john j. gallagher , rn, msn, ccns, ccrn, rrt - aacn · pdf filejohn j. gallagher , rn, msn,...
TRANSCRIPT

375375
AACN Advanced Critical Care Volume 25 , Number 4 , pp 375 - 386
© 2014 AACN
DOI: 10.1097/NCI.0000000000000059
Management of Blunt Pulmonary Injury John J. Gallagher , RN, MSN, CCNS, CCRN, RRT
John J. Gallagher is Clinical Nurse Specialist/Trauma Program Manager, Hospital of the University of Pennsylvania, 3400 Spruce St, Philadelphia, PA 19104 ( [email protected] ).
The author declares no conflicts of interest.
Introduction Chest trauma accounts for 25% of all civilian deaths due to trauma, second only to severe head injury. 1 The thoracic cavity contains mul-tiple organ systems that may be injured, including the pulmonary, cardiovascular, digestive, and musculoskeletal systems. Rapid and systematic evaluation of the patient to identify and manage these injuries is essential to reduce associated death and disability. Inju-ries of the pulmonary system must be identi-fied in the initial assessment, because they can be immediately life-threatening. 1–5 Similar to other traumatic injuries, chest trauma results from both blunt and penetrating mechanisms of injury. Penetrating injuries include stab or gunshot wounds as well as impalement. Blunt injuries result from falls, motor vehicle or motorcycle crashes, pedestrian/vehicle colli-sions, explosions, and other blunt force mech-anisms. 3–5 Blunt chest injuries may be more challenging to identify, as external evidence of injury may not indicate the degree of underly-ing organ injury. 1 , 4 , 5 Blunt pulmonary injuries
are a prime example of this complexity. The identification and management of these inju-ries are the focus of this article.
Scope of Injury Blunt pulmonary injuries are caused by a trans-fer of force to the thoracic cavity that injures underlying structures. The bony thorax (ribs and sternum), pleural space, intrathoracic airways, and the lung parenchyma may be injured. These injuries may occur singularly or in combination, depending on the underlying mechanism. 1 , 3–5 For the purpose of this discus-sion, the focus is primarily on blunt injuries that involve the pleural space, airways, and lung.
ABSTRACT Thoracic injuries account for 25% of all civil-ian deaths. Blunt force injuries are a subset of thoracic injuries and include injuries of the tracheobronchial tree, pleural space, and lung parenchyma. Early identification of these injuries during initial assessment and resuscitation is essential to reduce associ-ated morbidity and mortality rates. Manage-ment of airway injuries includes definitive airway control with identification and repair of tracheobronchial injuries. Management of pneumothorax and hemothorax includes pleural space drainage and control of ongo-ing hemorrhage, along with monitoring for
complications such as empyema and chylo-thorax. Injuries of the lung parenchyma, such as pulmonary contusion, may require sup-port of oxygenation and ventilation through both conventional and nonconventional mechanical ventilation strategies. General strategies to improve pulmonary function and gas exchange include balanced fluid resuscitation to targeted volume-based resuscitation end points, positioning ther-apy, and pain management. Keywords: chest trauma , hemothorax , pneu-mothorax , pulmonary contusion , tracheo-bronchial injury
Copyright © 2014 American Association of Critical-Care Nurses. Unauthorized reproduction of this article is prohibited.
NCI-D-14-00039-Online.indd 375NCI-D-14-00039-Online.indd 375 21/10/14 2:53 PM21/10/14 2:53 PM

WWW.AACNADVANCEDCRITICALCARE.COM GALLAGHER
376
Injuries Involving the Pleural Space
Pneumothorax Blunt force injuries of the chest may result in collection of air (pneumothorax), blood (hemo-thorax), or a combination of the 2 within the pleural space. Pneumothorax occurs primarily when the lung is lacerated by the ribs or when the lung is compressed, which causes a disrup-tion of the lung’s integrity and allows air to col-lect between the parietal and visceral pleura. In some cases, the pneumothorax may be rela-tively small, and evaluation with serial chest radiographs (CXRs) may be preferable to place-ment of a chest tube. 3 , 6 , 7 Patients may complain of chest pain as a result of air in the pleural space and associated rib fractures. Diminished breath sounds and subcutaneous emphysema may be noticeable, but respiratory distress may not be present. These patients are usually moni-tored for worsening respiratory distress, along with having serial CXRs, to detect expansion of the pneumothorax and potential need for chest tube placement. For patients who require posi-tive pressure ventilation (PPV) and/or general anesthesia, the decision may be made to insert a chest tube, as a pneumothorax can expand under PPV, resulting in a tension pneumotho-rax. However, more recent data support obser-vation of stable patients with pneumothorax who require PPV. 3 , 6 , 8
In some cases, pneumothorax may not be present on the initial CXR before or immedi-ately after intubation. After a period of PPV, a pneumothorax may be detected on repeat films or during computed tomography (CT) of the chest. Such an occult pneumothorax occurs in approximately 5% to 15% of patients with blunt injury. 7 , 9–14 Of those with an occult pneu-mothorax, approximately 10% require chest tube placement. 8 Ongoing evaluation for devel-opment of physiological changes indicating a tension pneumothorax is essential. Reduction in oxygen saturation, increases in peak inspira-tory pressure, and unexplained hypotension should prompt suspicion of tension pneumo-thorax.
Tension Pneumothorax Tension pneumothorax can occur as air rapidly collects in the pleural space around the injured lung. The increasing pressure compresses the mediastinal structures, shifting them to the side opposite the injury, ultimately compressing the
uninjured lung. Clinically, the patient may exhibit decreased or absent breath sounds on the injured side and palpable subcutaneous emphysema across the chest, with a tracheal shift from midline to the uninjured side as a late finding. High peak inspiratory pressures may develop in patients undergoing mechani-cal ventilation, triggering ventilator alarms for high pressure and low tidal volume/minute ventilation. Compression of the heart and great vessels reduces cardiac preload and increases afterload, causing obstructive shock. Back pressure on the venous system results in jugular vein distention if adequate blood volume is pre-sent in the intravascular space. Tachycardia and hypotension deteriorating into cardiac arrest may be manifested as pulseless electrical activity. If an arterial catheter is present, the waveform may become dampened or flat. 2 , 3 , 8
Treatment of Tension Pneumothorax Tension pneumothorax is rapidly fatal and requires immediate intervention. Rapid needle decompression with a large 16- or 14-gauge, 2.25-inch (5.7-cm) peripheral venous catheter inserted into the second or third rib intercostal space at the midclavicular line should be per-formed immediately to relieve the tension pneumothorax. This needle decompression should be followed by insertion of a chest tube. In patients who arrive in cardiac arrest after blunt traumatic injury, bilateral needle decom-pression followed by bilateral placement of chest tubes may be undertaken as part of the initial assessment and interventions. 2 , 3
Chest tube size depends on the size of the patient and on the condition being treated. In trauma resuscitation, larger tubes such as 32F or 36F are often placed on the basis of findings on initial physical examination rather than CXR. 2 , 3 , 8 Because the underlying condition may be either pneumothorax or hemothorax, a larger tube will facilitate rapid drainage of blood with less potential for tube occlusion. Decisions to place smaller chest tubes may be made depending on radiological findings and the patient’s condition. In trauma patients, the chest tube is usually placed at the fourth or fifth rib intercostal space between the anterior and midaxillary line. 2
In most cases, a chest tube inserted and connected to a negative-pressure chest drainage unit will result in reexpansion of the lung. Intermittent bubbling in the water seal chamber
Copyright © 2014 American Association of Critical-Care Nurses. Unauthorized reproduction of this article is prohibited.
NCI-D-14-00039-Online.indd 376NCI-D-14-00039-Online.indd 376 21/10/14 2:53 PM21/10/14 2:53 PM

VOLUME 25 • NUMBER 4 • OCTOBER–DECEMBER 2014 BLUNT PULMONARY INJURY
377
of the chest drain should be expected with PPV breaths or the patient’s spontaneous breathing. Continuous bubbling in the water seal chamber not associated with drainage system leaks, loss of dressing integrity, or chest tube dislodgment should prompt suspicion of an unresolved lung defect such as a bronchopleural fistula or bron-chial injury. A decision may be made to place a second chest tube to assist in further lung expansion and to perform a bronchoscopy to identify potential bronchial injuries. 3 , 7 , 8 , 15
Hemothorax In blunt chest injury, hemothoraces may result from intercostal vessel injury and lung lacera-tion associated with rib fractures or from injury of the great vessels in the chest. 3 , 8 , 16 In many cases, bleeding associated with injury of the intercostal artery or vein is limited. Reex-pansion of the lung and evacuation of the hemothorax reduce further bleeding from the low-pressure intercostal vessels. The volume of blood after initial insertion of the chest tube and the presence of ongoing bleeding dictate the need for thoracotomy to identify and stop hemorrhage. A massive hemothorax is defined as 1500 mL or more initially from the chest or the presence of 200 mL of blood per hour for 4 hours. 3 , 8 , 15 The underlying cause of massive hemothorax may be laceration of the lung, pulmonary artery or vein, or aorta.
Although hemothorax may be identified by initial drainage of blood from the chest tube, a CXR also may be helpful. Initial CXR in the trauma resuscitation room is often taken as an anterior to posterior view with the patient supine. Findings consistent with hemothorax on an anteroposterior CXR include haziness of the lung fields on the affected side. Up to 1000 mL of blood may be present in the pleural space in such cases, and the amount may be difficult to quantify with the patient in this position. 3 , 16 An upright CXR is ideal for diag-nosis of hemothorax. If the patient is in the semi-Fowler position, fluid may appear at the base of the affected hemithorax, blunting the costophrenic angle. The presence of 200 mL of blood or more may produce this result. CXR findings associated with hemothorax that may indicate aortic injury include blood collected in the left apical pleural space (apical cap) and large hemothoraces on the left side. Increas-ingly, focused assessment with sonography for trauma (FAST) is being used to diagnose pneu-mothorax and hemothorax before CXR.
Pneumothorax may be identified by “nonslid-ing” between the visceral and parietal pleura with breathing/ventilation on the affected side. Hemothorax may appear as an anechoic region (appearing black or without echo reverbera-tion) just above the diaphragm. 3 , 16 Similar to its use in the diagnosis of other traumatic injuries/conditions, the accuracy of focused assessment with sonography for trauma is highly operator dependent.
Treatment of Hemothorax Management of hemothorax includes insertion of a large chest tube as described earlier to evacuate blood from the pleural space and reexpand the lung. 2 , 3 , 8 , 16 Through the use of an autotransfusion chest drain system ( Figure 1 ), the collected blood may be given back to the patient, possibly reducing the need for transfu-sion of allogeneic blood products. Limitations of this process include patients who require ongoing massive transfusion, suspected con-tamination of the collected blood, known met-astatic disease, and extended duration of time from collection to transfusion. 17 , 18
Ongoing care of the patient with pneumo-thorax or hemothorax includes monitoring for changes in respiratory condition and onset of distress. Monitoring the chest drainage system for patency is essential, as clots may form in the thoracostomy tube or drainage system. 3 , 16 In addition to creating conditions that may result in tension pneumothorax or hemotho-rax, retained blood in the pleural space can clot and form an empyema. Removal of these collections may require the use of radiologic or video-assisted thoracoscopic drainage or thor-acotomy. 7 , 19 , 20 Ongoing drainage of blood and serous fluid may be expected for several days, especially with changes in the patient’s posi-tion that facilitate drainage of retained blood from the pleural space. If bloody output increases, or hourly output is consistently 200 mL or greater, the surgical team should be notified, as the patient may require a thoracot-omy for surgical management of bleeding. 3 , 7 , 16
Thoracic Duct Injury Blunt injury of the thoracic duct is rare and often associated with blunt injuries of the chest or neck. In blunt trauma, the duct may rupture just above the diaphragm during hyperexten-sion injuries of the thoracic spine. 21–23 Clinically, this condition may be diagnosed by chylous drainage from a chest tube. The classic
Copyright © 2014 American Association of Critical-Care Nurses. Unauthorized reproduction of this article is prohibited.
NCI-D-14-00039-Online.indd 377NCI-D-14-00039-Online.indd 377 21/10/14 2:53 PM21/10/14 2:53 PM

WWW.AACNADVANCEDCRITICALCARE.COM GALLAGHER
378
description of “milky white” drainage may be absent if the chyle is mixed with blood or pleu-ral fluid and may be more noticeable as bloody drainage subsides. If suspected, drainage may be sent to the laboratory to identify the pres-ence of triglycerides. Triglyceride levels greater than 110 mg/dL (to convert to millimoles per liter, multiply by 0.0113) may be diagnostic, whereas levels between 50 and 110 mg/dL may require further lipoprotein analysis. In addi-tion to thoracic drainage, treatment includes low-fat diet, parenteral nutrition, and in some cases ligation of the duct. 21–23
Airway Injuries Tracheobronchial injuries occur in 0.2% to 8% of patients with blunt trauma. These inju-ries include partial or full transection of the trachea, left or right main bronchi, or lower bronchial segments. Blunt mechanisms associ-ated with airway injury include hyperextension of the neck, compression of the chest, or rapid deceleration, resulting in avulsion of the air-way. Rapid deceleration can disrupt the air-way in regions where the airway structures transition from fixed positions to more mobile ones, such as the pulmonary hilum. In 80% of cases, disruption occurs within 2.5 cm of the carina. 3 , 8 , 15 , 24
Clinical Features and Initial Management Clinical manifestations of airway disruption depend on the location of the injury. Tracheal injuries manifest with subcutaneous emphy-sema of the chest and neck, dyspnea, stridor, hoarseness, and hemoptysis. Airway injuries within the chest cavity and those affecting the main bronchi can result in pneumomediasti-num and/or pneumothorax. Both may be detectable on CXR or CT scan of the chest. 3 , 8 , 15
The management of airway injuries depends on the location and severity of injury. Tracheal injuries may be identified during endotracheal intubation or after placement of an endotra-cheal tube. Placement of the tube and inflation of the cuff can result in further tracheal disrup-tion or transection, depending on the location of injury. If the injury is bridged by the endotracheal tube, the airway may be ade-quately secured. However, if the injury is below the cuff, PPV may further disrupt the defect and result in worsening subcutaneous emphysema. 3 , 8 , 24 Bronchoscopic evaluation and assistance with placement of the endotracheal tube may be required to bridge the level of the defect and adequately secure the airway. Emer-gent surgical options to manage the airway in tracheal injury may be limited, depending on
Copyright © 2014 American Association of Critical-Care Nurses. Unauthorized reproduction of this article is prohibited.
Figure 1: Chest drain system with autotransfusion capability. This fi gure is available in color in the article
on the journal Web site, www.aacnadvancedcriticalcare.com , and the iPad. Reprinted with permission from
Atrium Medical Corporation.
NCI-D-14-00039-Online.indd 378NCI-D-14-00039-Online.indd 378 21/10/14 2:53 PM21/10/14 2:53 PM
VOLUME 25 • NUMBER 4 • OCTOBER–DECEMBER 2014 BLUNT PULMONARY INJURY
379
the depth of injury. Although surgical crico-thyrotomy is usually the procedure of choice for emergent surgical creation of an airway, placement of the airway through the cricothy-roid membrane may be well above the injury level, failing to adequately secure the airway. 25–29 Emergency tracheostomy may be the best option in this circumstance.
Diagnosis of Bronchial Injuries Diagnosis of bronchial injuries may be challeng-ing in patients with blunt trauma. Unlike pene-trating mechanisms, where trajectory may assist in determining underlying airway injury, blunt mechanisms provide no such clues. The findings on clinical assessment noted earlier may be pre-sent. CXR and CT of the chest may reveal pneumothorax, pneumomediastinum, or both. Persistent pneumothorax, despite insertion of a chest tube and the presence of a continuous air leak should increase suspicion of bronchial injury ( Figure 2 ). 3 , 8 , 27 , 28 , 30–33 Normally, pneumo-thorax and presence of an air leak resolve with reexpansion of the lung after placement of a thoracostomy tube. In the case of bronchial injury, the airway defect fails to seal, providing a continuous source of air leakage into the pleu-ral space. In addition, the patient may have worsening respiratory distress, as tidal volume is consistently lost through the thoracostomy tube. Other more common reasons for persis-tent pneumothorax and air leak should be ruled
out, including blockage or clotting of the thora-costomy tube, necessitating placement of a sec-ond tube. 27,28,30,31,33
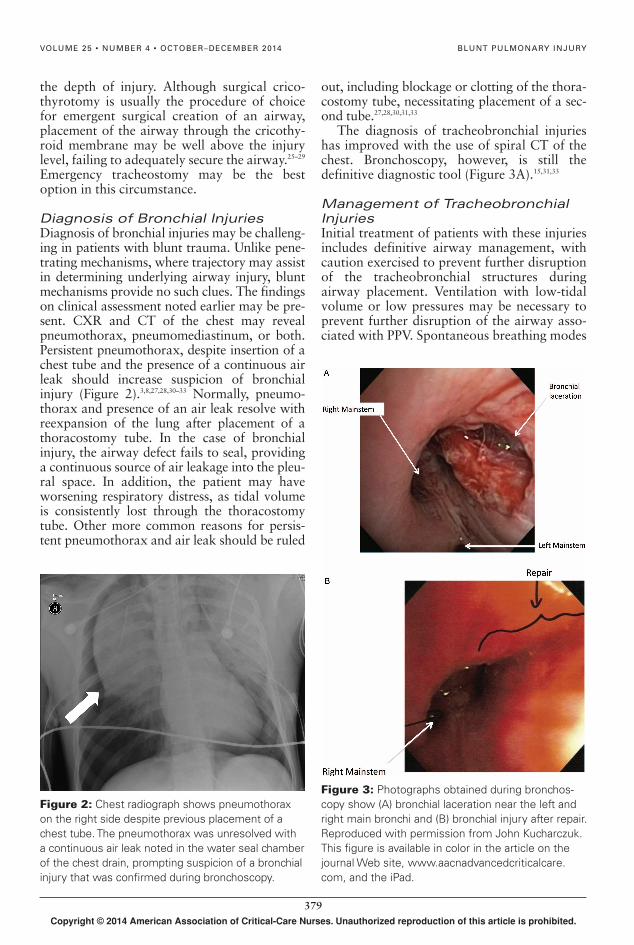
The diagnosis of tracheobronchial injuries has improved with the use of spiral CT of the chest. Bronchoscopy, however, is still the definitive diagnostic tool ( Figure 3A ). 15 , 31 , 33
Management of Tracheobronchial Injuries Initial treatment of patients with these injuries includes definitive airway management, with caution exercised to prevent further disruption of the tracheobronchial structures during airway placement. Ventilation with low-tidal volume or low pressures may be necessary to prevent further disruption of the airway asso-ciated with PPV. Spontaneous breathing modes
Figure 2: Chest radiograph shows pneumothorax
on the right side despite previous placement of a
chest tube. The pneumothorax was unresolved with
a continuous air leak noted in the water seal chamber
of the chest drain, prompting suspicion of a bronchial
injury that was confi rmed during bronchoscopy.
Figure 3: Photographs obtained during bronchos-
copy show (A) bronchial laceration near the left and
right main bronchi and (B) bronchial injury after repair.
Reproduced with permission from John Kucharczuk.
This fi gure is available in color in the article on the
journal Web site, www.aacnadvancedcriticalcare.
com , and the iPad.
Copyright © 2014 American Association of Critical-Care Nurses. Unauthorized reproduction of this article is prohibited.
NCI-D-14-00039-Online.indd 379NCI-D-14-00039-Online.indd 379 21/10/14 2:53 PM21/10/14 2:53 PM

WWW.AACNADVANCEDCRITICALCARE.COM GALLAGHER
380
such as pressure support ventilation may achieve this goal by supporting negative intrathoracic pressure associated with sponta-neous breathing, rather than the higher driving pressures associated with traditional PPV. Such management is, however, dependent on the patient’s ability to maintain the spontaneous breathing efforts necessary to use these modes. 3 , 24 , 28 , 34
Definitive repair of these injuries is based on the location and severity of injury. Some inju-ries such as those that affect less than one-third the diameter of the airway may be managed nonoperatively. Others may require thoracot-omy with surgical repair ( Figure 3B ). Insertion of a double lumen ET tube may be necessary to perform single lung ventilation on the unin-jured side, while repair of the injury takes place. 3 , 15 , 26 , 28
Pulmonary Contusions Pulmonary contusions are common in blunt chest injury and may be associated with rib frac-tures and flail chest. These injuries result from compression or rapid deceleration forces applied to the chest wall and lung parenchyma. Com-mon mechanisms of injury in the civilian sector include motor vehicle or motorcycle crashes with impact on the chest wall, pedestrian/motor vehicle collisions, and falls. 4 , 5 , 35–39
The overall impact of this energy applied to the lung is injury of the pulmonary interstitium or alveoli, resulting in bleeding into and around these structures. Localized inflamma-tion results in further damage and increases permeability of the alveolar capillary mem-brane, causing transudation of plasma-rich fluid into the alveoli. In addition, type II alveo-lar cells responsible for surfactant production are compromised, as is the function of sur-factant already present in the alveoli. The net effect is alveolar collapse, impaired gas exchange, and development of pulmonary shunt conditions. This effect may be further compounded if the patient aspirates gastric contents or blood into the uninjured lung, fur-ther worsening gas exchange. 1 , 3–5 , 36 , 37
Pulmonary Blast Injury Mechanism Blast injuries are more common in the combat setting, representing related but unique pat-terns of energy distribution that cause the underlying injury. Gas- or air-containing organs such as the lungs and bowel are vulner-able to injury from blast effect because of 3
related but distinct events. First, the blast energy creates a shearing (spalling) effect at the interface between gas and liquid in the alveoli. Second, low-density alveolar tissue is separated from heavier hilar tissue because of the differ-ent response motions to the blast. The third event occurs after the blast wave passes, result-ing in rebound or overexpansion of the alveoli. These mechanisms are distinct from injury associated with blast-associated projectiles striking the chest wall and causing underlying pulmonary injury, or deceleration injury of pulmonary structures after the victim is thrown against a stationary object. 36 , 40
Initial signs and symptoms of patients with blast injury may be similar to those of patients with general pulmonary contusion in that oxy-genation disturbances may be subtle at first, progressing over hours with decreasing oxygen saturation. Frothy sputum and frank hemopty-sis also may be present, representing more sig-nificant disruption of the alveolar capillary membrane. Mechanical ventilation may be required, though risk of systemic air embolism has been described as a potential complication of PPV as air is forced into the vascular space across the alveolar capillary disruption. 39 Reduction of peak inspiratory ventilation pres-sure may be beneficial. This reduction may be achieved through low tidal volume or pressure-targeted ventilation, as well as pressure sup-port ventilation in spontaneously breathing patients. 39
Diagnosis of Pulmonary Contusion Pulmonary contusion is diagnosed on the basis of mechanism of injury as well as results of clinical and radiological evaluation of the patient. Significant blunt force energy applied to the thorax along with the presence of rib fractures should raise suspicion of pulmonary contusion. Clinical findings may include chest pain, dyspnea, and hemoptysis. Worsening hypoxia, hypercarbia, and work of breathing may necessitate intubation and institution of mechanical ventilation. In intubated patients suctioning of blood from the endotracheal tube may be common. Increases in peak air-way and plateau pressures, as well as decreas-ing static lung compliance, also may be found. 1,5,35,37,41,42
Although CXR is a standard part of the ini-tial diagnostic evaluation, only 47% of pulmo-nary contusions may be detected on such images. Detection may increase to 92% by 24
Copyright © 2014 American Association of Critical-Care Nurses. Unauthorized reproduction of this article is prohibited.
NCI-D-14-00039-Online.indd 380NCI-D-14-00039-Online.indd 380 21/10/14 2:53 PM21/10/14 2:53 PM
VOLUME 25 • NUMBER 4 • OCTOBER–DECEMBER 2014 BLUNT PULMONARY INJURY
381
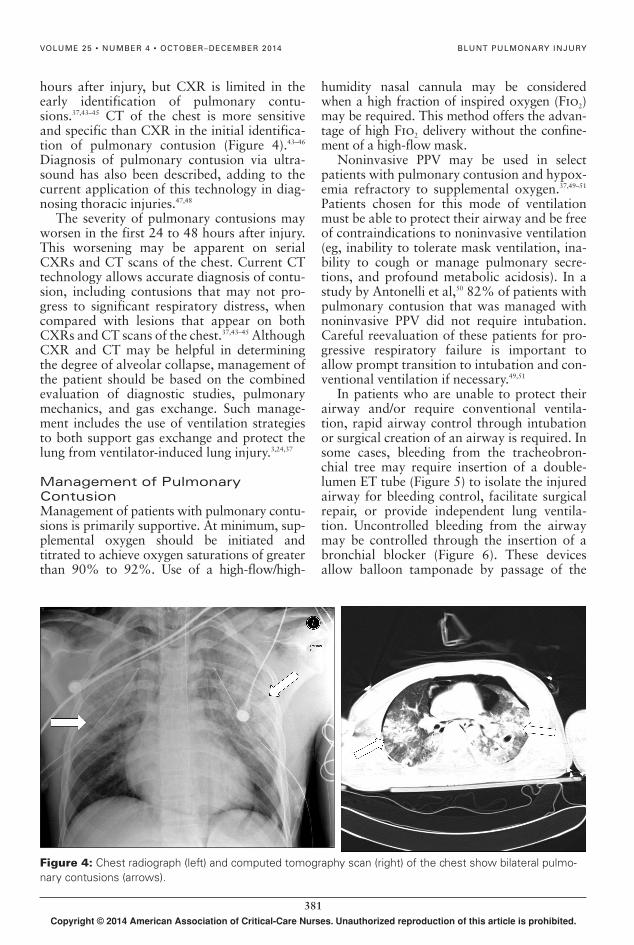
Figure 4: Chest radiograph (left) and computed tomography scan (right) of the chest show bilateral pulmo-
nary contusions (arrows).
hours after injury, but CXR is limited in the early identification of pulmonary contu-sions. 37 , 43–45 CT of the chest is more sensitive and specific than CXR in the initial identifica-tion of pulmonary contusion ( Figure 4 ). 43–46 Diagnosis of pulmonary contusion via ultra-sound has also been described, adding to the current application of this technology in diag-nosing thoracic injuries. 47 , 48
The severity of pulmonary contusions may worsen in the first 24 to 48 hours after injury. This worsening may be apparent on serial CXRs and CT scans of the chest. Current CT technology allows accurate diagnosis of contu-sion, including contusions that may not pro-gress to significant respiratory distress, when compared with lesions that appear on both CXRs and CT scans of the chest. 37 , 43–45 Although CXR and CT may be helpful in determining the degree of alveolar collapse, management of the patient should be based on the combined evaluation of diagnostic studies, pulmonary mechanics, and gas exchange. Such manage-ment includes the use of ventilation strategies to both support gas exchange and protect the lung from ventilator-induced lung injury. 3 , 24 , 37
Management of Pulmonary Contusion Management of patients with pulmonary contu-sions is primarily supportive. At minimum, sup-plemental oxygen should be initiated and titrated to achieve oxygen saturations of greater than 90% to 92%. Use of a high-flow/high-
humidity nasal cannula may be considered when a high fraction of inspired oxygen (F io 2 ) may be required. This method offers the advan-tage of high F io 2 delivery without the confine-ment of a high-flow mask.
Noninvasive PPV may be used in select patients with pulmonary contusion and hypox-emia refractory to supplemental oxygen. 37 , 49–51 Patients chosen for this mode of ventilation must be able to protect their airway and be free of contraindications to noninvasive ventilation (eg, inability to tolerate mask ventilation, ina-bility to cough or manage pulmonary secre-tions, and profound metabolic acidosis). In a study by Antonelli et al, 50 82% of patients with pulmonary contusion that was managed with noninvasive PPV did not require intubation. Careful reevaluation of these patients for pro-gressive respiratory failure is important to allow prompt transition to intubation and con-ventional ventilation if necessary. 49 , 51
In patients who are unable to protect their airway and/or require conventional ventila-tion, rapid airway control through intubation or surgical creation of an airway is required. In some cases, bleeding from the tracheobron-chial tree may require insertion of a double-lumen ET tube ( Figure 5 ) to isolate the injured airway for bleeding control, facilitate surgical repair, or provide independent lung ventila-tion. Uncontrolled bleeding from the airway may be controlled through the insertion of a bronchial blocker ( Figure 6 ). These devices allow balloon tamponade by passage of the
Copyright © 2014 American Association of Critical-Care Nurses. Unauthorized reproduction of this article is prohibited.
NCI-D-14-00039-Online.indd 381NCI-D-14-00039-Online.indd 381 21/10/14 2:53 PM21/10/14 2:53 PM

WWW.AACNADVANCEDCRITICALCARE.COM GALLAGHER
382
device into the affected airway through the artificial airway with the assistance of a bron-choscope. Alternatively, selective intubation of the bronchus on the affected side by using a conventional endotracheal tube, or a double-lumen endotracheal tube, may be done to con-trol bleeding and allow injury repair. 1,3,4,24,37,42
Mechanical Ventilation Mechanical ventilation of patients with pulmo-nary contusion may present some challenges. Overall, the strategies are aimed at improving oxygenation and ventilation while protecting the lung. Patients with pulmonary contusion are at risk for development of pneumonia and acute respiratory distress syndrome. 53 , 54 The success of standard approaches to alveolar reexpansion such as high positive end-expiratory pressure (PEEP) and recruitment maneuvers may depend on the degree of consolidation in the contused region of the lung. During these maneuvers, the goal is to reexpand atelectatic regions. How-ever, such tactics may overdistend normal regions of the lung while having minimal impact on the consolidated area of contusion. This overdistention may result in ventilator-induced lung injury from volutrauma in the uninjured lung, with little improvement in the injured lung. Overdistention of normal alveoli also may compress associated pulmonary capillaries, reducing perfusion to these alveoli, and result-ing in dead space ventilation units. This com-pression also may redirect blood flow toward collapsed alveoli, worsening the existing shunt. 1 , 5 , 24 , 55
Given the degree of lung injury, lung-pro-tective ventilation strategies should aim for improving oxygenation and limiting further lung injury. This strategy includes limiting ven-tilation plateau pressure (alveolar surrogate pressure) to less than 30 cm H 2 O and prevent-ing end-tidal collapse. These goals may be achieved through the use of low-tidal-volume ventilation and application of PEEP. Low-tidal-volume ventilation uses a tidal volume of 4 to 8 mL/kg of predicted body weight. 56 Other ventilation options include pressure control ventilation, with or without inverse ratio venti-lation. Inverse ratio ventilation uses shortened expiratory times to prevent full exhalation before the next breath, which results in the accumulation of auto-PEEP (intrinsic PEEP) to recruit alveoli and prevent alveolar collapse during exhalation. 57 , 58 Variations of pressure control ventilation include biphasic (bilevel) ventilation and airway pressure release ventila-tion. Both of these pressure modes allow coex-isting spontaneous breathing efforts by patients, while maintaining the benefits of the pressure control mode of ventilation’s breath pressure and flow patterns of breath delivery. In the case of airway pressure release ventilation,
Figure 5: Double-lumen endotracheal tube used
to isolate the lung for interventions such as single-
lung ventilation or independent lung ventilation. This
fi gure is available in color in the article on the journal
Web site, www.aacnadvancedcriticalcare.com , and
the iPad.
Figure 6: (A) The bronchial blocker balloon fully in-
fl ated into the right main bronchus. (B) Fully infl ated
balloon in the entrance of the left main bronchus.
Reprinted with permission from Campos. 52
Copyright © 2014 American Association of Critical-Care Nurses. Unauthorized reproduction of this article is prohibited.
NCI-D-14-00039-Online.indd 382NCI-D-14-00039-Online.indd 382 21/10/14 2:53 PM21/10/14 2:53 PM

VOLUME 25 • NUMBER 4 • OCTOBER–DECEMBER 2014 BLUNT PULMONARY INJURY
383
very short expiratory times between ventilator breaths are designed to prevent alveolar collapse. 1 , 59 , 60 Other ventilation options may include high-frequency percussive ventilation or high-frequency oscillation ventilation to both recruit and protect the lung. 61 , 62
Regardless of the mode or strategy chosen, reducing tidal volume to protect the lung may result in hypercapnia. Permissive hypercapnia is the allowable increase in Pa co 2 associated with the use of lower tidal volumes to protect the lung from ventilator-induced injury. This hypercapnia may be required for a period of time until alveolar reexpansion can occur, restoring the normal lung capacity. Hypercap-nia is usually tolerated well in most patients. There are no consistently recommended titra-tion end points for hypercapnia. Hypercapnia resulting in an arterial pH as low as 7.2 is con-sidered acceptable. 63–65
In addition to the preceding ventilation techniques, isolated single-lung ventilation of the uninjured lung, or independent lung venti-lation, may be an option to customize tidal volume and PEEP to the uninjured and injured lung. 24 , 42 , 66 With both options, the injured lung can be isolated, preventing aspiration of blood and secretions into the uninjured lung. Inde-pendent lung ventilation uses 2 ventilators (1 for each lung) that can be synchronized or allowed to ventilate each lung asynchronously through a double lumen ET tube. This tech-nique is useful for severe unilateral lung contu-sions or bilateral contusions of different severity. Independent lung ventilation is often maintained until the disparities in lung mechanics between the injured lung and the uninjured lung begin to resolve. Monitoring of peak and plateau pressures, lung compliance, and radiographic findings may guide decisions to convert to whole-lung ventilation and fur-ther ventilator liberation. 24 , 66
Severe unilateral or bilateral pulmonary contusions may result in the inability to oxy-genate or ventilate the patient conventionally. In these cases, extracorporeal membrane oxy-genation (ECMO) may be required to main-tain pulmonary support and lung rest. Although ECMO is potentially beneficial, there is risk of increased bleeding into the con-tused lung associated with the anticoagulant used in the ECMO circuit. 67–69 A detailed dis-cussion of ECMO as a pulmonary support strategy is provided in the article by Schulman et al 70 in this issue.
Fluid Resuscitation in Blunt Pulmonary Injury Restoration of vascular blood volume may be required as part of the initial resuscitation of injured patients. Although restoring blood vol-ume is necessary to improve global tissue oxy-genation, overresuscitation with fluids should be avoided. Recent evidence supports balanced fluid resuscitation to achieve adequate organ perfusion while limiting the harmful effects of fluid volume overload. This balanced approach has been described in several clinical conditions including penetrating trauma, and is especially true of patients with lung injury. The adminis-tration of crystalloids to treat pulmonary contu-sion may increase pulmonary interstitial edema, worsening gas exchange. 5 , 37 , 42 , 71–73 In patients with pulmonary contusion, vascular volume optimization should be based on optimizing oxygen delivery: delivering blood components to restore blood loss and correct coagulopathy while preventing and correcting hypothermia. Crystalloid administration should be limited and should be based on reliable dynamic end points of fluid resuscitation that reflect improve-ments in cardiovascular volume and function, rather than unreliable pressure-based parame-ters such as central venous pressure and nonspe-cific physiological parameters such as heart rate and urine output. 74–76
Currently, reliable end points include echocardiography evaluation of cardiac chamber and vena caval filling volumes, eval-uation of stroke volume change with volume challenge, and evaluation of variations of stroke volume and pulse pressure to deter-mine the benefit of vascular volume replace-ment. 77–79 Pressure-based parameters such as central venous pressure and pulmonary capil-lary wedge pressure have proven consistently unreliable as surrogates for changes in vascu-lar volume. 74 , 75 Further, those pressures may be falsely elevated with the use of PPV because the positive pressure is transmitted to the venous system, which further compli-cates the use of vascular pressures as end points for fluid resuscitation. 80–82
Positioning Therapy Positioning therapy in blunt pulmonary injury is aimed at improving ventilation/perfusion matching through expansion of collapsed alve-oli and matching perfusion to the best-ventilated regions. In addition, positioning therapy assists in mobilizing blood and
Copyright © 2014 American Association of Critical-Care Nurses. Unauthorized reproduction of this article is prohibited.
NCI-D-14-00039-Online.indd 383NCI-D-14-00039-Online.indd 383 21/10/14 2:53 PM21/10/14 2:53 PM

WWW.AACNADVANCEDCRITICALCARE.COM GALLAGHER
384
secretions for removal to further assist in achieving these goals. There are 2 opinions related to positioning patients with a unilateral lung injury. 5 , 24 , 37 , 55 When the injured lung is placed in the dependent position, bleeding may be isolated to the injured side, limiting drainage from the injured lung into the uninjured lung. In this situation, positioning the patient injured side down may afford time to control bleeding or isolate the injured lung. The other option is to place the uninjured lung in the dependent position to optimize gravitational perfusion to the uninjured or best-ventilated lung. This positioning may improve ventilation/perfusion matching on the uninjured side and improve oxygenation. In addition, this option places the injured lung in the nondependent position, pro-viding opportunity for reexpansion. 24 , 37
In either case, positioning should be based on the clinical condition of the patient and what position achieves optimal gas exchange while facilitating lung expansion. In the absence of uncontrolled hemorrhage and risk of aspiration of blood into the uninjured lung, placement of the uninjured lung in the depend-ent position will support ventilation/perfusion matching and is the best option for improving gas exchange.
This goal may be achieved through manual repositioning, the use of continuous lateral rotation beds, or by placing the patient prone. Prone positioning may be helpful with bilat-eral lung injury, where consolidation is present along the dorsal surface of the lung. Move-ment to the prone position may assist with the reexpansion of these collapsed regions and improve matching with the perfusion that remains primarily in this posterior region, even when the patient is placed prone. 83–85
Pain Management Pain associated with blunt chest injuries can be significant, often resulting in additional compli-cations associated with hypoventilation if not managed appropriately. Pain management should facilitate 3 objectives: ability to main-tain the work of breathing unassisted, partici-pation in pulmonary hygiene efforts such as coughing and deep breathing, and ability to mobilize within and out of bed as appropriate to improve ventilation and limit complications associated with immobility. Finally, if the patient requires treatment with mechanical ventilation, pain management should facilitate ventilator liberation. 86–88
Pain Management Strategies Pain management strategies for patients with blunt chest injury include a parenteral analge-sic, local and regional blocks, and epidural analgesia. Parenteral opioid analgesic agents are effective for acute pain and may be deliv-ered intermittently, continuously, or as patient-controlled analgesia. Although such analgesics are commonly used, there is a risk of overseda-tion and other opioid-associated adverse effects. Local and regional analgesia may be directed to the area of injury, reducing the need for and duration of use of other analgesics. Epidural analgesia is delivered to the epidural space, interrupting pain transmission at the dorsal horn of the spinal cord. 42 , 86–88 This tech-nique provides superior analgesia while limit-ing the systemic adverse effects of parenteral agents. Although effective, epidural catheter placement may not be possible in patients with coexisting spinal column fractures or patients who have been taking anticoagulants. Other agents such as nonsteroidal anti-inflammatory drugs may be used as well. 42 , 87
Conclusion Blunt pulmonary injuries are common and require early identification during initial assessment and resuscitation to limit associ-ated morbidity and mortality. Definitive airway management and support of oxygena-tion and ventilation should be anticipated. This may include management of hemorrhage from the bronchopulmonary tree, as well as implementation of nontraditional ventilation strategies. Fluid resuscitation should be guided by end points that reflect volume responsive-ness, such as improvement in stroke volume, to avoid an unnecessary positive fluid balance that may worsen pulmonary gas exchange. Finally, adjunctive support strategies, includ-ing pain management and positioning, are essential to improve patient’s comfort and limit pulmonary complications as well as com-plications associated with immobility.
REFERENCES 1. Kiraly L , Schreiber M . Management of the crushed
chest . Crit Care Med . 2010 ; 38 ( 9) (suppl ): S469 – S477 . 2. ATLS Subcommittee, American College of Surgeons’
Committee on Trauma, International ATLS Working Group . Advanced trauma life support (ATLS): The ninth edition . J Trauma Acute Care Surg . 2013 ; 74 ( 5 ): 1363 – 1366 .
3. Bernardin B , Troquet JM . Initial management and resuscitation of severe chest trauma . Emerg Med Clin North Am . 2012 ; 30 ( 2 ): 377 – 400 .
Copyright © 2014 American Association of Critical-Care Nurses. Unauthorized reproduction of this article is prohibited.
NCI-D-14-00039-Online.indd 384NCI-D-14-00039-Online.indd 384 21/10/14 2:53 PM21/10/14 2:53 PM
VOLUME 25 • NUMBER 4 • OCTOBER–DECEMBER 2014 BLUNT PULMONARY INJURY
385
4. Miller DL , Mansour KA . Blunt traumatic lung injuries . Thorac Surg Clin . 2007 ; 17 ( 1 ): 57 – 61 .
5. Wanek S , Mayberry JC . Blunt thoracic trauma: flail chest, pulmonary contusion, and blast injury . Crit Care Clin . 2004 ; 20 ( 1 ): 71 – 81 .
6. McGillicuddy D , Rosen P . Diagnostic dilemmas and cur-rent controversies in blunt chest trauma . Emerg Med Clin North Am . 2007 ; 25 ( 3 ): 695 – 711 .
7. Mowery NT , Gunter OL , Collier BR , et al. Practice manage-ment guidelines for management of hemothorax and occult pneumothorax . J Trauma . 2011 ; 70 ( 2 ): 510 – 518 .
8. O’Connor JV , Adamski J . The diagnosis and treatment of non-cardiac thoracic trauma . J R Army Med Corps . 2010 ; 156 ( 1 ): 5 – 14 .
9. Ball CG , Kirkpatrick AW , Feliciano DV . The occult pneu-mothorax: what have we learned ? Can J Surg . 2009 ; 52 ( 5 ): E173 – E179 .
10. Barrios C , Tran T , Malinoski D , et al. Successful man-agement of occult pneumothorax without tube thora-costomy despite positive pressure ventilation . Am Surg . 2008 ; 74 ( 10 ): 958 – 961 .
11. de Moya MA , Seaver C , Spaniolas K , et al. Occult pneu-mothorax in trauma patients: development of an objec-tive scoring system . J Trauma . 2007 ; 63 ( 1 ): 13 – 17 .
12. Moore FO , Goslar PW , Coimbra R , et al. Blunt traumatic occult pneumothorax: is observation safe? Results of a prospective, AAST multicenter study . J Trauma. 2011 ; 70 ( 5 ): 1019 – 1023 .
13. Ortega-Carnicer J , Martin-Rodriguez C , Portilla-Botelho M . Occult pneumothorax . Resuscitation . 2006 ; 71 ( 1 ): 4 – 5 .
14. Wilson H , Ellsmere J , Tallon J , Kirkpatrick A . Occult pneumothorax in the blunt trauma patient: tube thora-costomy or observation ? Injury . 2009 ; 40 ( 9 ): 928 – 931 .
15. Zarama V , Velasquez M . Mainstem bronchus transec-tion after blunt chest trauma . J Emerg Med . 2013 ; 44 ( 1 ): 187 – 188 .
16. Meyer DM . Hemothorax related to trauma . Thorac Surg Clin . 2007 ; 17 ( 1 ): 47 – 55 .
17. Salhanick M , Corneille M , Higgins R , et al. Autotransfu-sion of hemothorax blood in trauma patients: is it the same as fresh whole blood ? Am J Surg . 2011 ; 202 ( 6 ): 817 – 821 .
18. Smith WZ , Harrison HB , Salhanick MA , et al. A small amount can make a difference: a prospective human study of the paradoxical coagulation characteristics of hemothorax . Am J Surg . 2013 ; 206 ( 6 ): 904 – 909 .
19. Billeter AT , Druen D , Franklin GA , Smith JW , Wrightson W , Richardson JD . Video-assisted thoracoscopy as an important tool for trauma surgeons: a systematic review . Langenbecks Arch Surg . 2013 ; 398 ( 4 ): 515 – 523 .
20. Cetindag IB , Neideen T , Hazelrigg SR . Video-assisted thoracic surgical applications in thoracic trauma . Thorac Surg Clin . 2007 ; 17 ( 1 ): 73 – 79 .
21. Chinnock BF . Chylothorax: case report and review of the literature . J Emerg Med . 2003 ; 24 ( 3 ): 259 – 262 .
22. Crnojevic LJ , Hodgetts TJ , Chambers D , Partridge RJ . Bilat-eral traumatic chylothorax: a complication of a fracture of the thoracic spine . Injury . 1997 ; 28 ( 9/10 ): 681 – 682 .
23. McCormick J 3rd Henderson SO . Blunt trauma-induced bilateral chylothorax . Am J Emerg Med . 1999 ; 17 ( 3 ): 302 – 304 .
24. Rico FR , Cheng JD , Gestring ML , Piotrowski ES . Mechanical ventilation strategies in massive chest trauma . Crit Care Clin . 2007 ; 23 ( 2 ): 299 – 315 .
25. Devitt JH , Boulanger BR . Lower airway injuries and anaesthesia . Can J Anaesth . 1996 ; 43 ( 2 ): 148 – 159 .
26. Juvekar NM , Deshpande SS , Nadkarni A , Kanitkar S . Perioperative management of tracheobronchial injury following blunt trauma . Ann Card Anaesth . 2013 ; 16 ( 2 ): 140 – 143 .
27. Johnson SB . Tracheobronchial injury . Semin Thorac Cardiovasc Surg . 2008 ; 20 ( 1 ): 52 – 57 .
28. Karmy-Jones R , Wood DE . Traumatic injury to the tra-chea and bronchus . Thorac Surg Clin . 2007 ; 17 ( 1 ): 35 – 46 .
29. Dillon JK , Christensen B , Fairbanks T , Jurkovich G , Moe KS . The emergent surgical airway: cricothyrotomy vs. tra-cheotomy . Int J Oral Maxillofac Surg . 2013 ; 42 ( 2 ): 204 – 208 .
30. Ong VY , Tan KH . No air leak on PPV does not exclude tracheobronchial injury after blunt chest trauma . Heart Lung Circ . 2008 ; 17 ( 2 ): 163 – 166 .
31. Chu CP , Chen PP . Tracheobronchial injury secondary to blunt chest trauma: diagnosis and management . Anaesth Intensive Care . 2002 ; 30 ( 2 ): 145 – 152 .
32. Conti M , Benhamed L , Porte H , Wurtz A . Iatrogenic tra-cheobronchial injury: a support to nonsurgical man-agement . Ann Thorac Surg . 2008 ; 85 ( 5 ): 1843 – 1844 .
33. Cosper GH , Dassinger MS . Tracheobronchial injury diagnosed by computed tomography scan: a case report . J Pediatr Surg . 2009 ; 44 ( 3 ): 648 – 650 .
34. O’Connor JV , Kufera JA , Kerns TJ , et al. Crash and occupant predictors of pulmonary contusion . J Trauma . 2009 ; 66 ( 4 ): 1091 – 1095 .
35. Bastos R , Calhoon JH , Baisden CE . Flail chest and pul-monary contusion . Semin Thorac Cardiovasc Surg . 2008 ; 20 ( 1 ): 39 – 45 .
36. Clemedson CJ . Blast injury . Physiol Rev . 1956 ; 36 ( 3 ): 336 – 354 .
37. Cohn SM , Dubose JJ . Pulmonary contusion: an update on recent advances in clinical management . World J Surg . 2010 ; 34 ( 8 ): 1959 – 1970 .
38. Hamrick MC , Duhn RD , Carney DE , Boswell WC , Ochsner MG . Pulmonary contusion in the pediatric population . Am Surg . 2010 ; 76 ( 7 ): 721 – 724 .
39. Plurad DS . Blast injury . Mil Med . 2011 ; 176 ( 3 ): 276 – 282 . 40. Keneally R , Szpisjak D . Thoracic trauma in Iraq and
Afghanistan . J Trauma Acute Care Surg . 2013 ; 74 ( 5 ): 1292 – 1297 .
41. Hamrick MC , Duhn RD , Ochsner MG . Critical evaluation of pulmonary contusion in the early post-traumatic period: risk of assisted ventilation . Am Surg . 2009 ; 75 ( 11 ): 1054 – 1058 .
42. Simon B , Ebert J , Bokhari F , et al. Management of pulmo-nary contusion and flail chest: an Eastern Association for the Surgery of Trauma practice management guideline . J Trauma Acute Care Surg . 2012 ; 73 ( 5) (suppl 4 ): S351 – S361 .
43. Deunk J , Poels TC , Brink M , et al. The clinical outcome of occult pulmonary contusion on multidetector-row computed tomography in blunt trauma patients . J Trauma . 2010 ; 68 ( 2 ): 387 – 394 .
44. Kea B , Gamarallage R , Vairamuthu H , et al. What is the clinical significance of chest CT when the chest x-ray result is normal in patients with blunt trauma ? Am J Emerg Med . 2013 ; 31 ( 8 ): 1268 – 1273 .
45. Peters S , Nicolas V , Heyer CM . Multidetector computed tomography–spectrum of blunt chest wall and lung injuries in polytraumatized patients . Clin Radiol . 2010 ; 65 ( 4 ): 333 – 338 .
46. de Moya MA , Manolakaki D , Chang Y , et al. Blunt pulmo-nary contusion: admission computed tomography scan predicts mechanical ventilation . J Trauma . 2011 ; 71 ( 6 ): 1543 – 1547 .
47. Ball CG , Ranson MK , Rodriguez-Galvez M , Lall R , Kirkpatrick AW . Sonographic depiction of posttrau-matic alveolar-interstitial disease: the hand-held diag-nosis of a pulmonary contusion . J Trauma . 2009 ; 66 ( 3 ): 962 .
48. Stone MB , Secko MA . Bedside ultrasound diagnosis of pulmonary contusion . Pediatr Emerg Care . 2009 ; 25 ( 12 ): 854 – 855 .
49. Ambrosino N , Guarracino F . Unusual applications of noninvasive ventilation . Eur Respir J . 2011 ; 38 ( 2 ): 440 – 449 .
50. Antonelli M , Conti G , Moro ML , et al. Predictors of failure of noninvasive positive pressure ventilation in patients with acute hypoxemic respiratory failure: a multi-center study . Intensive Care Med . 2001 ; 27 ( 11 ): 1718 – 1728 .
51. Chiumello D , Coppola S , Froio S , Gregoretti C , Con-sonni D . Noninvasive ventilation in chest trauma:
Copyright © 2014 American Association of Critical-Care Nurses. Unauthorized reproduction of this article is prohibited.
NCI-D-14-00039-Online.indd 385NCI-D-14-00039-Online.indd 385 21/10/14 2:53 PM21/10/14 2:53 PM

WWW.AACNADVANCEDCRITICALCARE.COM GALLAGHER
386
systematic review and meta-analysis . Intensive Care Med . 2013 ; 39 ( 7 ): 1171 – 1180 .
52. Campos JH . Lung isolation techniques for patients with difficult airway . Curr Opin Anaethesiol . 2010 ; 23 ( 1 ): 12 – 17 .
53. Barlow M , Prince JM . Predicting outcomes in the set-ting of blunt thoracic trauma . J Surg Res . 2013 ; 183 ( 1 ): 100 – 101 .
54. Janus TJ , Vaughan-Sarrazin MS , Baker LJ , Smith HL . Predictors of pneumonia in trauma patients with pulmonary contusion . J Trauma Nurs . 2012 ; 19 ( 3 ): 139 – 147 .
55. Sutyak JP , Wohltmann CD , Larson J . Pulmonary contu-sions and critical care management in thoracic trauma . Thorac Surg Clin . 2007 ; 17 ( 1 ): 11 – 23 .
56. Anonymous . Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The acute respiratory distress syndrome network . N Engl J Med. 2000 ; 342 ( 18 ): 1301 – 1308 .
57. Singer BD , Corbridge TC . Pressure modes of invasive mechanical ventilation . South Med J . 2011 ; 104 ( 10 ): 701 – 709 .
58. Haas CF . Mechanical ventilation with lung protective strat-egies: what works ? Crit Care Clin . 2011 ; 27 ( 3 ): 469 – 486 .
59. Walkey AJ , Nair S , Papadopoulos S , Agarwal S , Rear-don CC . Use of airway pressure release ventilation is associated with a reduced incidence of ventilator-asso-ciated pneumonia in patients with pulmonary contu-sion . J Trauma . 2011 ; 70 ( 3 ): E42 – E47 .
60. Daoud EG , Farag HL , Chatburn RL . Airway pressure release ventilation: what do we know ? Respir Care . 2012 ; 57 ( 2 ): 282 – 292 .
61. Allan PF , Osborn EC , Chung KK , Wanek SM . High-frequency percussive ventilation revisited . J Burn Care Res . 2010 ; 31 ( 4 ): 510 – 520 .
62. Short K , Bougatef A , Khusid F , Kenney BD , Miller K . High-frequency percussive ventilation . Respir Care . 2010 ; 55 ( 12 ): 1762 – 1764 .
63. Cortes GA , Marini JJ . Update: adjuncts to mechanical ventilation . Curr Opin Anaesthesiol . 2012 ; 25 ( 2 ): 156 – 163 .
64. Hodgson CL , Tuxen DV , Davies AR , et al. A randomised controlled trial of an open lung strategy with staircase recruitment, titrated PEEP and targeted low airway pressures in patients with acute respiratory distress syndrome . Crit Care . 2011 ; 15 ( 3 ): R133 .
65. O’Croinin D , Ni Chonghaile M , Higgins B , Laffey JG . Bench-to-bedside review: permissive hypercapnia . Crit Care . 2005 ; 9 ( 1 ): 51 – 59 .
66. Katsaragakis S , Stamou KM , Androulakis G . Independ-ent lung ventilation for asymmetrical chest trauma: effect on ventilatory and haemodynamic parameters . Injury . 2005 ; 36 ( 4 ): 501 – 504 .
67. Garlick J , Maxson T , Imamura M , Green J , Prodhan P . Differential lung ventilation and venovenous extracor-poreal membrane oxygenation for traumatic bronchop-leural fistula . Ann Thorac Surg . 2013 ; 96 ( 5 ): 1859 – 1860 .
68. Biderman P , Einav S , Fainblut M , Stein M , Singer P , Medalion B . Extracorporeal life support in patients with multiple injuries and severe respiratory failure: a single-center experience ? J Trauma Acute Care Surg . 2013 ; 75 ( 5 ): 907 – 912 .
69. Gothner M , Buchwald D , Schlebes A , Strauch JT , Schild-hauer TA , Swol J . Use of extracorporeal membrane oxygenation in combination with high-frequency oscil-latory ventilation in post-traumatic ARDS . Acta Anaes-thesiol Scand . 2013 ; 57 ( 3 ): 391 – 394 .
70. Schulman CS , Bibro C , Downey DB , Lasich C . Transfer-ring patients with refractory hypoxemia to a regional extracorporeal membrane oxygenation center: key considerations for clinicians . AACN Adv Crit Care . 2014 ; 25 ( 4 ): 351 – 364 .
71. Robinson BR , Cotton BA , Pritts TA , et al. Application of the Berlin definition in PROMMTT patients: the impact of resuscitation on the incidence of hypoxemia . J Trauma Acute Care Surg . 2013 ; 75 ( 1) (suppl 1 ): S61 – S67 .
72. Neamu RF , Martin GS . Fluid management in acute res-piratory distress syndrome . Curr Opin Crit Care . 2013 ; 19 ( 1 ): 24 – 30 .
73. National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network . Wiedemann HP , Wheeler AP , Bernard GR , et al. Comparison of two fluid-management strategies in acute lung injury . N Engl J Med . 2006 ; 354 ( 24 ): 2564 – 2575 .
74. Osman D , Monnet X , Castelain V , et al. Incidence and prognostic value of right ventricular failure in acute res-piratory distress syndrome . Intensive Care Med . 2009 ; 35 ( 1 ): 69 – 76 .
75. Kumar A , Anel R , Bunnell E , et al. Pulmonary artery occlusion pressure and central venous pressure fail to predict ventricular filling volume, cardiac performance, or the response to volume infusion in normal subjects . Crit Care Med . 2004 ; 32 ( 3 ): 691 – 699 .
76. Marik PE , Cavallazzi R . Does the central venous pres-sure predict fluid responsiveness? An updated meta-analysis and a plea for some common sense . Crit Care Med. 2013 ; 41 ( 7 ): 1774 – 1781 .
77. Pinsky MR . Heart-lung interactions . Curr Opin Crit Care . 2007 ; 13 ( 5 ): 528 – 531 .
78. Pinsky MR , Payen D . Functional hemodynamic moni-toring . Crit Care . 2005 ; 9 ( 6 ): 566 – 572 .
79. Renner J , Scholz J , Bein B . Monitoring fluid therapy . Best Pract Res Clin Anaesthesiol . 2009 ; 23 ( 2 ): 159 – 171 .
80. Pinsky MR . Cardiovascular issues in respiratory care . Chest . 2005 ; 128 ( 5) (suppl 2 ): 592S – 597S .
81. Namendys-Silva SA , Dominguez-Cherit G . Mechanical ventilation can cause changes in pulmonary circula-tion . Crit Care Med . 2010 ; 38 ( 8 ): 1759 – 1760 .
82. Feihl F , Broccard AF . Interactions between respiration and systemic hemodynamics. Part II: practical implica-tions in critical care . Intensive Care Med. 2009 ; 35 ( 2 ): 198 – 205 .
83. Guerin C , Reignier J , Richard JC , et al. Prone position-ing in severe acute respiratory distress syndrome . N Engl J Med . 2013 ; 368 ( 23 ): 2159 – 2168 .
84. Jozwiak M , Teboul JL , Anguel N , et al. Beneficial hemo-dynamic effects of prone positioning in patients with acute respiratory distress syndrome . Am J Respir Crit Care Med . 2013 ; 188 ( 12 ): 1428 – 1433 .
85. Lee JM , Bae W , Lee YJ , Cho YJ . The efficacy and safety of prone positional ventilation in acute respiratory dis-tress syndrome: updated study-level meta-analysis of 11 randomized controlled trials . Crit Care Med . 2014 ; 42 ( 5 ): 1252 – 1262 .
86. Ahn Y , Gorlinger K , Alam HB , Eikermann M . Pain-associ-ated respiratory failure in chest trauma . Anesthesiol-ogy . 2013 ; 118 ( 3 ): 701 – 708 .
87. Simon BJ , Cushman J , Barraco R , et al. Pain manage-ment guidelines for blunt thoracic trauma . J Trauma . 2005 ; 59 ( 5 ): 1256 – 1267 .
88. Pressley CM , Fry WR , Philp AS , Berry SD , Smith RS . Predicting outcome of patients with chest wall injury . Am J Surg . 2012 ; 204 ( 6 ): 910 – 913 .
Copyright © 2014 American Association of Critical-Care Nurses. Unauthorized reproduction of this article is prohibited.
NCI-D-14-00039-Online.indd 386NCI-D-14-00039-Online.indd 386 21/10/14 2:53 PM21/10/14 2:53 PM