ischemic mitral regurgitation: unusual approaches for correction
TRANSCRIPT

Ischemic Mitral Regurgitation: Unusual Approachesfor Correction
Judy Hung
Published online: 1 September 2010# Springer Science+Business Media, LLC 2010
Abstract Ischemic mitral regurgitation (MR) results fromischemic left ventricular distortion with tethering of themitral leaflets. The standard surgical therapy for ischemicMR is mitral ring annuloplasty, often performed at the timeof coronary artery bypass surgery. However, ring annulo-plasty is associated with an up to 30% recurrence rate ofMR, as it does not directly address ventricular distortionand tethering of the mitral leaflets and there is often furtherventricular remodeling following bypass surgery. Thisarticle reviews the background and mechanism of ischemicMR and unusual approaches to this important yet difficultto treat valvular problem.
Keywords Mitral regurgitation . LV remodeling
Introduction
Ischemic mitral regurgitation (MR) is a common compli-cation of coronary artery disease that conveys adverseprognosis, more than doubling the risk of late death [1–3].It occurs in approximately 25% of patients followingmyocardial infarction and in up to 50% of patients withheart failure and cardiomyopathy [4–8]. This adverseprognosis is related to the degree of MR, with thedevelopment of just mild MR contributing to mortality [4,5]. MR is also frequent in patients with global left
ventricular (LV) dysfunction, and is a potent stimulus foradverse LV remodeling, which begets further MR. Themechanism of ischemic MR relates to remodeling anddistortion of the ischemic left ventricle following infarction[9, 10]. Ischemic LV distortion leads to thinning anddisplacement of the myocardium supporting the papillarymuscles (PMs) to which the mitral leaflets are anchored.Displacement of these muscles tethers the leaflets andrestricts leaflet closure, resulting in MR (Fig. 1) [11].
Although ischemic MR may be reduced with contractileimprovement due to coronary revascularization, thisrequires sufficient functional improvement to change LVdimensions and reduce tethering [12–18], which may notoccur in the chronically infarcted heart. Aklog et al. foundthat following revascularization alone, moderate or severeMR persisted in 77% of patients [19]. Standard surgicaltherapy for functional MR at the time of revascularizationinvolves placing an annuloplasty ring, designed to restorecoaptation by correcting posterior annular dilation.
While ring annuloplasty is effective in some patients,results are variable, with important (moderate or greater)persistent MR often recurring months postoperatively inapproximately 30% of patients [20–24]. Importantly,however, annuloplasty aims at a moving target: initiallyeffective annuloplasty may later fail as the left ventriclecontinues to remodel and tethering increases [25]. Ringinsertion also shifts the posterior annulus anteriorly, whilethe ischemic PM remains posterior, which restricts theanterior excursion of the posterior leaflet toward coaptationwith the anterior leaflet [26].
Disappointment with the benefits of annuloplasty alone,in view of the added risks of prolonging cardiopulmonarybypass and ischemic time and the relatively high mortality[27], led McGee et al. from the Cleveland Clinic toconclude that “the development of additional techniques is
J. Hung (*)Cardiac Ultrasound Laboratory, Massachusetts General Hospital,Boston, MA, USAe-mail: [email protected]
J. HungHarvard Medical School,Boston, MA, USA
Curr Cardiovasc Imaging Rep (2010) 3:396–402DOI 10.1007/s12410-010-9043-7
necessary to achieve more secure repair of functionalischemic mitral regurgitation” [24].
Chordal Cutting
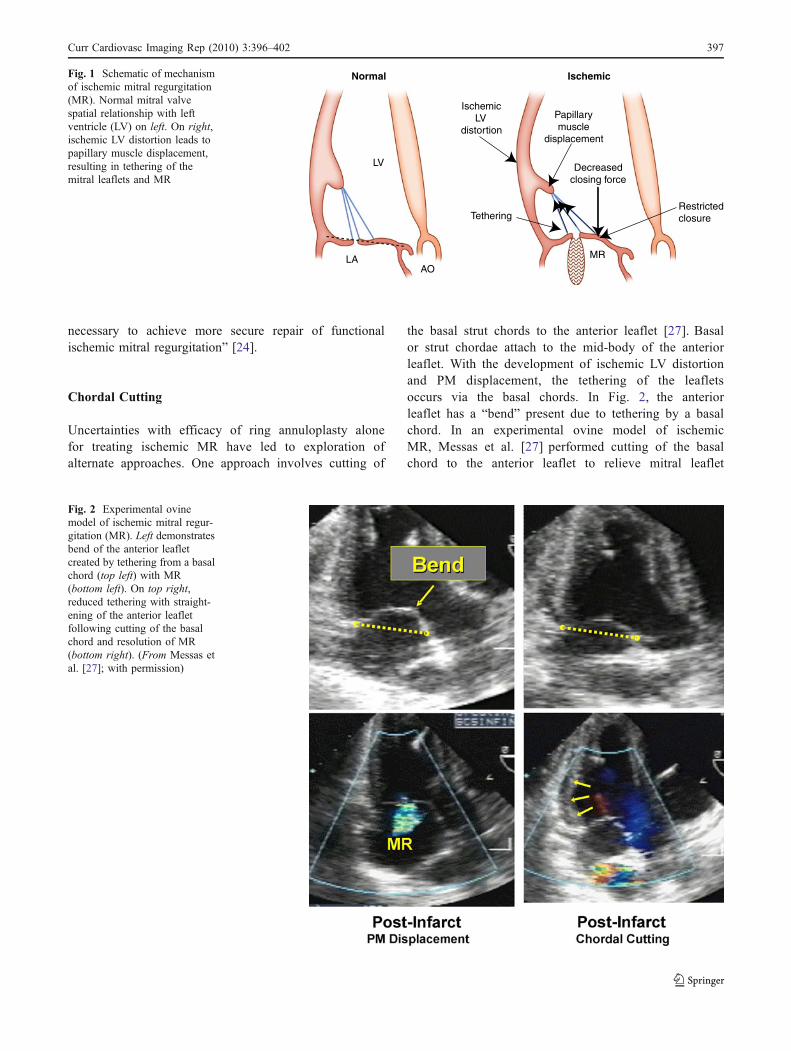
Uncertainties with efficacy of ring annuloplasty alonefor treating ischemic MR have led to exploration ofalternate approaches. One approach involves cutting of
the basal strut chords to the anterior leaflet [27]. Basalor strut chordae attach to the mid-body of the anteriorleaflet. With the development of ischemic LV distortionand PM displacement, the tethering of the leafletsoccurs via the basal chords. In Fig. 2, the anteriorleaflet has a “bend” present due to tethering by a basalchord. In an experimental ovine model of ischemicMR, Messas et al. [27] performed cutting of the basalchord to the anterior leaflet to relieve mitral leaflet
LV
LA
Normal
AO
Ischemic
MR
TetheringRestrictedclosure
Papillarymuscle
displacement
IschemicLV
distortion
Decreasedclosing force
Fig. 1 Schematic of mechanismof ischemic mitral regurgitation(MR). Normal mitral valvespatial relationship with leftventricle (LV) on left. On right,ischemic LV distortion leads topapillary muscle displacement,resulting in tethering of themitral leaflets and MR
Fig. 2 Experimental ovinemodel of ischemic mitral regur-gitation (MR). Left demonstratesbend of the anterior leafletcreated by tethering from a basalchord (top left) with MR(bottom left). On top right,reduced tethering with straight-ening of the anterior leafletfollowing cutting of the basalchord and resolution of MR(bottom right). (From Messas etal. [27]; with permission)
Curr Cardiovasc Imaging Rep (2010) 3:396–402 397

tethering and demonstrated reduction in MR comparedto controls.
Borger et al. [28••] compared 49 patients with coronaryartery disease and MR who underwent standard therapywith coronary artery bypass graft and mitral valve annulo-plasty to 43 patients who also underwent chordal cutting ofthe basal chord. There was no difference in mortalitybetween the group that also had chordal cutting and thegroup that did not (Fig. 3). However, there was a significantdecrease in MR in the group that underwent chordal cutting(Fig. 4).
Ventricular Approaches
Direct remodeling of the left ventricle by repositioning ofthe PMs is another approach that has been proposed as atherapeutic target to reduce ischemic MR. A number ofsurgical therapies (both experimentally and in patients)that reposition the PMs to reduce tethering of the mitralleaflets have been developed as adjunctive or alternateapproaches to standard mitral ring annuloplasty (Table 1)[29••, 30–33].
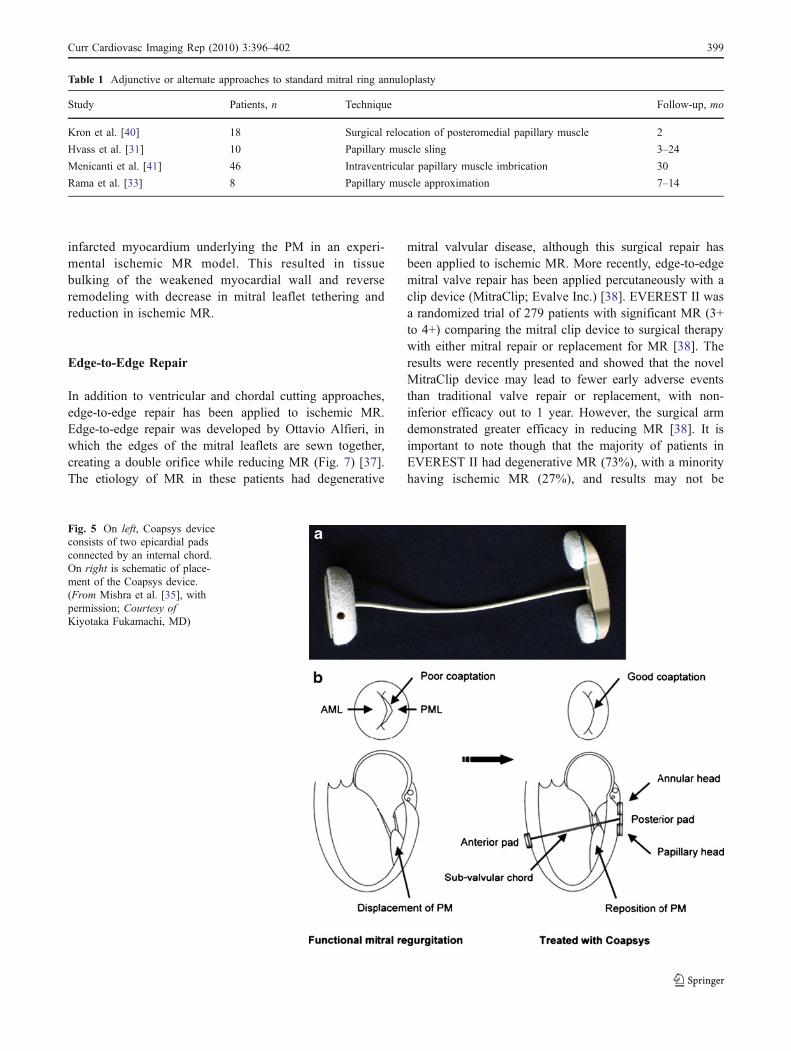
The Coapsys device (Myocor Inc.) was one of the firstdevice-based ventricular approaches designed to treatischemic MR [34]. This device consists of two epicardialpads that are connected through an internal cord (Fig. 5)[34]. It has the advantage over ring annuloplasty in that itcan be placed on a beating heart without cardiopulmonarybypass [35]. Follow-up of the first 11 patients with aCoapsys device and off-pump coronary artery bypass graftshowed an improvement in reoperative MR grade 2.9±0.5to grade 1.1±0.8 at 1 year (P<0.05) [35]. A phase 2 trialwas completed but has not been reported, and the companyis no longer active.
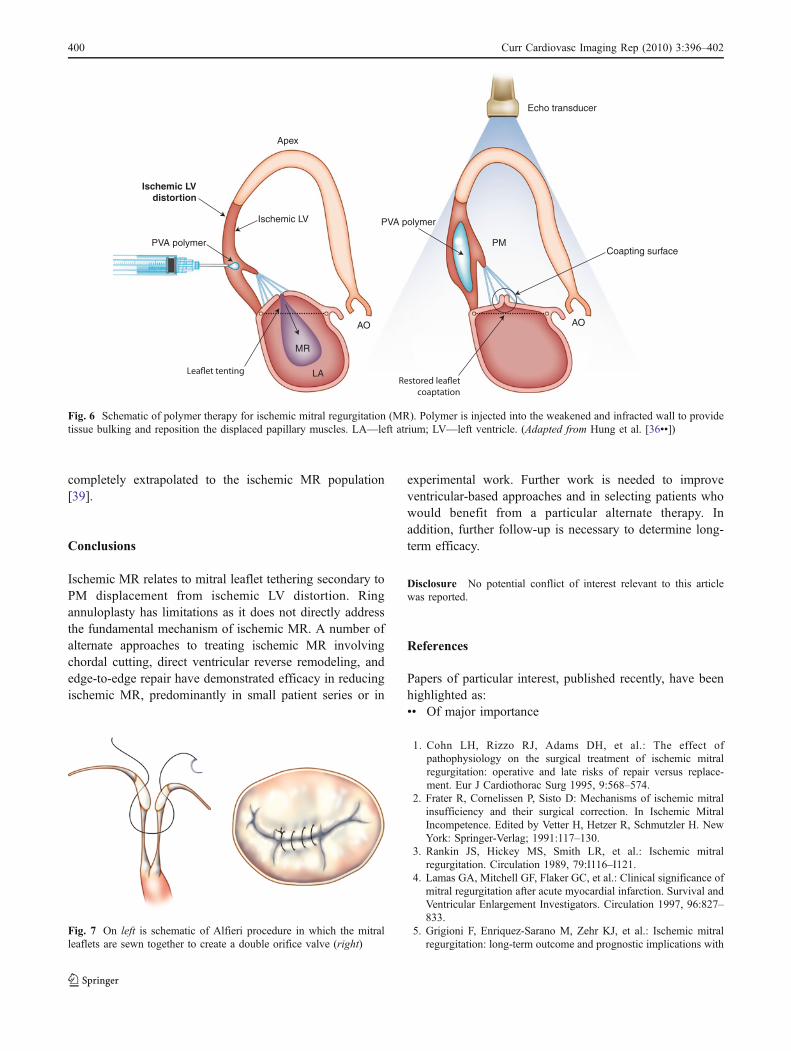
Although ventricular approaches more directly addressthe fundamental mechanism of ischemic MR, theyremain relatively invasive. Most recently, a polymer-based approach to ventricular remodeling has beenreported experimentally with efficacy in reducing MR(Fig. 6). A polymer-based approach has the potentialadvantage of being less invasive than the other surgicaltechniques. A biocompatible polymer, polyvinyl alcohol,was specially formulated to gel once injected into themyocardium [36••]. This polymer was injected into
Sur
viva
l, %
100
80
60
40
20
0
0 6 12 18Months postoperatively
24
4349
1031
18
Numbers at risk
Chordal-cuttingControlP = 0.8
Fig. 3 No difference in survival between the ring annuloplasty andchordal cutting group versus ring annuloplasty–only group. (Adaptedfrom Borger et al. [28••])
4+
2+
1+
0
4+
3+
2+
1+
0
4+
3+
2+
1+
0
4+
3+
2+
1+
0
Pre-op(3.0 ± 0.9)
Post-op(1.4 ± 1.3)
Pre-op(2.8 ± 0.8)
Post-op(0.9 ± 0.9)
Ring only Ring + chordal cutting
23
1
111
221
983
5331
211
1
478
3
74
3+
Fig. 4 Chordal cutting grouphad greater reduction inmitral regurgitation than ringannuloplasty–only group.(Adapted from Borger et al.[28••])
398 Curr Cardiovasc Imaging Rep (2010) 3:396–402
infarcted myocardium underlying the PM in an experi-mental ischemic MR model. This resulted in tissuebulking of the weakened myocardial wall and reverseremodeling with decrease in mitral leaflet tethering andreduction in ischemic MR.
Edge-to-Edge Repair
In addition to ventricular and chordal cutting approaches,edge-to-edge repair has been applied to ischemic MR.Edge-to-edge repair was developed by Ottavio Alfieri, inwhich the edges of the mitral leaflets are sewn together,creating a double orifice while reducing MR (Fig. 7) [37].The etiology of MR in these patients had degenerative
mitral valvular disease, although this surgical repair hasbeen applied to ischemic MR. More recently, edge-to-edgemitral valve repair has been applied percutaneously with aclip device (MitraClip; Evalve Inc.) [38]. EVEREST II wasa randomized trial of 279 patients with significant MR (3+to 4+) comparing the mitral clip device to surgical therapywith either mitral repair or replacement for MR [38]. Theresults were recently presented and showed that the novelMitraClip device may lead to fewer early adverse eventsthan traditional valve repair or replacement, with non-inferior efficacy out to 1 year. However, the surgical armdemonstrated greater efficacy in reducing MR [38]. It isimportant to note though that the majority of patients inEVEREST II had degenerative MR (73%), with a minorityhaving ischemic MR (27%), and results may not be
Table 1 Adjunctive or alternate approaches to standard mitral ring annuloplasty
Study Patients, n Technique Follow-up, mo
Kron et al. [40] 18 Surgical relocation of posteromedial papillary muscle 2
Hvass et al. [31] 10 Papillary muscle sling 3–24
Menicanti et al. [41] 46 Intraventricular papillary muscle imbrication 30
Rama et al. [33] 8 Papillary muscle approximation 7–14
Fig. 5 On left, Coapsys deviceconsists of two epicardial padsconnected by an internal chord.On right is schematic of place-ment of the Coapsys device.(From Mishra et al. [35], withpermission; Courtesy ofKiyotaka Fukamachi, MD)
Curr Cardiovasc Imaging Rep (2010) 3:396–402 399
completely extrapolated to the ischemic MR population[39].
Conclusions
Ischemic MR relates to mitral leaflet tethering secondary toPM displacement from ischemic LV distortion. Ringannuloplasty has limitations as it does not directly addressthe fundamental mechanism of ischemic MR. A number ofalternate approaches to treating ischemic MR involvingchordal cutting, direct ventricular reverse remodeling, andedge-to-edge repair have demonstrated efficacy in reducingischemic MR, predominantly in small patient series or in
experimental work. Further work is needed to improveventricular-based approaches and in selecting patients whowould benefit from a particular alternate therapy. Inaddition, further follow-up is necessary to determine long-term efficacy.
Disclosure No potential conflict of interest relevant to this articlewas reported.
References
Papers of particular interest, published recently, have beenhighlighted as:•• Of major importance
1. Cohn LH, Rizzo RJ, Adams DH, et al.: The effect ofpathophysiology on the surgical treatment of ischemic mitralregurgitation: operative and late risks of repair versus replace-ment. Eur J Cardiothorac Surg 1995, 9:568–574.
2. Frater R, Cornelissen P, Sisto D: Mechanisms of ischemic mitralinsufficiency and their surgical correction. In Ischemic MitralIncompetence. Edited by Vetter H, Hetzer R, Schmutzler H. NewYork: Springer-Verlag; 1991:117–130.
3. Rankin JS, Hickey MS, Smith LR, et al.: Ischemic mitralregurgitation. Circulation 1989, 79:I116–I121.
4. Lamas GA, Mitchell GF, Flaker GC, et al.: Clinical significance ofmitral regurgitation after acute myocardial infarction. Survival andVentricular Enlargement Investigators. Circulation 1997, 96:827–833.
5. Grigioni F, Enriquez-Sarano M, Zehr KJ, et al.: Ischemic mitralregurgitation: long-term outcome and prognostic implications with
Apex
Ischemic LV
Ischemic LVdistortion
PVA polymer
PVA polymer
MR
LA
AO AO
PMCoapting surface
Echo transducer
Fig. 6 Schematic of polymer therapy for ischemic mitral regurgitation (MR). Polymer is injected into the weakened and infracted wall to providetissue bulking and reposition the displaced papillary muscles. LA—left atrium; LV—left ventricle. (Adapted from Hung et al. [36••])
Fig. 7 On left is schematic of Alfieri procedure in which the mitralleaflets are sewn together to create a double orifice valve (right)
400 Curr Cardiovasc Imaging Rep (2010) 3:396–402

quantitative Doppler assessment. Circulation 2001, 103:1759–1764.
6. Stevenson LW, Bellil D, Grover-McKay M, et al.: Effects ofafterload reduction (diuretics and vasodilators) on left ventricularvolume and mitral regurgitation in severe congestive heart failuresecondary to ischemic or idiopathic dilated cardiomyopathy. Am JCardiol 1987, 60:654–658.
7. Junker A, Thayssen P, Nielsen B, Andersen PE: The hemody-namic and prognostic significance of echo-Doppler-proven mitralregurgitation in patients with dilated cardiomyopathy. Cardiology1993, 83:14–20.
8. Koelling TM, Aaronson KD, Cody RJ, et al.: Prognosticsignificance of mitral regurgitation and tricuspid regurgitation inpatients with left ventricular systolic dysfunction. Am Heart J2002, 144:524–529.
9. Godley RW, Wann LS, Rogers EW, et al.: Incomplete mitralleaflet closure in patients with papillary muscle dysfunction.Circulation 1981, 63:565–571.
10. Ogawa S, Hubbard FE, Mardelli TJ, Dreifus LS: Cross-sectionalechocardiographic spectrum of papillary muscle dysfunction. AmHeart J 1979, 97:312–321.
11. He S, Fontaine AA, Schwammenthal E, et al.: Integratedmechanism for functional mitral regurgitation: leaflet restrictionversus coapting force: in vitro studies. Circulation 1997, 96:1826–1834.
12. Otsuji Y, Handschumacher MD, Schwammenthal E, et al.:Insights from three-dimensional echocardiography into the mech-anism of functional mitral regurgitation: direct in vivo demon-stration of altered leaflet tethering geometry. Circulation 1997,96:1999–2008.
13. Llaneras MR, Nance ML, Streicher JT, et al.: Pathogenesis ofischemic mitral insufficiency. J Thorac Cardiovasc Surg 1993,105:439–442; discussion 442–443.
14. Llaneras MR, Nance ML, Streicher JT, et al.: Large animal modelof ischemic mitral regurgitation. Ann Thorac Surg 1994, 57:432–439.
15. Otsuji Y, Handschumacher MD, Liel-Cohen N, et al.: Mechanismof ischemic mitral regurgitation with segmental left ventriculardysfunction: three-dimensional echocardiographic studies in mod-els of acute and chronic progressive regurgitation. J Am CollCardiol 2001, 37:641–648.
16. Lai DT, Tibayan FA, Myrmel T, et al.: Mechanistic insights intoposterior mitral leaflet inter-scallop malcoaptation during acuteischemic mitral regurgitation. Circulation 2002, 106(Suppl 1):I40–I45.
17. Yiu SF, Enriquez-Sarano M, Tribouilloy C, et al.: Determinants ofthe degree of functional mitral regurgitation in patients withsystolic left ventricular dysfunction: A quantitative clinical study.Circulation 2000, 102:1400–1406.
18. Otsuji Y, Kumanohoso T, Yoshifuku S, et al.: Isolated annulardilation does not usually cause important functional mitralregurgitation: comparison between patients with lone atrialfibrillation and those with idiopathic or ischemic cardiomyopathy.J Am Coll Cardiol 2002, 39:1651–1656.
19. Aklog L, Flores KQ, Chen RH, et al.: Does coronary arterybypass grafting alone correct moderate ischemic mitral regurgita-tion? Circulation 2000, 102:II–492.
20. Hung J, Handschumacher MD, Rudski L, et al.: Persistence ofischemic mitral regurgitation despite annular ring reduction:mechanistic insights from 3D echocardiography. Circulation1999, 100:73.
21. Liel-Cohen N, Otsuji Y, Vlahakes GJ, et al.: Functional ischemicmitral regurgitation can persist despite ring annuloplasty: mech-anistic insights. Circulation 1997, 96:I–540.
22. Calafiore AM, Gallina S, Di Mauro M, et al.: Mitral valveprocedure in dilated cardiomyopathy: repair or replacement? AnnThorac Surg 2001, 71:1146–1152; discussion 1152–1153.
23. Tahta SA, Oury JH, Maxwell JM, et al.: Outcome after mitralvalve repair for functional ischemic mitral regurgitation. J HeartValve Dis 2002, 11:11–18; discussion 18–19.
24. McGee EC, Gillinov AM, Blackstone EH, et al.: Recurrent mitralregurgitation after annuloplasty for functional ischemic mitralregurgitation. J Thorac Cardiovasc Surg 2004, 128:916–924.
25. Hung J, Papakostas L, Tahta SA, et al.: Mechanism of recurrentischemic mitral regurgitation after annuloplasty: continued LVremodeling as a moving target. Circulation 2004, 110(Suppl 1):II85–II90.
26. Kuwahara E: Mechanism of recurrent/persistent ischemic/func-tional mitral regurgitation in the chronic phase after surgicalannuloplasty: importance of augmented posterior leaflet tethering.Circulation 2006, 114(1 Suppl):I529.
27. Messas E, Guerrero JL, Handschumacher MD, et al.: Chordalcutting: a new therapeutic approach for ischemic mitral regurgi-tation. Circulation 2001, 104:1958–1963.
28. •• Borger MA, Murphy PM, Alam A, et al.: Initial results ofthe chordal-cutting operation for ischemic mitral regurgitation.J Thorac Cardiovasc Surg 2007, 133:1483–1492. This studysummarizes the largest clinical experience with chordalcutting.
29. •• Liel-Cohen N, Guerrero JL, Otsuji Y, et al.: Design of a newsurgical approach for ventricular remodeling to relieve ischemicmitral regurgitation: insights from 3-dimensional echocardiogra-phy. Circulation 2000, 101:2756–2763. This was the initialexperimental study proposing a ventricular approach to treatingischemic MR.
30. Hung J, Guerrero JL, Handschumacher MD, et al.: Reverseventricular remodeling reduces ischemic mitral regurgitation:echo-guided device application in the beating heart. Circulation2002, 106:2594–2600.
31. Hvass U, Tapia M, Baron F, et al.: Papillary muscle sling: a newfunctional approach to mitral repair in patients with ischemic leftventricular dysfunction and functional mitral regurgitation. AnnThorac Surg 2003, 75:809–811.
32. Menicanti L, Di Donato M, Frigiola A, et al.: Ischemic mitralregurgitation: intraventricular papillary muscle imbrication with-out mitral ring during left ventricular restoration. J ThoracCardiovasc Surg 2002, 123:1041–1050.
33. Rama A, Praschker L, Barreda E, Gandjbakhch I: Papillarymuscle approximation for functional ischemic mitral regurgitation.Ann Thorac Surg 2007, 84:2130–2131.
34. Fukamachi K, Inoue M, Popović ZB, et al.: Off-pump mitral valverepair using the Coapsys device: a pilot study in a pacing-induced mitral regurgitation model. Ann Thorac Surg 2004,77:688–692.
35. Mishra YK, Mittal S, Jaguri P, Trehan N: Coapsys mitralannuloplasty for mitral regurgitation. One year results. AnnThorac Surg 2006, 81:42–46.
36. •• Hung J, Solis J, Guerrero JL, et al.: A novel approach forreducing ischemic mitral regurgitation by injection of a polymer toreverse remodel and reposition displaced papillary muscles.Circulation 2008, 118(14 Suppl):S263–S269. This study presentsexperimental evidence for a polymer-based approach to reverseremodel the ventricle.
37. Ottavio AJ, Marsano F, DeBonis M, et al.: The double-orificetechnique in mitral valve repair: A simple solution for complexproblems. J Thorac Cardiovasc Surg 2001, 122:674-681.
38. Feldman T, Wasserman HS, Hermann HC, et al.: Percutaneousmitral valve repair using the edge-to-edge technique: six month
Curr Cardiovasc Imaging Rep (2010) 3:396–402 401

results of the EVEREST Phase I Clinical Trial. J Am Coll Cardiol2005, 46:2134–2140.
39. Maud L, Gaarg P, Massaro J, et al.: The EVEREST IITrial: Design and rationale for a randomized study ofthe Evalve Mitraclip system compared with mitral valvesurgery for mitral regurgitation. Am Heart J 2010, 160:23–29.
40. Kron IL, Green GR, Cope JT: Surgical relocation of the posteriorpapillary muscle in chronic ischemic mitral regurgitation. AnnThorac Surg 2002, 74:600–601.
41. Menicanti L, Di Donato M, Frigiola A: Ischemic mitralregurgitation: intraventricular papillary muscle imbrication with-out mitral ring during left ventricular restoration. J ThoracCardiovasc Surg 2002, 123:1041–1050.
402 Curr Cardiovasc Imaging Rep (2010) 3:396–402