is advanced lung cancer becoming a chronic disease?
TRANSCRIPT

Is advanced lung cancer becoming a chronic disease?
James Chung-Man HO (何重文) M.D. FRCP Associate Professor, The University of Hong Kong
Honorary Consultant, Department of Medicine Specialist in Respiratory Medicine Queen Mary Hospital, Hong Kong
1

Disclosures • Received honoraria for lectures or
served as advisory board consultant for AstraZeneca, BMS, Roche, Boehringer Ingelheim, Eli Lilly, Pfizer, and MSD
• Received research funding from Roche and AstraZeneca

Outline of Lecture
• Lung cancer statistics • Advances in anticancer
options • Current management
algorithm of advanced non-small cell lung cancer
• Conclusions
3

4

Incidence rate: 2014
5 HK Cancer Registry
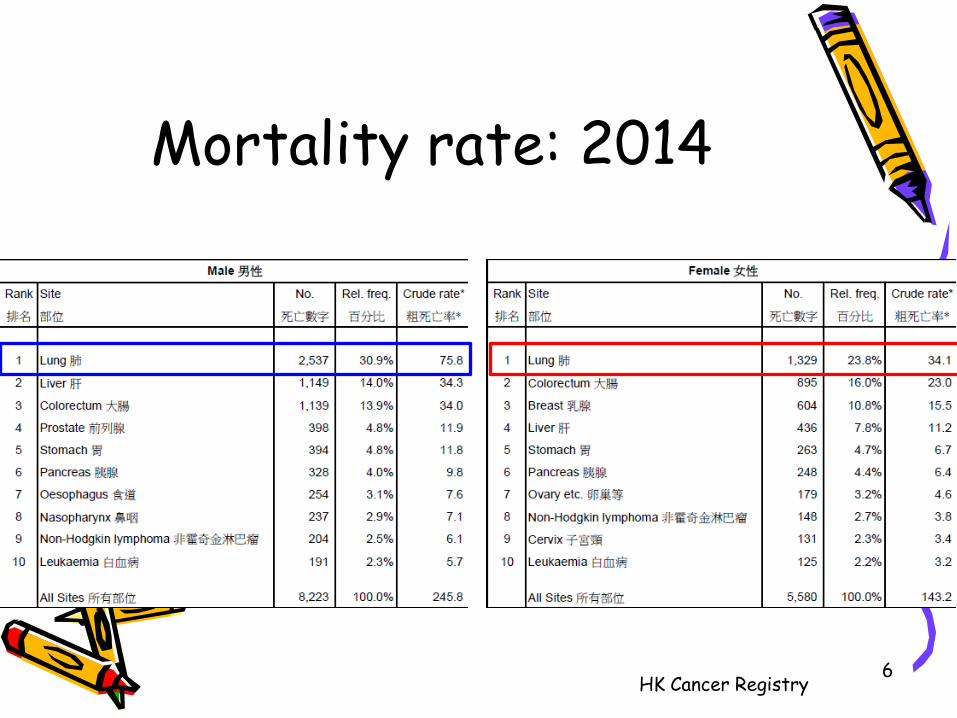
Mortality rate: 2014
6 HK Cancer Registry

Incidence of lung cancer in HK: Male (ASR)
7
↓ 18%
HK Cancer Registry

Mortality of lung cancer in HK: Male (ASR)
8
↓ 27%
HK Cancer Registry

Incidence of lung cancer in HK: Female (ASR)
9
↓ 9%
HK Cancer Registry
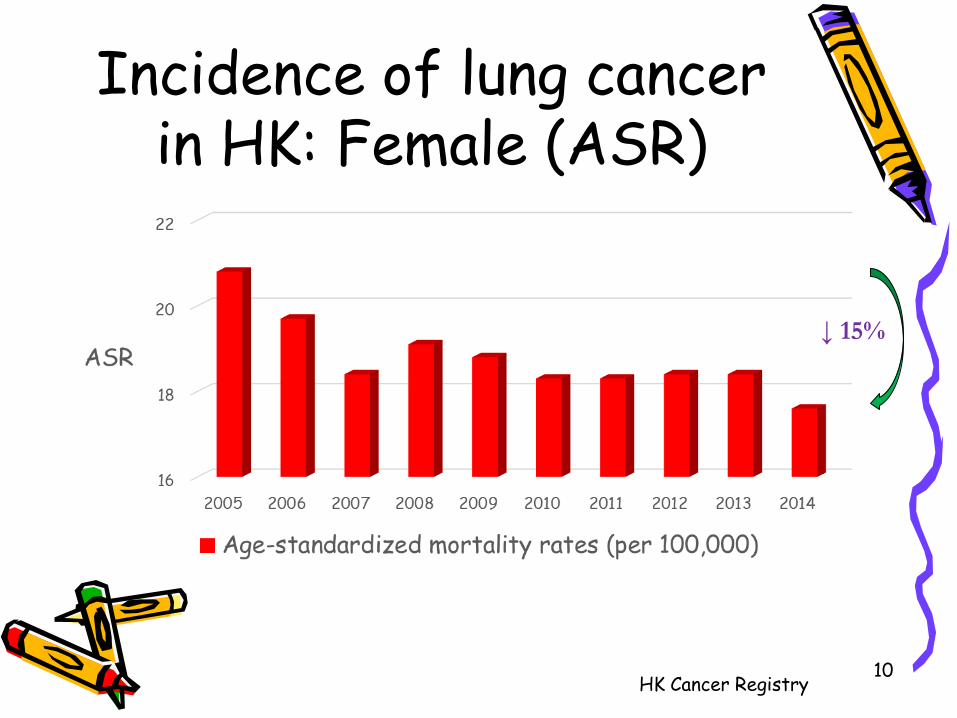
Incidence of lung cancer in HK: Female (ASR)
10
↓ 15%
HK Cancer Registry

Survival rates for lung cancer (stage III/IV): QMH Resp
11
N=44 N=54 N=66 N=79 N=71
61-83% adenocarcinoma Mean age 60-64 yrs
Unpublished data

12

PKC: clinical presentation • M/62 • Chronic cough • Chest Xray: L lung shadow in Aug
2013 • Workup confirmed lung
adenocarcinoma (EGFR L858R + T790M) 13

Driver mutations in NSCLC are heavily influenced by ethnicity
14
France1
China3
EGFR 40%
Unknown 29%
KRAS 7%
EML4-ALK 7%
MET 5%
BRAF 2%
PTEN 6%
Japan2
1. Barlesi F et al. Lancet 2016;387:1415–26; 2. Mitsudomi T. Jpn J Clin Oncol 2010;40:101–6; 3. Wu YL, Ann Oncol 2011;22 (suppl 9):Abstract 33.

Spectrum of EGFR Mutations
15
Tyrosine Kinase Domain Exons 18-24
Exon 18
EGFR Gene
Exon 19 Exon 20 Exon 21
G719C G719S G719A
5%
Del E746-A750 Del E746_S752>V Del E746_T751>A
Del E746_T751 Del L747_A750>P
Del L747_E749 Del L747_P753>Q Del L747_P753>S
Del L747_S752 Del L747_T751>P
Del L747_T751 Del S752_I759
& additional deletions
~45%
T790M D770_N771 (ins NPG) D770_N771 (ins SVQ)
D770_N771 (insG) S768I
~5%
L858R L861Q
~45%
Lynch et al., 2004 Paez et al., 2004 Sharma et al., 2007 Hirsch and Bunn, 2009
Sensitivity
Resistance

PFS = progression-free survival; OS = overall survival. .
EGFR TKIs vs Chemotherapy in EGFR M+ NSCLC (1L)
EGFR TKI Trial N EGFR
mutaiton ORR* (%)
PFS* (months)
OS* (months)
First Generation
TKI
Gefitinib
IPASS 1217 261 71 vs 47 P<0.001
9.5 vs 6.3 HR 0.48 (0.36-0.64)
21.6 vs 21.9 HR 1.00 (0.76-1.33)
NEJ002 224 224 74 vs 31 P<0.001
10.8 vs 5.4 HR 0.32 (0.24-0.44)
27.7 vs 26.6 HR 0.89 (0.63-1.24)
WJTOG 3405 172 172 62 vs 32
P<0.0001 9.2 vs 6.3
HR 0.0.5 (0.34-0.71) 36 vs 39
HR 1.19 (0.77-1.83)
Erlotinib
EURTAC 173 173 58 vs 15 P-value NR
9.7 vs 5.2 HR 0.37 (0.25-0.54)
22.9 vs 19.6 HR 0.92 (0.63-1.35)
OPTIMAL 165 154 83 vs 36 P<0.0001
13.1 vs 4.6 HR 0.16 (0.10-0.26)
22.8 vs 27.2 HR 1.19 (0.83-1.71)
ENSURE 217 216 63 vs 34 P=0.0001
11.0 vs 5.6 HR 0.42 (0.27-0.66)
26.3 vs 25.5 HR 0.91 (0.61-1.31)
Second Generation
TKI Afatinib
LUX-Lung 3 345 308 69 vs 44 P=0.001
13.6 vs 6.9 HR 0.41 (0.31-0.56)
31.6 vs 28.2 HR 0.78 (0.58-1.06)
LUX-Lung 6 364 324 74 vs 31 P<0.0001
13.7 vs 5.6 HR 0.26 (0.19-0.36)
23.6 vs 23.5 HR 0.83 (0.62-1.09)
*Results described refer to common mutations only
Mok TS et al. N Engl J Med. 2009;361:947-57; Fukuoka M et al. J Clin Oncol. 2011;29:2866-74; Maemondo M et al. N Engl J Med. 2010;362:2380-98; Mitsudomi T et al. Lancet Oncol. 2010;11:121-8; Yoshioka H et al. J Clin Oncol. 2014;32(suppl):abstract 8117; Rosell R et al. Lancet Oncol. 2012;13:239-46; Leon L et al. ESMO 2014. Abstract 1273P; Zhou CC et al. Lancet Oncol. 2011;12:735-42; Zhou CC et al. J Clin Oncol. 2012;30(suppl):abstract 7520; Wu YL et al. Ann Oncol. 2015;26:1883-9; Sequist LV et al. J Clin Oncol. 2013;31:3327-34; Wu YL et al. Lancet Oncol. 2014;15:213-22; Yang JC et al. Lancet Oncol 2015;16:141-51.

PFS in EGFR mutation positive and negative lung adenoca: IPASS
Cox analysis with covariates; HR <1 implies a lower risk of progression on gefitinib; ITT population
Mok TS et al. NEJM 2009;361:947-57
HR (95% CI) = 0.48 (0.36, 0.64) p<0.0001
No. events gefitinib, 97 (73.5%) No. events C/P, 111 (86.0%) Median PFS G, 9.5 months Median PFS C/P, 6.3 months
Gefitinib (n=132) Carboplatin/paclitaxel (n=129)
EGFR mutation positive
132 71 31 11 3 0 129 37 7 2 1 0
108 103
0 4 8 12 16 20 24
Gefitinib C/P
0.0
0.2
0.4
0.6
0.8
1.0
Prob
abili
ty o
f pr
ogre
ssio
n-fr
ee
surv
ival
Patients at risk : Months
EGFR mutation negative
HR (95% CI) = 2.85 (2.05, 3.98) p<0.0001
No. events gefitinib , 88 (96.7%) No. events C/P, 70 (82.4%) Median PFS G, 1.5 months
Median PFS C/P, 5.5 months
91 4 2 1 0 0 85 14 1 0 0 0
21 58
0 4 8 12 16 20 24 0.0
0.2
0.4
0.6
0.8
1.0
Prob
abili
ty o
f pr
ogre
ssio
n-fr
ee
surv
ival
Gefitinib (n=91) Carboplatin/paclitaxel (n=85)
Months

PKC: clinical presentation • LU lobectomy in private in Aug 2013 • Adjuvant chemotherapy x 4 cycles in
Aug-Nov 2013 • PET-CT in July 2014: disease
recurrence with L pleural nodules/effusion
• Started Tarceva in Oct-Dec 2014 no response
18

PKC: clinical presentation • Referred to QMH for clinical trial
option • VATS pleural biopsy in Jan 2015:
confirmed adenocarcinoma (EGFR L858R + T790M)
• Considered for AURA 3 trial
19
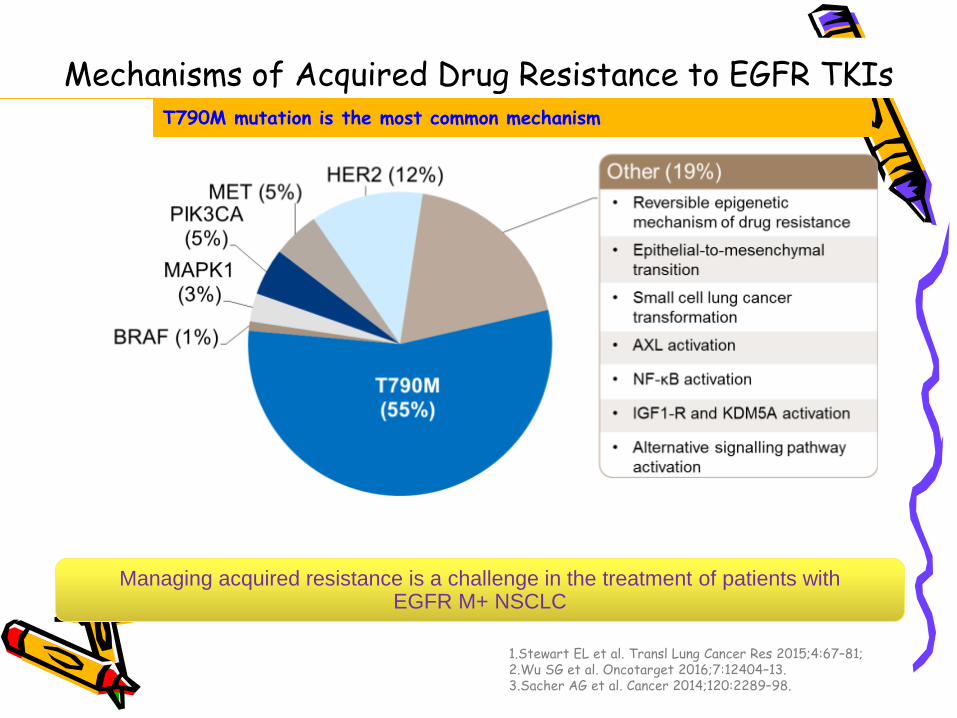
Mechanisms of Acquired Drug Resistance to EGFR TKIs
T790M mutation is the most common mechanism
Managing acquired resistance is a challenge in the treatment of patients with EGFR M+ NSCLC
1.Stewart EL et al. Transl Lung Cancer Res 2015;4:67–81; 2.Wu SG et al. Oncotarget 2016;7:12404–13. 3.Sacher AG et al. Cancer 2014;120:2289–98.

Three Generations of EGFR TKIs: Potency and Specificity
Gefitinib
EGFRm
T790M
Wt
Afatinib Osimertinib
EGFRm
T790M
T790M
Wt
Wt
EGFRm 1x
10x
100x
Rel
ativ
e IC
50
Li D, et al. Oncogene. 2008;27:4702-4711. Ranson M, et al. WCLC 2013. Abstract MO21.12. Moyer JD, et al. Cancer Res. 1997;57:4838-4848. Kancha RK, et al. Clin Cancer Res. 2009;15:460-467.
T790M
EGFRm
Wt
Erlotinib

AURA (Ph I/II) & AURA 2 (Ph II): Osimertinib (80 mg QD) for EGFR T790M Resistance
Efficacy Parameter AURA (Ph II extension,
T790M+) (N=201)
AURA 2 (Ph II, T790M+) (N=210)
Overall (N=411)
Objective Response Rate* (95% CI)
57% (50, 64)
61% (54, 68)
59% (54, 64)
Complete Response 0 1% 0.5%
Partial Response 57% 60% 59%
Duration of Response
• 96% of patients in both trials had ongoing responses at the time of primary analysis
• mDOR had not been reached with duration of ongoing responses ranging from 1.1 to 5.6 months
*Objective response rate determined by RECIST v1.1 as assessed by Independent review
US approval of Osimertinib for EGFR T790M+ NSCLC on 13 Nov 2015
Janne et al. N EnglJ Med. 2015;372:1689.

PKC: clinical presentation • Eligible for AURA 3 trial • Received AZD9291 (osimertinib)
since Feb 2015 • Very well tolerated • CT reassessment: partial response • Last follow-up on 13 Apr 2017
23

PKC: CT thorax Jan 2015 Feb 2016
24

PKC: CT thorax Jan 2015 Feb 2016
25

AURA 3: PFS
26 Mok TS et al. NEJM 2017;376:629-40

27
Mok TS et al. NEJM 2017;376:629-40

WYC: clinical presentation
28
Incidental finding of left lung shadow
on chest X-ray in 2008 during routine body
check
PET-CT: primary tumour in left
hilar node, two satellite
nodules in LUL, mediastinal
lymph nodes
Mediastinoscopy in private hospital:
adenocarcinoma EGFR WT, T4N2
Referred to hospital authority
oncology unit
• Male, 36 years-old • Ex-light smoker • Performance score: 0

WYC: clinical presentation
29
Advised chemoradiotherapy
treatment
July 2008
CT of thorax
Multiple tumors: ~8 cm mass in LUL; bilateral multiple
lung nodules, multiple mediastinal and
supraclavicular nodes
April 2010
Patient returned: cough, mild shortness
of breath
Patient refused
treatment
6 cycles of chemotherapy with
carboplatin/paclitaxel + bevacizumab (SOC)
April 2010
Stable disease
October 2010
Progressive disease: stable extracranial disease but new
metastases in the brain

WYC: clinical presentation
30
Nov 2010 Dec 2010
WBRT (concurrent with
pemetrexed)
5 cycles of pemetrexed
(every three weeks)
PET-CT
PD + new bone metastases
(L4 vertebra and right ilium)
March 2011
Erlotinib
Progressive disease
Assessed for eligibility to
PROFILE 1005: ALK positive
tumour
June 2011
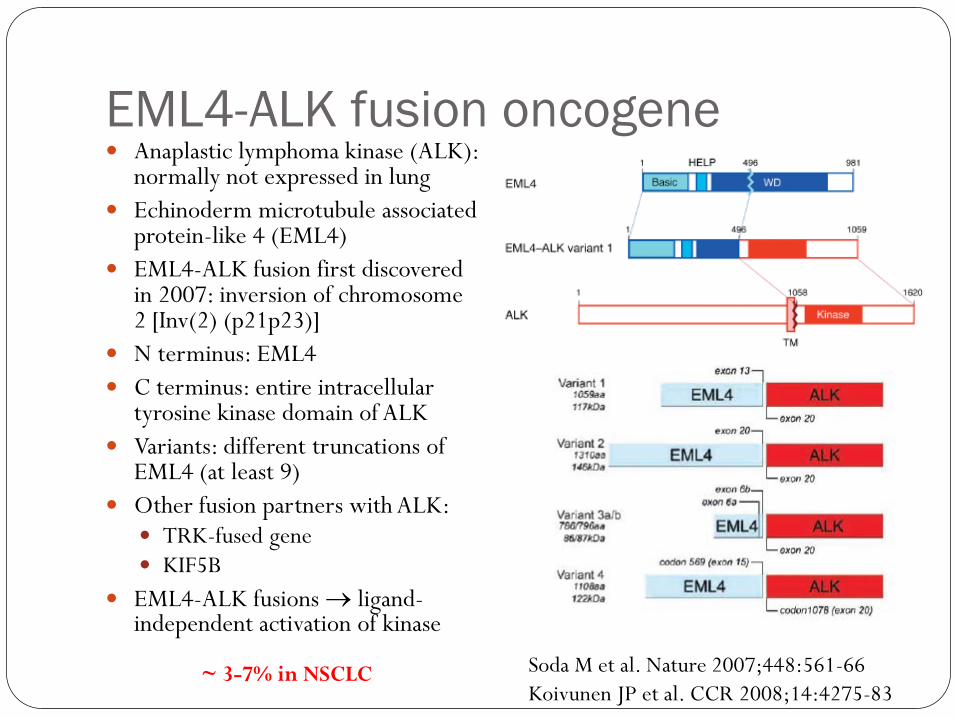
EML4-ALK fusion oncogene Anaplastic lymphoma kinase (ALK):
normally not expressed in lung Echinoderm microtubule associated
protein-like 4 (EML4) EML4-ALK fusion first discovered
in 2007: inversion of chromosome 2 [Inv(2) (p21p23)]
N terminus: EML4 C terminus: entire intracellular
tyrosine kinase domain of ALK Variants: different truncations of
EML4 (at least 9) Other fusion partners with ALK:
TRK-fused gene KIF5B
EML4-ALK fusions → ligand-independent activation of kinase
Soda M et al. Nature 2007;448:561-66 Koivunen JP et al. CCR 2008;14:4275-83
~ 3-7% in NSCLC

Predictive biomarkers for ALK
FISH IHC
Typical population with ALK fusion Neversmokers or ex-light smokers Adenocarcinoma Young age of onset Solid pattern with abundant signet ring cells EGFR WT
IPASS population
IPASS population with EGFR WT, around 33% will have EML4-ALK
IPASS population in Asians ~ 60% EGFR activating mutations
Mok TS et al. NEJM 2009;361:947-57

PROFILE 1005: study design
34
• Phase II, single-arm, multicenter study; ~1,100 patients1,2
1. Riely G, et al. Abstract 166. Presented at IASLC Chicago Multidisciplinary Symposium in Thoracic Oncology 2012, Chicago,
Illinois, 6–8 September, 2012; 2. Kim D, et al. Ann Oncol 2012;23(Suppl 9):ix402:Abstract 1230PD.
Crizotinib 250 mg BID PO; continuous daily dosing
Key eligibility criteria: ●ALK-positive NSCLC by central laboratory
– Local test allowed on case-by-case basis per protocol amendment (January 2011)
●ECOG PS: 0–3
●≥1 prior line of chemotherapy
●Stable/controlled brain metastases allowed
Primary endpoints: ● ORR ● Safety/tolerability Secondary endpoints include: ● OS ● PFS ● Duration of response ● Time to response ● PRO/HRQoL
Treatment

PROFILE 1014: study design
35 aStratification factors: ECOG PS (0/1 vs 2), Asian vs non-Asian race, and
brain metastases (present vs absent); cAssessed by IRR Solomon BJ, et al. N Engl J Med 2014;371:2167−77.
Key entry criteria ● ALK-positive by
central FISH testing
● Locally advanced, recurrent, or metastatic non-squamous NSCLC
● No prior systemic treatment for advanced disease
● ECOG PS 0−2 ● Measurable disease ● Stable treated brain
metastases allowed
N=343
Crizotinib 250 mg BID PO,
continuous dosing (N=172)
Pemetrexed 500 mg/m2
+ cisplatin 75 mg/m2 or carboplatin AUC
5–6 q3w for ≤6 cycles (N=171)
Endpoints
● Primary – PFS (RECIST v1.1,
by IRR)
● Secondary – ORR – OS – Safety – PROs
(EORTC QLQ-C30, QLQ-LC13, EQ-5D)
R A N D O M I Z E a
Accrual period: January 2011 − July 2013
Crossover to crizotinib permitted after progression

PROFILE 1014: primary endpoint – PFS by IRR (ITT population)
36 Solomon BJ, et al. N Engl J Med 2014;371:2167−77. a2-sided stratified log-rank test
Crizotinib (n=172)
Chemotherapy (n=171)
Events, n (%) 100 (58) 137 (80)
Median, mo 10.9 7.0
HR (95% CI) 0.45 (0.35−0.60)
pa <0.001
Crizotinib Chemotherapy
No. at risk: Crizotinib 172 120 65 38 19 7 1 0 Chemotherapy 171 105 36 12 2 1 0 0
Time (months) 0 35
PFS
prob
abilit
y (%
)
100
80
60
40
20
0 20 15 10 5 25 30

WYC: clinical course
37
July 2011
Enrolled in PROFILE 1005
September 2011
Crizotinib
Partial response, stable in the brain
Scan at baseline Scan after 2 months

WYC: clinical course
38
September 2011
Crizotinib
Partial response, stable in the brain
Scan after 2 months
October 2012
Small new right high parietal brain lesion (2.3 x 3.2 x 2.5 mm)
detected

WYC: clinical course
39
September 2011
Crizotinib
Partial response
April 2013
Progressive thoracic disease
Stable brain disease
October 2012
Continue crizotinib
New brain metastasis

Acquired Resistance in ALK+ NSCLC • ALK-rearranged (ALK+) NSCLC is sensitive to
crizotinib1–3
• Most patients develop resistance to crizotinib4,5
– Usually within 1–2 years – CNS relapses are common6
• Mechanisms of resistance are diverse4,5
– ALK resistance mutations – Alternative signalling pathways
amp, amplification; mut, mutation. 1. Camidge DR, et al. Lancet Oncol. 2012;13:1011-1019; 2. Kim D-W, et al. ESMO; 2012. Abstract 1230PD; 3. Shaw AT, et al. ESMO; 2012. Abstract LBA1_PR; 4. Katayama R, et al. Sci Transl Med. 2012;4:120ra17; 5. Doebele RC, et al. Clin Cancer Res. 2012;18:1472-1482; 6. Takeda M, et al. J Thorac Oncol. 2013;8:654-657.

2nd generation TKI ceritinib: ASCEND-5
41
• Phase III, randomized (1:1), controlled, multicenter study; 231 patients
Scagliotti, G. Abstract LBA42. Presented at ESMO 2016 Congress in Copenhagen, Denmark, 9 October, 2016.
Kim, DW. Lancet Oncol. 2016;17:452-63
Ceritinib (750 mg/d) Key eligibility criteria: ●ALK-positive NSCLC by central laboratory
●≥1 prior line of chemotherapy
●Previous treatment with an ALK inhibitor
●ECOG PS: 0–3
●Stable/controlled brain metastases allowed
Primary endpoint (PFS) results: Median 5.4 vs 1.6 months, HR=0.49, (P<0.001)
Chemotherapy (pemetrexed [500 mg/m2] or
docetaxel [75 mg/m2])
Previous exploratory data from the Phase 1 ASCEND-1 trial also reported improved intracranial responses to ceritinib in patients with brain metastases

No. of patients at risk Ceritinib Chemo
ASCEND 5: PFS
42
115 116
87 45
68 26
40 12
31 9
18 6
12 2
9 2
4 2
3 0
2 0
1 0
0 0
0
20
40
60
80
100
Censoring times
0 2 4 6 8 10 12 14 16 18 20 22 24
Prob
abili
ty o
f PFS
(%)
Time (Months)
Ceritinib 750 mg (N=115)
Chemotherapy (N=116)
Events, n (%) 83 (72.2) 89 (76.7)
Median (95% CI), months 5.4 (4.1, 6.9) 1.6 (1.4, 2.8)
Hazard ratio (95% CI) 0.49 (0.36, 0.67)
Log-rank p-value < 0.001
Scagliotti G et al. ESMO 2016

WYC: clinical course
43
April 2013
Progressive thoracic disease by CT scan
May 2013
Ceritinib through the CLDK378A2201 trial
Stable disease; transient interruption
due to hepatitis

Stable response to ceritinib
44
May 2013 July 2013
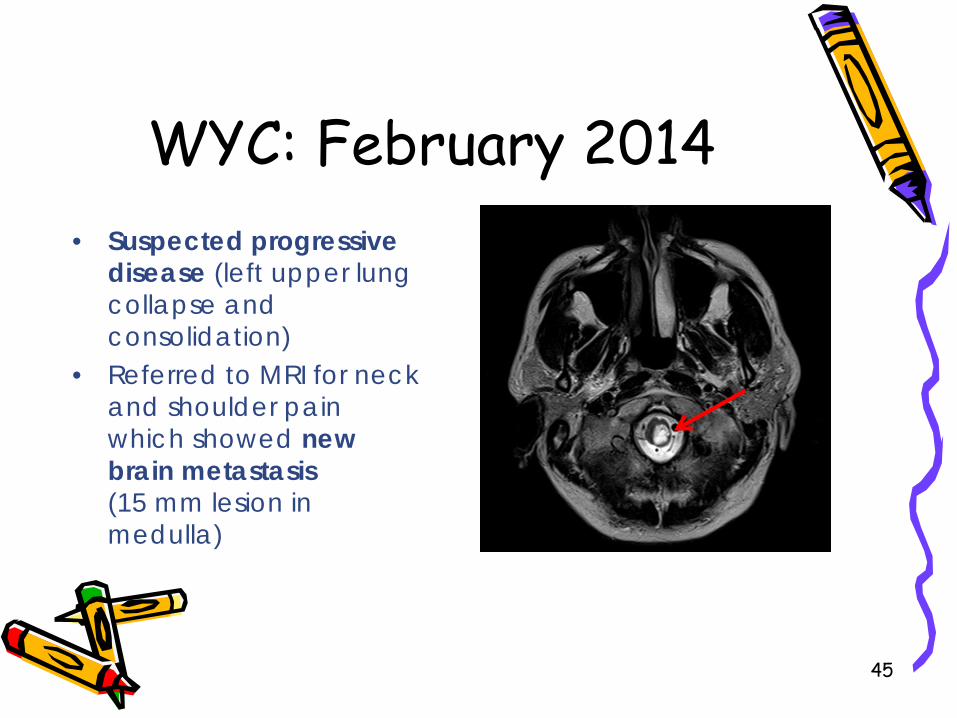
WYC: February 2014
45
• Suspected progressive disease (left upper lung collapse and consolidation)
• Referred to MRI for neck and shoulder pain which showed new brain metastasis (15 mm lesion in medulla)

WYC: clinical course
46
Stereotactic radiotherapy for brainstem lesion
February 2014
Continue treatment with ceritinib post-progression
April 2014
Progressive thoracic disease and new brain
metastasis
Stable disease in thorax and CNS

Medullary lesion post-stereotactic radiotherapy
47
3 months 11 months
July 2014 March 2015

WYC: clinical course
48
February 2014
Continue treatment with ceritinib post-progression
April 2014
Stereotactic radiotherapy for brainstem lesion
Progressive thoracic disease and new brain
metastasis
Stable disease in thorax and CNS
March 2015
Ceritinib withheld due to increased ALT
for 2 weeks
PD in CNS

Alectinib • Alectinib has demonstrated high potency and
selectivity, and promising antitumor effects in NSCLC
• Preclinical studies: active against several mutant forms of ALK that confer resistance to crizotinib, including the gatekeeper mutation L1196M – Phase III ALUR results suggest longer PFS with
alectinib compared with chemotherapy in pretreated patients
– Ongoing Phase III study (ALEX)
49 Wong KM et al. Drugs Today (Barc) 2015;51:161–70.
Wolf, J. Ann Oncol 2016;27(suppl_6): 1290TiP http://www.roche.com/media/store/releases/med-cor-2017-04-03.htm

J-ALEX: Phase III study design
50 Kim YH, et al. Presented at the IASLC 17th World Conference on Lung Cancer.
December 4–7, Vienna, Austria, 2016. Presentation No. 5597. Nokihara T, et al. Presented at ASCO Annual Meeting. June 3–7, Chicago, IL, 2016.
Stratification factors:
R 1:1
Key Entry Criteria • Stage IIIB/IV or recurrent
ALK-positive NSCLC • ALK centralized testing (IHC and FISH or RT-PCR) • ECOG PS 0-2 • ≥1 measurable lesion
assessed by investigator • Treated/asymptomatic brain
metastases allowed • ≤1 prior chemotherapy
Alectinib 300 mg BID PO, 28-day cycle
(N=100)
Crizotinib 250 mg BID PO, 28-day cycle
(N=100)
Endpoints •Primary - PFS assessed by IRF*
•Secondary - OS - ORR - PK - HRQoL - Time to CNS progression - Safety
Clinical stage (IIIB/IV vs recurrent) Prior chemotherapy (0 vs 1) ECOG PS (0/1 vs 2)
Objective: To demonstrate superiority in PFS with alectinib compared with crizotinib in previously untreated patients or patients received one line of chemotherapy, based on
independent review
● Randomized controlled multi-center open-label Phase III study comparing the efficacy and safety of alectinib versus crizotinib (44 sites)

J-ALEX: PFS by CNS disease
51 Kim YH, et al. Presented at the IASLC 17th World Conference on Lung Cancer. December 4–7, Vienna, Austria, 2016. Presentation No. 5597.
Without CNS disease at baseline With CNS disease at baseline
100
80
60
40
20
0
PFS
rate
(%)
0 6 12 18 27 24 21 3 9 15 1
Alectinib Crizotinib
Time (months) No. of patients at risk
40 28
22 12
63 48
28 16
5 3
80 63
89 75
89 74
100
80
60
40
20
0
PFS
rate
(%)
0 6 12 18 27 24 21 3 9 15 1
Alectinib Crizotinib
Time (months) No. of patients at risk
9 12
5 2
13 17
8 5
4 1
13 23
14 29
14 28
1
Alectinib (N=89)
Crizotinib (N=75)
Event 24 (27.0%) 42 (56.0%) Median [95% CI] 20.3 [17.5 ; -] 10.0 [8.2 ; 13.9] P-Value 0.0001 HR [95% CI]a 0.37 [0.22 ; 0.62]
Alectinib (N=14) Crizotinib (N=29)
Event 1 (7.1%) 16 (55.2%) Median [95% CI] - [- ; -] 10.2 [6.5 ; 14.2] P-Value 0.0062 HR [95% CI]a 0.09 [0.01 ; 0.74]
Alectinib Crizotinib
Alectinib Crizotinib
Alectinib demonstrated greater efficacy in patients with CNS disease versus crizotinib
However, it should be noted that there was an imbalance in patients with brain metastases at baseline (crizotinib = 29 vs alectinib = 14) as
this was not a stratification factor for randomization

WYC: clinical course
52
March 2015
Decrease in multiple brain lesions including
brainstem
Continued on ceritinib
May 2015
Applied for compassionate use of
alectinib
Continued on ceritinib
December 2015
PD in medullary lesion
Initiated alectinib

Response to alectinib in CNS
53
June 2016 December 2015
WYC experienced occasional, transient myosistis on alectinib

WYC: Summary of therapy progress
54
Erlotinib
Aug 2010
Ceritinib
May 2013
Alectinib Chemotherapy
Mar–June 2011
ALK mutation identified
Dec 2015
Stereotactic radiotherapy
Progression
Partial response
Stable disease
Progression
Crizotinib
July 2011
WBRT
Progression Progression
Progressive CNS disease
Patient passed away:
19 Apr 2017
~ 6 years

NCCN guideline version 5.2017 NSCLC: 1L
Metastatic disease
Adenoca Large cell
NSCLC NOS
Squamous cell ca
Molecular testing
(EGFR, ALK, ROS1);
EGFR +
ALK +
ROS1 +
PD-L1 + EGFR/ALK/ROS1 –ve or unknown
PD-L1/ EGFR/ALK/ROS1 –ve or unknown
Consider molecular
testing (EGFR, ALK,
ROS1) esp. in nonsmokers,
small bx, mixed
histologies; 55

Emerging 1L treatment algorithm
Advanced lung adenoca/selected squamous
cell ca
Specific TKIs
EGFR/ALK/ROS1 driven
EGFR/ALK/ROS1 WT
PD-L1 ≥ 50%
Pembro
PD-L1 1-49%
Chemotherapy options 1.pem/platinum (nonsquamous) 2.Bev + chemo
(nonsquamous) 3.Gem or taxane
/platinum (squamous) Based on KEYNOTE 024 data and NCCN guideline
EGFR/ALK/ROS1 / PD-L1 –ve or
unknown

∗ Non-small cell lung cancer is a heterogeneous disease with diverse molecular profile
∗ Early detection of actionable targets (e.g. EGFR mutations, ALK or ROS1 rearrangement) allows specific targeted therapies
∗ Emerging anticancer therapies (esp. targeted therapy and immunotherapy) significantly improve the general outlook for advanced lung cancer
∗ Advanced lung cancer is now becoming a chronic disease
Conclusions

∗ Respiratory team (medical and nursing): QMH ∗ Co-investigators of clinical trials ∗ Research nurse (Christina Yan) ∗ Research coordinators (Vivian Li, Joy Zhang) ∗ All patients and their families taking part in clinical
trials
Acknowledgements