iom_meeting_tanzania_day_1_v02
DESCRIPTION
http://cddep.org/sites/cddep.org/files/iom_meeting_tanzania_day_1_v02.pdfTRANSCRIPT

Tanzania: AMFm Evaluation and Future Direction
September 2012
1

2
Overall successes and challenges of the AMFm in Tanzania
Successes
• Significant positive response from private sector
• Achieved significant gains on dimensions of availability,
affordability, and market share, particularly in private
for-profit outlets
• All participants are eager to see the program continue
Challenges
• Delay between approval of the program and first orders
actually arriving in country meant the full-scale program
was short, not enough time to evaluate impact
• Lack of transparency
• First Line Buyers have expressed frustration at
lack of transparency in order approval process
• Little information about what comes next
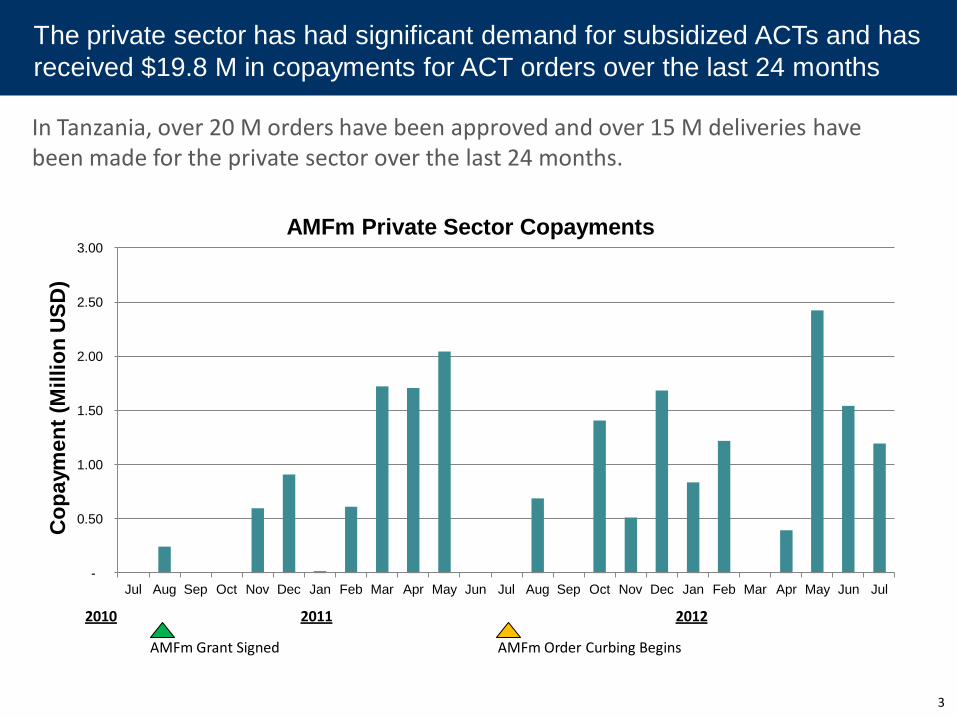
In Tanzania, over 20 M orders have been approved and over 15 M deliveries have been made for the private sector over the last 24 months.
The private sector has had significant demand for subsidized ACTs and has
received $19.8 M in copayments for ACT orders over the last 24 months
AMFm Order Curbing Begins
2010 2012
AMFm Grant Signed
2011
3
-
0.50
1.00
1.50
2.00
2.50
3.00
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul
Co
pa
ym
en
t (M
illi
on
US
D)
AMFm Private Sector Copayments

NOT FOR CIRCULATION
The public sector in Tanzania has also benefitted from the AMFm, with an
additional 10 M orders approved, bringing total AMFm orders to 30M
0% 0%0%0%0%
0%
0%0%
Total
30.4
67%
33%
Jul-
12
100%
Jun-
12
1.9
100%
May-
12
4.8
55%
45%
Apr-
12
1.5
29%
71%
Mar-
12
1.6
100%
Feb-
12
1.4
0%
100%
Jan-
12
0.9
100%
Dec-
11
1.6
100%
Nov-
11
0.6
100%
Oct-
11
1.4
0%
100%
Sep-
11
0.0
Aug-
11
0.7
0%
87%
13%
Jul-
11
0.0
Jun-
11
0.0
May-
11
1.9
100%
Apr-
11
6.3
0%
22%
78%
Total
1.4
Feb-
11
0.9
100%
Jan-
11
0.1
100%
Dec-
10
0.9
Mar-
11
Nov-
10
0.8
100%
Oct-
10
0.0
Sep-
10
0.0
Aug-
10
0.2
100% 100%
Private not-for-profit
Private for-profit
Public
Orders approved by sector (M)
Note: Only includes orders uploaded to Global Fund website; Data cleaned to remove repeat approved orders and negative deliveries
Source: Global Fund website
Sector
4
Month order approved
100%
1.9
5
Diarrhea and pneumonia treatment offer perhaps the greatest untapped opportunities to further progress towards MDG 4…
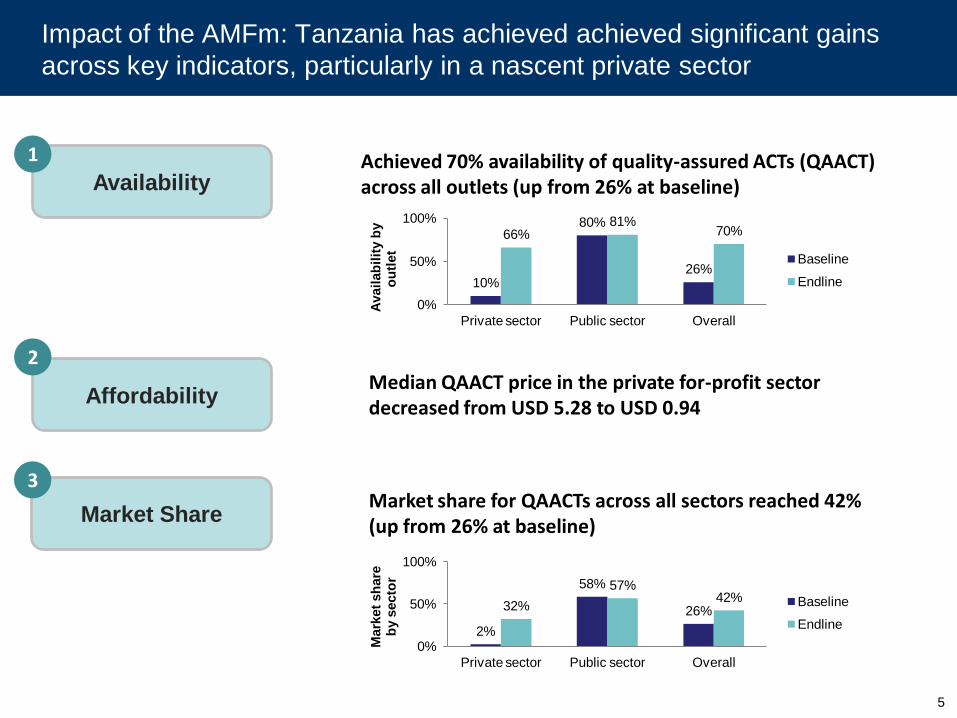
Availability
1
Affordability
Achieved 70% availability of quality-assured ACTs (QAACT) across all outlets (up from 26% at baseline)
2
Market Share
3
Median QAACT price in the private for-profit sector decreased from USD 5.28 to USD 0.94
Market share for QAACTs across all sectors reached 42% (up from 26% at baseline)
10%
80%
26%
66% 81%
70%
0%
50%
100%
Private sector Public sector Overall
Avail
ab
ilit
y b
y
ou
tlet
Baseline
Endline
2%
58%
26% 32%
57% 42%
0%
50%
100%
Private sector Public sector Overall
Mark
et
sh
are
b
y s
ecto
r
Baseline
Endline
Impact of the AMFm: Tanzania has achieved achieved significant gains
across key indicators, particularly in a nascent private sector

As we look forward, transition planning will need to address Tanzania’s
specific country context
Variation in Pf prevalence across Tanzania
Tanzania’s target:
Reduce burden of
malaria by 80% from
2007 levels by end of
2015
Tanzania is working to develop an integrated private sector management
strategy that will both achieve the country’s goals for malaria reduction
and improve value for money
6 Source: Malaria Atlas Project, which combines several surveys of malaria prevalence. A new Malaria Indicator Survey will be coming out later
this year (most recent was 2007).

Internal Document Internal Document
Tanzania has established a Private Sector Case Management Task Force to
address the AMFm transition as well as case management strategy broadly
Respond to
changing
epidemiology
by
strategically
scaling up
diagnosis
Sustain and
improve upon
treatment
gains made
during AMFm
Phase I
Align
regulatory
policies
with case
management
targets
Task Force
Launch
Diagnosis
Sessions
Final
Review
Treatment
Sessions
Regulatory
Approval
Costing
the
Strategy
Where we are now June 2012 December
2012
First
draft
Global Fund
decision
Estimate
needed
funding and
calculate gap
7
Outputs:
1) Private Sector Case Management Strategy document
2) Model for financing
3) Funding gap analysis
8
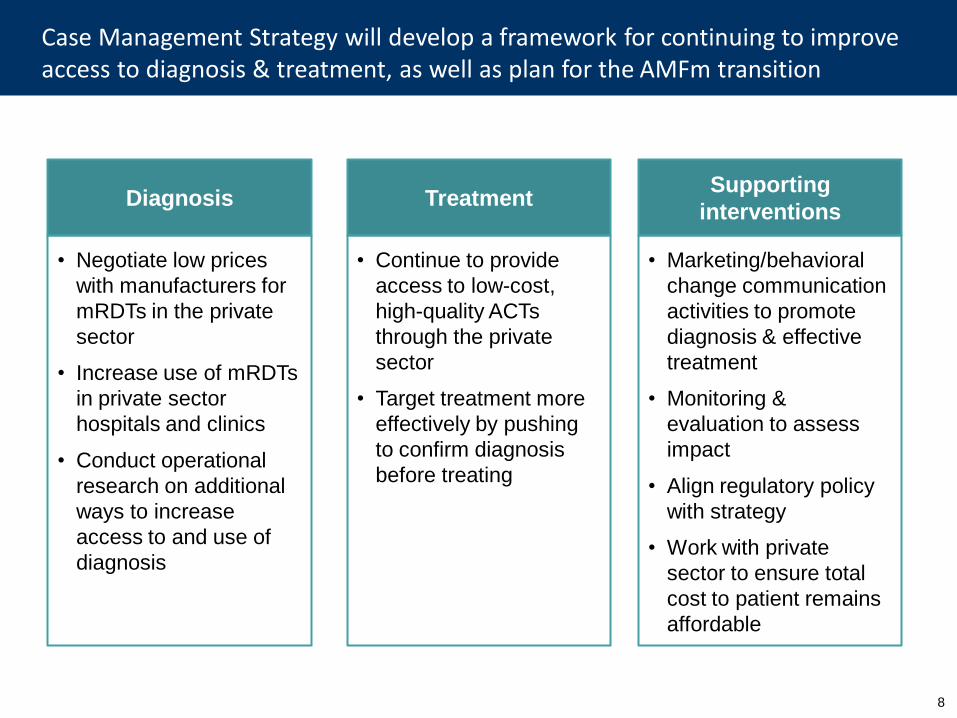
Case Management Strategy will develop a framework for continuing to improve access to diagnosis & treatment, as well as plan for the AMFm transition
Diagnosis
• Negotiate low prices
with manufacturers for
mRDTs in the private
sector
• Increase use of mRDTs
in private sector
hospitals and clinics
• Conduct operational
research on additional
ways to increase
access to and use of
diagnosis
Treatment
• Continue to provide
access to low-cost,
high-quality ACTs
through the private
sector
• Target treatment more
effectively by pushing
to confirm diagnosis
before treating
Supporting
interventions
• Marketing/behavioral
change communication
activities to promote
diagnosis & effective
treatment
• Monitoring &
evaluation to assess
impact
• Align regulatory policy
with strategy
• Work with private
sector to ensure total
cost to patient remains
affordable

9
Future of the AMFm: reactions to “semi-integrated” modification
options, in the context of Tanzania’s private sector
Scenario Pros Cons Summary / Preliminary
evaluation
Diagnosis focus
Fits with current policies and overall strategy
Potential problems with access, compliance, perceptions, total final cost to patients
Promising, but need to think about access problems and final total price to patient
Age targeting Targets a share of population with disproportionate malaria burden
Difficult to monitor/regulate at retail level, possible pack stacking, shift burden to adults
Could be implemented, but have to acknowledge that leakage would occur
Geographic targeting
Deals with problem of varying malaria endemicity; supplier networks could handle regional targeting
Difficult to monitor/regulate at retail level, likely leakage to non-target regions
Could be implemented, but have to acknowledge that leakage would occur
Partial subsidy Relatively easy to implement – same structure as current program
Potential drop in ACT use with higher price and shift to lower-quality treatments
Feasible, but have to consider impact on number of people treated

10
Task Force has begun to address how various AMFm modification
options could be implemented
Scenario Actions needed for implementation Additional ways to target limited
funding
Diagnosis focus
• Increase access to mRDTs through informal drug outlets (would require operational research & eventual policy change)
• Select ADDOs and pharmacies for scale-up based on a particular profile (e.g. geographic location, facilities, health background)
• Reduce ACT subsidy level
Age targeting • To monitor & enforce, would need ground-up change in regulation & reporting systems
• Lower age limit for subsidy
• Combine age + geographic targeting
Geographic targeting
• To monitor & enforce, would need ground-up change in regulation & reporting systems
• Could package drugs to show intended region
• Rank regions by highest malaria burden
Partial subsidy • Work with private sector to keep margins down so that final price is not prohibitively expensive
• Combine with other types of targeting to give different subsidy levels to different groups (though harder to implement)

11
Questions for the group
1) How can the country case management strategy & transition planning
process better align with the on-going transition planning work at the global
level?
2) If the modified AMFm program does not meet our country’s funding needs
to implement our case management strategy plan, where else could we
seek funds? How can we plan for this now?
3) Are there other groups we should coordinate with, or which we could seek
technical assistance from, as we work to build our case management
strategy?
4) Do other countries have experiences we could learn from regarding best
practices for implementing targeted subsidies or diagnosis scale-up?

12
Summary
Tanzania looks forward to getting input from the global community as we
plan our strategy to reduce malaria mortality & morbidity
AMFm
results
• AMFm has resulted in significant gains in availability, affordability,
and market share of ACTs, particularly in the private sector
• Program participants are eager to see it continue
• There is a strong interplay between the public and private sector
that should continue in future programs
Planning
for the
future
• A Private Sector Case Management Task Force has started
planning for future private sector case management strategy and
the AMFm transition
• Initial strategy plans include a scale-up of diagnosis in the private
sector
• Out of the semi-integrated AMFm modification options under
discussion, age and geographic targeting would pose the most
challenges for implementation, but we have begun to discuss how
we could manage the implementation of all options