it doesn’t work if it doesn’t get into your lungs!scasthmaalliance.org/pdf/asthma med-device...
TRANSCRIPT

It doesn’t work if it doesn’t get into
your Lungs!
Aimee Tiller, RN, AE-C
Asthma Nurse Coordinator
Pediatric Pulmonology, MUSC

Asthma Medications

Asthma Medications
Short acting beta agonists (SABAs)
- quick relief
- relieves acute bronchospasm
- fast onset 5-15 minutes
Examples: Albuterol (Proventil, Ventolin, ProAir), Levalbuterol (Xopenex), Pirbuterol (Maxair)

Asthma Medications
Inhaled Corticosteroids
Gold standard in chronic asthma management
Inhibits late phase response
Treats inflammatory component of asthma
Low systemic bioavailability
Most common side effects – thrush, hoarseness – can be avoided by rinsing mouth

Asthma Medications
Inhaled Steroids
Some evidence of growth slowing during first year (? 1 cm)
If on high dose, long term – consider bone density, optho screening
Examples – Fluticasone (Flovent HFA), Budesonide (Pulmicort Respules / Flexhaler), Beclomethasone (QVAR)
Asthma Medications
Long acting beta agonists (LABAs)
Intended for use in pts with moderate to severe asthma uncontrolled on a medium dose ICS
Helpful in pretreating before exercise in children who find pretreating with albuterol doesn’t last long enough
Examples are Serevent or Foradil

Asthma Medications
LABAs - Currently a black box warning on all LABAs and products containing LABAs
SMART study:
compared salmeterol to placebo
increased asthma related deaths in salmeterol group, especially among African Americans
Overall low use of ICS in both groups, fewer in AA’s
Most likely, salmeterol was masking asthma symptoms
Take home message – not first line therapy, use with ICS, choose candidates wisely
Examples: Salmeterol (Serevent), Formoterol (Foradil)

Asthma Medications
Combination Products – ICS + LABA
Useful in moderate to severe asthma
Helpful in kids who need both products – convenient for pt, providers don’t need to worry that pt is only taking the LABA
Examples (Advair – fluticasone and salmeterol, Symbicort – budesonide and
formoterol)

Asthma Medications
Leukotriene Modifiers:
Stops inflammatory cascade
ICS still first line treatment, though can consider monotherapy in those with mild symptoms
May be helpful in those with associated allergy symptoms
Examples – montelukast (Singulair) – preferred as is once daily dosing

Asthma Medications
Methylzanthines
Long acting bronchodilators
Requires close monitoring of drug levels
Can cause toxicity with permanent CNS damage
Recheck levels if symptoms of toxicity, continued asthma symptoms, or with viral illnesses
Rarely used in pediatrics because of these issues
Examples: Theophylline

Asthma Medications
Mast cell stabilizers:
Anti-inflammatories
Not as effective as ICS
Often require TID – QID dosing
Rarely used in children because of the above
Examples: Cromolyn, Nedocromil (Tilade)
Asthma Medications
Medications are available in several delivery forms:
Metered dose inhalers – should be used with a spacer
Dry powder inhalers Nebulized Oral – tablet / liquid Goal is to pick the best route of delivery for each
patient

Asthma Medications
Special Considerations
Nebulized medications – especially Pulmicort must be delivered with a face mask in young children – no blow by!
Flovent, QVAR, and Advair – must be BID dosing – when weaning, wean dose, not frequency
Pulmicort or Asmanex may be given once daily

Asthma Medications
Age considerations
Flovent (44mcg) – approved down to age 4 years
QVAR – approved down to age 5 years
Pulmicort Respules – approved down to 12 months
Singulair approved down to age 6 months
Symbicort – approved down to age 12 years
Advair diskus – approved down to age 4 years
Advair HFA – approved down to age 12

Asthma Medications
Using an MDI with spacer and mask
1. Remove the cap
2. Shake the MDI
3. Assemble the MDI in the chamber
4. Apply the mask to face
5. Depress canister
6. Watch child take 5-6 breaths

Asthma Medication
Using an MDI with spacer 1. Remove the cap 2. Shake the MDI 3. Assemble the MDI
mouthpiece in the chamber
4. Seal lips around spacer and exhale
5. Depress canister and slowly inhale (should not whistle)
6. Hold breath 10 seconds 7. Exhale

Asthma Medications
Care of an aerochamber
Wash in warm soapy water about once a week
A film within the spacer is normal and should not be “scrubbed out” helps eliminate static
Rinse and shake off excess water
Allow to air dry – do not towel dry
Asthma Medications
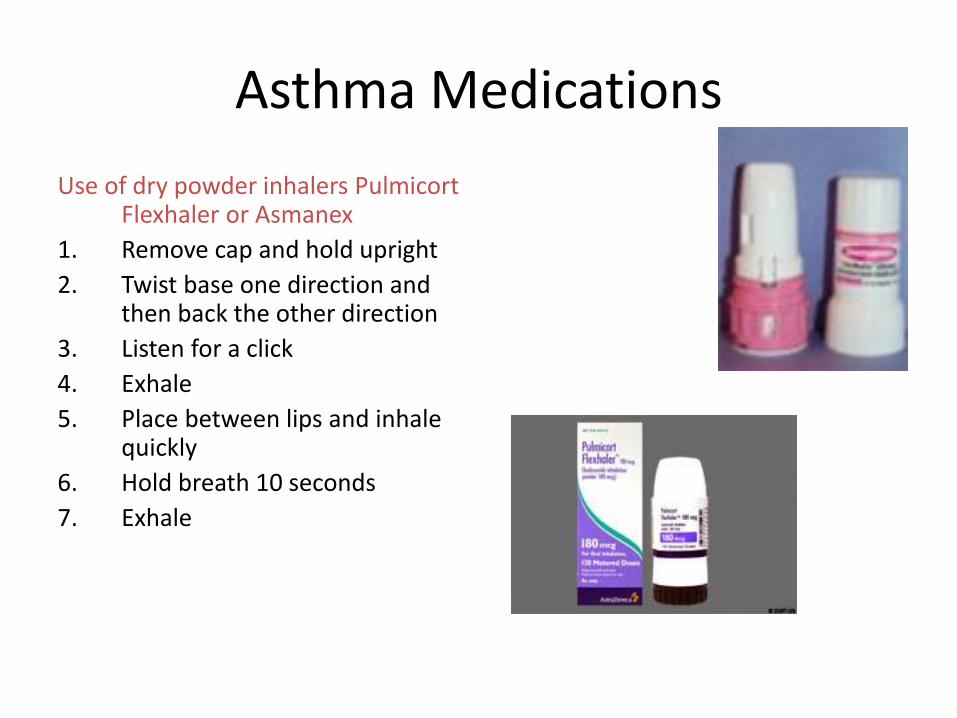
Use of dry powder inhalers Pulmicort Flexhaler or Asmanex
1. Remove cap and hold upright
2. Twist base one direction and then back the other direction
3. Listen for a click
4. Exhale
5. Place between lips and inhale quickly
6. Hold breath 10 seconds
7. Exhale

Asthma Medications Use of a diskus – Advair,
Servent 1. Open the diskus 2. Slide the lever until it
clicks 3. Exhale 4. Seal lips around mouth
piece and inhale quickly 5. Hold breath x 10
seconds 6. Exhale and close the
disk

Asthma Medications
Use of a nebulizer 1. Attach tubing to air outlet 2. Unscrew top of medicine cup 3. Fill cup with med and replace cap 4. Turn on compressor 5. Place mask on face or mouthpiece in mouth 6. Normal breathing or slow deep breaths for
duration of treatment – usually small amount of med that can’t be nebulized
7. Complete treatment and turn off compressor

Asthma Management
Education is key – repeat over and over
Show patient and family how to use the device chosen – check technique at every visit
Written asthma action plans
Peak flow monitoring

Asthma Action Plan

Asthma Action Plans: • Updated and reviewed at every visit •Copy given to family and given extra copy for school, daycare, etc… •Daily medicines in green zone also include meds for allergies and reflux •Include Peak Flow Zones for those pts of age

Peak Flow Meters: A peak flow meter is a small, hand-held device used to monitor a person's ability to breathe out air. It measures the airflow through the bronchi and thus the degree of obstruction in the airways -Measures the patient’s maximum speed of expiration, or peak expiratory flow rate (PEF)

Asthma Management
Peak flow meters
Home device where patients blow as hard as they can into device to get reading
Norms are based on height
Usually results divided into green zone (>80% predicted), yellow zone 60-80% predicted) or red zone (< 60% predicted)

Asthma Management
Peak flow meters
Choose candidates wisely – adds “one more thing”
Helpful in kids who are poor perceivers or parents who are unsure “if this is asthma”
Can be done daily, or prn after establishing child’s “norm”

Trouble shooting Considerations if not getting better
- They aren’t taking their medication (check a refill history)
- They aren’t taking their medication correctly (check technique)
** Both come from lack of understanding
- Not the right medication for that child
- Not the right delivery method for that child
- Co-morbid condition – GERD, allergies, sinusitis
- Environmental factors – smoke, allergens
- It’s not asthma – VCD, CF, airway anomaly
Asthma Management
Compliance
A HUGE ISSUE with asthma
A 2005 study showed that:
An ICS is filled an average of 2.29 x / yr
Advair diskus filled an average of 3.98 x / yr
Singulair is filled an average of 4.33 x / yr
Bottom line – suspect poor medication adherence – call the insurance company or pharmacy for a refill history

Asthma Management
Assessing compliance
Ask how many doses they think they miss a week
Ask where the controller inhaler is located
Ask who is responsible for remembering the medication
Ask parent if they personally observe each dose
Ask parent if they check the dose counter

Asthma Management
Improving compliance Acknowledge that it’s a difficult thing Suggest the inhaler not be kept in the child’s bedroom
or even bathroom Ask parents not just to remind the child, but to
personally observe each dose – good time to bring up developmental considerations
Remind parent that certain inhalers do have counters, and if they don’t most inhalers have exactly enough for 30 days – then the medicine is gone, even if the inhaler doesn’t feel empty

Asthma Management
Improving compliance
Use sticker calendars to help remember doses
Consider med choices carefully – do they really need every they’re on, can something be QD vs BID, etc
Get the school involved
Encourage positive reinforcement
Frequent follow up

Asthma Management
School and Daycare issues
Educate caregivers on s/s of asthma and how to relieve symptoms
Every child should have a rescue medication available at school and staff should be trained to administer it – check expiration dates
Provide school with written asthma action plan and emergency phone numbers
Encourage participation in physical activity – recess, PE, sports activities

Summary:
•Make sure patient and family know difference between controller vs. rescue •Patient and family should have Asthma Action Plan and understand it •Patient and family should correctly know how and when to administer meds •Review inhaler technique and review/update AAP at every clinic visit
