j brushborder coeliac disease: histochemical evaluation · histology lactase trehalase isomaltase...
TRANSCRIPT

Brush border enzymes in coeliac disease:histochemical evaluation
J Mercer, M E Eagles, I C Talbot
AbstractTwo hundred and ninety four duodenaland jejunal mucosal biopsy specimensfrom patients with coeliac disease,treated and untreated, and other condi-tions were examined histologically and byhistochemical staining for five peptidaseand three disaccharidase enzymes todetermine profiles of activity. Suppres-sion of activity paralleled the histologywith the following enzymes: lactase, tre-halase, brush border endopeptidase,dipeptidyl peptidase H and isomaltase.Lactase, trehalase, and brush borderendopeptidase were specifically suppres-sed in untreated coeliac disease and werediagnostically useful. Examination of a
combination of enzymes is recommen-
ded.
Department ofHistopathology,Leicester RoyalInfirmary, LeicesterLE1 5WWJ MercerM E EaglesDepartment ofPathology, St Mark'sHospital, City Road,London EC1V 2PSI C TalbotCorrespondence to:Dr Jane MercerAccepted for publication16 November 1989
Coeliac disease is diagnosed by the finding ofsubtotal villous atrophy on a jejunal biopsyspecimen followed by recovery on a gluten freediet. Clinical recovery, however, may take timeto establish and the histological assessment of abiopsy specimen may sometimes be difficult.Although subtotal villous atrophy has beenregarded as an essential diagnostic feature, a
few patients with less mucosal damage havebeen found to improve on a gluten free diet,"qand degrees of villous atrophy have been des-cribed in conditions other than coeliac disease.2An additional technique which providessupportive evidence for the diagnosis wouldtherefore be useful.
In 1956 Frazer described the disappearanceof the toxic effect of gliadin peptides in coeliacdisease after digestion with an extract of pig'sintestinal mucosa and concluded that the han-dling of these peptides occurred in the mucosalwall.5 Since then there has been considerableinterest in the enzymes of the small intestinalmucosa in patients with coeliac disease andvarious methods have been used to study manydifferent enzymes. In biochemical assays on
homogenised mucosa some authors haveshown a reduction in peptidase67 anddisaccharidase`1' activities in untreated coeliacdisease. Biochemical assays, however, fail totake into account the fact that many of theseenzymes have more than one location withinthe mucosa. 12 Accurate location ofenzymes canbe achieved by electron microscopy and byimmunocytochemistry, but immunoreactivityfor lactase and sucrase-isomaltase has beenshown to correlate poorly with enzymeactivity. 1
Histochemical techniques show both the
location and activity of an enzyme and can beapplied to small samples of tissue such asendoscopic biopsy specimens. The histo-chemical demonstration of enzyme loss incoeliac disease was first described by Padykulaet al.14 Several subsequent histochemicalstudies have shown a loss or reduction of bothpeptidase and disaccharidase enzymes in activecoeliac disease,6 12 15-19 and at least partialrecovery on a gluten free diet has beenfound."2"9 Such studies can provide a usefulassessment of mucosal damage in coeliacdisease. 12We have used histochemical techniques to
assess the activity of three disaccharidase andfive peptidase enzymes which are normallylocated in the upper small intestinal mucosa.Enzyme activity is related to both the his-tological appearances of the mucosa and to theclinical diagnosis. A simple grading system,which can easily be applied routinely, is used toassess enzyme activity.
MethodsTwo hundred and ninety four biopsyspecimens were obtained from 267 patients: 20patients had more than one biopsy specimentaken. The specimens were taken for the diag-nosis of clinically suspected coeliac disease,assessment ofresponse to a gluten free diet, andinvestigation of anaemia, weight loss, diarr-hoea, failure to grow in childhood, abnormalbutterfat or xylose absorption tests, or a com-bination of these symptoms. The followinginformation was recorded for each patient; age,sex, diet, duration of gluten free diet, symp-toms at presentation and final diagnosis (fromsubsequent investigation and follow up). Thepatients were grouped on final diagnosis (table1). A final diagnosis was not availble for everypatient as some were lost to follow up andothers continue to be investigated. All patientsgrouped as "normal" had both a histologicallynormal biopsy specimen and were found tohave no clinically important illness as a resultof clinical investigations. Biopsy specimensgrouped as "other diagnoses not involvinggastrointestinal tract" included those from
Table 1 Clinical groups: diagnosis after investgation
No ofGroup cases
Normal 8Untreated coeliac disease 34Cocliac on GFD 37Other diagnoses affecting gastrointestinal tract 39Other diagnoses not affecting gastrointestinal tract 49
GFD = gluten free diet.
J Clin Pathol 1990;43:307-312 307 on 29 M
arch 2019 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.43.4.307 on 1 A
pril 1990. Dow
nloaded from
Mercer, Eagles, Talbot
Table 2 Histochemical methods
Enzyme Substrate Notes Referencefor method
Lactase IBF (1, 4) Synthetic substrate Lojda & Kraml 1971"Isomaltase Isomaltose (3) Multistep method using Loida 196720
GOP-PMS-NBT (1) in agaroseTrehalase Trehalose (4) Multistep method using Lojda 196521
GO-PMS-NBT (1) in agaroseDipeptidyl peptidase II (DPP II) Lysyl-alanine-4MNA (1, 5) Coupling agent = Fast Blue B Gossrau 197721
Gossrau & Lojda 198018Dipeptidyl peptidase IV (DPP IV) Glycyl-proline-4MNA (1, 5) As above Lojda 19796Aminopeptidase A (APA) L-glutamyl-4MNA (1, 5) As above Lojda & Gossrau 1980"Aminopeptidase M (APM) L-leucyl-4MNA (1, 5) As above Nachlas et al 1960"Brush border endopeptidase (BBE) Glutamyl-alanyl-alanyl- Incubation on semipermeable Loida 1979"
alanine-4MNA (1, 5) membrane
(1) IBF= 5-bromo-4-chloro-3-indolyl-f-D-fucoside4MNA= 4-methoxy-2-naphthylamideGO-PMS-NBT = glucose oxidase-phenazine methosulphate-nitroblue tetrazolium.
(2) Sigma, Poole, Dorset(3) Fluka, Glossop, Derbyshire(4) Serva, Uniscience Ltd, London(5) Bachem, Bubendorf, Switzerland(6) Other chemical sources - agarose type VII - Sigma, Poole, Dorset
- Harris's haematoxylin - Ortho Diagnostics, High Wycombe, Bucks
patients who, after clinical investigation, had-for example, iron deficiency anaemia due tonon-gastrointestinal haemorrhage, menor-rhagia, dietary anaemia, thyrotoxicosis, hypo-thyroidism, Sjogren's syndrome, depressionand delayed puberty resulting from hormonalabnormalities. Those biopsy specimensgrouped as "other diagnoses involving thegastrointestinal tract" included those frompatients whose final diagnosis was Crohn'sdisease, ulcerative colitis, Menetrier's syn-drome, cow's milk allergy, irritable bowel syn-drome and diverticular disease. The age rangeof patients was 7 months to 89 years. Fifteenpatients were under 1 year old, 59 patients werebetween 1 and 15 years, and the remaining 220were adults.
Biopsy specimens were obtained eitherendoscopically or by Crosby capsule and werereceived fresh. Half of each biopsy specimenwas fixed, paraffin wax embedded, routinelyprocessed, and stained with haematoxylin andeosin for histological examination. The otherhalf was orientated on cork under a dissectingmicroscope and frozen in isopentane cooledin liquid nitrogen. Samples were placed in air-tight tubes and stored in liquid nitrogen untilrequired.
HISTOCHEMICAL TECHNIQUESBiopsy specimens were processed in batches ofeight. Using cryostat sections 8 jim thick, theunfixed sections (except those for lactase) weredelipidised in equal parts of chloroform andacetone at 40C for five minutes. Sections wereincubated with the substrate appropriate toeach enzyme, as described previously (table2).6 15 1722 After incubation, sections for pep-tidases were rinsed in distilled water, chelatedin 2% copper sulphate for five minutes, rinsedagain and fixed in 10% formalin for fiveminutes, then washed and mounted inAquamount. Sections for isomaltase and tre-halase were washed in warm distilled water andthen fixed and mounted as described for pep-tidases. Sections for lactase were rinsed, fixedin 10% formalin, counterstained with 0-1%nuclear fast red in 5% aluminium sulphate,washed, dehydrated, and cleared and mountedin Xam. Negative controls were treated iden-
tically but lacked only the substrate. Allchemicals were of the highest grade (BDH,Poole, Dorset), unless otherwise stated(table 2).
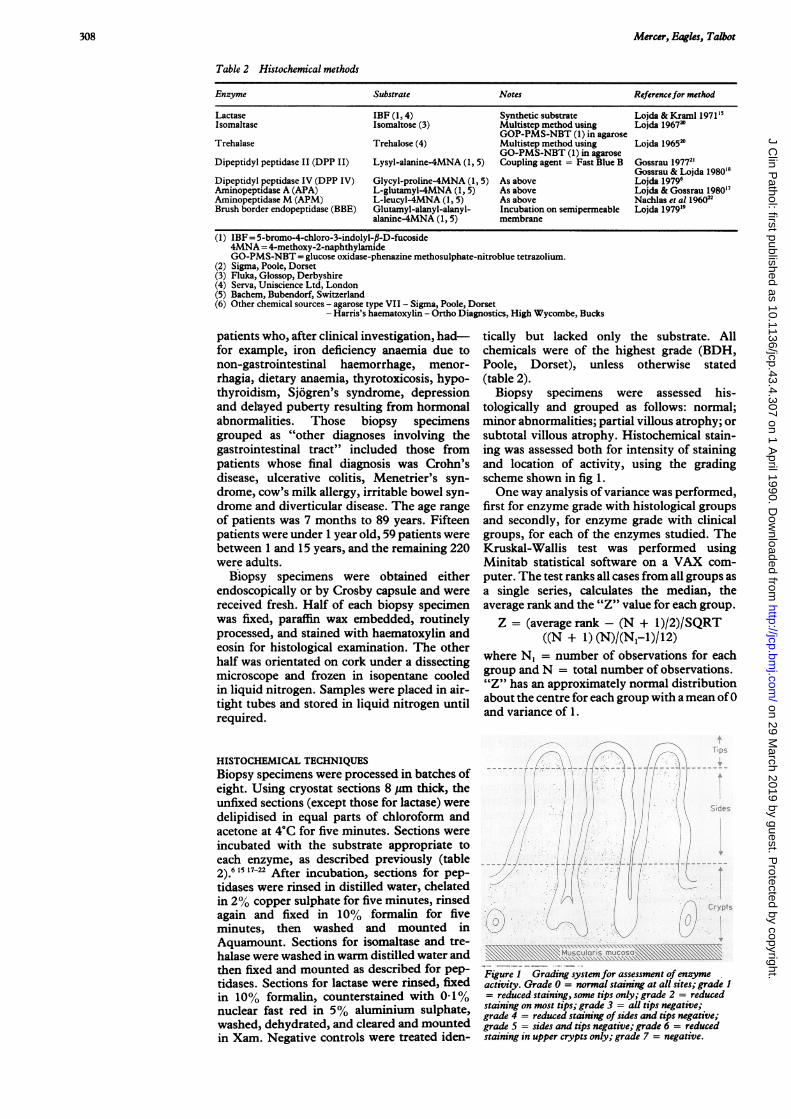
Biopsy specimens were assessed his-tologically and grouped as follows: normal;minor abnormalities; partial villous atrophy; orsubtotal villous atrophy. Histochemical stain-ing was assessed both for intensity of stainingand location of activity, using the gradingscheme shown in fig 1.One way analysis of variance was performed,
first for enzyme grade with histological groupsand secondly, for enzyme grade with clinicalgroups, for each of the enzymes studied. TheKruskal-Wallis test was performed usingMinitab statistical software on a VAX com-puter. The test ranks all cases from all groups asa single series, calculates the median, theaverage rank and the "Z" value for each group.Z = (average rank - (N + 1)/2)/SQRT
((N + 1) (N)/(N1-1)/12)where N, = number of observations for eachgroup and N = total number of observations."Z" has an approximately normal distributionabout the centre for each group with a mean of0and variance of 1.
\ g g ' 'MtS C.-J -12':5> ' .J, CX,. 6
Figure 1 Grading systemfor assessment of enzymeactivity. Grade 0 = normal staining at all sites; grade I= reduced staining, some tips only; grade 2 = reducedstaining on most tips; grade 3 = all tips negative;grade 4 = reduced staining of sides and tips negative;grade 5 = sides and tips negative; grade 6 = reducedstaining in upper crypts only; grade 7 = negative.
308
on 29 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.43.4.307 on 1 April 1990. D
ownloaded from

Brush border enzymes in coeliac disease
Figure 2 Normalstainingfor BBE-grade 0.
Figure 3 Partial villousatrophy in coeliac disease;stainingfor lactase isnegative -grade 7.
A .
'iq
The result of analysis gives the Kruskal-Wallis statistic "H", which has about the samedistribution as x2 with degrees of freedom =
n-i, where n = the number of groups.Probability values for H were obtained fromtables.
ResultsIn the normal cases all the enzymes studiedshowed well localised activity in the brushborder of the upper third of the crypts, thesides, and the tips of the villi (fig 2). Bothaminopeptidase enzymes also stained the lowertwo thirds ofthe crypt epithelium. In abnormalcases the enzyme staining for the peptidasesand lactase was lost sequentially from the tipsof villi, followed by the sides and crypts.Individual enzymes, however, were affected toa variable degree and examples are shown infigs 3 and 4. The methods used for trehalaseand isomaltase gave a more diffuse, generalisedstaining of the biopsy specimen and so couldonly be graded as positive (grade 0), reduced(grade 5), or negative (grade 7).
Analysis of variance between enzyme gradeand histological group showed a highly sig-nificant correlation ( < 0O001) for each of thefollowing enzymes: lactase, trehalase, isomal-tase, DPP II and BBE. The median enzyme
'I,?~_ #__s -?rM- A f
ok
..°- b-
Figure 4 Subtotal villous atrophy in coeliac disease;stainingfor APA is positive -grade 0.
grades for each histological group are shown intable 3. Calculation ofaverage rank (not shown)for each group showed ranking, in increasingorder, from normal histology to subtotal villousatrophy for these enzymes. Biopsy specimenswith subtotal villous atrophy showed thegreatest enzyme loss, with a median grade of 7for all three disaccharidases, and 6, and 6-5,respectively, for DPP II and BBE. Grades forthe group with partial villous atrophy wereslightly lower than those for subtotal villousatrophy but were significantly higher than forthose of the groups with normal histology orminor changes. The best differentiation be-tween groups was given by trehalase, followed,in order, by lactase, BBE, DPP II, and isomal-tase.A significant correlation was also shown
between the same enzymes and the clinicaldiagnosis (lactase, trehalase, and BBE: p <0-001; isomaltase and DPP II: p < 005). Themedian enzyme grade for the diagnostic groupsare shown in table 4. There was considerableoverlap between the enzyme grades for thenormal, other disorders, and other gastrointes-tinal disorders groups but these were clearlydistinguished from the two coeliac groups. Theuntreated coeliac patients gave the highestgrades.There was no significant correlation between
enzyme grade and either histology or diagnosisfor the enzymes DPP IV, APA, and APM (fig4). No association was shown between age andenzyme grade or between sex and enzyme gradefor any of the enzymes studied.
All of the biopsy specimens with subtotalvillous atrophy and all except three of thosewith partial villous atrophy were from patientswith coeliac disease. The three exceptions eachpresented with iron deficiency anaemia and anabnormal butterfat absorption test. Onepatient, a 41 year old man, also had B12deficiency and pernicious anaemia was sub-
Table 3 Analysis of variance ofenzyme grade with histology
Median enzyme grades
Histology Lactase Trehalase Isomaltase BBE DPPII DPPIV APA APM
Normal 30 00 00 30 30 10 10 00Mild changes 3 0 5 0 0 0 2-0 3 0 0.0 0 0 0.0Partial villous atrophy 7 0 7-0 5 0 5-0 4 0 0.0 0.0 0.0Subtotal villous atrophy 7-0 7-0 7-0 6-5 6-0 2-0 2-0 0.0Number of observations 244 272 130 173 217 76 78 79Kruskal-Wallis "H" statistic 68-47 82-42 24-24 51-81 31 40 3-642 5 140 1-722Significance 0-001 0-001 0 001 0-001 0-001 Not signif Not signif Not signif
309
F.-..A
ip %:.
I'.,a I
I....
,-?' t
----ax-ffi 2
on 29 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.43.4.307 on 1 April 1990. D
ownloaded from
Mercer, Eagles, Talbot
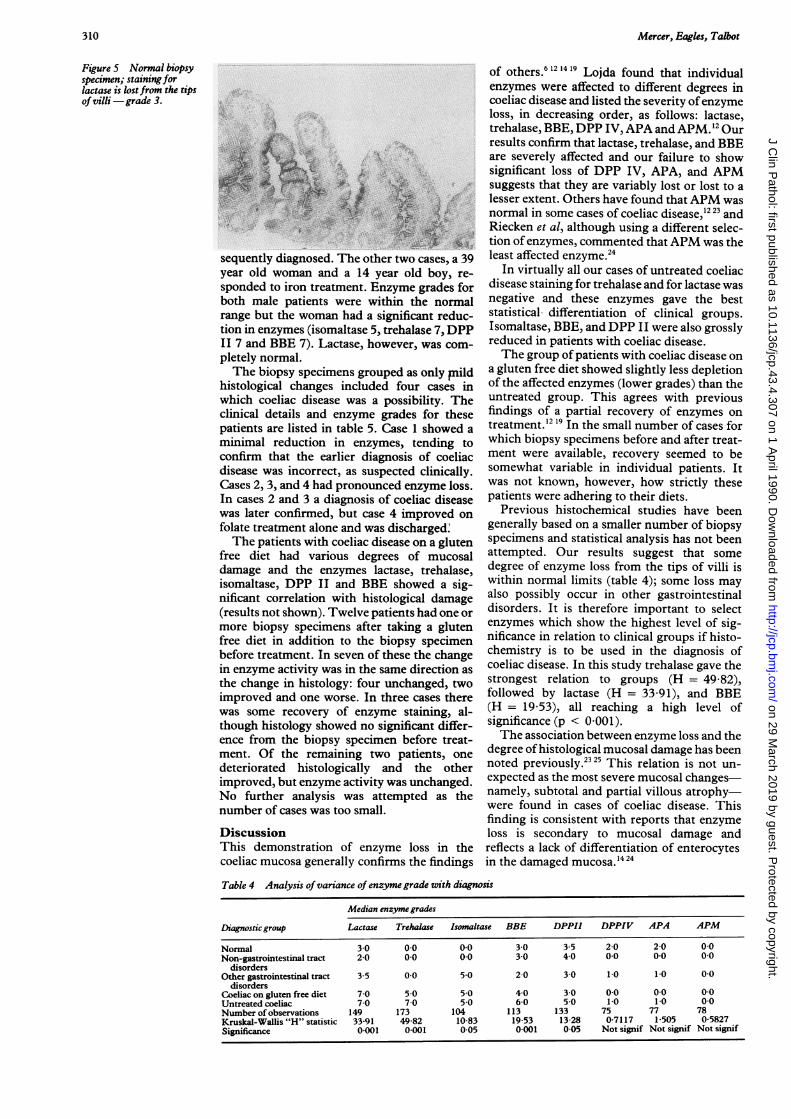
Figure 5 Normal biopsyspecimen; staining forlactase is lostfrom the tipsof villi -grade 3.
12
-~~~~~~~~~-A
sequently diagnosed. The other two cases, a 39year old woman and a 14 year old boy, re-sponded to iron treatment. Enzyme grades forboth male patients were within the normalrange but the woman had a significant reduc-tion in enzymes (isomaltase 5, trehalase 7, DPPII 7 and BBE 7). Lactase, however, was com-
pletely normal.The biopsy specimens grouped as only pnild
histological changes included four cases inwhich coeliac disease was a possibility. Theclinical details and enzyme grades for thesepatients are listed in table 5. Case 1 showed aminimal reduction in enzymes, tending toconfirm that the earlier diagnosis of coeliacdisease was incorrect, as suspected clinically.Cases 2, 3, and 4 had pronounced enzyme loss.In cases 2 and 3 a diagnosis of coeliac diseasewas later confirmed, but case 4 improved on
folate treatment alone and was discharged.The patients with coeliac disease on a gluten
free diet had various degrees of mucosaldamage and the enzymes lactase, trehalase,isomaltase, DPP II and BBE showed a sig-nificant correlation with histological damage(results not shown). Twelve patients had one ormore biopsy specimens after taking a glutenfree diet in addition to the biopsy specimenbefore treatment. In seven of these the changein enzyme activity was in the same direction asthe change in histology: four unchanged, twoimproved and one worse. In three cases therewas some recovery of enzyme staining, al-though histology showed no significant differ-ence from the biopsy specimen before treat-ment. Of the remaining two patients, onedeteriorated histologically and the otherimproved, but enzyme activity was unchanged.No further analysis was attempted as thenumber of cases was too small.
DiscussionThis demonstration of enzyme loss in thecoeliac mucosa generally confirms the findings
of others.6 12 1419 Lojda found that individualenzymes were affected to different degrees incoeliac disease and listed the severity ofenzymeloss, in decreasing order, as follows: lactase,trehalase, BBE, DPP IV, APA and APM. 2 Ourresults confirm that lactase, trehalase, and BBEare severely affected and our failure to showsignificant loss of DPP IV, APA, and APMsuggests that they are variably lost or lost to alesser extent. Others have found that APM wasnormal in some cases of coeliac disease,'2 23 andRiecken et al, although using a different selec-tion ofenzymes, commented that APM was theleast affected enzyme.24
In virtually all our cases of untreated coeliacdisease staining for trehalase and for lactase wasnegative and these enzymes gave the beststatistical differentiation of clinical groups.Isomaltase, BBE, and DPP II were also grosslyreduced in patients with coeliac disease.The group of patients with coeliac disease on
a gluten free diet showed slightly less depletionof the affected enzymes (lower grades) than theuntreated group. This agrees with previousfindings of a partial recovery of enzymes ontreatment.'2 19 In the small number of cases forwhich biopsy specimens before and after treat-ment were available, recovery seemed to besomewhat variable in individual patients. Itwas not known, however, how strictly thesepatients were adhering to their diets.
Previous histochemical studies have beengenerally based on a smaller number of biopsyspecimens and statistical analysis has not beenattempted. Our results suggest that somedegree of enzyme loss from the tips of villi iswithin normal limits (table 4); some loss mayalso possibly occur in other gastrointestinaldisorders. It is therefore important to selectenzymes which show the highest level of sig-nificance in relation to clinical groups if histo-chemistry is to be used in the diagnosis ofcoeliac disease. In this study trehalase gave thestrongest relation to groups (H = 49 82),followed by lactase (H = 33 91), and BBE(H = 19 53), all reaching a high level ofsignificance (p < 0 001).The association between enzyme loss and the
degree of histological mucosal damage has beennoted previously.2325 This relation is not un-expected as the most severe mucosal changes-namely, subtotal and partial villous atrophy-were found in cases of coeliac disease. Thisfinding is consistent with reports that enzymeloss is secondary to mucosal damage andreflects a lack of differentiation of enterocytesin the damaged mucosa. 14 24
Table 4 Analysis ofvariance of enzyme grade with diagnosis
Median enzyme grades
Diagnostic group Lactase Trehalase Isomaltase BBE DPPII DPPIV APA APM
Normal 3-0 0 0 0.0 3 0 3-5 2-0 2-0 0.0Non-gastrointestinal tract 2-0 00 00 3-0 40 00 00 0 0
disordersOther gastrointestinal tract 3-5 0 0 5-0 2 0 3-0 1.0 1 0 0 0
disordersCoeliac on gluten free diet 7-0 5 0 5-0 40 3 0 00 0 0 0.0Untreatedcoeliac 7-0 7-0 5-0 6-0 5-0 1 0 1 0 0 0Numberofobservations 149 173 104 113 133 75 77 78Kruskal-Wallis "H" statistic 33-91 49-82 10-83 19 53 13 28 0-7117 1 505 0-5827Significance 0 001 0-001 0-05 0 001 0-05 Not signif Not signif Not signif
310
on 29 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.43.4.307 on 1 April 1990. D
ownloaded from

Brush border enzymes in coeliac disease
Table 5 Possible cases of coeliac disease with only mnnor histological abnormalities
Enzyme gradesCaseNo Lactase Trehalase Isomaltase BBE DPPII Clinical details
1 3 0 0 0 0 17 year old female; coeliac diagnosed at age 7 months, offGFD for 5 years at time of biopsy ? Not coeliac
2 7 7 5 6 - 38 year old female; diarrhoea, epigastric pain + anaemiaat time of biopsy. Repeat biopsy 4 months later - partialvillous atrophy Improved on GFD
3 7 7 - - 7 77 year old female; abdominal pain, weight loss,abnormal butterfat + xylose absorption at time ofbiopsy. Improved on GFD. Died two years later fromsmall bowel lymphoma
4 4 7 7 7 6 64 year old female; folate deficiency and abnormalbutterfat absorption at time of biopsy. Improved onfolate treatment and discharged without furtherinvestigation
The exceptional cases, which showedenzyme loss disproportionate to histologicalchanges, are of particular interest. The threepatients with anaemia and partial villous atro-phy, of which two had normal enzymes, aredifficult to explain. Shiner in 1959 reportedpartial villous atrophy in association with folicacid deficiency,2 but neither iron deficiency norpernicious anaemia are usually associated withclinically important mucosal damage. Cases 2,3, and 4 in table 5 had only minor histologicaldamage but pronounced enzyme loss andprobably all represent true cases of coeliacdisease. In two of these subsequent recovery ona gluten free diet tended to confirn this. Incase 4 the patient was discharged after im-provement on folate treatment and the diag-nosis remains open. Repeated sampling of themucosa in one patient shows variation in thedegree of histological damage2326 and ourpatients may have had more severe mucosalchanges at adjacent sites. Enzyme assessmentin these cases provided evidence to support adiagnosis of coeliac disease and the diagnosismay have been missed on histology alone.The grading system used in this study asses-
sed both the site and intensity of staining.Although the site of staining could not beassessed for trehalase and isomaltase, stainingfor lactase, BBE, and DPP II was frequentlyabsent or reduced on the tips of villi in bothclinically normal patients (table 4) and inhistologically normal biopsy specimens (table3). The site of staining loss therefore seems tobe an important part of the assessment. Insubtotal villous atrophy villi are virtuallyabsent and so it is only possible to assessstaining along the luminal surface and in thecrypts. Staining of the luminal surface forlactase, BBE, and DPP II was invariably absentin subtotal villous atrophy so that assigning agrade to this area was never a problem. Absenceof staining on the luminal surface was quiteoften associated with weak staining of theupper crypts, confirming previous findingsthat the greatest enzyme loss occurs from theluminal surface.'2 14 23Enzyme activity has been shown to vary with
age, sex, and site of biopsy in biochemicalassays.27 We were unable to show any correla-tion with age or sex, but the small number ofchildren in this study may be partly responsiblefor this. Biopsy specimens were obtained bothendoscopically and via a Crosby capsule, but
any effect of the difference in site was notanalysed. Keane et al used both types ofbiopsyspecimens and found that all sites from thesecond part of the duodenum to distal jejunumwere adequate for enzyme assessment.' All theenzymes used in this study have previouslyshown in both the jejunum and duodenum."'9
In conclusion, our results suggest that thehistochemical assessment ofenzymes is a usefuladdition to routine histology in the diagnosis ofcoeliac disease and may occasionally directattention to cases which would have beenmissed on histology alone. It also provides abaseline for assessing mucosal recovery aftertreatment. The choice of enzymes is importantand our results show lactase, trehalase, andBBE to be the most useful. Although thedisaccharidases are generally more severelyaffected than the peptidase enzymes, lactasedeficiency is well known to occur as a primaryenzyme defect and as an acquired phenomenonin many gastrointestinal disorders, andprimary trehalase deficiency has also beendescribed.'s Examination of a combination ofenzymes is therefore recommended.
We thank the clinicians who cooperated in this study, especiallyDr D Carr-Locke. We are also grateful to Dr Carole Jagger forher invaluable advice on statistical methods, and to MrsMargaret Hornby for typing the manuscript.
1 Roy-Choudhury D, CookeWT, TanDT, Banwell JG, SmitsBJ. Jejunal biopsy: criteria and significance. Scand JGastroenterol 1966;1:57-74.
2 Shiner M. Small intestinal biopsy: diagnostic and researchvalue. Proc Roy Soc Med 1959;52:10-4.
3 Egan-Mitchell B, Fottrell PF, McNicholl B. Early or pre-coeliac mucosa: development of gluten enteropathy. Gut1981;22:65-9.
4 O'Farrelly C, Graeme-Cook F, HourihaneD O'B, FeigheryC. Histological changes associated with wheat proteinantibodies in the absence of villous atrophy. J Clin Pathol1987;40: 1228-30.
5 Frazer AC. Discussion on some problem of steatorrhoea andreduced stature. Proc Roy Soc Med 1956;49:1009-13.
6 Loida Z. Studies on dipeptidyl (amino) peptidase IV(glycyl-proline-naphthylamidase) II. Blood Vessels.Histochemistry 1979;59:153-66.
7 Sjostrom H, Noren 0, KrasilnikoffPA, Gudmand-Hoyer E.Intestinal peptidases and sucrase in coeliac disease. ClinChim Acta 1981;109:53-8.
8 Andersen KJ, Schionsby H, Skagen DW. Jejunal mucosalenzymes in untreated and treated coeliac disease. Scand JGastroenterol 1983;18:251-6.
9 O'Grady JG, Sterens FM, Keane R, et al. Intestinal lactase,sucrase, and alkaline phosphatase in 373 patients withcoeliac disease. J Clin Pathol 1984;37:298-301.
10 Bramble MG, Zucoloto S, Wright NA, Record CO. Acutegluten challenge in treated adult coeliac disease: a mor-phometric and enzymatic study. Gut 1985;26:169-74.
11 Andersen KJ, Schjonsby H, Skagen DW, Haga HJ. Enzymeactivities in jejunal biopsy samples from patients withadult coeliac disease with and without steatorrhoea. ScandJ Gastroenterol 1983;18:365-8.
12 Loida Z. Proteinases in pathology. Usefulness of histo-chemical methods. J Histochem Cytochem 1981;29(3A):
311
on 29 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.43.4.307 on 1 April 1990. D
ownloaded from

Mercer, Eagles, Talbot
481-93.13 Loida Z, Smidova J, Kolinsrkja J, Kraml J. A conparative
_study of lactase and sucrase-isomaltase activities andimmunoreactivities in jejunal biopsies of patients suffer-ing from the mnalabsorption syndrome. Histochem J 1984;16:373-6.
14 Padykula HA, Strauss EW, Ladman AJ, Gardner FH. Amorphological and histochemical analysis of the humanjejunal epithelium in nontropical sprue. Gastroenterology1961;40:735-65.
15 Loida Z, Kraml J. Indigogenic methods for glycosidases III.
An improved method with 4-Cl-5-Br-3-Indolyl-B-D-fucoside and its application in studies of enzymes in theintestine, kidney and other tissues. Histochemie1971;25:195-207.
16 Lojda Z. The histochemical demonstration of peptidases bynatural substances. Histochemistry 1979262:305-23.
17 Lojda Z, Gossrau R. Study on aminopeptidase A. Histo-chemistry 1980;67:267-90.
18 Gossrau R, Lojda Z. Study on dipeptidyl peptidase II (DPP11). Histochemistry 1980;70:53-76.
19 Lojda Z. The histochemical demonstration of brush borderendopeptidase. Histochemistry 1979;64:205-21.
20 Lojda Z. Some remarks concerning the histochemicaldetection of disaccharidases and glucosidases. Histochemie1965,5:339-60.
21 Gossrau R. Peptidasen. I. Histochemische Untersuchungen
mit 2-Naphtylamiden und Hexazonium-p-rosanilin.Ifistochemistry 1977;54:311-30.
22 Nachlas MM, Mavis B, Rosenblatt D, Seligmas AM.Improvement in histochemical localisation of leucineaminopeptidase with a new substrate, L-leucyl-4-meth-oxy-2-naphthylamide. Journal of Biophysical and Bio-chemical Cytology 1960;7:262-4.
23 Spiro HM, Filipe MI, Stewart JS, Booth CC, Pearse AGE.Functional histochemistry of the small bowel mucosa inmalabsorptive syndromes. Gut 1964;5: 145-54.
24 Riecken EO, Stewart JS, Booth CC, Pearse AGE. Ahistochemical study on the role of lysosomal enzymes inidiopathic steatorrhoea before and during a gluten-freediet. Gut 1966;7:317-32.
25 O'Grady JG, Stevens FM, Keane R, et al. Intestinal lactase,sucrase and alkaline phosphatase in 273 patients withcoeliac disease. J Clin Pathol 1984;37:298-301.
26 Scott BB, Losowsky MS. Patchiness and duodenal-jejunalvariation ofthe mucosal abnormality in coeliac disease anddermatitis herpetiformis. Gut 1976;17:984-92.
27 Keane R, O'Grady JG, Sheil J, et al. Intestinal lactase,sucrase and alkaline phosphatase in relation to age, sex andsite of intestinal biopsy in 477 Irish subjects. J Clin Pathol1983;36:74-7.
28 Bergoz R, Vallotton M-C, Loizeau E. Trehalase deficiency.Prevalence and relation to single-cell protein food. AnnNutr Metabol 1982;26:291-5.
312
on 29 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.43.4.307 on 1 April 1990. D
ownloaded from