kennedy, w. robert; wile,.marcia title. studies of medical
TRANSCRIPT

DOCUMENT RESUME
ED 124 086 HE 007,950
AUTHOR Kennedy, W. Robert; Wile,.MarciaTITLE. Studies of Medical Students' Activities on Core
Surgical Clerkships:A Preliminary Report.',PUB DATE Apr 76NOTE 35p.; Presented at the American Educational Research
Association Annual Meeting (San Francisco,ft,California, April 1976)
EDRS PRICE .MF-$0.83 HC-$2.06 Plus Postage.DESCRIPTORS *Clinical Experience; Conference Reports; Field
Experience Programs; Health Occupations Education;*Higher EducatioA Internship Programs'; *MedicalEducation; Medical Students;Thys.icians; PracticumSupervision; *Student Experience; *Surgical
,TechniciansIDENTIFIERS *Case Western Reserve University
'ABSTRACTThe core surgical clerkship is described as the most
intensive clinical experience during the student's first three years,and one which is extremely difficult to examine systematically. Theresearch strategy, methodologies, data collected, and major findingsof a study of such clerkships are 'deported. The data from more than1600 hours of observation and self-reports of 77 miedical studentsprovided a substantial base of descriptive information aboult thecommonality and diversity of experiences. No judgment as to thequality of the experiences has been undertaken; rather, questionsabout students' activities have developed that have begun a processof examination to determine if such experiences are consistent orirnconsistent pith good educational planning. Major concerns areoutlined regarding equitable distribution of time, student-patientcontact without direct supervision, purposes of conferences, rolesand responsibilities of faculty towardthe medical clerk, proceduresthat all students Should learn, and instructional possibilities inthe operating room- it is concluded that the-se studies are abeginning of a systematic examination to determine whether learningunder the circumstances of he core clerkship can be optimized.(LBH)
i
******************************************************4!******.******?*** Documents acquired by ERIC include many informal unpublished* materials not available from other sources. ERIC makes every effort ** to obtain the best copy available. Nevertheless, items of marginal *
.* reproducibility are often enc9untered and this affects the ality *
* of the microfiche and,hardcopy reproductions ERIC makes ava lable. *
* via the ERIC Dodument Reproduction Service (EDRS) . EDRS of *
* responsible for the quality-of the original document. Reproductions ** supplied by ERRS are the best that can be made from the original.***********************************************************************
1

X
Studies of Medical Students' Activities
on Core Surgical' Crkships:
A Preliminary Repoist e-
W. Robert Kennedy, ';Th.D.; Marcia.Z.,Wile, Ph.D.
Case Western Reserve University
School of Medicine
U S DEPARTMENTOF HEALTH,
EDUCATION &WELFARENATIONAL INSTITUTE OP
EDUCATION
THIS DOCUMENT HAS BEEN REPRO.DUCE 0 EXACTLY AS RECEIVED FROMTHE PERSON ORORGANIZATION ORIGIN.AT tpC. IT POINTS
OF VIEW OR OPINIONSSTATED DO NOTNECESSARILY REPRE-SENT OFFICIAL
NATIONAL INSTITUTE OFEOUf.AT ION POSITION OR POLICY
Presented at the American Educ ational Research
Asociation Annual ceting, April 1976, San
Francisco, Californi4. 54E6;5) 0
2
A
ti
. I
Studies of Medical Students' ActAlti on Core Surgical Clerkship
A Prellminary Report
W. Robert kennedy,, Ph.D., Marcia Z. Wile, Ph,D.
Case Western Reserve Onivers4ty Sch000l Of Medicine
.11
The c1ertship as an:educational...expert ce has Acome an est blished
paft of the medical school curriculum. It is gene ally the 11 tinten&ive
clinical experience during the students`ftrst three and directly
follows the basic science core. Although it has critical importance ty,the
development of the student as a physician, it is one of the most difficult
segments of the curriculum to examine systematically. A number of significant
reasons extst for this situayon including theoriability of hospital
services; diversity of attending faculty and house staff as to-their roles,
activities and interest; the patient census; ,the lack,of a fund of informa-
tion,common to the firstjao-years of medical education; and the problems
of clinical evaluation of students. These factors are 'compounded by, in
many instances,' the 'institutionalization" of'-the,clerkship experience.
That is, many departments have become so accustomed to having the program that
faculty often have great'difficultksteppt4ba&-to determine Whetheieduca-,
tional goals are clear and logical, if activities are.indeed meaningful
experien or students, and what, if any, changes pre necessary. Many
times specific goals and objectives are not described or even available,
making student and faculty expectations, roles, and activities even more
va'iable and-learning, potentially,,mpre episodic.
For these reasons, the Core Clerkship Coordinator, Dean for Medical /Education, and the Division of Research in Medical Education'undertook
a series of three studies to simply define "what the students were doing on
the clerkships." This paper describes the research strategy, the Methodologies
developed and used, the data collected, and major finding& of the study.

STRATEGY
The clerkship experience at Case Western Reserve University School of
Medicine has-been in a process of evolution for.over twenty years. The
development of'the formal Inodel!_for. the cur-riulum in the-early 1950's.1
included the teaching by subject committee and introduction of three,
phase,t,,(Ham, 1962) Phase 1 -- Normal Biology of Man. -
Phase 2 -- Pathologic W13,siologY and Principles,\' of Medicine -7
Phase 3 -- Clinical Medicine. and Patient Care
In 1964, the Comdttge on Clinical Teaching reported; on the status of under-,
graduate education to the CoTmittee on Medical Educition (CME). The 'eME.,
then-made recommended changes in the third and fourth years which included-
completion of the basic clinical experience by the end orthe third year, and,,
the fourth,year as an elective program in advahOed'clinical science with
increased patient resRonsibility. I.n 1967, efforts were undertaken to
describe specific educational goals and objectives for the introductory and4 '
core clerkship using the.cognitive, affective, anti psychoMotor,domains.
Although significant efforts were 'made in these directions, riot all clerkships,
.'weft "so described and p a tices-continued as previously.
4- Beginning in the lat sixties, serious efforts to increase enrollment i
_ were undertakers _and clas4sim'increased-neatly sixty percent-over three years.. .
1 .
Of necessity, ditionallhospitaTs and services were added for clerkships with, I
. Most beirig unfamiliar with such eduCational-missions and responsibilities.i
,. .This 'created other 0oblIems ih addition to tkose previously listed. StudentI-
4., grievances included pooff definition-Of the clerkship experience, lack ofi
-appropriate supervision too much scut-work,'and a general lack of confidence
-in evaluatibn approache

3
)During 1973, a strategy began tg evolve- concerning the examination of
the clerkships. Built` from the "discrepancy model," quesOgns concerning the
#*sible lack ofcongrbence between intended and actual periences began td
emerge. Such questiops as "what are the students-doing?" muchtime do4
they read?" how mulch patient contact are they having?" evolved. fjUantifcatiOn,k'
and pbt the making of value judgements about the quality Of the egkeriences
(
was the researoh thrust.- 1
In January 1974, a pilot study of approximately 400 hours of observation'
of students' activities on the pediatric, medicfne, surgery, obstetriCs/gyne-
f
coloby, and psychiatry clerkshipEdwas completed (Figure 1). The purposes were
pre-testing and refinement of forms, data collection.procedures, and the4
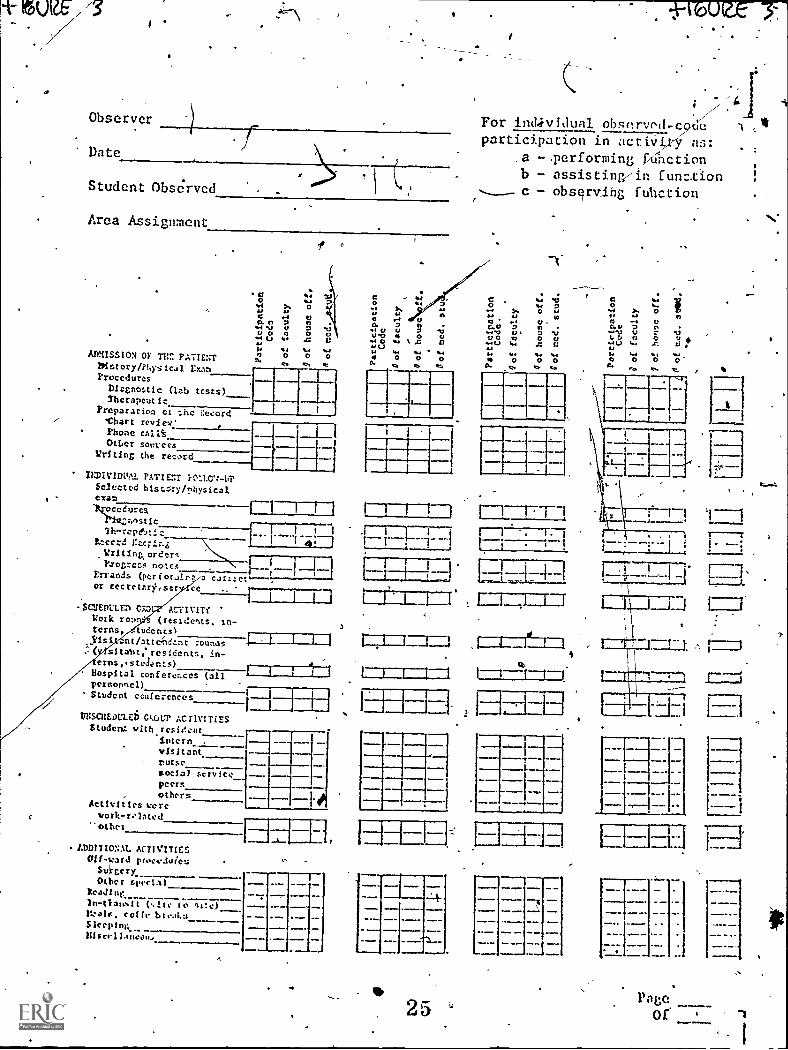
development of the necessary logistic1 support . Thd form used (Figure 2)
had been carefull.rdvolved`with the assistan p of several fourth-year students
and approved by the clinical faculty. F owing the study,,the instrument ,
was,revi5ed to include students' level of particiOation in the activity_ .
.
(performing, assisting, observing, and/or discussing) and those persons Slith,
whom they wereworking (Figure 3). These changes were the product of both
Alb
ti
research interests and the demonstrated capabilities of the observers to
validly collect such information. 1
Study 1: Structured Observations of Medical Students' Activities on.the
( Core' Surgical Clerkship
Based upon the results of the,pilot study, clerkship director the
Department of Surgery were appr9ached about pursuing an intensive de criptive
study of their services. Since this Department had developed an ex ensive
'definition of goals and objectives (DePalma 1974) which were being ollowed /
at two of the four hospitals, it was felt an anal)Itis of students' activities
might be useful,to faculty: The intent was not Oatd collection f r change
applications; but rather description'of current experiences.
5

_
r
VIThe *poses of the planned study were to:
f
(A) observe and'rec6rd studgnts' activities on the ward,and in the
operating.room;1
(B) define the, levels of responsibility they exercised in patient contact
and with ,whom (faculty, house staff, nurses, oth0s);
*
(C) the quantity'and varieties of verbal interactions they had in the4
operating room.
Data Collection Procedures
Observers:. Thirteen undergraduate pre-medic,al,studenWaere employed,
as observers and given an eight -hour training session which incliided four
hou'm of actual observation df medical students, reCording of information,----e
and familiarization with all 'sites, faculty,,andprocedures. The,study was
conducted duringt.ptersessignp January 1975, when the obser;/ers were free from
academic responsibilities and could follow their assigned surgery schedules.
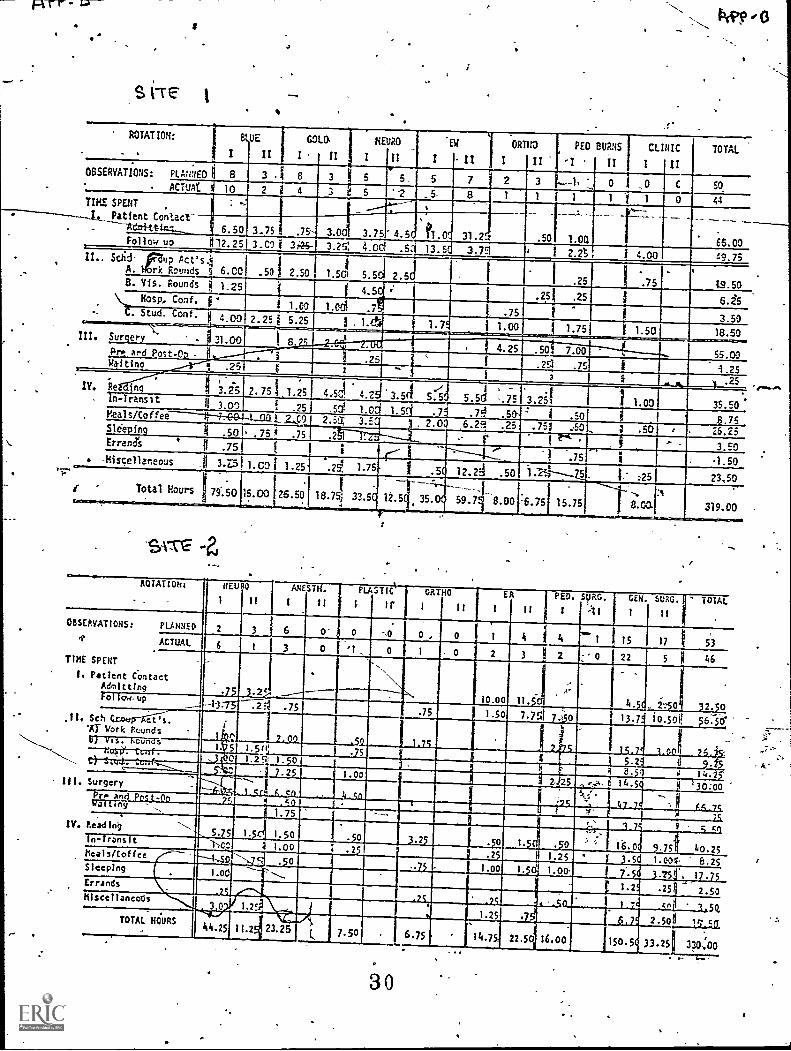
Sites: 'The four affilidted training sites participating in this
study were a large metropolitan qosOi.tal--Sife 1, a university ho4ital--Site 2,
a veteransAhOspital--Site 3, and a commun.! hospital--1 Site 4..
.
Instrumentation tI
s
The forms previously described (Figure 3) were usled in-this study and a 4
,...-
...h,
second sectioa was added to' include operating room verbal. interact' (Ffgure 4interactionThecobservers were regutred to indicate in fifteen minute units thcmprima
. .(
'activity which had occurred for the entire period\ q observation (generally11
eight hOurs). In the event they could not make such a d etermination, they
6
were encouraged to. ask -their medical student for assistance.
cheduling-the observations
The 4pedule for data collIction was developed with the following
parameters:
(a) o bservations would b e'don.e during the working day (I = 7 a.m..to 3 p.m.)
and evening (II = 3, p.m. toll p.m.), foe the period January 6 -01.:Ough 31, inclusive.4:161,
AP
6

(b) a 20 percent 11\inimumof the possible. student work gays would be
observed . For exampld,%a site with 4 stUdents would have 80 possible obser-
vation periods (4 x 20 days withOut weekends). Twenty perceht of this.would
4
be 16 possible observations. As such, the schedule-for the four sites was: ,
Site Planned` Observations Saturday/Sunday
1 50 Yes
2 53
\25Yes
3
4 ,t7 **.No
The 20 percent minimummas used as a guideline with deviations being made to
,sample subrotationsat different sites a specific nutber of times;' For
example, the director wantedonesithrotation seen three times at night. TKis:
was donebut:resulted in additional- observations to the pre-determined'
number. II. . /-. '.
t
(c clerkship directors would determine those subiotatidns td.be sampled
,. .
and theolumber of desired observations for each (i.e., neurosurgery, ENT,
._
general, surgery)..
(di) assignAents for observers at each site would be rahAom by subrotation
I.
. . -
anderhourunitst ..throughout students on
the rot4tion,at the assigned tithe'were also randothly selected from available
.E.
'Schedifes and.i.f., for any reason, they were unavailable, the observer was/ .
Oven lternate 'names.
7 A

Final Scheduled-
The fpllowing table compares the planned and actual obser-vations.by
subrotation and time (I or II), at each 13f the 'four sites.
Gen. Surg.I II
, SITE 1
teuro ERI a I Ii
OrthoI II
Ped Burns Clinic. TotalI II I II
PLANNED ' 8 3 5.
5
7
8
2r-411,
1
3
1
1
1
0 ,
1
0
1
0
o
50
44ACTUAL
10 2 5 2
SITE
Neur6 Anesth. Plastic Ortho ER
I II II I. II I II II
Ped Burns i! Total
I II., I II,- ,
PLANNED 2- 3 6 0 0 0 0 0 1 , 4 4 1 15s 17 53
ACTUAL 6 1, 3 0 1 0 1 0 2 3 2 Q 22 5 46
.1
SITE 3
tiaj .Surg.
I II
-Mi nor -Surg... Total
I II
PLANNED 11 . 3 25
ACTUAL 11 '5 . 4 25
SITE 4
Ortho ER
I I I I , II
tr
ENT CV-Thor Gen. Sufg. Total
Ho I' r I I II
'PLANNED 4 2 0 . jo, 2 2 5 1 7 4 27
ACTUAL 4. 0 1 1 2 0 4 . 1 6 7 - 26
8
9
WI/

'11
, .
Findings
The data derivedfrom the 1000 hours of observation are. presented in. %AL ,
selected forrsince the amount of information as massive and more pertinent
(as was intended) for hospital service application.
"What are the students doing in specific types of in-pient
activities?".
The tables in Appendix A show the number of,hours and percent time, per
activity for "morning", "evening", and "total" for,students observed across
the four training sites.
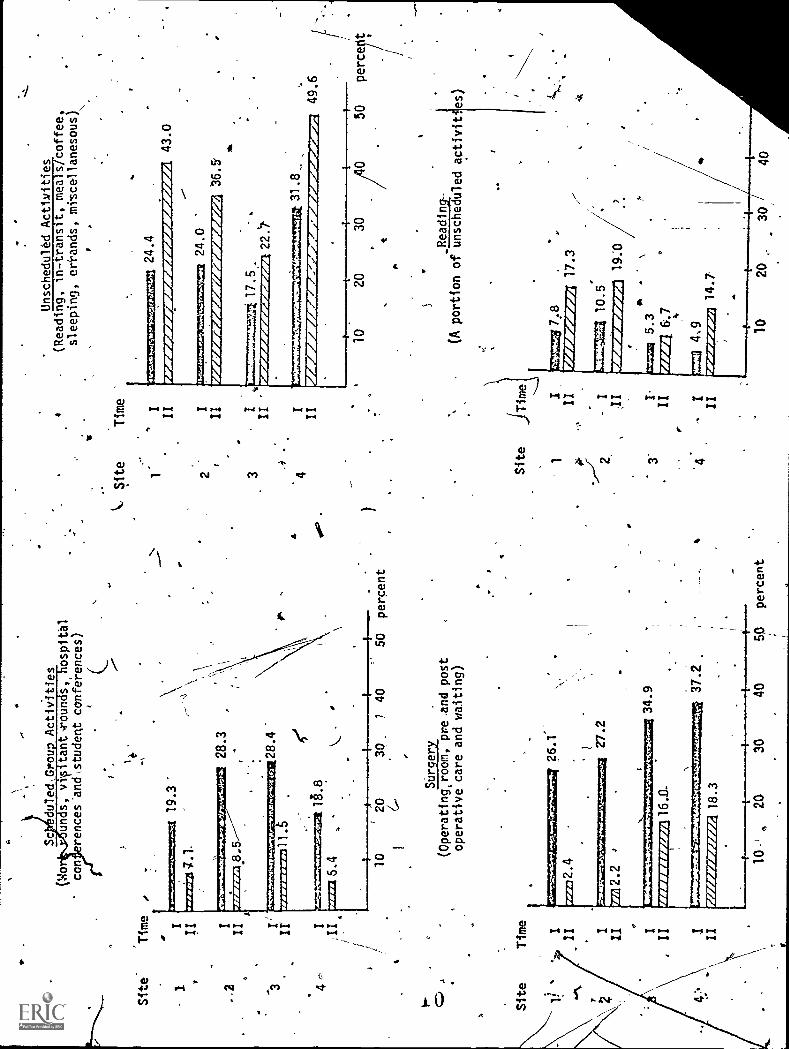
The four nfajor categories of.activitiei defined in the'observational
study were: patient contact -- scheduled group activities- -- surgery --
diunscheduled activities.' Included in "unscheduled activities" was reading.
A comparison of these major categories across the four sites is presented
in the following -bar graphs.
Patient Contact(Admitting-and follow -up)
Site Time
3 I
II
4 7). I
II
FP 1=1=30.2
AumwommwawinftrommeZmumnrowAW
20.2
45.5
W. I.IIIIIMIAINVOM
.TVe 19.3
mumarrarriurAmilmu
rsuaavowaromesur.0,744WIRge
1 1
.11I
25.8
49.8
53.0
0 30"' 40 50 60 percent
9
I
a
ptiv*ar
Site'
I
..2 3
Time
II IY
Wo con
VM
O&
LU
IN
Sc
duled.Grou
Activities
s, vv tantroun s,
ospital
rences'and\student conferences)
7 1.
19.3'
Oft
M7.
1011
470,
171.
7.1,
4.7A
4re0
"..4
.04,
1740
1411
7/71
/41%
11.5
4I r========itlg.8
6 4
..
Site
Time
7
I
II I
,II
.4
28.3
28.4
I
.71
10
20
30.
740
50
percent
C,
24
Surgery
(Operatingcroom, preand post
operative care and waiting)
26.1'
rn
2.2
27.2
MIN
SIM
EN
IZA
MIA
16.0.
477g
wtv
ra0:
47.q
34.9
AP7
7.0"
1411
4,14
4.46
6-44
6064
1FA
V"
18.3
37.2
10
420
30
40
50
percent
Site
Time
1
Unscheduled Activities
(Reading, in-transit, meals/coffee,
sleeping, eri-ands, miscellanesous)
I'73====gZSE21 24.4
II I
3.2=
q=5:
22:=
24.0
III
/50WWWWIEWAIMORAMOGREM
36.5
3I II
.drg
agra
mpr
o:or
.22.`7
.4
.
'4
I31.8_
II
1
43.0
49.6
Site
Time
10
20
30
t
_Reading-
(A portion of unscheduled activities)
50
perce t
3'
r

Students' activities differed "patieA
evening shits with the greater percentage a
and"surgical pursuits, and hospital adniiss
prevailed' across all sites.
r.
t contact" frgil thejnorning to
night due to fewer "scheduled"
on procedures. The pattern
"Scheduled activities" differed on the morning rotations because Sitev
2 and 3 allotted more time to "Work rounds" and "student conferences.'
"Visitant' rounds" were fairly constant across sites as were "h spital
conferences," with Site 1 having fewer ,student attendees. Overall, similar
patte prevailed for evening activities across sites with servicediffering
in visitant rounds (Site 1 having the lowest of 0.2 percent) and student
conferences, (Site 3 having 6.7 percent; and the others ofr2 or less percent).
"Surgery activities" tended to occur primarily dyring the morning
.
'
rotations as would be expected. Evening surgery did not reach the level at,,
Sitesl and 2 as did Sites 3 and 4. However, at the latter two,.,
sites, the
nr
surgery was primarily done, not by faculty; bueby residents; and students on
these rotations were encouraged to assist them. {Upon questioning the students
stated they enjoyed both the'experience and the responsibility assumed).
The number of students on these clerkships was 4 (as compared with 10 and
11 at Sites 1 and 2), and this may haves contributed to closer relationships.'
The evening hours we?- -Without the structure common to the morning routines.
-
Therefore, more time was'spent'reading, going to x-ray or labs (in- transit),
having coffee/meals,orjust sitting around talking or doing personal errands
(a trip to the-W-11< or to the library). Unscheduled activities prevailed, with -
more,patient-admitting (all sites) and patient followup (Sites 2 and 3) than
during the day. )This generally occurred on the general surgery and emergency
room subrotations (s.ee tables in Appendix B).
.
rt
11
AB

. I
"In 'patient-contact,' whit levels of responsibility, areaercised and With whom Ifaculty; house staff, nurses, others?"
The summarY-Tika des'cribe morning and'evening rotations for each site
and are presented in tabular form in Appendix C.
It_was found that at least 60 percent of students' "patient-contact"
was spent performing the admission/follow-up activities (ranging from 64 roent
at Sjte 2 to 91 percenfat Site 1). Activities in "assistance" "observing"
were constant except far, Site 2 which had a higher perc-. --agin these
./categories46This was possible due to the hig tuber of clerks (10) on this
service and their having greater oppor i'ty to "watch" house staff rather
-than "perform.* Site °3 had a higher incidence of "performance" since there are
no interns at this hospital and students fill this role quite readily.
-----1--,Efforts were madee determine with whom the students interact during
the "patient-contact" acties The next table presents this information.
The vast majority of the time was spent with house staff; with house officers
and facility accounting for 100 percent of all the-supervision, discussion, etc.
with students. At no time was any other person (i.e., nurse) observed in
Athis ca-Patity.
Patient Contact
HOUTS of Contact With-,--
SITES
1 2 ,3" 44
Faculty 11.00 11.75 1.56 4.00
House Officers 59.25 58.50 18.00 11.25
Nurses/-
0 0 0 0
.Others 0 . 0 11- 0.
Student Alone...--
TOTAL HOURS
* 18.7 45.50 36.00 15:75,,
\
89.00 115.75 55.50 31.00'
I
, .

12
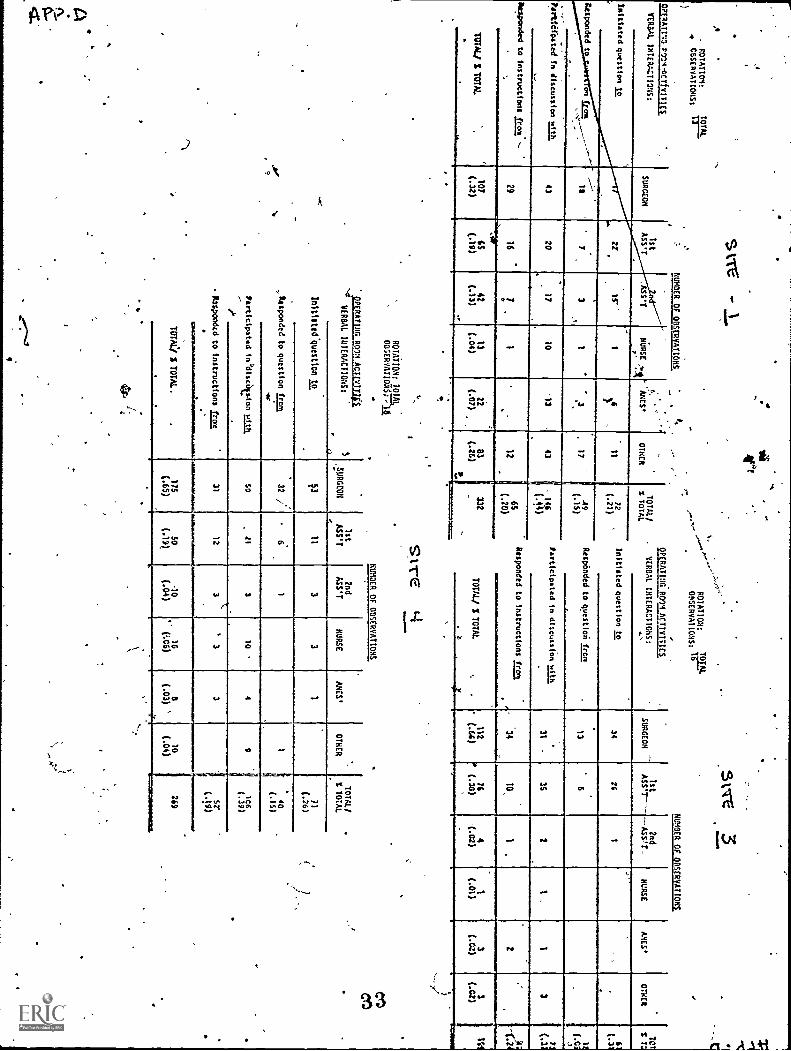
"Whaf-guantity and varieties of verbal interactions occurred
in the operating room ?"
\\,,,
The purpose of collecting these data was to examine students interactions
in the operating room. Were they included in discussions of procedures,.far
anatomy, physiol9gy, or were they ignored? The tables in Appendix D
present the cumulative totals of all operating room interactions which were
observed at the four sites. Interpretation is difficult and individual
criticgl incidents are much more meaningful to faculty. Many variables
tenet° interact to make this situation of value to students. It was found
that individual personalities, the patient's problem, number of persons in
the room were fattors that tended to make the situation rather unpredictable.
I certain instances, howerver, consistent patterns of behavior were found,I
:.such as. the surgeon'who consistently fajlitd to note the Presence of the'
,
-clerk. _Other surgeons not only were aware of the medical student's presence,
but actively engaged in a lively oriented discussion to familiarize
the clerk ith the marry facets of the simgical intervention. Dependingdon
various factors, students also. interacted 4ith the residents, and occasionally
with nurses and anesthesiologists,
13

Study 2: Task Analysis of Medical Studentt.44ctivities on Core '1-frgica'S,Clerkships
The second component of the surgical clerkship study was an analysis of
the'tasks and activities experiehced by third-year medical students at the
four training sites. Its objectivewas tQ describe the 6pes of experiences
and the students' level of participatioriin the activities.
Instrumentation 4
\\The general surgery taskjnventory of 319 ?iems,preliiously used in a
house officer survey, served as the model for the data collection. The
six clerkship directors Were asked to select tasks which they would expect to
be experienced by clerks during the two-month rotation on their surgical
C.service. Within this list, high priority tasks were designated. Following
final individual review of the inVentoryty the clerkship directors, they met
as a group with thy Clinicall coordinator and the authors to determine the final
1
_ item selections. The criterion for inclusion was the appropriatepets of the
task for medical students at this particular phase of their educational
experiehce, and 200 tasks arid activities were'-identified.
A second consideration was the description of the "level of pafticipa-
tion" of the clerks in each activity. At the group meeting, it was decided
to use the following descriptive categories for the tasks: np experience;
NNonly observed; only assisted; observed and assisted; observed aeld performed
NN
with supervision; essistedsand performed with ,supervision; observed,
assisted and performed with supervion; performed with superviSion; and
performed without supervision. For another group of activities sucWas
"attending grand rounds" and "presen4ng reports in conferences" the, two
responses were "experienced the activity" or "did not experience the
activity."

14
The revised 200 item inventory was distributed to the clerkship directors
for their critique and approval. Based upon their comments a final inventory
consisting of 196 items was evolved, the content validity of which had been
ascertained by the subject expert consensus--that is, the persons who were
directing the educational experience.
It should be.str ss d tth the purpose of the instrumentwas to describe
the overall clerkship activities and not to assess individual student performance
or to compare training sites. The emphasis was on providing information con-_
e,rning the breadth and depth of the surgical clerkship experience without
the implication that the clerks should have performed or had contact with .
all the tasks and activities identified
Figure 5 and 6 present the cover letter and a sample page of the inventory.
L.--The inventory was distributed to each 6T -the medical students who had been
- ..
assignedvlto surgical clerkship rotations in the period.December 1, 1974 to
January 31, 1975. This incldded the one monthl'n which the observation stiAly
was completed. The same inventory was given to the students who had served
on the surgical clerkships from February 1, 1975 to March 31, 1975, and
April, 1975 to May 31, 1975, and was completed during the final of their4
clerkships. The students recorded,their responses on optical scanning sheets
and were given the option to remain anonymous, and to write suggestions fdr
improvement of the clerkship or any other comments they could off6r. The
optical scanning sheets-were then computer-processed to provide frequency
distributions for each item. The subjective comments were transcribed and ,
the data analyzed for each training site for.e ch rotation.

Student Particpation
Of the 91 students assigned o the surgical ckei<ships for the Ihree
rotations, 77 returned completed inventories. Twenty-two were from the first
0. rotation (32 assigned), Rwere from the second ,rotation (31 assigned}, and
assigned).26 were from the third rotation (28 asslgned). The observation study was
a factor in lowering the respopse in the first rotation, especially at one
hospital. In spite of ine fact that medical students were told that they
were not being eValutted, during the last week some of the clerks at Site 1'
failed to complete the instrument. The number :of respondents from each
site for each rotation is presented in the following table.
Task and Activity Inventory Respondents
OspitalSite / Rotation 1.
12/1/75 - 1/31/ 5
Respondents Assigned
Rotation 2
2/1/35 - 3/31/75
Respondents Assigned
Rotation.3
4/1/75-5/31/75
Respondents Assigned
1 5 12 10 11 8 8
9 12 10 11 10 11
3 4 '4 4 3
4 4 5 5 5
TOTAL 22 32 29 31 26 28
Findings
The diversity of the experience reported by students at each of the four
training hosRitals Was very apparent. This was reflected in both the number of
experiences and the degree of involvement. A profile was identified for each,.
hospital site which was consistent throughout the three rotations of data
collection.
i 6

16
It,was anticipated that certain activities would be experiehced by all
students in all hospitals. However, the only one which was indicated by all
77 students was participation in special "student conferences." All but two
persons mentioned they had conferred-with peers or physicians regarding
patient-agement. For instance, there were a few students who had not ,
participated in teaching rounds at three of the sites; at one site two students
had not engaged in work rounds; and nine Students did not attend grand rounds
at one site. More than a third of the clerks indicated that they had not been
c-
given opportunities to suggest topics for classes or conferelies and only about
half mentioned that they'had presented reports in conferences. Ten percent of
the clerks responded that they had not read or reviewed general medical 'litera-
ture during their clerkship and thirtypercent indicated that they had had no
expeiience researching the literature regarding a particular patient's problem.
Mostof the items referred to specific tasks and to the level of particiPa-
,
tion in which the students engaged--from no experience to performance without
'supervision. There were no tasks in which every student repoked performance
without supervision. All but one or two ,clerks indicated they had performed ,
unsupervised the ophthalmoscopic and otcadpic examinations, auscultation of .
heart and luK.Q1 fields, and palpation of pulses. _Eighty-three percent/students reported they had, obtained and recorded medicaysurgical histories
without supervision, with the remaining studentstindicating they had performed
this task under supervision. One student's experience with the initial physical
examination was limited to observation only; the rest of the clerks actually
.performed the examination, with all but eight doing this Unsupetvised. Five
students reported they had had no experience in taking vital signs at any time
in their clerkship. Four of these students had been assigned to the same train-
ing site and represented, all th4Te rotations. With one exception, the otherNN,
clerks' ocompl-ished this task with no supervision. .

AThere was reported liore direct and unsupervisdd experiences in bask
involving physical exalt nation and work-up,.interpretng laboratory results
evaluating signs and symptoms, and patient communicati6n, and education. 0
Three-fourths of the studAts reported they had answered-patients' questions
and informed patients of prOcedures without supervision. Most of them
indicated experiences reassuring patients, explaining mtnor surgical
procedures, and instructing 'patients in care of their incision. However, /
about a third reported no experience in counseling the patienetfid/or the
family regarding a terminal illness or counseling related to a ptychomatic
complaint:
Among the six broadly defined objectives for the core surgical-Oerkship
was the acquisition qf coihon psychomotor techniques. Diagnostic manual.
skills 'included lumbar puncture, tharacentesis, and arterial puncture;
therapeGtfc manual skills included intravenous cut-dowh.and cardi.ac resus-..
0
citation; adjuvant manual skills included -nasogastrie intubation and-bladder
catherization. The responses to the task gems 'related to tt4se skills
revealed that a significant proportion of clerks at,a'il sites had had no
experience whatsoeveh with these skills including observation; 43 students
indicated no experience with thbracentesis; 37 had no'contact with an infra-.
venous cut-down; and 27 students responded "no aperier46 with external
'cardiac massage. From two to nine students indicated no experience.with)-
venipuncture, arterial puncture, catheter insertion, Bladder catherization,
nasogastric intubation, tracheal intubation and protpscopy.
In the observation component of this investigation, it was found that
operating room activities occupied from 17 percentto 27 percent of'the
clerks' time. However, there were many surgical procedures with which most
students reported limited experiences. These included aspiration of breast
cysts, hemorrhoidettomy, vagotomy, hiatus hernia repair, vein ligation,
adrenalectom', and pancreatiocoduodenectomy. Specific items concefning

participation in lung, cardiac, esophageal, urologic, spinal c. d; and ophthal-
,
Szologic surgery for example, revealed few students had beenin olved in these4-
procedures other than observing, and many - indicated no experience.
Limitations
The accuracy of the, ttiCients' self-reports concerning t ose activities.
which they had expepeenced and'at what level they had-parti ipaied, is
difficult to determine. In several instances, the validity of the responses
was qiiestioned, p rticularly concerning the performance of certain surgical
` procedures. For/example, two students indicated they had erformed laparasopy
without supervision, 10 clerks reported they had prescribed medications
#,
unsupervised, and 2 indicated they had petformed aneurys ectomies under" -
supervision.
Since These were retrospective observations and co plpted anonymously,
cheCking was not possible. The critical factor was not the identification
of these possible "invalid" or "inappropriate",inciden s.Rather,the emphasis,
was on the overall profile of tasks common across the our sites. Such profiles,
:did emerge which werd`Gansistent throughout the three lerkhip rotations, as
a =1",
well as unique to each.
19 .

Discussion
These studies were-directed at the description of the four surgical
core clerkships through the regular activitie of third year_students, %
assigned totheM. . The intent was tocollecCinformation which would define
the experience in terms of:
- What the students were-doing
Whe7F7tiiia_activities were being done
-- Where they took placer
- - And with Whom the students were interacting.
Clinical core clerkships are a,dramatic change in the educational activfties
of the medical-student. `Learning, quickly becomes a more personal responsibility
without reliance or guidance from "cognitive testt;" it is more epis" and, .
the product of interactions with patient's, interns', and visitants; and-it tends0'
to be relatively unstructured without the core of information so readily
identifiable in previous instruc,tional situations. The "clerkshig, depending-
upon the motivations of inaldual students can either be a- very good, average,
or very poor learning-experience. However, since not all the responsibijity
should be the students' exclusively, what arethe characteristics of a "good
clerkship"? What shOuld the medical students be,expected to doand/or learn
in these situations?
At the CWRU School of Medicine, the goals and objectives of the core
surgery clerkship have been described-and implemented to varying degrees -in
each of the four services. With this as a starting point, research efforts
were directed toward the determination of the degree of discrepancy,if any,4.1.
between what faculty thought students were doing and what was actually
occurring. The rationale for this approach was to categorize questions about
the purposes and merits of students' activities prior to the introduction to4,st
any "change" orientation.
201I

20
AAny exomination of the clerkship as an educational pursuit must begin
with the premise that "divgrsity" is commonplace. Na ply do vatients
differ, bbt also hospital routines, attending faculty, interns, residents,
and others. Such diversity, however, 'should not be equated with overOelmina
disequfl rium. Students-have, and will probably continue, to TearriT-to
professionalize,*and to become practitioners oimedticine. The critical concern
is whether there is sufficient guidance system, to facilitate the students'
development toward these ends. For example, should students know what toA
expect on a clerkship beyond the schedule of nights on`Ynd off? What compe-
tencies are to be evolved? What services are they to render and under whatF
circumstances?. Undoubtedly, many such questions prevail across clerkships.
However, since each site is unique, each must work within its idiosyncratic
constraints. Students learning on a service without interns will probably,.
have greater respon'sibility and learn more through experience than cervices
with interns. Services with male and female. patients will provide mored 4\
learning exper;ienthan those with only,males. These-characteristics are
' to be buit upon es much as posSibltand to' do this, data about actual
activities are of value.e
The data from more-than-a thousand hours of observation and.self-reports
of 27 medical students have Oovided a substantial base of descripti\e.informa-.
,
tion about the commonality and ,diversity of experiences across the four sites.j. e .
No judgement as to the "quality" of the experiences has been undertaken,as yet;
rather, questions about students' activities have developed which have b un
ia process of examination to determine if such experiences are consistent or
inconsistent with good educational planning. Among the major concerns
,identified thus far are the following:

C
* What is an equitable distribution of time across "patient contact",
"structured activities", "surg ", and,"unstructured activities"? When
does an area become Overemphasized (greater than 30% per category)?
* Should' the stuaents be "peric-aing" so much t area of "patient
,' contact'; without direct su*rvis.ion? Who is available to-identify (and
correct) constant errors which may be occurring?
* Wt are the purposes of conferences? How are topics determined far
discussion. Should students be:given greater roles in selection?
What should faculty roles and responsibilities 15e, relatiA to the
medical clerk?
* What procedures should all students learn? ,Are there any at all?.
* In the 0. R.,what are the instructional possibilities? Is it merely
a passive situation or should more active roles be ascribed'to clerks?
Many other-questiont have evolved. These istudes are a beginning of
a systematic examination'to'deTermine whether learning under the circumstances
of the core clerkship can b0441timized. At minimum, can the potential_of
r
the experience be more early delineated so that students can have a greater
understanding of wilat they are to learn, how they may learn it, and thole
eas for -which they and accountable?
I
a

rr
J
"
SURGICAL CLERKSHIP STUDY
SUMMARY OF MORNINGOBSERVATIONS
ma
.
-ACTIVIM,CATEGGRYt
.,..
At
.er,,
IA
A. hrs
0 14e
.-------/
At
1A hrs
gt L vL.-11
hrs.
At
'
C2
,
4Ars.
Q hrs
- %
Q2
A hrs
B hes
A%
131;
A hrs
.,.............e.s..=.
I.
Patient Contact
AdtOttfn;
**follow-up
,
Subtotal
_13q,001
(53.25)
,..1
i.
Ill
2
S.8
2.2
1,31
.00
.%4
i44 2.5
131111
.....i72.1))--...
14
I{r
9.50l
i ,....,..t2
0,1.
:1
12.1
_nW5.)-
4
20.2
.17-
19
(1!4.75)
20.9
'(152.25)
.1
L..
gl.
Scheduled Cv-oa, ActIvIt
es
-*'
Vork Pounds
visita-R-Noun s
'''
lidspltal Frulds,
Student conter
ex%
n)
9.2
.
-T7r----.7-
10.50
2,00
3.3
ft]
_.L.7......__4_51-24_....
INCEP
lin;
---6
p..lo
19
_Sp.
(.151._
m._
Ra.0
it
17.75 )
4.4
g8
1L.17-2.51:___
-1174
28.3
024 (74,51.11
D .
o;
it*
.i0.2
'
11
/1.2L/
Subtotal
.'
19.3
(39.75)
284.4
(3211aL
1e.8
173.00) ._.2169.50),
,..... __
III,
Surgery o. a.
also
-74.0
65_21
10-1
'
1!)...501
MIL
EV
Pre/Post-0p
11.00
0.
.5
1.1
1.75)
.00)
(197.M._
:.3
0.0
12.2.
1.;
q__.5.7...q._-..
O.
2t
9.75)
(46.25)
30.1
1(210.25)
Vatting
0.1
.
.25
2.(
.0
\_3.5
.0
34.4
(715
Subtotal
26.1
(51 23):
21__
IV, Unachtdaled Attly Cles
10
5,3
.A.9
'
o;
0.2
.
J-7
. DO
R.o
1c
.1).2)
142(11/%5)
-tft
-Tra
ns.
:
16.00
-67-00)
2.:
}2R.001
lel
...6..01
1.25
...........,
7.00
(---1-725
1Qo
2.2
1 1.3_5a)---_
8. SL
6.
143 7c)
.2
0.3
'
1( 6.75)
.
Heals/Cott r
(15.15
4.7
-LLB)
'1Z25.1
6.2
sleeotno
Errands
1.2
,50 o
0.
2.29
1.1
90.9
).00y
Q 4
00.3
Ij
6.c192_____
Miscella
ous
4 2
t4.2
.0
2.9
( 3.25
86.
'
1 4
'
Subt
24.4
°(50.50)
24.0
....
...___
NIM
MO
NS.
/100.0
-(63.75)
,..........12.1.5......,,,..=.0.1.251,...______31
100 1
038.
24.7
1
(172,Z5L.
.
per
.....
.
to
o
eo
TOTALS
% hrs.
.
1J1116,11/11
62.8
11.
,-
65.9=MIMI
6..4
.
% tOta
hrs. observ.
411
z1.
...
..,....-
1111111111/111
MIMONIONIMOOMMIUMOONMS
Fr
4
. . -

Date
January
14
II
III
V
VI
17
HOURS OF VHCORRIT ORS
Pedi trics Psychiatry
10;25
0 9.75.
10.'00 - 10.00
18 11.50 12.00
21 10.25 8.50
22 11.75 12.00
VII 24
VIII 25
Totals
.r
10.00
9.50
'86.75
8.75
9.00
80.25
ADMISSION OF THE PATIENTHistoiv/Pnsicni 'axamProceduresDiagnostic (lab tests)Therapeutic
P4eparation of the RecordChart reviewPhone callsOther sources
Uriting the record_
INDIVIDJAL P;TIENT FOLLOW -UP.Sol-oz.:ea ::lszoryipnysica.
ION PER SERVICE
Medicine. Surgery ,OW/t-yn
12.75 -11.00 10.00
11.00
11.25
12.00
11.50
10.50,
12.00
13.00
93.00'
9.0d 12.00
10.00
9.00
12.00.
12.00
12.00
10.00
85.00
P160t2i-
5.5
8.0,
.10.75
10.00
8.50.
.8.25
73.00
exaraProceduresDiagnosticTherapauric
Record keepingErrands (perfo.ming-acarrier or _secretary service)
SCH,p--tROUP ACTIVITIESAor.- -ounds Lrt..sioents,
etns, st::.!ents)Isitant/attenaant rounds(visitant, resi.lents,interns, stuuenzs)Hospital conferences (allpersonnel)Stugint conferences
UNSCHEDULED CROVP ACT:VIT:ESStuaent with. rest. ent
internvisitantnursesocialpeersothers
Activities werework-r4lated
--othor
service
ADDITI=1- ACTIVITIESOff-ward procedures
SurgeryOther special
Readi-lsIn-transit (site to siteMeals, coffee breaksSleeping'Mrscellttgous .
24
Observer
Date
Student ObsCrved
Area Assignment
ADMISSION OF n PATIENTMr-tory/Physical ExamProcedures
Diagnostic (lab tests).Therapeutic
Preparation of he :cord*Chart revicw:__Phone CallOther sources
VrItinz the record
ec0
.4P. 0.4 1.1
20
M<I
I. W0 0 0C. .01
INDIVIWAL PATIENT 1.0:1.0.:41'
:elected hiscsry/physicalexam
/(54:!vres
- ensue
111-rap6tfcLace:.'. 1:ctFf.:;
Writing. order;P.rozrcts notes
Errands (perforJir7 carzte---,or cecretarirser cc 0
-$CUEOCLED OS3 ACTIV1TfVolk rot'. (residents. In-terns, tudencs1his .ntiattendcnt rounas
,"( sitabt,'residencs, in-ernststedents)_Hospital conferences (allpersonnel)Student conferences
___JVIISC1tEDLE6 MAT ACrIVITiSS
Studena withresiiicnt
intern_ -
visitant -ralcse
soda) servicepeersothers
Activitics werework-related
-Pawl
-LIZIIIONAL ACTIVITIESOff-ward pse.edviesSvkZeTY__Other special
Itradiot
lo-tiaostt to %ttst)
Itzal, coifs. Ds..A.::
SicepInit
HiscellAscou,
d MO 2m aO N 0d V0. 0.00 2 *0W 0 0a O0 X X glmu
W ,a44 0 00. o e e
4-teuze
. ,
//.
For ind4vidual observotl -code
participation in activiAl'=
,a .performingWactionb assistinW in fun:tionc observing fuhetion
0 0a a 0O ... V-0.0 2 0
70 v %I
... .C.) W1.1 0 0 0= U
Uail. 4. mO 0 0 00.° e e e
00I
0.e 5:...e:C1.. ;It
U UAO 0 0 0'
Co
.a.-
I i . I
II
, 1_21
t
IE]
25
.1:_-11-.±-E-1 LEM

4
. .
ie
Observer udent Observed
Date Time In O.R.
1st 2nd
STUDENT
InItlat Question to
tesponds to Question from
Participates in discussion wit
Responds to instructions from
Participation Code
i. performing functionb, assisting in function
c. observing function
1st 2ndSurgeon j Ass't. Ass't. Nurse, Ancsth. Other
Iist 15'j
2nd 151,
0
;4
ra
3rd '4th
Ej
STUDENT
MedicalStudentsThee Present
I.24'
3. -
4.
* * *
1st 2nd
Surgeon Assit. Ass't. Nurse Anesth. Other
e InItiafes'Question to
Responds to Questi;!,h from
Participates in discussion with
Responds to instructions from
MedicalStudents -Time Present *I 3rd 1.511
1.
2.
t
4th .151.44
1.
2.
3.
4:
26 .

9
.ACTIVITY CATEGORY:
At
82
11t.
is
SUR0I101. CLERKSHIP STUDY
i_SUMMARY OF OBSERVATIONS
t-.r
e 2.
s a
S.
.
,
A brs
AZ
A hrs
At
A hrs
'0 hrs
et
15 hrs
zff=
1,07
01~.
exm
oa-
A hrs
At
0 hrs
Ot
1.11
Patient Con(ect
Follow:1g-
31-1
/i4-9?)
1,
Adnittlrg
36 3
/26.9
-Subtotal
114
SCheduled Grcup Activities
York pounds
.Visitant Rounds
Hospital R.-40WS
1
40.
0 hrs
et
=Z
s
2 0/
Student Conferences
ri
/s.6
Subtotal
15.0
24.3
111.
Surgery O.R,
Pre/Post-O.
valtind
410
1Y.
UnsEhe led ctivities
Read! 9
j,
11.1
In-Trnsft
2.7 "w
)7.2
0.14
1.2
070.2
0.2
.510.8
0.1
otal
17.7
L'
8:7
Ax,.
2
..50
0.5
1.r0
7.4
.50
Neal /Coffee
Stee:Ina
-Err nds
-MPS elianeous
16.Er
A hrs
et
aN
o.
L25
(13.
00)
3.1
1.5
-
2:75)
1016-
TES
'a
r(130.25L
22.1
(4o.-oo)
74.7
.7
(56.50)
22.1.
(7 3.00)
5,$
17.3
1.8
17.751
6.1
( 2.50j
"
0 ,
:1:
1,
3..L
5q)
1.0
;14
.715
-.50
).-3
9'
(31
. 0 0
)
5.75
)
28.7
(291.241
6 4
(
2.!
17!
74)
29 cg)
7? 7c1c.,
(27.
00)
214.
t/7--
1/44
.50)
21.5
1 2.2
/(
19.2
(Is
00)
'7'4)
1.75)
1,3
11
sg)
-2.9
_150.50)
.30.7 ____15121
23,
Subtotal
----,.-2121994221-1-
26.8
Zr
mI
100:0
TOTALS
.119totalobserv.
Observed
10Q,0'
(319 00)
100.0
,
.%
.31.4.
,326
i-
L'`D
6:1 /.
,
10. 0)
8.3
3.251
'1.1
11.0Q
8.8
1,50
( 7.
00)
0.
2.001
16.25)
/5)
0.3
(.s
o)19
.1(35.25)
10.0
2.2
7.0
0.8
0.8
(.716-7.51_
(77 15)
71 8 25
(7.751
9.4 .
(35 )
8.o
(7o.00)
100.2
1184
0100.0
17.8
18.7
330.50
100.0
..
.
184.75)
8.o
28.8
100.0
100.
0
(RI 75)
(2.9
1,24
01-
(lot 5.25 .1.
.I
3 2

( ACTIVITT-1CPACCRY1
I.
Patient Contact
Adsittina
a Follow-uo
.,
Subtotal
It.
Scheduled Ottess Activit
--
,''
Rork Pounds
Visitant noun s
Hospital Rrulds
ft.^
-"`
-'
SURGICAL CLERKSHIP
STUDY
SUMMJ\RY OF MORNINGOBSERVATIONS
A. hrs
0 hrs
A% it
it
0%
I A hrs
n hrs
7334:o01-__
20.2
151,251
23,2 )
30.Q
Q28.3
(.74,5111
At
02
=======*==m
ilofrs
4 hrs
At
A hrs
02
11 hes
Student Colterc ces
Subtotal
(39.75)
2.2
J3-J
00
12.1
(14.75)
4%
A hrs
1,
LI
1(
1 51
. 25)
2814
(322151,
18.8
12001
52,50
1.00 (51.):
-74.0
0.
_165.15
.75
Li
5.p
21...2
(71.50)
l3_t
X50 5
.00)
34.9
39.7 3
0.0
22
,
30.1
(210.25)
IV.
Unsched.ted nett..
Readino
Irt-Transtt
PealstCoff
Sleeping
Errands
OuS
Subtotal
per
.4. nn
TOTALS
% hrs.
rrting tlbspry
; iota
hrs. observ.
24.0
(63.75)
100.0
79.6
(261.00)
25.1
57)
_IL.9
1,1
.i.35
0.8
1.2
7.00
1,2
1.1
C17
230.2
0.9
Fri.-
AP-
-0.4
1-11_
(.50)
2.9
C57153
0.1
[22.25)
17.5
100,1
(113
.75)
11,8
_38.752
99.9
65%9
(121.75)
6.3
Li 7c)
0.9
(( 6.251
0.9
6-Q91-__-
6.5
(45.25)
24.7
1(172-75/.
190.90
t4
69.4
j(704.751
,1
r^.

SURGICALeLERKSHIP STUDY
SUMMARY OF EVENING OBSERVATIONS
it
ACTIVITY CATECift:
----
-
So
Patient Contact
At
A hrs l,0 hrs
'
AO
.
it%IArSCWMPanlaWTOMOM
.
hrs
.
0 hrs
A%
Oi
A hrs
0 hrs
.
A%
et
A hrs
0 hrs
al
-a
..
A hrs
O r
rom=========
.-
=1=7.a
*
.,171..,5____,__
.-4,
-9
--8
ej,at:___-__A
U-431---
Ili(h
iTo.so
'
elkigi
Aimittlno
.1.11..u,
2..3
..2-1 5
...,....114.-
H118i(
.13.:.5.q-:......25
1-UAL-------
514---.==...-..4.545.1
_____45-8
1-(112A0,
Subtotal,
-45.5_
--=====p....--
v4,53.50)
-==..,==.
.41
-....
____116_25)
.
it,
Scheduled Crou, Activities
2.. 50)
4.75)
00)91(
7.75)
.( I.7C
(1.50)
[--..if-2.-----9.
(4.00l
..1...7-4UL.7.51---
1,3,
h_ool
( 2A.:254---
( 25.51),
vork Oct.dis
4.0
( 4.50)
'4 4
3.00
,
1177'01
.....3.0
1.1
0.0
2,2,
1.9'
/ .,
5)L______
(..5.251
Ylsitant Ncuads
0.2
f-.25)
Hospital- 12:on4S
-0.-
0)
? ?
6.4
8.2
.
Student Ccn.erences '
2.0
2.2;)
050
_6,2
11.5
'SiOtotal
===.....LL'...../X4)
8s5
===:-.....__---.._
-...........--.
._,=._.......:-.
di,'
2 a
18.3
8.751-6,7
,
J. 22.20
2.50.-
1.241
1( 26.50)
___.
lit.
Surgeryo. R
.(...245Q)
...---
2,2
014 9
1.1
*
11000i
l.72
0)
0-R
11
).75)
1.0
1)
(ti.52)J
8.5
0.2
L....2.51....a...;
L_.an.l.._7._%____a..n
__/...2 75)
ozo
0Pre/Poct-On
,o0
0.Q
16.0
I-7o(1.0.75),
.Vaitino
.0
7
.
( -1.5o)
sobt?t,)
......,-:...-...............
2.4
1_5.....sol_____2
001IL
.#_.
IV. Unscheduled Activities
Seadillst
inTransst
.La.so
19.o
12..75)
6.7L
9125)14:71'
3.0
.31.00
41419d----7
1_5
A.
1.00l
.2o.7.51
1L-50)-
.9
-5771
4.00)
25).__-____Q-8
'111::It " ,
4.)
.._2
08.6
.so)
0-6
(27.5r
(...2.0
1.2.00
115_,
5,50)
.25)
MeaIs/Coiien
Seepins
Errands
o.
._Lot00
t
.50
.4,50
1.1
.
'
22.7
100
1
.75)
3.75)(15,25)
0.0206
'69..
.00),
0.4I
.00(31.25)
.
3L5
ftlicelle.ncous
.1'
Subtotal
'
43.0
NllnMraIMIIIII
6i
0.
........16,5___
11
(24.5°
If
it
.
2 per
s-F.
TOTALS " % evening observation
35.3
(117q5)20.4
(67.501
37.2
(67.25)
34.1
-
(63.00)
30.6
(310 50)
-
2 total hirs. observ.
11,1
6_7
6.6-
,2
--
-.
.
-
.
,.
-S
T.*
r rIt
S
ROTATION: 8
' IUE GOLO
II I .
NERO
II I_
II'Ex
I IIORM*
I IIP60
`IBURNS
11
CLINIC
1 rrTOTAL
OBSERVATIONS: PLAN360 ' 8ACTUAL 10
3 I 8
2 i 4
3 5
3 d 5 WA5
_ 5111Malliell
8 1 i 1
0
1 I
,01
C
050
44TIME SPENT ,
.75
1111111MWINEI3.00 3.75' 4.5 11.0 31.2.- .50
- .1.00
.
66.00
Patient ContactAdrift ti 6.50 3-75Follow uo 012.25 3.03 i 346- 3.25 4.0 .53 13.5. 3.751 ' i 2.2, i 4.00 49.75II.. Stlid Pup Act's.hA. Kork Rounds fi 6.CC .50 2.50
i1.501 5.5*. 2.5CI I .25 .75 19.508. Vis. Rounds R. 1.25 11111n11111111111 .25 .2.5 1 6.5Hosp, Conf. I'
1 1.00 IA .7z1 ( 3.50
, . Stud. Cont.11 4.00 2.25i 5.25 1 1.C1" 1.7' i Loo 1 1.751 1 1.50 18.50III. Sur er 31.00 8 ,f, 4.25 .50 7.00 55.00Pr. and Post-0 - i .25 i .261 .75 i 1.25ilaitino j .251 I I -
1 a 5 .25IV. Re ing 3.25 2.75 1 1.25 4.5C 4.24.3.54 57.15 5.54 .75 3.251 1.00 35.50. In-Iransst 0 3.00 1 .25 .5d 1.03 1.5. .7- .7_91 .50- ' i .50 8.76Keals/Co f f e.-.----r649-1-1 -Oa 1_2..00 2.5X 3.5 3 2.03 6.29 .25 .753 .601_ 3 .50 r 26.25Side.' .50 ' .75 75 111.1111_11111111 -- 111.11M1.11.111111 ' 3.50Errands 0 .75 1 * IMIIINI11 -1 .75 i 1.50Miscellaneous 3.z5 i. co i 1.25 .2 1-75 .112.2 .50 23,50
Total Hours 79-.50 15.00 126.50 18.7 33.5 12.9. 35. 59.7'--8.00 :6.75 15.75 I 8-..00-:1 319.00
ROTATIOdi NEU
I
0
II
ARESTH.
1 11
ELASTIC
I if
ORTHO
I Ii
ER
t II
PED.
s
SURG.
:It
GEN.
I
SORG. ! TOTAL
II
05SCAVATIONS: PLANNED 2 3 6 0- 0.
-10 0, 0 I 4 i 4 15.
17 534' ACTUAL 6
I 1 3 0 1 - 0 2
10.00M1111.11._..01.50
3 1 2 ' 0 22
13.7'
5 g 46
.
2. 0
10.50i 610"
TIME SPENT
1. Patient Contact
Admitting __mg7.75 .1 0
o mqup
.1E. Sch Gran-K York Round: IN
5
01.5(/
1.25 1. 0
IIM111M119151111111110.110.11111111.1=1111
mNMI NEMZEin 5.21
, .9.
14 Vis. hcund-s
-...,..
e. lit 2-2 .1.11 1.00IIIIMIREMI ,,,, 14. ' 30.00
111. Surgery
N411111111111111111-- 114111111111111111.1111111111111111111111141.111111
11111111IMINEPr. and P.MTrifi
IY. teadIngI 5.75 nilliEl.50 11111 . 0 . Orraithilit
.25
1.00 I. 1.00 111.111Mr
t1 .0.111111[
.5d
-.
40.251.000. 8.25
.?5 , 17.75
.25 2.50
rn1 511
n- 'WS t1:CC ; 1.00 1 .2
Meals /Coffee IMIRM 0Sleeping 1.00
11111111111111111111111E1MEM=Errands MM.IMO=MiscellaneousMiscellanes
3 041191111111TOWTOTAL HOURS112
7.50
MIN6.75
EMIEn 16.00. 150.5
2.50!! 1$.5ff
33.251 330.00
30
0

Srre.
.
ROTATION: .
'o
tIAJOR
I IIH
1
NOR
ItTOTAL
08SERVATIMS: PLANUO I .11., .
S 5' 6 3 25ACTUAL 11 '5 - 5 4 25
Time Spent:
. I. Patient Contact .. Admitting , '1.00 8.50 1..50 8.50 19.50Follow uP
35Dn..
12 nn I arse 4 cn 1 r)4 P.
U. Schad CrotIp Act's.: A) Wirk Rounds
I 9.00
t: ,71
1.50 2.50 11.008) Vis: Rounds 4 2.00 .75 -2.76
Nosy. Conf, 1 1.25 . 3.75 5.00C) Student Conf. 1' 8_25 4.50 6.50 19.25 1
III. furgery1 18.75 . 6.75 , 15.75 : 3t25 44.50
- 1.,fre And Post -0o 1 1.00 . . .50 .25 .25 0 2.00haiting. 4.00
0 4.00_ IV. Tters--19'="-- .1 5 74 74 ) cn M in 6
In-Transit1 .50 1.75 .75 .25
2.00 1.50
1
1
3.25_
11.00Kcils/Coffee 5.00 2.50
Sleeping-1.25. 25.- 1 1
, 1.50. Eftands . .50 .75. .-
. .
.50 :.
--
1 1.75. Misttllaneous . .. 1.25: 2. 2.75
. t f fm I - . 7.80.'TOTAL NOURI.: 72.50' 44.00. .A1.25 23.25 '1 181.00 J
4-
App e.4'
ROtAT101/:. 4
.
. ORTHO
I II 'I I
EA
11
EHT
I II
CV-THOR.-I
11
air.
1
sm.I)
-TOTAL
)3SERVATI04il' PLANNED4 '2 1 0
01
2 5 1 4 27+ ACTUAL4 0 1 I 2 0 4 1 6 7
,---
26rinE SPENT:
1. Patient Contact' Admitting .74 2.25
.40 1 1.50
,.
10.74
.
1.5.75Follow up
II. Scharou-p-Act's.A Work Rounds
4.00'.2.5 3.001 .75
-
1.50 1.50 4.25 '.501 45.75
'-.. ,-
-' 3.25 1.7.
4 Vis Round";1.25 .50 1.00 .50Rosp. Conf. 1 1.00 I 1.50 ' 2.75 1.50 6.75C) Stud. Conf.
aI
.00 2.00 . . 1 .00 11.00111. Surgery ,
1.25 6.25" : 3.7575 3.00 19.25 . 4.00 50.75Pre end Post-O. I 2.50
. .25 1.251 1.2VattingL
. .IIIIIIIF
=MINN1.00
, 1.75
Mgs
IIIA
1.75
It
16.25
.50
1 4
111. Reading.
gs
IIIIITIIIIIMIMMNIM.75
1nTrAnsit. .25 .
heals/Coffee, 1.50 :.1.00 1.25 2.76
Sleeping
allig-Errands_
..5 0. Miscellaneous
1.00 .75 2.50 11.25 1.25 6. o
TOTAL HRS. 2 0 7. 5 8.00 14.50 SMINITIMIMI 46. 184.75
4-P
31

ROI44104:
0fiCR94710051
pAilt
irr Fe
1.1
ti.,?
trat
. OF
RE
SF
OM
MT
I. /T
Y
mission Q>,.
PERFORM
hrs
ASSIST
.
hrs
OBSERVE
hrs
DISCUSS
hrs
TOTAL POURS/
% HO1RS
His
tery
/Phy
lltal
W22.50
2.00
-
.
.4.50
29.00
(.26)
Procedures (eisy/thersp)
',40.
CO
5. /5
,...-.....
.75
' 16.50
(.15)
)record Prepsr4tion
i'75
:50
,..
. 25
)
L.50
-5.00
(.05)
IdrIcing the Record
.,
12.00
.
.75
41.kt....:,J...41,,,A1.
,12.75
(.12)
11c4-up.
ss.
.
Selected Physical Era".
7.25
1.00
.75
1.25
12.26
(Al)
Procedures :
9.75
5.25
5.75
'2.75
23.50
(.21)
Accord Keeping
11.75
o11.75
(.12)
sow
ww
w./N
NS
.;;A
ME
MO
MP
41"
.,
-
110.75
TOTAL NOLAS/
Ti MPS
79.00
'.,
(.71)
15.25
(.14)
12.00
(.11)
450
(.04)
ROTATION:
TOTA
ADOSERIATIOWS:
ATIEliT re
1
ti-e
-2,
LEVEL OF RESPONSIBILITY
64Ission
PERFORM'
hrs
ASSIST
hrs
OBSERVE
hrs
DISCUSS
Ars
TOTAL Howls/
S HOURS
H16t0r5 /Physical Esasa
10.25
1.50
.75
12.50
(.15)
Procedures (dSag/theraP)
.5.50
1.00
1.25
7.75
(.09)
lecord ?reparation
'2.50
.25
1.75
4.50
(.05)
Writing the Record
5.75
.50
.25
6.50
(.00
e.
11w
-up
C.
,
-
..
.
Selected tlySICil ELLS
5.75
2.00
3.00
10.75
(.13)
Procedures
..
15.25
7.00
.5.25
.60
20.00
(.33)
Record Keeping
if.75
2.75
"1.25
1.25
14.00
(.17)
......
04.00
'9-
--._-.
TOTAL HOURS/
SHMS
.53.75
(.64
)15.00
WO)
11.75
(.14)
.
3.50
(04).
i
.
,
ROTATIOM:
;Hog
rom
pvA
TIo
ns:
25.-
,.
.MEM CO:ITACT
LEVEL OF RCM:15181MT
!mission
EgroRm
hrs
ASSIST
hrs
-00SERVE
hrs
OISC6SS
I
hrs
(TDIAL HOURS/
S WOOS
HiStOry/PhySlel
12.00
,12.00
(.23)
FrocelOres (dfag/thew)
.50
.7S
1.25
(.01)
Record Preparation
.75
..75
(.01)
Writing the Record
5.50
,.
5.50
(.16)
Ilow
-op
4elected.Physfc41 Exio
75
1.00
25
4
2.00
(04)
Procedures
c20.75
1.75
50
23.00
(.43)
Record Keeping
-4.00
.50
0.50
(.10)
TOTAL HMS/
1 104145,
48.25.
(.91)
f
4.00
Goa
)<
.75
(.01
).
I43.00 ..._.
Fo1
FAT;EIT ro
ROTATtOII: :
IOTAL
OBSERVATIONS:
7
St-t
e-LEVEl. OF ILEsrONS1011.1/
a
clIsston
PERFORM
hrs
Asstt:'
.hrs
08SCAvE
hrs
DISCUSS
hrs
.TOTAL HWAS/
S 1
13(1
25
History/Physical Exam
9.50
.75
.
10.25
(.36)
Procedures
lig/therap
.25
.
..
25
(01)
cord Preparation
2.50
.
2.50
(.09)
rltng the
Rsc
or1.00
11.00
(.04i
rlow4P
0.
e ected 'hystce EXLM
.
F.
1.75
2.75 .
.25
4.75
(.17)
Procedures
4.50
1,75
1.25
7.50
(.27)
to _ Keeping
2.00
'4
.2.00
(.07?
TOTAL BovaS/-
IS BOUR5
,21.50
.76
4.50.
(.16)
2.25
(.04)
23:25
___
6
S VrE
,
.ROTATION:
TOTAL
SURGEON
1st
Asser
CSSERSATIEAS:
OPERA1 ro:m-acTivITIE$
VERBAL INTERACTIORS:
Initiated question it
2Z
Responded to
on IEFEM
1$
tertlEiOated fn discussion with
43
20
heisponded to instructions fiat.--
2916
TO
TA
L/ ITOTAL
107(.32)
IS(.19)
NUMOER OF OBSERVATIONS
sib
rOPSERvAIIONS:
ROTATION:
IVA-
QP(RAT
TOTAL/
.VER
OTHER
S TOTAL
72
(.21)
33
.17
!nit'
-49
Respo
(.15)
1710
'13
43
i146
(i1)
112
65(.20)
42(.13)
(.0413)(.0t7i)
03332
(.26)
',VERA
VER
POO
Rat
SirtI
404
ltzsoa
ROTATION: TOTAL
OD5ERIATI6471t
tert1
Res
s tTE
3
HUMBER OF OBSERVATIONS
IUGR014 ACTIVITIES
_.
SURGEON
Ist
ASST " -----ASSIT-
2nd
NURSE
AYES'
°TRES
TOT
%13
Al INTERACTIONS:
..,
Ard question to
34
26
1.
61
(.31
Ided to question from
.13
.
5.
I
14
Apated in discussion till
31
-35
2.
1.
13
71
(.2I
ded to instructions I=
,
.34
.
101
.
..
2
.
;41
-1..2
TOTAL/ % TOTAL
4T
112
(-EA)
76
. (.38)
4
'(.02)
1
(.01)
3
(.02)
.
3(.62)
.
I
191
.LAMM
S tre
HUVOER OF OBSERVATIONS
1110 R003 AGTIVITISS
01 INTERACTIONS:
3.SURGEON
ASST
..;
1st
2nd
ASST
NURSE
ARES'
OTHER
TOTAL/
% TOTAL
itequestIon to
§3
11
33
171
(.26)
idled to question from
32
/6
11
40
(.15)
mr
:Ipsted indtscbtion tin.
so
21
310
49
IC6
(.39)
Mod to instructions
rote31
175
(.65)
12
3,
33
52"
(.10
.
TO
TA
L/S TOTAL.
.SO
(.19)
-10
(.04)
16
'
('.C6)
0
(.03)
10
(.04)
269
.,

CI ASE WESTERN RESERVE UNIVERSI.T''Y. CLEIVEL'AND, OHIO 441d6.
. May 15, 1975
TO: Phase 3 Surgical Clerks
1. Cb 01?,e-
FROM: Clerkship Directors of the Department of Surgery:Drs. Frederick S. Cross, Ralph G. DePalma, BrownM.'Dobyns, Kent H. Johnston, James C. Jones, JerryS. Wolkoff
At the request of the Clerkship Directors of the Departmentof Surgery and the Dean for Medical Education,of the School ofMediciae,'a surgical clerkship s.tiidy is being/, undertakdn by the.Division of Research in Medical Education. As, part, of this stuAy,'we are asking yop to complete thA,enclosed task and activityinventory.-.
,,!
The Clerkship Directors of the Department of Surgery hayeidentified those tasks and activities which might be experiencedin the surgical- clerkships. The-informatioe provided by thisinventory will help determine if the surgical clerks af'the fourtraining sites participated in these experiences. This inventorydoes not imply that each clerk will have performed or even parti-cipated in all of,these activities. 'Its purpose-is to assess theclerkship; experience, not the student. Each hospital will be'identified. The'students may remain anonymous if_they do notwish to sign the.inventory. .
Please lase the answer sheets provided to recordyourresponses to the items. The answercode is indicated on eachpage of the inventory. Answer'sheet No. 1 isto be used forItems 1 through 100; answer sheet,fNo. 2 is to be used for Items1.4 through 196. Please return, the answer sheets to'the Directorof your clerkship,
'"If youhave any suggestions for the improvement of thesurgical clerkship, please write them on the blank sheet-provided.
Thank you for your invaluable assistance.
FSC/RGD/BMD/kHJ/JCJ/JSW/r1
chool of Medicine .
epartment of 3urgcry 34

*Plcouraz- January1975
Case Western Reserve Univerity'School of MedicineDepartmentof Surgery
Itr'
SURGICAL CLERKSHIP ACTIVITY/TASK .I4VENTORY
Use answer'sheet No. 1 for Items 1 = J00DIRECTIONS: For Items 1 through 9 answer "A" if you experienced
- the activity 4n your surgi,cal'clerkship; or."B" if you did notexperience the,.activity. 41acken the sliace.under the selectedletter On the anM,/et sheet.
A = experienced the activity. B did not experience the activity
1.- Participate in teaching rounds
Participate in work rounds
44Atteni,grand rtunds,
4. Atpend special student-oriented conferences
5. Suggest .topics for 0assc-eWc-Onferenal
G. Present reports in
7. Read/review etal medidal literature
search literature concerning a particular patient'sor,eblem
9. Confer with peers or M.D;'s on patient manageMent
DIRECTIONS: Use the key outlined belowito report youi experiencein' your surgical clerkship with each ofiCk2,following tasks. Selectthe category which describes how yOu most *EommonIly participated,_Blacken-the space under the selected answer on the answer sheet.Select -
"z's
A = No experience0B = Only observed-. !
C = Only assisted'p = Observed and assisted
= Observed and perfamed:*ith'supervision... Assisted and performed With supervision
G = Observed, assistdd and performed with supervisionH.= Performed with supervision.I = ferfOrmed without sup6Tvision
10. Obtain and recoTd medical /surgical history
11. Mike entries on medical recorcis
12. Plan/modify diagnostic procedures according to patienits.response/need
13. AsseSs patient's general appearance
35.