introduction trends and policy solutions physical overvie · trends and policy solutions in adult...
TRANSCRIPT

Trendsand
Policy Solutions
in
IntroductionMedicaid and health care costs continue to rise due to increased use of medications and long-term care, as well as higher incidence of pre-ventable illness and disabling conditions. Cost-containment strategies are failing, and policymakers are confronting the root causes of rising costs, namely chronic diseases. Obesity is a primary cost driver, causing or complicating many chronic conditions.
While each individual’s weight is a personal issue, obesity rates and as-sociated costs in the United States have increased dramatically in recent years and warrant public policy attention. Personal choices affect health care costs throughout the population, both for the public and private sectors. Addressing the rise in obesity means acknowledging that per-sonal responsibility, consumer choice and public interests need to be balanced. Confronting obesity in the United States will require efforts by policy-makers, individuals, communities, businesses, health care provid-ers and the marketplace.
This Toolkit provides policy-makers with discussions about obesity, in-cluding data and trends, and solutions being implemented or consid-ered by states and legislators across the country.
What is Obesity?Overweight and obesity result from consuming more energy—or food—than is burned through activity or exercise. Primary behavioral factors that cause obesity are physical inactivity and poor nutrition. Lack of environmental supports for healthy choices where we work, live and play contribute to these risks.1
Trends and Policy Solutions
in Adult Obesity, Physical
Activity and Nutrition
Overview
Obesity 15-Year Trends Among U.S. Adults, Behavioral Risk Factor Surveillance System, 1988 and 2003
(BMI ≥30 or ~ 30 lbs overweight for 5’4” person)
No data <10% 10%–14% 15%–19% 20%–24% ≥25%
BRFSS, 2003BRFSS, 1998
Source: Behavioral Risk Factor Surveillance System, CDC.

Trends in Obesity, Physical Activity and NutritionIt is estimated that 65 percent—or 191 million—of American adults are overweight, while 30 percent—or 60 million—of American adults over age 20 are obese.2 In 1991, no states reported obesity rates at or above 20 percent. Today, approximately 35 states have obesity rates above 20 percent. In four of these states, at least one-quarter of adults are obese.3
Physical Activity. Despite the proven benefits of physical activity, more than 50 percent of American adults do not get enough physical activity to provide health benefits, and 24 percent are not active at all in their leisure time.
Healthy Eating. Less than one-quarter of adults in the United States eat the recommended five or more servings of fruits and vegetables each day. In the last 30 years, caloric intake has increased for both men and women.
Health Disparities in Obesity. Obesity disparities exist across gender, age, race and education levels.
In 2003, more men than women got the recommended amount of physical activity. Women were also more likely to report no leisure-time physical activity.4
About one-half of white adults met the physical activity recommendation while slightly more than one-third of black and Hispanic adults did. As educational attainment increased, so did the proportion of adults meeting recommendations for physical activity. Half of college graduates met the physical activity recommendation while only one-third of those with less than a high school education did.
Why Fight the Obesity Epidemic?The Human and Financial Costs of ObesitySome believe obesity is a personal issue that should not involve the government. However, federal, state and local governments finance the treatment of obesity-related illnesses, and the health costs associated with obesity now exceed the costs of tobacco use.5
Obesity costs America $117 billion annually, including $61 billion in di-rect medical costs for treatment of related diseases, plus $56 billion in indirect costs such as lost productivity.6
Health care costs are 36 percent higher and medication costs are 77 percent higher for an obese person compared to an individual at a healthy weight.7
If 10 percent of adults began a regular walking program, $5.6 billion in heart disease costs could be saved.
A sustained 10 percent weight loss can reduce an overweight person’s lifetime medical costs by between $2,200 and $5,300 by lowering costs associated with hypertension, Type 2 diabetes, heart disease, stroke and high cholesterol.
The Benefits of Physical Activity and Healthy EatingHealth experts recommend that Americans get 30 minutes or more of physical activity8,9 every day and eat a balanced, low-fat diet high in whole grains, fruits and vegetables. Physical activity and healthy eating help control weight and can reduce risk for heart attack, colon cancer, diabetes, osteoporosis, high blood pressure and stroke. Physical activity also:
reduces falls and injuries among older adults;relieves arthritis pain;
n
n
n
n
n
Body Mass IndexAdult overweight and obesity are determined by using weight and height to calculate body mass index (BMI), which is directly related to body fat.
$23.50
$12.80
$28.10
$14.10
Out-of-pocket
Private
Medicaid
Medicare
U.S. Medical Spending on Overweight and Obesity, 1998
(in billions)
Source: Finkelstein, EA, Fiebelkorn, IC, Wang, G. National Medical Spending Attributable to Overweight and Obesity: How much, and Who’s paying? Health Affairs 2003;W3;219–226.
�
Adult Weight Status
BMI Weight Status
Below 18.5 Underweight
18.5–24.9 Normal
25–29.9 Overweight
30.0 and Above Obese
Data on Obesity Deaths: What Does It Mean?
Recently, new estimates have been released on obesity deaths in the United States. These new data suggest that while fewer Americans die from obesity every year, many are living with costly and debilitating illnesses.
Despite the debate about the number of obesity deaths, there is no question that obesity is on the rise, and Americans continue to make unhealthy choices. Americans continue to gain weight and do not meet recommendations for physical activ-ity and healthy eating.
There is also overwhelming evidence and scientific agreement about the high cost and tragic health impact of obesity. Obesity causes serious illnesses, complicates other chronic diseases, results in dis-ability and reduces quality of life.
alleviates symptoms of anxiety and depression; andreduces hospitalizations, doctor visits and medications.
What Legislators Can Do about ObesityState legislators nationwide have been actively pursuing solutions to Amer-ica’s obesity epidemic. Arenas worth policy-makers’ attention include:
Health CareHealth care providers can address weight and the risk for serious chronic disease and disability as part of routine clinical care. Health insurers can provide coverage for prevention-oriented practices and benefits such as nutrition and physical activity counseling.
Legislators can support these efforts by setting minimum insurance stan-dards and providing tax and other incentives for insurers to cover preven-tion-oriented care.
Agriculture, Food Supply and NutritionIndustries involved in growing and supplying food can provide a broad range of profitable and healthy choices where consumer demand exists. The agriculture and food industries can produce more fresh fruits and vegetables and continue to offer nutritious alternatives in food venues.
Legislators can support these efforts by urging state and private agricul-ture entities to promote healthy eating, providing leadership to promote voluntary healthy food labeling in restaurants and grocery stores and supporting local agriculture by linking growers with food programs for underserved populations.
CommunitiesCommunity partnerships—local governments and civic, professional and faith based organizations working with people in their homes, schools, and parks –- can be among the most effective tools for improving health. For example, neighborhoods can promote healthy living by creating safe walking and biking paths.
Legislators can support these efforts by providing resources to commu-nity-level campaigns that promote physical activity and healthy eating, encouraging zoning and planning decisions that promote health and encouraging collaboration among state agencies in dealing with obe-sity issues.
State Government, Businesses and EmployersState governments can help individuals, businesses and communities prevent, detect and treat illness. Employers can provide incentives for healthy employees and offer programs and benefits for healthy living. Businesses can join together to find solutions to health care challenges and collaborate in public-private partnerships with government.
Legislators can support these efforts by setting nutrition standards in state government food services, working with insurance companies to offer premium breaks for employers that enact preventive health and wellness initiatives, and offering individuals pre-tax spending options for health or wellness related expenses.
Individuals While government can establish broad priorities and set policy to sup-port healthy individual behavior, individuals must ultimately become educated about healthy eating and physical activity, make healthy choices, engage in their own care and wellness, and use health care re-sources wisely.
Legislators can support individuals by addressing obesity in a variety of
n
n
policy arenas; and by providing options and incentives to promote physi-cal activity and healthy eating to employers, businesses, health care pro-viders and insurers, and communities.
End NotesTo avoid stigma, and because the formula for calculating overweight is different for children, the terms at-risk and overweight are used when referring to children and youth. This is discussed further in CSG’s Toolkit on Trends and Policy Solutions in Youth ObesityFlegal KM, Carroll MD, Ogden CL, Johnson CL. Prevalence and trends in obesity among US adults, 1999-2000. JAMA 288:1723-7. 2002.U.S. Department of Health and Human Services, Centers for Disease Control and Prevention. Behavioral Risk Factor Surveillance System, 2003. Retrieved from http://apps.nccd.cdc.gov/brfss/ on April 25, 2005No leisure-time physical activity is defined as no reported leisure-time physical activities (i.e., any physical activities or exercises such as running, calisthenics, golf, gardening, or walking) in the previous month.Sturm, R. The Effect of Obesity, Smoking, and Drinking on Medical Problems and Costs. Health Affairs 21(2):245-253, 2002.U.S. Department of Health and Human Services. The Surgeon General’s call to action to prevent and decrease overweight and obesity. 2001. Sturm, R. The Effect of Obesity, Smoking, and Drinking on Medical Problems and Costs. Health Affairs 21(2):245-253, 2002. Recommended physical activity is defined as reported moderate-intensity activities in a usual week (i.e., brisk walking, bicycling, vacuuming, gardening, or anything else that causes small increases in breathing or heart rate) for at least 30 minutes per day, at least 5 days per week; or vigorous-intensity activities in a usual week (i.e., running, aerobics, heavy yard work, or anything else that causes large increases in breathing or heart rate) for at least 20 minutes per day, at least 3 days per week or both. This can be accomplished through lifestyle activities (i.e., household, transportation, or leisure-time activities).Centers for Disease Control and Prevention, Behavioral Risk Factor Surveillance System. Retrieved from http://apps.nccd.cdc.gov/PASurveillance/DemoCompareResultV.asp?State=1&Cat=2&Year=2003&Go=GO on April 25, 2005.
1�
2�
3�
4�
5�
6�
7�
8�
9�
This publication was prepared by Michael Fierro and Debra Lightsey of Bearing Point, Inc. for The Council of State Governments’ (CSG) Healthy States Initiative. Funding for this publication was
provided by the U.S. Department of Health and Human Services, Centers for Disease Control and Prevention (CDC) under Cooperative Agreement Number U38/CCU424348. Its contents are the
responsibility of the authors and do not necessarily represent the official views of CDC or CSG.

Trendsand
Policy Solutions
in
eyond Cost Containment:
Introduction
Americans’ waistlines and their perspectives on obesity are rapidly changing. One study shows that 39 percent of Americans will be obese and 75 percent will be overweight by 2008.1 Three-quarters
of Americans see obesity as a disease and think that treatment should be included in their health plan
benefits.2 These changes are driving an increased demand for obesity surgeries, which according to the National Institutes
of Health, cost approximately $100,000 per patient when follow-up care and treatment costs are included.
As the United States struggles with these costs and demands on the health care system, there is also debate about the classification of obe-sity as a disease, assessing fees based on weight for insurance premiums and covering obesity treatment and surgery options as a health ben-efit. Health care providers, insurers and beneficiaries will all experience changes in the way health care is delivered based on state and federal obesity policies. Medicare, the Internal Revenue Service and other fed-eral agencies are changing their definitions of obesity, which is driving changes at the state level.
Obesity and weight are very personal issues, and all Americans need to take steps to achieve a healthy weight. However, both public and private health insurers spread costs and risks across large populations, so per-sonal choices have societal effects.
Legislators, as stewards of public dollars, are entering into the fray by addressing these issues in the health care system. State policy-makers need to look beyond traditional benefit decisions in Medicaid and health plans to the root causes of increasing costs: obesity, physical inactivity and poor nutrition. State legislators can push the health care system to fight obesity by:
establishing minimum insurance coverage requirements for obesity prevention and treatments;encouraging providers and consumers to adopt best practices in treating and preventing obesity; andencouraging worksite wellness and employee benefit programs.
n
n
n
State Policies that Support Health Care Solutions for Obesity
Why Address Obesity in the Health Care System?
Obesity is associated with increased illness and death from chronic diseases such as heart disease, stroke and diabetes. Weight loss and improved physical activity and nutrition lead to reduced risk for diabetes and cardiovascular disease, along with improving blood pressure, cholesterol levels and blood glucose levels. This translates to reduced cost for employers, health plans, insurers and consumers. Additionally, methods for treating obesity—physical activity and healthy eating—are fundamental components of clinical standards of care, in addition to medications and surgery. Physical activity and healthy eating are primary ways to treat diseases such as heart disease, stroke and diabetes.
Which Treatments Work?
Health care providers and their overweight or obese patients have a variety of effective options to manage and reduce weight. These options include:
dietary therapy approaches such as low-calorie diets and lower-fat diets; increasing physical activity patterns; behavior therapy techniques; pharmacotherapy; surgery; and combinations of these techniques.
Demand for obesity treatments is growing rapidly, with some insurance companies reporting up to a 50 percent increase per year for the past several years.3 Insurers and health care purchasers are looking at options for containing costs and providing the best care to their beneficiaries.
n
n
n
n
n
n
�
Over the last 10 years, the number of weight loss surgeries performed has
skyrocketed from less than 20,000 in 1992 to over 100,000 in 2003.
Source: American Society for Bariatric Surgery, www.asbs.org
The National Institutes of Health have recommended the fol-lowing interventions for obesity:4
Dietary therapy: A regimented dietary plan includes a low calorie diet to support weight loss. Physical activity: Increasing physical activity is an essential component of weight loss therapy and the prevention of weight re-gain. When physical activity is added to a weight loss regimen, the risks for cardiovascular disease and diabetes are reduced even more than with weight loss alone. Behavior therapy: Strategies help individuals overcome barriers to comply with a prescribed diet or exercise regimen, including stress management, stimulus control, problem solving, contingency management, cognitive restructuring and social support.Combined therapy: A combined intervention of behavior therapy, a low calorie diet and increased physical activity provides the most successful therapy for weight loss and weight maintenance. This type of intervention should be maintained for at least six months before considering pharmacotherapy.
n
n
n
n
Strategies for Weight Loss and Weight Maintenance

Health care providers, health plans and insurers have begun addressing obesity, physical activity and nutrition by:
educating providers on the latest best practices in preventing and treating obesity;encouraging beneficiaries to be healthy through worksite wellness and employee benefit programs; and covering weight loss and surgical treatment when appropriate.5
Recent Health Care Sector Trends on ObesityWhile obesity is not widely classified as a disease among insurers, it is classified as such by numerous health and scientific agencies.6,7,8,9,10,11 Among federal agencies, there is not agreement about the classification of obesity as a disease. In 2001, however, the Internal Revenue Service ruled that medical expenses for treating obesity medically or with phar-maceuticals were tax deductible, subject to limitations and specific ex-clusions of most food costs.12 And now both the Social Security Admin-istration and the Food and Drug Administration acknowledge obesity as a disease. For both Social Security and the FDA, obesity is a qualifying condition for disability payments and related drug therapies, and adver-tising restrictions on dietary supplements apply to products promoted as weight loss aids.13,14 In 2004, the Centers for Medicare and Medicaid Services announced that Medicare would allow payments for reason-able and effective obesity treatments. This ruling prompted an analysis of “reasonableness” of costs by the Medicare Coverage Advisory Com-mittee.
Covering Weight Loss SurgeryThe federal Agency for Health Care Research and Quality found that
n
n
n
�
Strategies for Weight Loss and Weight Maintenance
Pharmacotherapy: In carefully selected patients, appropriate drugs can augment additional weight loss options.Weight loss surgery/bariatric surgery (including gastric bypass or gastric banding): Weight loss surgery is typically viewed as a last resort option for morbidly obese patients who have exhausted other options. The surgeries alter the size of the stomach and routing of food to achieve a feeling of fullness, reducing the amount of food, fat and calories absorbed. Guidance on diet, physical activity and behavioral and social supports are necessary both prior to and after the surgery.
n
n

Adult Weight Status
BMI Weight Status
Below 18.5 Underweight
18.5–24.9 Normal
25–29.9 Overweight
30.0 and Above Obese
for morbidly obese patients—those with BMI greater than or equal to 40—surgical interventions were far more successful than obesity drugs or diet therapy. For patients with BMI’s between 35 and 40, the data were inconclusive. Due to high demand for gastric bypass surgery among state employees, Louisiana launched a study to examine the financial ef-fects of gastric by-pass surgery on the overall health care costs of obese patients within their state’s employee health plan. The Louisiana Office of Group Benefits, which covers 250,000 state employees and public teachers, agreed to pay for 40 state employees to receive gastric bypass surgery as part of a pilot program testing the procedure’s effectiveness at treating morbid obesity. The state pays a $25,000 capped fee if the surgery is deemed medically necessary and the person consents. If the study shows savings, gastric bypass treatment may become a routinely covered procedure under health insurance plans.
Educating Providers and Consumers on Best PracticesTo help determine the most effective ways to treat and prevent obe-sity, Kaiser Permanente (KP) conducted studies and surveys of their members and the American public on obesity. The most recent survey showed that three-quarters of Americans see obesity as a disease and think that health plans should cover obesity treatments. Overall, a per-son’s own weight had little impact on his or her view of obesity.15 KP also assessed the health and weight of its members and found that it cov-ered an estimated 4.4 million overweight or obese adult members out of 7 million total adult members and that the total cost of care for obese members was 44 percent higher than for members who maintained a healthy weight.
Tracking BMI in members’ electronic medical records: KP is using its efforts to establish electronic medical records to institute universal BMI measurement of all members to assess weight trends. Monitoring patient BMI information over time helps clinicians discuss the topic with patients and intervene when necessary. Establishing appropriate clinical management tools: KP created the Healthy Lifestyles Programs, a series of in-depth online weight management and fitness, smoking cessation, stress reduction and nutrition programs for members.Educating providers: KP developed the Weight Management Source Book to educate providers about options available to members on weight management and bariatric surgery.
Highmark (Blue Cross/Blue Shield) recognized the impact and preva-lence of obesity and initiated a comprehensive approach to specifically address childhood obesity. Additionally, Highmark has begun address-ing obesity with a variety of approaches, including:
Community-level activity: Highmark convened a policy forum of obesity experts and community leaders and funded a childhood obesity media campaign. The Highmark Challenge for Healthier Schools has provided $900,000 in grants to schools to introduce nutrition and physical activity programs and to fund a system-wide physical education and nutrition curriculum in grades K–8 affecting 28,000 children. In Central Pennsylvania, over 32,000 elementary students have received daily planners that include health messages and tips. Provider and consumer education: Highmark developed a tool kit that includes obesity identification and treatment guidelines,
n
n
n
n
n
Adult overweight and obesity are determined by using weight and height to calculate body mass index (BMI), which is directly related to body fat.
�
�
parent self-help materials on nutrition and activity, a BMI calculator and other materials. It also created an online weight management initiative for members.Worksite wellness program: Highmark established a worksite wellness program for Highmark employees.Bariatric surgery and weight loss medications: Highmark provided these medical interventions to members who meet defined criteria and have sought intervention through an approved weight management program for at least six months prior to the procedure. Prescription weight loss drugs are currently covered for an underlying condition related to obesity.
Worksite Wellness and Employee BenefitsWest Virginia Public Employee Insurance Agency (PEIA),16 the largest in-surer in the state with 212,000 members, has conducted a number of programs under its Pathways to Wellness Initiative, aimed at keeping its members healthy, fit and eating properly. Recently, PEIA found that those not exercising regularly cost $268 per person more than their counter-parts. The agency launched a program targeting sedentary behavior. One year after its inception, the agency reaped the benefits of its efforts: the number of members who exercised over an hour a week doubled from 17 percent to 35 percent. Pathways’ programs include:
WellSteps One Risk Management Program: All programs include support through a telephone coach at varying levels. Employer clients have the option of customizing criteria for telephone counseling and adding additional local options such as community or worksite programs. Fees are based on the level of service selected.Supersize and Portions Campaign: PEIA launched a campaign to educate members on food consumption and appropriate portion size to maintain a healthy weight. The agency conducted a mass media campaign warning members about fast food consumption with tools to choose healthy foods. Messages included “Biggie Fries=Biggie Thighs” and “Super Size Food=A Super Size You.”Stepping Stones Pedometer Program: To promote physical activity, PEIA distributed pedometers to members who requested them and provided tools to track their steps. When screened for the Pathways Initiative, members were encouraged by clinicians to participate.
North Carolina Prevention Partners and the state’s Department of Health and Human Services created the BASIC Preventive Insurance Benefits Ini-tiative to increase availability and use of preventive services. BASIC en-courages employers to:
purchase preventive benefits; partner with private and public health plans to establish or enhance insurance products with benefits coverage for preventive services; continuously update and promote a profile of all North Carolina preventive services insurance products via the Internet; create and disseminate prevention tools to be shared by North Carolina health plans, health systems and health care professionals; and raise consumer awareness about the importance of preventive care.17
What Legislators Can Do about ObesityLegislators across the country have begun addressing obesity in the health care system by introducing legislation to create dedicated trust funds, establish minimum insurance requirements to cover weight loss
n
n
n
n
n
n
n
n
n
n

�
and surgical treatments, modify Medicaid to offer obesity treatment benefits and set up commissions to study the impact of obesity on their state’s health care system. Innovative solutions are: 18
California Senate Bill 564 (2005-pending) would create the California Healthy Trust Fund and an additional tax on cigarettes at the rate of $.025 for each cigarette distributed. Money generated from the tax would fund public health programs to prevent childhood obesity and diabetes.Idaho House Bill 0696 (2004-enacted) directs the Department of Health and Welfare to conduct a pilot project to determine the effectiveness of weight control therapies in the state’s Medicaid program.Maryland House Bill 462 (2005-enacted) creates a task force to study requiring insurance coverage of obesity treatments.
Establishing Insurance Coverage Minimum RequirementsMaryland Senate Bill 868 (2004-enacted) requires that certain health insurance policies offer optional coverage of surgical treatment of morbid obesity.New Jersey Assembly Bill 1515 (2004-pending) requires managed care programs to cover treatments for obesity in adults on a fee-for-service basis. Idaho House Bill 708 (2004-not enacted) would have required health insurance companies to cover expenses resulting from weight reduction services or from morbid obesity.
Covering Weight Loss and SurgerySouth Carolina S1235 (2004-enacted) recognizes the use of gastric bypass surgery for the treatment of morbid obesity as a valid and important procedure with specific preference for treatment provided by board certified bariatric surgeons.Virginia SB1081 (2003-enacted) provides mandated coverage for the treatment of morbid obesity through gastric bypass surgery or such other methods recognized by the National Institutes of Health (NIH) as effective for the long-term reversal of morbid obesity.Missouri HB1088 (2004-not enacted) would require insurance companies to offer coverage for treatment of morbid obesity if the policy holder chooses such coverage.Tennessee HB2246 (2004-not enacted) would require health insurance policies to offer optional coverage for surgical treatment for clinically severe obesity.
n
n
n
n
n
n
n
n
n
n
�
ConclusionWhile no one action or policy will solve the obesity issue, legislators have numerous opportunities to support healthy living through their state’s health care system, providers and residents. While much discussion has focused on requiring insurers to provide benefits such as gastric bypass surgery, state legislators have many options in supporting the health care system to reduce obesity, improve physical activity and nutrition and reduce illness and costs in their states.
Legislators can:
examine costs to state government and state economies from obesity, related illnesses and lost productivity;convene health care and government agencies to implement obesity prevention and management initiatives;work to establish worksite wellness programs for state and private employers;consider including nutrition counseling and physical activity counseling in minimum insurance coverage requirement policies, in accordance with NIH guidelines; andencourage the use of technology and innovative tools for providers and consumers to maintain a healthy weight or support weight loss.
n
n
n
n
n
�
End NotesJames Hill, PhD, Presentation at Edelman Corporation’s Opportunities for Government and Industry to Address the Obesity Epidemic, a Panel Discussion. March 12, 2003. Retrieved from www.edelman.com/events/Obesity_Epidemic/startwm.html on May 2, 2005.Kaiser Family Foundation, Employer Health Benefits 2004 Annual Survey.“As Obesity Spreads, Employers and Insurers Question Gastric Bypass Surgery Coverage”, Reprinted from the Jan. 12, 2004 issue of Managed Care Week. Retrieved from www.aishealth.com/ManagedCare/Product/MCWEmployersQuestionBypass.html on May 2, 2005Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults, The Evidence Report, National Institutes of Health, National Heart, Lung and Blood Institute, No. 98-4083, 1998Health Plans Emerging As Pragmatic Partners in Fight Against Obesity, National Institute for Health Care Management Foundation. April 2005. World Health Organization, the National Academy of Sciences, the National Institutes of Health, the Food and Drug Administration, the Social Security Administration, the International Classification of Diseases, the Federal Trade Commission and the Internal Revenue ServiceClinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults, The Evidence Report, National Institutes of Health, National Heart, Lung and Blood Institute, No. 98-4083, 1998. p.xi.Weighing the Options, Criteria for Evaluating Weight-Management Programs, Food and Nutrition Board, Institute of Medicine, Paul R. Thomas, Editor. National Academy Press, Washington, D.C. 1995WHO Press Release 46, 12 June 1997.The ICD-9-CM lists “Obesity and other hyperalimentation” as #278 in the Endocrine, Nutritional, Metabolic and Immunity Disorders sectionFederal Trade Commission/Partnership for a Healthy Weight Partnership Principles. Retrieved from www.consumer.gov/weightloss/principles.htm#obesity on May 3, 2005.IRS Publication 502 for 2004 tax yearFederal Register, January 6, 2000, Vol. 65, p. 1028.Federal Register, Vol. 65, No. 94, May 15, 2000, p. 31039.Retrieved from ckp.kp.org/newsroom/national/archive/nat_041130_obesity.html on April 30, 2005PEIA Pathways to Wellness: An Assessment of Health Screenings, 1998-2003. August 2004. State Approaches to Childhood Obesity: A Snapshot of Promising Practices and Lessons Learned. National Academy for State Health Policy. April 2004.Bills are enacted unless otherwise noted.
1�
2�3�
4�
5�
6�
7�
8�
9�10�
11�
12�13�14�15�
16�
17�
18�
This publication was prepared by Michael Fierro and Debra Lightsey of Bearing Point, Inc. for The Council of State Governments’ (CSG) Healthy States Initiative. Funding for this publication was
provided by the U.S. Department of Health and Human Services, Centers for Disease Control and Prevention (CDC) under Cooperative Agreement Number U38/CCU424348. Its contents are the
responsibility of the authors and do not necessarily represent the official views of CDC or CSG.

Trendsand
Policy Solutions
in
IntroductionEmployers and businesses are as involved as individuals and commu-nities in the current obesity epidemic. Employers are paying much of the increased health care costs due to obesity and related diseases, and businesses are suffering from lost productivity and absenteeism due to employees’ poor health and disability.
The costs of health benefits are already high—averaging $9,950 annu-ally per employee nationally, for family coverage.1 As costs continue to increase, employers and businesses are struggling to pay for employee health care. These costs are shifted to employees, and they also struggle to make ends meet.
Addressing root causes of obesity is necessary to maintain a healthy economy. Obesity is a greater trigger for health problems and increased health spending than smoking or drinking. Individuals who are obese have 30 to 50 percent more chronic medical problems than those who smoke or drink heavily.2 The total cost of obesity for U.S. companies is estimated at $13 billion per year. Health insurance costs related to obesity comprise the largest percentage of the total ($8 billion), followed by paid sick leave ($2.4 billion), life insurance ($1.8 billion) and disability insurance ($1 billion).3
States are major employers in the United States and are not immune from the rising costs as-sociated with obesity.
To date, state legislators have focused attention primarily on schools and children and less on adults, businesses or worksites. However, there are many options available to legislators who seek to assist businesses and workers in promoting good health and addressing health costs associated with obesity, including:
encouraging worksite wellness programs;implementing healthy nutrition standards for employee cafeterias and vending machines;creating programs to reward employers for promoting good health among employees; andencouraging employers to work with insurers to offer premium breaks to employees who participate in health promotion and disease prevention activities.
The Role of State Government, Businesses and Employers Employers and U.S. businesses have responded to increased costs by shifting from just paying for the treatment of chronic diseases to paying for prevention efforts. Many employers are tack-ling health issues through worksite wellness programs; obesity, physical activity and nutrition are the primary targets. Employers that address obesity in the workplace can: reinforce and maintain healthy employee behaviors; encourage employees to take an active role in their per-sonal health; reduce health care costs; reduce short-term sick leave; and increase productivity.
n
n
n
n
Employer Paid Costs Attributable to Overweight
and Obesity
Source: US Department of Health and Human Services. Prevention Makes Common Cents: Estimated Economic Costs of Obesity to US Business, 2003.
60%Medical Costs
40%Paid sick leave, life insurance and disability
insurance
Healthy Bottom Line:State Government, Businesses and Employers

�
To achieve those results, employers have many options, including:
educating employees and other beneficiaries about healthy behaviors and company benefits available to promote good health;providing employees with financial and non-financial incentives to be physically active, maintain or attain a healthy weight and eat healthy foods; implementing worksite wellness programs for employees;improving the work environment to encourage healthy behavior, such as: supplying healthy foods in vending machines and cafeterias; implementing workplace nutrition policies and servings more healthy foods at work-sponsored events and meetings; renovating stairwells to make them more attractive; prompting employees to use the stairs; andproviding pedometers to employees and encouraging walking, jogging and running.assuring worksites are conducive to physical activity, including setting standards for new construction and new acquisition of workspace that allow and promote use of stairwells and walking.
Recent Employer Sector Trends on ObesityObesity has been a focus of attention for state and local employers as well as private sector employers in recent years. While responsibilities are slightly different, with state governments operating Medicaid and other programs, both public and private sectors are addressing obesity in similar ways.
State Government EmployersIn 2004, South Dakota Governor Mike Rounds along with the State Employee Health Plan introduced a wellness program called HealthySD.gov. The statewide program assists 23,000 employees, COBRA participants and retirees, along with their covered spouses who participate in the State Employee Health Plan in setting physical activity and nutrition goals, assessing their fitness and nutrition habits and monitoring their success in the program. Those who join HealthySD.gov can be reimbursed for some of their medical out-of-pocket expenses such as deductibles and co-payments along with membership fees to fitness and nutrition centers. Participants can receive up to $300 per plan year in a Health Risk and Wellness Account. Additional incentives for employees and spouses include a $50 account bonus for completing the health screening and health risk questionnaire, and $100 bonus for actively participating in the online wellness program and reaching at least one goal.In 2004, Arkansas Governor Mike Huckabee introduced Healthy Arkansas and the Healthy Weight Initiative. As part of Healthy Arkansas, state employees receive a $20 health insurance premium reduction if they participate in a voluntary health risk survey, and they are advised about how their health behavior could affect their health insurance premiums in the future. The state also began offering nutrition counseling and smoking cessation aids to Medicaid recipients and state employees. In the governor’s office, workers are offered “walking breaks” instead of smoking breaks. The Arkansas Fitness Challenge, a component of the Initiative, is a contest between two teams of employees. The pilot project had teams from the Arkansas Department of Health and Arkansas Blue Cross and Blue Shield participate in cardiovascular exercises for three months. Results showed that during the contest respondents reported improved health, increased days per week of exercise, and lowered their blood pressure, cholesterol, weight and blood sugar.Delaware’s Health Rewards—a partnership between Blue Cross Blue Shield and Cardio Kinetics—conducted a pilot study of the fitness of 100 randomly selected state employees. Participants were given an extensive initial health assessment. Participants received physician referrals when appropriate and advice on how to improve their short- and long-term health. Officials estimate the pilot program has saved the state more than $62,000 in health care costs for the 100 participants, and they expect to see additional long-term savings because the participants improved their cardiovascular capacity, lost weight and quit smoking. The program has since been expanded to 1,500 employees and will save an estimated $1 million annually.4 Delaware officials report the following results of the pilot project:
n
n
n
n
n
n
n
n
n
n
n
n
n
�
55 of the participants who originally reported their fitness activity as sedentary were active at least three times per week;two of the five smokers who attended the assessment quit smoking; andthe number of emergency room visits for the pilot group decreased significantly compared to a control group.
Private Sector EmployersIn 2003, in response to growing need by member organizations, the National Business Group on Health created the Institute on the Costs and Health Effects of Obesity. The institute is a two-year project aiming to reverse obesity trends and their harmful effects on U.S. businesses, worker health and productivity.
Union Pacific Railroad’s Health Track program, including its Reduce Obesity Now initiative, aims to improve its employees’ physical and mental health through lifestyle change and risk reduction. The company offers Health Track to 47,000 employees and has shown a 34 percent drop in medical claim costs attributable to preventable chronic disease risk factors over the last 10 years. Union Pacific also determined that some of these same risk factors (stress, overweight and over age 45, tobacco use and perceived health status) are predictors of safety incidents on the job. Union Pacific Railroad received the Washington Business Group on Health President’s Healthy Weight, Healthy Lifestyles Award for Health Track in 2005.5 Motorola offers wellness and work/life programs to its 45,000 U.S. employees and beneficiaries. Motorola invests $6 million annually in wellness and work/life programs, and has shown:
for every $1 invested in wellness benefits, $3.93 were saved; an 2.4 percent increase in annual aggregate health care costs for participating employees, compared to an 18 percent increase for non-participants; and$6.5 million annual savings in medical expenses for medical diagnoses such as obesity, hypertension, and stress compared with non-participants.
What Legislators Can Do About ObesityWhile businesses and employers have been busy implementing programs and worksite policies to improve health, legislatures have been looking at ways state laws can support these efforts. Much of the effort has been very recent, coming in the 2004 and 2005 legislative sessions.
Supporting Healthy BehaviorsWashington Senate Bill 5066 (2005-pending) would acknowledge that the Legislature supports and promotes healthy lifestyles and that lowering the cost of joining fitness clubs and organizations will remove barriers for people becoming physically active. It modifies the taxation of personal training services.
Promoting Physical Activity Through Alternative CommutingMinnesota House File 1011 (2005-pending) would require the commissioners of transportation, health, public service and interested non-profit agencies to establish and operate an employee transportation program promoting bicycle commuting by state employees. The bill would tie state agencies’ capital improvement plans to participation in the program and promoting alternative transportation and physical activity. It would also require the state to provide facilities to promote bicycle commuting such as indoor or sheltered bike parking, showers and dressing areas for bikers, and installation of bicycle racks for state employees traveling by bicycle.
Tax Incentives New Jersey Assembly Bill 3715 (2005-pending) would allow a business tax credit and gross income tax credit for employer expenditures providing physical fitness benefits to employees. Under the bill, employers could write off 10 percent of the cost of establishing a fitness facility, financially supporting an employee athletic team, paying for an employee’s health club dues, hiring staff to educate or counsel employees on nutrition, fitness and health, or the cost of a financial incentive for employees to be active.
º
º
º
n
n
º
º
º
n
n
n
Indiana House Bill 1781 (2005-pending) would provide a state tax credit to employers who implement worksite health promotion programs for their Indiana employees. Virginia House Bill 1818 (2005-pending) would provide a tax credit to employers accommodating employees who bicycle to work to include the purchase of bike racks and installing showers in business facilities. Under the bill, any individual who rides his bicycle to and from work at least 10 days per month would be entitled to a tax credit of $15 per month.
ConclusionLegislators have many tools in their arsenal for supporting businesses’ and employers’ efforts to address obesity, and its related healthcare costs and effects on worker productivity. Legisla-tors have already introduced a number of bills designed to encourage employers to promote worksite wellness, while balancing profitability in the marketplace. Worksite wellness has been shown to be a wise investment, and promoting good health among employees can help curtail health care costs associated with obesity.
Legislators can:
work with state agencies, such as the public health agency, to establish worksite wellness programs that focus on employee physical activity, nutrition and healthy weight maintenance; assist businesses with limitations on liability for promoting physical activity by creating reasonable liability waivers to protect workplaces and other institutions that provide time, facilities, equipment or support for physical activity from frivolous lawsuits stemming from activity-related injuries;adopt nutrition standards in state workplaces and encourage businesses to follow them, including directing agencies responsible for food procurement, including cafeterias, food service and vending machines, to set standards that at least 50 percent of the food served meets guidelines for healthy food choices; establish new standards for state construction that incorporate designs that encourage and facilitate physical activity;create a reward program for businesses and employers that meet and exceed efforts to promote good health and address obesity in the workplace or community;support private employer health promotion efforts by working with insurance companies to offer premium breaks for employers that enact preventive health and wellness initiatives, and also provide incentives for health maintenance organizations and health care providers to take more active roles in making prevention a priority; andoffer pre-tax, flexible spending options to state employees and/or private sector employees to pay for eligible health and wellness related expenses.
n
n
n
n
n
n
n
n
n
End NotesKaiser Family Foundation. Employer Health Benefits 2004 Annual Survey. Available at www.kff.org/insurance/7148. Roland Sturm, UCLA/RAND Managed Care Center for Psychiatric Disorders, The Effects of Obesity, Smoking and Drinking on Medical Problems and Costs, Health Affairs, March/April 2002.Prevention Makes Common Cents: Estimated Economic Costs of Obesity to U.S. Business, DHHS, 2003.The Council of State Governments, 2004 Innovation Awards Program. Retrieved from http://www.csg.org/CSG/Programs/innovations/2004/default.htm on May 10, 2005.Press Release “National Business Group on Health Announces Winners of its President’s Awards for Excellence in Health Care Benefits.” Retrieved from http://www.wbgh.org on May 9, 2005.
1�2�
3�4�
5�
This publication was prepared by Michael Fierro and Debra Lightsey of Bearing Point, Inc. for The Council of State Governments’ (CSG) Healthy States Initiative. Funding for this publication was
provided by the U.S. Department of Health and Human Services, Centers for Disease Control and Prevention (CDC) under Cooperative Agreement Number U38/CCU424348. Its contents are the
responsibility of the authors and do not necessarily represent the official views of CDC or CSG.

rom the Statehouse to the County Seat
IntroductionIn the balance between personal responsibility and social responsibility, commu-nity is the fulcrum. The best intentions to eat well can be thwarted when produce is unavailable or unaffordable. Families who don’t feel safe to ride a bike or play at the park may be found sitting on the couch. And citizens who feel alone in their desire to change health habits—or who don’t know where to start—may remain stuck in behaviors that cause obesity and chronic diseases.
Communities can improve these environments, and legislators can help. State leg-islators are leaders in their communities, serve as their voices in the statehouse and continue to influence the health of their hometowns in profound ways. For example, state legislators can:
support or create comprehensive community campaigns;encourage collaboration among state land use, transportation and health experts;support walkable and bikeable transportation alternatives; andsupport access to healthy foods in communities.
The Role of Communities The rise in obesity over the last 20 years represents a cultural shift. The choices we make as in-dividuals are influenced by our community surroundings, from our neighbors’ attitudes to bus routes. For example:
Building communities for easy automobile access discourages safe walking and biking. People living in low-density counties walk less, weigh more and are more likely to be obese or have hypertension than those living in denser counties.1 Access to sidewalks makes people 28 percent more likely to be physically active. Walking trails are even more effective—access to trails leads to a 55 percent increase in physically active people.2 Walking groups, buddy systems and other social supports increase physical activity time by 44 percent and frequency of physical activity by 20 percent. These programs improve fitness levels, lower percentage of body fat, increase knowledge about exercise and improve confidence in the ability to exercise.3 States with a higher number of fast food restaurants per resident and higher number of fast food restaurants per mile had higher obesity prevalence,4 while access to supermarkets has been shown to increase fruit and vegetable consumption.
n
n
n
n
n
n
n
n
State Policies that Support Healthy Communities

Recent Community Trends on ObesityCommunity-wide CampaignsBroad-based, community-wide campaigns to increase physical activity—including media messages, self-help groups, and community events—are proven to increase the level of physical activity and the fitness of both adults and children.3
California’s Project LEAN is a program of the California Department of Health Services and the nonprofit Public Health Institute to increase healthy eating and physical activity. The program uses a multi-faceted, regional, grassroots approach to improving eating and physical activity. Among its successes:
Seventy-eight percent of low-income Latina mothers in the north central coast Project LEAN region reported eating five servings of fruits and vegetables per day, up from 58 percent. Women attended community classes, tasted fruits and vegetables at their grocery stores, saw the 5-A-Day message on appointment cards from their doctors and heard local radio personalities promote the message on their favorite radio stations.In San Jose, fruit and vegetable intake increased by an average of more than one serving per day, and produce purchases increased from an average of $242 to $629, or 260 percent, among Jobs Corps students over six weeks. The program included taste tests, educational materials, provider education, media communications and fruit and vegetable policies in the Jobs Corps cafeteria.
Black Churches United for Better Health 5-A-Day Project worked with 50 black churches in North Carolina to improve healthy eating. Each intervention church identified a Nutrition Action Team to plan and implement church activities. The program used lay health advisers to provide support to church members as they were encouraged to increase fruit and vegetable consumption. Results suggest that the program was highly successful in achieving increased fruit and vegetable consumption in a rural African American population.
Community and Street Scale Urban DesignCommunity design is significantly associated with physical activity. In fact, the gold-standard Community Guide to Preventive Services recently recommended both community- and street-scale urban design and land use approaches as effective interventions to increase physical activity. Based on this association, states and communities are developing policies that promote more mixed-use zoning , street connectivity and residential density as interventions that can have lasting public health benefits.3 Local governments typically have jurisdiction for community zoning and planning, and state governments often provide incentives for local actions that promote health.
As part of efforts to help stem the rising tide of diabetes among Hispanic Americans living in Arizona-Mexico border communities, the Border Health Strategic Initiative fosters community-based approaches to diabetes prevention and control. Community groups met regularly for more than two years, focusing primarily on policies that support physical activity and healthier nutrition through community design. By collaborating with planning commissions, parks and recreation and private companies, two grants were secured to support new walking trails. The trails were coupled with efforts to change the community’s culture in other ways, including improved physical education and food options in elementary schools and grocery store promotion of healthier foods.6 St. Louis University and the Missouri Department of Health worked together to promote physical activity programs in rural communities in the Bootheel and Ozark areas of Missouri. In a comprehensive campaign, community coalitions formed walking clubs, built walking trails, started exercise classes in community churches and organized special events to promote physical activity. Forty-two percent of community residents used walking trails established through the program and almost 60 percent of trail users reported increasing their physical activity. Women and people with lower educational levels—groups at high risk for physical inactivity—may be especially responsive to walking trails.7
The Robert Wood Johnson Foundation’s Active Living by Design program encourages changes in design, transportation and policies to promote active living in 25 community partnerships across the country. These communities bring together diverse partners from public health, city planning, transportation, architecture and other fields to promote policies, planning and physical projects that make active communities possible.
Community Access to Healthy FoodsStates are taking action to make healthy food more accessible in communities and schools, and to better inform consumers about the foods they buy.
North Carolina’s The Winner’s CircleSM Healthy Dining Program promotes healthy foods anywhere people eat away from home. The Department of Health and Human Services trains local health coalitions to
n
º
º
n
n
n
n
n
�

�
recruit restaurants, worksite cafeterias, vending machines and other eating venues and analyzes their menus to identify and label healthy foods. Team Nutrition and the Department of Public Instruction have extended the program to public schools in an effort to label and actively promote healthy meals and side items throughout the school system. NC Prevention Partners, a nonprofit, works with chain restaurants to identify healthy menu items.Washington state is working with food assistance programs to address the link between hunger and obesity. The Access to Healthy Food Coalition includes state and local government, private industry (restaurants, distributors, growers/packers, vending machine distributors, supermarkets and food/beverage manufacturers) and nonprofits (food banks, health coalitions, etc.). The coalition works to improve access to healthy foods in food banks and communities. It also works with growers and emergency food distributors to move healthy foods from the fields to needy families as soon as it is available.
What Legislators Can Do about ObesityLegislators across the country are addressing obesity in communities through legislation in a number of ways.
Create comprehensive community campaignsFlorida Laws, Chapter #338 (2004-enacted) requires the Department of Health to promote healthy lifestyles and reduce the prevalence of overweight and obesity in the state through public awareness campaigns; technical assistance, training and resources on healthy lifestyles and chronic diseases; and development, implementation and use of all available research methods to collect data and track the incidence and effects of weight-gain, obesity and related chronic diseases. Maine House Bill 112 (2005-not enacted) would have established the Maine Obesity Prevention Fund for coordinated school health programs, annual assessment of BMI for students, increased availability of fresh produce in schools, media campaigns encouraging healthy diets and physical fitness.
Encourage collaboration among state land use, transportation and health expertsCalifornia Senate Concurrent Resolution 4 (2005-passed) encourages leadership in all branches and levels of government; local action by communities; initiatives by schools and workplaces; increased recreation and physical activity that is accessible for all Californians; expanded healthy food options in restaurants, markets and homes; and increased emphasis on health education and prevention of obesity and diabetes.Washington Senate Bill 5186 (2005-enacted) directs county and city comprehensive plans to use urban planning approaches that promote physical activity. Transportation planning in cities, towns and counties should incorporate policy and infrastructure changes that promote non-motorized transit.
Support walkable and bikeable transportation projectsMassachusetts Acts, Chap. #291 (2004-enacted) provides funding for specific trails, rail trails, multi-use pathways and bike paths. It defines rail trails as a property converted from the former use as a railroad right-of-way to a use as a publicly owned, improved and maintained corridor for bicycle, pedestrian and other non-motorized public transportation, recreation and associated purposes.Florida House Bill 603 (2005-not enacted) would have required incorporation of bicycle and pedestrian ways into state, regional and local transportation plans and programs; and established bicycle lanes if there were sufficient right-of-way whenever there was construction, reconstruction or other change of any state transportation facility.Illinois House Bill 467 (2005-pending) would require the commuter rail division to adopt rules to allow commuters to bring bicycles onto trains. Under the bill, bicycles would—at a minimum—be allowed on trains during non-rush hours and on weekends.
Support access to healthy food in communitiesPennsylvania Laws, Act #22 (2004-enacted) creates a statewide development program directed at supermarkets, specifically targeted at underserved urban and rural areas. Vermont House Joint Resolution 47 (2004-enacted) supports the establishment and expansion of community, neighborhood and youth gardens and increases their accessibility to disadvantaged population groups. Oregon Senate Bill 289 (2005-pending) would appropriate moneys to the Department of Human Services for provision of fruits and vegetables from farmers’ markets to individuals eligible for the Women, Infants and Children Program.
n
n
n
n
n
n
n
n
n
n
n

ConclusionLike politics, environmental change is local. By supporting community campaigns and surroundings that pro-mote physical activity and nutrition, state legislators can improve their hometowns and their neighbors’ health. These same actions can promote the economic health of communities and states, both by creating economic development and other benefits, and by preventing costly chronic diseases consuming state budgets.
Legislators can:
Support or create comprehensive community campaigns. Through appropriations or other legislation, lawmakers can provide resources and direction for statewide or smaller campaigns that support community-level involvement in promoting healthy behaviors through proven and promising strategies.Consider health consequences of infrastructure decisions. Transportation, business licensing, and land use decisions often have health consequences, and those consequences too often are not taken into account. Lawmakers can ensure that health consequences are part of legislative and regulatory decisions that affect community structure.Encourage local zoning and planning decisions that promote health. While much of the authority to regulate communities lies with local government, state lawmakers can provide incentives and forums for improving health through these important local decisions. Encourage collaboration among state agencies. Bringing together parks, recreation, education, transportation, public safety and public health experts in the state can have a powerful impact on the quality and coordination of state policies affecting community health.Be a champion for health-promoting communities. As leaders of their hometowns, lawmakers can be powerful advocates for improving surroundings to promote health.
End NotesEwing, R., Schmid, T., Killingsworth, R., et al. (2003). Relationship between urban sprawl and physical activity, obesity, and morbidity. American Journal of Health Promotion, 18, 47-57.Humpel, N. et al. (2002), Environmental Factors Associated with Adult’s Participation in Physical Activity. American Journal of Preventive Medicine. 22; 188-199.Task Force on Community Preventive Services, (2005). Physical Activity. In The Guide to Community Preventive Services: What Works to Promote Health? (S. Zaza, P. Briss, and K. Harris, eds.). Oxford University Press, pp 80-113.Maddock, J. (2004). Relationship between obesity and the prevalence of fast food restaurants: state-level analysis. American Journal of Health Promotion. 19(2), 137-143.Frank, LD, Schmid, TL, Sallis, JF, Chapman, J & Saelens, B. (2005). Linking objective physical activity data with objective measures of urban form, American Journal of Preventive Medicine. 28 (2S2), 117-125Zuckerman, M. & Zuckerman, E. (2004), Special action groups for policy change and infrastructure support to foster healthier communities on the Arizona-Mexico border. Public Health Reports. 119 (1), 40-47.CDC, Preventing Obesity and Chronic Diseases through Good Nutrition and Physical Activity. http://www.cdc.gov/nccdphp/pe_factsheets/pe_pa.htm
n
n
n
n
n
1�
2�
3�
4�
5�
6�
7�
This publication was prepared by Michael Fierro and Debra Lightsey of Bearing Point, Inc. for The Council of State Governments’ (CSG) Healthy States Initiative. Funding for this publication was
provided by the U.S. Department of Health and Human Services, Centers for Disease Control and Prevention (CDC) under Cooperative Agreement Number U38/CCU424348. Its contents are the
responsibility of the authors and do not necessarily represent the official views of CDC or CSG.

Trendsand
Policy Solutions
in
IntroductionAgriculture policy in the United States is a central issue in the national debate on obesity. The United States has an abundance of food and food options, the least expensive food in the world and Americans spend only about 10 percent of their disposable income on food.1
While growers and food companies might make an easy target to blame for Americans’ unhealthy eating habits, the fact is individuals are choosing unhealthy diets and not meeting dietary recommenda-tions. In 2002, Americans spent almost half their total food budget on
food away from home, an increase from 27 percent in 1962.2 Food eaten away from home tends to be higher in calories than food prepared at home. Current federal law does not require fast food and restaurant foods to include the mandatory labeling found on food purchased in stores. To better educate consumers on the food they are eating, some states are working to implement voluntary labeling, and some restaurants voluntarily supply nu-trition information to inform consumers.
Since agriculture is a cornerstone of the U.S. economy, drastic changes in regulation or subsidies could have serious consequences. American food companies, including fast food, have begun responding to consumer demand and changing tastes by offering healthier options. State legislators have many options to support a healthy agricultural economy while balancing the needs of their residents’ health. While the majority of recent food policy attention has focused on schools, legislators can also work to:
provide more food content information to consumers;implement higher nutritional standards in government food programs; andsupport local agriculture by promoting in-state-grown fruits and vegetables.
The Role of Agriculture, Food Supply and NutritionAgriculture, food supply and nutrition are integral parts of the obesity epidemic solution. The federal government invests billions of dollars in the agriculture sector, which is chan-neled partly through state governments and partly to farmers. Jurisdiction and respon-sibility for nutrition assistance programs, food stamp programs, the Women, Infant and Children (WIC) program and national nutritional guidelines rest with the U.S. Department of Agriculture. In addition, USDA regulates the nation’s food supply and suppliers. Improv-ing American diets requires addressing supply—through agriculture and food policy—and creating demand, making eating healthy foods everyone’s individual responsibility.3
n
n
n
ultivating Health in a Healthy Economy:Agriculture and Food Supply
Recent Agriculture, Food Supply and Nutrition Trends on ObesityFood producers, suppliers, vendors and related government agencies have sought to improve health, consumer knowledge and consumption of locally grown produce in recent years through a variety of interventions. While some are not directly targeting obesity, much can be done outside the scope of obesity prevention to help consumers eat healthy foods.
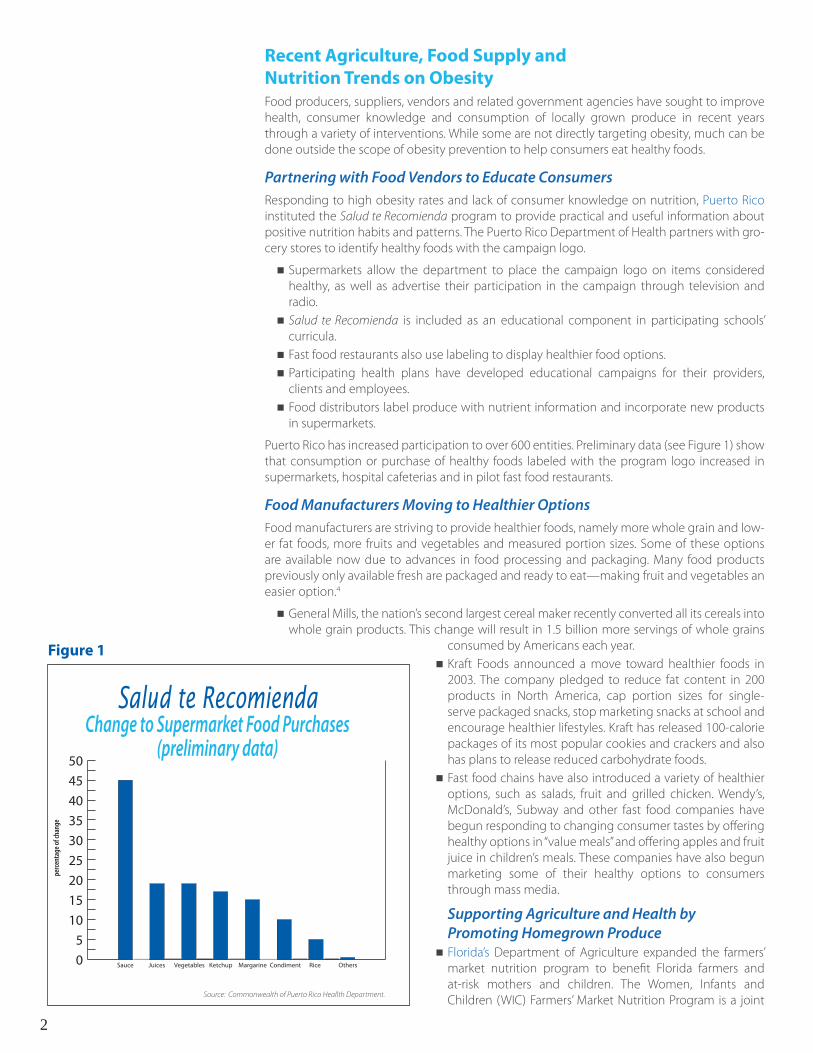
Partnering with Food Vendors to Educate ConsumersResponding to high obesity rates and lack of consumer knowledge on nutrition, Puerto Rico instituted the Salud te Recomienda program to provide practical and useful information about positive nutrition habits and patterns. The Puerto Rico Department of Health partners with gro-cery stores to identify healthy foods with the campaign logo.
Supermarkets allow the department to place the campaign logo on items considered healthy, as well as advertise their participation in the campaign through television and radio. Salud te Recomienda is included as an educational component in participating schools’ curricula. Fast food restaurants also use labeling to display healthier food options. Participating health plans have developed educational campaigns for their providers, clients and employees. Food distributors label produce with nutrient information and incorporate new products in supermarkets.
Puerto Rico has increased participation to over 600 entities. Preliminary data (see Figure 1) show that consumption or purchase of healthy foods labeled with the program logo increased in supermarkets, hospital cafeterias and in pilot fast food restaurants.
Food Manufacturers Moving to Healthier OptionsFood manufacturers are striving to provide healthier foods, namely more whole grain and low-er fat foods, more fruits and vegetables and measured portion sizes. Some of these options are available now due to advances in food processing and packaging. Many food products previously only available fresh are packaged and ready to eat—making fruit and vegetables an easier option.4
General Mills, the nation’s second largest cereal maker recently converted all its cereals into whole grain products. This change will result in 1.5 billion more servings of whole grains
consumed by Americans each year.Kraft Foods announced a move toward healthier foods in 2003. The company pledged to reduce fat content in 200 products in North America, cap portion sizes for single-serve packaged snacks, stop marketing snacks at school and encourage healthier lifestyles. Kraft has released 100-calorie packages of its most popular cookies and crackers and also has plans to release reduced carbohydrate foods. Fast food chains have also introduced a variety of healthier options, such as salads, fruit and grilled chicken. Wendy’s, McDonald’s, Subway and other fast food companies have begun responding to changing consumer tastes by offering healthy options in “value meals” and offering apples and fruit juice in children’s meals. These companies have also begun marketing some of their healthy options to consumers through mass media.
Supporting Agriculture and Health by Promoting Homegrown Produce Florida’s Department of Agriculture expanded the farmers’ market nutrition program to benefit Florida farmers and at-risk mothers and children. The Women, Infants and Children (WIC) Farmers’ Market Nutrition Program is a joint
n
n
n
n
n
n
n
n
n
�
Figure 1
0
5
10
15
20
25
30
35
40
45
50
perce
ntag
e of c
hang
e
Sauce Juices Vegetables Ketchup Margarine Condiment Rice Others
Source: Commonwealth of Puerto Rico Heallth Department.
Salud te Recomienda Change to Supermarket Food Purchases
(preliminary data)

program of the Florida Department of Agriculture and Consumer Services, the Florida Department of Health and the U.S. Department of Agriculture that began in Florida in 1998. The program provides pregnant, postpartum or breastfeeding women, and children between the ages of one and five who participate in the WIC program with nutritional information on the importance of including fresh fruits and vegetables in their diet. Each recipient also receives $20 worth of coupons that can be exchanged for nutritious fresh fruits and vegetables. The coupons can be used only at authorized local community farmers’ markets to purchase fresh produce from Florida farmers. The program also provides farmers with additional consumers for their fresh produce. In 2002, more than 26,000 clients received coupons, which were redeemed for more than $200,000 in produce supplied by 145 participating farms. 5
The North Carolina Farm to School Program was formed in 1997 through a partnership between the Department of Defense and the Markets and Food Distribution Division of the North Carolina Department of Agriculture and Consumer Services. All school districts in North Carolina are eligible to participate in the North Carolina Farm to School Program. About 60 school districts participated in 2004.
What Legislators Can Do about ObesityState legislators have focused their attention on innovative ways to implement agriculture and food policies that support healthy eating. Changes to advertising, rules in government food programs and food labeling policies to inform consumers have been put in place.
AdvertisingCalifornia Senate Joint Resolution 29 (2004-enacted) calls on the Federal Trade Commission to develop and implement nutrition standards for children and to ensure that advertising time is reserved during TV programs that have a significant youth audience to encourage fruit and vegetable consumption and physical activity. The resolution also calls on food and beverage companies, restaurants, retail stores, advertising agencies, sports and entertainment industries and print, broadcast and Web-based media in California to adhere to a voluntary code of practice—developed by experts—that would contain guidelines and standards for responsible food and beverage advertising and marketing aimed at children.Maine Senate Bill 263 (2005-not enacted) would have directed school boards to prohibit advertising of foods and beverages other than healthy foods and beverages on school grounds after September 2007.
Food SubsidiesSouth Dakota House Bill 1308 (2004-enacted) implements a food sales tax refund program led by the Department of Social Services to provide sales tax refunds on food purchases made in accordance with bill provisions to South Dakota families who are at or below 150 percent of the federal poverty level. The bill does not refund taxes on purchases of alcohol, tobacco, soft drinks, candy and prepared foods. Colorado House Bill 1129 (2002-enacted) requires the State Board of Health to promulgate rules to implement a farmers’ market nutrition program to distribute to the Women, Infants, and Children Program participants, contingent upon state funding.Illinois Senate Bill 76 (2003-enacted) creates the Nutrition Outreach and Public Education Act and authorizes grants to community-based organizations for outreach activities. It also establishes a nutrition outreach and public education program within the Department of Public Health to enroll targeted populations in federal food and nutrition assistance programs. Connecticut Public Act 04-222 (2004-enacted) requires the commissioner of administrative services, when purchasing or contracting for the purchase of dairy products, poultry, eggs, fruits or vegetables to give preference to those products grown or produced from within the state, when such products are comparable in cost. It also requires the commissioner to establish and administer a program—within available resources—to certify grocery and food stores as “Connecticut Farm Fresh Markets,” and restaurants as “Connecticut Farm Fresh Restaurants.”
n
n
n
n
n
n
n
Many states have passed or consid-ered legislation to limit the liability of food manufacturers, sellers, distribu-tors and marketers for legal claims resulting from an individual’s obesity, weight gain or health conditions re-lated to obesity. Fifteen states have enacted legislation limiting the food industry’s liability.6
Food Industry Liability Limitations

Promoting Locally Grown Fruits and VegetablesNew Hampshire Senate Concurrent Resolution 1 (2005-passed) establishes a farm viability task force, which includes agricultural agencies and all agricultural interests, and suggests that the state should promote the positive attributes of New Hampshire agriculture by highlighting successful activities and groups such as community-supported agriculture and farmers’ markets. New York Chaptered Law 248 (2004-enacted) establishes farm, apple and cuisine trails. A farm trail is defined as a group of food producers who sell complementary food products, are in close proximity, sell their products in a cooperative manner and use maps and other directional devices to market their products. Apple trails are similar groups that sell apples and other fruit products, while cuisine trails sell unusual, unique or hard to find fresh farm and food products. The law requires the state Department of Agriculture to market the trails.
Labeling and Consumer InformationCalifornia Senate Bill 281 (2005-pending) establishes the 5 A Day for Better Health program within the Department of Health Services to promote public awareness of the need to increase the consumption of fruits and vegetable as part of a low-fat, high fiber diet. It requires the department to develop a program that encourages schools to provide fruits and vegetables to pupils and provides requirements for contracts with qualified organizations for services to implement this program.
ConclusionMany options are available to state legislators to achieve agriculture policy change locally. States can promote healthy eating in addition to adding to or strengthening current USDA or other federal guidelines on farming and food production. States also benefit from promoting and delivering fresh local fruits and vegetables to low income, underserved or other populations.
Legislators can:
work with state agencies responsible for agriculture, education, health and economic development to educate consumers on healthy eating;provide resources and leadership to promote restaurants’ and grocery stores’ participation in voluntary food and menu labeling programs;implement higher nutritional standards in government food programs; and support local agriculture by promoting partnerships between local growers and schools, and publicly-funded food programs to provide fruits and vegetables and information on healthy eating to improve consumers’ access to fresh and healthy foods.
n
n
n
n
n
n
End NotesPandemic obesity: agriculture’s cheap food policy is a bad bargain. (Business and Nutrition), James E. Tillotson, Nutrition Today Sept-Oct 2003 v38 i5 p186(5).Variyam, Jayachandran N., Nutrition labeling in the food-away-from-home sector: an economic assessment. Economic research report, United States Department of Agriculture, Economic Research Service; Number 4.Variyam, Jayachandran N., The Price is Right, Amber Waves, United States Department of Agriculture, Economic Research Service; Volume 3, Issue 1. February 2005.Variyam, Jayachandran N., The Price is Right, Amber Waves, United States Department of Agriculture, Economic Research Service; Volume 3, Issue 1. February 2005.Florida Department of Agriculture and Consumer Services. Retrieved from www.florida-agriculture.com/consumers/wic.htm. On May 5, 2004.Arizona, Colorado, Florida, Georgia, Idaho, Illinois, Louisiana, Maine, Michigan, Missouri, New Hampshire, South Dakota, Tennessee, Utah, and Washington
1�
2�
3�
4�
5�
6�
This publication was prepared by Michael Fierro and Debra Lightsey of Bearing Point, Inc. for The Council of State Governments’ (CSG) Healthy States Initiative. Funding for this publication was
provided by the U.S. Department of Health and Human Services, Centers for Disease Control and Prevention (CDC) under Cooperative Agreement Number U38/CCU424348. Its contents are the
responsibility of the authors and do not necessarily represent the official views of CDC or CSG.

Trendsand
Policy Solutions
in
State Legislative Information Related to Nutrition and Physical Activityhttp://apps.nccd.cdc.gov/DNPALeg/
Search this CDC Web site for state-level bills related to nutrition and physical ac-tivity.
Links to State and Territorial Health Officialswww.astho.org/index.php?template=regional_links.php
Find state and territorial health depart-ment officials at this Association of State and Territorial Health Officials Web site.
State-Level Estimated Costs of Obesitywww.cdc.gov/nccdphp/dnpa/obesity/economic_consequences.htm
Estimated costs associated with adult obesity for each state are listed on this CDC Web page.
State-Based Physical Activity Program Overviewhttp://apps.nccd.cdc.gov/DNPAProg/
This CDC Web site provides information about physical activity programs involv-ing state departments of health. Use this site to research programs, gather ideas and share information.
Obesity Trendswww.cdc.gov/nccdphp/dnpa/obesity/trend/index.htm
This CDC Web page is a rich source of statistics about the prevalence of obesity among adults, children and adolescents in the states.
ResourcesState-by-State Information on the Web
Health Recommendations for the Public
Overweight and Obesity: What You Can Dowww.surgeongeneral.gov/topics/obesity/calltoaction/fact_whatcanyoudo.htm
Recommendations from the U.S. Surgeon General for the public about how physical activity can help people combat obesity.
Publications from the President’s Council on Physical Fitness and Sportshttp://www.fitness.gov/council_pubs.htm
Includes a wide variety of downloadable publications written for the general pub-lic about how to get or stay healthy, adopt more healthy eating habits and increase physical activity.
MyPyramid.govwww.mypyramid.gov
This U.S. Department of Agriculture Web site can be used to help individuals make smart food choices and find the right bal-ance between food and physical activity.
Dietary Guidelines for Americans 2005www.healthierus.gov/dietaryguidelines
Produced by the U.S. Department of Health and Human Services and the U.S. Depart-ment of Agriculture, the dietary guidelines provide science-based advice to reduce risk for major chronic diseases through diet and physical activity.
Links to Nutrition and Physical Activity Publications and Web Resourceswww.cdc.gov/nccdphp/dnpa/obesity/ resources.htm
This CDC Web site contains links to many resources designed to provide nutrition and physical activity advice for the general public.

Policy Reports and RecommendationsA Nation at Risk: Obesity in the United States—A Statistical Sourcebookhttp://www.rwjf.org/files/publications/other/AH_NationAtRisk.pdf
Produced by the American Heart Associa-tion and the Robert Wood Johnson Foun-dation, the sourcebook shows how preva-lent obesity has become and examines the factors that contribute to patterns of unhealthy eating and insufficient physical activity.
Designing and Building Healthy Placeswww.cdc.gov/healthyplaces
This CDC Web site provides a wealth of resources and policy recommendations related to the link between health and the environment, including the “built” environ-ment.
F as in Fat: How Obesity Policies are Failing in Americahttp://healthyamericans.org/reports/obesity
A publication of the Trust for America’s Health, this report describes state-by-state obesity levels, state school policies on nu-trition and health education and commu-nity-focused initiatives in those states.
Health Plans Emerging as Pragmatic Partners in the Fight Against Obesity www.nihcm.org/ObesityReport.pdf
Produced by The National Institute for Health Care Management, this report ex-amines eleven large health plans and their efforts to fight obesity.
Healthy Workforce 2010: An Essential Health Promotion Sourcebook for Employers, Large and Smallwww.prevent.org/publications/Healthy_Work-force_2010.pdf
Funded by the Robert Wood Johnson Foun-dation, this sourcebook is designed to help employers understand how investments in worksite health promotion/disease preven-tion can benefit both employers and em-ployees.
Preventing Obesity and Chronic Disease through Good Nutrition and Physical Activityhttp://www.cdc.gov/nccdphp/pe_factsheets/pe_pa.htm
Produced by the CDC, this Web page con-tains general statistics regarding obesity and the economic implications of obesity as well as promising approaches and exam-ples of state programs for the prevention of obesity.
Straight Talk about Obesity and Healthwww.prevent.org/publications/Obesity%20Impact-v2.pdf
This issue brief from Partnership for Preven-tion summarizes the evidence about over-weight, obesity, the health consequences of these conditions and the associated eco-nomic costs.
State Employee Wellness Initiativeshttp://www.nga.org/cda/files/05WELLBRIEF.pdf
Produced by the National Governor’s As-sociation, this issue brief outlines the major wellness initiatives implemented by gover-nors in recent years.
The Guide to Community Preventive Services (Community Guide)/Physical Activitywww.thecommunityguide.org/pa/default.htm
Provides evidence-supported recommen-dations about population-based interven-tions to increase levels of physical activity.
The Obesity Epidemic— How States Can Trim the Fatwww.nga.org/cda/files/OBESITYIB.pdf
Produced by the National Governor’s As-sociation, this issue brief outlines programs and policies states can use to address the causes of the obesity epidemic.
The Surgeon General’s Call to Action to Pre-vent and Decrease Overweight and Obesitywww.surgeongeneral.gov/topics/obesity
Addresses prevention and treatment of overweight and obesity in the United States as a major public health problem.
This publication was prepared by Michael Fierro and Debra Lightsey of Bearing Point, Inc. for The Council of State Governments’ (CSG) Healthy States Initiative. Funding for this publication was
provided by the U.S. Department of Health and Human Services, Centers for Disease Control and Prevention (CDC) under Cooperative Agreement Number U38/CCU424348. Its contents are the
responsibility of the authors and do not necessarily represent the official views of CDC or CSG.
Trendsand
Policy Solutions
in
For state legislators looking for methods to combat the obesity epidemic among adults, there are many policy arenas to address, many possible actions to take and many roles to play.
Help public and private sector employees fight obesity by:working with state agencies to establish worksite wellness programs that focus on employee physical activity, nutrition and healthy weight maintenance;assisting businesses with limitations on liability for promoting physical activity by creating reasonable liability waivers to protect workplaces and other institutions that provide time, facilities, equipment or support for physical activity from frivolous lawsuits stemming from activity-related injuries;adopting nutrition standards in state workplaces and encouraging businesses to follow them;working with agencies responsible for food service—including cafeterias, food service and vending machines—to set standards that at least 50 percent of the food served meets guidelines for healthy food choices;establishing new standards for state construction that incorporate designs encouraging and facilitating physical activity;creating an award program for businesses and employers that meet or exceed efforts to promote good health and address obesity in the workplace or community;supporting private employer health promotion efforts by working with insurance companies to offer premium breaks for employers that enact preventive health and wellness initiatives; andoffering pre-tax, flexible spending options to state employees and/or private sector employees to pay for eligible health and wellness related expenses.
Give communities the support they need to encourage more active living by:
supporting or creating comprehensive community campaigns to promote healthy behaviors;considering the health consequences of legislative and regulatory decisions that affect community planning, land use and infrastructure;bringing together parks, recreation, education, transportation, public safety and public health experts to coordinate state policies affecting community health; andbecoming a champion for improving community environments to promote health.
¸
¸
¸
¸
¸
¸
¸
¸
¸
¸
¸
¸
What Legislators
Can Do About Adult
Obesity
An Action Checklist
Encourage the health care system to fight obesity more effectively by:
encouraging the use of technology and innovative tools for providers and consumers to maintain a healthy weight or support weight loss;providing incentives for health maintenance organizations and health care providers to take more active roles in making prevention a priority;examining and drawing attention to costs to state government and state economies from obesity-related illnesses and lost productivity; convening health care and government agencies to implement obesity prevention and management initiatives;working to establish worksite wellness programs for state and private employees; andconsidering including nutrition counseling and physical activity counseling in minimum insurance coverage requirement policies, in accordance with National Institutes of Health (NIH) guidelines.
Support broader access to healthier foods by:working with state agencies responsible for agriculture, education, health and economic development to educate consumers on healthy eating;providing resources and leadership to promote restaurants’ and grocery stores’ participation in voluntary food and menu labeling programs;implementing higher nutritional standards in government food programs; andsupporting local agriculture by promoting partnerships between local growers and schools, and publicly-funded food programs to provide fruits and vegetables and information on healthy eating to improve consumers’ access to fresh and healthy foods.
¸
¸
¸
¸
¸
¸
¸
¸
¸
¸
�
This publication was prepared by Michael Fierro and Debra Lightsey of Bearing Point, Inc. for The Council of State Governments’ (CSG) Healthy States Initiative. Funding for this publication was
provided by the U.S. Department of Health and Human Services, Centers for Disease Control and Prevention (CDC) under Cooperative Agreement Number U38/CCU424348. Its contents are the
responsibility of the authors and do not necessarily represent the official views of CDC or CSG.