intrapartum labor and delivery. 5 factors to consider in planning your nursing care passenger: the...
TRANSCRIPT

Intrapartum
Labor and Delivery
5 factors to consider in planning your nursing care
• Passenger: the fetus
• Passageway: pelvis, uterus, vagina
• Powers: contractions, pushing
• Position: of mom
• Psych response: culture, experiences, preparedness, etc.

The Passenger
• Head Diameter– suboccipitobregmatic 9.5
– occipitofrontal 11.5
– occipitomental 12.5
– biparietal 9.5
– bitemporal 8
• Shoulders

Lie
• Fetal lie- the relationship of the long axis of the baby to the long axis of the mother– horizontal
– longitudinal
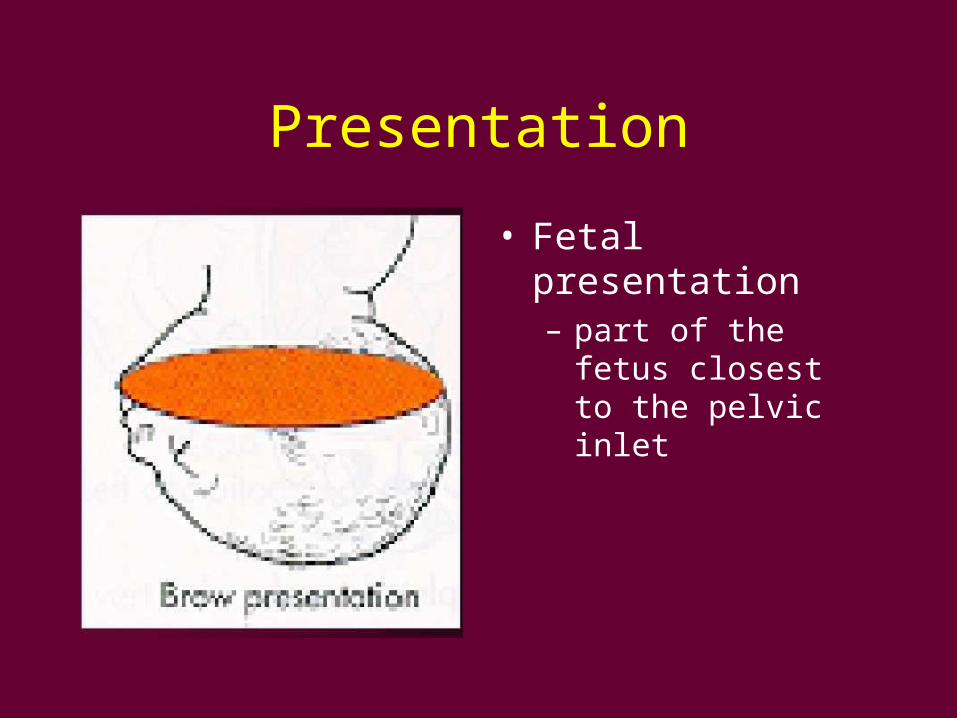
Presentation
• Fetal presentation– part of the fetus closest
to the pelvic inlet

Fetal Attitude
• The relationship of the fetal parts to each other
“Universal Flexion”

Station and Engagement
• Station--the relationship of the biparietal diameter of the infant to the ischial spines of the mother
• Engagement=station 0

Floating/ballotable

Position
• The relationship of fetal landmarks (denominators) to the maternal pelvis
occiput=head flexed
mentum=head extended (face presentation)
brow=head partially extended
sacrum=breech
acromium process=shoulder

Categories of position/presentation
VERTEX• ROA• LOA• ROT• LOT• ROP• LOP• OA• OP
BREECH• RSA• LSA• RST• LST• LSP• RSP• SA• SP

The most common fetal position



Asynclitism
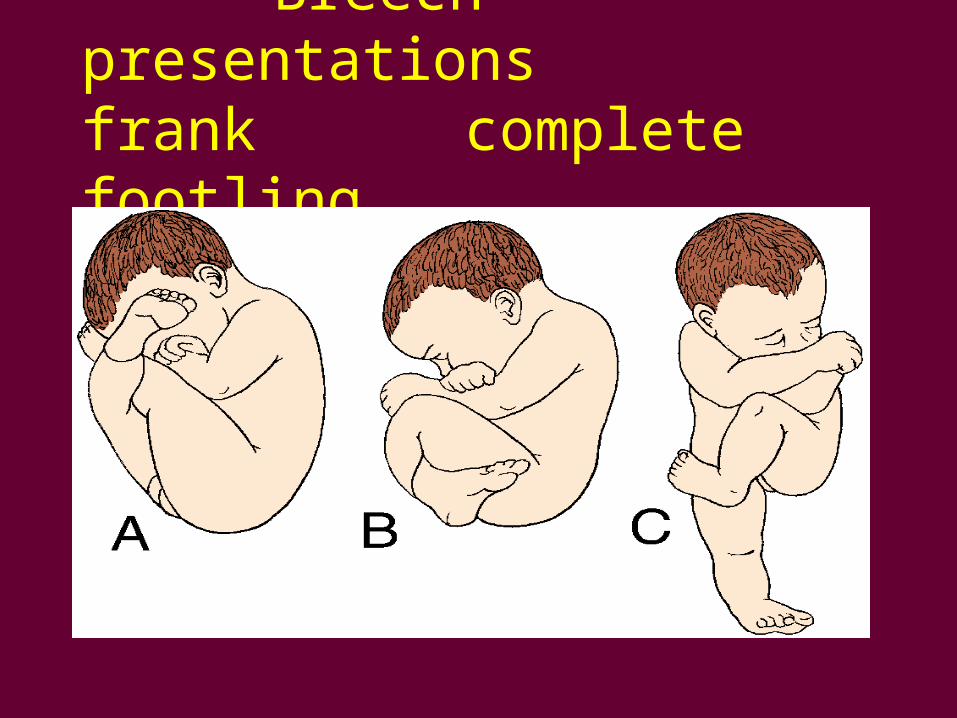
Breech presentationsfrank complete footling

Determination of Position, Presentation, Lie, Attitude, Station, and Engagement
• Ultrasound examination
• Leopold’s Maneuvers
• Vaginal Exam
• Location of fetal heart sounds

Placenta
• Previa• Abruptio• Normal Placental
Separation• Placenta Accreta
The passage
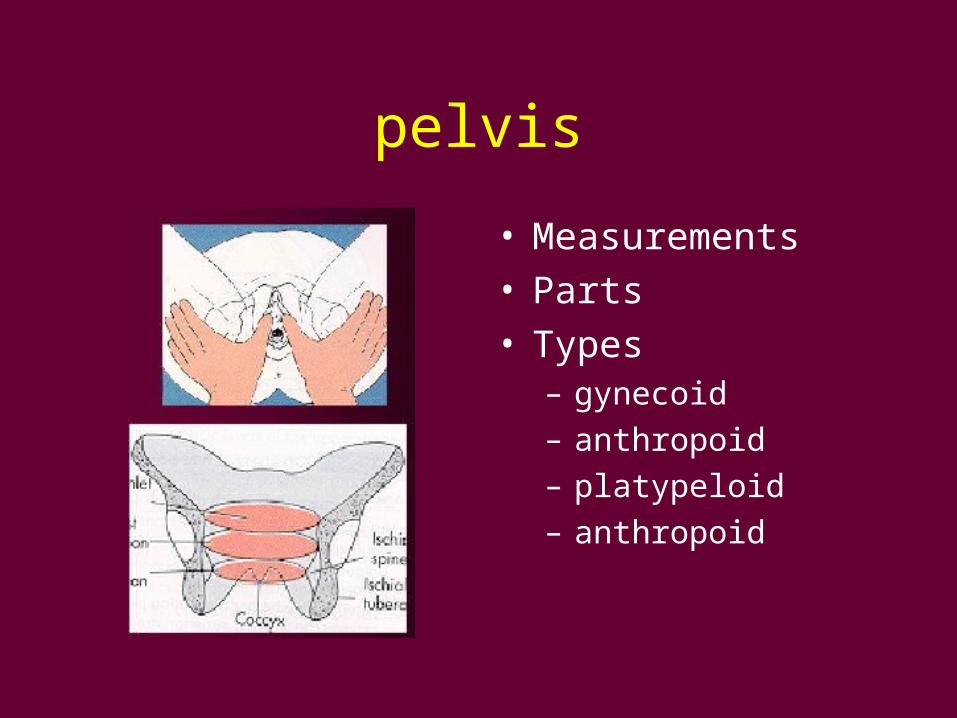
pelvis
• Measurements• Parts• Types
– gynecoid
– anthropoid
– platypeloid
– anthropoid

Soft Tissue
• Uterus• Cervix• Vagina
The powers
Uterine contractions
“pushing”
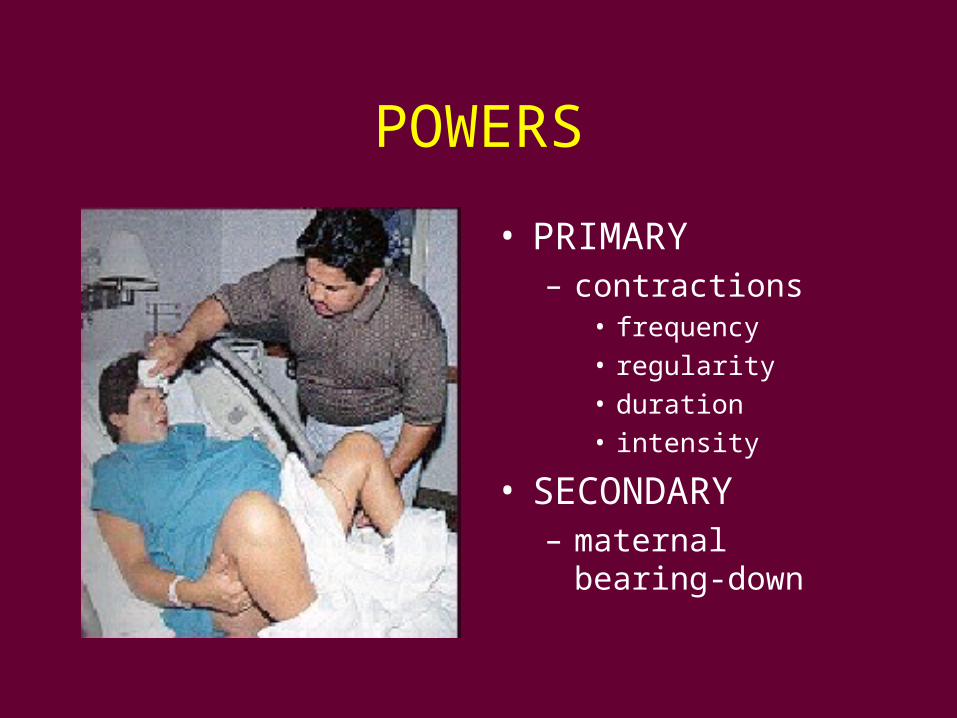
POWERS
• PRIMARY– contractions
• frequency
• regularity
• duration
• intensity
• SECONDARY– maternal bearing-down

Uterine Contractions
Contraction wave starts in pacemakers at the cornual ends of fallopian tubes and descends down to lower uterine segment

The Maternal Position

Gravity and Cardiac Output
Psychological Response

Psychological Response• Maternal Past
experiences• preparedness• support• financial stability,
impact of another child
• other children to care for
• cultural meaning of children, fertility

The Process of Labor
Initiation of Labor
“Lightening” Cervical “ Ripening”/Effacement


Premonitory Signs of Labor• Lightening
• cervical ripening
• 1-3lb wt loss
• increase in vaginal secretions
• mucous plug expelled
• backache
• braxton hicks contractions
• “nesting”
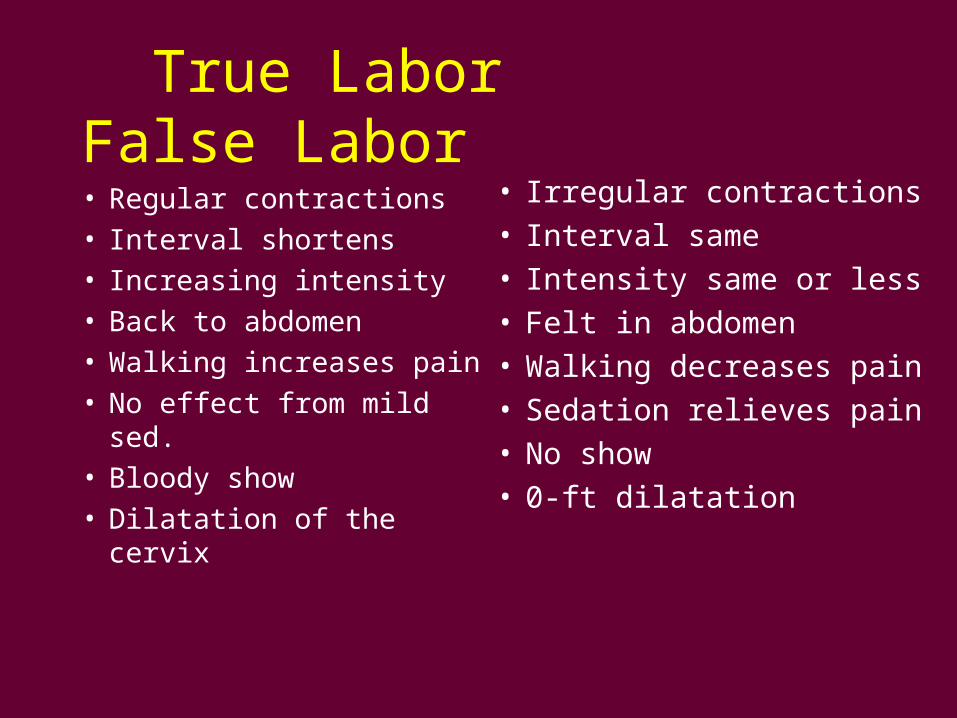
True Labor False Labor
• Regular contractions• Interval shortens• Increasing intensity• Back to abdomen• Walking increases pain• No effect from mild sed.• Bloody show• Dilatation of the cervix
• Irregular contractions• Interval same• Intensity same or less• Felt in abdomen• Walking decreases pain• Sedation relieves pain• No show• 0-ft dilatation

Causes of the Onset of Labor
• Changes in uterus, cervix, pituitary
• Fetal hormonal secretions
• Increasing uterine– distension– intrauterine pressure
• Aging placenta
MECHANISM NOT COMPLETELY UNDERSTOOD
Mechanism of Labor• Engagement
• Descent
• Flexion
• Internal Rotation
• Extension
• Restitution
• Expulsion

Engagement
• Biparietal diameter of the baby reaches the ischeal spines of the mother

Descent
• Pressure• uterine contractions• maternal bearing-
down
Measured by station r/t
ischial spines

Flexion
• The smallest diameter into pelvis
• Pressure of uterus on breech causes chin to flex on chest

Internal Rotation
• Baby turns from OT to OA (usually)
other positions possible
e.g. OP

Extension
• Head extends upward
In a normal vertex delivery the head is born by the process of extension
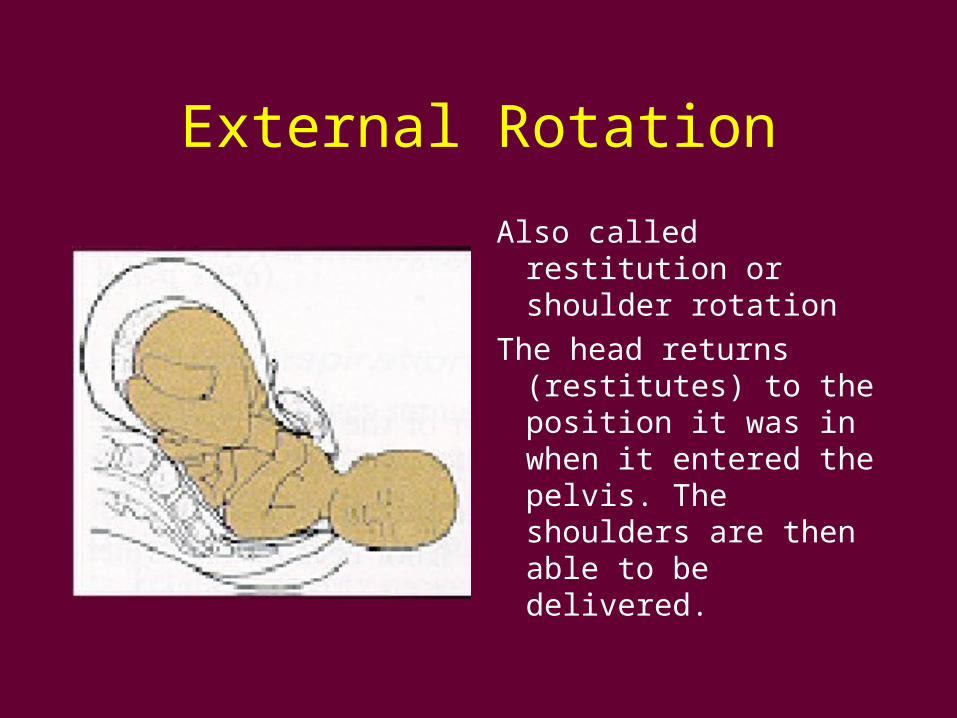
External Rotation
Also called restitution or shoulder rotation
The head returns (restitutes) to the position it was in when it entered the pelvis. The shoulders are then able to be delivered.

Expulsion
The baby is delivered



THE STAGES OF LABOR

FIRST STAGE
From onset of labor to full dilitation and effacement
• latent stage (0-3 cm)
• active stage (4-7 cm)
• transitional phase (8-10 cm)
• “complete” at 10 cms
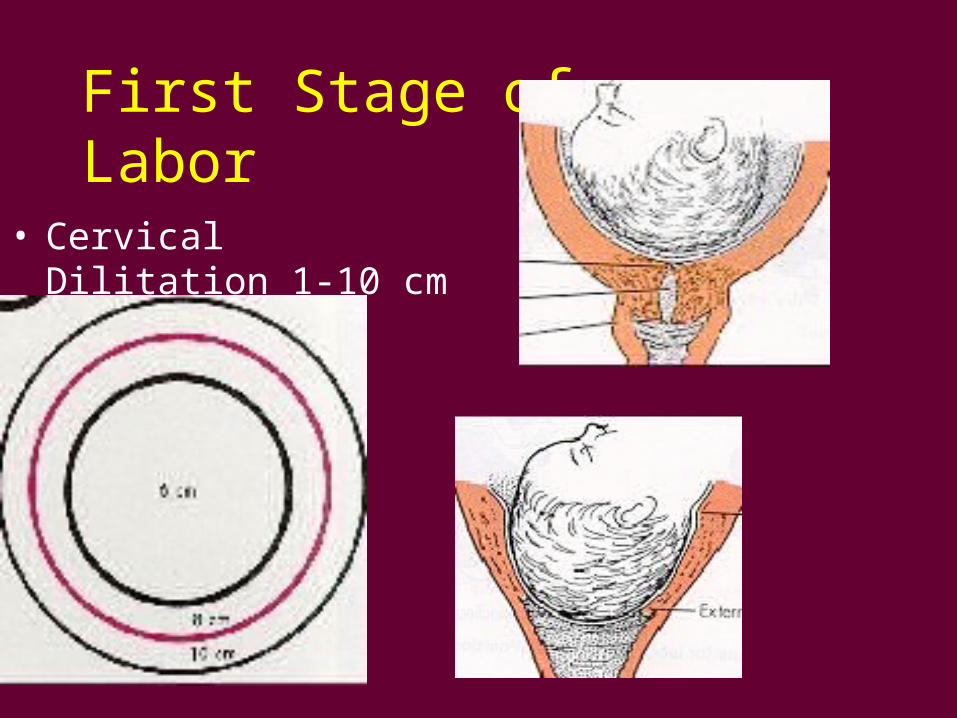
First Stage of Labor
• Cervical Dilitation 1-10 cm

Signs of transition
• Increased bloody show
• rectal pressure
• tremors in thighs, legs
• Feels she is losing control

Second Stage, from full diliation and effacement to delivery

Third stage--delivery of Placenta

Placental Separation
Placental separation occurs because the uterus contracts but the placenta cannot, so it buckles and separates
Pressure of the uterine walls cause it to slide downward
Gentle fundal pressure and traction on the cord complete its delivery
Mechanisms of Placental Expulsion
• Duncan (maternal side first--separates from edges 30% of the time)
• Shultz (fetal side first--separates in center
70% of the time)

Fourth Stage
• Fourth stage of Labor• four hours after
delivery--stabilization period

Maternal and Fetal Adaptationsto delivery
Maternal AdaptationsAll systems affected
Cardiovascular--uterine shunting during labor
• Blood volume 40% at term
• CO2>50% during labor
• Heart rate increases
• Supine hypotension syndrome
NEVER LEAVE A LABORING WOMAN
SUPINE

Respiratory
• more efficient gas exchange (increase in alveolar ventilation
• diaphragm displaced upward so FRC • Capillary Engorgement in respiratory tract
leads to edema and friability of mucous membranes.
Gastrointestinal Changes• GI-- motility food absorption
• lower tension of esophageal sphincter
• higher gastric acidity and gastric volume (r/t placental secretion of gastrin)
• Increased intragastric pressure (from uterus)
Danger of vomiting and aspiration of vomitus during labor. Antacid may be given before CS or delivery

Renal Function
• Renal-- GFR
• Renal plasma flow 75% above normal
• Glycosuria due to increased load of glucose by GFR
• Dilitation of the renal calyces= incidence of urinary tract infections
Endocrine--progest. oxytocin, PGs
Musculoskeletal-- lactic acid
Integumentary--diaphoresis

FETAL ADAPTATIONS
• Measured via FHT’s
• Fetal scalp sampling
• Vaginal vs. C-sect birth
• Rising PCO2 levels during second stage and after cord cut initiate respirations

Fetal scalp blood sampling

NURSING IMPLICATIONS FOR LABOR AND DELIVERY

Initial L&D assessment• Ht. And Wt. and gain• EDC• maternal age• allergies• med/surg/ob history• lab work• prenatal care
• Contractions• FHT’s• vaginal discharge• ROM?• Color of fluid• Support person• interaction with
support person

Physical exam--Leopolds Maneuvers

Vaginal Exam
Determines• Presentation• Position• Station• Effacement• Dilitation• Molding

Fetal Heart Tones

Rupture of Membranes (ROM)
• Artificial AROM• Spontaneous SROM• Premature PROM
– Nitrazine test to determine if fluid is urine or amniotic fluid

Amniotic Fluid
Note:
• Color
• Character
• Amount
• Odor
Check fetal heart tones after ROM, possibility of prolapsed cord
Infection possible with rupture >24hrs

Labor Monitoring

Contractions
Time• Frequency• Duration• Intensity• Interval• Regularity• Degree of uterine
relaxation between contractions

Fetal Monitoring
• Baseline FHT--between contractions
Normal 120-160 BPM
Labor is a fetal stressor
Reduction of O2 with every contraction

Fetal Tachycardia
• Prematurity• mild hpoxia compensation• tocolytic agents• maternal fever BMR• Atropine or vagal inhibitors• activity• infection
Fetal Bradycardia
• Hypoxia
• drugs
• maternal hypotension
• cord compression
• fetal heart block or anomaly
• impending demise

Variability, the beat to beat changes in heart rate

Possible causes of variability
• Sleeping infant
• Prematurity
• Anomalies
• Anticholinergics, e.g. atropine
• Analgesicics
• Hypoxia

Accelerations
• The increase in fetal heart tones with contractions or fetal movement
• Positive indicator of fetal adjustment to stress

Early Decelerations

Early Decelerations
Begin with the contraction and return to baseline after the contraction
No treatment necessary
These are normal

Variable Decelerations
Variable Decelerations
V shaped or U shaped decelerations of variable onset
• ascertain type
• positional changes
• pelvic exam to see if cord has prolapsed
• O2 by mask at 10L/min

Late Decelerations

Late Decelerations
Decelerations in which the FHT does not return to baseline p contraction
Particularly ominous if coupled with decreased variability
• Give O2 at 10L min
• Reposition (off vena cava)
• DC oxytocin infusion
• If not improved--immediate delivery

External Monitoring

Internal Monitoring

Obstetrical Emergencies

Prolapsed Cord
• ROM with presenting part high and unengaged
• Malpresentation• Polyhydramnios

Nursing Actions
• Trendelenburg Position
• Knee Chest Position
• Hold Presenting Part up with a gloved hand
• Notify Physician/Midwife
• Anticipate Immediate Delivery– C section if delivery not imminent– Vaginal delivery only if ready to deliver

Fetal Distress
• Late Decelerations or prolonged variables, low or absent variability with bradycardia– Turn on L side
– Administer O2
– Discontinue Pitocin– Notify MD/midwife if not improved by nursing
actions

Other Emergencies
• Placental abruption
• Uterine rupture
• Eclampsia

Uterine HyperstimulationFailure of the uterus to
completely relax in
between contractions, or
contractions closer than
1” apart.• Turn off pitocin• Turn onto L side
• Administer O2
• Monitor FHT’s• Notify MD

Admission to Labor Unit
• VS, FHT’s Status of Membranes
• Onset of Labor
• Contractions--run a baseline monitor strip
• Vaginal Exam
• Possibly ambulate and clear liquids

Supporting Measures
Position• Upright• L side if in bed• Ambulate if not
contraindicated
Breathing techniques• watch for
hyperventilation

Support People
Coach, emotional supportnourishment, comfort measures


Pain in Labor is NORMALCaused by:
• hypoxia of compressed muscle cells
• compression of nerves in cervix or LUS by interlocking muscle fibers
• stretching of cervix
• stretching of perineum
• bladder distension
• tension/anxiety/fear
• oxytocin (stronger contractions)

Non pharmacologic pain relief methods
• Acupuncture• TENS• distraction• ambulation• imagery• hydrotherapy• therapeutic touch• hypnosis• acupressure• positioning

Pain Relif in LaborAnalgesia and Anesthesia
Analgesia
• Narcotics--can affect baby (Narcan)– demerol, morphine, stadol
• Tranquilizers– vistaril(hydroxyzine), phenergan
(promethazine)
• Sedatives– secobarbital, etc.

Anesthesia
• Local (sub-q injection into the perineum)
• Regional– paracervical, pudendal, epidural, spinal
• General– inhalation– intravenous

Choice of analgesia or anesthesia based on
• Pt. Condition• labor status• risks• personell
• local practice• physician’s preference• pt’s preference
Goal of anesthesia/analgesia
Pain relief that’s simple to use w/o
• endangering mother or baby
• decreasing efficiency of uterine contractions
• diminishing ability of mom to cooperate
• causing need for operative intervention

PUDENDAL BLOCK

Epidural Anesthesia
• Rapid infusion of RL IV to prevent hypotension
• Causes sympathetic blockade and BP
• Position uterus off of vena cava
• Monitor BP q. 3 minutes until stable
• Monitor FHT, frequently (fetal bradycardia)
Culture and Childbirth
• FOB has differing roles according to culture
• Must consider cultural differences– expression of pain– modesty– importance of extended family– rites and rituals concerning placenta, and
cutting the umbilical cord

Nursing assessment in 2nd stage
• FHT’s• Contractions• BP• Control• Effectiveness of
bearing down efforts• Perineal status

Assessment findings in 2nd StageObjective:
increasing bloody show
BP up with bearing down
Subjective:
irritable
Duration:
if < 2hr, MD will intervene
Breathing--needs coaching
Nursing Dx
• Ineffective breathing pattern
• altered comfort
• ineffective coping pattern

Implementation of Nursing Care
• Support• Encouragement• Rest between
pushes/contractions• positioning

Preparation for Delivery
• The room• the warmer, infant
supplies• delivery supplies• perineal prep
Delivery
• Assess position• avoid precipitous
delivery--control!

Episiotomy

Dystocia--difficult labor
• Abnormal contraction pattern– primary and secondary uterine inertia
• Bony Dystocia– CPD (cephalo-pelvic disproportion)
• Soft Tissue Dystocia– previa, tumors, cervical edema
Dystocia
• CPD
• malposition
• malpresentation
• multiple gestation
Induction of Labor
Indications
• PIH, preeclampsia
• post term
• previous precipitous delivery
• distance from hospital
• convenience
Dangers of Induction• Prolapsed cord
• prolonged labor
• pain
• prematurity
• failureCS
• uterine hypertonus rupture
• lacerations
• hemorrhage
• fetal anoxia
• precipitous delivery

Induction of Labor (Stimulation/Augmentation
• Natural--nipple stimulation
• Medical– AROM– “Stripping” membranes– Laxatives/enemas– Laminaria
• Chemical– oxytoxics– prostaglandins

Forceps Delivery
• Full diliation• engaged head• no CPD

Vacuum Extractor
• Requires ROM• Vertx presentation• No CPD


Cesarean Delivery
• Classical or Low Cervical
• Usually a regional anesthetic, unless emergency--then general
Indications for Cesarean deliveryMaternal factors
PIH, Diabetes, Heart
dis.,Infections (herpes),
age?
Fetal Status
distress, death, anomalies
Mat/Fetal Factors
Dystocia, Inertia, FTP,
Uterine rupture, Hemm.,
prolapsed cord, CPD,
malpres., plac. Insuff.
Miscellaneous factors
Previous C sections
multiple gestations
monitoring?
Defensive medicine?
Consumer pressure?
Lack of experience with difficult deliveries?
VPB syndrome?
(very precious baby)


VBAC
• Vaginal Birth After Cesarean
• Usually attempted unless previous classical incision or type unknown
Requisite for VBAC• Previous low cervical incision
• No CPD
• No placenta previa or abruption
• “double set up” and prep
• Careful monitoring oxytoxics
• single fetus
• vertex presentation

Malpresentations

Breech extraction step 1

Breech extraction step 2

Breech extraction step 3

Breech extraction step 4

Breech delivery (Piper forceps to aftercoming head)
Shoulder Dystocia
Etiology
• Macrosomia due to maternal diabetes
• Prolonged gestation
• Fetal anencephaly

Shoulder dystocia delivery
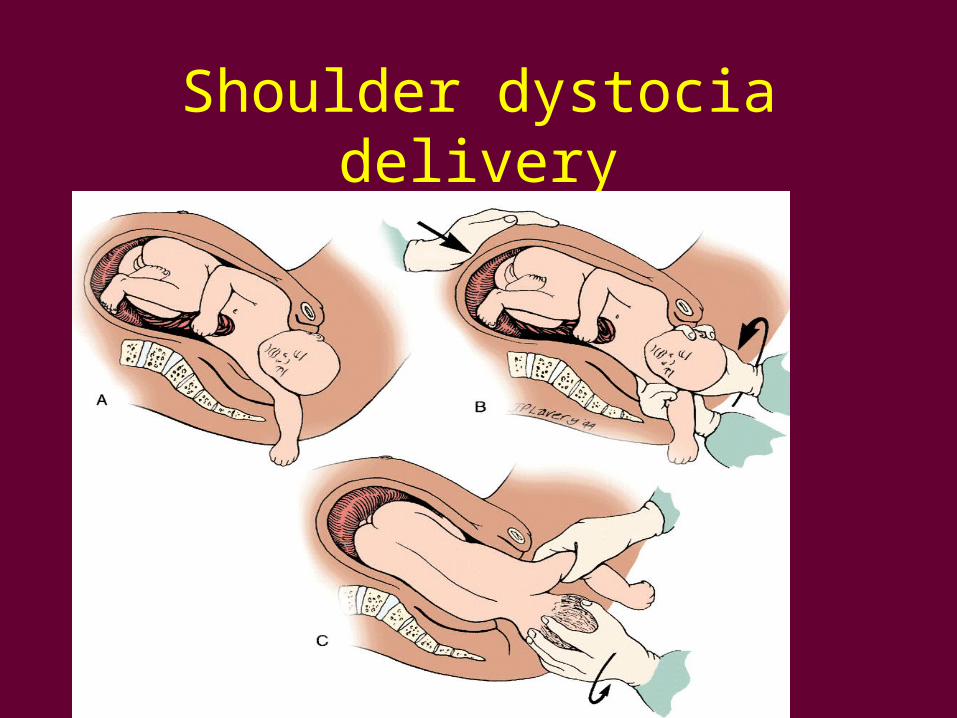
Shoulder dystocia delivery

Uterine Atony
• Large baby
• Long labor
• grand multipara
• multiple gestation
• MgSO4
• Retained placenta
