intrauterine & intravaginal drug delivery system
TRANSCRIPT
PRESENTED BY
DEORE PRASHANT ASHOK
Department of Pharmaceutics M. Pharm. II Semester (2014-2015)
Intrauterine & Intravaginal Drug Delivery System
R. C. Patel Institute of Pharmaceutical Education and Research, Shirpur .
1
[email protected] Mo.09881261646
3-Mar-15
Contents
1. Introduction
2. Anatomy & Physiology of female reproductive system
3. Intravaginal DDS
4. Factors affecting vaginal absorption
5. Ideality of Intravaginal DDS
6. Classification of Intravaginal DDS
7. Advantages & Disadvantages
8. Intrauterine DDS
9. Advantages & Disadvantages
10. References
3-Mar-15 2

Introduction
• Vagina and Uterus are the route for administration of contraceptives ,
antifungals and antimicrobials.
• These are used for local or systemic absorption.
• Because of vast network of blood vessels, vaginal wall is suitable for
dug absorption.
• The rate and extent of drug absorption may vary depends upon
1) Formulation factors
2) Physiology
3) Age of patient
4) Menstrual cycle
3-Mar-15 3

• Vulva
• Vagina
• Uterus
• Fallopian
tubes
• Ovary3-Mar-15 4
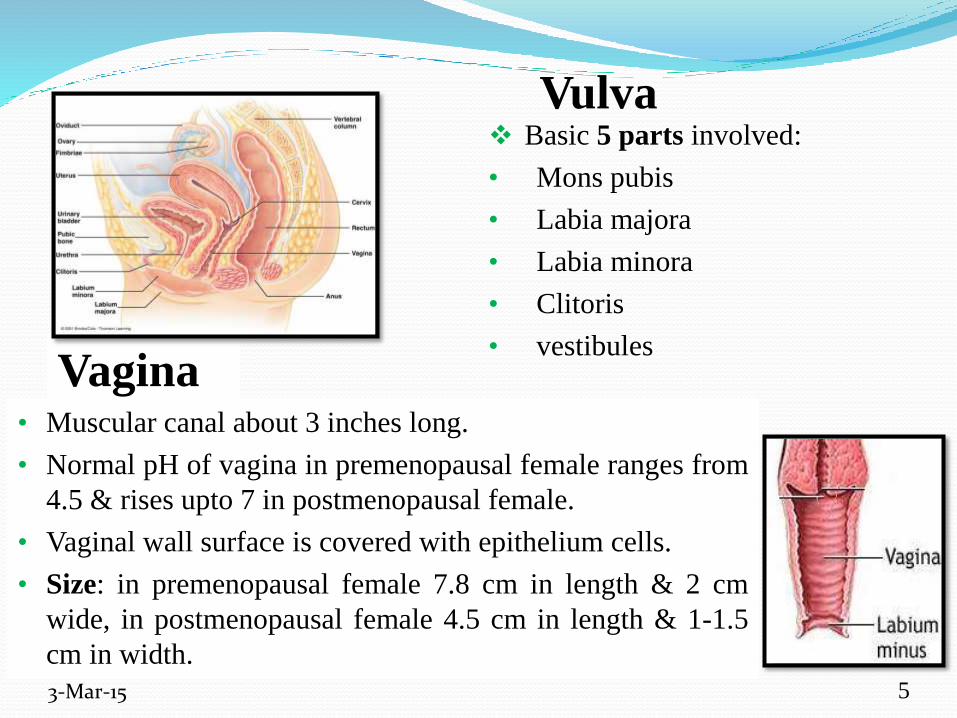
Vulva Basic 5 parts involved:
• Mons pubis
• Labia majora
• Labia minora
• Clitoris
• vestibules
3-Mar-15
Vagina• Muscular canal about 3 inches long.
• Normal pH of vagina in premenopausal female ranges from
4.5 & rises upto 7 in postmenopausal female.
• Vaginal wall surface is covered with epithelium cells.
• Size: in premenopausal female 7.8 cm in length & 2 cm
wide, in postmenopausal female 4.5 cm in length & 1-1.5
cm in width.
5
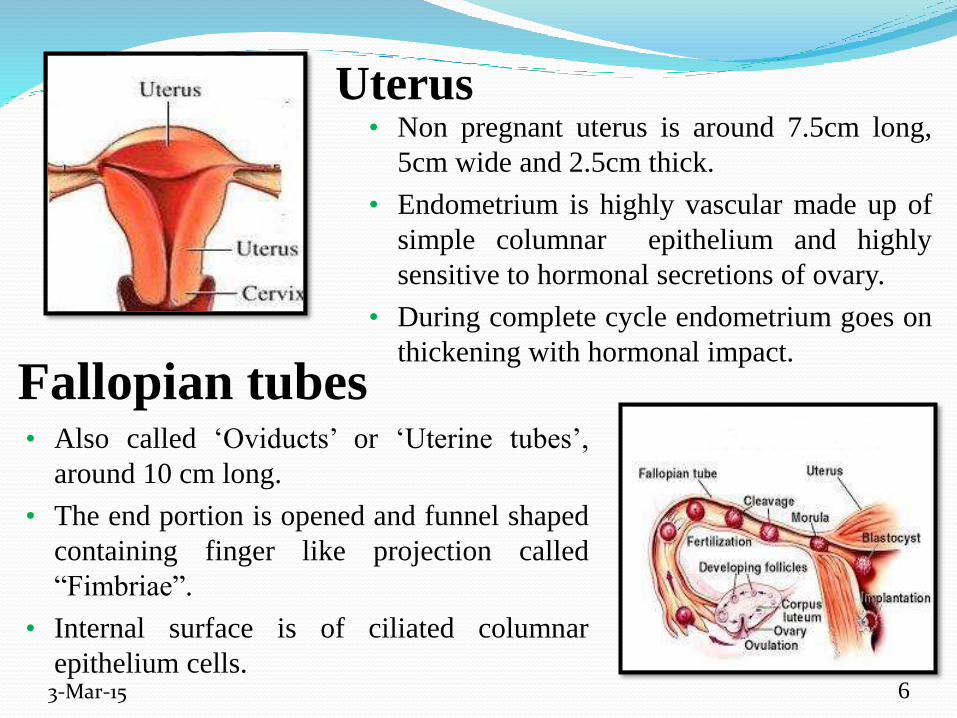
Uterus• Non pregnant uterus is around 7.5cm long,
5cm wide and 2.5cm thick.
• Endometrium is highly vascular made up of
simple columnar epithelium and highly
sensitive to hormonal secretions of ovary.
• During complete cycle endometrium goes on
thickening with hormonal impact.
3-Mar-15
Fallopian tubes• Also called ‘Oviducts’ or ‘Uterine tubes’,
around 10 cm long.
• The end portion is opened and funnel shaped
containing finger like projection called
“Fimbriae”.
• Internal surface is of ciliated columnar
epithelium cells.6

Ovary• Two ovaries, one on either side of the
uterus.
• These are having shape and size of
unshelled almonds.
• There are ovarian follicles containing
oocytes in various stages of
development.
3-Mar-15
• Matured follicle which releases secondary oocyte is called Graafian
follicle.
• Ovaries produces hormones including progesterone and estrogen,
inhibin and relaxin.
7
Intravaginal Drug Delivery System
• Traditionally used system as contraceptive and to treat vaginal
infections.
• The formulations given by this route are in solid, liquid and semisolid
system.
• It may be intended for local effect or systemic action.
• Systemic absorption by dense network of blood vessels is advantage
over oral route.
• The first truly controlled drug delivery systems for used in vagina
were developed in 1970, when the first vaginal ring was used for
delivery of medroxyprogesterone acetate for contraception.
• Vaginal rings are most common long term drug delivery system
currently used.
3-Mar-15 8
Factors affecting vaginal drug
absorption
• It is important to design formulation as well as device used for
administration.
• Factors can be categorized as:
1) Physiological factors:-
Factors related to the vaginal physiology include:
a. pH of vagina (3.5- 4.9)
b. Effect of menstrual cycle on permeability of vaginal epithelium
c. Vaginal fluid volume
d. Viscosity of vaginal fluid
e. Pressure exerted by rectal wall on dosage form affect vaginal blood
flow.
3-Mar-15 9

2) Physicochemical factors:-
• Factors related to physico-chemical properties of drug such as:
a. Viscosity (semisolids)
b. Concentration and Volume for administration
c. Type of dosage form
d. Molecular size of drug
3-Mar-15 10
Ideality of Intravaginal DDS
1) Component should melt at vaginal temperature i.e. at 37oC.
2) Device should be nontoxic and nonirritating.
3) Formulation should be nonsensitive on vaginal pH.
4) Formulation should have wetting and emulsifying properties.
5) It should be stable on storage.
6) Formulation should have proper viscosity to avoid leakage of drug
from vagina (for semisolid).
7) Formulation should have proper bioadhesive properties to increase
contact time between membrane and formulation.
3-Mar-15 11

Classification of Intravaginal DDS
A. Localized :
1) Barrier contraception
(Diaphragm, Cervical cap,
Sponge)
2) Prevention/Treatment of infection
( Gels, Cream, Ointment)
3-Mar-15 12
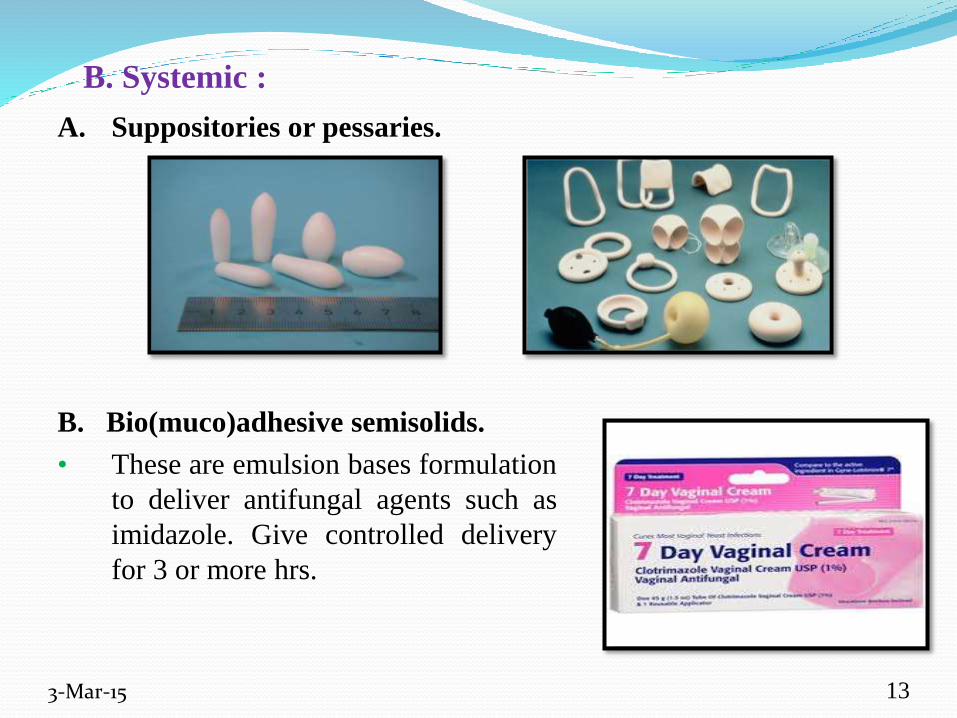
B. Systemic :
A. Suppositories or pessaries.
B. Bio(muco)adhesive semisolids.
• These are emulsion bases formulation
to deliver antifungal agents such as
imidazole. Give controlled delivery
for 3 or more hrs.
3-Mar-15 13
b. Elastomeric intravaginal rings( IVR):
1) Matrix (homogeneous dispersion)
2) Reservoir (core)
3) Sandwich (shell)
Elastomer exert slight tension on vaginal wall,
more suitable for hydrophobic drugs.
Normally designed to contain steroidal
hormones.
3-Mar-15
C. Solid polymeric carriers.
a. Solid hydrogels:
Having swelling property which enables the
drug to diffuse out of the macromolecular
network.
eg. Nu-gel ( Johnson & Johnson)
14

1) Matrix type :-
• Drug is homogeneously dispersed through out
the polymer matrix.
• Drug release from this type follows First order.
2) Reservoir type:-
• Drug is located within the centralized core that
is surrounded by drug free silicon sheath acts as
rate controlling membrane for drug diffusion.
• It follows Zero order fashion.
3) Sandwich type:-
• Consists of narrow drug containing layer
positioned between non-medicated impervious
central core & non-medicated outer rate
controlling band.
• Small and constant release of drug.3-Mar-15 15
Other novel approaches :
1) Medicated Vaginal Tampons- A medicated vaginal tampon,
approved as a medical device by the Food and Drug Administration
(FDA) .
• This bifunctional tampon contains a polymeric delivery system
(strips) that absorb menstrual fluid while gradually releasing lactic
acid and citric acid.
• eg. Brilliant pH tampons
3-Mar-15 16
2) Vaginal Films-
• Vaginal films are polymeric drug delivery systems shaped as thin
sheets, usually ranging from 220 to 240 μ m in thickness.
• These systems are often square (approximately 5cm × 5cm),
colorless, and soft, presenting a homogenous surface.
• Vaginal films are produced with polymers such as polyacrylates,
polyethylene glycol, polyvinyl alcohol, and cellulose derivatives.
• eg.VCF (vaginal contraceptive films)
3-Mar-15 17

Advantages
• Minimal systemic side effects.
• Irritation to the stomach and small intestine associated with somedrugs can be avoided.
• An increase in bioavailability.
• First pass metabolism can be avoided.
• Contact with digestive fluid is avoided, thereby preventing enzymaticdegradation of some drugs.
• Self medication is possible.
• Drug delivery can be stopped by removing the dosage form. e.g.vaginal rings
• Rapid drug absorption and quick onset of action can be achieved.
• The vaginal bioavailability of smaller drug molecule is good.
• The bioavailability of larger drug molecules can be improved by meansof absorption enhancer.
3-Mar-15 18
Disadvantages
• Patient incompliance.
• Only few drugs are administered by this route.
• Some of the drugs are sensitive at the vaginal pH.
• Local irritation because some drugs variability in drug absorption related
with menstrual cycle, menopause and pregnancy.
• Gender specificity.
• Influence with sexual intercourse.
• Some time leakage of drugs from vagina and wetting of undergarments.
3-Mar-15 19
Animal modelsVaginal mucosa permeability:-
1) The fundamentals of vaginal absorption of drug can be
studied on female rabbits.
2) It doesn’t exhibit an estrus cycle so its vaginal tissues
shows consistency in the histological, biochemical
and physiological properties not ordinarily seen in
other mammals.
3) But the rabbits may not be suitable for CR dosage
forms due to lack of estrus cycle.
4) Rhesus monkeys are excellent animal model for CR
dosage form as they are having estrus cycle of approx
28 days like human female.3-Mar-15 20
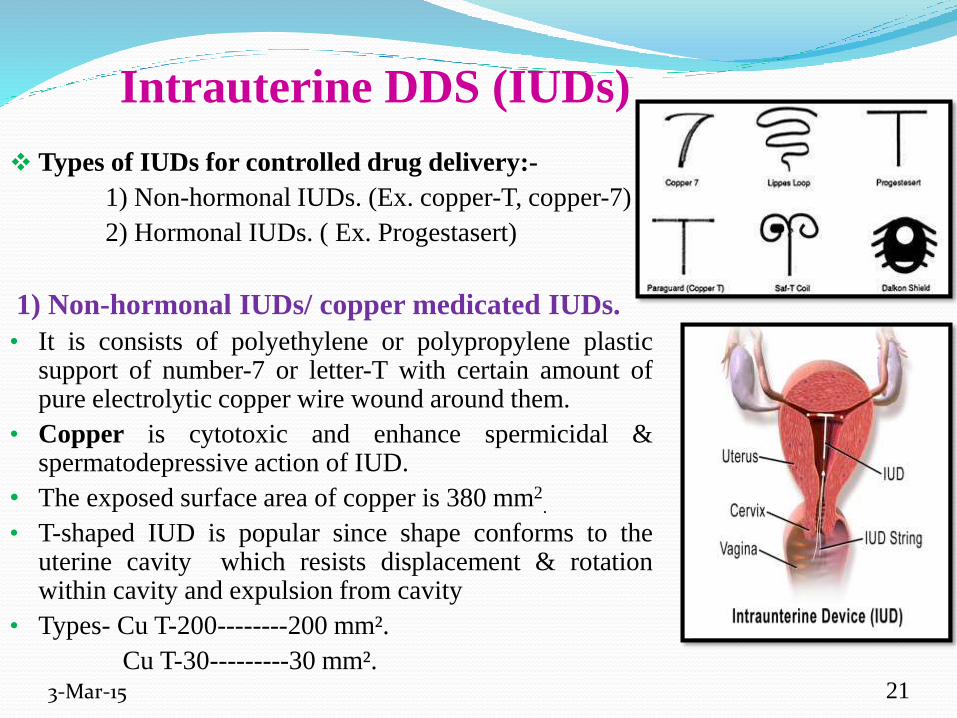
Intrauterine DDS (IUDs)
Types of IUDs for controlled drug delivery:-
1) Non-hormonal IUDs. (Ex. copper-T, copper-7)
2) Hormonal IUDs. ( Ex. Progestasert)
1) Non-hormonal IUDs/ copper medicated IUDs.
• It is consists of polyethylene or polypropylene plasticsupport of number-7 or letter-T with certain amount ofpure electrolytic copper wire wound around them.
• Copper is cytotoxic and enhance spermicidal &spermatodepressive action of IUD.
• The exposed surface area of copper is 380 mm2.
• T-shaped IUD is popular since shape conforms to theuterine cavity which resists displacement & rotationwithin cavity and expulsion from cavity
• Types- Cu T-200--------200 mm².
Cu T-30---------30 mm².3-Mar-15 21
2) Hormonal IUDs.
• T-shaped device made of polyethylene framethat measures 32 mm in both vertical andhorizontal direction.
• There is silicone reservoir containing dispersedlevonogestrel or progesterone on vertical stemand further enclosed in a sleeve of ratecontrolling membrane of ethylene-vinylcopolymer.
• It prevents pregnancy up to 5 yrs by steadilyreleasing small amount of progesterone directlyin to uterus.
• It works by thickening the cervical mucous sothat sperm have more difficulty to swim throughuterus.
• For some women it may also prevent ovulationfrom occurring.
3-Mar-15 22

Advantages
Non-hormonal:-
• Safe.
• Immediately and highly effective.
• Long term (up to 10 yrs) effect- Freedom from having to remember to
use contraceptives regularly or at the time of intercourse.
• Cost effective (no on going cost after initial insertion)
• Reversible (rapid return of fertility after removal).
3-Mar-15 23
Hormonal :-
• After about 5 months nearly all women will experience light periods
only.
• After 12 months about 20% of women will have no periods at all.
• Can be used to treat excessively heavy menstrual bleeding
• Reduces period pain in many women.
• May be suitable for women approching menopause as it provides
effective contraception and can continue to be used as the
progesteron component for hormone replacement therapy.
3-Mar-15 24
Disadvantages
Non-hormonal:-
• Requires visit to trained physician for insertion and removal.
• Some risk of expulsion within first year.
• for some women, increased menstrual bleeding and cramping.
• Lack of protection against STDs, including HIV.
Hormonal :-
• Irregular bleeding pattern in the early stages (irregular bleeding and
cramping during first few weeks or months after insertion.)
• Some women experiences backache for several days or weeks after
insertion.
• Nausea, headache.
• Weight gain.
3-Mar-15 25
References• Chien Y. W. (2007), Novel Drug Delivery Systems, Revised and
Expanded, Marcel Dekker, Inc., New York, Second Indian Reprint , Vol.-
50, p. 529-629.
• Tortora G. J. & Grabowski S. R. (2003), Principles of Anatomy &
Physiology, 10th edition, p.1028-1039.
• Brahmankar D. M. & Jaiswal S. B. (2009), Biopharmaceutics and
Pharmacokinetics A Treatise, 2nd edition, Vallabh Prakashan, p. 502-508.
• Bandyopadhyay A.K. (2008), Novel drug delivery system, 1st edition,
Everest publishing house, p. 215-220.
• Keshwani Bhawana & Arora Pankaj (2014), Novel concepts in vaginal
drug delivery, Journal of Pharma research, 3 (10) 184-187.
• Chatterjee Arkendu & Kumar Lalit (2009), On overview of Intra-vaginal
Drug delivery system, Journal of Pharmacy research, 2 (4) 698-700.
3-Mar-15 26

Thank You
3-Mar-15 27