is antibiotic prophylaxis of any use in nephro-urology? · •non refluxing megaureter ... is...
TRANSCRIPT

Is antibiotic prophylaxis of any use in nephro-urology?
Giovanni Montini
Pediatric Nephrology and Dialysis Unit University of Milan
Italy

UTI_VUR

Bacteria and Humans: diverse behaviours!!
Bacteria
• Extremely numerous
• Memorise generational experiences within a few hours
• Capacity to transfer vast quantities of information in seconds
• Extraordinary ability to adapt under the selective pressure of antibiotics
• Outstanding collaboration
Humans
• Often few and isolated
• Endless discussions!!
• Difficulty in confronting and resolving issues
• Tendency to maintain the same diagnostic and therapeutic approaches
• Scarce collaboration for the most part







Causes of CKD (n=1197)
Hypodysplasia and VUR
24.7%
PUV
10.2%
Glomerulopathies
6.8% Other uropathies
12.2% Hypodysplasia
13.9%
Others
13.2%
Heredithary
nephropathies
15.4%
HUS
3.6%
ItalKid 2003

0
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4 5 6 7 8 9 10 11 12
months
Cumulative
%
2 3 3,5 4 5 6 6,5 7 8 8,5 9,5 10 11 12
years
males
females
Age at diagnosis of VUR
Age at diagnosis of vesicoureteral reflux (as cumulative percent) by sex in children with CRF (n:187)
ItalKid 2002

Gonzalez Celedon PN 2007 176 CAKUT children

6.7%
5.7%
8%
27.5%
42.8%
n = 516

The old concept
G. Montini, I. Hewitt and K Tullus

J De Bessa, J Urol 2015


May 4, 2014

Hoberman, NEJM 2014
71/126 toilet-
trained children
VUR GRADE II-III = 80%

RESULTS: primary endpoint
The treatment proved statistically significant, but of doubtful clinical value: requiring 16 or 22 patient years of antibiotics to prevent 1 UTI or 1 febrile UTI, respectively

RESULTS
p. NS
p < 0,001
The treatment group had in excess of 600 years of prophylaxis without a
demonstrable effect on scar formation but a much higher propensity to induce
bacterial resistance

Guidelines Antibiotic prophylaxis Others interventions
NICE
Not for routine use
Treat dysfunctional elimination syndromes and constipation
Drink an adequate amount of fluid Do not delay voiding
AAP
Not for routine use Not considered
ISPN
For reflux III-V Recurrent febrile UTI*
Not considered
* ≥3 febrile UTIs within 12 months


Reflux grades of all RCTs of antibiotic prophylaxis
VUR grade n
0 549
I-II 777
III 577
IV 172
V 5
Total 2080
Previous studies

THE PREDICT TRIAL
Antibiotic Prophylaxis and REnal Damage In Congenital abnormalities of the kidney and urinary Tract
Giovanni Montini Nefrologia e Dialisi Pediatrica Policlinico Sant’Orsola-Malpighi Bologna
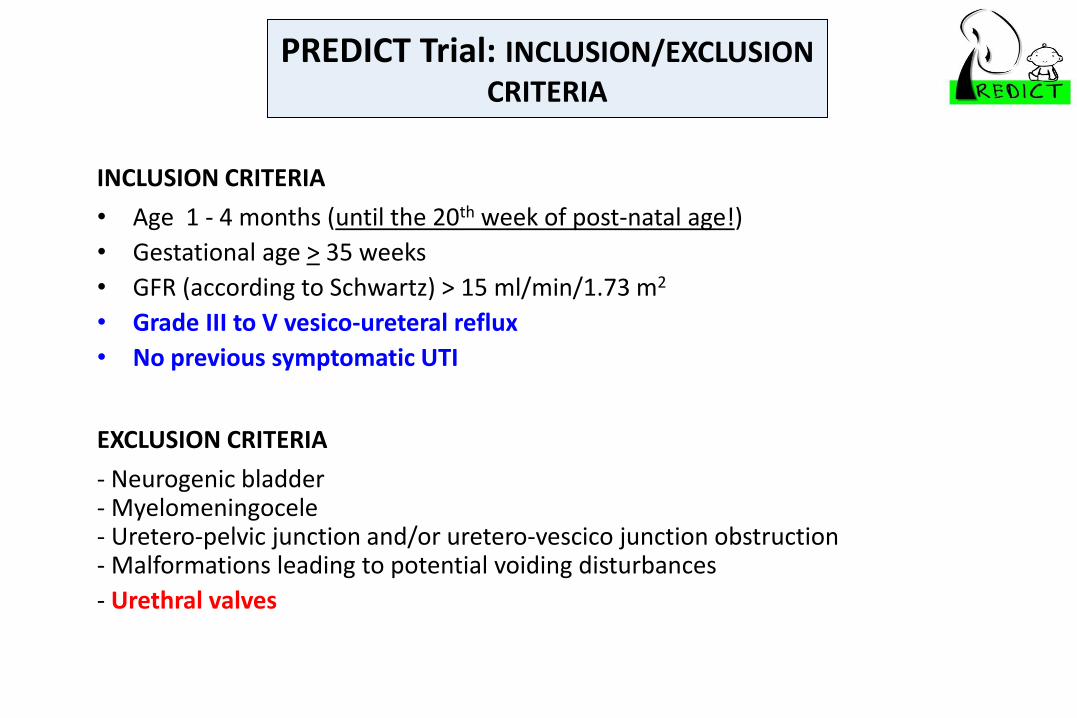
PREDICT Trial: INCLUSION/EXCLUSION CRITERIA
INCLUSION CRITERIA
• Age 1 - 4 months (until the 20th week of post-natal age!)
• Gestational age > 35 weeks
• GFR (according to Schwartz) > 15 ml/min/1.73 m2
• Grade III to V vesico-ureteral reflux
• No previous symptomatic UTI
EXCLUSION CRITERIA
- Neurogenic bladder - Myelomeningocele - Uretero-pelvic junction and/or uretero-vescico junction obstruction - Malformations leading to potential voiding disturbances
- Urethral valves

326 ( 436 )PATIENTS with VUR III-V
36 months FOLLOW-UP
STRATIFICATION Renal damage
CAKUT (prenatal or postnatal US screening)
PRE-RANDOMIZATION renal function, US, VCUG and DMSA
GROUP B Antibiotic
prophylaxis
GROUP A Follow-up
RANDOMIZATION
24 months (renal function, US + DMSA +/- VCUG+ BMI)
60 months (renal function, US + DMSA + VCUG+ BMI)

END-POINTS
Primary end point: first symptomatic urinary tract infection during the 24-
month observation period.
Secondary end point: febrile UTIs, number of new renal scars at the 2 years
follow-up DMSA scan, development of renal function, hypertension and/or
proteinuria, anatomical growth of the kidneys at 2 and 5 years follow-up,
evaluation of the natural course of renal function for hypo-dysplastic kidneys
during the first 5 years of life and evaluation of BMI at 2 and 5 years of age.

Nitrofurantoin (1.5-2 mg/kg/day) Co-amoxiclav (15 mg/kg/day) Cefixime (2 mg/kg/day) Trimetropim/sulfametoxazole (2.5 mg/kg/day)
ANTIBIOTIC PROPHYLAXIS
ONCE DAILY AT EVENING
According to the local antibiotic resistance pattern of E. coli
Each single patient may switch from one antibiotic to another.

Alberici I et al EUR J Ped 2015
Inpatients UC: resistance to E.coli

STATE OF THE ART: COUNTRIES
14 EUROPEAN COUNTRIES

Aims: - explore the modification in gut microbiota induced by antibiotic exposure in early infancy - Modifications in the pattern of resistance genes coded by gut microbiota (gut resistome profile).
GUT MICROBIOTA
collect and freeze a STOOL SAMPLE from every patient
8 time points:
(0, 4, 8, 12, 24, 36, 48, 60 months)

Current Understanding of Febrile Urinary Tract Infections and Renal Scarring.
Montini G et al. N Engl J Med 2011;365:239-250

Cystitis: antibiotic prophylaxis
- If frequently recurrent but > antibiotic resistance
- Short periods (1-3 months)
- Main aim is to remove symptoms secondary to
cystitis and then to evaluate bladder function
with no concomitant infection
- Cranberry ??

Results
Mean duration of follow-up was 47±30 months (12 to 78 months). The mean age of diagnosis in the cases that were not discovered prenatally was 10±19 months (1 week–77 months).
24%

During follow-up, a high rate of spontaneous regression
was observed.
At 7 years of follow-up, 70% of POM had
regressed spontaneously

What about prophylaxis? • In the first year of life, 30/44 received antibiotic prophylaxis.
–7 UTIs occurred during 199 patient months with prophylaxis
– 19 UTIs during 244 patient months without prophylaxis
– Prophylaxis appeared particularly effective in the first 6 months of life, where an 83% reduction of UTI rate was found.
• In the second year of life 38% received antibiotic prophylaxis
• In the third year of life 21% received antibiotic prophylaxis
reduction of UTI incidence on proph by 55% (0.94 vs. 0.42 UTIs per year, p<0.05)
0.46 UTIs/year without prophylaxis
0.14 UTIs/year without prophylaxis

NO Prophylaxis
• Hydronephrosis
• Neurogenic bladder and CIC
• Non dilating Refux

YES Prophylaxis
• Dilating Reflux
• Non Refluxing Megaureter
• Recurrent cystitis
• Urethral valves

Is antibiotic prophylaxis of any use in nephro-urology?
Giovanni Montini
Pediatric Nephrology and Dialysis Unit University of Milan
Italy