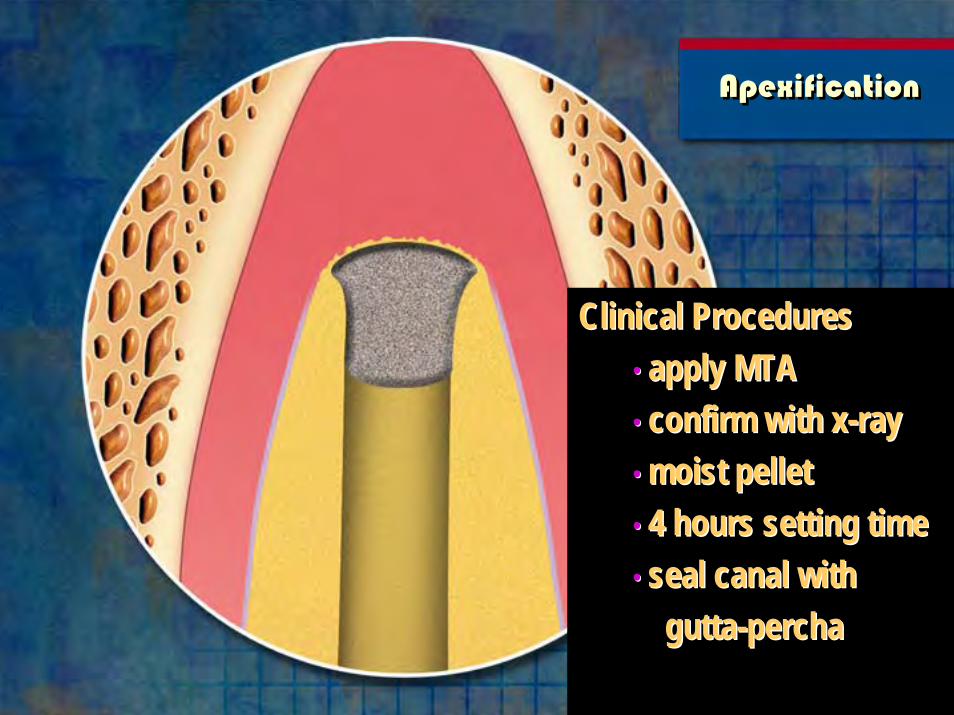
ApexificationApexification
Clinical Procedures• apply MTA• confirm with x-ray• moist pellet• 4 hours setting time• seal canal with
gutta-percha
Clinical ProceduresClinical Procedures•• apply MTAapply MTA•• confirm with xconfirm with x--rayray•• moist pelletmoist pellet•• 4 hours setting time4 hours setting time•• seal canal with seal canal with
guttagutta--perchapercha


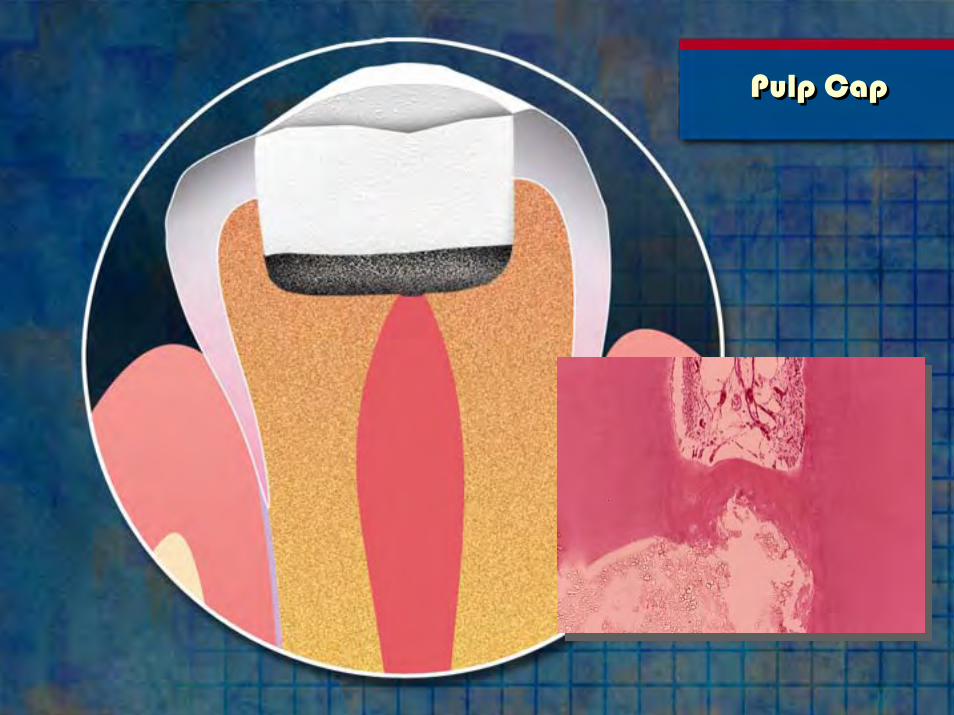
Pulp CapPulp Cap

PulpotomyPulpotomy
Indications• large pulp exposure• no symptoms
IndicationsIndications•• large pulp exposurelarge pulp exposure•• no symptomsno symptoms
PulpotomyPulpotomy
Clinical Procedures• MTA• moist pellet• temp filling• 1 week perm filling• check vitality every
3 to 6 months
Clinical ProceduresClinical Procedures•• MTAMTA•• moist pelletmoist pellet•• temp fillingtemp filling•• 1 week perm filling1 week perm filling•• check vitality every check vitality every
3 to 6 months3 to 6 months

Internal Resorption
Repair
Internal Resorption
Repair


Extra-radicularPerforation Repair
Extra-radicularPerforation Repair

Pre-OpDr. Lisa Germain
Pre-OpDr. Lisa Germain

5 month follow-up5 month follow-up

Iatrogenic PerforationMTA repair
4 – 6 hour setting timeNEVER USE RCPREP, PROLUBE
OR GLYDE WITH MTA
Iatrogenic PerforationIatrogenic PerforationMTA repairMTA repair
4 4 –– 6 hour setting time6 hour setting timeNEVER USE RCPREP, PROLUBENEVER USE RCPREP, PROLUBE
OR GLYDE WITH MTAOR GLYDE WITH MTA


FurcationPerforationFurcation
Perforation

FurcationPerforation Repair
FurcationPerforation Repair
Procedures
• MTA
• moist pellet
• temp filling
• complete RCT
• perm filling
ProceduresProcedures
•• MTAMTA
•• moist pelletmoist pellet
•• temp fillingtemp filling
•• complete RCTcomplete RCT
•• perm fillingperm filling

Furcal MisadventureFurcal Misadventure

Furcal MisadventureFurcal Misadventure

Furcal MisadventureFurcal Misadventure

Furcal MisadventureFurcal Misadventure
Root End RepairRoot End Repair
• flap• osteotomy• root-end resection• root-end preparation• control bleeding• lack of moisture control
makes MTA unmanageable
•• flapflap•• osteotomyosteotomy•• rootroot--end resectionend resection•• rootroot--end preparationend preparation•• control bleedingcontrol bleeding•• lack of moisture control lack of moisture control
makes MTA unmanageablemakes MTA unmanageable

Root End RepairRoot End Repair
Place MTA with small carrier• condense• moist pellet• do not rinse!• suture
Place MTA with small carrierPlace MTA with small carrier•• condensecondense•• moist pelletmoist pellet•• do not rinse!do not rinse!•• suturesuture