iroko pain management digest - cloud object … master v53...pain management digest editorial board...
TRANSCRIPT

A
IROKO
PAINMANAGEMENTDIGEST2013

PAIN MANAGEMENT DIGEST
Editorial Board
Christina Barrington, PharmDDirectorHumana, Great Lakes RegionChicago, IL
Christopher V. Goff, JD, MAChief Executive Officer and General CounselEmployers HealthCanton, OH
Jeff Livovich, MDMedical DirectorNational Policy and OperationsAetnaScottsdale, AZ
Bill McCarberg, MDKaiser Permanente, San Diego (retired)Adjunct Assistant Clinical Professor, University of California San DiegoNeighborhood Healthcare, Federally Qualified Healthcare ClinicSan Diego, CA
Scott R. Taylor, BS Pharm, RPh, MBAExecutive Director, Office of Industry RelationsGeisinger Health SystemDanville, PA
®
This 2013 Iroko Pain Management Digest is designed to serve as an educational resource for managed care organizations that seek a broader understanding of the issues surrounding pain management. The content of this report was prepared by ReCon Marketing Solutions, LLC, with the guidance of an editorial board, and it is based on independently conducted primary and secondary research. Iroko provided financial support for this report and the editorial board.
The 2013 Iroko Pain Management Digest
Produced by ReCon Marketing Solutions, Medford, NJ
www.ReConMarketingSolutions.com
Managing Editor and Research Director - Marsha Fisher
Editorial and Research - Meredith Scheiner
Project and Market Research Director - Betsy Dennison
Creative Director - Lin Kossak
ReCon Management
Sal Cofoni, [email protected]
Dean Reid, [email protected]

1
Table of ContentsIntroduction Managed Care Issues and Answers in Pain Management.......................................................................2
Survey Methodology and Research .........................................................................................................5
Chapter 1 Medical and Pharmacy Director Perspectives on Pain Management.....................................................6
Employer Survey: Interim Results .....................................................................................................11
Chapter 2 Practices in Pain Treatment and Management: A Physician Survey ....................................................12
Chapter 3 Pain Management: The Patient Experience .........................................................................................17
Chapter 4 Issues and Answers for MCOs ...............................................................................................................22
Pennsylvania: Building a Foundation for Successful Treatment of Low Back Pain .............................22
New England: A Pharmacy Director-Driven Program to Address Opioid Risk .................................24
Ohio: Building State Policies and Procedures Through a Pain Management Task Force ....................26
Chapter 5Treating Pain: Mixed Models and Modalities .......................................................................................27
New Treatments, New Goals .............................................................................................................27
Current Multimodal Therapeutic Choices ........................................................................................28
Multidisciplinary and Interdisciplinary Care: A Focus on Outcomes ................................................29
The Rehabilitation Institute of Chicago Center for Pain Management: Chronic Pain Program .........29
Establishing Coverage for Multidisciplinary Pain Programs ...............................................................30
Chapter 6 Building on Successful Pain Management Programs ...........................................................................31
University of Washington Center for Pain Relief: A Large Multidisciplinary Model ..........................31
Washington: Addressing Opioid Risk ...............................................................................................32
Missouri: A Medical Home Model Provides Comprehensive Pain Management for a Large Medicaid and Uninsured Population ....................................................................................33
California and Oregon: Evaluating Regional Pain Management Programs ........................................34
Improving Clinical Trial Design and Interpretation ..........................................................................35
Appendix ................................................................................................................................................37
References ..............................................................................................................................................40

2
PAIN MANAGEMENT DIGEST
PreludeIn the spring of 2009, a national managed care workgroup1 gathered with an aim of building consensus among medical and pharmacy directors as to how their plans could achieve the following goals:
• Alleviate barriers to effective management of pain
• Create “best practices” in pain management within each participant’s own organization
• Shift organizational perspectives to regard chronic pain as a chronic disease
This workgroup agreed upon the barriers to achieving these goals, and suggested paths to follow in addressing the core issues:
Barriers
• Lack of commonly accepted guidelines
• Tenacity and complexity of chronic pain
• Difficulty determining whether treatment is working
• Fragmentation of the healthcare system across pain treatment providers
Paths to improvement
• Managed care plans need to partner with physicians to improve treatment and management of pain
• Patients with chronic pain need multidisciplinary treatment and multimodal medication plans
The 2009 group had identified exactly those issues that remain troubling to medical and pharmacy directors today.
2013 — Improving Pain ManagementPain management discussions have moved into the national spotlight, largely through the attention of national reports such as Relieving Pain in America from the Institute of Medicine (IOM) in 2011, but also because, over the past
decade, there has been a shift in policies and coverage within health plans and a changing treatment paradigm within phy-sician practices (Chapters 4, 5, and 6). The IOM estimated that more than 100 million adults (more than a third of the population), experiences some sort of chronic pain.2
As the survey data in Chapters 1, 2, and 3 of this publica-tion show, preferred treatments and coverage for those treatments vary across respondents. There are good reasons for the variability. First, an unusually diversified array of treatments and modalities are used for pain relief, not all of which are dependably effective across differentiated types of patients even when they have similar diagnoses.
Second, the clinical trials used to bring new medications to the market focus on treatment of acute pain, although chronic pain is much more prevalent and more difficult to address clinically. This impedes development of evidence-based guidelines for chronic pain. In Chapter 6 we pres-ent the ways that researchers have begun to establish pain classifications to strengthen the rigor of clinical trials of pain treatments, but also to better evaluate treatments when used for patients with specific pain diagnoses.
The most difficult problem in successfully achieving pain management’s clinical goals is made clear in the IOM report, which contends that despite the currently available range of treatment options, pain remains undertreated across the country. National statistics and statistics from the Pain Management Digest survey groups confirm this view. Surveys from our managed care directors show that 50% of managed care organization (MCO) directors believe pain is being undertreated; only 17% believe it is appropriately treated. While 38% of our full physician sample believes that pain is appropriately treated, a third believe it is undertreat-ed. The remainder of these survey respondents believe pain is overtreated.
IntroductionManaged Care Issues and Answers in Pain Management

3
Figure 1. The Pain Management Digest survey groups’ perception of how well pain is being treated across the United States
All Physicians N=220 Pain Specialists n=47 MCO N=46All Physicians N=220 Pain Specialists n=47 MCO N=46All Physicians N=220 Pain Specialists n=47 MCO N=46
29%
Pain is usuallyundertreated
Pain is appropriately
treated
Pain is usuallyovertreated
38%33%
38%38%
17%
23%
33%
50%
Acute and Chronic PainPain management practice guidelines emphasize that it is crucial to treat acute pain appropriately to avoid its pos-sible progression to chronic pain.3,9 We make the distinc-tion between the two types of pain in our survey reports and in interviews reported in this publication.
Acute pain: Most people understand and expect acute pain as a result of injury. Acute pain is a normal sensation triggered in the nervous system that alerts us to the need to take care of ourselves.2
Chronic pain: In surveys, from 10% to 20% of patients report having chronic pain when it is defi ned as persistent pain lasting at least 3 months.10 In our surveys we defi ned chronic pain as lasting 3 months or longer. Physiological-ly, chronic pain results in many changes in the peripheral and central nervous system, which are thought to aid in its persistence.11 More simply, a chronic pain continues when it should not.12
There are important social and economic consequences of undertreated pain:
• Unrelieved pain results in more emergency room visits, longer hospital stays, more outpatient visits, and missed work or job loss.3,4
• Over time, acute pain may transition to chronic pain and chronic pain can become an illness in itself.5
Diagnosis and assessment of specifi c pain complaints are dif-fi cult, and treatment guidelines are sometimes inconsistent. Pain arises from multiple causes including surgery, injury, and disease, and each patient’s pain is likely to present some-what uniquely.
Incidence of Pain: According to national medical statistics, the annual incidence of pain that lasts longer than a day stands at 26% among adults.6 It’s estimated that, annually, 25 million adults will experience acute pain, and 50 million will endure chronic pain for 3 months or longer.7
Findings from a 2010 Massachusetts survey are typical oftreatment patterns across the country. Investigators found that a quarter of the state’s population experiences pain lasting more than 3 months. Primary care providers (PCPs) treat 60% of the Massachusetts patients with pain. An even
greater number of elderly patients (67%) and minorities (76%) depend on PCPs for pain management.8
Health System Costs Resulting from Pain: In the US, persistent pain costs $560 to $635 billion annually. Research based on national medical expenditure data found that the costs of persistent pain exceed the economic costs of the six most costly major diagnoses—cardiovascular diseases ($309 billion); neoplasms ($243 billion); injury and poisoning ($205 billion); endocrine, nutritional, and metabolic diseases ($127 billion); digestive system diseases ($112 billion); and respiratory system diseases ($112 billion).2 Note from the researchers: Unlike these diagnosed conditions, pain affects a much larger number of people, by a factor of about four com-pared with heart disease and diabetes and a factor of nine compared with cancer. Thus, the per-person cost of pain is lower than that of the other conditions, but the total cost of pain is higher.2
National costs are sobering, but they do not refl ect the costs of pain as MCOs and patients experience them. Pain treat-ment is not easy to track using claims data because pain is experienced across a range of reimbursement codes for other

4
PAIN MANAGEMENT DIGEST
Key Recommendations From the Institute of Medicine2
Recommendation 2.1: Improve the collection and reporting of data on pain. The National Center for Health Statistics, the Agency for Healthcare Research and Quality, other federal and state agencies, and private organizations should improve and accelerate the collection and reporting of data on pain.
• Theeffectivenessoftreatmentinreducingpainandpain-relateddisability,determinedthroughresearchonthecomparative effectivenessofalternativetreatments(includingindifferentpatientpopulations),toidentifypeoplemostlikelytobenefit(or not)fromspecifictreatmentapproaches.
Recommendation 2.2: Createacomprehensivepopulationhealth-levelstrategyforpainprevention,treatment,management,education, reimbursementandresearchthatincludesspecificgoals,actions,timeframes,andresources.
Recommendation 3.5: Revisereimbursementpoliciestofostercoordinatedandevidence-basedpaincare.Payersandhealthcareorganiza-tionsshouldworktoalignpaymentincentiveswithevidence-basedassessmentandtreatmentofpain.Optimalcareofthepatientshouldbethe focus.
conditions. Pain itself is a symptom more often than a primary condition and is hidden within the claims system.
Even appropriate treatment can lead to additional costs—from treatment of side effects, from referrals that are not tracked as continuation of an existing condition, or from exacerbations over time. Patients pay directly for treatments that may not be covered by their insurance, and patients without insurance pay what they can, and then suspend therapy without resolution of pain. They may next appear at an emergency room. Some of those costs are presented in the introduction to Chapter 5 on page 27.
Guidelines for Pain Management: MCOs continue to seek consistency in guidelines that address pain treatments so that they can confidently move forward with programs and coverage decisions that treat pain effectively and simultaneously manage the risk of opioid abuse. For that reason, medical and pharmacy directors are relying on guidelines such as the American Pain Society 2009 Clinical Guidelines for the Use of Chronic Opioid Therapy in Chronic Noncancer Pain13 and the Washington State Medical Direc-tors’ Guidelines.14 These guidelines support MCO pharmacy programs that seek to identify patients at risk through the use of claims data. (Chapter 4)
Physicians and pain specialists have welcomed broader opportunities to learn about evidence-based pain manage-ment procedures and medicines, and have pursued broad-ened avenues to obtain pain specialist credentialing.2
A Thank You to Editorial ReviewersThis monograph on pain was suggested, guided, and reviewed by the editorial board members listed on the inside front cover. Additional information about current practices is based on more than 20 interviews with board members and with the experts in pain management across the country. All interviewees reviewed our drafts of their comments. Our editorial board reviewed all text and edited or suggested changes to strengthen our information.
We thank these knowledgeable and generous contribu-tors who are furthering the science of pain management. Without them, our understanding of issues and answers would be much poorer.
TodayToday, it is possible to believe that appropriate treatment of pain is, in fact, more easily found across the country than it was just a decade ago. Our interviews profile a range of successful pain management models from many regions. (Chapters 4, 5, and 6) And through our surveys, it is clear that a wide array of healthcare providers are expanding pain management services and are reaching more patients with treatment.

and to have been treated with at least one type of prescription pain medication, such as a COX-2 inhibitor, non-steroidal anti-infl ammatory drug (NSAID), opioid or opioid combi-nation. Types of pain could include pain resulting from an operation or surgery, fi bromyalgia, neuropathic pain caused by diabetes or other medical conditions, migraine headache, or musculoskeletal pain.
Patients with cancer-related pain were not included in this survey sample because the causes and treatments of their pain are so different from other types of pain. Figure 1 shows the geographical distribution of each survey group.
Figure 1. Regional* distribution of survey respondents
Percentages may not total 100% due to rounding.*US Census regions are defi ned as follows:Northeast: CT, ME, MA, NH, NJ, NY, PA, RI, VTMidwest: IL, IN, IA, KS, MI, MN, MO, NE, ND, OH, SD, WISouth: AL, DE, DC, FL, GA, KY, LA, MD, MS, NC, OK, SC, TN, TX, VA, WVWest: AK, AZ, CA, CO, HI, ID, MT, NV, NM, OR, UT, WA, WY
24%
20%
24%
33%
34%
22%
21%
22%
23%
27%
27%
24%
MCOs(n=46)
Physicians(n=220)
Patients(n=211)
Northeast Midwest South WestNortheast Midwest South WestNortheast Midwest South WestNortheast Midwest South West
5
Survey Methodology and ResearchSurvey design and data analysis were performed by ReCon Marketing Solutions, LLC, Medford, New Jersey, a healthcare research and communications fi rm. ReCon designed 3 proprietary survey instruments with the direction and review of an indepen-dent editorial board. Surveys were developed to collect informa-tion from core stakeholder groups: managed care organizations (MCOs), physicians, and patients. The fi rst 3 chapters of this publication report fi ndings from those surveys.
Secondary research and interviews with pain management physi-cians and payers were performed to verify the direction of data analysis and to report on initiatives in the fi eld that the editorial board determined to be of interest to the key stakeholders.
Recruitment and FieldingReCon engaged Research Now to program and fi eld the physician and patient surveys to their proprietary database. Potential MCO participants were recruited from ReCon’s managed care database and received a link to the online survey.
A forth survey (for employers) was fi elded by the Employers Health Coalition to its members in order to add that stakeholder perspective. Because that survey was still in the fi eld at the time this publication was completed, only interim data from July 28, 2013 are presented on page 11.
MCO, physician, and patient surveys were in the fi eld on an overlapping schedule from May 21 to June 2, 2013. Those who met qualifi cation criteria and submitted a completed survey were reimbursed for their time.
Respondents to all 4 surveys were assured that individual survey responses and the respondents’ names and company affi liations would be held in strict confi dence by ReCon. The fi nal report refl ects blinded and aggregated data.
Prequalifi cation CriteriaRespondents from the 3 core survey groups had to meet specifi c prequalifying criteria to ensure the integrity of their responses:
• Directors from MCOs were prequalifi ed to have knowledge of their organizations’ policies and services regarding pain man-agement
• Physicians were prequalifi ed to be current practitioners and to be actively treating patients with acute or chronic pain
• Patients were prequalifi ed to have been treated by a doctor or other healthcare provider for pain within the past 12 months
Data Analysis and Reporting
ReCon collected, clarifi ed, aggregated, analyzed and reported the resulting data using the Statistical Package for the Social Sciences. All data were blinded and aggregated across each full sample of respondents (denoted as ALL), as well as by specifi c demographic characteristics, as applicable to each survey population.
The Pain Management Digest editorial board (page 1) reviewed the survey analyses and interpretations, and the fi nal manuscript. Statements or opinions contained within the report refl ect the responses of survey respondents and interviewees, and do not necessarily refl ect those of our sponsor, Iroko Pharmaceuticals, LLC.

6
PAIN MANAGEMENT DIGEST
Medical and Pharmacy Director Perspectives on Pain Management
DemographicsOverall, 46 medical and pharmacy directors from managed care organizations (MCOs) responded to this survey. Most respondents (89%) represent managed care health plans, and 11% represent pharmacy benefit management organizations (PBMs). Most (68%) are pharmacy directors and 32% are medical directors.
The organizations represented in this sample offer a range of plan designs, with 89% offering commercial benefits covering more than 134 million members. Many also offer managed Medicare (72%) and managed Medicaid (61%) plans. (Figure 1)
Figure 1. Percentage of MCOs offering commercial, managed Medicare and managed Medicaid plans
Overall Overall lives Lines of Business* N=46 N=198,903,799
Commercial (n=41) 89% 134,289,669
Managed Medicare (n=33) 72% 42,291,443
Managed Medicaid (n=28) 61% 22,322,687
*Responding organizations may operate more than 1 line of business. Note: The reporting of covered lives by health plans and PBMs may result in double counting of lives.
IntroductionPain Management Under Commercial and Government BenefitsPerhaps no other condition is treated across a more fragment-ed healthcare system than that which serves patients with pain. Every region in the country has its own multiplicity of health care providers who offer medicinal, surgical, interven-tional, psychological, rehabilitative and physical therapies, as well as providers who offer complementary and alternative methods (CAM) to patients with pain.
Referrals among these physicians and other care providers —and among facilities—is a daily part of doing business. Additionally, the range of medications being used for pain is expansive and multimodal, often combining use of nonopi-oid and opioid analgesics, as well as drug classes commonly referred to as “adjuvant analgesic drugs,” medications that are used to treat other conditions but have been found to be ef-fective in treatment of pain patients (eg. antidepressants and anticonvulsants).1
Contracting arrangements with these providers are as central to health plan profitability, as is the organization’s ability to provide coverage for the most effective and highest quality healthcare possible while maintaining a healthy medical loss ratio (MLR). Moreover, tracking costs related specifically to pain treatment is notoriously difficult, primarily because of multiple coding issues. Also, office visits for pain evalua-tion and treatment are poorly reimbursed for PCPs. A recent review in the Clinical Journal of Pain said, “The overwhelm-ing problem for chronic pain management is how to realign the financial incentives with what is the best available care for the patient.”2
MCO Survey ResultsIn the Pain Management Digest survey, a third of the or-ganizations that responded (15 MCOs) reported having the ability to track costs across medical and pharmacy benefits,
Respondents were asked to provide information specific to each of these 3 lines of business when they were able to do so. Therefore, the total number responding to questions about commercial, Medicare, and Medicaid plan practices will vary. This is particularly evident in responses to ques-tions regarding pharmacy benefit designs and drug manage-ment under those benefits.

7
and 40% of them can also track costs related to adverse events occurring from use of pain medications. These capa-bilities support initiatives that can improve care and reduce costs.
However, very few (7%) of the responding MCOs have mechanisms in place that can help them evaluate the ef-ficacy of pain treatments. Those who have begun to address evaluation of treatment say they have investigated mortality data, provider claims, member claims, and pharmacy board prescription monitoring reports. Others are looking at emer-gency visits, inpatient surgical practices, days in intensive care, and hospital readmissions.
Across the healthcare system, plan directors are aware that pain management may not be delivered as well as it could be. Fewer than 20% of medical and pharmacy directors who responded to the Pain Management Digest survey believe that pain is “appropriately treated.”
Not many plans have tried to correlate specific pain patients to specific cost and utilization data. Therefore, when asked to
rank pain treatment according to its total costs to the plan, pain was thought to be least costly of 6 conditions. Diabetes was ranked most expensive, cardiovascular disease was next, and oncology, respiratory conditions, and mental health fol-lowed in that order.
Nevertheless, when asked how concerned these organiza-tions were with the total costs of pain management, 50% of respondents reported a high level of concern (8, 9, and 10 on the scale).
In Figure 2, responses from this survey group show that only in the treatment of acute pain—primarily addressed through medical benefits related to hospitals and surgical centers—are plan directors relatively satisfied with the current practic-es. There is a high level of dissatisfaction with management of the transition between inpatient and outpatient services, concern about substance abuse risks, a broad disparity across the group as to satisfaction with chronic pain treatment, and awareness that treatment has not effectively reduced inpa-tient admissions.
Figure 2. MCO satisfaction with stated goals of therapy
Completely dissatisfied Completely satisfied
Goals of Appropriate Therapy 1 2 3 4 5 6 7 8 9 10
Effective management of acute pain 2% 0% 7% 9% 11% 17% 15% 33% 7% 0%
Effective management of chronic pain 4% 4% 20% 9% 22% 17% 20% 4% 0% 0%
Effective management of pain during transition care between inpatient 2% 4% 9% 13% 22% 22% 22% 4% 2% 0% and outpatient services
Reduced inpatient admissions due to pain 7% 0% 17% 20% 22% 9% 17% 7% 2% 0%
Overall cost of healthcare consumed in 2% 7% 26% 20% 26% 9% 11% 0% 0% 0%
association with pain management
The risk of substance abuse associated with 9% 22% 24% 15% 15% 9% 7% 0% 0% 0%
pain management
Figure 2 lists common goals that a plan would value in designing pain management benefits and policies. Across the full scale, respon-dents’ responses cluster in midrange, but shaded boxes indicate that respondents’ satisfaction with achieving the stated goals is fairly positive for the first 3 listed and is negative regarding costs of care and management of opioid risks.
Rated on a scale of 1-10, with 1 indicating completely dissatisfied and 10 indicating completely satisfied.
CHAPTER 1 — Medical and Pharmacy Director Perspectives on Pain Management

8
PAIN MANAGEMENT DIGEST
It is possible that plans underestimate their costs for pain treatment. Figure 3 indicates that nearly a third of respon-dents estimated that 20% to 50% of members are taking pain medications. IOM data sources claim that the preva-lence of pain has made it the most costly condition in the nation (at $635 billion), with pain adding incremental costs to the healthcare system that range between $261 and $300 billion dollars annually. The remainder resulted from reduced productivity.3
Pain management programs: The dissatisfaction level expressed by these respondents refl ects the fi nding that very few have policies or programs in place to improve pain man-agement through a structured approach. (Figure 4) While
over a third (35%) said that pain management is a part of their case management programs, only 4% (2 plans) have a program that is as structured as other disease management programs. An additional 9% believe they will have such programs within 2 years.
Those MCO programs include medication management to reduce opioid abuse and diversion, and they offer addic-tion counseling. Also, they offer alternative treatments to compliment medication regimens that are not working well enough to reduce the pain. These include but are not limited to physical and behavioral therapies and complementary and alternative methods (CAM). In addition, MCOs actively provide ongoing patient and physician education through multiple methods, including personal case manager outreach and phone counseling.
Considerably more MCOs offer pain management educa-tional information to providers (18%) and members (30%), primarily through newsletters and mailings. Three MCOs reported having pain management programs specifi cally for geriatric members with pain. One of those MCOs is a man-aged Medicare plan.
Although MCOs may not have programs of their own, a substantial number (41%; n=17) reimburse treatment from multidisciplinary/interdisciplinary pain programs, and an additional 7% have plans to do so within the next 2 years. Because there are no national accreditation criteria for pain centers, MCOs approach selection of and reimbursement
Figure 4. Percentage of MCO respondents having active pain management programs
Will have this capability Yes No within the next 2 years
MCO has a care/case management program for pain management 35% 57% 9%
MCO is aware of national guidelines for pain management 70% 30% *
MCO has a structured pain management program, similar to other disease management programs 4% 89% 7%
MCO offers provider education on pain management 18% 75% 7%
MCO offers patient education on pain management 30% 68% 2%
MCO has a specifi c program for geriatric patients with pain 7% 93% 0%
MCO reimburses claims from multidisciplinary/interdisciplinary pain programs 41% 52% 7%
*not applicable
Figure 3. Estimated percentage of members who at any given point in time are on pain medication
59%
20%
7%
7%
4%4%
<10%
10–20%
21–30%
32–40%
41–50%
Don’t know
Almost 80% of MCO directors estimate that, at any given point in time, from 10% to 30% of covered members are being treated for pain.

9
Figure 6. MCO satisfaction with the support the plan extends to PCP pain management practices
1 2 3 4 5 6 7 8 9 10
0%
4%
9%
17%15%
24% 24%
7%
0% 0%
1= Completely dissatisfied 10= Completely satisfied
Rated on a scale of 1-10, with 1 indicating completely dissatisfi ed and 10 indicating completely satisfi ed.
In Figure 5, it’s clear that few MCOs (4%) are highly satisfi ed with their current approach to pain, and only 7% (in Figure 6) are satisfi ed with their organizations’ support of good pain management practices among PCPs. A solid majority, however, rated satis-faction between a 4 and 7 on the 10-point scale, indicating a moderate level of satisfaction.
1 2 3 4 5 6 7 8 9 10
2%4%
13% 13%
20% 20%
24%
4%
0% 0%
1= Completely dissatisfied 10= Completely satisfied
Figure 5. MCO satisfaction with their current approach to addressing pain as a clinical issue
Methods MCOs use to reimburse multidisciplinary pain programs as reported by survey respondents
• Planscontractdirectlywithrecognizedcentersinthe coverage region• Coverageafterpriorauthorizationandreferralfroma participating provider• Paincentersarecredentialedbytheplan• Paincentersandreferralsarepartoftheplan’spatient centered medical home model• Eachinterventiongeneratesaseparateclaimbycode; notbundled;nodailycharge• Painspecialistsandpaintreatmentfacilitiesarewithin the provider network
for such care in multiple ways (see below). Figures 5 and 6 indicate the level of satisfaction MCO managers report in their approaches to pain management.
Analgesic medication management: This survey asked MCOs about their practices and opinions regarding coverage and value of COX-2 inhibitors, oral NSAIDs, topical and transdermal NSAIDs, long- and short-acting opioids, trans-dermal opioids, and buprenorphine products. Figure 7 sum-marizes respondents’ satisfaction with the medication’s clinical effi cacy, clinical safety, and cost.
With the exception of oral NSAIDs, few respondents con-sidered costs of these treatments to be satisfactory; 70% are
satisfi ed with costs of oral NSAIDs. Almost 40% were also satisfi ed with the costs of short-acting opioids.
Overall, only a third of respondents reported a high level of satisfaction with clinical effi cacy, and even fewer were satisfi ed with safety of the listed therapeutic agents. Over-all, 30% to 35% were satisfi ed with the clinical effi cacy of oral NSAIDs, long-acting opioids, short-acting opioids and transdermal opioids. Only 13% were satisfi ed with effi cacy of COX-2 inhibitors.
Only 26% expressed a high level of satisfaction with clinical safety of topical/transdermal NSAIDs and COX-2 inhibitors (rating them at 8, 9 or 10 on a scale of 1 to 10).
Figure 7. Level of satisfaction by drug type
Clinical ClinicalDrug Type Effi cacy Safety Cost
COX-2 inhibitors 13% 26% 4%
Oral NSAIDs 35% 15% 70%
Topical/Transdermal NSAIDs 2% 26% 7%
Long-Acting Oral Opioids 35% 4% 4%
Short-acting Oral Opioids 30% 9% 37%
Transdermal Opioids 24% 9% 2%
Buprenorphine products 15% 11% 2%
On a scale of 1-10, with 1 indicating complete dissatisfaction and 10 indicating complete satisfaction, these percentages of respondents responded with an 8-10 rating.
CHAPTER 1 — Medical and Pharmacy Director Perspectives on Pain Management

10
PAIN MANAGEMENT DIGEST
Reasons for dissatisfaction are most often related to side ef-fects associated with currently available medications. Conse-quently, the FDA in its post-marketing directive documents for prescribers and for patients are focused on safety and prevention of side effects. For example, when using prescrip-tion NSAIDs, patients are cautioned to take the medication exactly as prescribed, and use the lowest effective dose for the shortest duration consistent with the individual patient treatment goals.4
In a different survey question about the value of pain medi-cations, respondents were asked to rank the most valuable attributes of the three most prescribed pain medications (with 1 as the highest value and 3 as the lowest).
• COX-2 inhibitors: 1–clinical efficacy; 2–safety; 3–cost
• Prescription NSAIDs: 1–clinical efficacy; 2–cost; 3–safety
• Oral opioids: 1–clinical efficacy; 2–safety; 3–cost.
Cost of pain medications to the plan: Almost all respon-dents (98%) believe that the value of prescription NSAIDs is highly commensurate with their cost. MCOs also value short acting opioids (87% of respondents). Other product types in this list were not viewed as having as high a value compared with their cost to the plan.
In general, pain medications are not being highly managed by these MCOs. The majority focus on quantity limits, with oral opioids attracting the most attention: 71% of commer-
Barriers to adequately evaluating pain management as reported by MCO survey respondents
• Painisverysubjective;noteasilymeasurable• Notenoughdataarecapturedtoknowhowwell membersarebeingtreatedforpain• Noestablishedclinicalmechanismtoevaluate effectiveness of treatment• Chronicpainishighlycomplexandtherearetoofew specialists• Ambiguityofclaimsdata• Totalcostsareimpossibletodetermine• Plansaretertiarytocare;nointeractionwithpatient or provider• Highvolumeofpatientswithpain;broadrangeof indications;toomuchtoaddresswithcurrentplan resources
Pain in the Workplace: An Employer Coalition SurveyA surprising finding in the results of the MCO survey was that only 1 of the 46 MCO respondents has a partner-ship program with its employer customers to improve pain management treatment practices. However, that respondent reported that the program has succeeded in making benefit design changes which prevent opioid abuse and, thus, is reaching a goal of reducing costs related to misuse.
On page 11, the Pain Management Digest presents early results from a proprietary survey of employer benefit plan managers and medical directors who are members of a national employer coalition.
cial plans and 64% of Medicare plans. COX-2 inhibitors are managed through quantity limits by 54% of commercial plans, and are also subject to step-therapy by 49%.
NSAIDs are the least restricted of the three types of medica-tions. Quantity limits were applied to NSAIDs by about 29% of commercial plans and 33% of Medicare plans. Oral opioids are restricted in terms of quantity limits but less re-stricted by prior authorizations or step therapy requirements.
In a closer look at how cost was spread across a range of pain medications, respondents estimated the portion of spending each agent contributed to the total pharmacy benefit spend for pain medications. Opioids were considerably more costly than the other medications listed, and they are estimated to account for 41% of the total. Prescription NSAIDs at 18% of the total and COX-2’s at 11% compose about 30% of the total, with opioid combination products at 12% of the total. Buprenorphine products accounted for 10% of total spending. “Other agents” accounted for 9% and included antidepressants, neurologic pain products for migraine, other analgesic patches, anticonvulsants, and toradol.
MCO respondents continue to struggle with multiple barriers that impede their ability to put policies in place to support effective, appropriate pain management for their members and generally improve quality of care delivered by providers who treat patients with pain. (See the “Barriers” reported by these respondents in the box on this page)

11
In an abbreviated analysis of this Employers Health Coalition survey, responses from 17 companies are reported, represent-ing 88,140 employees and dependents enrolled in health benefi t plans. Company size ranges from 154 to over 27,000 employees. Across this sample, employers pay an average 72% of the health plan premium for their employees.
Survey results: Using pharmacy and medical claims data, respondents reported that cardiovascular disease ranks fi rst in regard to its cost impact, followed by cancer and diabetes. Cost of pain ranked fourth, followed by respiratory condi-tions, and mental health. Relative prevalence of chronic conditions among plan members was reported as well, with diabetes ranking fi rst, followed by hypertension, cardiovas-cular disease, pain, and allergies.
Forty-seven percent of respondents estimated that 10% to 25% of medical claims represent procedures to relieve or manage pain, with 53% estimating the same percent-age range for pharmaceutical claims for pain medications. (Figure 1)
The impact of pain on employee productivity was also explored, and chronic low back pain and other joint, neck or muscular pain were judged to have the most negative impact. Migraine or other headache, and arthritis were reported in third and fourth position.
When asked to report concerns relating to pain medications (COX-2 inhibitors, non-narcotic prescription pain reliev-ers, opioids and fi xed combination products with opioids), respondents were most concerned with employees’ use of opioids and opioid combinations (40%). They specifi cally cited concerns about safety, disqualifi cations for driving or operating machinery, and addiction. Gastrointestinal or renal side effects were concerns regarding COX-2 inhibitors and non-narcotic prescription pain relievers, followed by con-cerns about cost and overuse.
When asked about concerns related to pain management within their companies, 80% said they are most concerned that employees having diffi culties with narcotic medications may create safety issues within the workplace, 60% are most concerned with the costs related to pain management, and 53% are concerned that there may be overuse or abuse of narcotic pain relievers among covered members. A closely re-lated issue is that these respondents say that they don’t know how to assess the impact of pain-related effects on worker productivity while at work.
Employer Survey: Interim Results*
Figure 1: Estimated percentage of employers’ healthcare benefi t claims related to pain management
Medical claimsMedical claimsPharmacy claims
20%
20%
53%47%
0%
20%20%
Less than 10%
Between 10%–25%
Greater than 50%
Don’t know
Between 26%–50%
7%
7%
7%
TheEmployersHealthCoalition,Inc.isanot-for-profit501(c)(3)organizationfoundedin1983withofficesinOhio.Itpro-videsmemberorganizationswithproductsandservicesthathelpmaximizethevalueofthehealthandwellnessbenefitsdeliveredtoitsmemberorganization’semployees.Today,thecoalitionrepresentsmorethan300memberorganizationswithcoveredlivesin50states.
*Survey fi ndings on this page come from an early analysis of partial responses (from 17 of a fi nal 21 respondents). The survey was still in the fi eld when this publication was written.
CHAPTER 1 — Medical and Pharmacy Director Perspectives on Pain Management

12
PAIN MANAGEMENT DIGEST
Practices in Pain Treatment and Management: A Physician Survey
DemographicsOf the 220 physicians who responded to this survey, 27% practice in a primary care setting, and 14% practice in a multispecialty group. Forty-one percent are in a private or group single-specialty setting. (Figure 1) In the full, 220-physician sample, 47 respondents (22%) self-reported a primary or secondary specialty in pain medicine or pain management. (Figure 2 in boxed text)
Fourteen percent of the full sample, and 21% of pain specialists, practice in a multispecialty group; 45% of pain specialists are in primary care practice settings; and 17% are affi liated with a pain management clinic.
Figure 1. Practice affi liations, full survey group and pain specialists
ALL PS Practice Settings N=220 n=47
Private practice, primary care 15% 30%
Private practice, single specialty 21% 19%
Group practice, primary care 12% 15%
Group practice, single specialty 20% 15%
Group practice, multispecialty 14% 21%
Affi liated with a university or 19% 19%academic center
Affi liated with a community hospital 22% 23%
Affi liated with a major medical center 9% 9%
Community clinic 6% 2%
Pain management clinic 4% 17%
Respondents were asked to select all that applied and percentages may total >100%.PS=Pain Specialist.
Among these physicians, reimbursement through commer-cial plans accounted for 42% of total income, with Medicare providing 25% and Medicaid providing 18%. Cash pay-ments from patients to the physician practice stand at 8% overall and at 10% among the pain specialist subgroup.
IntroductionAs mentioned in the MCO survey, a major goal of pain management is to increase the numbers of patients with pain who receive appropriate, effective treatment, not only because patients benefi t, but also because the health system itself benefi ts. First, such therapy reduces the strain that undertreated pain puts on services, and appropriate treat-ment that follows accepted guidelines is likely to reduce costs
Pain Specialists
Primary specialtyn=26
Secondary specialtyn=21
Not a pain specialistn=173
79%
12%
10%
Physicians who specialize in pain management come to that clinical expertise by multiple routes: through practice experience, and through recognition and/or credentialing from a number of professional organizations.
Physicians already board certifi ed by the American Board of Medical Specialties (ABMS) in anesthesiology, physical medicine and rehabilitation, or psychiatry/neurology are also eligible to obtain a subspecialty certifi cation in pain medicine. More recently, the American Academy of Pain Management has also offered an accreditation program that recognizes a specialty in pain management. The pro-gram credentials physicians as well as pain management centers that meet specifi c qualifi cations.1,2
Figure 2. Percentage of respondents having a primary or secondary specialty in pain management or pain medicine
13
associated with using treatments that are not needed or are ineffective. Physicians are the pivot point between the patients and the insurer; and for pain patients, the fi rst doctor to treat their pain is likely to be a primary care physician (PCP)
Researchers agree that PCPs treat the majority of people who have chronic pain,2,3 and a primary care practice is where most people fi rst report a pain. This is the key point of entry to the health system. Consequently, the treatment offered by a PCP to a new pain patient is critical.1
• If a new pain complaint is resolved swiftly, it can make a difference in halting a possible progression to chronic pain.
• If an already chronic pain is addressed effectively, its im-pact can be reduced and may lead to fuller functionality.
The number of pain specialists is increasing but is still inadequate to treat all patients who might benefi t from a specialist consult. Between 2000 and 2009, only 3,488 physi-cians became ABMS board certifi ed in pain medicine.2
To meet the growing need for effective treatment of patients with pain, the US health system has begun a determined effort to broadly extend educational information about pain treatment to PCP practices—with a particular focus upon physicians practicing in an Accountable Care Organization (ACO) or a patient-centered medical home.
Medical schools, CME providers, some payer organizations, and physician-led pain management societies encourage publications and programs to expand the understanding of the clinical skills used in the treatment of pain.
Survey ResultsPain Management PracticesAcross this sample, physicians treat a mean 321 pain pa-tients monthly. Pain specialists, not surprisingly, treat more; the mean monthly volume reported by them is 363 pain patients. As estimated across the full sample of specialty and PCP practices, pain is the most often treated condition, diabetes is next and cardiovascular disease is third.
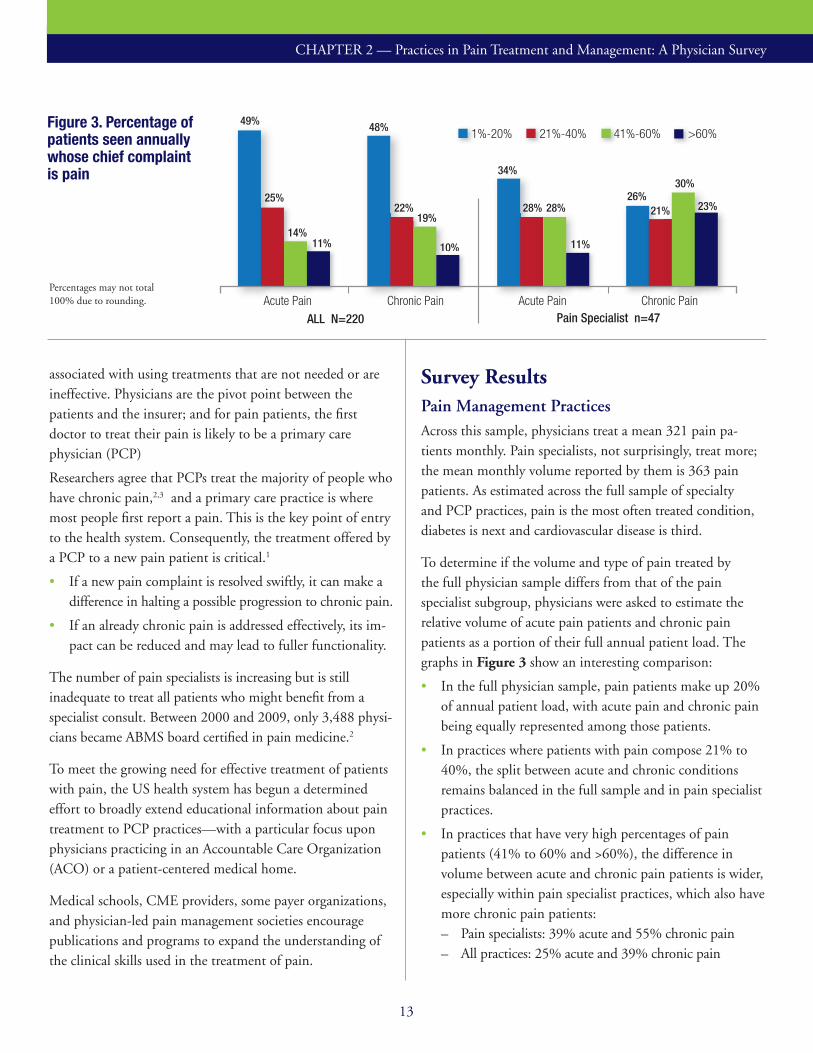
To determine if the volume and type of pain treated by the full physician sample differs from that of the pain specialist subgroup, physicians were asked to estimate the relative volume of acute pain patients and chronic pain patients as a portion of their full annual patient load. The graphs in Figure 3 show an interesting comparison:
• In the full physician sample, pain patients make up 20% of annual patient load, with acute pain and chronic pain being equally represented among those patients.
• In practices where patients with pain compose 21% to 40%, the split between acute and chronic conditions remains balanced in the full sample and in pain specialist practices.
• In practices that have very high percentages of pain patients (41% to 60% and >60%), the difference in volume between acute and chronic pain patients is wider, especially within pain specialist practices, which also have more chronic pain patients: – Pain specialists: 39% acute and 55% chronic pain– All practices: 25% acute and 39% chronic pain
Figure 3. Percentage of patients seen annually whose chief complaint is pain
1%-20% 21%-40% 41%-60% >60%
10%10%10%
ALL N=220
14%11%
49%
25%
Acute Pain Chronic PainPain Specialist n=47
Acute Pain Chronic Pain
48%
22%19%
34%
28%26%
11%
28% 23%
30%
21%
Percentages may not total 100% due to rounding.
CHAPTER 2 — Practices in Pain Treatment and Management: A Physician Survey
14
PAIN MANAGEMENT DIGEST
2 to 31 4 to 5 more than 5
Number of different medications
49%60%
31%30%
13%7% 7%3%
ALL N=220 Pain Specialists n=47 ALL N=220 Pain Specialists n=47 ALL N=220 Pain Specialists n=47
Figure 4. Percentage of pain patients being treated with 1 or more analgesic medications
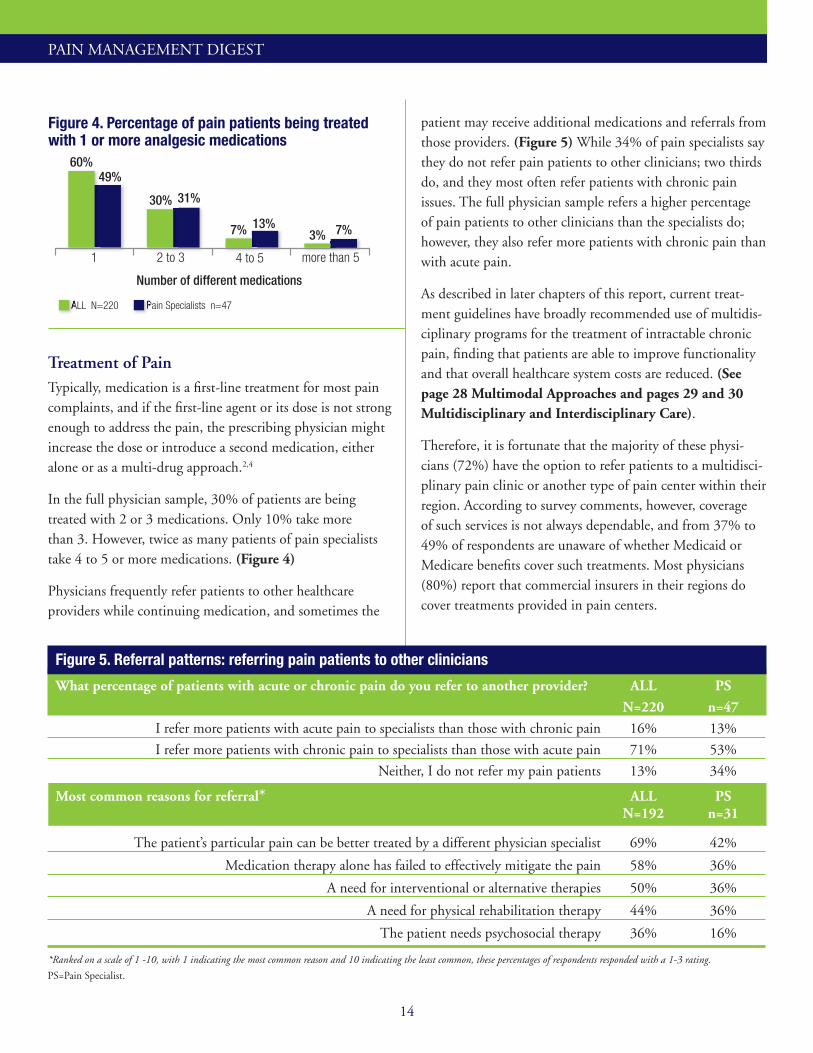
Treatment of PainTypically, medication is a fi rst-line treatment for most pain complaints, and if the fi rst-line agent or its dose is not strong enough to address the pain, the prescribing physician might increase the dose or introduce a second medication, either alone or as a multi-drug approach.2,4
In the full physician sample, 30% of patients are being treated with 2 or 3 medications. Only 10% take more than 3. However, twice as many patients of pain specialists take 4 to 5 or more medications. (Figure 4)
Physicians frequently refer patients to other healthcare providers while continuing medication, and sometimes the
patient may receive additional medications and referrals from those providers. (Figure 5) While 34% of pain specialists say they do not refer pain patients to other clinicians; two thirds do, and they most often refer patients with chronic pain issues. The full physician sample refers a higher percentage of pain patients to other clinicians than the specialists do; however, they also refer more patients with chronic pain than with acute pain.
As described in later chapters of this report, current treat-ment guidelines have broadly recommended use of multidis-ciplinary programs for the treatment of intractable chronic pain, fi nding that patients are able to improve functionality and that overall healthcare system costs are reduced. (See page 28 Multimodal Approaches and pages 29 and 30 Multidisciplinary and Interdisciplinary Care).
Therefore, it is fortunate that the majority of these physi-cians (72%) have the option to refer patients to a multidisci-plinary pain clinic or another type of pain center within their region. According to survey comments, however, coverage of such services is not always dependable, and from 37% to 49% of respondents are unaware of whether Medicaid or Medicare benefi ts cover such treatments. Most physicians (80%) report that commercial insurers in their regions do cover treatments provided in pain centers.
Figure 5. Referral patterns: referring pain patients to other clinicians
What percentage of patients with acute or chronic pain do you refer to another provider? ALL PS
N=220 n=47
I refer more patients with acute pain to specialists than those with chronic pain 16% 13%
I refer more patients with chronic pain to specialists than those with acute pain 71% 53%
Neither, I do not refer my pain patients 13% 34%
Most common reasons for referral* ALL PS N=192 n=31
The patient’s particular pain can be better treated by a different physician specialist 69% 42%
Medication therapy alone has failed to effectively mitigate the pain 58% 36%
A need for interventional or alternative therapies 50% 36%
A need for physical rehabilitation therapy 44% 36%
The patient needs psychosocial therapy 36% 16%
*Ranked on a scale of 1 -10, with 1 indicating the most common reason and 10 indicating the least common, these percentages of respondents responded with a 1-3 rating.
PS=Pain Specialist.
15
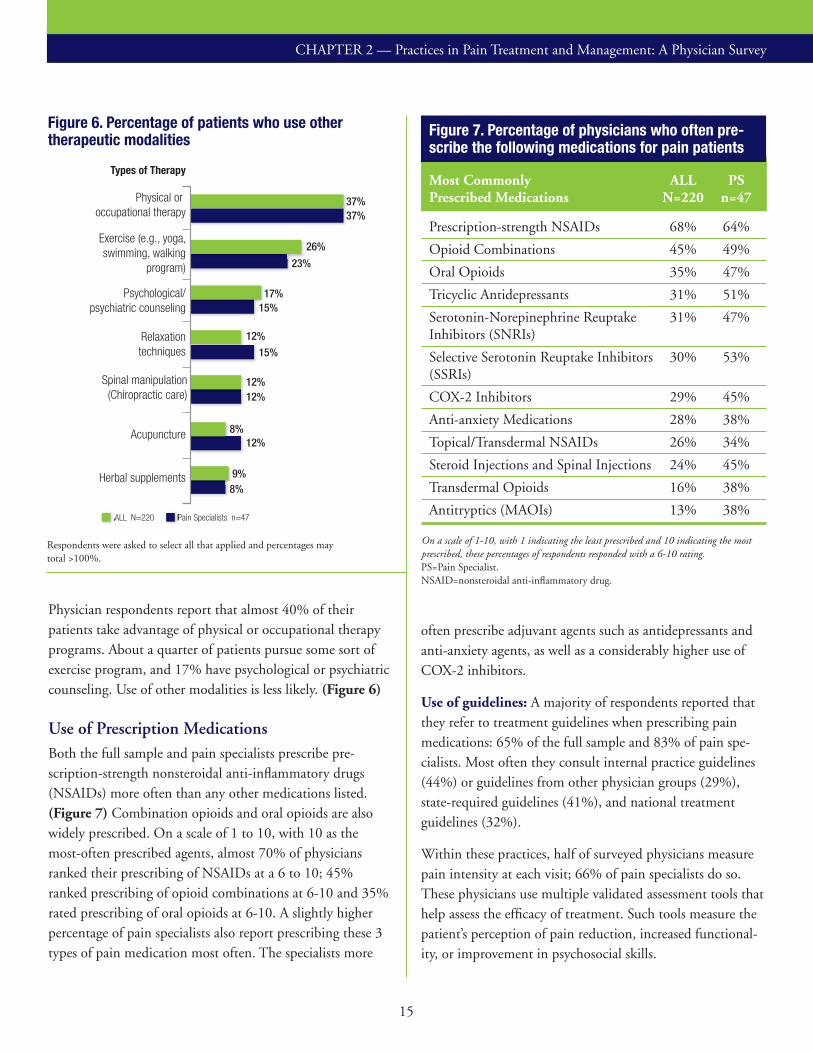
Physician respondents report that almost 40% of their patients take advantage of physical or occupational therapy programs. About a quarter of patients pursue some sort of exercise program, and 17% have psychological or psychiatric counseling. Use of other modalities is less likely. (Figure 6)
Use of Prescription MedicationsBoth the full sample and pain specialists prescribe pre-scription-strength nonsteroidal anti-infl ammatory drugs (NSAIDs) more often than any other medications listed. (Figure 7) Combination opioids and oral opioids are also widely prescribed. On a scale of 1 to 10, with 10 as the most-often prescribed agents, almost 70% of physicians ranked their prescribing of NSAIDs at a 6 to 10; 45% ranked prescribing of opioid combinations at 6-10 and 35% rated prescribing of oral opioids at 6-10. A slightly higher percentage of pain specialists also report prescribing these 3 types of pain medication most often. The specialists more
Figure 6. Percentage of patients who use other therapeutic modalities
ALL N=220 Pain Specialists n=47ALL N=220 Pain Specialists n=47
37%37%
26%
23%
17%15%
12%
15%
12%12%
12%8%
8%9%
ALL N=220 Pain Specialists n=47
Physical or occupational therapy
Exercise (e.g., yoga, swimming, walking
program)
Psychological/psychiatric counseling
Relaxation techniques
Spinal manipulation (Chiropractic care)
Acupuncture
Herbal supplements
Types of Therapy
often prescribe adjuvant agents such as antidepressants and anti-anxiety agents, as well as a considerably higher use of COX-2 inhibitors.
Use of guidelines: A majority of respondents reported that they refer to treatment guidelines when prescribing pain medications: 65% of the full sample and 83% of pain spe-cialists. Most often they consult internal practice guidelines (44%) or guidelines from other physician groups (29%), state-required guidelines (41%), and national treatment guidelines (32%).
Within these practices, half of surveyed physicians measure pain intensity at each visit; 66% of pain specialists do so. These physicians use multiple validated assessment tools that help assess the effi cacy of treatment. Such tools measure the patient’s perception of pain reduction, increased functional-ity, or improvement in psychosocial skills.
Figure 7. Percentage of physicians who often pre-scribe the following medications for pain patients
Most Commonly ALL PSPrescribed Medications N=220 n=47
Prescription-strength NSAIDs 68% 64%
Opioid Combinations 45% 49%
Oral Opioids 35% 47%
Tricyclic Antidepressants 31% 51%
Serotonin-Norepinephrine Reuptake 31% 47%Inhibitors (SNRIs)
Selective Serotonin Reuptake Inhibitors 30% 53%(SSRIs)
COX-2 Inhibitors 29% 45%
Anti-anxiety Medications 28% 38%
Topical/Transdermal NSAIDs 26% 34%
Steroid Injections and Spinal Injections 24% 45%
Transdermal Opioids 16% 38%
Antitryptics (MAOIs) 13% 38%
On a scale of 1-10, with 1 indicating the least prescribed and 10 indicating the most prescribed, these percentages of respondents responded with a 6-10 rating.PS=Pain Specialist. NSAID=nonsteroidal anti-infl ammatory drug.
Respondents were asked to select all that applied and percentages may total >100%.
CHAPTER 2 — Practices in Pain Treatment and Management: A Physician Survey

16
PAIN MANAGEMENT DIGEST
Prescribing pain medications: A majority of physicians re-port that they follow recommended practices when prescribing opioids: 65% of the full sample and 81% of pain specialists say that they educate patients about opioid risks, and 55% also routinely administer urine drug tests and ask patients to sign a contract when an opioid is prescribed. (Figure 8)
The factors that limit the level of prescribing the agents listed in Figure 9 are well established in the literature and among prescribers. In this survey, both the full sample and pain spe-cialists agreed on which of the key factors in the drug profi le cause the most concern and, thereby, limit their prescribing. A majority of prescribers considered abuse potential and the risk of opioid-induced tolerance to be the most limiting fac-tors in their prescribing of opioids. No other characteristics of any pain medication agents caused so high a level of concern. Clinical safety and incidence of side effects regarding use of COX-2 inhibitors was a highly limiting factor for 30% of all respondents but of <30% pain specialists. Side effects was also a limiting factor when prescribing NSAIDs for >30% of all physicians and >40% of pain specialists.
No doubt because of the limitations mentioned, relatively few physicians believe that the available drug therapies for pain are able to address the broad goals of pain therapy shown in Figure 10. Physicians ranked their satisfaction on a scale of 1 to 10 with 1 being completely dissatisfi ed, and 10 completely satisfi ed.
Physicians reported a modest level of satisfaction with clini-cal effi cacy, and they report that the patients they prescribe these drugs for have a lower level of satisfaction than the prescribers do.
Figure 8. Physician practices when prescribing opioids
55%
65%
81%
39%
ALL N=220 Pain Specialists n=47 ALL N=220 Pain Specialists n=47 ALL N=220 Pain Specialists n=47
Give patients educational information about risks
associated with prescription opioid pain relievers
Routinely administer urine tests to check for
opioid abuse
Ask patients to sign a pain contract or an opioid
treatment contract when an opioid is prescribed for them
33%
55%
Figure 9. Limiting factors of COX-2 inhibitors, oral NSAIDs, oral opioids, and opioid combinations
Drug classifi cation ALL PS N=220 n=47
30% or more physicians identifi ed the listed drug charac-teristics as the most limiting factors in prescribing the drug
COX-2 Inhibitors Clinical safety/incidence of side effects 30% <30%
Oral NSAIDs Clinical safety/incidence of side effects 36% 40% Potential, serious adverse events 33% 43% Patient tolerability <30% 34%
Oral Opioids Clinical safety/incidence of side effects 35% 38% Potential, serious side effects 42% 51% Patient tolerability <30% 34% Abuse potential 72% 57% Opioid-induced tolerance 57% 45% Fear of prescribing 32% 40%
Opioid Combinations Potential, serious side effects 38% 34% Abuse potential 56% 41% Opioid-induced tolerance 44% 38%
On a scale of 1-10, with 1 indicating the least limiting and 10 indicating the most limiting, 30% or more respondents rated these at 8-10.PS=Pain Specialist.
Figure 10. Satisfaction with ability to affect broad goals of pain therapy ALL PSGoals of therapy N=220 n=47
Effective management of acute pain 35% 28%
Reduced inpatient admissions due 25% 28%to pain
Effective management of pain during transition care between inpatient and 16% 30%outpatient services
The risk of substance abuse associated 14% 26%with pain management
Effective management of chronic pain 12% 21%
Overall cost of healthcare consumed in 11% 23%association with pain management
On a scale of 1-10, with 1 indicating complete dissatisfaction and 10 indicating complete satisfaction, these percentages of respondents responded with an 8-10 rating.PS=Pain Specialist.

17
Pain Management: The Patient Experience
DemographicsA total of 211 patients completed the full survey. Almost half (104 patients) were 60 years old or older. More than two thirds of the sample was female (71%) and 29% was male. Patient respondents to this survey were currently being treated or had been treated with a prescription pain medica-tion within the past 12 months. They may have been treated in a physician’s offi ce, or in a clinic, hospital, or emergency department.
Figure 1. Percentage of patients reporting a pain complaint within the past 12 months, by type of pain
All N=211 Over 60 n=104All N=211 Over 60 n=104
60% 63%
23% 25%18% 12%
MusculoskeletalPain
Post-surgicalPain
NeuropathicPain
Survey Demographics
Patient GroupsAll=full sample (N=211)
Types of PainMusculoskeletal Pain (n=126)Neuropathic Pain (n=38)Post-surgical Pain (n=47)
Defi nitions of pain as used in this survey
Musculoskeletal Pain: arising from multiple sources such as but not limited to injury; back/neck pain; arthritis; muscle, bone, or joint pain.
Neuropathic Pain: arising from fi bromyalgia, migraine, or neuropathic pain caused by diabetes or some other chronic condition.
Post-surgical Pain: arising from an operation, surgery or procedure that took place in a hospital, doctor’s offi ce, or clinic.
While the majority of patients classifi ed their pain as muscu-loskeletal, nearly a quarter of the sample reported having a pain that originated with a surgical procedure. Fewer (18%)reported having neuropathic pain. (Figure 1)
Among the types of prescription pain medications these respondents have been taking, relatively few had been pre-scribed a COX-2 inhibitor, but almost 40% of patients have had an opioid prescription, and 51% have had an NSAID prescription at some time. (Figure 2)
Opioid combination medications are commonly prescribed for a wide range of acute pain conditions, and 81% of re-spondents with post-surgical pain report having taken these agents. Overall, more than half of respondents have received prescription NSAIDs, and 59% have received an opioid combination medication.
Most respondents were covered by insurance; 96% overall. Half were covered by an employer-sponsored health plan, 29% had Medicare with drug coverage, and 11% had
Figure 2. Percentage of patients having taken a prescription medication for pain over the past 12 months
Musculoskeletal pain n=126All N=211
Neuropathic pain n=38 Post-surgical pain n=47
47%47%47%Opioid
Combinations
PrescriptionNSAIDs
Opioids
COX-2Inhibitor
59%55%
81%51%
55%50%
43%
37%37%40%
32%
12%14%
13%9%
Respondents were asked to select all that applied and percentages may total >100%.
CHAPTER 3

18
PAIN MANAGEMENT DIGEST
Medicare without drug coverage. Commercial coverage was less prevalent among those over 60 years old (39%). Six per-cent of the full sample and 9% of those over 60 had military or Veteran’s Affairs (VA) benefits. Only 4% of this sample had Medicaid benefits.
Many were currently being treated with pain medications, and 54% of the full sample was also taking medication for anxiety and/or depression. Just over 30% had been treated for a cardiovascular condition and 19% were treated for diabetes during the previous 12 months.
IntroductionThe impact of persistent pain is profound. It affects patient’s lives and it affects the healthcare system that continues to cover costs related to pain that is not successfully treated. In a 2006 survey from the American Pain Foundation (APF), Voices of Pain, more than half of the national respondent group reported that they had no control over their pain even though they were currently being treated. More than 75% were depressed, and only 14% were satisfied with current medications.1 Older patients are known to be even more deeply compromised by pain than younger adults.2
In the Pain Management Digest survey, 70% of respon-dents have suffered from pain-related sleeplessness, 60% report a reduction of their daily functionality, and 39% are depressed. Thus, the patient experiences reported in our sur-vey are similar to those in the APF survey, showing that for people with chronic pain, control over their pain and their lives becomes “an elusive goal.”1
Typically, guidelines for pain management recommend a “stepped” approach in prescribing medications. These are consistent with directives from the FDA to use “the lowest effective NSAID dose for the shortest duration consistent with the individual patient treatment goals,”3 and with guidelines for older adults from the American Geriatrics Society,4 which recommend “initiating pain medications with low doses followed by careful upward titration, including use of frequent pain assessments for dosage reassessment.” (See Appendix on page 37)
For example, acetaminophen is commonly used as initial treatment for musculoskeletal pain; NSAIDs (other than COX-2 inhibitors) are also a common first choice and may
be preferred for patients with chronic inflammatory pain. NSAIDs are also deemed to be helpful as an effective short-term option in addressing breakthrough pain. Opioid treat-ments are reserved, if possible, for intractable pain.4
• Our survey asked patients what analgesics they are taking and what their experience is in using these common pain medications: NSAIDs, COX-2 inhibitors, opioids, and opioid combinations.
Survey ResultsThe patient experience: Despite the fact that 96% of this patient sample has healthcare coverage and access to a range of therapies, a majority of surveyed patients with chronic pain reported that their pain had not been completely resolved with treatment. Nevertheless, when respondents were asked if they experienced a difference in their level of pain before and after treatment, 62% reported having the highest level of pain pos-sible before treatment. Only 17% had so high a level of pain after treatment began. Treatment made a positive difference.
Figure 3. Characteristics of patients being treated for an active pain complaint
Musculo- Neuro- Post- skeletal pathic surgical ALL Pain Pain Pain N=163* n=99 n=33 n=31
Patients with an active continuing pain complaint
84% 85% 85% 81%
Number of times patients visited a healthcare provider for the same pain complaint over the previous 12 months
Once 11% 12% 12% 7%
2 to 4 50% 51% 46% 52%
5 to 8 25% 23% 30% 23%
9 to 12 3% 4% 0% 3%
Weekly 4% 3% 6% 3%
Monthly 5% 4% 6% 7%
Patients who are currently taking prescribed pain medications
89% 91% 88% 84%
*At the time surveyed, 163 of the total 211 patient respondents were experiencing an active pain condition and were being treated for it. 89% of those were being treated for a continuing pain.
19
Figure 4. Time to pain resolution for patients who have previously had or currently have a pain complaint that lasted longer than 3 months—a chronic pain
1 to 3 weeks 1 to 3 months 3 to 6 months 6 to 12 months
Not Yet Resolved
Time to Resolution
ALLN=181
5%7%
11%
8%
4% 5%
11% 11%
7%5% 5%
8% 8%
11% 11%
17%
Musculoskeletal Pain n=108
Post-surgicalPainn=36
NeuropathicPainn=37
ALLN=181
Musculoskeletal Pain n=108
Post-surgicalPainn=36
NeuropathicPainn=37
69% 74% 70%53%
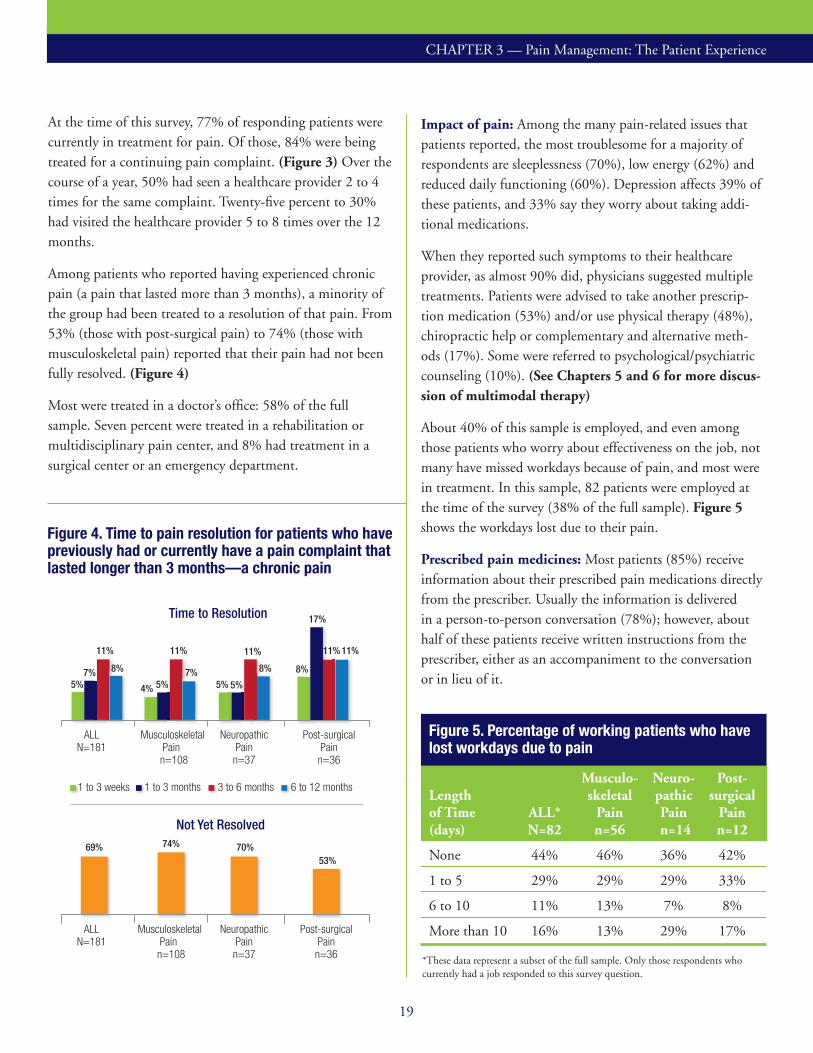
At the time of this survey, 77% of responding patients were currently in treatment for pain. Of those, 84% were being treated for a continuing pain complaint. (Figure 3) Over the course of a year, 50% had seen a healthcare provider 2 to 4 times for the same complaint. Twenty-fi ve percent to 30% had visited the healthcare provider 5 to 8 times over the 12 months.
Among patients who reported having experienced chronic pain (a pain that lasted more than 3 months), a minority of the group had been treated to a resolution of that pain. From 53% (those with post-surgical pain) to 74% (those with musculoskeletal pain) reported that their pain had not been fully resolved. (Figure 4)
Most were treated in a doctor’s offi ce: 58% of the full sample. Seven percent were treated in a rehabilitation or multidisciplinary pain center, and 8% had treatment in a surgical center or an emergency department.
Impact of pain: Among the many pain-related issues that patients reported, the most troublesome for a majority of respondents are sleeplessness (70%), low energy (62%) and reduced daily functioning (60%). Depression affects 39% of these patients, and 33% say they worry about taking addi-tional medications.
When they reported such symptoms to their healthcare provider, as almost 90% did, physicians suggested multiple treatments. Patients were advised to take another prescrip-tion medication (53%) and/or use physical therapy (48%), chiropractic help or complementary and alternative meth-ods (17%). Some were referred to psychological/psychiatric counseling (10%). (See Chapters 5 and 6 for more discus-sion of multimodal therapy)
About 40% of this sample is employed, and even among those patients who worry about effectiveness on the job, not many have missed workdays because of pain, and most were in treatment. In this sample, 82 patients were employed at the time of the survey (38% of the full sample). Figure 5 shows the workdays lost due to their pain.
Prescribed pain medicines: Most patients (85%) receive information about their prescribed pain medications directly from the prescriber. Usually the information is delivered in a person-to-person conversation (78%); however, about half of these patients receive written instructions from the prescriber, either as an accompaniment to the conversation or in lieu of it.
Figure 5. Percentage of working patients who have lost workdays due to pain
Musculo- Neuro- Post-Length skeletal pathic surgical of Time ALL* Pain Pain Pain(days) N=82 n=56 n=14 n=12
None 44% 46% 36% 42%
1 to 5 29% 29% 29% 33%
6 to 10 11% 13% 7% 8%
More than 10 16% 13% 29% 17%
*These data represent a subset of the full sample. Only those respondents who currently had a job responded to this survey question.
CHAPTER 3 — Pain Management: The Patient Experience

20
PAIN MANAGEMENT DIGEST
Fifteen percent of patients do not receive information from the prescriber, and they make use of a number of resources to gain needed information: 31% talk to the pharmacist at the drug store, 44% get written instructions from the pharma-cist, 69% read the information that comes with the prescrip-tion, 25% look online, and 31% report that they don’t need information because they have had the same drug prescribed previously and they know how to take it.
Of the full sample of patients, 38% received a prescription for an an opioid medication; 64% received the prescription from a PCP, while 35% received it from a physician special-ist, and 25% from a pain management specialist. Figure 6 shows the percentage of patients who take over-the-counter pain medicines and who have received prescriptions for 10 commonly used analgesics. The most highly prescribed agents are NSAIDs and opioid combination products. Because patients reported all medications “they have taken or are currently taking,” the percentages do not indicate whether they have taken these medications simultaneously.
Figure 6. Percentage of respondents who have taken or are currently taking these pain medications
Musculoskeletal Neuropathic Post-surgical ALL Pain Pain Pain Type of Medication N=211 n=126 n=38 n=47
Pain relievers that you can buy in the drugstore 86% 87% 84% 85%
Prescription NSAIDs 50% 50% 53% 47%
Opioid Combinations 46% 44% 47% 49%
Opioids 38% 40% 42% 30%
Steroid Injections and Spinal Injections 27% 27% 29% 23%
Anti-anxiety Medications 20% 20% 26% 15%
Selective Serotonin Reuptake Inhibitors (SSRIs) 18% 15% 32% 15%
COX-2 Inhibitor 14% 15% 13% 11%
Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs) 12% 9% 26% 11%
Tricyclic Antidepressants 8% 5% 16% 9%
Respondents were asked to select all that applied and percentages may total >100%.
Patients were asked to describe their satisfaction with their current level of pain relief and with their current healthcare providers. About a quarter of responding patients are highly satisfied with the pain relief they have achieved (ranking satisfaction at an 8, 9, or 10, on a scale of 1 to 10 with 10 as complete satisfaction). Fifty-eight percent are highly satisfied with their healthcare providers.
When asked about how many prescription pain medications they are currently taking, about a quarter of patients reported that they are not taking any prescription pain agent; 36% are taking 1 prescribed medication, 34% are taking 2 or 3, and 5% are taking 4 or more. Those levels were consistent among patients older than 60 and among patients with musculo-skeletal pain.
When asked what action they would take first if a pain medication doesn’t work well enough, 28% would call the doctor with a request for another medication; 31% would first add over-the-counter medications; 13% say they might take additional pills from their prescription.

21
As Figure 7 shows, adequacy of pain relief is a consistant con-cern, regardless of which agent is mentioned. Approximately 40% of respondents rank pain relief at the top of a 1-10 scale. The table shows that 40% or more patients are also concerned about the potential serious side effects of COX-2 inhibitors and oral opioids.
Side effects from pain medications: Almost half of these patients have experienced side effects from pain medica-tions: 46% overall and from 43% to 58% according to type of pain. (Figure 8) Few, however, had side effects serious enough to need treatment. The highest percentages of those receiving treatment by a physician or in a hospital are among patients with neuropathic pain, at 27%, and among 15% of those with post-surgical pain.
In conclusion: Findings from the patient survey are in agree-ment with fi ndings from the IOM report that a signifi cant percentage of patients with pain will continue to need pain treatment over long periods of time. The IOM predicts that the overall prevalence of pain will continue to increase in the US, primarily due to the aging of the population.6
Figure 8. Percentage of patients with side effects and percentage whose side effect was treated by a physician or required hospitalization
46%
16%
36%
11%
44%
13%
58%
27%
43%
15%
Side effects requiring hospitalization or doctor visitAll side effects
ALLN=211
>60n=104
Musculo-skeletal
Painn=126
NeuropathicPainn=38
Post-surgicalPainn=47
Figure 7. Top concerns for patients taking pain medications
COX-2 Prescription-strength Oral Combination Inhibitors NSAIDs Opioids Opioids
Concerns n=29 n=105 n=80 n=97
The cost of the medicine to me 55% 22% 25% 21%
Concern about coverage by health insurance 52% 12% 26% 19%
Concern about potential, serious side effects 48% 26% 40% 28%
Is it safe for me to take? 45% 30% 43% 31%
The medicine provides adequate pain relief 45% 37% 36% 40%
The side effects will keep me from taking it as directed by my doctor 34% 23% 26% 18%
Concern about it being habit forming 24% 15% 40% 27%
My willingness to take the medicine as directed 14% 11% 18% 13%
My ability to take the medicine as directed 14% 8% 13% 9%
On a scale of 1-10, with 1 indicating the least concern and 10 indicating the most concern, these percentages of respondents responded with an 8-10 rating.
This survey suggests that, despite concerns, patients depend on medication and other treatment interventions. Almost half (45%) are concerned about obtaining adequate relief with any of the prescription medications they take for pain, but 89% who have an active, continuing pain are taking prescribed medications.
CHAPTER 3 — Pain Management: The Patient Experience

22
PAIN MANAGEMENT DIGEST
Issues and Answers for MCOs
IntroductionIn the next 3 chapters, the Pain Management Digest reports on interviews with physicians and organization directors who have successfully addressed many of the major gaps that im-pede improvement of pain care. The editorial board directed us to these “best practices” in the hope that this information may be helpful to other organizations that are pursuing or planning their own initiatives.
Research for this monograph, however, has made it clear that there are multiple unmet needs in pain management; so many that we cannot adequately cover them in these pages. Nevertheless, we hope that the information shared by your colleagues will prompt conversation and investigation into how our healthsystem can reach 2 intertwined aspirations: the need for comparative effectiveness data that assess the real world efficacy, safety and costs of the diverse therapies for pain, and the need for action that forges broad consensus on guidelines for the treatment of pain.
Pennsylvania: Building a Foundation for Successful
Treatment of Low Back Pain
Geisinger Health System is an integrated health services organization widely recognized for its innovative use of the electronic health record (EHR), and the implementa-tion of successful care models. The system serves more than 2.6 million residents throughout 44 counties in central and northeastern Pennsylvania.
An Interview with Scott R. Taylor, BS Pharm, RPh, MBA, Executive Director, Office of Industry Relations at Geis-inger Health System in Danville, PA
Every successful initiative depends on the strength of its foundation, and this one began with building consensus and fostering collaboration across 3 key stakeholder groups: primary care physicians, employer customers, and health
plan directors. With the help of 10 nationally known pain experts, this group’s interaction is a model of planning toward a very specific goal: system-wide improvement in the treatment of low back pain. During a Pain Management Digest (PMD) interview, Dr Taylor explains how his organization rolled out a pilot program.
PMD: Geisinger has multidisciplinary pain centers within its system, why didn’t you invite them to the planning sessions?
Taylor: Pain is treated differently within specialty pain centers. The target of our low back pain program is the pain that doesn’t get referred to pain centers—the majority of pain—that which is treated in PCP offices. The decision to focus almost exclusively on PCPs is controversial, but we believe not everyone needs a pain specialist. Moreover, there aren’t enough pain specialists practicing to treat the number of patients with pain. (This is why using prescribing thresholds [eg, the opioid “high daily dose” from a guideline] as a referral trigger is problematic.) Instead, our approach has been to find out how the national experts address high opioid doses and teach PCPs what to do when patients reach these thresholds.
PMD: How do you implement a pain management program across an integrated system like Geisinger?
Taylor: To drive the program, you need people who can ap-ply the experts’ model practice plan to all types of providers. One part of the plan may work for our system pharmacists; another application may fit nurse practitioners, etc. It’s im-portant to be thinking about how to broaden the applicabil-ity of the program from the very beginning.
For example, when we started a stakeholder meeting by ask-ing, “How do we manage low back pain?” the outside experts presented the diagnostic tools and treatment algorithms they develop and test. Right away, our system providers told the academics that the tools might be excellent, but they don’t use them. Identifying this disconnect spurred conversation about how to bridge that gap.

23
Also, through our cross-stakeholder discussions, we’ve come to understand that the patient expects to leave the first appointment with something, and this “something” is not necessarily a pill. Some patients won’t be happy unless they leave with a prescription for physical therapy, or a referral for an imaging test, just something they think they need. Many patients are not satisfied if the provider says, “Rest.” So, the provider needs to figure out what the patient wants and what the patient needs—which are not always the same thing.
PMD: What do you do if the patient wants the wrong thing?
Taylor: Well, this is exactly why starting out with the right pain assessment is crucial; it helps the PCP to avoid this problem. Pain assessment is not simply a pain severity score. It also involves a mental health and functional status battery that includes a stress/anxiety/fear component, as well as the patient’s medical history. This complex assessment is what we’re training our providers to do better.
PMD: Tell us about the physician education process.
Taylor: We are using technology to create shared decision-making. During the encounter, the physician has his or her own expertise to rely on as well as electronic access to recommended guidelines. The provider is able to share this information verbally and visually with the patient so that the patient feels as though he or she has a say in the treat-ment path. Our approach keeps providers informed about guidelines and treatment options, and helps keep the patient involved with that provider and in the health system.
PMD: We know that Geisinger’s use of the electronic health record (EHR) must be part of the process, but from a topline view, what else is important in use of medical technology?
Taylor: Computer software is being used to guide provid-ers in asking questions that create a global assessment of the patient’s pain. The technology also allows different parties to be involved. The nurse, patient and provider can do part of the assessment. The software tracks the assessment, and when the provider enters his or her treatment recommenda-tion to close out the encounter, he or she can see what the expert guidelines would recommend in the same or a similar circumstance. The PCP’s treatment recommendations might match up, or not. Either way, it becomes a learning experi-ence for the physician.
Treatment of Low Back Pain Is Discordant with National Guidelines2
Using data from the National Center for Health Statistics, researchersfoundthattrendsinbackpaintreatmentstrate-gies in the US are “discordant” with current guidelines. Data wereobtainedfrom23,918outpatientvisitsatwhichthechiefsymptomorprimarydiagnosiswasbackorneckpain.
• Guideline-discordantindicators:imaging,narcotics, and referrals to physicians.
• Guideline-concordantindicators:NSAIDsor acetaminophen and referrals to physical therapy.
Years Years 1999-2000 2009-2010
Narcoticusepervisit 19.3% 29.1%
NSAIDusepervisit 36.9% 24.5%
Tomograms/MRIs 7.2% 11.3%
Physicianreferrals 6.8% 4.0%
Radiographsremainedsteadyat17%
Physicaltherapyreferralsremainedsteadyat20%
MRI=magnetic resonance images
BetweenJanuary1999andDecember2010opioidprescriptions and the use of nonguideline treatments increased,whileuseofguideline-recommendedtreat-ments decreased.
Source:CaseyDE. JAMA Intern Med.2013July29.2
Figure 1. Percentage of adults reporting pain, by selected causes, 20091
Cause of Pain US Average
Low back pain 28%Knee pain 20%Severe headache or migraine 16%Neck pain 15%Shoulder pain 9%Finger pain 8%Hip pain 7%
Source: IOM (Institute of Medicine) 2011. As adapted from Centers for Disease Control and Prevention, National Center for Health Statistics, 2009.
CHAPTER 4 — Issues and Answers for MCOs

24
PAIN MANAGEMENT DIGEST
For instance, the doctor might decide to recommend an MRI, and the guidelines might recommend physical therapy and a strength evaluation plus an anti-inflammatory agent. The provider sees this other option and now has a choice. In many cases, the provider might choose a hybrid approach and use the assessment tools to gather more information before ordering an expensive MRI.
PMD: Does every provider in the Geisinger clinic have access to this software?
Taylor: Every clinic we operate uses an EHR, but not every clinic has access to the clinical decision-support software. We pilot different interventions in 2 to 4 clinics at a time. We monitor how the new tools are working and whether they disrupt clinical flow or practice patterns. Then, we ask for physician and staff feedback. We want to make the “right thing” the easiest thing to do! If we get it right in the pilots, the sponsor may want to support the dissemination of the software or use the same methodology in every clinic. Or the clinic itself might have the resources and IT budget to support the software.
PMD: How do you know you’re on the right track?
Taylor: The market test for us is when a colleague in another state wants to do something similar and asks us how to get started. That convinces us that we’re filling a need in the marketplace, and that our underlying approach is good enough to become broadly applicable—not limited to only one patient population [low back patients].
Of course, what works at Geisinger isn’t going to work for every plan or organization. However, we are an excellent laboratory, with great clinical experts, willing patient/con-sumers and a focus on outcomes that exceed expectations and keep the cost of care below the rest of the market, this takes honest open communication among all stakeholders. Directors of managed care organizations have to continually talk about the types of programs that are being implemented elsewhere, and keep a discussion going about what is work-ing within their own organizations and what is not working. Surely, there are multiple ways to take innovative approaches to pain management. This one seems to be off to a good start among our PCPs.
New England: A Pharmacy Director-Driven Program to
Address Opioid Risk
Multiple surveys, including those in this publication, show that payers, physicians and patients are concerned about risks associated with opioids used for pain management. They worry about addiction for susceptible patients, and they worry about diversion or abuse. As one pharmacy benefit director said, “Addressing issues of overprescribing or opioid overuse is about good care. It’s not about costs, it’s the right thing to do.”
In most plans, PBM data reports are available that enable a plan pharmacy director to identify high usage of opioids. In-terventions to address overuse or inappropriate use have be-come fairly well documented, with examples in place across the country. Nevertheless, implementing focused change takes persistence, buy-in, and a good pharmacy team.
“When a chronic pain patient is using opioids at the highest daily level in the guidelines and that isn’t enough, it’s not always abuse, it is very possible that the patient has become-opioid-tolerant. The patient’s pain has stopped responding to increased dosage—it signals a need for a different approach to treatment,” explained the program director.
In fact, a first decision in implementing an opioid overuse program is to determine what threshold should be used to flag a possible opioid problem. Those thresholds vary in most states. Whatever threshold is determined, the plan then has to adopt one of many guideline formulas to calculate the individual’s morphine-equivalent dose (MED) across a range of opioid agents that may be prescribed. (Opioid Conversion Guidelines Are Variable, page 25)
This New England plan’s proposed program, like many established ones, is based on initiating case management when a pain patient is identified as having reached the highest level of safe opioid use. The directors decided that they wanted to be very clear with members and physicians that they were not trying to keep opioids from patients who needed them, and that the intervention flag is regarded as an

25
Key elements in programs that address opioid risk3
Pharmacy Lock-in
Provider Use of Validated Screening Tools
• Screener and Opioid Assessment for Patients with Pain (prior to initiation of long-term opioid therapy)
• Current Opioid Misuse Measure (monitoring patients who are being prescribed long-term use of opioids)
• Opioid Risk Tool (prior to initiation of long-term opioid therapy)
Written Adherence Agreement between Provider and Patient
• Review of potential risks
• Definitions such as “tolerance,” “dependence,” and “addiction”
• Obligations of therapy such as regular assessment and monitoring, urine drug testing, and pill counts
Urine Drug Testing
• Advise laboratories which drugs are of interest to help ensure accurate results
Adapted from McCarberg B. Postgraduate Medicine. 2011;123(2):119-130.
opportunity to engage the patient in an expert assessment process. “We would also involve the patient’s prescriber in the process. Our approach is to provide multidisciplinary support for the patient as needed and to recommend evalua-tion by appropriate providers. In some instances that provid-er may be a behavioral health or substance abuse therapist, in other cases, it may be a physiatrist, or a medical specialist.”
A major partnership supports the opioid risk program—one between the pharmacy program director and the plan’s primary care practices, especially those that are recognized as being patient-centered medical homes. “That way, all kinds of providers for that patient are on a feedback loop to the PCP.”
The program’s planners recognize that, for full, across-the-system participation in the program, the plan has to do a considerable amount of informational and educational outreach to all providers in the network, including hospitals, chiropractors, physical therapists, and psychological and behavioral health providers. “We will have to introduce the program over time, letting it continue to evolve as a truly broad, well educated team is established.” However, so that identification of patients at risk can be made as soon as possible, we will begin by moving identified patients into already established case/care management programs.”
Opioid Conversion Guidelines Are Variable4
Physiciansandpharmacistshaveexpressedahighlevelofconcernthatopioidconversionguidelinesandtablesare inconsistent,whichhinderspolicyandtreatmentdecision-making.Arecentstudygroupreviewedanumberofsuchguidelines andpresentedtheirfindingsattheAmericanPainSociety’s32ndAnnualScientificMeeting.Investigatorsagreedthat“opioidconversionguidelinesvarysubstantially”.
• Theanalysisexamined9evidence-basedpainmanagementguidelines,4nationalguidelines,and5stateguidelines.
• Researchersfoundhighvariabilityacrossguidelinesformorphine-equivalentdosedeterminations(primarilyinvariable ratiosandfixedratios)andinprovidinganequianalgesicdoseformethadone.
• Innationalguidelines,broadvariabilitywasobservedforhydromorphoneandoxycodone;however,consistencywas observedacrossstateguidelines,allofwhichfollowedtheWashingtonStateAgencyMedicalDirectors’Groupguideline.
Erensen J. McLean SA. American Pain Society 32nd Annual Scientific Meeting. Abstract 193. Presented May 9, 2013.
CHAPTER 4 — Issues and Answers for MCOs

26
PAIN MANAGEMENT DIGEST
Ohio: Building State Policies and Procedures Through Pain
Management Task Force Teams
With a goal of reducing the number of opioid-related deaths in Ohio, the state’s health plans, led by the state’s Medicaid plans and workers’ compensation agencies, have engaged in a broader effort—the establishment of a statewide initiative to support pain management provid-ers and improve patient outcomes. Today, commercial insurers are also joining the task force committees.
The Ohio task force teams quickly broadened their motiva-tional goal, realizing that payers and physicians had to first address core issues of pain management if they wanted to lower death rates. Michael Howcroft, RPh, who has been a part of the task force committee process explained, “Dur-ing task force sessions with anesthesiologists and primary care physicians, we learned that acute pain (for instance post-surgical pain) can very quickly turn into chronic pain, usually within 60 to 90 days. Once that happens, treatment is transformed, moving into the use of a full range of drug classes in order to help patients with chronic pain.
This multipharmaceutical treatment then adds an additional risk, that of serious adverse events and drug-drug interac-tions (DDIs). Consequently, we are taking a very close look at all the ways we can treat chronic pain patients.”
Task Force Team Objectives:
• Determine how to discern drug-related cause of death on death certificates
• Investigate various morphine equivalent dose (MED) guidelines
• Explore guidelines for adults with dementia and also for children with pain
• Determine educational needs of physicians who treat pain
• Engage pain specialists and PCPs
• Educate plan pharmacy and therapeutics (P&T) committees and drug utilization review (DUR) groups
“The overriding goal now is to educate plan directors, members, and providers to use the most effective approach to managing pain. We don’t want those with true pain to not be treated, but we want to use all types of therapies. We are currently trying to build consensus across all of Ohio’s health plans.”
Useful Guidelines and Literature Reviews to Support Best Practice Initiatives
• AmericanPainSociety:InterventionalTherapies,Surgery,andInterdisciplinaryRehabilitationforLowBackPain:AnEvidence-Based ClinicalPracticeGuideline.20095
• AmericanPainSociety:ClinicalGuidelinesfortheUseofChronicOpioidTherapyinChronicNoncancerPain.20096
• AmericanPainSociety:DiagnosisandTreatmentofLowBackPain:AJointClinicalPracticeGuidelinefromtheAmericanCollegeof PhysiciansandtheAmericanPainSociety.20077
• PreventingChronicPainFollowingAcutePain:RiskFactors,PreventiveStrategies,andtheirEfficacy.McGreevyK,BottrosMM,RajamSN. JohnsHopkinsUniversity.PublishedinEuropean Journal of Pain Supplement 8
• InternationalAssociationfortheStudyofPain(IASP)Pain Clinical Updates.December20129
• SpecialReport:ChronicNoncancerPain—Long-TermOpioidBenefitsandHarms.BlueCrossBlueShieldAssociationTechnical AssessmentProgram10

27
Treating Pain: Mixed Models and Modalities
IntroductionThe progression from acute pain to chronic pain has be-come a significant clinical issue in the United States, and the number of patients progressing to chronic pain continues to increase. In 2012, the American Society of Anesthesiologists Task Force on Acute Pain Management reported the follow-ing clinical consequences of inadequately controlled acute pain:1
• Longer recovery time
• Delayed ambulation and daily functioning
• High incidence of surgery-related complications
• Increased time in the intensive care unit and longer hospital lengths of stay
• Higher incidence of hospital readmissions
• Increased potential for progression from acute to chronic pain2
A retrospective study looking at the progression from acute to chronic pain found that between 10% and 50% of people who receive the most common surgical operations go on to experience chronic pain.3
In 2010, the American Hospital Association reported 10
million inpatient surgeries and 17.4 million hospital out-patient surgeries.5 There is an enormous opportunity to improve clinical response and provider practices at this point in the patient’s hospital experience.
Figure 1. Pain is the most common reason for return to the ER or readmission to the hospital after same-day surgeries4
Pain 38%
Surgical 21%
Other 17%
Medical 14%
Bleeding 4%
Adverse drug event 3%
Nausea/vomiting 3%
ER=emergency room Coley KC et al. J Clin Anesth. 2002; 14:349-353.
New Treatments, New Goals
Pain research has brought significant advances to the treatment of patients with pain but additional research is needed. Two major avenues of investigation are to clarify the mechanisms that account for differences between individuals in their pain experience and to understand the mechanisms involved in the transition from acute to chronic pain.6
One broad-based goal of recently developed treatment op-tions is to make pain medication safer. Another goal is to create entirely new options for treatment of pain. As re-searchers slowly untangle pain’s complex pathophysiology, novel therapeutic targets are emerging. This is a short summary of some expected introductions to the market.
New FormulationsSubmicron NSAIDs: New technology is being used to produce submicron particle formulations of NSAIDs. “Currently available formulations of NSAIDs are associated with significant risk for adverse events, which increases with dose and duration of use,” said Alan Gibofsky, chief investigator in Phase 3 trials. “Lower dose options that reduce the amount of medication in a patient’s bloodstream, while preserving efficacy and onset of action, may be a valuable addition for physicians.” Submicron NSAIDs are currently in Phase 3 clinical trials. The American Academy of Pain Medicine 2013 Annual Meeting. Abstract #109 and Iroko Pharmaceuticals LLC. Website, available at www.iroko.com/node/127 Accessed August 7, 2013.
Tamper-resistant opioids: Investigation continues into opioid formulations that deter patients from crushing, dissolving or ingesting too many tablets. Thus far, physical
CHAPTER 5

28
PAIN MANAGEMENT DIGEST
barriers that make pills crush-resistant are the most promis-ing approach. Crush-resistant opioids are available and have been effective at reducing abuse. Butler, S. J Pain. 2013;14(4):351-358. Cicero, T, N Engl J Med. 2013;367(2):187-189.
Adding sequestered opioid antagonists that render misused opioids inert and adding aversive components, such as niacin, are two other avenues of investigation. Some experts worry that chemical additives may cause adverse events in patients who don’t misuse or abuse opioids and may prevent legitimate dose increases.Stanos, S. Mayo Clin Proc. 2012;87(7):683-694.)
Opioid dependence: Zubsolv (buprenorphine/naloxone) was FDA approved in 2013. Similar to Suboxone, Zubsolv is a once-daily sublingual medication approved for mainte-nance and treatment of opioid dependence. Zubsolv’s menthol flavor and fast dissolve time may also encourage adherence to therapy.http://www.accessdata.fda.gov/drugsatfda_docs/label/2013/204242s000lbl.pdf. Accessed July 20, 2013.
Research Leading to Novel Therapeutic TargetsClinical trials have begun on N- and T-type calcium channel blockers that may modulate neuropathic pain signaling.Lee M. Z160: A potent and state-dependent, small molecule blocker of N-type calcium channels effective in nonclinical models of neuropathic pain, The 32nd Annual Scientific Meeting of the American Pain Society. May 8-11, 2013.
Also preclinical data suggests blocking the AC1 enzyme produced in the spinal cord and brain neurons during nerve injury may control pain. Other targets currently under in-vestigation include these: CB receptors, TRP channels, P2X receptors, and glial cells.Zhuo M. Drug Discov Today. 2012;17(11-12):573-582.) Rao, P, Mohamed T. J Pain Res. 2011; 4: 279–286.
Current Therapeutic Choices
Pharmacologic Treatments Acetaminophen COX-2 inhibitors Nonsteroidal anti-inflammatory drugs (NSAIDs) Opioids Topical agents Adjuvant medications Muscle relaxants, anticonvulsants Antidepressants and antianxiety agents
Interventional Treatments Trigger-point injections Epidural steroids Facet injections Nerve blocks Ablation techniques Intrathecal and epidural drug-delivery systems Percutaneous spinal procedures Surgical interventions
Physical Reconditioning Physical therapy Occupational therapy Vocational rehabilitation and disability management
Behavioral and Psychotherapy Behavioral therapy Psychological/psychiatric therapy Stress management Relaxation therapy Cognitive/behavioral therapy
Complementary and Alternative Methods (CAM) Acupuncture Chiropractic treatment Meditation/yoga Massage Transcutaneous electronic nerve stimulation (TENS)Source: Adapted from Turk DC, Wilson HD, Cahana A. Treatment of chronic non-cancer pain. Lancet. 2011;377(9784):2226-2235.7
Physicians currently prescribe a range of analgesic medica-tions, adjuvant medications, and interventional procedures to relieve patients’ pain. The adjuvant medications used most frequently are muscle relaxants, anticonvulsants and anti-depressants, which were originally indicated for other uses but have been proven to help specific types of chronic pain. For patients with persistent chronic pain, especially those with musculoskeletal pain, physicians often refer patients to
Multimodal Approaches: Recently released guidelines for opioid treatment of noncancer pain reiterated evidence that “chronic pain is a complex condition that may involve biological, psychological and environmental fac-tors,” and that “when pain is accompanied by comorbid-ities, impaired function, or psychological disturbances, opioid use is likely to be most effective as part of a multi-modality treatment that addresses all those domains.” 8
multidisciplinary programs. The approach to multimodal treatment of pain has gained acceptance from insurers and guideline developers.

29
Multidisciplinary and Interdisciplinary Care: A Focus on Outcomes
Among physicians who treat pain, most have come to believe that a multidisciplinary pain program (MPP) is the most successful treatment approach for patients who have chronic noncancer pain. Such programs depend on the interaction of 2 or more healthcare providers who design a treatment program that includes medical therapy, behavioral and psychotherapeutic interventions, physical reconditioning, and education.9
Several groups, including the American Pain Society (APS) and the International Association for the Study of Pain (IASP), have made efforts to define the different types of multispecialty care available to pain patients. Most groups agree that multidisciplinary care is the broadest category and describes care provided by several specialties.
Multidisciplinary care involves varying amounts of commu-nication. Providers may work in a stand-alone, multispecialist center, perhaps affiliated with a hospital or academic center, or providers may be part of a medical home clinic, a single-specialty group or an individual practice.
Multidisciplinary care may or may not be interdisciplinary. Steven Stanos, Center of Pain Management, Rehabilita-tion Institute of Chicago (RIC) writes, “Interdisciplinary, as a treatment model, includes multiple disciplines working together, usually in one facility, to facilitate communication and goal setting and to improve outcomes.”10 Interdisciplin-ary care often dovetails with integrative medicine centers that provide nutrition, supplements, yoga, meditation, massage, acupuncture, and pharmacologic treatment.
The Bravewell Collaborative defines integrative medicine as “an approach that puts the patient at the center and addresses the full range of physical, emotional, mental, social, spiritual, and environmental influences that affect a person’s health.” Notably, the Bravewell survey of
integrative medicine centers across the country, found that chronic pain is perceived to be the clinical condition able to be treated most effectively within such a model.11
The Rehabilitation Institute of Chicago Center for Pain Management
Chronic Pain Program
Another successful multi-specialty model is an interdisciplin-ary pain rehabilitation program (IPRP). Dr Stanos recently examined features unique to successful IPRPs. He explains, “IPRPs combine individual occupational therapy, pain psy-chology, relaxation therapy, counseling, vocational rehabilita-tion services, nursing education, and aerobic conditioning.”10
The Center for Pain Management (CPM) evolved from an inpatient program at RIC. Currently, “the CPM evaluates approximately 1,000 new patients per year. The payer mix includes 25%-30% workers compensation, 45%-50% com-mercial insurance, and 20% Medicare/Medicaid.10
Typically, treatment programs run 3-6 weeks. Moving pa-tients toward appropriate medication regimens and getting patients back to work are a large part of the CPM program. CPM’s success is due in part to understanding which patients it cannot treat. Patients are monitored closely, and those who don’t progress are discharged early to other, more appropriate providers.
According to the American Pain Society, establishing orga-nizational “stop-rules,” like those implemented at the RIC, are crucial to appropriate and effective interdisciplinary care. Such recommendations can protect people with chronic pain from excessive, costly, and often invasive assessments and treatments. It can also inform third-party payers regarding achievement of maximum medical improvement and closure of disability claims.12
CHAPTER 5 — Treating Pain: Mixed Models and Modalities

30
PAIN MANAGEMENT DIGEST
Establishing Coverage for Multidisciplinary Pain Programs13
Aetna has had a clinical policy bulletin for the coverage of multidisciplinary pain center treatment since 1998. It is reviewed and updated annually so that it reflects the current, evidence-supported, clinical assumptions about who benefits from this type of treatment. It also outlines the “medical necessity” pathways to coverage.
The Aetna Clinical Policy Bulletin13 on clinical pain pro-grams states, “The goal of such programs is to give patients the tools to manage and control their pain, and thereby improve their ability to function independently… Collabo-ration among therapists, psychologists, and other supportive resources is important to delivering effective pain treat-ments.”
The Aetna process is triggered by a referral from an Aetna PCP or attending physician for admission to an outpatient, multidisciplinary program. The admission is deemed “medically necessary” if the following criteria are met:
• Any surgical or acute medical treatment that is indicated has been performed
• Member has experienced chronic non-malignant pain for 6 months or more
• Member has failed conventional methods of treatment
• After a mental health evaluation, primary psychiatric conditions have been treated as indicated
• Member’s work or lifestyle has been significantly impaired due to chronic pain
• Cause of the pain is unknown or is attributable to a physical cause
This criteria list is essentially a profile of the type of patient who, according to the published literature, has been able to benefit from an outpatient, comprehensive, interdisciplinary approach to chronic, intractable pain.
There is a companion patient profile list of “contraindica-tions,” in other words, the types of psychological or behav-
ioral barriers that impair a patient’s ability to benefit from comprehensive, interdisciplinary treatment. Benefiting from such programs requires discipline, hard work, and a long-term commitment to self-care.
Also determined through current literature reviews, Aetna states that “single modality pain clinics and single disciplin-ary pain clinics are considered not medically necessary and are inappropriate for comprehensive treatment of members with chronic pain.”
Aetna’s current policy is founded on a continuing annual review of literature-based assessments of multidisciplinary pain programs for chronic noncancer pain. The primary policy development follows findings from a treatment evaluation report that was prepared for the Agency for Healthcare Research and Quality (AHRQ) and was pub-lished in 2011.9 In that review, a wide range of painful conditions were reviewed, 90% of which included chronic back pain, the most commonly treated type of pain in the United States and the leading cause of disability.14
Recommendations to Stakeholders That Will Facilitate Interdisciplinary Pain Care12
• Visionthatencompassesacommitmentto interdisciplinary care
• Communicateandinculcatethatvisionwithfacility administration,referralsources,providers,patientsbeing treated, and the community at large
• Allocationofstafftimetoorganize,implement,monitor, and modify services and programs
• Appointmentorassignmentofprofessionalandsupport stafftofacilitatecare,documentation,andquality improvementprojects
• Allocationofspaceasneededtoexpediteandencourage communication and opportunities for team interaction
• Assureappropriatespaceavailableforprovisionofcare that involves multiple providers
• Provision/creationofaninterdisciplinary(electronic) records systemTurk, D, Stanos S, et al. Interdisciplinary Pain Management. American Pain Society. 2012.

31
University of Washington Center for Pain Relief: A Large Multidisciplinary Model
In 2011, the Center for Pain Relief at University of Washington (UW), had 13,770 patient visits. Among these were 6,750 acute pain visits and 3,650 chronic pain visits. Pain patients are seen at six UW medical centers throughout the Seattle area. This multidisciplinary model includes specialists in neurology, anesthesiology, psychia-try, psychology, radiology, rehabilitation medicine, oral medicine, pharmacy, and complementary and alternative medicine (CAM). Pain, mood, and function assessment tools are used in every clinical encounter. Prescription-monitoring services include second-opinion clinics, an Emergency Department Information Exchange (EDIE), and urine drug testing.
Building on Successful Pain Management Programs
An Interview with Dennis Turk, PhD, Professor, Depart-ment of Anesthesiology Pain Medicine at the University of Washington and Director of the Center for Pain Research on Impact, Measurement & Effectiveness at UW Medicine
A major initiative under way at UW Center for Pain Relief is a web-based program that gathers provider input throughout the patient encounters as well as patient-reported informa-tion: a short patient questionnaire about pain and opioid use is completed at every visit and added to the patient’s electronic medical record. Analysis capabilities built into the system will help determine which types of patients benefit from which treatments, and UW is hopeful it will eventually help guide payers in reimbursement decisions. Dr Turk adds, “Gathering patient information together [from multiple treatment centers] creates a larger sample from which to draw on in order to answer question about treatment ef-ficacy. This assumes consistency in diagnoses and treatment protocols, which there is not, yet.” However, efforts are being made in this direction. (See page 36)
Stepped care in collaborative pain treatment: Stepped care is the foundation of UW’s approach to pain. PCPs evaluate patients and provide standard first-line therapy, including assessment of the patient’s ability for self-managed care. Dr Turk, explains, “The emphasis is on starting at a low level by giving information and reassurance, and encouraging pa-tients to be active and to self-manage their pain with gentle exercises, over-the-counter analgesics, and performance of usual activities as much as possible with gradual increases.”
If pain persists for several weeks, the patient proceeds to a more detailed treatment plan, which may include a pain spe-cialist, physical therapy, and psychological consult. Pain that continues for more than a month or six weeks requires more aggressive intervention by an interdisciplinary team. “For persistent pain, you have a critical window between 3 and 6 months to return that patient to reasonable functionality.This doesn’t mean that his or her pain is gone, but that it has improved and is tolerable. If you don’t treat at that point and
IntroductionInnovative organizations have rallied to meet the challenges inherent in pain management: opioid misuse, performing research evaluations of programs and treatments, building databases for collection of outcome measurements, identi-fying workable protocols for multimodal therapy that also recommend treatment of pain-related complications (such as opioid abuse, depression, and disability).
One thing all these programs have in common is an inte-grated, patient-centered, multidisciplinary approach to pain. Another is the use of a stepped care approach, which (sup-ported by guidelines) recommends the simplest and least expensive therapy early in the management of the pain.
Here, we present interview-based descriptions of well- known successes, and of a few lesser known successes that can be replicated by determined innovators in their own organizations.
CHAPTER 6

32
PAIN MANAGEMENT DIGEST
address functionality then, you’re on your way to a long-term significant pain problem with a high level of disability,” says Dr Turk.
Telehealth: Not all patients have access to multidisciplinary pain centers. UW’s Telehealth is a regional telemedicine program for pain treatment that is based on the University of New Mexico Health Sciences Center Project Extension for Community Health Care Outcomes (ECHO). Project ECHO and the UW Department of Pain Medicine cover five states including Washington, Wyoming, Alaska, Montana, and Idaho. Local providers consult with UW specialists via web-based videoconferencing.
For community providers outside the UW system, the university developed the web-based Pain Medicine Pro-vider Toolkit, which includes opioid prescribing guidelines, patient assessment tools and handouts, UW referral infor-mation, and information on opioid legislation. The site also offers CME opportunities for pain-care education, pain-related publications, and journal articles. (see: http://depts.washington.edu/anesth/education/pain/index.shtml.)
Washington: Addressing Opioid Risk
Today, the risk of opioid abuse and misuse is a well-known problem. The US Food and Drug Administration (FDA) requires manufacturers to develop and submit a risk evaluation and mitigation strategy (REMS) for long-acting and sustained-release opioids. Legislation to reduce opioid abuse is in place in most states. Washington (WA) has perhaps the most far-reaching legislation directed at opioid prescribing, and its corresponding treatment guide-lines have become the model for other states.
Opioid prescribing legislation in WA was spurred by the doubling of opioid-related deaths between 2004 and 20071, and by rising costs, including criminal justice expenses, which reached $55.7 billion nationally.2 In 2007, the Washington State Agency Medical Directors’ Group (AMDG), a coalition representing all the state’s public payers, developed an opioid prescribing guideline that included the first established dosing threshold recommenda-
tion and a web-based calculator for determining a patient’s total daily morphine-equivalent dosing (MED) level.3
A review of workers’ compensation data before and after the AMDG recommendations shows a 35% decrease in the proportion of people taking more than 120mg/day MED, and a 50% decrease in opioid-related deaths from 2010 to 2012.4 In 2010, WA passed legislation requiring providers to adhere to the AMDG dosing guideline. Dr Turk notes, “This change has been very helpful and the downward trend is continuing.” The law, he notes, “does not prohibit prescrib-ing high doses of opioids, but says providers should consult with a specialist if they are considering prescribing more than 120mg MED for patients who are not improving in pain and function. Providers might consult with a specialist and decide to go forward with a higher opioid dosage.”
Long-term opioid safety: Dr Turk points to a lack of long-term efficacy and safety data on opioid use and a growing body of research that suggests opioids may have risks beyond abuse and addiction. He says, “We’re just starting to learn about the effects of long-term opioid use on hormones and we’re seeing more reports on opioid-induced hyperalgesia: some patients feel less pain as they come off opioids; the longer you take opioids, the more you require those types of medications.” Interdisciplinary Pain Rehabilitation Pro-grams frequently make reducing or stopping opioid use a priority. In many instances this means switching patients to a more appropriate medication, rather than eliminating the need for pharmacologic therapy.
Key Elements of the Washington State AMDG Opioid Dosing Guideline3
• Initiatingandtransitioningopioidtherapy
• Assessingandmonitoringchronicopioidtherapythrough outcomes assessment and prescription monitoring
• Taperinganddiscontinuingopioidtherapy
• “YellowFlag”warningdoseof120-mgmorphine equivalentdose(MED).Whenthisdoseisreached, consultation with a pain specialist is recommended if the patienthasnotexperiencedsubstantialimprovement basedonvalidatedpatient-reportedoutcometools**AMDG recommends the Opioid Risk Tool, PHQ-9 to screen for depression severity, CAGE-AID to screen for alcohol or drug problems, and Two-item Graded Chronic Pain
Building on Successful Pain Man-
agement Programs

33
Missouri: A Medical Home Model Provides Comprehensive Pain
Management for a Large Medicaid and Uninsured Population
The patient-centered medical home model evolved in tandem with a growing awareness that, in the US, pri-mary care practices play a pivotal role in prevention and management of chronic illness. For Karl Haake, MD, an anesthesiologist, this view of a comprehensive, team-based approach seemed to be the obvious key to providing effective pain treatment to the Medicaid and uninsured patients that were being treated in a federally qualified health center (FQHC) in central Missouri (MO).
An Interview with Karl Haake, MD, Pain Clinic Director at the Community Health Center of Central Missouri in Jefferson City.
Dr Haake, who was an interventional pain specialist in a private practice, began his clinic work after recognizing that underinsured patients were resorting to emergency room (ER) visits for pain treatment. Dr Haake approached Joseph E. Pierle, MPA, the CEO of the Missouri Primary Care As-sociation (MPCA), which represents the state’s community health centers in providing a better option for these patients. Together the two established a comprehensive pain man-agement program within the Community Health Center of Central Missouri (CHCCMO). CHCCMO is actually a group of 4 clinics that serve the mostly rural communi-ties of central Missouri. The pain program operates in the Jefferson City clinic and is directed by Dr Haake. His efforts there have earned him a 2012 Recognition Award from the National Committee for Quality Assurance (NCQA) Back Pain Recognition Program.
Building a regional pain management program: Cur-rently, Dr Haake sees 50 to 60 patients a week at various locations across Missouri. In addition to pain specialist care, nurse visits, and behavioral health visits with a psychologist or licensed social worker are part of the pain program. Fol-lowing the medical home model, other team provider visits are scheduled the same day as the clinician visits. The clinic
also provides dental and pediatric care. Dr Haake notes, “Offering pain care had an added benefit: the clinic has started seeing more patients for other primary care services as well.”
Initially, new patients were referred to CHCCMO’s pain program by their local ERs. “We visited ERs around the area and said, ‘if you have patients who keep coming in for pain, send them to us and we will keep treating them so they can stop going to the ER,” explains Dr Haake. “By word of mouth, what we were doing spread among community health centers. PCP private practices also began sending Medicaid or uninsured patients with pain to us.”
This grass-roots approach extends to educating community physicians about comprehensive pain management. “Refer-rals allow us to help the patients and let PCPs know if they are on the right track,” says Dr Haake, “If they’re not, we can tell them what we would recommend.”
Educational outreach: Dr Haake holds conferences for phy-sicians within the FQHC system and makes site visits to dis-cuss pain treatment strategies with providers and office staff. Dr Haake says, “The entire staff needs to know what the patient’s expectation should be, what is good medicine, what is safe medicine. It’s a problem when a patient calls for refills and gets a sympathetic ear from the secretary but comes into the clinic and gets a different message from the nurse or doc-tor. We found that a single-message approach removed a lot of the frustrations common to pain management.”
Treatment Assessment at CHCCMOAnelectronicmedicalrecordtrackspainscores,theOswes-trydisabilityindex(whichisadministeredateveryvisit),andfunctionalitychanges:“Arepatientsexercisingmore,improv-ing their diet, stopping smoking, and taking more interest in their overall health?”
CHCCMOiscollaboratingwiththeDepartmentofMentalHealthandtheStateofMOtodeterminethebestwaytousethedataithascollected.Additionally,saysDrHaake,“Weareworking with the state Medicaid director to pull claims data. Anecdotally,we’veseenareductioninopioidprescriptions,andweareinterestedinseeingiftherehasbeenareductioninERvisits,injections,andsurgeries.”
Building on Successful Pain Man-
agement Programs
CHAPTER 6 — Building on Successful Pain Management Programs

34
PAIN MANAGEMENT DIGEST
Clinic-wide, nurses are trained to know who the pain pa-tients are. System-wide, the pain clinic is working with PCPs to identify those patients with acute pain who would benefit from early consultation with a pain specialist. Dr Haake ex-plains, “The disproportionate share of mental health comor-bidities among the Medicaid population puts these patients at risk for all kinds of medical problems, especially with opioid use. We are tying to get our PCPs to recognize these patients and understand that if ibuprofen, acetaminophen, and ice are not working, they probably should not prescribe an opioid, but should refer them to pain specialist so the specialist can figure out why pain is lingering and what other issues might be going on.”
A successful model spreads: Medicaid and uninsured patients from across the state have been visiting the Jefferson City pain clinic, so Dr Haake and the MPCA are expand-ing the program to other health centers, including one in St. Joseph, MO, that has partnered with its local hospital. Earlier this year, a secondary site was established in Wentz-ville, MO, just outside of St. Louis. Next, the pain program will be used in an urban setting for the first time, in Kansas City. Dr Haake says, “MPCA has been at the forefront of various strategies to improve the medical home model and provide better patient care. What we have done in Missouri is very unique and as far as we know we’re the first to deliver comprehensive pain management in an FQHC setting.”
California and Oregon: Evaluating Regional Pain Management Programs
To implement its pain management program, Kaiser Permanente relied on regional resources already in place. Bill McCarberg, MD, one of the founders of the Kaiser initiative, explains, “The regional pain centers grew organically from the expertise and therapy focus of the physicians in that region. Kaiser was open to building on strengths rather than forcing a common, centralized model.”
An Interview with Bill McCarberg, MD, Kaiser Permanente, San Diego (retired) Adjunct Assistant Clinical Professor University of California San Diego.
Kaiser Permanente began to look at the establishment of pain management centers by surveying its practitioners and administrators, reviewing the available literature, and inter-viewing healthcare leaders throughout the US. Guidelines from the American Pain Society and the Agency for Health Care Policy and Research were also reviewed and incorporat-ed into an integrated model of pain management with varied regional focuses. Dr McCarberg explains, “Each medical cen-ter has a different method of dealing with pain. For example, my pain treatment program in San Diego developed along-side an already strong cognitive behavioral program, whereas the Fontanna, CA, pain program focuses on an opioid abuse program because addiction specialists were already in place.”
Despite varied provider specialists, all Kaiser’s pain programs offer the core components of an interdisciplinary program: provider education, interdisciplinary teams in the primary care setting, group counseling and self-management classes, case management, and methods to evaluate outcomes. An electron-ic medical record allows data collection and provides continu-ity across patient visits to specialists, PCPs, and multidisci-plinary pain clinics, which are established in each of Kaisers’ primary care service areas. Kaiser lists 15 pain management clinics in northern California and 12 in southern California.
Kaiser assesses program efficacy: Northwest Permanente (KPNW) covers Oregon and Southern Washington and has been evaluating the efficacy of its pain management programs there since its inception in 1996. Initially KPNW tracked up to 18 pain patient variables, but after 5 years of research, data showed that only six variables were sensitive enough to measure quality. Pared-down data collection now includes these outcome measures:
• Pain score at patient encounters
• Sleep interference
• Patient satisfaction with pain management efforts and treatment effects
• Number of outpatient visits
• Number of pharmacy prescriptions filled
To compare populations from different regions, KPNW stratifies pain patients into a three-tiered system based on pain level, functionality, prescription utilization, and depression/anxiety diagnoses.

35
Program Efficacy Results5
• AnalysisoftheKPNWprogram’sfirst5yearsshowed costspergroupperhourwerehigherinstart-up programsbecauseoftraining,butovertime,cost droppedfrom$308pergroupperhourin1996to$38 pergroupperhourin2001.
• Casemanagementandgroupvisitswithaninterdis- ciplinary team within the primary care setting (physician, nurse, social worker, pharmacist, and physical therapist) reducedthenumberofpatientsreferredtospecialists and multidisciplinary care centers that provide a higher level of interventional treatments and higher cost therapies.
• InSalem,Oregon,between1997(whentheprogram wasimplemented)and1998,ERvisitsforchronicpain werereducedby43%.(Kaiserdiscoveredthattracking ERvisitsisareliablemeasureformemberswithaccess toonlyonehospital,butnotifmemberscanaccess multipleERs).
Common Elements of Successful MCO Pain Man-agement Programs
• Electronic Medical Records
• Multidisciplinary or interdisciplinary care
• Case managers
• Provider education and collaboration with pain specialists
• Evaluation of programs (common criteria include ER vis-its, surgeries, hospitalizations, and/or opioid utilization)
• Measureable goals gathered from patient self-reporting, medical history, and a physical examination
• Regular patient satisfaction measurement
Less common elements, but used by the most highly developed programs
• Multidisciplinary pain center(s) for interventional therapy and integrated, more aggressive care for the most severe patients
• Opioid prescribing guidelines that require referral to a pain specialist
• Complementary and alternative medicine
• Integrated data collection and review of methodologies to evaluate programs
• Claims data review to identify points of intervention
Improving Clinical Trial Design and Interpretation
Evaluating the efficacy of pain therapies is complicated by more than inconsistent diagnoses and treatment protocols. Pain is now understood to be a biopsychosocial condi-tion that requires a multimodal approach. This means that each patient’s pain is different and must be treated individually. How to collect and produce meaningful data within this multifaceted therapeutic area has been the mission of the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT), now operating as the Analgesic, Anesthetic, and Addiction Clinical Trial Translations, Innovations, Opportunities, and Networks (ACTTION) in a public-private partner-ship with the FDA.
An Interview with Dennis Turk, PhD
There are multiple ways to approach the evaluation of pain medications and related therapies. Dr Turk, co-chair of IMMPACT and co-director of the Executive Committee for ACTTION, explains, “One particular therapy is not going to help 100% of patients. In general, you could estimate that somewhere between 40%-50% of patients would have about a 30% improvement in pain from one particular therapy.6 Moreover, statistical significance, clinical meaningfulness, and cost effectiveness are not the same things.”
Rather than looking at efficacy on a patient-by-patient basis, Dr Turk and his colleagues recommend looking at the relative cost-effectiveness of drug therapy. Dr Turk adds, “The ques-tion to determine efficacy and coverage policies should not be, ‘does a treatment have a beneficial effect?’ but rather, does the treatment have a positive outcome compared to what the alternatives are, on what outcomes, and at what cost?’ One expensive therapy used now might be cost-effective if the alternative is not using it and risking intervention with even more costly therapies down the line.”
As an example, he continued, “We could ask how much a payer spent on a patient in the year prior to pain rehabilita-tion, how much did rehabilitation cost, and how much did the payer spend in the year after rehabilitation.” While at the University of Pittsburgh, Dr Turk and his colleagues there found they needed to see a significant outcome in only about
CHAPTER 6 — Building on Successful Pain Management Programs

36
PAIN MANAGEMENT DIGEST
1 in 10 patients to make a therapy cost effective when it was compared to more expensive alternatives.
A Taxonomy of PainThe ACTTION group has also recently partnered with the American Pain Society (APS) to develop an evidence-based taxonomy of pain. Begun in 2013, Dr Turk estimates the project will take 2 to 3 years to complete.
The absence of standardized diagnostic criteria—a taxono-my—complicates clinical research, contributes to inconsis-tent treatment guidelines, and raises multiple coding issues that hamper a plan’s data collection. Dr Turk explains, “In a 2-month period at our University of Washington pain center there were 485 different diagnoses given for people coming in with pain problems. Now that can’t really be possible but
it’s what happens because of overlapping classifications and terminologies.”
Dr Turk says, “We just started the process of developing a classification for chronic pain, and we will eventually go on to acute pain. Coming up with standardized ways of diag-nosing and assessing pain and trying to make suggestions about what we know about the underlying mechanism of pain will take time.”
The World Health Organization (WHO) is also address-ing taxonomy. WHO is releasing its updated International Classification of Disease (ICD-11) in 2015 and has asked the International Association for the Study of Pain (IASP) to contribute a chapter on pain. Developing appropriate chronic pain ICD-11 codes is their first priority.8
IMMPACT Research7
Overthelastdecade,IMMPACTcollaborationsandanalyseshave resulted in numerous studies advancing clinical trial designinterpretation.Someexamplesinclude:• Developingoutcomemeasuresforpainclinicaltrials: IMMPACTrecommendations.Pain.2006;125:208-215. (Turk DC, Dworkin RH, et al.) • Interpretingtheclinicalimportanceofgroupdifferencesin chronicpainclinicaltrials:IMMPACTrecommendations. Pain. 2009;146:238-244.(DworkinRH,TurkDC,etal.)• Researchdesignconsiderationsforconfirmatorychronic painclinicaltrials:IMMPACTrecommendations.Pain. 2010;149:177-193.(DworkinRH,TurkDC,etal.)• Coreoutcomemeasuresforopioidabuseliabilitylabora- toryassessmentstudies:IMMPACTrecommendations. Pain. 2012;153:2315-2324.(ComerSD,ZacnyJP,etal.)• Systematicreviewofthepsychometricproperties,interpret- abilityandfeasibilityofself-reportpainintensitymeasures for use in clinical trials in children and adolescents. Pain. 2006;125:143-157.(StinsonJN,KavanaghT,etal.)• Developmentandinitialvalidationofanexpandedandrevised versionoftheShort-formMcGillPainQuestionnaire(SF- MPQ-2). Pain.2009;144:35-42.(DworkinRH,TurkDC,etal.)• Outcomemeasuresinplacebo-controlledtrialsofosteo- arthritis:responsivenesstotreatmenteffectsintheREPORT database.OsteoarthritisandCartilage,2011;19:483-492. (DworkinRH,Peirce-SandnerS,etal.)
Foraccessto10yearsofIMMPACTresearchandrecom-mendations,includingalistofupcomingpublications,see:http://www.immpact.org/publications.html.
An MCO Call to ActionPain is expected to remain a major issue in the United States as the population ages and as long as pain continues to be an undertreated condition. While those situations could drive the healthcare system deeper into the maze of high costs and compromised health, multiple developments described in these pages are positive. Data and interviews lead us to believe that industry stakeholders can make an important difference in how pain is managed and that many have already mounted practical, successful programs.
It is also promising that, despite continued inconsistency across morphine equivalent dose recommendations, treatment guidelines seem to be in agreement as to goals of therapy, management of risk, importance of treating acute pain to resolution, and use of a stepped care approach for chronic pain. And soon, physicians and patients may have more treat-ment options because government reports (such as the IOM) are calling for increased funding for research into mechanisms of pain and new medications to address those mechanisms.
A final hopeful sign is that MCO survey respondents indi-cated an interest in collaborations with physicians, pharma-cists, and covered members to address risks and to make effective treatment available to all who need it. We hope this digest sparks a dialogue among those who have the power to make changes in the system and in the management of pain.

37
AppendixA Review of Key Regulatory Directives for Use of
Commonly Prescribed Pain Medications
Acetaminophen (prescription-strength)1
Acetaminophen is widely and effectively used in both pre-scription and over-the-counter (OTC) products to reduce pain and fever. It is one of the most commonly used drugs in the US. Examples of prescription products that contain acetaminophen include hydrocodone with acetaminophen (Vicodin, Lortab), and oxycodone with acetaminophen (Tylox, Percocet).
The Food and Drug Administration (FDA) is asking drug manufacturers to limit the strength of acetaminophen in prescription drug products, which are predominantly combi-nations of acetaminophen and opioids. This action will limit the amount of acetaminophen in these products to 325 mg per tablet, capsule, or other dosage unit, making these prod-ucts safer for patients. The total number of tablets or capsules that may be prescribed and the time intervals at which they may be prescribed will not change as a result of the lower amount of acetaminophen.
In addition, a Boxed Warning highlighting the potential for severe liver injury and a Warning highlighting the potential for allergic reactions (eg, swelling of the face, mouth, and throat, difficulty breathing, itching, or rash) are being added to the label of all prescription drug products that contain
acetaminophen. The directives do not affect over-the-counter (OTC) acetaminophen.
• The FDA maintains that products containing acetamino-phen have a warning statement in labeling regarding liver damage, which includes a maximum daily dosage of 4,000 mg, noting that some manufacturers of generic or branded agents that are sold without prescription (OTC) already voluntarily limit daily doses to below that level.
Non steroidal anti-inflammatory drugs (NSAIDs) Safety and tolerability are key factors in choice of analgesics. Even with their established clinical efficacy in pain manage-ment and importance in patient care, nonsteroidal anti-inflammatory drugs (NSAIDs) have the potential to cause serious gastrointestinal (GI), cardiovascular (CV), and renal adverse events (AEs).2-4
An overwhelming consensus from various regulatory and medical organizations recommends the use of the lowest effective dose of NSAIDs for the shortest duration of time to minimize the risk of serious AEs and to be consistent with individual treatment goals.5-13 Regulatory post-marketing directives include those shown in Figure 1, and focus on using the lowest dose possible to meet treatment goals, especially when beginning therapy.
*NICE recommendation with respect to use of NSAIDs in osteoarthritis.EMA=European Medicines Agency. FDA=United States Food and Drug Administration. NICE=National Institute for Health and Clinical Excellence.
Figure 1. Regulatory Agency Guidance
FDA NICE* EMA Health Canada
“Use of the lowest effective dose for the shortest duration consistent with the individual patient treatment goals.”5
“Oral NSAIDs/COX-2 inhibitors should be used at the lowest effective dose for the shortest possible period of time.”6
“All patients should take the lowest effective dose of non-selective NSAIDs for the shortest time necessary to control symptoms.”7
“To minimize the potential risk for an adverse event, the lowest effective dose should be used for the shortest possible duration.”8

38
PAIN MANAGEMENT DIGEST
Figure 2 shows summarized recommendations from five important medical society guidelines for the treatment of pain: Osteoarthritis Research Society International (OARSI), American Heart Association (AHA), American Gastroenterological Association (AGA), American College of Rheumatology (ACR), and American Geriatrics Society (AGS).9-13
Opioids and Opioid Combinations14
In September of 2013, the FDA announced class-wide safety labeling changes and new post-marketing study requirements for all extended-release and long-acting (ER/LA) opioid analgesics intended to treat pain.
The stated reason for the changes was “to reduce the serious risks of long-acting and extended-release opioids while still seeking to preserve appropriate access for those patients who rely on these medications to manage their pain.”
The updated indication states that ER/LA opioids are indi-cated for the management of pain severe enough to require daily, around-the-clock, long-term opioid treatment and for which alternative treatment options are inadequate.
Figure 2. Guidance from Medical Associations
AGA ACR OARSI AGS
“GI risks may be decreased through similar attention to risk factors and use of co-therapy. Risk can be reduced through the use of the lowest effective dose for the shortest duration of time.”9
“If a patient and provider agree to utilize an NSAID…then the lowest effective dose of the least expensive agent should be con-sidered first line.”10
“Non-steroidal anti-inflammatory drugs (NSAIDs) should be used at the lowest effective dose but their long-term use should be avoided if possible.”11
“…dosing for most patients requires initiation with low doses followed by care-ful upward titration, including frequent reassessment for dosage adjustments and optimum pain relief and for adverse effects.”12
AHA
“…it may be reason-able to consider an NSAID…however this should be coupled with the realization that effective pain relief may come at the cost of a small but real increase in risk for cardiovascu-lar or cerebrovascular complications.”13
ACR=American College of Rheumatology; AGA=American Gastroenterological Association;AGS=American Geriatrics Society; AHA=American Heart Association; OARSI=Osteoarthritis Research Society International.
The updated indication further clarifies that, because of the risks of addiction, abuse, and misuse, even at recommended doses, and because of the greater risks of overdose and death, these drugs should be reserved for use in patients for whom alternative treatment options (e.g., non-opioid analgesics or immediate-release opioids) are ineffective, not tolerated, or would be otherwise inadequate to provide sufficient manage-ment of pain; ER/LA opioid analgesics are not indicated for as-needed pain relief.
The FDA is also requiring a new boxed warning on ER/LA opioid analgesics to caution that chronic maternal use of these products during pregnancy can result in neonatal opioid withdrawal syndrome (NOWS). In addition, the FDA is notifying ER/LA opioid analgesic application hold-ers of the need for changes to the following sections of drug labeling: Dosage and Administration; Warnings and Precau-tions; Drug Interactions; Use in Specific Populations; Patient Counseling Information, and the Medication Guide.
Once the safety labeling changes are finalized, modifications will also be made to the ER/LA Opioid Analgesics Risk Evaluation and Mitigation Strategy (REMS), to reflect the updated information.

39
Figure 3 summarizes the benefits, risks and clinical issues that are reflected in FDA reports and directives related to use of the 3 medicines most often used to treat pain.
Figure 3. Features of commonly used analgesics
Acetaminophen
Analgesic Benefit Risk
• Used to treat mild-to-moderate pain15
• In recommended dosages, it can be a helpful adjunctive therapy and avoids the GI, CV and renal toxicities associated with NSAIDs16
• Acetaminophen-related liver injury is a leading cause of acute liver failure.17
In 2007, a Centers for Disease Control and Prevention (CDC) population-based report estimates that annually there are 1,600 cases of all-cause acute liver failure, of which the majority are attributed to acetaminophen use.17
In 2011, FDA issued a safety communication limiting the amount of acetaminophen in prescription products to 325 mg per dosage unit. FDA maintains that the maximum adult daily dose of acetaminophen OTC products should not exceed 4,000 mg.18
• Although tolerance to opioids may occur over time, some adverse effect (ie, central nervous system or respiratory depression, leading to death) limit their use.19
• In 2010, 16,651 overdose deaths were attributed to opioid analgesics – a four-fold increase from the number of overdose-related deaths reported in 1999. About 3 out of 4 pharmaceutical overdose deaths in 2010 were associated with an opioid analgesic such as oxycodone, hydrocodone and methadone.20
• Patients taking opioids are at risk for developing tolerance, physical dependence, opioid-induced hyperalgesia, allodynia and addiction which may ultimately lead to opioid abuse.19
• Although NSAIDS may help alleviate pain, their use is associated with a dose-dependent risk of serious AEs2-4:
– Upper GI complications – CV events – Acute renal failure (ARF)
Opioids Often prescribed to manage moderate-to-severe pain15
NSAIDs A popular pharmacologic option among general practitioners for the treatment of mild-to-moderate pain and are typically a first-line choice for acute pain15
APPENDIX

40
PAIN MANAGEMENT DIGEST
ReferencesIntroduction Issues and Answers in Pain Management1. Stanos, S. Summary of the Managed Care Work Group on Pain Management. http://www.managedcarecme.com. Accessed August 6, 2013.2. IOM (Institute of Medicine). 2011. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Washington, DC: The National Academies Press.3. American Society of Anesthesiologists Task Force on Acute Pain Management. Practice guidelines for acute pain management in the perioperative setting. Anesthesiology. 2012;116(2):248-273.4. Stewart WF, Ricci JA. Chee E, Morganstein D, Lipton R. Lost productive time and cost due to common pain conditions in the US workforce. JAMA. 2003; 290:2443-2454.5. Sinatra R. Causes and consequences of inadequate management of acute pain. Pain Med. 2010;12:1859-1871.6. National Center for Health Statistics. Health, United States, 2006. With Chartbook on Trends in the Health of Americans. Hyattsville, MD. 2006.7. Dubois M, Gallagher RM, Lippe P. Pain medicine position paper. Pain Med. 2009;10(6):972-1000.8. Massachusetts Pain Initiative Pain Survey. Executive Summary. 2010. http://www.masspaininitiative.org/files/MassPI%20Pain%20Survey%20-%20Executive%20Summary%20v3.pdf. Accessed Spetember 6, 2013.9. American Society of Anesthesiologists Task Force on Chronic Pain Manage-ment and the American Society of Regional Anesthesia and Pain Medicine. Prac-tice Guidelines for Chronic Pain Management. Anesthesiology. 2010;112:1-1.10. Gatchel RJ, Okifuji A. Evidence-based scientific data documenting the treatment and cost-effectiveness of comprehensive pain programs for chronic nonmalignant pain. J Pain. 2006;13(8):715-724.11. Sessle, BJ. The pain crisis: What it is and what can be done. Pain Research and Treatment. 2012, Article ID 703947. doi:10.1155/2012/703947. 12. American Chronic Pain Association (ACPA). ACPA resource guide to chronic pain medication and treatment. 2013. http://www.theacpa.org/uploads/ACPA_Resource_Guide_2013_Final_ 011313.pdf. Accessed August 18, 2013.13. Chou R, Fanciullo GJ, Fine PG, et al. Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain. J Pain. 2009;10(2):113-130.14. Agency Medical Directors’ Group. Interagency guideline on opioid dosing for chronic non-cancer pain. 2010. http://www.agencymeddirectors.wa.gov/ opioiddosing.asp. Accessed August 6, 2013.
Chapter 1 Medical and Pharmacy Director Perspectives on Pain Management1. ACPA resource guide to chronic pain medication and treatment. 2013. 2. Loeser J, Cahana A. Pain medicine versus pain management: ethical dilemmas created by contemporary medicine and business. Clin J Pain. 2013;29:311-316.3. IOM (Institute of Medicine). 2011. Relieving Pain in America.4. Federal Drug Administration. Postmarketing Drug Safety Information. http://www.fda.gov/downloads/Drugs/DrugSafety/PostmarketDrugSafetyInforma-tionforPatientsandProviders/UCM106241.pdf. Accessed August 21, 2013.
Chapter 2 Practices in Pain Treatment and Management: A Physician Survey1. Dubois M, Gallagher RM, Lippe P. Pain Med. 2009;10(6):972-1000.2. IOM (Institute of Medicine). 2011. Relieving Pain in America.3. Breuer B, Cruciani R, Portenoy RK. Pain management by primary care physicians, pain physicians, chiropractors, and acupuncturists: a national survey. South Med J. 2010;103(8):738-47.
4. ACPA resource guide to chronic pain medication and treatment. 2013.
Chapter 3 Pain Management: The Patient Experience1. American Pain Foundation. Voices of chronic pain survey. 2006.2. Reid MC, Bennett DA, Chang WG, et al. Improving the pharmacologic management of pain in older adults: identifying the research gaps and methods to address them. Pain Med. 2011;12(9):1336-1357.3. National Center for Health Statistics. Health, United States, 2006. 4. American Geriatrics Society Panel on Pharmacological Management of Persistent Pain in Older Persons. Pharmacological management of persistent pain in older persons. J Am Geriatr Soc. 2009.5. Tauben D. International Association for the Study of Pain (IASP). 2012. Chronic pain management: measurement-based step care solutions. Pain: Clinical Updates. 2012; 20(8). http://www.iasp-pain.org/AM/AMTemplate.cfm?Section=Pain_Clinical_Updates1&Template=/CM/ContentDisplay.cfm&ContentFileID=3229. Accessed September 5, 2013.6. IOM (Institute of Medicine). 2011. Relieving Pain in America.
Chapter 4 Issues and Answers for MCOs1. IOM (Institute of Medicine). 2011. Relieving Pain in America.2. Casey DE Jr. Why don’t physicians (and patients) consistently follow clinical practice guidelines? Comment on “worsening trends in the management and treatment of back pain.” JAMA Intern Med. 2013;July 29. doi:10.1001/jamainternmed.2013.76723. McCarberg B. Pain management in primary care: Strategies to mitigate opioid misuse, abuse, and diversion. Post Graduate Medicine. 2011;123(2):119-130.4. Erensen J, et al. American Pain Society (APS) 32nd Annual Scientific Meeting. Abstract 193. Presented May 9, 2013.5. Chou R, Loeser J, Owens DK, et al. Interventional therapies, surgery, and interdisciplinary rehabilitation for low back pain: an evidence-based clinical practice guideline from the American Pain Society. Spine (Phila Pa 1976). 2009 May 1;34(10):1066-1077.6. Chou R, Fanciullo GJ, Fine PG, et al. J Pain. 2009;10(2):113-130.7. Chou R, Qaseem A, Snow V, et al. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007 Oct 2;147(7):478-91.8. McGreevy K, Bottros MM, Rajam SN. Preventing chronic pain following acute pain: risk factors, preventive strategies, and their efficacy. Eur J Pain Suppl. 2011;5(2):365-372.9. Tauben D. IASP. Pain: Clinical Updates. 2012; 20(8). 10. Yang Y. Blue Cross and Blue Shield Association. Special report: Chronic noncancer pain—long-term opioid benefits and harms. Technol Eval Cent Assess Program Exec Summ. 2012 Oct;27(1). http://www.bcbs.com/blueresources/tec/vols/27/27_01.pdf. Accessed September 6, 2013.
Chapter 5 Treating Pain: Mixed Models and Modalities1. American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology. 2012;116(2):248-273.2. IOM (Institute of Medicine). 2011. Relieving Pain in America.3. Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet. 2006 May 13;367(9522):1618-25.4. Coley KC, Williams BA, DaPos SV, Chen C, Smith RB. Retrospective evalua-tion of unanticipated admissions and readmissions after same day surgery and associated costs. J Clin Anesth. 2002;14(5):349-353.

5. Trendwatch Chartbook 2013. Avalere Health. American Hospital Association Annual Survey Data, 2011, for community hospitals. US Census Bureau: National and State Population Estimates. July 1, 2011. http://www.aha.org/research/reports/tw/chartbook/ch3.shtml. Accessed August 16, 2013.6. Sessle, BJ. 2012, Article ID 703947. doi:10.1155/2012/703947.7. Turk DC, Wilson HD, Cahana A. Treatment of chronic non-cancer pain. Lancet. 2011;377 (9784):2226-2235.8. Chou R, Fanciullo, Fine PG, et al. J Pain. 2009;10(2):113-130. 9. Agency for Healthcare Research and Quality (AHRQ) Technical Brief Number 8. Multidisciplinary pain programs for chronic non-cancer pain. 2011. 10. Stanos S. Focused review of interdisciplinary pain rehabilitation programs for chronic pain management. Curr Pain Headache Rep. 2012;16:147-152.11. Horrigan B, Lewis S, Abrams D, Pechura C. Integrative Medicine in America. How Integrative Medicine is Being Practiced in Clinical Centers Across the United States. The Bravewell Collaborative. February 2012. 12. Turk D, Stanos S, et al. Interdisciplinary pain management. American Pain Society. http://www.americanpainsociety.org/uploads/pdfs/2010%20Interdisci-plinary%20White%20Paper-FINAL.pdf. Accessed August 6, 2012.13. Aetna Clinical Policy Bulletin: Chronic Pain Programs (Last review 5/10/13). http://www.aetna.com/cpb/medical/data/200_299/0237.html. Accessed August 6, 2013.14. National Center for Health Statistics. Health, United States, 2006.
Chapter 6 Building on Pain Management Programs1. Centers for Disease Control and Prevention. Overdose deaths involving prescription opioids among Medicaid enrollees-Washington, 2004-2007. MMWR. 2009;58(42):1171-1175. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5842a1.htm. Accessed August 6, 2013.2. Cahana A, Dansie EJ, Theodore BR, Wilson HD, Turk DC. Redesigning delivery of opioids to optimize pain management, improve outcomes, and contain costs. Pain Med. 2013;14:36-42. 3. Agency Medical Directors’ Group. Interagency guideline on opioid dosing for chronic non-cancer pain. 2010. 4. Franklin GM, Mai J, Turner J, et al. Bending the prescription opioid dosing and mortality curve: Impact of the Washington State opioid dosing guideline. Am J Ind Med. 2012;55:325–331. 5. Donovan M, Jacobs PO, Blake, M. KPNW integrated pain management program. The Permanente Journal. 2002;6(2):24-34.6. Turk DC, Wilson HD, Cahana A. Lancet. 2011;377:2226-2235.7. IMMPACT Consensus Recommendations. http://www.immpact.org/ publications.html. Accessed August 6, 2013.8. International Association for the Study of Pain (IASP). IASP e-newsletter. August 2013. http://enews.iasp-pain.org/AM/Template.cfm?Section=Home&SECTION=HOME&TEMPLATE=/CM/ContentDisplay.cfm&CONTENTID=17195. Accessed September 5, 2013.
Appendix1. FDA Drug Safety Communication: Prescription acetaminophen products to be limited to 325 mg per dosage unit; boxed warning will highlight potential for severe liver failure. http://www.fda.gov/Drugs/DrugSafety/ucm239821.htm. Published January 13, 2011. Accessed September 14, 20132. Castellsague J, Riera-Guardia N, Calingaert B, et al; on behalf of the inves-tigators of the Safety of Non-steroidal Anti-inflammatory Drugs (SOS) Project. Individual NSAIDs and upper gastrointestinal complications: a systematic review and meta-analysis of observational studies (the SOS Project). Drug Saf. 2012;35(12):1127-1146.3. McGettigan P, Henry D. Cardiovascular risk with non-steroidal anti-inflammatory drugs: systematic review of population-based controlled observational studies. PLoS Med. 2011;8(9):1-18.
4. Huerta C, Castellsague J, Varas-Lorenzo C, Rodriguez LAG. Nonsteroidal anti-inflammatory drugs and risk of ARF in the general population. Am J Kidney Dis. 2005;45(3):531-539.5. US Food and Drug Administration. Public health advisory - FDA announces important changes and additional warnings for COX-2 selective and non-selective non-steroidal anti-inflammatory drugs (NSAIDs). http://www.fda.gov/Drugs/Drug-Safety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm150314.htm. Published April 7, 2005. Accessed Sept. 12, 2013.6. National Institute for Health and Clinical Excellence. The care and management of osteoarthritis in adults. http://www.nice.org.uk/CG059. Published February 2008. Accessed Sept. 12, 2013.7. European Medicines Agency. EMA press release. http://www.ema.europa.eu/docs/en_GB/document_library/Press_release/2009/11/WC500014477.pdf. Published August 2, 2005. Accessed Sept. 12, 2013.8. Health Canada. Basic product monograph for nonsteroidal anti-inflammatory drugs (NSAIDs).http://www.hc-sc.gc.ca/dhp-mps/prodpharma/applic-demande/guide-ld/nsaid-ains/nsaids_ains-eng.php. Published November 23, 2006. Accessed Sept. 12, 2013.9. American Gastroenterological Association, Wilcox CM, Allison J, Benzuly K, et al. Consensus development conference on the use of nonsteroidal anti-inflammatory agents, including cyclooxygenase-2 enzyme inhibitors and aspirin. Clin Gastroenterol Hepatol. 2006;Sep;4(9):1082-1089. http://www.cghjournal.org/article/S1542-3565(06)00428-9/fulltext?refissn=0016-5085&refuid=S0016-5085%2808%2900049-8. Accessed September 14, 2013.10. American College of Rheumatology Ad Hoc Group on Use of Selective and Nonselective Nonsteroidal Anti-inflammatory Drugs. Recommendations for use of selective and nonselective nonsteroidal antiinflammatory drugs: an American College of Rheumatology white paper. Arthritis Rheum. 2008;59(8):1058-1073.11. Zhang W, Moskowitz RW, Nuki G, et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarth Cartil. 2008;16(2):137-162.12. American Geriatrics Society Panel on the Pharmacological Management of Persistent Pain in Older Persons. Pharmacological management of persistent pain in older persons. J Am Geriatr Soc. 2009;57(8):1331-1346.13. Antman EM, Bennett JS, Daugherty A, Furberg C, Roberts H, Taubert KA; for the American Heart Association. Use of nonsteroidal antiinflammatory drugs: an update for clinicians: a scientific statement from the American Heart Association. Circulation. 2007;115(12):1634-1642.14. United States Food and Drug Administration (FDA). FDA announces safety labeling changes and postmarket study requirements for extended-release and long-acting opioid analgesics. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm367726. Published September 10, 2013. Accessed September 16, 2013.15. Buurma A, Sosa MP, Witt AS. Pain management study: acute pain. Burlington, MA: Decision Resources; 2012.16. Kinkade S. Evaluation and treatment of acute low back pain. Am Fam Physician. 2007;75(8):1181-1188.17. United States Food and Drug Administration (FDA). http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/DrugSafetyandRiskManagementAdvisoryCommittee/UCM164897.pdf. Published May 22, 2009. Accessed Sept. 13, 2013.18. United States Food and Drug Administration (FDA). http://www.fda.gov/ downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM310477.pdf. Accessed June 28, 2013.19. Chang G, Chen L, Mao J. Opioid tolerance and hyperalgesia. Med Clin North Am. 2007;91(2):199-211.20. CDC Press Release: Opioids drive continued increase in drug overdose deaths. http://www.cdc.gov/media/releases/2013/p0220_drug_overdose_deaths.html. Accessed March 28, 2013.
41

®
©2013 Iroko Pharmaceuticals, LLC DAC_245_(0913)