journée d’automne de la ssc - schweizerische ...€¦ · (paired-samples t-test) sedentarity ......
TRANSCRIPT

Prof. FranProf. Franççois Mach, MDois Mach, MDDivison of CardiologyDivison of Cardiology
Geneva University HospitalGeneva University [email protected]@hcuge.ch
www.cardiologywww.cardiology--geneva.chgeneva.ch
Bern, le 25 novembre 2010Bern, le 25 novembre 2010
PrPréévention dvention déépistage:pistage:
JournJournéée de d’’automne de la SSCautomne de la SSC

Office FOffice Fééddéérale de la Statistique rale de la Statistique NeuchâtelNeuchâtel 20062006
Health in SwitzerlandHealth in Switzerland

LipidsLipidsHypertHyperteensionnsion
AgeAge
SmokingSmoking
ObesitObesityy
NutritionNutrition
Familial HistoryFamilial HistorySedentaritySedentarity
GenderGender
GeneticGenetic
DDiabetesiabetes
Can be modifiedCan be modified
Can not be modifiedCan not be modified
Cardiovascular risk factorsCardiovascular risk factorsCardiovascular risk factors

Am J Public Health 2005
Male 35-74 year oldData from the “Bus santé” Geneva
Cardiovascular risk factorsCardiovascular risk factorsCardiovascular risk factors

LancetLancet 20020044;;364364::937937
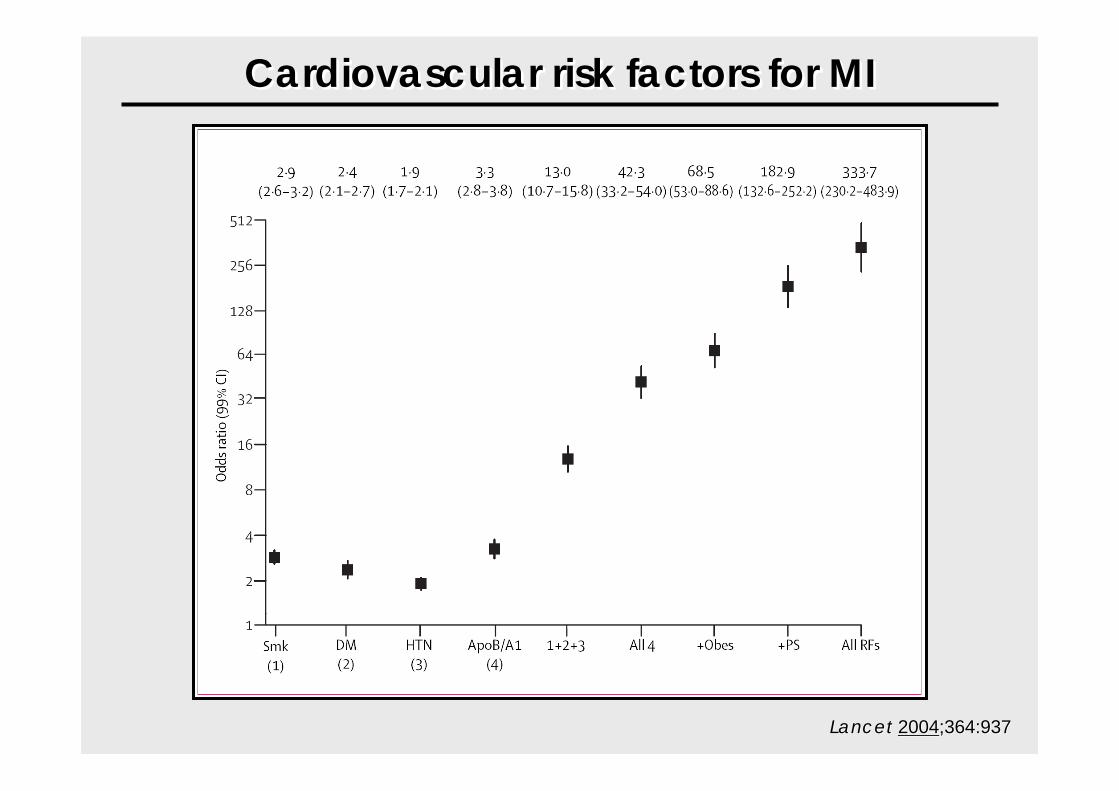
Cardiovascular risk factors for MICardiovascular risk factors for MICardiovascular risk factors for MI

LancetLancet 20020044;;364364::937937
Cardiovascular risk factors for MICardiovascular risk factors for MICardiovascular risk factors for MI

LancetLancet 20020044;;364364::937937
Cardiovascular risk factors for MICardiovascular risk factors for MICardiovascular risk factors for MI

8080--90% of acute 90% of acute MI are MI are
predictable !predictable !
Lancet 2004;364:937
CV Risk Factors & AtherosclerosisCVCV Risk Factors & Risk Factors & AthAtheerosclroscleerosrosisis

p=0.0001p=0.0001
Durée de suivi(ans)
Durée de suivi(ans)
11 55 1010 1515 2020
100%100%
90%90%
80%80%
70%70%
Prob
abilit
éde
surv
iePr
obab
ilité
de su
rvie
FC <60 bpmFC <60 bpm
60< FC <80 bpm60< FC <80 bpm
80 < FC <100 bpm80 < FC <100 bpm
FC >100 bpmFC >100 bpm
19’386 sujets - “Check-up”
FC par ECG
Suivi moyen: 18.2 ans
19’386 sujets - “Check-up”
FC par ECG
Suivi moyen: 18.2 ans
Heart rate and life expectancy within general population

• 5713 men
N Eng J MedN Eng J Med 20052005;352:1951;352:1951
• Mean follow.up 23 years
Heart rate and life expectancy within general population

•24 913 patients
Patients with coronary disease
Eur Heart JEur Heart J 20052005;26:867;26:867
•Median follow-up was 14.7 years
Heart rate and life expectancy within patients

MYO
CA
RDIA
L O
MYO
CA
RDIA
L O
22D
EMA
ND
DEM
AN
D
DIA
STO
LIC
TIM
ED
IAST
OLI
C T
IME
HEART RATEHEART RATE
O2 consumptionDiastolic time
Heart rate is a risk factor for myocardial ischemia

Predisposition Presymptomatic Symptomatic
Primary
Secondary
Tertiary
Prevention
Internist 2008;49:146
Cardiovascular PreventionCardiovascular Prevention

Tabacco and and Cardiovascular RiskTabacco and and Cardiovascular Risk
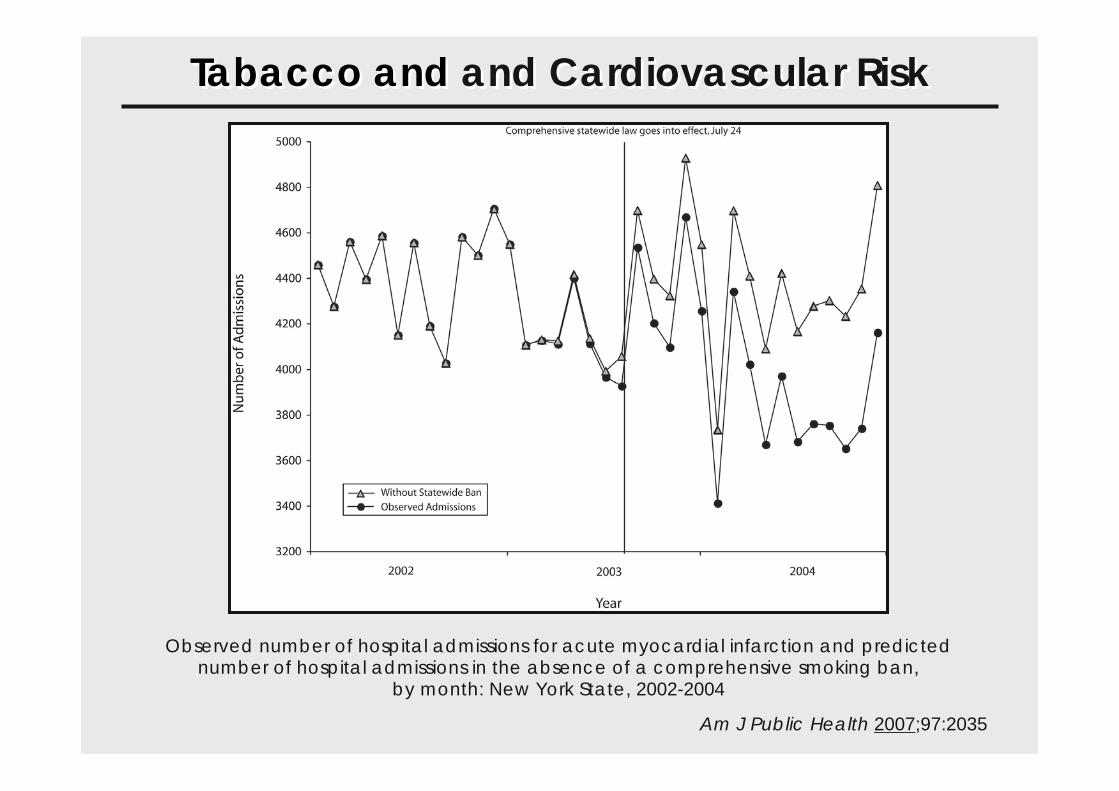
Am J Public Health 2007;97:2035
Observed number of hospital admissions for acute myocardial infarction and predicted number of hospital admissions in the absence of a comprehensive smoking ban,
by month: New York State, 2002-2004
Tabacco and and Cardiovascular RiskTabacco and and Cardiovascular Risk

LipidsLipidsHypertHyperteensionnsion
AgeAge
SmokingSmoking
ObesitObesityy
NutritionNutrition
Familial HistoryFamilial HistorySedentaritySedentarity
GenderGender
GeneticGenetic
DDiabetesiabetes
Can be modifiedCan be modified
Can not be modifiedCan not be modified
Cardiovascular risk factorsCardiovascular risk factors

Cardiovascular risk factorsCardiovascular risk factors
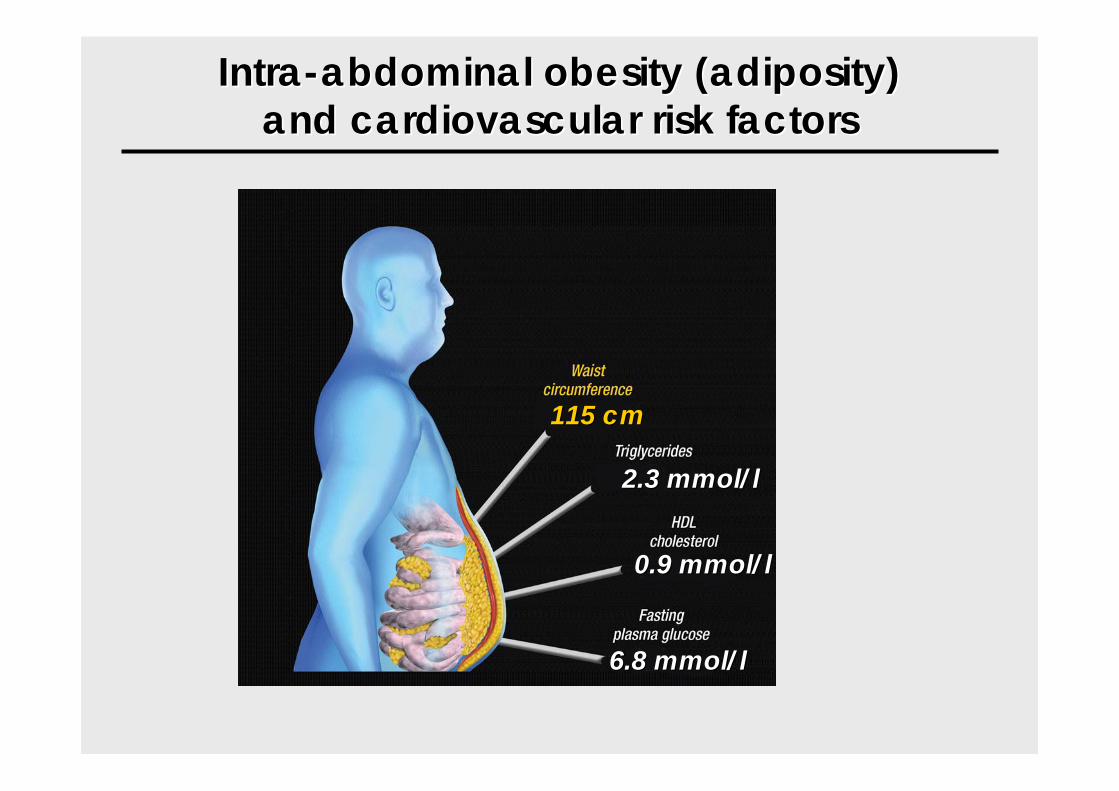
IntraIntra--abdominal obesity (adiposity)abdominal obesity (adiposity)and cardiovascular risk factorsand cardiovascular risk factors
115 cm115 cm
2.3 mmol/l2.3 mmol/l
0.9 mmol/l0.9 mmol/l
6.8 mmol/l6.8 mmol/l

Perform physical activity in daily life…Perform physical activity in daily lifePerform physical activity in daily life……

• Do not use elevators but only escalators at working place
• For 12 weeks
Sedentarity - InterventionSedentarity - Intervention
Effects on the use of escalators instead of elevators at workingplacefor better cardiovascular primary prevention:
Intervention within employee of the Geneva University Hospital

<0.001+ 0.22V02 max (l/min)
+17.25
+ 3.21- 1.77
- 1.86- 0.21
- 0.35- 1.67
- 0.18- 0.55
Mean diff.
<0.001Stairs (Floors -up /day )
<0.001V02 max (ml/kg/min)
0.03Diastolic BP (mmHg )
0.07Systolic BP (mmHg )
0.2FFM (Kg)
0.03Fatmass (Kg)
<0.001Waist circ (cm)
0.04BMI (Kg/m2 )
0.02Weight (Kg)
p
<0.001+ 0.22V02 max (l/min)
+17.25
+ 3.21- 1.77
- 1.86- 0.21
- 0.35- 1.67
- 0.18- 0.55
Mean diff.
<0.001Stairs (Floors -up /day )
<0.001V02 max (ml/kg/min)
0.03Diastolic BP (mmHg )
0.07Systolic BP (mmHg )
0.2FFM (Kg)
0.03Fatmass (Kg)
<0.001Waist circ (cm)
0.04BMI (Kg/m2 )
0.02Weight (Kg)
p
Pre and post intervention analysis(paired-samples t-test)
Sedentarity - InterventionSedentarity - Intervention

Sedentarity - InterventionSedentarity - Intervention

Prédisposition Présymptomatique Symptomatique
Primaire
Secondaire
Tertiaire
Prévention
Internist 2008;49:146
Cardiovascular PreventionCardiovascular Prevention

ELIPS: a MultiELIPS: a Multi--dimdimeensionansionall preventpreventiion on pprogram after ACrogram after ACSS

Phase 1
Inclusion before
ELIPS
(n=1500, control group)
Phase 2
Inclusion after
ELIPS
(n=1500, treated group)
Bio-clinical trial (12 months Follow-Up)
Quality trial(3 weeks after inclusion)
Bio-clinical trial (12 months Follow-Up)
Quality trial(3 weeks after inclusion)
ELIPS®
I° Endpoint: CV Death, MI or recurrent ischaemia, CVA, TIA or lower limb ischaemia
2° Endpoint: each 1° Endpoint, Bio-clinical : BMI ↓, LDL ↓, CRP ↓, HDL↑
Inclusion: ACS
ZH, BE, LS, GE: SPUM project
Program Start December 2010Program Start December 2010
www.spum-acs.ch

La réadaptation cardiaque est un programme multidisciplinaire bien défini
• Évaluation médicale
• Prise en charge des facteurs de risque
– Diabète, obésité, tabagisme, dyslipidémie, HTA
• Conseils nutritionnels
• Interventions psycho-sociales
• Conseils en activité physique
• Entraînement physique
Circulation 2007;115:2675

Les bénéfices cliniques de la réadaptation cardiaque sont bien établis
• ↘ 20% mortalité totale
• ↘ 26% mortalité cardiaque
• Recommandation de classe I (ACC/AHA)
– Maladie coronarienne et insuffisance cardiaque chronique
Am J Med 2004;16:682Circulation 2007;115:2675
La réadaptation cardiaque est habituellement divisée en 3 phases
• Phase I: intra-hospitalière
• Phase II: précoce après un évènement CV (3-6 mois)
• Phase III: au long cours
World Health Organization 1980

Plusieurs indications à la réadaptation cardiaque sont reconnues
• Infarctus du myocarde / syndrome coronarien aigu
• Revascularisation percutanée / chirurgicale
• Chirurgie valvulaire
• Transplantation cardiaque
• Insuffisance cardiaque chronique
• Insuffisance artérielle périphérique
J Am Coll Cardiol 2007;50:1400

3 modalités de réadaptation cardiaque de phase II sont possibles
• Dans un centre ambulatoire
• Dans un centre stationnaire
• À domicile

Dalal HM et al. BMJ 2010;340:5631

Ø différence significative en terme d’amélioration de la capacité
fonctionnelle entre les 2 programmes

L’introduction de ce type de programmes en Suisse est probablement moins
adaptée • Réseaux de soins et de transport très denses• Programmes de réadaptation plus intensifs 5x/sem• Système de soins encore solvable…
…mais ils pourraient être utiles dans certains cas:
• Patients indépendants et instruits• Patients âgés• Comme relais vers la réadaptation de phase III

Mieux rMieux rééspirerspirer……Manger mieuxManger mieux……
Bouger plusBouger plus……
Conclusions/MessagesConclusions/Messages

“prevention is better than cure”“prevention is better than cure”

Cardiovascular protection should start as soon as possibleCardiovascular protection should start as soon as possible……

EuroPrevent Congress 2011 EuroPrevent Congress 2011 EuroPrevent Congress 2011
International Congress Center Geneva, Geneva, April 14-16, 2011 International Congress Center Geneva, International Congress Center Geneva, Geneva, April 14Geneva, April 14--16, 2011 16, 2011

MerciMerciMerci
Prof. François Mach, MDCardiology Division
Department of Internal MedicineGeneva University [email protected]
www.cardiology-geneva.ch
Réunion d’automne SSCBern, le 25 novembre 2010Bern, le 25 novembre 2010

12 essais cliniques randomisés comparant une réadaptation à domicile versus dans
un centre• Population étudiée:
– Patients ayant présenté un infarctus du myocarde, un angor, une insuffisance cardiaque ou une revascularisation coronarienne
• Programmes de réadaptation: – 8 complets (exercice + éducation et/ou prise en charge
psychologique), 4 seulement exercice– Durée 6 à 25 semaines, 1 à 5x/semaine, 25 à 60 min


Comparaison des différents points d’aboutissement entre les 2 types de
programmes
No études Modèle d’estimation Estimation de l’effet
(95% CI) P
Capacité fonctionnelle 14 Diff. moy. standard -0.11 (-0.35 à 0.13) 0.36
TA systolique 9 Différence moyenne -0.51 (-4.63 à 3.61) 0.77
TA diastolique 7 Différence moyenne 1.85 (0.74 à 2.96) 0.001
Cholestérol total 7 Différence moyenne 0.13 (-0.05 à 0.31) 0.16
HDL-C 5 Différence moyenne -0.06 (-0.11 à -0.02) 0.004
LDL-C 4 Différence moyenne 0.15 (-0.01 à 0.31) 0.06
Tabagisme 5 Risque relatif 1.02 (0.76 à 1.37) 0.88
Suivi complet 10 Ratio de risque 1.00 (0.97 à 1.04) 0.83
Mortalité 4 Risque relatif 1.31 (0.65 à 2.66) 0.45
Coûts 4 Pas de différence significative
La réadaptation à domicile a étédéveloppée chez des patients post-IM
à bas risque à partir de 1980• Pour les patients ne pouvant pas participer en groupe (éloignés,
âgés, travailleurs indépendants, minorités ethniques…)
• Populaire actuellement surtout en Grande-Bretagne
• « The Heart Manual »– Livre / journal de bord / CD relaxation / CD-ROM information– Visite infirmière initiale 1 h– Programme de 6 semaines– Suivi téléphonique 1x/sem
Circulation 1984;70:645Int J Cardiol 2007;119;202

ACS: a poor prognosisACS: a poor prognosis
STEMI NSTEMI
30-Day Mortality 8 % 6 %
1-Year Mortality 9 % 11.6 %
GRACE Registry. Am J Cardiol 2004;93:288Eur Heart J 2007;28:1409

ACS: a poor prognosisACS: a poor prognosis
• Why is the recurrence rate so high ?
Because of under use of recommended therapy by the physician
Because atherosclerosis is a chronic disease with a complex treatment
Because of the lack of therapeutic adhesion by the patient

Patient-level intervention
Health care providers-level intervention Health care providers-level intervention
System-level interventionSystem-level intervention
Auer R. Circ 2008;
26 studies; 37'585 patients with one year follow up
How to improve therapeutic adherence?How to improve therapeutic adherence?

Time
Insulin1921
Antibiotics1945
Patient education1972
diabetesTE has optimalized application of
biomedical advances
Mor
talit
y
Courtesy: A. Golay

Multi-dimensional
ACS: a poor prognosis
To improve quality of care of patients with an ACS
To improve quality of information and education
To improve therapeutic adhesion
TO IMPROVE OUTCOME
Why ELIPS ?Why ELIPS ? ELIPS

How to improve therapeutic adhesion:How to improve therapeutic adhesion:
By motivatingBy motivating
By educatingBy educating
ACS: a poor prognosisELIPSELIPS ELIPS
The patient experience:The patient experience:Acute coronary syndromeAcute coronary syndrome
•• Sudden eventSudden event•• Rapid therapeutic Rapid therapeutic
responseresponse•• Impressive technical Impressive technical
resourcesresources•• Immediate perceptible resultsImmediate perceptible results
Educational intentions:Educational intentions:manage amanage a chronic diseasechronic disease
•• Make the patients aware of Make the patients aware of their diseasetheir disease
•• Promote lifestyle changesPromote lifestyle changes•• Improve adherence to Improve adherence to
treatmenttreatment
The TPE challenge The TPE challenge «« acute acute -- chronicchronic »»
TPE: Therapeutic Patient Education
PassivePassive ActiveActive

52
Tools of CommunicationTools of Communication

Multi-dimensional
1st of October 20101st of October 2010
DVD

Multi-dimensional
1st of October 20101st of October 2010
DVD

For patientsFor Healthcare providers
Multi-dimensional
1st of October 20101st of October 2010
web

Multi-dimensionalMobile App

www.elips.ch
1) Tools of information1) Tools of information comprehension comprehension and motivation of the patient by using uniformand motivation of the patient by using uniformmessages: messages: PatientPatient--level interventionlevel intervention
ELIPS
For Hospitals and outpatient practices

2) Motivational Interviews2) Motivational InterviewsA new technique of communication for A new technique of communication for Health Care Providers: Health Care Providers: HCPHCP--level interventionlevel intervention
b) A training course in motivational interviews (2 days)
A structured learning process for HealthCare Providers including:
a) An e-learning to approach this new technique of communication (90 min)
c) A control of the process on site by a specialized nurse
For Hospitals
ELIPS

3) Standardization of therapy for patients with ACS3) Standardization of therapy for patients with ACS
1) A critical pathway for hospitals
2) A discharge card of treatment for patients and outpatient practices
TO IMPROVE QUALITY OF CARE
ELIPS

Tools offered to GPs, internists, cardiologists for their patients
Novel information tools about ACS and Atherosclerosis:ELIPS:
- a standardized discharge card of treatment- a website, an e-learning- an educational DVD- information flyers & wall chart
and …..- symposiums of information for outpatient and physicians organized by local university hospitals
3) Standardization of therapy for patients with ACS3) Standardization of therapy for patients with ACSELIPS
ACS: a poor prognosisThank youThank youDr Lukas AltwegDr Reto AuerDr Vincent BarthassatDr David CarballoDr Sebastian CarballoPr Jean-Claude ChevroletDr Pierre ChopardMme Suzanna ConvertProf Jacques CornuzDr Pascal GachePr Alain GolayMme Christelle GuillaumeDr Pierre-Frédéric KellerDr Roland KlingenbergPr Thomas LuscherPr François MachDr Christian Matter
Mme Suzanne MuellerPr Thomas PernegerDr Lorenz RaeberMme Agnies ReffetMme Ariel Richard-ArlaudDr Nicolas RodondiDr Marco RoffiM. Allen SavardMme Florence ScherrerM. Franck SchneiderM. Philippe SigaudDr Johanna SommerPr Pierre VogtPr Gérard WaeberPr Stephan Windecker
ELIPS

La fondation GEcor
Abbott VascularAstraZenecaBiotronikBoston ScientificBristol-Myers SquibbCordisDaichii-SankyoEli LillyEssexGE-Healthcare MedicalGlaxo Smith KlineInvatec
MSDPfizerSanofi-aventisServierSt. Jude MedicalTakeda
ACS: a poor prognosisThank youThank you ELIPS

♀♀
0Patients (%)
♂♂
20 40 60
Circulation 1993;88:2548
Framingham Heart Study (n=5144)
Infarctus ou mort subite comme 1ère présentation
Premier événement peut être le dernier !Premier Premier éévvéénement peut être le dernier !nement peut être le dernier !

Multi-dimensionalE-learning

ACS: a poor prognosisPatient
s (%
) 15.2
0.0
5.0
10.0
15.0
20.0
Cardiovascualr Mortality / MI / Stroke
Established atherosclerotic arterial disease
5.3
at risk of atherothrombosis
1 patient out of 7 will experience a
recurrence of a CV event (MI, Stroke,
Cardiovascular Death, angina, PAD) within the next 12 months following an ACS.
N=68’236 patients
Steg P.G. JAMA. 2007;297:1197‐1206.
ACS: a high rate of reccurent CV event

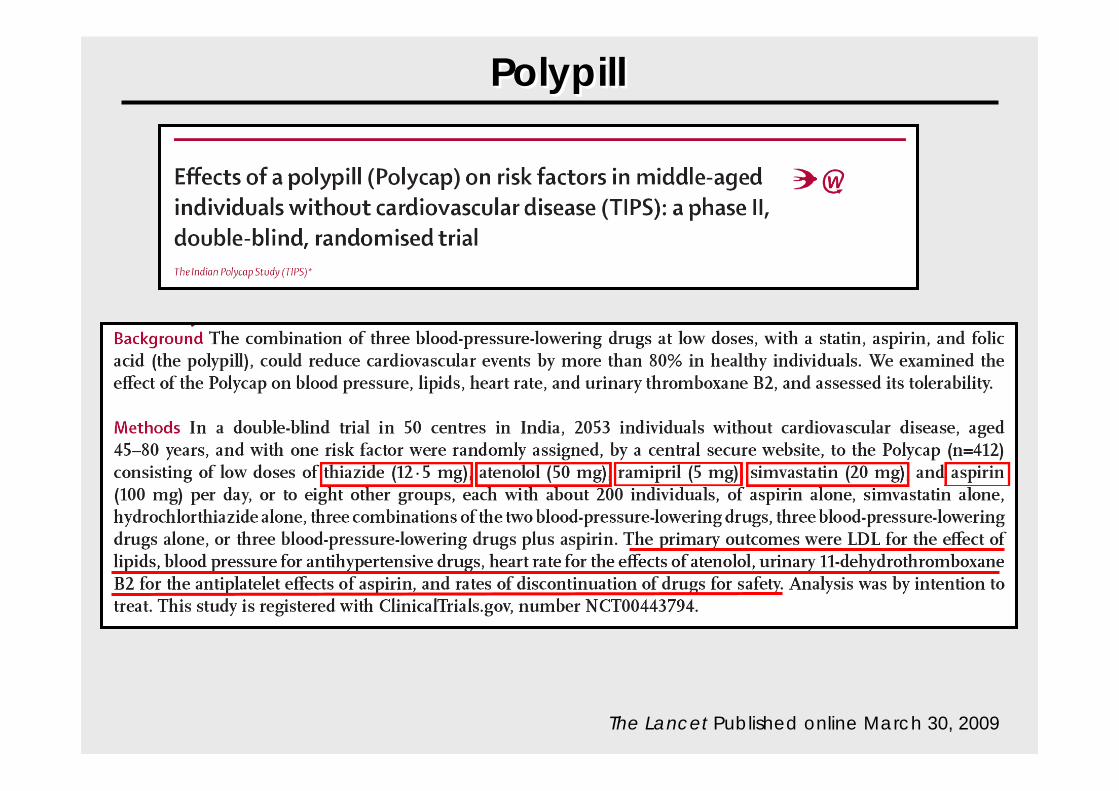
PolypillPolypillPolypill
The Lancet Published online March 30, 2009

The Lancet Published
PolypillPolypill

PolypillPolypill
The Lancet Published
LancetLancet 20020044;;364364::937937
Cardiovascular risk factors for MICardiovascular risk factors for MICardiovascular risk factors for MI

Limitations avouées et non avouées
• Patients à bas risque, sécurité non établie pour IC par ex.• Hétérogénéité des patients et des programmes
• Réadaptation en centre semble supérieure si programme intensif
• Réadaptation cardiaque validée par programmes en centre
• Difficulté de motivation hors d’un groupe• Pas de supervision étroite (contrôles/corrections)• Bon niveau d’éducation nécessaire

Mensonges et Propagande

Women
0Patients (%)
Men
20 40 60
Circulation 1993;88:2548
Framingham Heart Study (n=5144)
MI or SD as 1st Presentation
PreventionPreventionPrevention

Primary PreventionPrimary Prevention Secondairy PreventionSecondairy Prevention
Cardiovascular eventCardiovascular eventDiagnosois of atherosclerosisDiagnosois of atherosclerosis
Atherosclerosis Atherosclerosis –– Dynamic ProcessDynamic Process

Stress & Cardiac Rythm