jonathan t. bravman, md cu sports medicine division of sports medicine and shoulder surgery...
TRANSCRIPT

Obesity and OsteoarthritisMore than just wear and tear
Jonathan T. Bravman, MDCU Sports MedicineDivision of Sports Medicine and Shoulder SurgeryUniversity of Colorado Department of Orthopedics Denver, Colorado

Basis of the talk
Journal of the American Academy of Orthopaedic Surgery, March 2013

Purpose
Present data available in 2013 regarding: The effect of obesity on osteoarthritis The effect of weight loss and exercise for
treatment of osteoarthritis in obese patients
The traditional orthopaedic approach to obesity

Obesity and Osteoarthritis
OA
Biomechanical
Theories
Systemic Theories
Osteoarthritis is strongly correlated with high BMI

The Biomechanical Theories
The intuitive theoriesMost studies involve the kneeSurprising lack of data to support
them (presented evidence here is weak)
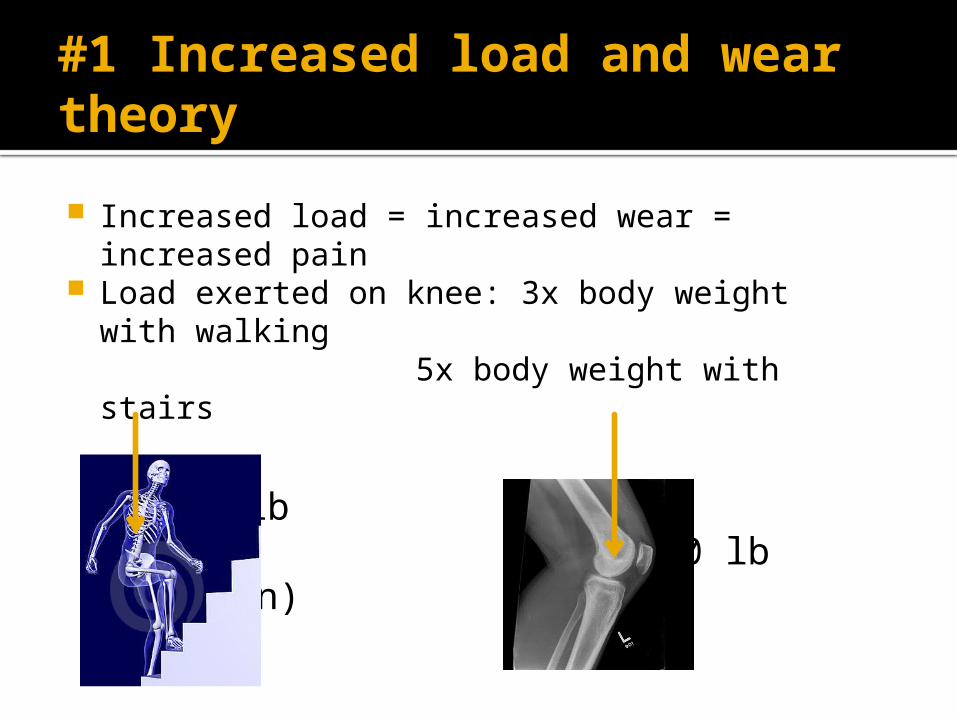
#1 Increased load and wear theory
Increased load = increased wear = increased pain
Load exerted on knee: 3x body weight with walking
5x body weight with stairs
200 lb 1000 lb (1/2 ton)
=

Increased load and wear
Obesity increases subchondral bone density and stiffness
Load is redistributed on cartilage causing increased wear

#2 Muscular deconditioning theory
Obese are generally deconditioned Relative quadriceps weakness, muscle
imbalance, and impaired control have been observed in adults with OA vs. none
Decreased muscle mass is associated with increased knee cartilage (Arthritis Rheum. 2005 Feb;52(2):461-7)
Reduced muscle strength relative to body weight causes early quadriceps fatigue in the obese: Reduced shock attenuation Increased loading Increased WEAR Increased variability in loading

BMI is associated with severity of joint space narrowing of the knee in varus malalignment (but not valgus)
Increased adduction moment increases medial compartment wear
Adduction moment increases with age in the obese but not in normal-weight individuals
#3 Malalignment causes increased wear theory

Malalignment smaller role than originally thought mediates other risk factors such as
obesity “The clinician should focus on what is
definitively modifiable…obesity, in particular”

Systemic Effects of Obesity Less intuitive, newer, possibly more important Adipose tissue is not just an energy depot White adipose tissue = immunologically active
organ Cytokines: small cell-signaling peptides Adipokines: pro-inflammatory cytokines
derived primarily from adipose tissue

The Adipokine Family
Important members: Leptin Resistin Adiponectin Visfatin
Active in cartilage regulationExact role of each is unclear but
many studies are currently underway

Leptin Present in synovial fluid of joints with OA levels in both synovial fluid and plasma
correlate closely with BMI Marked expression in OA cartilage and
osteophytes compared to minimal in normal cartilage
First to suggest that leptin plays an important role in pathophysiology of OA

Leptin paved the way for adipokines
Acts on hypothalamus to decrease food intake and increase energy expenditure
Closely linked to the immune systemSynovial fluid levels strongly linked
to radiographic severity of OA!!

Cartilage taken from TKA proceduresLeptin upregulated multiple MMPs in
cartilageLeptin levels correlate with multiple
MMPs in synovial fluid from OA pts
Conclusion: Leptin has a catabolic effect in OA joints

Adiponectin
Adipocyte-derived hormone with known anti-diabetic and anti-atherogenic properties
Found in OA synovial fluid and chondrocytes
Upregulates TIMP-2 and downregulates MMP-13
Researchers feel it is critically involved in pathogenesis of OA

Hand xrays compared at baseline and 6 years
Serum adipokines measured at baseline
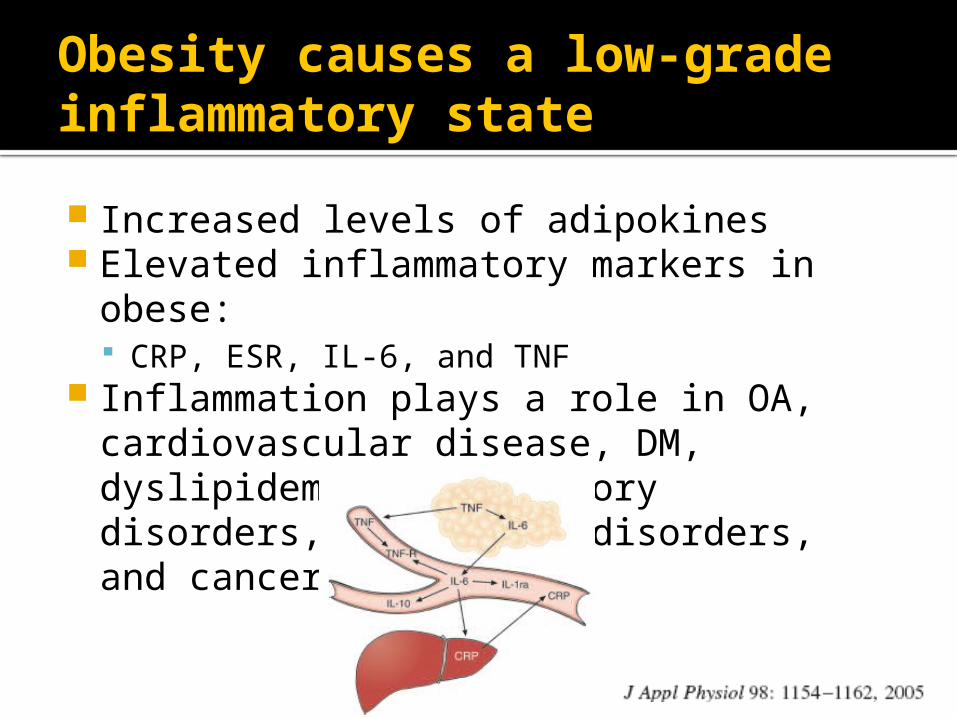
Obesity causes a low-grade inflammatory state
Increased levels of adipokines Elevated inflammatory markers in obese:
CRP, ESR, IL-6, and TNF Inflammation plays a role in OA,
cardiovascular disease, DM, dyslipidemia, respiratory disorders, autoimmune disorders, and cancer

Development of OA is both mechanical and metabolic
Mechanoreceptors on chondrocyte surfaces may detect obesity load and trigger intracellular signaling cascades
Adiposity is highly metabolic and inflammatory
Development of OA appears strongly correlated with disordered glucose and lipid metabolism
Adipokines may cause direct cartilage degredation
Is OA an inflammatory arthropathy?

Leptin and adiponectin are key mediators in inducing cartilage breakdown
Work with MMPs, nitric oxide, and interleukins
Therapeutic targets for OA treatment??

The Metabolic Syndrome
“a cluster of conditions…that occur together increasing your risk of heart disease, stroke, and diabetes”1. excess body fat around the waist2. increased blood pressure3. elevated insulin levels4. abnormal cholesterol levels
Being overweight and inactive are “major contributors”
Treatment: exercise, weight loss, eat healthy, and stop smoking

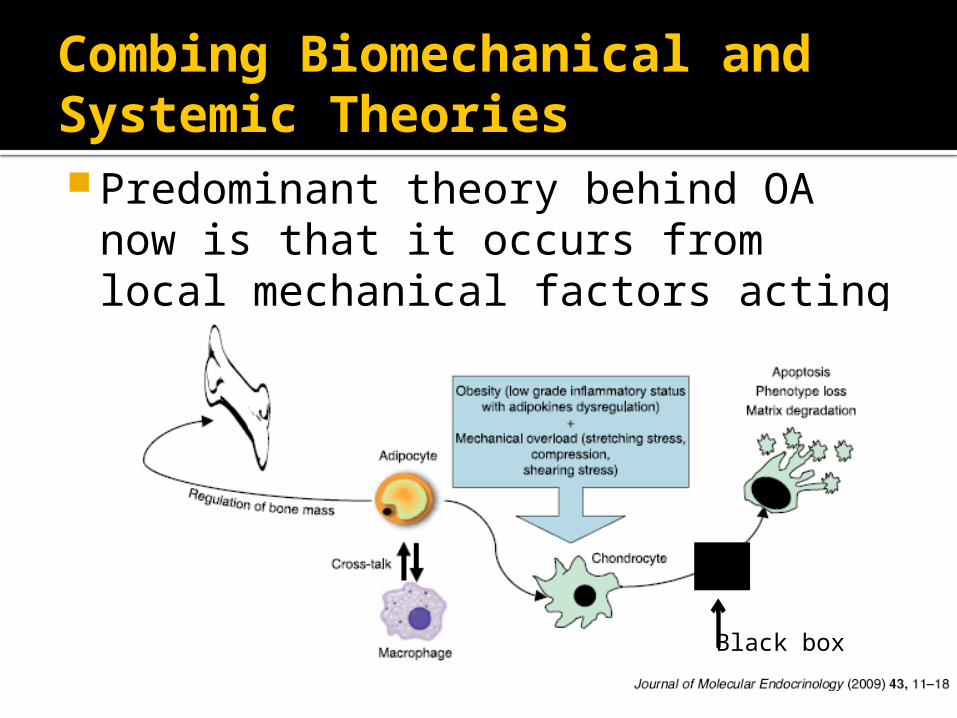
Combing Biomechanical and Systemic TheoriesPredominant theory behind OA now
is that it occurs from local mechanical factors acting in the context of systemic susceptibility
Black box

MSK pain in the obese patient Obesity and overweight are associated
with increased musculoskeletal pain The impact of pain on functional status
and health-related quality of life is greater in the the obese
The metabolic syndrome is associated with chronic pain
Central obesity is the metabolic syndrome component most directly associated with pain (beyond OA or neuropathy)

There is a strong relationship:
obesity depression
55%
58%

The question:
Is the patient’s knee pain caused by obesity or osteoarthritis or both?
How do we figure this out? 1. Weight loss trial2. Surgical trial (knee scope vs. TKA)
Is the risk of surgery justifiable to answer this?

Weight Loss as a Treatment for Joint Pain
Weight loss is difficult for physician and patient
Unfortunately, few studies have looked at MSK outcomes after weight loss: Wt loss reduces risk of symptomatic OA Bariatric surgery: decreases overall joint
pain

48 morbidly obese subjects → bariatric surg
Lost avg 90 lbs
MSK pain complaints:
100% preop 23% postop

Few new risk factors for OA have been identified in the past few years
The only 2 modifiable risk factors with sufficient evidence to support intervention for preventing OA: Weight loss Avoiding traumatic injury

Myokines: the anti-inflammatory effect of exercise
Exercise increases production of myokines from muscles → induces lypolysis + inhibits TNF + decreases insulin resistance

Summary
• Obesity is an epidemic in the US• Osteoarthritis is not just “wear and tear” and
adipose tissue is not just an energy storage organ• The medical risk:benefit ratio for weight loss in
obese patients approaches ZERO• Orthopaedic surgery is not a cure for obesity, but
weight loss has potential to cure orthopaedic conditions

Thank You References available:
Talk to him…please
Jonathan T. Bravman, MD