journal of clinical gerontology & geriatrics · this paper reports on a retrospective chart...
TRANSCRIPT

at SciVerse ScienceDirect
Journal of Clinical Gerontology & Geriatrics 4 (2013) 128e131
Contents lists available
Journal of Clinical Gerontology & Geriatrics
journal homepage: www.e- jcgg.com
Case report
Malignant otitis externa: An emerging scourge
S. Prasanna Kumar*, A. Ravikumar, MS, DNB, DLORCS, MAMS,L. Somu, MS, Nazrin Mohd Ismail, MBBSDepartment of ENT, Head, and Neck Surgery, Sri Ramachandra Medical College and Research Institute, Porur, Chennai 38, India
a r t i c l e i n f o
Article history:Received 23 October 2012Received in revised form12 February 2013Accepted 28 February 2013
Keywords:ElderlyDiabetesMalignant otitis externaMicroabscessesSequestrum
* Corresponding author. Department of ENT, Headachandra Medical College and Research Institute, Por
E-mail address: [email protected] (S
2210-8335 Copyright � 2013, Asia Pacific League of Chttp://dx.doi.org/10.1016/j.jcgg.2013.02.003
a b s t r a c t
Malignant otitis externa is an emerging problem in developing countries. We are seeing an increase inthis condition in elderly people with diabetes. This paper reports on a retrospective chart review of 18patients with malignant otitis externa in a tertiary care center. We have comprehensively discussed theclinical features, diagnosis, and management of this disease. Malignant otitis externa is suspected inhigh-risk patients, i.e., elderly individuals with diabetes, immunocompromised, and immunosuppressedpatients. Early and prolonged use of appropriate antimicrobials will reduce the morbidity and mortalityassociated with this condition. The role of surgery is limited to biopsy, the draining of microabscesses, orthe removal of sequestrum.Copyright � 2013, Asia Pacific League of Clinical Gerontology & Geriatrics. Published by Elsevier Taiwan
LLC. Open access under CC BY-NC-ND license.
1. Introduction
Malignant otitis externa (MOE) is a rare, rapidly spreading, life-threatening invasive infection of the external auditory canal andthe lateral skull base. Toulmouche is credited with first describingthis condition.1 Meltzer and Kelemen reported a case of pyocyaneusosteomyelitis of the temporal bone, mandible and zygoma, which isbelieved to be the first report of this condition in modern litera-ture.2 Chandler coined the term “malignant external otitis” anddescribed the clinical characteristics of this disease.3 Necrotizingotitis externa and skull base osteomyelitis are the other terms usedto describe this condition.
The incidence of MOE has increased in recent times. This may beattributed to an increase in awareness of the disease, better diag-nostic modalities, and an increase in the geriatric and diabeticpopulation in India.4 MOE was initially described as a disease of anelderly patient with diabetes.3 Since then, this entity has beendescribed by many in the geriatric population. The geriatric pop-ulation is more prone to cleaning their ears due to dry and itchyskin. In addition, diabetes alters the pH of the external auditorycanal and predisposes people to infection by altering the immuneresponse. MOE, although rare, has been reported in the immuno-suppressed and in children.
, and Neck Surgery, Sri Ram-ur, Chennai 38, India.. Prasanna Kumar).
linical Gerontology & Geriatrics. P
The awareness and understanding of this disease has changedthe way in which it is being dealt with. In this article, we retro-spectively audit the case records of patients diagnosed with, andmanaged for, malignant otitis externa.
2. Case series
The case records of 18 patients diagnosed as having malignantotitis externa and managed by the senior author or under his su-pervision over a period of 4 years from 2008 to 2011 were includedin the study. This study was carried out in the department of Ears,Nose, and Throat, Head, and Neck surgery of a tertiary care hospitalin South India. The descriptive data noted were age, sex, comorbidconditions, symptoms and signs at presentation, investigation done(including bacterial culture, fungal smear, and culture), treatment(antibiotics given, route, and duration), adverse events, complica-tions, and outcome. All these datawere summarized, tabulated, andanalyzed as shown in Table 1. (Initially a clinical diagnosis of MOEwasmade in 23 patients, but because biopsy of granulations provedto be malignant in five patients, they were excluded from theseries).
3. Discussion
MOE is a rapidly spreading infection, which originates at thebony cartilaginous junction of the external auditory canal. Its eti-ology is attributed to infection after trivial trauma, such as that of
ublished by Elsevier Taiwan LLC. Open access under CC BY-NC-ND license.

Table 1Details of the demographics, clinical, and microbiological outcomes of 18 patientstreated for malignant otitis externa in the tertiary care hospital.
Age at diagnosis(mean � SD)
62 � 8.5 years
Sex, male:female 8:1Ear affected (right:left) 1:1Comorbid condition Diabetes mellitus (100),
chronic kidney disease (30)Cranial nerves involvedFacial nerve only (VII) 12/18 (66.6)Multiple cranial nerves
(VII, IX,X and XII)3/18 (16.6)
Presenting symptoms Ear ache (nocturnal; 100)Persistent ear discharge (100)Facial weakness (66.6)Duration of symptoms lasting 45 days (average)
Presenting signs Ear discharge (100)External auditory canal (EAC) granulation (100)Tenderness EAC inferiorly (100)Facial weakness (66.6)
Organism isolateda Bacteria:� Pseudomonas aeruginosa, 9/18 (50)� Staphylococcus aureus, 4/18 (22)� Enterococcus faecalis, 1/18 (5.5)
Fungi:� Aspergillus fumigatus, 2/18 (11)� Candida albicans, 1/18 (5.5)
Polymicrobial:� P. aeruginosa þ A. fumigates, 2/18� S. aureus þ C. albicans, 1/18� S. aureus þ E. faecalis, 1/18� P. aeruginosa þ S. aureus, 1/18
No growth, 6/18 (33)Biopsyb Done in 8 cases to rule out malignancy in
suspected malignant otitis externa sentfor histopathological examination:� Squamous cell carcinoma (malignancy)in 5 patients (excluded from the series)
� Nonspecific chronic inflammatorychanges in 3 patients
TreatmentMedical Initial intravenous antimicrobial given:
Piperacillin-tazobactam, 8/18Ciprofloxacin, 4/18Cefoperazone-sulbactum, 3/18Linezolid, 1/18Amphotericin B, 2/18
Followed by oral antibiotics:CiprofloxacinCefpodoximeCefiximeItraconazole
Surgical Biopsy 3/18; microabscess, 1/18;sequestrum 1/18
Status (post-treatment) 15 complete recoveries2 relapses2 mortalites
Data are presented as n (%).a 5 patients had polymicrobial infection that was isolated on culture and
sensitivity.b Biopsy was taken in all suspected cases of malignant otitis externa not
responding to treatment or on clinical suspicion. All 5 cases that had evidence ofmalignancy on histopathological examination were excluded from the series.
Fig. 1. Granulation in the external auditory canal.
S. Prasanna Kumar et al. / Journal of Clinical Gerontology & Geriatrics 4 (2013) 128e131 129
aural irrigation or ear pricking.5 It starts as cellulites of the deepperiauricular tissue that subsequently spreads through the fissuresof Santorini to the adjoining skull base, causing periostitis, osteitis,chondritis, osteomyelitis and, eventually, multiple cranial nervepalsies.
Elderly people with diabetes are more prone to MOE. It is welldocumented that diabetes causes endarteritis and micro-angiopathy, leading to hypoperfusion in the subcutaneous tissue.6
Diabetes reduces the chemotactic and bactericidal activity of
human polymorphonuclear leukocytes. It also causes immunedysfunction and poor granulocyte function, which is believed toprolong the disease.7,8 Driscoll et al. have suggested that theincreased pH of the cerumen in patients with diabetes may be acontributing factor.9
In our study, the average age at diagnosis of MOE was 62 � 8.5years. All of the patients had uncontrolled type 2 diabetes mellitus.Of these, 25% had coexisting chronic kidney disease. MOE, althoughrare, has been reported in childrenwho are immunodeficient, thoseundergoing chemotherapy, or in transplantees who are on immu-nosuppressive therapy.10e12 Others who are at risk are thosesuffering from malnutrition and HIV.13,14
Diagnosis of MOE requires a high index of suspicion. There areno universally accepted specific criteria.11 The presence of persis-tent pain out of proportion to changes seen at otoscopy, purulentotorrhea with granulations, and resistance to local therapy for atleast 8e10 days are highly suggestive of MOE. The presence oflower cranial nerve palsy (VII, IX, X, XI, and XII) points to the spreadof disease to the skull base and is also an indicator of the extent andprognosis of the disease.
As shown in Table 1, the most common presenting symptom inour patients was persistent nocturnal otalgia and ear discharge inall patients. Two-thirds of patients presented with facial weakness.All of these patients had granulation in the external auditory canal(Fig. 1). Three patients had multiple cranial nerve palsy, withinvolvement of IX, X, and XII along with VII nerve palsy (Fig. 2).
Sterile swabs from the affected ear are necessary to identify theorganism. It is a practice in our institution to send a sterile swab forGram staining, bacterial culture, and fungal smear and culture,which is processed within 30 minutes to enhance the yield. Theseinvestigations are vital, as early therapy with appropriate antibi-otics is essential in achieving good cure rates and reduce themorbidity and mortality known to be associated with this disease.The most common causative organism implicated in MOE isPseudomonas aeruginosa.3,15 Staphylococcus aureus, particularlymethicillin-resistant S. aureus, Staphylococcus epidermidis, Proteus,and Klebsiella are the other bacteria implicated.16e19 Aspergillusniger, Aspergillus fumigatus, and Candida species are the commonfungi reported.20,21 It is not knownwhether fungi are the causativeagent or if they only alter the outcome in the management ofMOE. In our study, the most common organisms were P. aeruginosa(50%, 9/18), S. aureus (22%, 4/18), and Enterococcus faecalis (5.5%,1/18). Fungal potassium hydroxide (KOH) smearwas positive in 27%

Fig. 4. Computed tomography scan of the skull base showing a homogeneous softtissue shadow 2.4 cm � 1.5 cm with bone erosion extending from the right petroustemporal bone and carotid canal (arrows).
Fig. 2. A patient with multiple cranial nerve deficits. VII and XII nerve palsy is shown.
S. Prasanna Kumar et al. / Journal of Clinical Gerontology & Geriatrics 4 (2013) 128e131130
(5/18) of patients. A. fumigatus was isolated in two patients (11%),and Candida was isolated in one patient.
There was no growth in 33% of cases (6/18). This may be due tothe fact that these patients who had already been treated at otherhospitals prior to being referred to us were given oral/intravenous/topical antibiotics and this might have led to us not being able toisolate the organism in culture. All of these patients were empiri-cally treated with antipseudomonal antibiotics by us and theyresponded well to treatment. It is emphasized at this stage thatmicrobiological samples should be taken to identify the organismsprior to starting on antimicrobial therapy. Twenty-seven per cent(5/18) of patients with MOE had polymicrobial infection. Allpatients in whom fungi were isolated also had positive bacterialisolates on culture.
High-resolution computed tomography (CT) scan and/or mag-netic resonance imaging of the temporal bone are a useful adjunctto clinical diagnosis (Figs. 3 and 4). A high-resolution CT scan of thetemporal bone is the initial imaging modality of choice. It is
Fig. 3. Computed tomography scan of the skull base, axial section, showing erosion ofthe skull base and adjoining clivus (arrows).
economical, fast, and also helps in localizing the anatomical limitand bony involvement. This modality of imaging is not useful inmonitoring resolution of osteomyelitis because bone reminerali-zation takes time and does not reflect the progress of disease.22
Magnetic resonance imaging is useful in monitoring the extent ofsoft tissue swelling and also the intracranial extent of disease.22
Radioisotope scans (technetium 99/gallium 67) are useful inassessing MOE. Gallium 67 is a very sensitive, but nonspecific test,detecting and binding to actively-dividing cells. Serial scans can bedone to monitor treatment response and thus help in assessing theduration of antibiotic therapy.
Treatment involves a multidisciplinary approach, with treat-ment planned and discussed with the specialist concerned.Aggressive and adequate control of diabetes, the correction of
Fig. 5. Post-treatment improvement in facial nerve function of the same patientshown in Fig. 2.
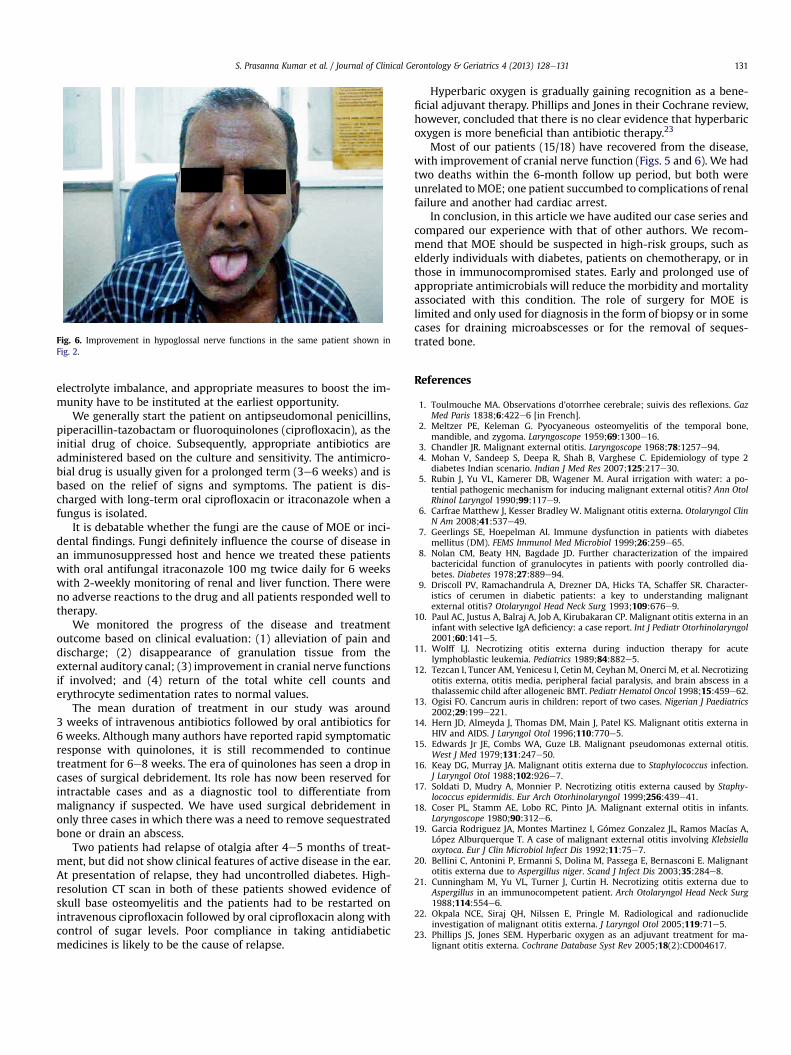
Fig. 6. Improvement in hypoglossal nerve functions in the same patient shown inFig. 2.
S. Prasanna Kumar et al. / Journal of Clinical Gerontology & Geriatrics 4 (2013) 128e131 131
electrolyte imbalance, and appropriate measures to boost the im-munity have to be instituted at the earliest opportunity.
We generally start the patient on antipseudomonal penicillins,piperacillin-tazobactam or fluoroquinolones (ciprofloxacin), as theinitial drug of choice. Subsequently, appropriate antibiotics areadministered based on the culture and sensitivity. The antimicro-bial drug is usually given for a prolonged term (3e6 weeks) and isbased on the relief of signs and symptoms. The patient is dis-charged with long-term oral ciprofloxacin or itraconazole when afungus is isolated.
It is debatable whether the fungi are the cause of MOE or inci-dental findings. Fungi definitely influence the course of disease inan immunosuppressed host and hence we treated these patientswith oral antifungal itraconazole 100 mg twice daily for 6 weekswith 2-weekly monitoring of renal and liver function. There wereno adverse reactions to the drug and all patients responded well totherapy.
We monitored the progress of the disease and treatmentoutcome based on clinical evaluation: (1) alleviation of pain anddischarge; (2) disappearance of granulation tissue from theexternal auditory canal; (3) improvement in cranial nerve functionsif involved; and (4) return of the total white cell counts anderythrocyte sedimentation rates to normal values.
The mean duration of treatment in our study was around3 weeks of intravenous antibiotics followed by oral antibiotics for6 weeks. Although many authors have reported rapid symptomaticresponse with quinolones, it is still recommended to continuetreatment for 6e8 weeks. The era of quinolones has seen a drop incases of surgical debridement. Its role has now been reserved forintractable cases and as a diagnostic tool to differentiate frommalignancy if suspected. We have used surgical debridement inonly three cases in which there was a need to remove sequestratedbone or drain an abscess.
Two patients had relapse of otalgia after 4e5 months of treat-ment, but did not show clinical features of active disease in the ear.At presentation of relapse, they had uncontrolled diabetes. High-resolution CT scan in both of these patients showed evidence ofskull base osteomyelitis and the patients had to be restarted onintravenous ciprofloxacin followed by oral ciprofloxacin along withcontrol of sugar levels. Poor compliance in taking antidiabeticmedicines is likely to be the cause of relapse.
Hyperbaric oxygen is gradually gaining recognition as a bene-ficial adjuvant therapy. Phillips and Jones in their Cochrane review,however, concluded that there is no clear evidence that hyperbaricoxygen is more beneficial than antibiotic therapy.23
Most of our patients (15/18) have recovered from the disease,with improvement of cranial nerve function (Figs. 5 and 6). We hadtwo deaths within the 6-month follow up period, but both wereunrelated toMOE; one patient succumbed to complications of renalfailure and another had cardiac arrest.
In conclusion, in this article we have audited our case series andcompared our experience with that of other authors. We recom-mend that MOE should be suspected in high-risk groups, such aselderly individuals with diabetes, patients on chemotherapy, or inthose in immunocompromised states. Early and prolonged use ofappropriate antimicrobials will reduce the morbidity and mortalityassociated with this condition. The role of surgery for MOE islimited and only used for diagnosis in the form of biopsy or in somecases for draining microabscesses or for the removal of seques-trated bone.
References
1. Toulmouche MA. Observations d’otorrhee cerebrale; suivis des reflexions. GazMed Paris 1838;6:422e6 [in French].
2. Meltzer PE, Keleman G. Pyocyaneous osteomyelitis of the temporal bone,mandible, and zygoma. Laryngoscope 1959;69:1300e16.
3. Chandler JR. Malignant external otitis. Laryngoscope 1968;78:1257e94.4. Mohan V, Sandeep S, Deepa R, Shah B, Varghese C. Epidemiology of type 2
diabetes Indian scenario. Indian J Med Res 2007;125:217e30.5. Rubin J, Yu VL, Kamerer DB, Wagener M. Aural irrigation with water: a po-
tential pathogenic mechanism for inducing malignant external otitis? Ann OtolRhinol Laryngol 1990;99:117e9.
6. Carfrae Matthew J, Kesser Bradley W. Malignant otitis externa. Otolaryngol ClinN Am 2008;41:537e49.
7. Geerlings SE, Hoepelman AI. Immune dysfunction in patients with diabetesmellitus (DM). FEMS Immunol Med Microbiol 1999;26:259e65.
8. Nolan CM, Beaty HN, Bagdade JD. Further characterization of the impairedbactericidal function of granulocytes in patients with poorly controlled dia-betes. Diabetes 1978;27:889e94.
9. Driscoll PV, Ramachandrula A, Drezner DA, Hicks TA, Schaffer SR. Character-istics of cerumen in diabetic patients: a key to understanding malignantexternal otitis? Otolaryngol Head Neck Surg 1993;109:676e9.
10. Paul AC, Justus A, Balraj A, Job A, Kirubakaran CP. Malignant otitis externa in aninfant with selective IgA deficiency: a case report. Int J Pediatr Otorhinolaryngol2001;60:141e5.
11. Wolff LJ. Necrotizing otitis externa during induction therapy for acutelymphoblastic leukemia. Pediatrics 1989;84:882e5.
12. Tezcan I, Tuncer AM, Yenicesu I, Cetin M, Ceyhan M, Onerci M, et al. Necrotizingotitis externa, otitis media, peripheral facial paralysis, and brain abscess in athalassemic child after allogeneic BMT. Pediatr Hematol Oncol 1998;15:459e62.
13. Ogisi FO. Cancrum auris in children: report of two cases. Nigerian J Paediatrics2002;29:199e221.
14. Hern JD, Almeyda J, Thomas DM, Main J, Patel KS. Malignant otitis externa inHIV and AIDS. J Laryngol Otol 1996;110:770e5.
15. Edwards Jr JE, Combs WA, Guze LB. Malignant pseudomonas external otitis.West J Med 1979;131:247e50.
16. Keay DG, Murray JA. Malignant otitis externa due to Staphylococcus infection.J Laryngol Otol 1988;102:926e7.
17. Soldati D, Mudry A, Monnier P. Necrotizing otitis externa caused by Staphy-lococcus epidermidis. Eur Arch Otorhinolaryngol 1999;256:439e41.
18. Coser PL, Stamm AE, Lobo RC, Pinto JA. Malignant external otitis in infants.Laryngoscope 1980;90:312e6.
19. Garcia Rodriguez JA, Montes Martinez I, Gómez Gonzalez JL, Ramos Macías A,López Alburquerque T. A case of malignant external otitis involving Klebsiellaoxytoca. Eur J Clin Microbiol Infect Dis 1992;11:75e7.
20. Bellini C, Antonini P, Ermanni S, Dolina M, Passega E, Bernasconi E. Malignantotitis externa due to Aspergillus niger. Scand J Infect Dis 2003;35:284e8.
21. Cunningham M, Yu VL, Turner J, Curtin H. Necrotizing otitis externa due toAspergillus in an immunocompetent patient. Arch Otolaryngol Head Neck Surg1988;114:554e6.
22. Okpala NCE, Siraj QH, Nilssen E, Pringle M. Radiological and radionuclideinvestigation of malignant otitis externa. J Laryngol Otol 2005;119:71e5.
23. Phillips JS, Jones SEM. Hyperbaric oxygen as an adjuvant treatment for ma-lignant otitis externa. Cochrane Database Syst Rev 2005;18(2):CD004617.