journal of jul 2015 - the society of physicians of hong...
TRANSCRIPT

Journal of THE SOCIETY OF PHYSICIANS OF HONG KONG
www.soPHYSICIANShk.orgVisit the web site for our monthly CME programmes for doctors
JUL 2015 • VOL. 7 • NO. 4
ISSN 2072-4209

To learn more or to subscribe risk-free,
visit learn.uptodate.com/HongKong15 or call +1-800-998-6374 | +1-781-392-2000.
We interpret the clinical research.
You apply it at the point of care.
is continuously updated based
on the latest medical research to bring you current
evidence-based recommendations.
Our unparalleled team of physicians and
editors places new research in the context
of the existing body of medical knowledge
using their professional expertise and
first-hand clinical experience.
This combination of Evidence & Experience
is invaluable in crafting point-of-care
recommendations trusted by more than
1 million clinicians worldwide.

JUL 2015 Journal of The Society of Physicians of Hong Kong | 44
Pictorial Medical History (13)Dr Lam Tat Chung, Paul (林達聰醫生)FRCP, FRCPsych, FHKAM (Medicine), FHKAM (Psychiatry)Specialist in Psychiatry (Private Practice)Honorary Clinical Assistant Professor, The University of Hong Kong
A tholos is a round house usually associated with a temple. In this picture the remains of the tholos can be clearly seen. The tholos at Epidaurus was built around 440 BCE. It contains an outer circle of 26 concentric Doric colonnade and an inner circle of 14 Corinthian columns. In its original days it was decorated with ornate paintings of Eros, the God of love and Methe, the Goddess of inebriation.
Message from the President
At the last Annual General Meeting of the society, the following were elected to the Executive Committee for 2015–2016.
Tholos at Asclepieion, Epidaurus
The President and Committee look forward to serving the Society and the medical community in the year to come.

45 | Journal of The Society of Physicians of Hong Kong JUL 2015
Introduction
Idiopathic pulmonary fibrosis (IPF) is defined as a specific form of chronic, progressive fibrosing inter-
stitial pneumonia of unknown aetiology. It occurs primarily in older adults, is limited to the lungs and is associated with a histologic and or radiologic pattern of usual interstitial pneumonia (UIP).1
To make a diagnosis of IPF the fol-lowings are required:
a. Exclusion of other known causes of interstitial lung disease (ILD) eg, connective tissue disease, drug toxicities and pneumoconiosis.
b. Presence of a UIP pattern on high-resolution computed tomography (HRCT) in patients not subjected to surgical lung biopsy.
c. Specific combination of HRCT and surgical lung biopsy pattern in patients subjected to surgical lung biopsy.1
From time to time, a multi-disci-
plinary team discussion between the pul-monologist, radiologist and pathologist is required and is shown to increase the diagnostic accuracy of IPF.
Epidemiology IPF’s prevalence and incidence
increase with age and are higher among males than females. According to a review in 2012, IPF prevalence in the USA was estimated to vary between 14–27.9 cases per 100,000 population using narrow case definitions, and 42.7–63 per 100,000 population using broad case definitions.2 The annual incidence of IPF in the USA was estimated at 6.8–8.8 per 100,000
population using narrow case definitions and 16.3–17.4 per 100,000 populations using broad case definitions.2
Disease Course and Pharmacological Treatment
The natural history of IPF is variable and unpredictable. While most patients with IPF demonstrate a gradual worsening of lung function over years, a minority of patients remain stable or decline rapidly. Some may experience episodes of acute worsening despite previous stability (Figure 1).1
In 2011, a joint statement by the
Idiopathic Pulmonary Fibrosis: A Novel Medication for an Untreatable Disease
Stable
Slow progression
Rapid progression
Dis
ease
pro
gres
sion
Time
Acute worsening
Figure 1. The natural history of IPF1Key words:
Dr Wong Wai Leung
MBBS (HK), MRCP (UK), FHKCP, FHKAM, FCCP, FRCP (London), FRCP (Glasgow)Assoicate Consultant, Department of Respiratory Medicine, Ruttonjee Hospital, Hong Kong
JUL 2015 Journal of The Society of Physicians of Hong Kong | 46
American Thoracic Society, European Respiratory Society, Japanese Respi-ratory Society and Latin American Thoracic Association (ATS/ERS/JRS/ALAT) on IPF extensively reviewed the available literature and came to a con-clusion that the following medication or treatment regime are strongly recom-mended against:2
1) Corticosteroid monotherapy2) Colchicine3) Cyclosporine4) Combined corticosteroid and
immune modulator therapy5) Interferon gamma 1b6) Bosentan 7) Etanercept
While the following medications or
treatment regimens were recommended as weakly against (“weak no”) (that is; these therapies should not be used in the majority of patients in IPF but may be a reasonable choice in a minority):2
1) Combined acetylcysteine, azathioprine and prednisolone therapy
2) Acetylcysteine monotherapy3) Anticoagulation4) Pirfenidone
Based on the evidence examined in this statement, there is no proven pharmacologic therapy for IPF. For well-informed patients who strongly demand pharmacologic treatment, it is suggested that therapies can be chosen from cat-egories of “weak no”.
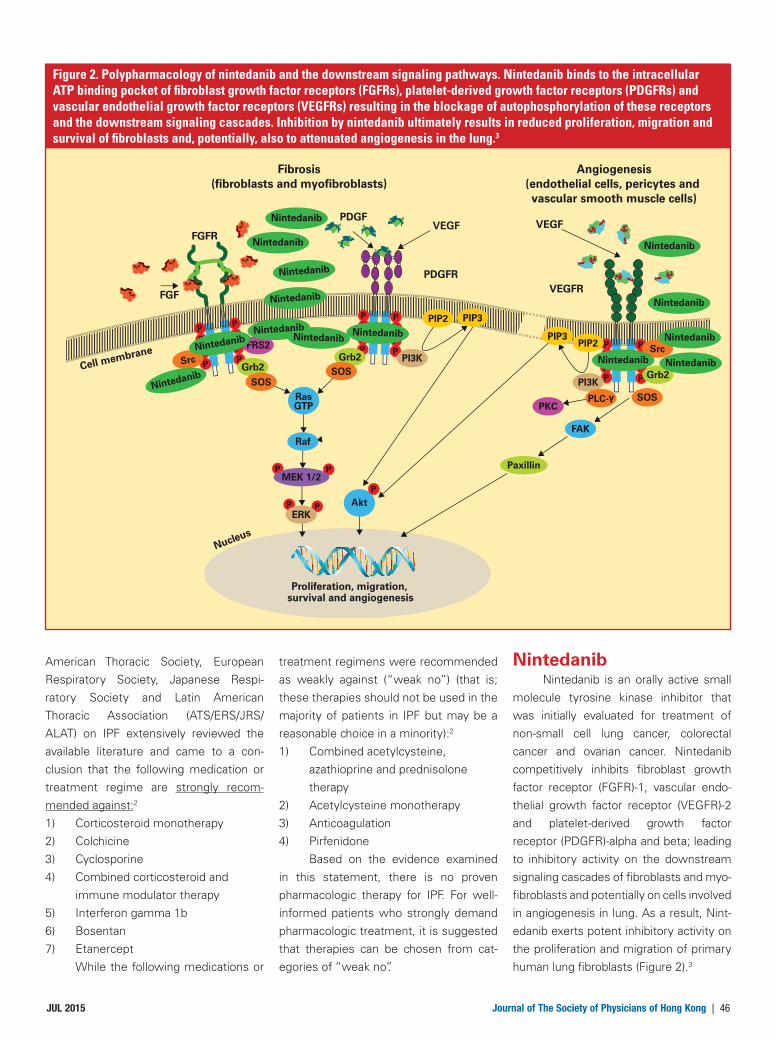
NintedanibNintedanib is an orally active small
molecule tyrosine kinase inhibitor that was initially evaluated for treatment of non-small cell lung cancer, colorectal cancer and ovarian cancer. Nintedanib competitively inhibits fibroblast growth factor receptor (FGFR)-1, vascular endo-thelial growth factor receptor (VEGFR)-2 and platelet-derived growth factor receptor (PDGFR)-alpha and beta; leading to inhibitory activity on the downstream signaling cascades of fibroblasts and myo-fibroblasts and potentially on cells involved in angiogenesis in lung. As a result, Nint-edanib exerts potent inhibitory activity on the proliferation and migration of primary human lung fibroblasts (Figure 2).3
Fibrosis(fibroblasts and myofibroblasts)
Angiogenesis(endothelial cells, pericytes and vascular smooth muscle cells)
FGFR
FGF
PDGFVEGF
VEGFRPDGFR
Cell membrane
Nucleus
VEGF
Proliferation, migration, survival and angiogenesis
ooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooo o o o o o oooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooooo
oooo
oo
ooooo
FAKRaf
RasGTP
Akt
P
P PP
P
PP
P P
P P
P
PP
P PP
P
PP
P P
P PP
P
P
P P
PI3K
PI3K
ERK
PKC
FRS2
MEK 1/2
Grb2
Grb2Grb2
Paxillin
SOS
SOS
SOS
SrcSrc
PLC-γ
PIP2 PIP3
PIP3PIP2
NintedanibNintedanib
Nintedanib
Nintedanib
Nintedanib
Nintedanib
Nintedanib
Nintedanib
Nintedanib
Nintedanib Nintedanib
Nintedanib
Nintedanib
Nintedanib
Figure 2. Polypharmacology of nintedanib and the downstream signaling pathways. Nintedanib binds to the intracellular ATP binding pocket of fibroblast growth factor receptors (FGFRs), platelet-derived growth factor receptors (PDGFRs) and vascular endothelial growth factor receptors (VEGFRs) resulting in the blockage of autophosphorylation of these receptors and the downstream signaling cascades. Inhibition by nintedanib ultimately results in reduced proliferation, migration and survival of fibroblasts and, potentially, also to attenuated angiogenesis in the lung.3

47 | Journal of The Society of Physicians of Hong Kong JUL 2015
A 12 month, phase 2 trial assessed the efficacy and safety of nintedanib compared with placebo in patients with IPF.4 A total of 432 patients were ran-domized to receive four different oral doses of nintedanib (50 mg once daily, 50 mg twice daily, 100 mg twice daily or 150 mg twice daily) or placebo. In the 150 mg twice daily group, forced vital capacity (FVC) declined by 0.06 litre per year as compared with 0.19 litre per year in the placebo group, a 68.4% reduction in the rate of loss with treatment group (p=0.01 with the hierarchical testing pro-cedure [Figure 3]). This dose also resulted in a lower incidence of acute exacer-bations when compared with placebo (2.4 vs 15.7 per 100 patient-years, p=0.02 [Figure 4]) and also a smaller decrease in the St George’s Respiratory Ques-tionnaire (SGRQ) score as compared with placebo (-0.66 vs 5.46, p=0.007).4
Nintedanib, 150 mg twice dailyNintedanib, 100 mg twice dailyNintedanib, 50 mg twice dailyNintedanib, 50 mg once dailyPlacebo
Day
Chan
ge in
FVC
(litr
es/y
r)
0
-0.25
-0.20
-0.15
-0.10
-0.05
0.00
0.05
0.10
50 100 150 200 250 300 350
Inci
denc
e of
acu
te e
xace
rbat
ions
per 1
2 m
onth
s at
risk
18
14
16
12
10
8
6
4
2
0
Placebo(N=87)
Nintedanib50 mg
once daily(N=87)
Nintedanib50 mg
twice daily(N=86)
Nintedanib100 mg
twice daily(N=86)
Nintedanib150 mg
twice daily(N=86)
Figure 3. Change in forced vital capacity (FVC) over time4
Figure 4. Incidence of acute exacerbations over 12 months4
0 15 29 43 85 169 253 365
No. of PatientsTotal 432 419 416 415 398 385 372 317Placebo 87 81 82 82 80 79 74 6150 mg once daily 87 85 82 80 78 72 71 6150 mg twice daily 86 85 86 86 82 81 80 71100 mg twice daily 86 84 84 84 80 82 79 67150 mg twice daily 86 84 82 83 78 71 68 57

JUL 2015 Journal of The Society of Physicians of Hong Kong | 48
The investigators concluded that nintedanib 150 mg twice daily was asso-ciated with a trend towards reduction in the decline in lung function, fewer acute exacerbations and better quality of life when compared with placebo.4
Two replicate 52 week, randomized, double blind, phase 3 trials (INPULSIS-1 and INPULSIS-2) were conducted to evaluate the efficacy and safety of nint-edanib 150 mg twice daily versus placebo in patients with IPF.5 A total of 1066 patients were randomly assigned in a 3:2 ratio to receive nintedanib or placebo. The adjusted annual rate of change in FVC was -114.7 ml with nintedanib versus -239.9 ml with placebo (difference 125.3 ml; 95% CI 77.7 to 172.8; p<0.001) in INPULSIS-1 and -113.6 ml with nint-
edanib versus -207.3 ml with placebo (difference 93.7 ml; 95% CI, 44.8 to 142.7; p<0.001) in INPULSIS-2 (Figure 5). INPULSIS-2 demonstrated a significant benefit in time to first acute exacer-bation with nintedanib versus placebo (hazard ratio, 0.38; 95%CI, 0.19 to 0.77; p=0.005) but this benefit was not seen in INPULSIS-1 (Figure 6). However, the pooled data analysis showed that nint-edanib had a significant benefit on the time to the first adjudicated acute exac-erbation (Figure 7).5 The most frequent adverse event in the nintedanib group was diarrhoea with a rate of 61.5% compared with 18.6% in the placebo group in INPULSIS-1.5
The investigators concluded that nintedanib reduced the rate of FVC
decline in IPF patients in both trials. In INPULSIS-2, the rate of acute exacer-bations was significantly lower in the nintedanib arm than in placebo, but this finding was not reproducible in INPULSIS-1. This heterogeneity may be due to the rare event rate of acute exac-erbations and therefore the study was underpowered in this regard. Diarrhoea was a frequent adverse event which led to discontinuation of study medication in less than 5% of patients (4.5% in INPULSIS-1 and 4.3% in INPULSIS-2).
Nintendanib was officially approved by the Food Drug Administration, USA on 15th Oct 2014 and by the European Medicines Agency on 19th Jan 2015 as a pharmacologic agent for the treatment of IPF.6,7
50
-50
0
-100
-150
-200
-2500 4 6 12 24 36 52
WeekNo. of PatientsNintedanibPlacebo
301198
2
303202
298200
292194
284192
274187
250165
No. of PatientsNintedanibPlacebo
315210
323215
315207
312209
303203
295196
269180
Nintedanib, 150 mg twice daily
Placebo
50
-50
0
-100
-150
-200
-2500 4 6 12 24 36 52
Week
2
Nintedanib, 150 mg twice daily
Placebo
INPULSIS-1
INPULSIS-2
Mea
n ob
serv
ed c
hang
e fr
om b
asel
ine
in F
VC (m
l)M
ean
obse
rved
cha
nge
from
bas
elin
e in
FVC
(ml)
Adjusted mean difference,109.9 (95% CI, 71.3–148.6)P<0.001
Adjusted mean difference,109.8 (95% CI, 70.9–148.6)P<0.001
Figure 5. Annual rate of decline and change from baseline over time in FVC in INPULSIS-1 and INPULSIS-25

49 | Journal of The Society of Physicians of Hong Kong JUL 2015
ConclusionIn the past, rapidly progressive IPF
was invariably fatal and the only available treatment was lung transplantation. This new pharmacological agent, which is able to slow down the deterioration of lung function and possibly reduce the rate of acute exacerbation in IPF patients, is an
exciting addition to our treatment arma-mentarium. Although longer-term data on the impact of nintendanib on mortality, quality of life, acute exacerbation and adverse event profile in IPF patients is still pending, we are happy that there is at least one more option for our patients.
References1. G Raghu, H Collard. An Official ATS/ERS/JRS/ALAT statement:
Idiopathic pulmonary fibrosis: Evidence-based guidelines for diagnosis and management. Am J Respir Crit Care Med 2011;183:788-824
2. L Nalysnyk, J Cid-Ruzafa. Incidence and prevalence of idiopathic pulmonary fibrosis: review of the literature. Eur Respir Rev 2012;21:126,355-361
3. L Wollin, E Wex. Mode of action of nintedanib in the treatment of idiopathic pulmonary fibrosis. Eur Respir J 2015;45:1434-1445
No. of PatientsNintedanibPlacebo
306202
309204
304200
292197
290197
283193
288197
282191
280191
275188
271186
267181
258178
233170
INPULSIS-1
INPULSIS-2
Cum
ulat
ive
inci
denc
e of
firs
t inv
estig
ator
-re
port
ed a
cute
exa
cerb
atio
n (%
)Cu
mul
ativ
e in
cide
nce
of fi
rst i
nves
tigat
or-
repo
rted
acu
te e
xace
rbat
ion
(%)
15
1314
1211
98
654321
10
7
00 30 60 90 120 150 373
Days
No. of PatientsNintedanibPlacebo
326217
329219
323215
217211
315210
306200
307206
302198
300195
295193
291190
286186
279181
259171
Days
180 210 240 270 300 330 360
0 30 60 90 120 150 373180 210 240 270 300 330 360
Placebo
Nintedanib, 150 mg twice daily
15
1314
1211
98
654321
10
7
0
Placebo
Nintedanib, 150 mg twice daily
Hazard ratio, 1.15 (95% CI, 0.54–2.42)P=0.67
Hazard ratio, 0.38 (95% CI, 0.19–0.77)P=0.005
Cum
ulat
ive
inci
denc
e of
firs
t inv
estig
ator
-re
port
ed a
cute
exa
cerb
atio
n (%
)
No. of PatientsNintedanibPlacebo
632419
638423
627415
609408
605407
589393
595403
584389
580386
570381
562376
553367
537359
492341
15
1314
1211
98
654321
10
7
00 30 60 90 120 150 373
Days180 210 240 270 300 330 360
Placebo
Nintedanib, 150 mg twice daily
HR 0.32 (95% CI; 0.16, 0.65)p=0.001
Figure 6. Time to first investigator-reported acute exacerbation in INPULSIS-1 and INPULSIS-25
Figure 7. Time to first acute exacerbation based on confirmed and suspected acute exacerbations (per adjudication) in INPULSIS-1 and INPULSIS-2 (pooled data)5
A complete list of references can be downloaded from www.SOPHYSICIANSHK.org


51 | Journal of The Society of Physicians of Hong Kong JUL 2015
THE SOCIETY OF PHYSICIANS OF HONG KONGTHE HONG KONG SOCIETY OF GASTROINTESTINAL MOTILITY
Sunday Symposium August 9, 2015
4:00 pm–4:30 pm Q & A
Registration Form: Fax to: 2856 2611 Attention to: Sherry Yuen of GileadWeb registration and further details: www.SOPHYSICIANSHK.org£ I wish to attend meeting and lunch on Aug 9, 2015 ($100)Name of Doctor (Surname first): _________________________________________ Tel: ___________________
I am a Member/Associate Member of £ SPHK £ GI Motility SocietyFree for Members and Associate Members of Hosting Societies


53 | Journal of The Society of Physicians of Hong Kong JUL 2015
THE SOCIETY OF PHYSICIANS OF HONG KONGSunday Symposium September 13, 2015
President: Dr Lam Tat Chung, Paul FRCP, FRCPsych, FHKAM(Medicine), FHKAM(Psychiatry)
11:00 am–11:30 am LATEST STROKE MANAGEMENT IN DAILY PRACTICE Dr Yuen Mang Ho Specialist in Neurology
11:30 am–12:00 pm HOW TO DELAY DISEASE PROGRESSION IN AF Dr Lai Wai Keung Specialist in Cardiology
12:00 pm–12:30 pm UPDATE IN HYPERTENSION MANAGEMENT IN RENAL DISEASE Dr Yung Chee Unn, Jonathan Specialist in Nephrology
12:30 pm–1:00 pm CORONARY ARTERY DISEASE (CAD) & LIPID MANAGEMENT Dr Li Siu Lung Specialist in Cardiology
1:00 pm–2:00 pm ––––––––––––––––– LUNCH –––––––––––––––––
2:00 pm–2:30 pm MANAGING KNEE OSTEOARTHRITIS - FROM CONSERVATIVE TO SURGICAL Dr Tse Lung Fung Specialist in Orthopaedics & Traumatology
2:30 pm–3:00 pm FATTY LIVER - AN UPDATE Dr Chow Tai Nin Specialist in Gastrointestinal Disease
3:00 pm–3:30 pm MANAGEMENT OF ALLERGIC RHINITIS IN ASTHMATIC PATIENT Dr Leung Cheuk Wa Specialist in Paediatrics
3:30 pm–4:00 pm UPDATE IN DM MANAGEMENT Dr Yeung Chun Yip Specialist in Endocrinology
4:00 pm–4:30 pm Q & A
Place: The Langham Hotel, 8 Peking Road, Tsimshatsui, Kowloon Enquiry: Tel: 2526 2626 (no telephone registration) CME under application.Fee: Non-members please pay $100 on admission (Do not mail your cheque)
First come first serve basis. Pre-registration is required.No confirmation will be sent for registration. Unsuccessful applicants will be notified.
Sponsor: Sanofi-Aventis Hong Kong Ltd
Registration Form: Fax to: 2506 2537 Attention to: Daniel Chan of Sanofi-AventisWeb registration and further details: www.SOPHYSICIANSHK.org£ I wish to attend meeting and lunch on Sep 13, 2015 ($100)Name of Doctor (Surname first): _________________________________________ Tel: ___________________
Free for Members and Associate Members on presentation of valid membership cards of THE SOCIETY PHYSICIANS OF HONG KONG

JUL 2015 Journal of The Society of Physicians of Hong Kong | 54
Nonalcoholic Fatty Liver Disease
IntroductionNonalcoholic fatty liver disease
(NAFLD) is a clinico-histopathological diagnosis. According to the American Association for the Study of Liver Diseases (AASLD), the diagnosis requires the presence of primary hepatic steatosis diagnosed by either imaging or histology, and exclusion of secondary hepatic fat accumulation (e.g. extensive alcohol consumption, steatogenic medi-cation or hereditary disorders).1 The histological spectrum ranges from fat accumulation in hepatocytes without concomitant inflammation or fibrosis (simple hepatic steatosis) to hepatic steatosis with a necroinflammatory component (steatohepatitis) that may or may not have associated fibrosis. Non-alcoholic steotohepatitis (NASH) may progress to fibrosis, cirrhosis and hepato-
cellular carcinoma in 50%, 15% and 4% of patients, respectively.2 NASH is now recognized to be a leading cause of cryp-togenic cirrhosis.3
PathogenesisThe pathogenesis of NAFLD is
likely to result from obesity-related insulin resistance and additional oxidative injury, as the liver is the central organ of lipid and glucose metabolism.4 The development of NAFLD (ie, steatosis) results from an increased influx of free fatty acids (FFA) derived from insulin-resistant adipose tissue, altered hepatic processing of dietary lipids delivered by lipoproteins, increased hepatic de novo lipogenesis, or impaired lipid export from hepatocytes. In a small proportion of patients, hepatic steatosis progresses to NASH with hepatocellular damage and inflammation, thereby elevating the risk for further progression to fibrosis, cirrhosis and hepatocellularcarcinoma (HCC).5 This is related to an imbalance of pro- and anti-inflammatory factors.6 FFA induce several cytochrome p-450 microsomal lipoxy-genases which produce hepatotoxic-free oxygen radical species.
EpidemiologyNAFLD is the most common liver
disorder in developed Western countries, affecting 20–40% of the general popu-lation. The major risk factors for NAFLD are central obesity, type 2 diabetes mellitus, hyperlipidaemia, and met-abolic syndrome.7 In Asia, large popu-lation-based surveys in China, Japan, and Korea indicate that the prevalence of NAFLD is now 12–24%.8 In 2011, a population study in Hong Kong reported that the prevalence of NAFLD was 27% and the estimated prevalence of advanced fibrosis in patients with fatty liver was 4%.9
Clinical manifestationsThe most common presentation
of NAFLD or NASH is asymptomatic elevation of liver aminotransferases. Sometimes patients will complain about fatigue or slight epigastric discomfort.10 Normally the AST/ALT ratio is less than 1; in contrast, the ratio in alcoholic hep-atitis is usually above 2.11,12 Alkaline phosphatase and hyperbilirubinemia are uncommon, but serum AST and ALT are elevated in 90% of patients. However, amongst patients with NAFLD, normal serum AST or ALT do not exclude the presence of advanced histologic features. Diabetes has been shown to be the only independent predictive factor for advanced fibrosis.13
DiagnosisUltrasonography is useful for the
detection of liver steatosis with a sen-sitivity of 60–94% and a specificity of 66–95% (Figure 1).14 However, this method is limited by its low sensitivity for mild steatosis, its inability to differ-entiate mild fibrosis from steatosis and to accurately quantify fatty infiltration. Computed tomography (CT) and magnetic resonance imaging (MRI) can also identify steatosis,15 but they are expensive and not widely applicable in clinical practice.
Transient elastography (TE) is accurate in diagnosing advanced liver fibrosis in most NAFLD patients.16 At a cutoff value of 7.9 kPa, the sensitivity, specificity, and positive and negative pre-dictive values for advanced fibrosis (F3 or above) were 91%, 75%, 52%, and 97%, respectively. With high negative predictive value and modest positive pre-dictive value, TE is useful as a screening test to exclude advanced fibrosis. However, failure to obtain 10 valid mea-surements ranged from 3–16% due to a high body mass index (BMI >30), which
Dr Ng Fook Hong
MB,BS(HK), MD (HK), MRCP(UK), FRCP (Edinburgh), FRCP (London), FRCP (Glasgow), FHKCP, FHKAM (Medicine)Specialist in Gastroenterology and Hepatology, Private PracticeHonorary Consultant in Gastroenterology and Hepatology, Ruttonjee HospitalHonorary Assistant Professor, Department of Medicine, University of Hong Kong
Key words:

55 | Journal of The Society of Physicians of Hong Kong JUL 2015
could interfere with the transmission of the ultrasound and the elastic impulses, thus limiting the correct estimation of liver stiffness. A new bigger tip probe (XL probe), specifically designed for obese patients has been developed. The explored region of interest of the new probe is located more deeply (3.5 cm vs 2.5 cm from the skin surface), thus overcoming the diagnostic difficulty due to the interposition of thickened subcu-taneous adipose tissue. When comparing the diagnostic performances of the two probes, the XL probe obtains more reliable results as compared with the M probe (failure rates of 7% vs 35%17 and 24% vs 55%18 respectively, defined as failure to obtain 10 valid measurements).
A promising new application of TE (Echosens, Paris, France) is the vibration-controlled TE (VCTE) device, which allows the calculation of the controlled attenuation parameter (CAP), useful for the non-invasive and accurate estimation of liver steatosis.19 A recent multicenter study demonstrated that the cut-offs for the CAP values in patients with steatosis ≥5%, ≥34% and ≥67% were 253 dB/m, 285 dB/m and 310 dB/m, respectively. The areas under the curves were 0.92, 0.92 and 0.88 for steatosis ≥5%, ≥34% and ≥67%, respectively.20
Liver biopsy is the only way to defin-itively diagnose NASH and also permits determination of disease severity. However, serious complications occurred in approximately 1% of patients21 with an overall mortality risk of 0.2%.22
Natural historyIn a population-based study in the
United States, patients with NAFLD had slightly lower overall survival than the general population (standardized mor-tality ratio of 1.34, 95% CI 1.00–1.76)23. Higher mortality was associated with increasing age, impaired fasting glucose, and cirrhosis. Most mortality was due to cardiovascular disease, although 14% was due to liver disease.24
In Hong Kong, a longitudinal study followed up 52 patients (age 44 +/- 9 years) with biopsy-proven NAFLD. Liver biopsies were repeated at month 36.25 Overall, 14 (27%) patients had fibrosis progression, 25 (48%) had static disease, and 13 (25%) had fibrosis regression. Reduction in BMI and waist circum-ference was independently associated with non-progressive disease activity and fibrosis.
NAFLD is associated with a high prevalence of colorectal adenomas. In a study conducted in Hong Kong, NAFLD
patients had a higher prevalence of colorectal adenomas (34.7% vs 21.5%; p=0.043) and advanced neoplasms (18.6% vs 5.5%; p=0.002) than healthy controls.26
TreatmentNAFLD has systemic conse-
quences as it worsens insulin resistance, predicts the emergence of metabolic complications and increases the risk for cardiovascular events. Thus, liver-directed therapy likely also has beneficial effects on extra-hepatic metabolic compli-cations.27 The management of co-mor-bidities such as obesity, hyperlipidemia, hypertension and diabetes mellitus is generally recommended and weight loss and increased physical activity can lead to sustained improvement in liver enzymes, histology, serum insulin levels, and quality of life in patients with NASH. Weight loss should be gradual and should not exceed 1.6 kg per week, since rapid weight reduction has been associated with worsening of portal inflammation and liver fibrosis.28
Liver protective and anti-inflam-matory drugs to prevent and treat ste-atohepatitis and advanced fibrosis may be considered.29 Essential phospholipids (EPL) is the highly purified fraction of phosphatidylcholine with polyunsaturated fatty acids.30 Phosphatidylcholine is an important structural component of cellular membranes and aids in the breakdown of fats.31 Incorporation of EPL into damaged hepatocyte cell membranes can restore the normal membrane structure. EPL has antioxidant activity and protects against lipid peroxidation, it also has an anti-fibrogenic effect.32 EPL also reduces the interaction between immune effector cells and hepatocytes.33 In a prospective study, EPL was shown to significantly improve the liver bio-chemistry after 8 weeks and reduce the degree of steatosis, necroinflam-mation and fibrosis after 6 months of therapy.34 In a recent longitudinal study of 315 patients, Essentiale-L showed a consistent improvement in both clinical
Figure 1. Ultrasound in diffuse steotosis: Fatty liver may be diagnosed if liver echo-genicity exceeds that of renal cortex and spleen and there is attenuation of the ultrasound wave, loss of definition of the diaphragm, and poor delineation of the intrahepatic architecture
Normal appearance of the liver at US. The echogenicity of the liver is equal to or slightly greater than that of the renal cortex (rc).
Diffuse fat accumulation in the liver at US. The echogenicity of the liver is greater than that of the renal cortex (rc). Intrahepatic vessels are not well depicted. The ultrasound beam is attenuated posteriorly, and the diaphragm is poorly delineated.

JUL 2015 Journal of The Society of Physicians of Hong Kong | 56
and laboratory parameters in patients with fatty liver disease. The decrease in liver enzyme levels from baseline was significant at Days 60 and 90 (p<0.05).35 No known toxicity or serious side effects have been reported.
The knowledge that vitamin E decreases oxidative stress provided a rationale for its evaluation in patients with NASH, and it was shown to signifi-cantly improve global histology scores.36 However, long-term vitamin E supple-mentation has been associated with increased risk of certain types of cancers, bleeding, and haemorrhagic stroke.37
Conclusions• Screening for non-alcoholic fatty liver
disease (NAFLD) should be performed in individuals who are either obese, diabetic or have metabolic syndrome.
• Ultrasonography is the first-line diag-nostic tool for NAFLD.
• Transient elastography, biomarkers and combined scoring systems are non-invasive tools for the diagnosis of hepatic steatosis and injury in NAFLD patients.
• First-line therapy for NAFLD includes weight loss achieved through calorie restriction and/or physical activity.
• Liver protective and anti-inflammatory drugs to prevent and treat steatohep-
atitis and advanced fibrosis may be used. Essential phospholipids, which have no known toxicity or serious side effects, may be considered.
• Treatment with vitamin E cannot be recommended due to uncertain long-term efficacy and safety.
References1. Chalasani N, Younossi Z, Lavine JE, Diehl AM, Brunt EM, Cusi K, et al.
The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology. Gastroenterology 2012;142:1592-609.
2. Brunt EM. Nonalcoholic steatohepatitis: definition and pathology. Semin Liver Dis. 2001;21:3-16.
3. Caldwell SH, Oelsner DH, Iezzoni JC, et al. Cryptogenic cirrhosis: clinical characterization and risk factors for underlying disease. Hepatology 1999; 29:664.
4. Dietrich P, Hellerbrand C. Best Practice & Research Clinical Gastroenterology 2014;28 : 637-653
5. Bosserhoff A, Hellerbrand C. Obesity and fatty liver are ‘grease’ for the machinery of hepatic fibrosis. Dig Dis 2011;29:377-83.
6. Day CP, James OF. Steatohepatitis: a tale of two “hits”? Gastroenterology 1998;114:842-5.
7. Powell EE, Cooksley WG, Hanson R, et al. The natural history of nonalcoholic steatohepatitis: a follow-up study of forty-two patients for up to 21 years. Hepatology 1990; 11:74.
8. Chitturi S, Farrell GC, Hashimoto E, et al. Non-alcoholic fatty liver disease in the Asia-Pacific region: definitions and overview of proposed guidelines. J Gastroenterol Hepatol 2007; 22:778.
9. Wong VW, Chu WC, Wong GL, Chan RS, Chim AM, Ong A, et al. Prevalence of non-alcoholic fatty liver disease and advanced fibrosis in Hong Kong Chinese: a population study using proton-magnetic resonance spectroscopy and transient elastography. Gut 2012;61:409-415
10. Bacon BR, Farahvash MJ, Janney CG, Neuschwander-Tetri BA. Nonalcoholic steatohepatitis: an expanded clinical entity. Gastroenterology 1994; 107:1103.
11. Cohen JA, Kaplan MM. The SGOT/SGPT ratio--an indicator of alcoholic liver disease. Dig Dis Sci 1979; 24:835.
12. Sorbi D, Boynton J, Lindor KD. The ratio of aspartate aminotransferase to alanine aminotransferase: potential value in differentiating nonalcoholic steatohepatitis from alcoholic liver disease. Am J Gastroenterol 1999; 94:1018.
13. Mofrad P, Contos MJ, Haque M, et al. Clinical and histologic spectrum of nonalcoholic fatty liver disease associated with normal ALT values. Hepatology 2003; 37:1286.
14. Festi D, Schiumerini R, Marzi L, Di Biase AR, Mandolesi D, Montrone L, et al. Review article: the diagnosis of nonalcoholic fatty liver disease e availability and accuracy of non-invasive methods. Aliment Pharmacol Ther 2013;37: 392-400.
15. Rofsky NM, Fleishaker H. CT and MRI of diffuse liver disease. Semin Ultrasound CT MR 1995; 16:16.
16. Wong VW, Vergniol J, Wong GL, Foucher J, Chan HL, Le Bail B et al.
Diagnosis of fibrosis and cirrhosis using liver stiffness measurement in nonalcoholic fatty liver disease.Hepatology. 2010;51:454-62.
17. Myers RP, Pomier-Layrargues G, Kirsch R, et al. Feasibility and diagnostic performance of the FibroScan XL probe for liver stiffness measurement in overweight and obese patients. Hepatology 2012; 55: 199–208.
18. de Ledinghen V, Vergniol J, Foucher J,El-Hajbi F, Merrouche W, Rigalleau V. Feasibility of liver transient elastography with FibroScan using a new probe for obese patients. Liver Int 2010; 30: 1043–8.
19. Sasso M, Miette V, Sandrin L, Beaugrand M. The controlled attenuation parameter (CAP): a novel tool for the non-invasive evaluation of steatosis using Fibroscan(®). Clin Res Hepatol Gastroenterol 2012; 36: 13–20.
20. Shen F, Zheng RD, Mi YQ, Wang XY, Pan Q, Chen GY, Cao HX, Chen ML, Xu L, Chen JN, Cao Y, Zhang RN, Xu LM, Fan JG. Controlled attenuation parameter for non-invasive assessment of hepatic steatosis in Chinese patients. World J Gastroenterol. 2014,28;:4702-11.
21. Seeff LB, Everson GT, Morgan TR, et al. Complication rate of percutaneous liver biopsies among persons with advanced chronic liver disease in the HALT-C trial. Clin Gastroenterol Hepatol 2010; 8:877.
22. West J, Card TR. Reduced mortality rates following elective percutaneous liver biopsies. Gastroenterology 2010; 139:1230.
23. Adams LA, Lymp JF, St Sauver J, et al. The natural history of nonalcoholic fatty liver disease: a population-based cohort study. Gastroenterology 2005; 129:113.
24. Söderberg C, Stål P, Askling J, et al. Decreased survival of subjects with elevated liver function tests during a 28-year follow-up. Hepatology 2010; 51:595.
25. Wong VW, Wong GL, Choi PC, Chan AW, Li MK, Chan HY, et al. Disease progression of non-alcoholic fatty liver disease: a prospective study with paired liver biopsies at 3 years.Gut. 2010;59:969-74.
26. Wong VW, Wong GL, Tsang SW, Fan T, Chu WC, Woo J, et al.High prevalence of colorectal neoplasm in patients with non-alcoholic steatohepatitis. Gut 2011;60:829-36.
27. Rafiq N, Bai C, Fang Y, Srishord M, McCullough A, Gramlich T, et al. Long-term follow-up of patients with nonalcoholic fatty liver. Clin Gastroenterol Hepatol 2009;7:234-8.
28. Andersen T, Gluud C, Franzmann MB, Christoffersen P. Hepatic effects of dietary weight loss in morbidly obese subjects. J Hepatol 1991; 12:224.
29. Fan JG, Jia JD, Li YM, Wang BY, Lu LG, Shi JP, Chan LY; Chinese Association for the Study of Liver Disease. Guidelines for the diagnosis and management of nonalcoholic fatty liver disease: update 2010: (published in Chinese on Chinese Journal of Hepatology 2010;18:163-166).J Dig Dis. 2011 ;12:38-44.
30. Kuntz E, Kuntz HD: HEPATOLOGY Springer 2008 page 856-867.31. Phosphatidylcholine (PC): Natural drug information. www.uptodate.com.
Assessed on 26 Dec 2011.32. Cao Q, Mak KM, Lieber CS.Dilinoleoylphosphatidylcholine prevents
transforming growth factor-beta1-mediated collagen accumulation in cultured rat hepatic stellate cells.J Lab Clin Med. 2002 ;139:202-10.
33. Neuberger J, Hegarty JE, Eddleston AL, Williams R.Effect of polyunsaturated phosphatidylcholine on immune mediated hepatocyte damage.Gut. 1983 ;24:751-5.
34. Dinakaran. Safety and efficacy of Essentiale-L on the treatment of non-alcoholic fatty liver disease. Indian J of Clinical Practice. 2003;7:51-58.
35. Padma L, Qayum Mukaddam, Abhijit Trailokya. An Observational Study of Essentiale-L in the Treatment of Patients with Fatty Liver Disease. Indian Journal of Clinical Practice, 2013 ;23: 735-739.
36. Sanyal AJ, Chalasani N, Kowdley KV, et al. Pioglitazone, vitamin E, or placebo for nonalcoholic steatohepatitis. N Engl J Med 2010; 362:1675.
37. Schürks M, Glynn RJ, Rist PM, Tzourio C, Kurth T. Effects of vitamin E on stroke subtypes: meta-analysis of randomized controlled trials. BMJ 2010;341:c5702.
CENTRAL DOCTORS STUDY GROUP
(For doctors working in Central)
Monthly CME meeting and lunch at Yung Kee RestaurantIf you are interested to receive the circular,
please send your name card to Dr Charles Ng at [email protected]

Sanofi Adv

JSPHK July 2015 issue Page 45 – Idiopathic Pulmonary Fibrosis: A Novel Medication for an Untreatable Disease Dr Wong Wai Leung (王偉樑醫生)
References:
1. G Raghu, H Collard. An Official ATS/ERS/JRS/ALAT statement: Idiopathic pulmonary fibrosis: Evidence‐based guidelines for diagnosis and management. Am J Respir Crit Care Med 2011;183:788‐824
2. L Nalysnyk, J Cid‐Ruzafa. Incidence and prevalence of idiopathic pulmonary fibrosis: review of the literature. Eur Respir Rev 2012;21:126,355‐361
3. L Wollin, E Wex. Mode of action of nintedanib in the treatment of idiopathic pulmonary fibrosis. Eur Respir J 2015;45:1434‐1445
4. L Richeldi, U Costabel. Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis. N Engl J Med 2011;365:1079‐87
5. L Richeldi, R M Du Bois. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. N Engl J Med. 2014;370:2071‐82
6. Food Drug Administration website. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm418994.htm
7. European Medicines Agency. http://www.ema.europa.eu