judith carta, ph.d. juniper gardens children’s project university of kansas presentation prepared...
TRANSCRIPT
When More Means Less: Cumulative Risks and their Impact on Children’s and Families’ Outcomes
Judith Carta, Ph.D.Juniper Gardens Children’s ProjectUniversity of Kansas
Presentation prepared for the Australian Centre for Child ProtectionUniversity of South AustraliaMarch 17, 2011

Except on one specific issue
Australia and the US have much in common and a wealth of knowledge and wisdom to share

It’s been a topic of recent discussion among our heads of state.

Juniper Gardens Children’s Project
A collaboration between university and community focused on prevention of risks associated with poverty
JGCP began in the mid-1960s when residents of NE Kansas City, KS, a low-income community, joined with University of Kansas Faculty to address concerns about child development.
JGCP’s New Home as of June, 2010
The Children’s Campus of Kansas City Multiple agencies worked
together on capital campaign to build a center of evidence-based practice
Model Infant-Toddler and Preschool Classrooms
One-stop shopping for services for families
Evaluation and referral to other family services
Focus on translation of research to practice

+Some of the things we’ve learned about the effects of poverty on children and how to PREVENT adverse outcomes.
Today’s Focus

1. Poverty exacts a toll on children in numerous ways.

More likely to live in a single-parent family
Family experiences food insecurity
Exposed to more environmental risks, toxins
In homes with parental substance abuse, maternal depression, lower levels of parent education
In low quality child care
Substandard housing
Unsafe neighborhoods
Parents much less likely to be employed
Less access to quality health care
Example of common risks for children in poverty
10
More likely to live in a single-parent family
Family experiences food insecurity
Exposed to more environmental risks, toxins
In homes with parental substance abuse, maternal depression, lower levels of parent education
In low quality child care
Substandard housing
Unsafe neighborhoods
Parents much less likely to be employed
Conditions for Poor Children Are Less Supportive
11
SingleParenthood
Poverty ViolentNeighborhood
InaccessibleHealth Care
LimitedEducation
Lim
ited S
ocia
l Functio
nin
g
Lack o
f Em
plo
ym
ent
Cu l
tur a
l Bia
s
De p
r ess
ion
Str
e ss
SubstanceAbuse History
PhysicalAbuse History
Mu l
t iple
Fo s
t er
Pla
c em
ent s
Abusiv
e In
tera
ctio
ns
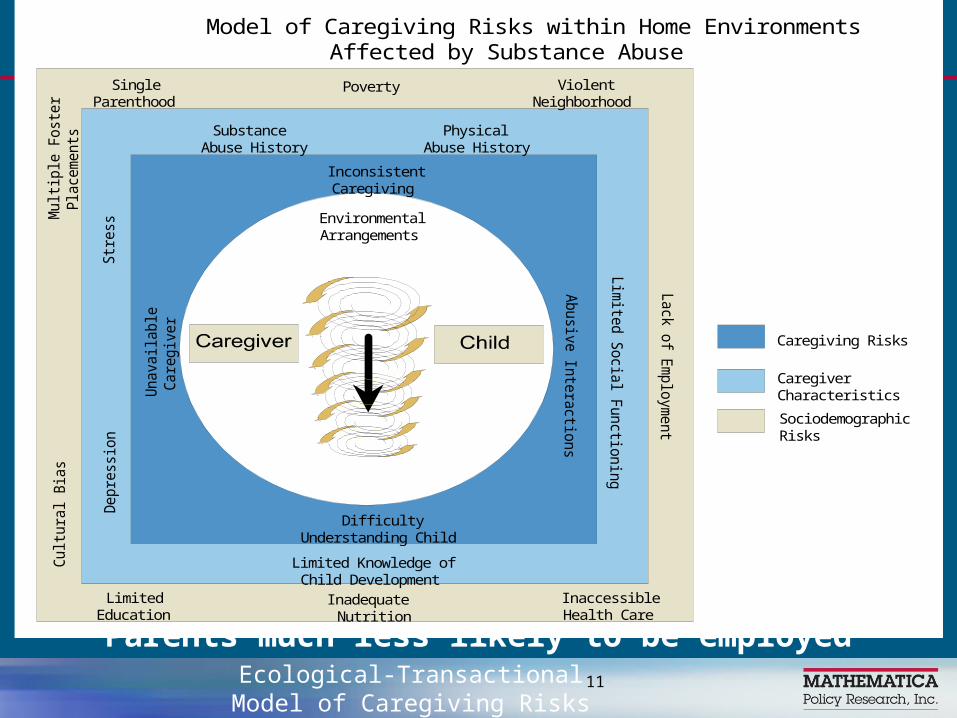
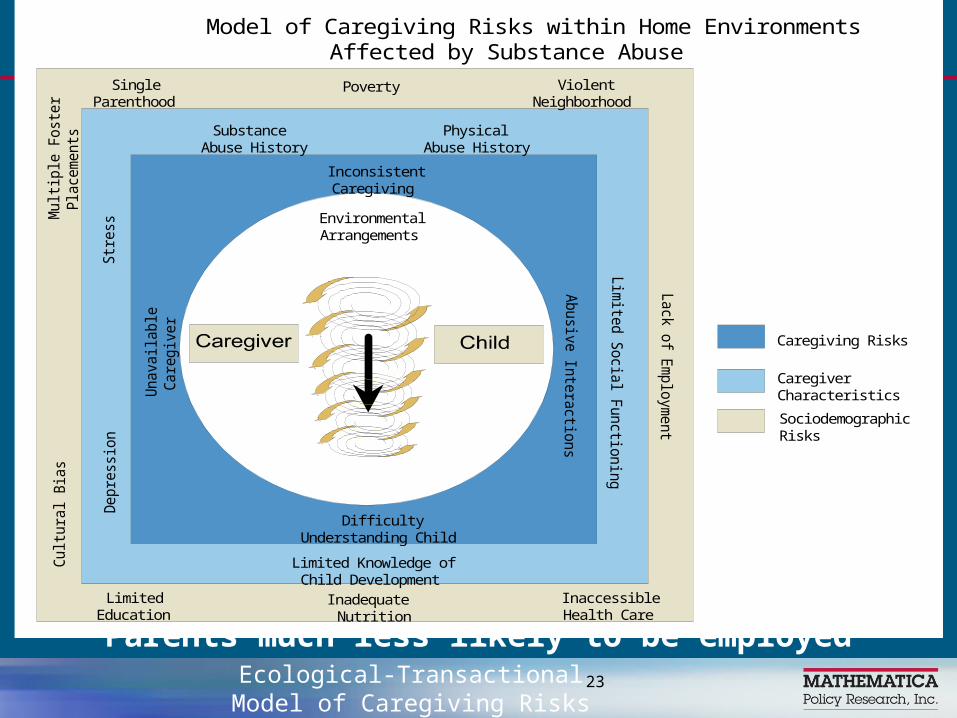
Model of Caregiving Risks within Home EnvironmentsAffected by Substance Abuse
Caregiving Risks
CaregiverCharacteristics
SociodemographicRisks
Un a
v ail a
b le
Ca r
e giv
erInconsistentCaregiving
EnvironmentalArrangements
DifficultyUnderstanding Child
Limited Knowledge ofChild Development
InadequateNutrition
Ecological-Transactional Model of Caregiving Risks

2. The consequences of poverty-related risks show up in numerous areas of development.
Born at lower birth weight Less successful in school1
More likely to show behavior problems (disobedience, impulsiveness) and, when older, commit crimes1
Higher risk of becoming a teen parent2
Experience more accidents and injuries2
Be poor as an adult2
Obesity2
Chronic health problems (asthma, anemia)2
Receive lower quality child care2
Consequences for Children in Poverty Are Really Different
13
_____________
1Duncan, Zio-Guest, & Kalil (2010) 2Moore et al. (2009).

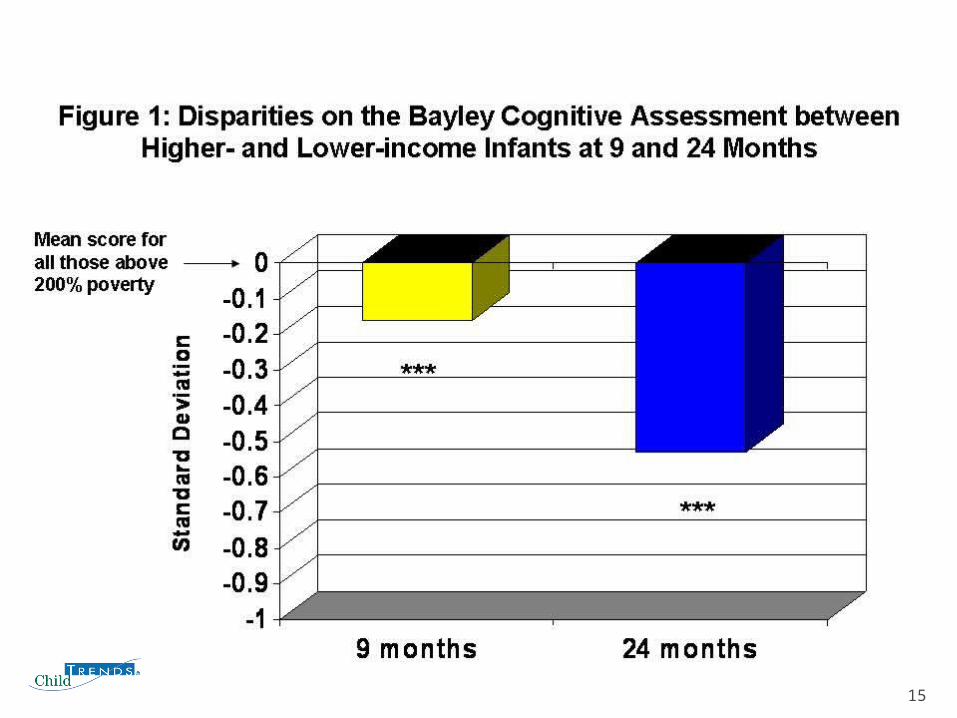
Early Childhood Longitudinal Study – Birth Cohort (ECLS-B)
Nationally-representative sample of approximately 11,000 children born in 2001
Data collected at 9 months, 24 months, 48 months, and in Kindergarten
Current analyses focus on 9 and 24 months• Analyses of the 9-month sample were limited to children
aged 8-11 months (N = 7,400)• Analyses of the 24-month sample were limited to
children aged 22-25 months (N = 7,200)
14
15
3. The influence of risks shows up early and grow over time.
Birth
Early Infancy
Late Infancy
Early Toddler
Late Toddler
Early Preschool
Late Preschool
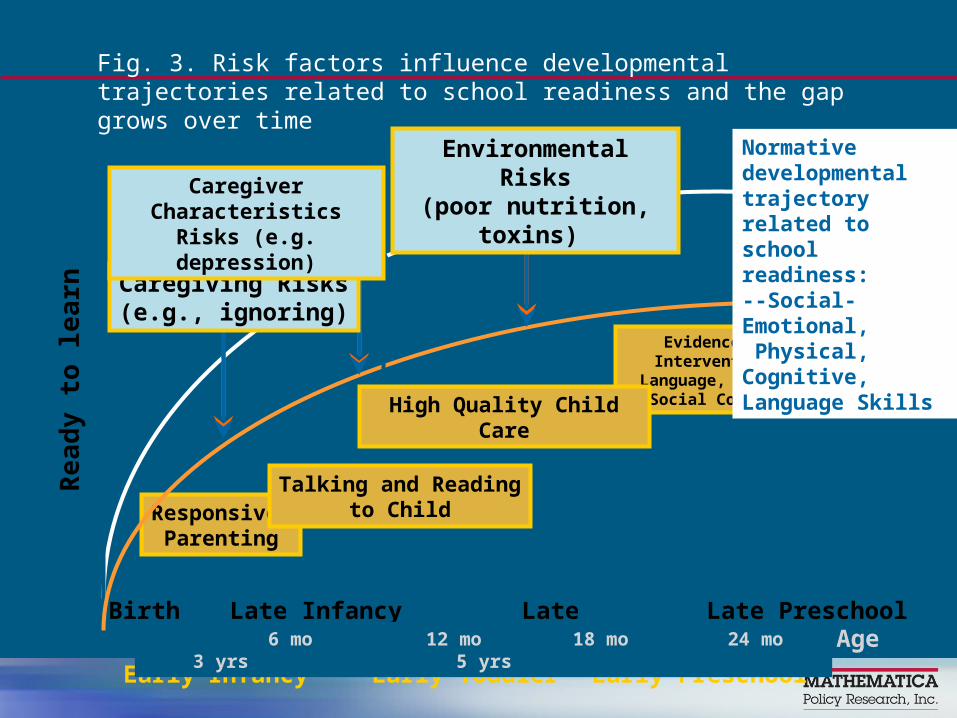
Responsive Parenting
Talking and Readingto Child
Evidence-Based Interventions in Language, Literacy, Social
Competence
Age 6 mo 12 mo 18 mo 24 mo 3 yrs 5 yrs
Re
ad
y t
o le
arn
High Quality Child Care
Caregiving Risks(e.g., ignoring)
Caregiver Characteristics Risks (e.g. depression)
Environmental Risks(poor nutrition, toxins)
Normative developmental trajectory related to school readiness:--Social-Emotional, Physical, Cognitive, Language Skills
Fig. 3. Risk factors influence developmental trajectories related to school readiness and the gap grows over time

4. Risks associated with poverty often accumulate and have a multiplicative effect on children’s outcomes.

19

Relationship Between Cumulative Environmental Risk and Developmental Outcome for High Exposure Group
Relationship Between Cumulative Environmental Risk and Developmental Outcome for High Exposure Group
0 1 2 3 4 5 6
Number of Environmental Risk Factors
86
88
90
92
94
96
98
Bat t
ell
e D
Q
In our study of the effects of prenatal drug exposure, preschool children prenatally exposed to drugs and alcohol WHO HAD GREATER NUMBERS OF RISKS had Developmental Quotients that were further from the norm of 100.

Why is it that we see this multiplier effect of risk?
21

From Lisbeth Schorr:
–An example of how the presence of risk factors and absence of protective factors can influence a child’s outcomes over time
– From Within Our Reach: Breaking the Cycle of Disadvantage
More likely to live in a single-parent family
Family experiences food insecurity
Exposed to more environmental risks, toxins
In homes with parental substance abuse, maternal depression, lower levels of parent education
In low quality child care
Substandard housing
Unsafe neighborhoods
Parents much less likely to be employed
Conditions for Poor Children Are Less Supportive
23
SingleParenthood
Poverty ViolentNeighborhood
InaccessibleHealth Care
LimitedEducation
Lim
ited S
ocia
l Functio
nin
g
Lack o
f Em
plo
ym
ent
Cu l
tur a
l Bia
s
De p
r ess
ion
Str
e ss
SubstanceAbuse History
PhysicalAbuse History
Mu l
t iple
Fo s
t er
Pla
c em
ent s
Abusiv
e In
tera
ctio
ns
Model of Caregiving Risks within Home EnvironmentsAffected by Substance Abuse
Caregiving Risks
CaregiverCharacteristics
SociodemographicRisks
Un a
v ail a
b le
Ca r
e giv
erInconsistentCaregiving
EnvironmentalArrangements
DifficultyUnderstanding Child
Limited Knowledge ofChild Development
InadequateNutrition
Ecological-Transactional Model of Caregiving Risks

The News is Not All Bad.

5. Responsive parenting can mediate the effects of poverty.
We know the qualities of parent interactions that promote children’s
development.
Consistent Warm Nurturing Stable Predictable Contingent
Enhancing Parent-Child Interaction is Critical
But where do you begin?
Parent Behavior Can Be affected by:
Immaturity and inexperience
Low educational attainment
Depression or other mental health problems
Family violence Substance abuse Economic stress Illness

In a Context of Multiple Risks
• Where Risks Affect Parenting,• Parenting Affects Child
Behaviors and• Child Behaviors Affect
Outcomes,
Where do you begin to intervene?

The Prevention Riddle
•What’s the best way to cut through the onion?

More likely to live in a single-parent family
Family experiences food insecurity
Exposed to more environmental risks, toxins
In homes with parental substance abuse, maternal depression, lower levels of parent education
In low quality child care
Substandard housing
Unsafe neighborhoods
Parents much less likely to be employed
Conditions for Poor Children Are Less Supportive
31
SingleParenthood
Poverty ViolentNeighborhood
InaccessibleHealth Care
LimitedEducation
Lim
ited S
ocia
l Functio
nin
g
Lack o
f Em
plo
ym
ent
Cu l
tur a
l Bia
s
De p
r ess
ion
Str
e ss
SubstanceAbuse History
PhysicalAbuse History
Mu l
t iple
Fo s
t er
Pla
c em
ent s
Abusiv
e In
tera
ctio
ns
Model of Caregiving Risks within Home EnvironmentsAffected by Substance Abuse
Caregiving Risks
CaregiverCharacteristics
SociodemographicRisks
Un a
v ail a
b le
Ca r
e giv
erInconsistentCaregiving
EnvironmentalArrangements
DifficultyUnderstanding Child
Limited Knowledge ofChild Development
InadequateNutrition
Ecological-Transactional Model of Caregiving Risks
Do you begin with the outer layers and work inward…(distal risks)?
Or address the center first (parent and child behaviors)?
We know that we cannot ignore the outer edge
Parents who are dealing with survival and safety will have difficulty responding to parent training.
Programs must be able to respond to families’ needs in a comprehensive, intensive and flexible way.

Shonkoff & Phillips, From Neurons to Networks, 2000
We must also focus on center
Relying simply on enhancing family support will probably not improve child outcomes.
Children can’t wait for distal risks to be ameliorated.
Programs that focus on enhancing specific parent-child interactions have greatest impact on child outcomes.
6. Our most promising interventions appear to be those that are comprehensive as well as focused and intensive.
How Intervention Programs Can Alter the Developmental Trajectories of Infants and Toddlers in Low-Income Families:
The Example of Early Head Start
36
Early Head Start Is an Intensive and Comprehensive
Two-Generation Program
Self-Sufficiency and Healthy Families
Parenting
Child Development
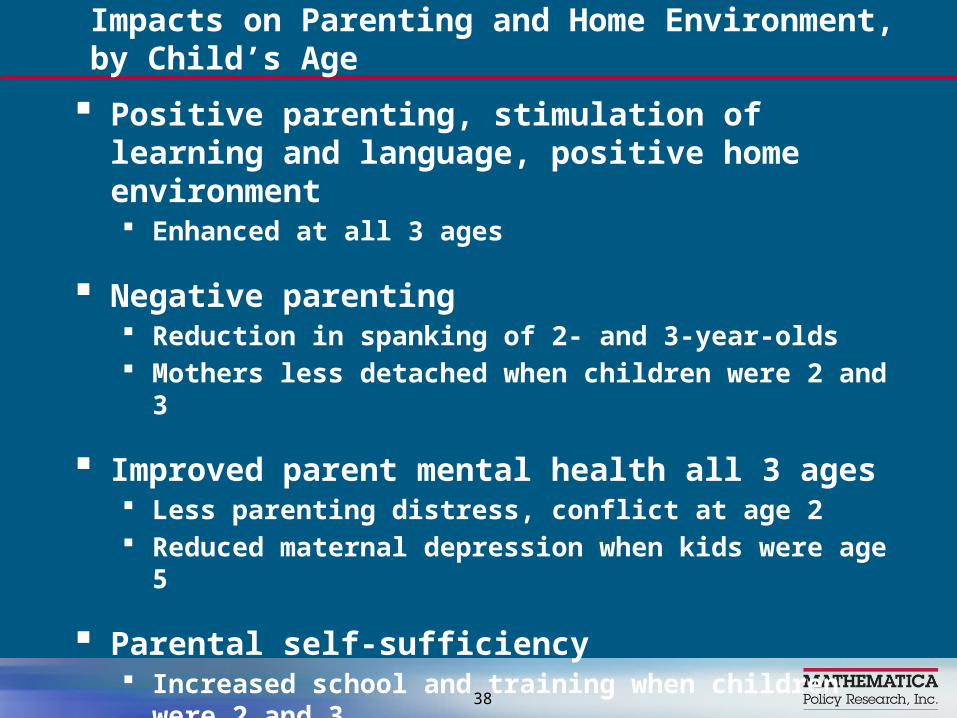
Positive parenting, stimulation of learning and language, positive home environment Enhanced at all 3 ages
Negative parenting Reduction in spanking of 2- and 3-year-olds Mothers less detached when children were 2 and 3
Improved parent mental health all 3 ages Less parenting distress, conflict at age 2 Reduced maternal depression when kids were age 5
Parental self-sufficiency Increased school and training when children were 2 and 3 No impacts on income
Impacts on Parenting and Home Environment, by Child’s Age
38

Social-emotional development Reduced aggression at 2, 3, and 5
Positive approaches to learning Enhanced at ages 3 and 5
Cognitive and “academic” skills Positive at ages 2 and 3 No impacts at age 5
Language development Vocabulary, English speakers at 2 and 3 Vocabulary, Spanish speakers at age 5
Some positive health effects at each age
Impacts on Children’s Development, by Age
39

7. Highest risk families may be least likely to show effects of
our intervention.

No impacts for families in highest risk group when children were 2 and 3 years old
Effects more likely among moderate-risk families when children were 2 and 3 years old.
EHS Impacts by Risk Levels
41

In general, higher risk families received less intervention More likely to drop out before their children reached
age 3 More likely to miss home visiting appointments Less likely to be fully engaged and involved during
home visits
Possible reasons for lower impacts for higher risk families
42
A dilemma: Families who need interventions most may be least likely to get them.
8. Technology may help us engage the most difficult to engage families.

Question: Could cell phones help?
Keep families engaged in a parenting intervention
Keep them from dropping out
Give parents ideas on how to use the parenting intervention throughout their daily activities
Strengthen relationship with home visiting/parenting coach

Purpose of Cell phone parenting project is to see if adding cell phones to a parenting intervention will:
Improve our ability to keep families from dropping out of the intervention.
Keep families more actively engaged in the intervention.
Help families learn to apply parenting skills throughout their daily activities with high fidelity, thus increasing the “dosage” of the intervention.
Overview of Design of Cell Phone Project
Randomized clinical trial testing the effectiveness of Cell Phone Enhanced Parenting
3 groups: Planned Activities Training (PAT) (like PPP) Cell Phone Enhanced Planned Activities
Training (CPAT) Wait-List Control Group

Planned Activities Training (from Project SafeCare©)
A research-based intervention that teaches parents to plan and structure activities to prevent challenging child behaviors.
Family coaches deliver training in homes in 5-7 sessions.
Coaches teach parents positive interaction skills and help parents teach child expectations, routines, simple rules.
Parents learn to engage the child in planning and preparing in advance for daily routines and play.

Cell Phone Enhanced ParentingParents in CPAT group: Given a cell phone and an allotment of
minutes provided by AT&T Receive twice daily text messages and
weekly phone calls from their coach CPAT mothers can use the phone to call/
text their coach and can also use it for other reasons but cannot go over their allotted minutes.
Text Messages: Questions A text message question is sent daily asking
about use of one aspect of PAT, their interactions with their child, or their child’s behavior “On a scale of 1-10 (10 is best), how did a
mealtime go today?” “Did you have fun with your child today?” “What is one cute thing your child did today?” “How did you catch your child being good
today?”
Messages designed so responses can be brief
CPAT: Other Ways Cell Phones Enhance PAT
One text message each day to remind parent to use a specific PAT strategy.
Cell phones are used to confirm home visits.
Text give parents up-to-date information about free fun community activities.

Sending Text Messages
Family Coaches send text messages and receive parents’ responses in different ways On the Family Coaches’ project cell phone Using Notepager Pro software – can be
scheduled in advance and sent to a group Using an email program
Options save time and allow family coach to schedule messages in advance

CPAT mothers demonstrated greater pre-post improvement than Control Group mothers on most observed parenting behaviors on the KIPS (Keys to Interactive Parenting Scale) (Comfort & Gordon, 2005)

Cohort One Data Showing Lower Attrition Rate for CPAT Group
Implications for practice
Reduced attrition and improved engagement of high-risk families may be worth cost of cell phones/minutes.
Cell phones increase ability to stay connected with highly mobile families.
Being able to stay in touch throughout the week can help us to strengthen relationships with hard-to-reach families.

Conclusions: It’s Time that More Risk Means More:
1. High quality comprehensive support services based on evidence-based practice.
2. Focus on providing parents with skills they need for supporting their children’s development.
3. Intensity that matches what families actually need.
4. Coordination and collaboration among agencies that provide these needed services to families.


You know how to get there!
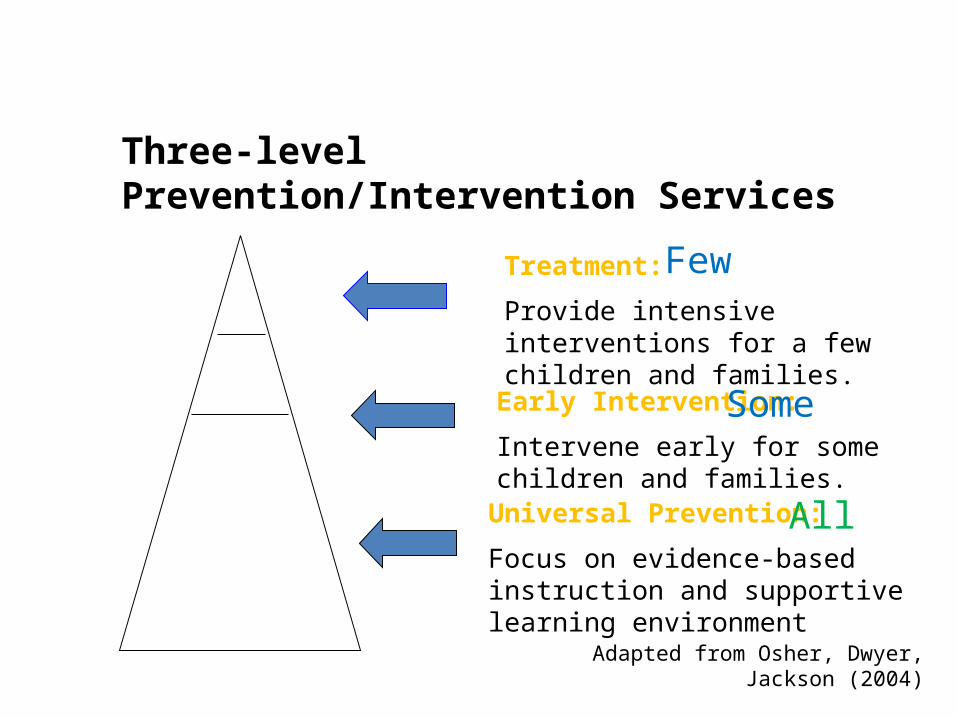
Three-level Prevention/Intervention Services
Treatment:
Provide intensive interventions for a few children and families.
Early Intervention:
Intervene early for some children and families.
Universal Prevention:
Focus on evidence-based instruction and supportive learning environment
Some
Few
All
Adapted from Osher, Dwyer, Jackson (2004)

Recommended practices for improving social-emotional learning (Meta-analysis of 57 programs by Durlack, in press)• Sequenced: Does the program apply a planned set of activities to develop skills sequentially in a step-by-step fashion?• Active: Does the program use active forms of learning such as role-plays and behavioral rehearsal with feedback?• Focused: Does the program devote sufficient time exclusively to developing social and emotional skills?• Explicit: Does the program target specifi c social and emotional skills?
Durlack, Journal of Community Psychology, in press)