intravitreal ranibizumab in the treatment of subretinal neovascularization in a case of punctate...
TRANSCRIPT

a r c h s o c e s p o f t a l m o l . 2 0 1 4;8 9(3):130–132
ARCHIVOS DE LA SOCIEDADESPAÑOLA DE OFTALMOLOGÍA
www.e l sev ier .es /o f ta lmologia
Short communication
Intravitreal ranibizumab in the treatment of subretinalneovascularization in a case of punctate innerchoroidopathy�
B. Jiménez ∗, I. Pinilla, J.A. Cristóbal, E. Mínguez, D. Pérez, N. Cruz, C. Peiro
Servicio de Oftalmología, Hospital Clínico Universitario Lozano Blesa, Zaragoza, Spain
a r t i c l e i n f o
Article history:
Received 22 March 2011
Accepted 7 November 2012
Available online 29 June 2014
Keywords:
Punctate inner choroidopathy
Neovascular membrane
Fluorescein angiography
Angiogenesis inhibitors
Ranibizumab
a b s t r a c t
Case report: We report the case of a 28-year-old woman suffering from loss of visual acuity
in her left eye, who presented an image suggestive of a subretinal neovascular membrane
in her left eye, and bilateral retinal lesions compatible with punctate inner choroidopathy
(PIC). She was treated with intravitreal ranibizumab obtaining excellent results.
Discussion: The differential diagnosis must be made between PIC and the rest of “white
dot syndromes” and the presumed ocular histoplasmosis syndrome (POHS). Antiangiogenic
drugs may be a good alternative for the treatment of such diseases when they develop a
subretinal neovascular membrane.© 2011 Sociedad Española de Oftalmología. Published by Elsevier España, S.L. All rights
reserved.
Ranibizumab intravítreo en el tratamiento de membrana neovascularsubretiniana en un caso de coroidopatía puntata interna
Palabras clave:
Coroidopatía punctata interna
Membrana neovascular
Angiografía fluoresceínica
Antiangiogénicos
r e s u m e n
Caso clínico: Se presenta el caso de una mujer de 28 anos con disminución de agudeza visual
en ojo izquierdo (OI) que presentaba una imagen sugestiva de membrana neovascular subre-
tiniana en OI y lesiones coriorretinianas bilaterales compatibles con coroidopatía punctata
interna (PIC) que fue tratada con ranibizumab intravítreo, obteniendo excelentes resultados.
Discusión: Debe realizarse el diagnóstico diferencial de la PIC con el resto de «síndromes de
Ranibizumab puntos blancos» y con el síndrome de presunta histoplasmosis ocular (SPHO). Los fármacosanti-VEGF pueden ser una
cuando desarrollan una m© 2011 Sociedad Espan
� Please cite this article as: Jiménez B, Pinilla I, Cristóbal JA, Mínguez Ede membrana neovascular subretiniana en un caso de coroidopatía pu
∗ Corresponding author.E-mail address: [email protected] (B. Jiménez).
2173-5794/$ – see front matter © 2011 Sociedad Española de Oftalmolo
buena alternativa como tratamiento de este tipo de enfermedades
embrana neovascular subretiniana.ola de Oftalmología. Publicado por Elsevier España, S.L. Todos los
derechos reservados.
, Pérez D, Cruz N, et al. Ranibizumab intravítreo en el tratamientontata interna. Arch Soc Esp Oftalmol. 2014;89:130–132.
gía. Published by Elsevier España, S.L. All rights reserved.
o l . 2 0 1 4;8 9(3):130–132 131
I
Pnapwrttdnwi
C
Fiop(
Fp
Fp3a
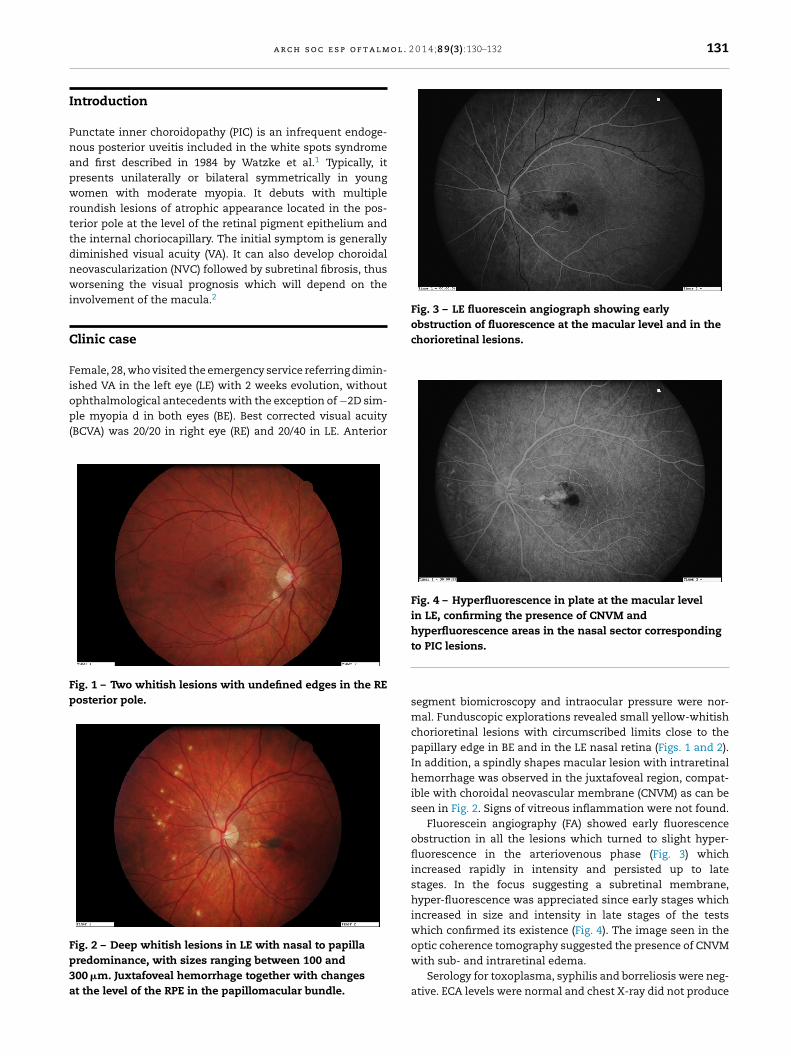
Fig. 3 – LE fluorescein angiograph showing earlyobstruction of fluorescence at the macular level and in thechorioretinal lesions.
a r c h s o c e s p o f t a l m
ntroduction
unctate inner choroidopathy (PIC) is an infrequent endoge-ous posterior uveitis included in the white spots syndromend first described in 1984 by Watzke et al.1 Typically, itresents unilaterally or bilateral symmetrically in youngomen with moderate myopia. It debuts with multiple
oundish lesions of atrophic appearance located in the pos-erior pole at the level of the retinal pigment epithelium andhe internal choriocapillary. The initial symptom is generallyiminished visual acuity (VA). It can also develop choroidaleovascularization (NVC) followed by subretinal fibrosis, thusorsening the visual prognosis which will depend on the
nvolvement of the macula.2
linic case
emale, 28, who visited the emergency service referring dimin-shed VA in the left eye (LE) with 2 weeks evolution, without
phthalmological antecedents with the exception of −2D sim-le myopia d in both eyes (BE). Best corrected visual acuityBCVA) was 20/20 in right eye (RE) and 20/40 in LE. Anterior
ig. 1 – Two whitish lesions with undefined edges in the REosterior pole.
ig. 2 – Deep whitish lesions in LE with nasal to papillaredominance, with sizes ranging between 100 and00 �m. Juxtafoveal hemorrhage together with changest the level of the RPE in the papillomacular bundle.
Fig. 4 – Hyperfluorescence in plate at the macular levelin LE, confirming the presence of CNVM andhyperfluorescence areas in the nasal sector corresponding
to PIC lesions.segment biomicroscopy and intraocular pressure were nor-mal. Funduscopic explorations revealed small yellow-whitishchorioretinal lesions with circumscribed limits close to thepapillary edge in BE and in the LE nasal retina (Figs. 1 and 2).In addition, a spindly shapes macular lesion with intraretinalhemorrhage was observed in the juxtafoveal region, compat-ible with choroidal neovascular membrane (CNVM) as can beseen in Fig. 2. Signs of vitreous inflammation were not found.
Fluorescein angiography (FA) showed early fluorescenceobstruction in all the lesions which turned to slight hyper-fluorescence in the arteriovenous phase (Fig. 3) whichincreased rapidly in intensity and persisted up to latestages. In the focus suggesting a subretinal membrane,hyper-fluorescence was appreciated since early stages whichincreased in size and intensity in late stages of the testswhich confirmed its existence (Fig. 4). The image seen in theoptic coherence tomography suggested the presence of CNVM
with sub- and intraretinal edema.Serology for toxoplasma, syphilis and borreliosis were neg-ative. ECA levels were normal and chest X-ray did not produce

l m o l
r
1
2
3
4
5
132 a r c h s o c e s p o f t a
relevant findings. The Mantoux test and haplotypes HLA B7,DR2 and A29 tests were likewise negative.
Treatment was decided with intravitreal injections ofranibizumab in LE in monthly administration up to 3 injec-tions. VA improved up to 20/30 after the first injection. Onemonth after the third injection BCVA reached 20/20 andremained stable up to the three-month examination. Tomo-graphic sections revealed the absence of intra- and subretinalfluid. During the year in which the patient was followed up inour service no symptoms or signs of activity were observed.
Discussion
The «white dot syndrome» comprises a group of infrequentendogenous choroidal inflammations requiring a precisedifferential diagnostic. Funduscopic signs discarded acuteposterior multifocal placoid pigmented epitheliopathy. Bird-shot choroidopathy was discarded due to negative HLA-A29and mismatching condition. The absence of spontaneous res-olution did not suggest evanescent white spot syndrome oracute retinal pigmentary epithelitis. Multifocal choroiditis wasnot considered due to the absence of vitritis and lack of activ-ity in the lesions. Presumed ocular histoplasmosis syndromeexhibits peripapillary atrophy and is associated to HLA B7 andDR2, which were absent in the patient of this case.
On the other hand, in the presence of choroiditis areas,infectious etiology must be excluded. Negative serology dis-carded syphilis, toxoplasmosis and Lyme’s disease. ChestX-ray, Mantoux test and normal ECA values discarded tuber-culosis and sarcoidosis.
The presence of CNVM associated to chorioretinal atro-phy with typical angiographic signs and absence of vitritis ina young Caucasian patients with moderate myopia led us toconsider PIC.
In what concerns therapeutic alternatives for CNVM,various options have been described such as argon laser pho-tocoagulation in juxta- and extrafoveal membranes, surgicalremoval or photodynamic therapy in subfoveal membranes,as well as treatment with corticoids.
The above methods have obtained limited visual results,high recurrence rates and, in the case of corticoids, fre-
quent side effects. At present, the efficiency of anti-VEGFdrugs has been demonstrated for treating CNVM associatedto ARMD. Accordingly, wider use of the anti-VEGF drugs has. 2 0 1 4;8 9(3):130–132
been proposed for counteracting angiogenesis secondary toother ocular diseases. The first studies published on theuse of antiangiogenics in PIC analyzed treatment of NVCwith bevacizumab, obtaining good morphological and visualresults.3
Among the few references on the use of ranibizumab,Menezo et al. described in 2010 an improvement of vision sta-bilization in 9 out of 10 patients with CNVM secondary to PICafter being treated with intravitreal ranibizumab with an aver-age of 1.9 injections (1–5).4 Cornish et al. also treated 9 casesof CNVM secondary to PIC with visual deterioration in a singlepatient with anti-VEGF drugs.5 The Clinic Case reported hereinis an additional example of the usefulness of ranibizumabfor treating these patients. Prospective studies are needed todemonstrate whether ranibizumab is an efficient and defini-tive alternative against subretinal neovascularization in thesediseases.
Conflict of interests
No conflict of interests has been declared by the authors.
e f e r e n c e s
. Watzke RC, Packer AJ, Folk JC, Benson WE, Burgess D, Ober RR.Punctate inner choroidopathy. Am J Ophthalmol.1984;98:572–84.
. Gerstenblith AT, Thorne JE, Sobrin L, Do DV, Shah SM, FosterCS, et al. Punctate inner choroidopathy: a survey analysis of 77persons. Ophthalmology. 2007;114:1201–4.
. Chan WM, Lai TY, Liu DT, Lam DS. Intravitreal bevacizumab(avastin) for choroidal neovascularization secondary to centralserous chorioretinopathy, secondary to punctate innerchoroidopathy, or of idiopathic origin. Am J Ophthalmol.2007;143:977–83.
. Menezo V, Cuthbertson F, Downes SM. Positive responseto intravitreal ranibizumab in the treatment of choroidalneovascularization secondary to punctate innerchoroidopathy. Retina. 2010;30:1400–4.
. Cornish KS, Williams GJ, Gavin MP, Imrie FR. Visual and opticalcoherence tomography outcomes of intravitreal bevacizumab
and ranibizumab in inflammatory choroidalneovascularization secondary to punctate innerchoroidopathy. Eur J Ophthalmol. 2011;21:440–5,http://dx.doi.org/10.530/EJO.2010.6117.