intestinal microbiota and glycemic...
TRANSCRIPT

4/3/2018
1
Intestinal Microbiota and Glycemic Control
Cynthia Lieu, Pharm.D., BCNSPLena Haddad, Ana Barron, Marina Boulos, Laila Fard
University of Southern California, School of PharmacyApril 15, 2018
Objectives
• Describe conditions that influence the composition of the intestinal microbiota
• Discuss the differences in the composition of the intestinal microbiota observed in individuals with and without diabetes
• Discuss interventions that impact glycemic control and diabetes through their effects on microbial balance
• Evaluate prebiotics, probiotics, specific nutrients, and dietary plans that impact glycemic control and diabetes through their effects on the intestinal microbiota
Microbiota
• Variable
– Inter-individual
– Intra-individual
• Predominantly bacteria
• Increased richness & diversity: better health
• Influenced by:
– Mode of birth
– Feeding after birth
– Environment
– Diet
• Influences health

4/3/2018
2
Intestinal microbiota
• Metabolism of nutrients
• Synthesis of vitamins
• Conversion of bile acids
• Modulation of immune system
• Defense against opportunistic pathogens
• Regulation of intestinal barrier function
• Xenobiotic metabolism
Predominant bacterial phyla in the human body
Phylum Class Examples
Firmicutes Bacilli; Clostridia Lactobacillus; Ruminococcus;Clostridium; Staphylococcus; Enterococcus; Faecalibacterium
Bacteroidetes Bacteroidetes Bacteroides;Prevotella
Proteobacteria Gammaproteobacteria; Betaproteobacteria
Escherichia; Pseudomonas
Actinobacteria Actinobacteria Bifidobacterium; Streptomyces; Nocardia
Pediatrics 2012: 129: 950-960
GI Microbiota: Type 2 Diabetes Mellitus
(T2DM) vs Healthy Individuals

4/3/2018
3
Overview of Differences in GI Bacteria T2DM vs. Healthy Individuals
Differences in GI Bacteria, T2DM vs. Healthy: Phyla Bacteroidetes and Firmicutes
● T2DM: Significant decrease in number of organisms from Phylum Firmicutes1
● Elevated number of organisms from Phylum Bacteroidetes1
○ Bacteria of this phylum are known to increase after consumption of fatty foods
● Bacteroidetes/Firmicutes (B/F) ratio significantly and positively correlates with reduced glucose tolerance1
1. Larsen N, et al. PLoS ONE. 2010; 5(2): e9085.
Differences in GI Bacteria, T2DM vs. Healthy: Short Chain-Fatty Acid producing bacteria
● T2DM: marked decrease in number of Short-Chain Fatty Acid (SCFA) producing Bacteria, including1,2,3:○ Eubacterium rectale○ Roseburia intestinalis○ Akkermansia muciniphila○ Faecalibacterium prausnitzii
● Short Chain Fatty Acids3,4,5,6
○ Decrease pro-inflammatory cytokine concentration and mucosal inflammation
○ Improve beta cell function○ Stimulate GLP-1 release
1. Qin, et al. Nature. 2012; 490(7418):55-60, 2. Zhang, et al. PLoS ONE. 2013; 8(8):e71108, 3. Sekirov, et al. Physiological Reviews. 2010; 90(3): 859-904, 4. McNeil. AmJClNut. 1984; 39(2): 338-342, 5. Kumar, et al. B J Nutr. 2011; 105: 561-73, 6. Zhao et al. Science. 2018; 359:1151-1156
4/3/2018
4
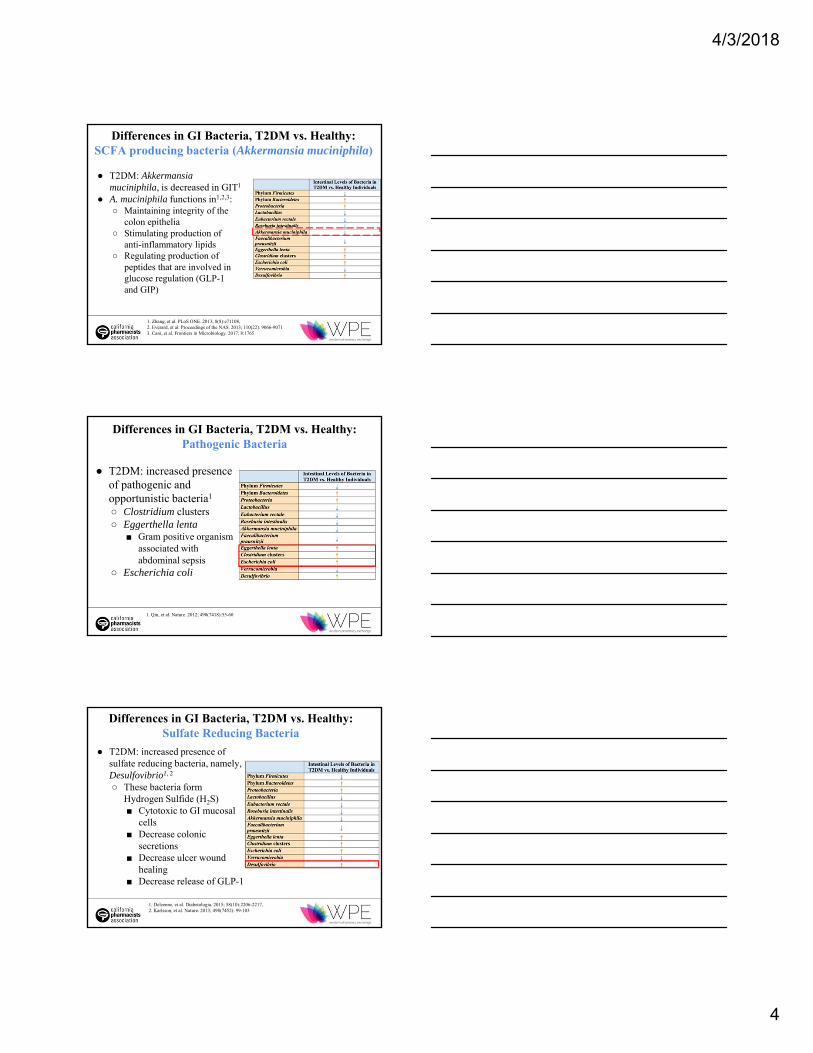
Differences in GI Bacteria, T2DM vs. Healthy: SCFA producing bacteria (Akkermansia muciniphila)
● T2DM: Akkermansiamuciniphila, is decreased in GIT1
● A. muciniphila functions in1,2,3:○ Maintaining integrity of the
colon epithelia○ Stimulating production of
anti-inflammatory lipids○ Regulating production of
peptides that are involved in glucose regulation (GLP-1 and GIP)
1. Zhang, et al. PLoS ONE. 2013; 8(8):e71108, 2. Everard, et al. Proceedings of the NAS. 2013; 110(22): 9066-90713. Cani, et al. Frontiers in Microbiology. 2017; 8:1765
Differences in GI Bacteria, T2DM vs. Healthy: Pathogenic Bacteria
● T2DM: increased presence of pathogenic and opportunistic bacteria1
○ Clostridium clusters○ Eggerthella lenta
■ Gram positive organism associated with abdominal sepsis
○ Escherichia coli
1. Qin, et al. Nature. 2012; 490(7418):55-60
Differences in GI Bacteria, T2DM vs. Healthy: Sulfate Reducing Bacteria
● T2DM: increased presence of sulfate reducing bacteria, namely, Desulfovibrio1, 2
○ These bacteria form Hydrogen Sulfide (H2S)■ Cytotoxic to GI mucosal
cells ■ Decrease colonic
secretions■ Decrease ulcer wound
healing■ Decrease release of GLP-1
1. Delzenne, et al. Diabetologia. 2015; 58(10):2206-2217,2. Karlsson, et al. Nature. 2013; 498(7452): 99-103
4/3/2018
5
T2DM: An Overview● T2DM: characterized by elevated plasma glucose,
deficit in secretion/action of insulin and incretins, and low level inflammation1,2
○ Moderate excess in systemic cytokine levels1
○ Cytokines activate Toll-like Receptors on peripheral tissues ■ Results in phosphorylation of proteins
regulating normal signaling through the insulin receptor1
■ Leads to peripheral insulin resistance
1. Moreno-Indias, et al. Frontiers in Microbiology. 2014; 5:190. 2. Shoelson, SE. J Clin Invest. 206; 116(8):2308-2318
T2DM: An Overview...continued● Key molecule involved in triggering inflammation →
Lipopolysaccharide (LPS)1
● Phylum Bacteroidetes: increased in those with T2DM
● LPS from these Gram negative organisms is shed
○ LPS translocates across the intestinal mucosa and triggers release of pro-inflammatory cytokines
○ Innate inflammatory process is triggered ■ Leads to the beta cell damage and insulin resistance
1. Moreno-Indias, et al. Frontiers in Microbiology. 2014; 5.
How does dysbiosis inside the intestine affect health/disease pathogenesis? A possible mechanism
● T2DM: increased intestinal permeability○ Impairment of tight junctions1
○ Results in translocation of bacterial endotoxin (LPS) paracellularly1
○ Mechanism producing low grade inflammation characteristic of T2DM1
● Modulating gut microbiota composition with prebiotics:1
○ Improved gut permeability○ Decreased inflammation○ Improved glucose tolerance
1. Han JL, Lin HL. 2014. World J Gastroenterol. 2014; 20(47):17737-45.

4/3/2018
6
Drugs & the microbiota
Alterations in intestinal microbiota:
How medications used to treat T2DM affect the microbiota
Metformin
Known MOA1
Activates AMPK
↓ glucose production in the liver
↑ insulin sensitivity
Enhancesglucose utilization
Mouse studies:
There may be more
Metforminmodulates the
gut microbiota towards a more beneficial state
1. Rotella et al. Curr Diabetes Rev 2006; 2(3): 307-315

4/3/2018
7
Akkermansia spp. population in lean vs obese mice1
Lean Mouse Obese/T2DM Mouse
Greater abundance of Akkermansia spp.
Decreased abundance of Akkermansia spp.
Presence of Akkermansia spp. inversely correlates with body weight in rodents & humans1
VS
1. Everard et al. Proc Natl Acad Sci U S A 2013; 110(22): 9066-9071.
Effect of Metformin on the gut microbiota of HFD-fed diabetic mice1
High Fat Diet (HFD)-fed, diabetic mouse
Metformin
↑ abundance of Akkermansia spp1,2
Correlated with improved metabolic parameters:- Amelioration of glucose intolerance1
- Reversed metabolic endotoxemia & insulin resistance3
1. Shin et al. Gut. 2014; 63: 727-7352. Lee et al. Appl Environ Microbiol 2014; 80(19): 5935-59433. Everard et al. Proc Natl Acad Sci U S A 2013; 110(22): 9066-9071
Significance:These findings suggest that:
Aside from its well-know MOA,
metformin may also be achieving its efficacy via its
modulation of the gut microbiota towards a more beneficial state
Pharmacologic manipulation of the
gut microbiota in favor of
Akkermansia spp. may be a potential
treatment for T2DM1.
Akkermansia spp. has a potential
role as a probiotic with antidiabetic
effects.1
*These were findings from mouse studies;
still need human studies
1. Shin et al. Gut. 2014; 63: 727-735

4/3/2018
8
Effect of Liraglutide on the microbiota of hyperglycemic mice1
Hyperglycemic mouse
Liraglutide
Changed overall structure of mouse’s microbiota by leading to:
↓ obesity-related phylotypes
↑ lean-related phylotypesAND
May be reason behind Liraglutide’s weight loss effect1
1. Wang et al. Sci Rep. 2016; 6: 33251
Effect of Saxagliptin on the microbiota of hyperglycemic mice1
In T2DM:
Bacteroides
Firmicutes
Decreased F to B ratio1
(Dysbiosis)
Saxagliptinadministration to
hyperglycemic mice
↑ F to B ratio1
(possibly correcting some of
the dysbiosis characteristic of
T2DM)
1. Wang et al. Sci Rep. 2016; 6: 33251
Effect of Sitagliptin on the microbiota of obese & T2DM rats1
Obese/T2DM Rat
Sitagliptin
↑ Roseburia1
(SCFA-producing bacteria)
↑ Bifidobacterium1
Improved insulin
sensitivity2
Improved glucose tolerance
& low-grade inflammation3,4
1. Yan et al. J Diabetes Res 2016; 2016: Article ID 20931712. Karlsson et al. Nature 2013; 498(7452): 99-1033. Cani. Gut.2009; 58(8): 1091-11034. Cani. Diabetologia 2008; 51: S34-S35

4/3/2018
9
Alterations in intestinal microbiota:
How medications that affect the gut microbiota may impact the risk of
T2DM/Obesity
Effect of antibiotics on the gut microbiota: overview
Antibiotics
Marked short-term
disturbances in the human gut
microbiota
Often incompleterecovery of gut
flora to its initial composition.1-4
Linked with development of obesity &
T2DM5-7
Use in children
associated with obesity later in life6
Significantly reduce
bacterial diversity in
the gut8
Broad > Narrow-spectrum8
1. Panda et al. PLoS One 2014; 9(4): e954762. Jernberg et al. ISME J 2007; 1: 56-663. Jakobsson et al. PLoS One 2010; 593); e98364. Dethlefsen et al. Proc Natl Acad Sci U S A 2010; 108 Suppl 1: 4554-45615. Thuny et al. PLoS One 2010; 5(2): e90746. Bailey et al. JAMA Pediatr 2014; 168(11): 1063-10697. Mikkelsen et al. J Clin Endocrinol Metab 2015; 100: 3633-36408. Czaja et al. Nutrition Health Food Sci 2017; 5(4): 1-21
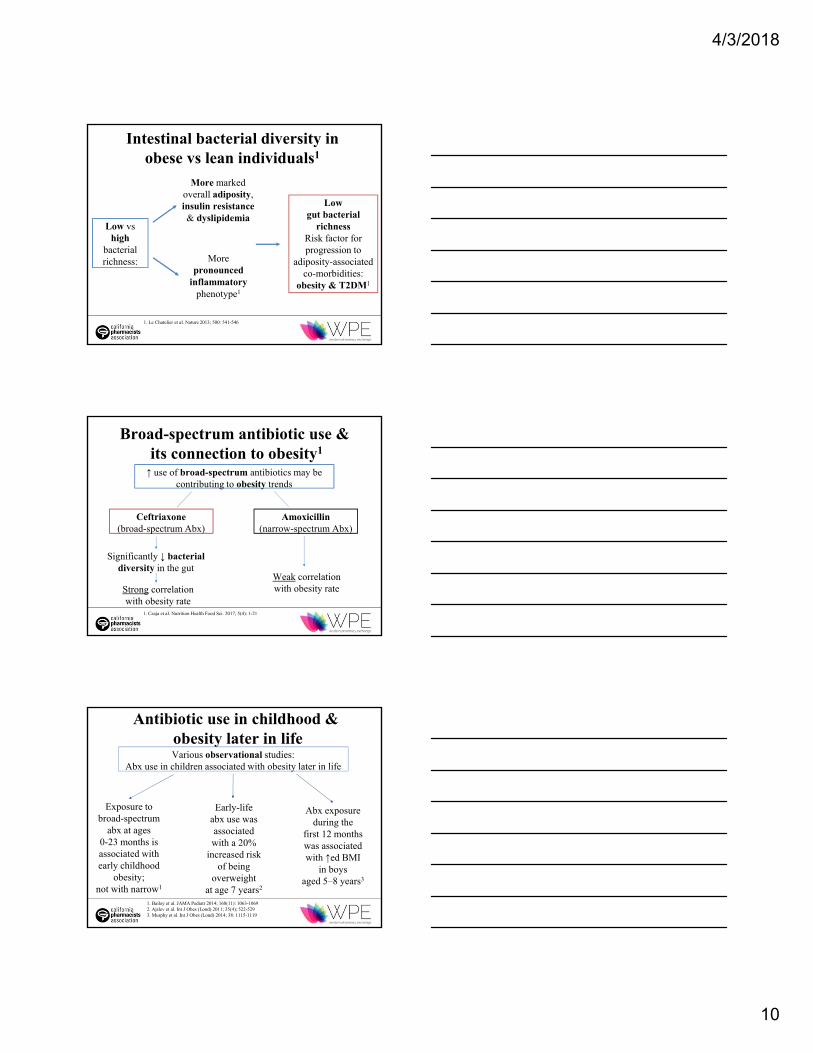
Intestinal bacterial diversity in obese vs lean individuals1
Obese
Low intestinal bacterial diversity
VS
1. Le Chatelier et al. Nature 2013; 500: 541-546
Lean
Greater intestinal bacterial diversity
4/3/2018
10
Low vs high
bacterial richness:
More marked overall adiposity, insulin resistance & dyslipidemia
More pronounced
inflammatory phenotype1
Low gut bacterial
richnessRisk factor for progression to
adiposity-associated co-morbidities:
obesity & T2DM1
Intestinal bacterial diversity in obese vs lean individuals1
1. Le Chatelier et al. Nature 2013; 500: 541-546
Broad-spectrum antibiotic use &its connection to obesity1
↑ use of broad-spectrum antibiotics may be contributing to obesity trends
Ceftriaxone(broad-spectrum Abx)
Amoxicillin(narrow-spectrum Abx)
Weak correlation with obesity rateStrong correlation
with obesity rate
Significantly ↓ bacterial diversity in the gut
1. Czaja et al. Nutrition Health Food Sci. 2017; 5(4): 1-21
Antibiotic use in childhood &obesity later in lifeVarious observational studies:
Abx use in children associated with obesity later in life
Exposure to broad-spectrum
abx at ages 0-23 months is associated with early childhood
obesity; not with narrow1
Abx exposure during the
first 12 months was associated with ↑ed BMI
in boys aged 5–8 years3
Early-life abx use was associated with a 20%
increased risk of being
overweight at age 7 years2
1. Bailey et al. JAMA Pediatr 2014; 168(11): 1063-10692. Ajslev et al. Int J Obes (Lond) 2011; 35(4); 522-5293. Murphy et al. Int J Obes (Lond) 2014; 38: 1115-1119

4/3/2018
11
Conclusion● Overall, these studies highlight the importance of implementing
more restricted use of antimicrobial agents
● Antibiotic use may damage the gut flora and lead to dysbiosisthat may contribute to the development of obesity & T2DM
● Implementation of appropriate antibiotic stewardship programs is critical, and ensures that that:○ Broad-spectrum antibiotics are only used when absolutely
necessary○ Regimens are promptly de-escalated when cultures and
sensitivities (C&S) are available○ Duration of therapy with broad-spectrum agents is limited
Food & the microbiota
Different Diets & the Microbiota
1.Kim, et al., Environ Microbiol Rep, 2013, 5: 765-7752.Fallucca, et al., Diabetes Metab Res Rev, 2014, 30: 48-54 3.Xiao, et al., Microbiol Ecol, 2014, 87: 357-367
4/3/2018
12
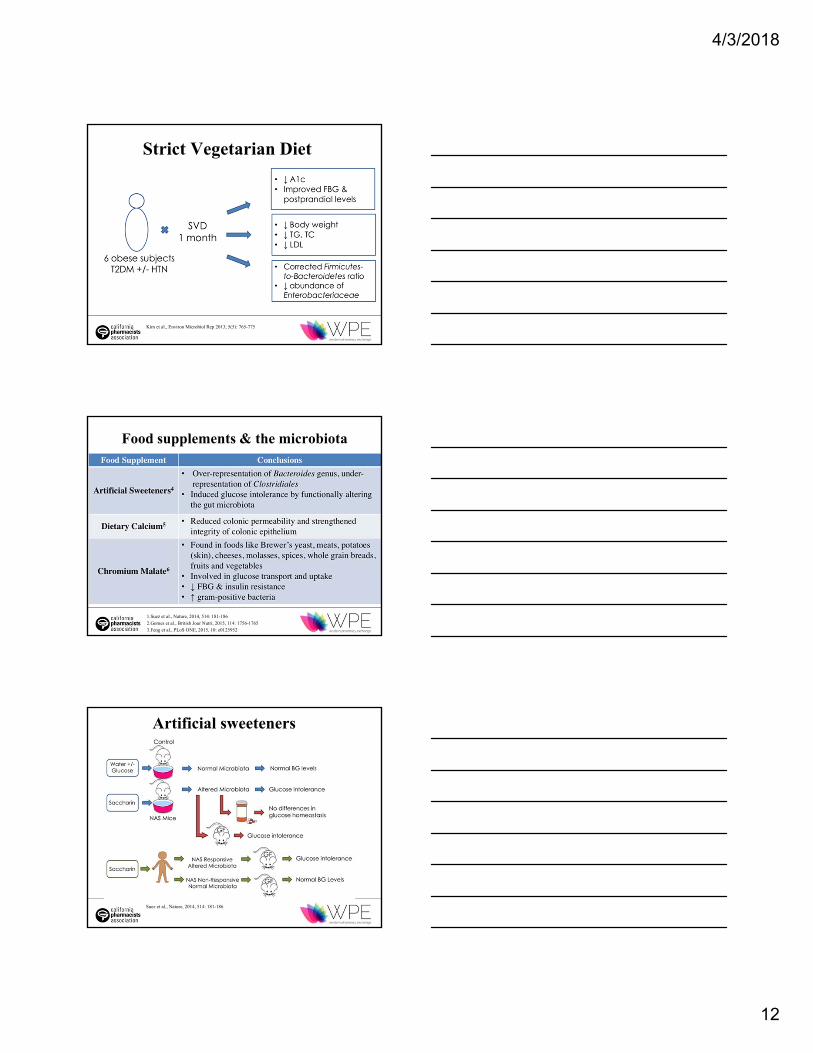
Strict Vegetarian Diet
Kim et al., Environ Microbiol Rep 2013; 5(5): 765-775
Food supplements & the microbiota
1.Suez et al., Nature, 2014, 514: 181-1862.Gomes et al., British Jour Nutri, 2015, 114: 1756-17653.Feng et al., PLoS ONE, 2015, 10: e0125952
Artificial sweeteners
Suez et al., Nature, 2014, 514: 181-186

4/3/2018
13
Food supplements & the microbiota... continued
1. Zhu et al., Intern Journ Food Sci & Nutr, 2016, 67: 686-6952. Roopchand et al., Diabetes, 2015, 64: 2847-2858
Conclusions
• Diets that are low in calorie and high in fiber are most influential in improving glucose intolerance
• Try to avoid consistently using artificial sweeteners, especially saccharin (Sweet’N Low)
• Calcium, chromium malate, bitter melon, and dietary polyphenols can benefit an individual with T2DM
Prebiotics/Probiotics & the microbiota

4/3/2018
14
Good Sources of Probiotics & Prebiotics
1. Le Barz M et al. Diabetes Metab J. 2015;39:291-3032. Gibson GR et al. Nutr. Res. Rev.2004;17:259–275
Effects of Prebiotics

4/3/2018
15
1. Dehghan P et al. Nutrition. 2014;30(4):418-423
2. Gibb RG et al. Am J Clin Nutr. 2015, 102: 1604-16133. Maki KC et al. J Nutr. 2012;142(4):717–234. Maziarz MP et al. Nutrition Journal. 2017;16(1)
Effects of Probiotics
VSL #3• 8 beneficial lactic acid bacteria1
– B. longum, B. infantis, B. breve, L. acidophilus, L. casei, L. delbrueckii ssp. bulgaricus, L. plantarum and Streptococcus salivarius ssp. thermophilus
• ↓ inflammatory mediators: TNF-alpha, IL-6, and hs-CRP1
– Compromise intestinal integrity– Complicate metabolic diseases
• Prevented ↑ in serum insulin concentration and rise in insulin resistance1
1. Jafarnejad S et al. Journal of Nutrition and Metabolism. 2016;1-8

4/3/2018
16
1. Asemi Z et al. Annals of Nutrition and Metabolism. 2013;63(1-2):1-92. Simon M et al. Diabetes Care. 2015; 38: 1827-18343. Everard A et al. mBio. 2014;5(3)4. He C, Shan Y, Song W. Nutrition Research. 2015; 35:361-367.
Fecal microbiota transplantation (FMT)
• Transfer of intestinal microbiota
• From healthy donor to patient
• To introduce or restore a stable microbial community in the gut
• Manipulation of altered intestinal microbiota
• Reinstall depleted bacterial species associated with disease
Xu, et al. World J Gastroenterol 2015; 21(1): 102-111
FMT: potential for increasing insulin sensitivity
• Double blind, randomized controlled trial
• 18 M, metabolic syndrome
• Half received fecal microbiota infusion from lean male donors (allogenic group), vs self-collected feces (control)
• After 6-wk infusion of microbiota from lean donors, marked increase:
– Insulin sensitivity
– Levels of butyrate-producing intestinal microbiota
• No significant changes found in control group
Vrieze, et al. Gastroenterology 2012; 143: 913-916

4/3/2018
17
FMT: potential for increasing insulin sensitivity
• 38 M, metabolic syndrome, BMI ≥ 30
• Fecal microbiota infusion from lean M donors, BMI < 25 (allogenic), vs own (autologous = control)
• 18 wks after FMT: microbiota similar to baseline; no significant effects on insulin sensitivity; no wt change
• 6 wks after FMT: responders vs non-responders
– Altered microbiota composition
– Peripheral & hepatic insulin sensitivity increased
– Significant increase in Akkermansia muciniphila
– Metabolic response dependent on decreased fecal microbial diversity at baseline
Knotte, et al. Cell Metab 2017; 26(4): 611-619.e6
Thank You!
Ana BarronUSC School of PharmacyEmail: [email protected]
Marina BoulosUSC School of Pharmacy Email: [email protected]
Laila FardUSC School of PharmacyEmail: [email protected]
Speaker Contact Information:
Lena HaddadUSC School of PharmacyEmail: [email protected]
Cynthia L. Lieu, Pharm.D, BCNSPUSC School of PharmacyOffice: (323) 442-1472Email: [email protected]