international journal of physiotherapy and research, int j ... · manual therapy techniques like...
TRANSCRIPT

Int J Physiother Res 2015;3(1):875-84. ISSN 2321-1822 875
Original Article
IMMEDIATE EFFECT OF THREE SOFT TISSUE MANIPULATIONTECHNIQUES ON PAIN RESPONSE AND FLEXIBILITY IN CHRONICPLANTAR FASCIITIS: A RANDOMIZED CLINICAL TRIALRenu B.Pattanshetty *1, Amit S.Raikar 2.*1 Assistant Professor, KLEU Institute Of Physiotherapy, Belgaum, Karnataka, India.2 Post Graduate Student, KLEU Institute Of Physiotherapy, Belgaum, Karnataka, India.
Background and Objectives: Plantar fasciitis is a common foot disorder in which patients have pain andtenderness at the sole of the foot. Rest, exercises, orthotics, taping, cryotherapy, therapeutic ultrasound, electricalstimulation, whirlpool bath, and iontophoresis have been widely used to relieve plantar pain. Long term use ofmanual therapy techniques like myofascial release technique, positional release therapy and passive stretchinghave been used in the past to reduce pain and improve ankle range of motion. The present study aimed toevaluate and compare the immediate effectiveness of myofascial release technique, positional release therapyand passive stretching on pain response and ankle flexibility in chronic plantar fasciitis.Material and methodology: A total of 60 participants with chronic plantar fasciitis were randomly allocated toGroup A (myofascial release group) and Group B (positional release group) and Group C (passive stretching).Therapeutic ultrasound with intensity of 1W/cm2 and frequency of 1MHz for 5 min was given for a singlesession to all the patients and then given the manual techniques. Visual analogue scale, range of motion of theankle were outcome measures that were assessed pre- and immediately post-interventional.Results: The study demonstrated statistical significant reduction in pain, in all three groups (p<0.0001). Anklerange of motion showed significant improvement in Group A (MFR). Group C (passive stretching) demonstratedsignificant improvement (p=0.001) as compared to Group B (PRT).Conclusion: All three manual techniques with therapeutic ultrasound were effective in immediate relief of painand improving ankle range of motion in subjects with chronic plantar fasciitis.KEYWORDS: Plantar fasciitis, myofascial release, positional release therapy, passive stretching, therapeuticultrasound.
ABSTRACT
INTRODUCTION
Address for correspondence: Dr. Renu B. Pattanshetty, MPT; Ph.D. Assistant Professor, KLEUInstitute Of Physiotherapy, Belgaum-590010, Karnataka, India. Contact No.: +919448482564E-Mail: [email protected]
International Journal of Physiotherapy and Research,Int J Physiother Res 2015, Vol 3(1):875-84. ISSN 2321-1822
DOI: 10.16965/ijpr.2015.101
The human ankle/foot complex meet the stabilitydemands of providing a stable base of supportfor the body in a variety of weight bearingpostures without undue muscular activities andenergy expenditure, and acting as a ‘rigid’ leverfor the mobility demands by dampening of rotat-
ions imposed by the more proximal joints of thelower limb,being flexible to absorb the shock ofthe superimposed body weight as the foot hitsthe ground and allowing the foot to conform tothe changing and varied terrain on which thefoot is placed. Four of Cailliet’s criteria fornormal foot are absence of pain, normal musclebalance, central heel and straight and mobile
Quick Response code
Access this Article online
International Journal of Physiotherapy and ResearchISSN 2321- 1822
www.ijmhr.org/ijpr.html
DOI: 10.16965/ijpr.2015.101
Received: 07-01-2015Peer Review: 07-01-2015Revised: None
Accepted : 23-01-2015Published (O): 11-02-2015Published (P): 11-02-2015

Int J Physiother Res 2015;3(1):875-84. ISSN 2321-1822 876
Renu B.Pattanshetty, Amit S.Raikar. IMMEDIATE EFFECT OF THREE SOFT TISSUE MANIPULATION TECHNIQUES ON PAIN RESPONSE ANDFLEXIBILITY IN CHRONIC PLANTAR FASCIITIS: A RANDOMIZED CLINICAL TRIAL.
toes [1].Plantar fascia called as plantar aponeurosis, liessuperficial to the muscles of the plantar surfaceof the foot. It has thick central part which coversthe central muscle of the 1st layer, Flexordigitorum brevis and is immediately deep to thesuperficial fascia of the plantar surface. It actsas a truss, maintaining the medical longitudinalarch of the foot, and assists during the gait cycleand facilities shock absorption during weightbearing activites[2].Foot complaints are common in general practiceand their incidence increases with age. Threeout of four people complains of foot pain duringthe course of a life time [3], While approximately20% of people aged 65 years or older complainsof non traumatic foot problems [4]. Plantarfasciitis has been experienced by 10% of thepopulation [5].The foot is subjected to various types of injurieslike laceration, contusion, ligaments sprains andrupture, fracture, penetrating wounds, etc Inaddition, pathologic changes are imposed on thefoot by congenital abnormalities, bacterial andfungal infections and dermatologic lesions, illfitting shoes,walking on hard surfaces [6].Different authors have described heel pain asachilles spurs, retrocalcaneal bursitis,subcalcaneal pain, posterior heel pain, plantarfasciitis etc. Heel pain commonly occurs inweight bearing due to inflammation of thicktissue at the sole. Stress to plantar fascia mayalso result from injury, or a bruise incurred whilewalking, running, or jumping on hard surfaces;or being overweight [7]. Hence, causes of heelpain may be described as plantar, lateral, medial,posterior, and diffuse [8], and may either becaused due to injury to the soft tissue, bone,nerve or plantar fascia [9].Plantar fasciitis an inflammation of the plantarfascia is one of the most common causes of footpain in which pain and tenderness are locatedinferiorly at the plantar fascia origin [10]. It ismore common in sports that involves running,long distance walking, dances, tennis players,basket ball players and non athletes whoseoccupation requires prolonged weight bearing[11]. Other causes are mechanical stressinvolving compressive forces making foots
longitudinal arch flat [5]. Repeated microtraumas cause inflammation at the origin of theplantar fascia over the calcaneal medicaltuberosity. Traction forces during the supportphase on gait lead to an inflammatory process,resulting in fibrosis and degeneration [12].There is a loss of flexibility as the diseaseprogresses due to calcaneal tendon retraction,fatigue, fascial inextensibility, and poormechanics [5].Though etiology is unknown in approximately85% of cases, plantar fasciitis can occur inassociation with various arthritides. In anathlete, plantar fasciitis appears to beassociated with overuse, training errors, trainingon unyielding surfaces and improper orexcessively worn foot wear. Sudden increase inweight bearing activity, particularly thoseinvolving running can cause micro-trauma to theplantar fascia. In elderly adults, plantar fasciitisis often attributable to poor intrinsic musclestrength and poor force attenuation secondaryto acquired pesplanusand compounded by adecrease in the body’s healing capacity [13].Patients with plantar fasciitis typically presentwith inferior heel pain on weight bearing andpain often persist for months to years. Pain maybe throbbing, searing or piercing, especially withthe first few steps in the morning or after periodsof inactivity. The discomfort often improves afterfurther ambulation but worsens with continuedactivity, often limiting daily activities. Thepatient usually has tenderness around themedial calcaneal tuberosity at the plantaraponeurosis [14].Medical and surgical management for plantarinclude non-steroidal anti inflammatory drugs,local cortisone injections, resection of thecalcaneal spur or part of the plantar fascia nearits origin, stripping off the soft tissue from theplantar surface of the calcaneus and excisionof the medial inferior tubercle of the calcaneus.Other therapies include acupuncture, electrongenerating devices, insoles with magnetic foil,extracorporeal shock wave therapy [15].Various physiotherapy treatment protocols havebeen advocated in the past such as rest, taping,orthotics,silicon heel cups, stretching, myo-fascial release and positional release therapy.

Int J Physiother Res 2015;3(1):875-84. ISSN 2321-1822 877
Renu B.Pattanshetty, Amit S.Raikar. IMMEDIATE EFFECT OF THREE SOFT TISSUE MANIPULATION TECHNIQUES ON PAIN RESPONSE ANDFLEXIBILITY IN CHRONIC PLANTAR FASCIITIS: A RANDOMIZED CLINICAL TRIAL.
Electrotherapy modalities liketherape-uticultrasound, phonophoresis, laser, microwavediathermy, iontophoresis, cryotherapy, contrastbath have been tried in past. Non weight-bearingstretching exercises have shown to helpful inreducing severe pain which occurs in the morning[16].Therapeutic Ultrasound is a method of applyingdeep heat to connective tissue [15] which playsan important role in relieving plantar heel painby both thermal and mechanical effect on targettissue resulting in increased local metabolism,circulation and extensibility of connective tissueand tissue regeneration. To obtain increase inthe viscoelastic properties of collagen, anelevation in tissue temperature of greater than3° to 4°C is indicated [17].Stretching of the shortened and contractedplantar flexors may positively influence anindividual’s functional activities of daily livingand decrease the risk of injury. Regardless ofthe type of fitness and rehabilitation program,the goal of stretching is to change the physicalcharacteristics of connective tissue [18].Myofascial release technique is a soft tissuemobilization technique mostly given in thechronic conditions that causes tightness andrestriction in soft tissues. This technique hasbeen proposed to act as a catalyst in theresolution of chronic plantar fasciitis [19].Positional release therapy is an indirectmyofascial technique focused on the neurologiccomponent of the neuro-vascular myofascialsomatic dysfunction.This technique is proposedto increase muscle flexibility by placing themuscle in a shortened position to promote-muscle relaxation in contrast to placing themuscle in a lengthened or stretched position[20].Since there is dearth of literature to show theimmediate effectiveness of myofascial releasetherapy, positional release technique andpassive stretching, in chronic plantar fasciitis,the present study was proposed to evaluate andcompare the three manual techniques onimmediate response to pain and flexibility inchronic plantar fasciitis. It was hypothesized thatthere would be no difference in pain andflexibility with myofascial release, positional
release therapy and passive stretching after asingle session in chronic plantar fasciitis.
METHODOLOGY
Participants: Subjects between 18 and 60 yearsold with chronic plantar fasciitis with durationof more than three months and willing toparticipate in the study were recruited. The datawas collected from the physiotherapy outpatientdepartment at an Indian tertiary care set-upduring the study period extending from ninemonths.Subjects were excluded if they hadclinical disorder where therapeutic ultrasoundis contraindicated such as infective conditionsof foot, tumor, and calcaneal fracture, metalimplant around ankle, Subjects with clinicaldisorder where myofascial release iscontraindicated such as dermatitis, Ankleankylosis, congenital foot deformities,corticosteroids injection in heel in past threemonths and subjects with referred pain due tosciatica and other neurological disorders wereexcluded.Ethical approval for the study was granted bythe Institutional Ethical Committee and theprocedures were conducted according to thedeclaration of Helsinki.Study design: This study was pre postexperimental design with random allocation ofthe subjects by envelope method to either ofthe three groups (myofascial group, positionalrelease group and passive stretching group)using non probability sampling method. Totalnumber of Sample size was calculated to be 60participants ( error = 80 and level ofsignificance = p 0.05)Procedure: Subjects were initially examined forassessing compliance with inclusion andexclusion criteria. In addition, demographic andanthropometry data of each subject wererecorded. After this initial evaluation, they wererandomly allocated to one of the three studygroups A, B and C respectively.Group A: Myofascial release group [19]Participants were placed in prone lying positionwith foot placed outside the plinth. Then the partwas cleaned and gel was applied to the involvedsite and then transducer head was moved in slowcircular manner for 5 minutes. Subjects underwe-
α≤

Int J Physiother Res 2015;3(1):875-84. ISSN 2321-1822 878
nt myofascial release manually by using thumband plantar cupping by using heel of hand andfingers technique for 10 min in supine lying forsingle session (photograph no. 2).Group B: Positional release group [20]Subjects were given positional release techniquemanually by applying brief mechanical pressureon the tender point with one fingertip in orderto determine tenderness. The foot was thenpositioned, into pure plantar flexion and gentlefine tuned by rotation, until the score in thetender point reduced to at least 70%. Thisposition was held for 90 seconds followingwhich slow release of pressure was applied andreturned to neutral position; this was carried outin a single session (Photograph. 3).Group C: passive stretching group [18] For stretching ankle plantar flexors , firstly the
Fig. 1: Consort Study Flow Chart.
soleus muscle was stretched with knee flexedand then gastrocnemius muscle was stretchedwith knee extended, over pressure was placedup on the bottom of the foot while the anklewas held in dorsi-flexion in supine lying. Passiveplantar fascia stretching was performed insupine lying by application of force distal to themetatarsophalangeal joints on the affected side,pulling the toes upward towards the shin until astretch was felt in the sole of the foot.Stretchings were performed for three repetitionseach held for count of 30 sec for a single sessionin supine lying (Photograph no. 3).Therapeutic ultrasound with intensity of1W/cm2 and frequency of 1MHz for 5 min wasgiven for a single session to all the patients.(Photograph no. 1)
Renu B.Pattanshetty, Amit S.Raikar. IMMEDIATE EFFECT OF THREE SOFT TISSUE MANIPULATION TECHNIQUES ON PAIN RESPONSE ANDFLEXIBILITY IN CHRONIC PLANTAR FASCIITIS: A RANDOMIZED CLINICAL TRIAL.

Int J Physiother Res 2015;3(1):875-84. ISSN 2321-1822 879
Renu B.Pattanshetty, Amit S.Raikar. IMMEDIATE EFFECT OF THREE SOFT TISSUE MANIPULATION TECHNIQUES ON PAIN RESPONSE ANDFLEXIBILITY IN CHRONIC PLANTAR FASCIITIS: A RANDOMIZED CLINICAL TRIAL.
Outcome measures:
1. Pain: This was recorded by 10 cm horizontalvisual analogue scale (VAS), the participantswere asked to mark their intensity of pain on a10 cm long line in the data collection sheet withnumbers 0 to 10 where 0 symbolized no painand 10 was severe pain.2. Ankle Range Of Motion (ROM): Ankle plantarand dorsi flexion ROM was measured byUniversal Goniometer. They were measured withsubjects in high sitting position with ankle placedin 90º as the starting position, this reading wastransposed and recorded as 0º.The Fulcrum wascentered over the lateral aspect of the lateralmalleolus, the proximal arm aligned with thelateral midline of the fibula, using the head offibula as the reference and the digital armparallel to the lateral aspect of the 5th
metatarsal. The average of the three readingswas recorded.VAS score and ROM for each group weremeasured pre and immediately post intervention,in all the 3 groups.
Data analysis:
Analysis of raw data was done using SPSSwindows version 13.0 version. Descriptivestatistics were used to define the demographiccharacteristics of the sample. Various statisticalmeasures such as mean, standard deviation andtests of significance such as Chi-Square test,student paired ‘t’ test, one-way Analysis ofVariance (ANOVA) and multiple comparisonScheffe test were utilized for this purpose.Nominal data using ‘F’ test , ANOVA andChi-Square test was done. Intra groupcomparison of the pre interventional and postinterventional outcome measures was done byusing student paired ‘t’ test whereas one wayANOVA and multiple comparison Scheffe testwas used to measure the inter group difference.Probability values less than 0.05 were consideredstatistically significant ( p 0.05).≤
RESULTSA total of 60 subjects with chronic plantarfasciitis accepted to participate in the study outof which 30 were males and 30 were females.There were 11 males and 9 females in group A,9 males and 11 females in group B, 10 males
and 10 females in group C. (c2 = 0.40, p=0.8187).The average age of the subjects in group A was34.25 ± 13.89 years, group B subjects was 36.60± 14.58 years and group C subjects mean agewas 37.85 ± 13.78 years. Age was well matchedin all three groups (F= 0.3367, p= 0.7155). Therewas no significant difference between the meanBMI values of the subjects in three the groups.(F= 0.4794,p= 0.6216)The pre-interventional values of Visual analoguescore within the group was 7.92 ± 0.98, 7.30 ±1.68, and 7.13 ± 1.56 in group A, B and Crespectively whereas post-interventional valuesof Visual analogue score was 3.68 ± 1.71, 3.13± 1.85, and 3.78 ± 2.03, in group A, B, and Crespectively. VAS scores were statisticallysignificant post interventional for all the threegroups (p < 0.0001). The inter group analysisfor VAS showed no significant difference in thereduction of pain when compared between allthe three groups.Values of pre-interventional ankle activedorsiflexion range of motion in group A was16.60 ± 1.10 degrees, group B was 16.60 ± 1.64degrees, and group C was 16.80 ± 1.54 degreeswhereas post-interventional ankle dorsiflexionrange in group A was 20.00 ± 1.03 degrees, groupB was 17.65 ± 1.57 degrees, and group C was20.30 ± 1.13 degrees. Comparing pre- and post-interventional valuesof ankle active dorsiflexionrange of motion, values in all the three groupshad shown statistical significant difference(p<0.0001). The inter group analysis for activedorsiflexion range of motion showed statisticallysignificant difference between group A versusgroup B (p<0.0001), group A verses group Cshowed no statistically significant difference(p=0.754), group B verses group C showedstatistically significant difference (p<0.0001).Comparison of pre-interventional versus post-interventional values, all the three groupsshowed statistical significant difference(p<0.0001) in improving ankle plantarflexionrange of motion. The inter group analysis for thesame showed statistically significant differencebetween group A and group B (p=0.0025).comparison of Group B and group C showedstatistically significant difference (p=0.0263).However, group A verses group C showed nostatistically significant difference (p=0.6912).

Int J Physiother Res 2015;3(1):875-84. ISSN 2321-1822 880
Photograph1: Patient receivingtherapeutic ultrasound.
Photograph 2: Patient receivingmyofascial release therapy.
Photograph 3: Patient receivingpositional release therapy.
Photograph 4: Passive stretching ofsoleus.
Photograph 5: Stretching of plantarfascia.
Photograph 6: Passive stretchingof gastrocnemius.
Table 1: Age distribution & Anthropometric variables.
Groups Mean Age (Years)
Mean BMI
Group A 34.25 ± 13.89 24.13 ± 2.21Group B 36.60 ± 14.58 23.60 ± 2.99Group C 37.85 ± 13.78 23.37 ± 2.25
Table 2: Gender Distribution in all the three groups.
Gender Group A Group B Group CMales 11 9 10
Females 9 11 10Total 20 20 20
Table 3: Mean changes in Visual Analogue ScaleScores (cms) in all the three groups.
Pre Treatment Post TreatmentGroup A 7.92 ± 0.98 3.68 ± 1.71Group B 7.30 ± 1.68 3.13 ± 1.85Group C 7.13 ± 1.56 3.48 ± 2.03
GroupsVisual Analogue Scale (cms)
Pre Treatment Post Treatment Pre Treatment Post Treatment
Group A 16.60º± 1.10º 20.00º ± 1.03º 41.35º ± 1.87º 44.05º ± 1.76ºGroup B 16.60º ± 1.64º 17.65º ± 1.57º 40.85º ± 3.07º 41.30º ± 2.90ºGroup C 16.80º ± 1.54º 20.30º ± 1.13º 40.85º ± 2.98º 43.40º ± 2.35º
GroupsDORSI FLEXION ROM PLANTAR FLEXION ROM
Table 4: Mean differences in ankle Range of Motion(ROM in degrees) in all the three groups.
Table 5: Comparison of VAS and ankle range of motionin all the three groups.
Dorsiflexion ROM Plantar-flexion ROM
Value
Visual Analogue Scale
Pre Treatment Vs. Post Treatment
Groups
<0.0001 Significant
Group A p
Group B p<0.0001
Significant<0.0001
Significant<0.0001
Significant<0.0001
SignificantGroup C p
Pre Treatment Vs.
Post Treatment
Pre Treatment Vs.
Post Treatment<0.0001
Significant<0.0001
Significant0.00043
Significant<0.0001
Significant
Table 6: Comparison of visual analogue scale score(VAS) in all the three groups (pre and post interventional)
VAS Score Source of variance SS DF MS F ‘p’Between group 6.9803 2 3.4902Within group 117.909 57 2.0686
Between group 3.1103 2 1.5552Within group 198.487 57 3.4822
Visual Analogue Scale
Pre Interventional 1.6872 0.1941
Post Interventional 0.4466 0.642
Table 7: Comparison of ankle dorsi-flexion ROM in allthe three groups.
Active ROM Source of variance SS DF MS F ‘p’Between group 0.5333 2 0.2667Within group 118.8 57 2.0842
Between group 84.233 2 42.116Within group 90.75 57 1.5921
DORSIFLEXION (ROM)
Pre Interventional 0.1279 0.8802
Post Interventional 26.453 7.468
Renu B.Pattanshetty, Amit S.Raikar. IMMEDIATE EFFECT OF THREE SOFT TISSUE MANIPULATION TECHNIQUES ON PAIN RESPONSE ANDFLEXIBILITY IN CHRONIC PLANTAR FASCIITIS: A RANDOMIZED CLINICAL TRIAL.
Int J Physiother Res 2015;3(1):875-84. ISSN 2321-1822 881
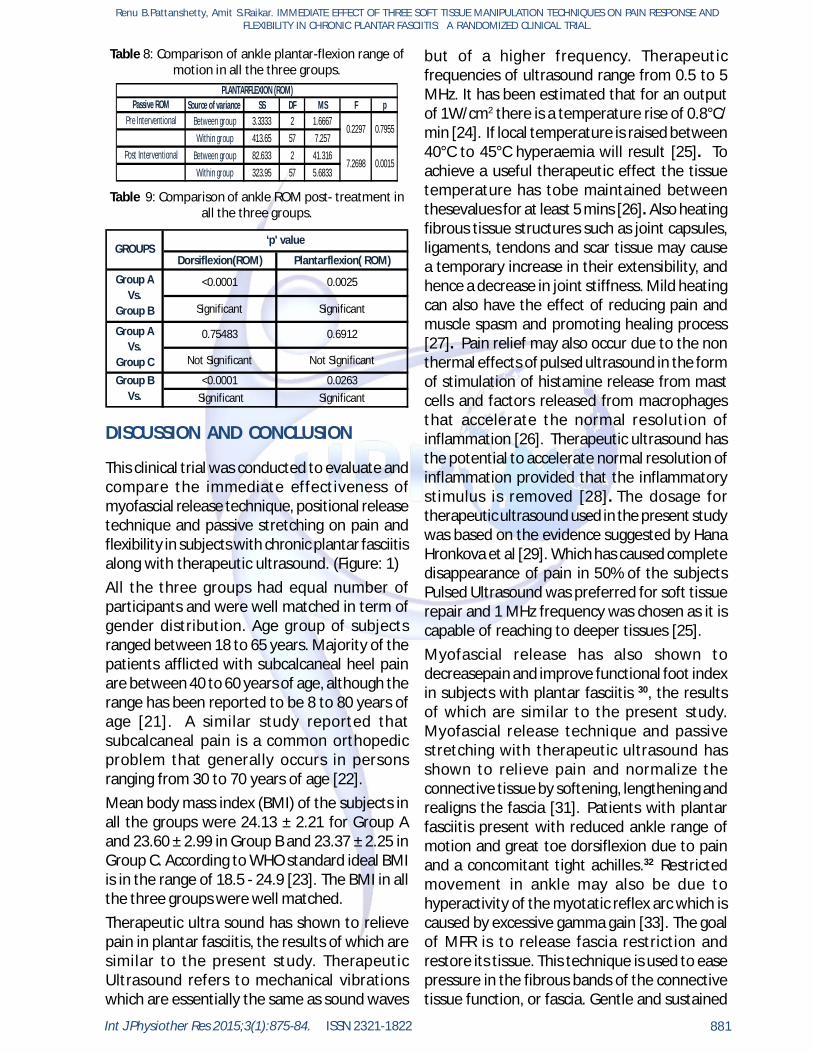
Table 8: Comparison of ankle plantar-flexion range ofmotion in all the three groups.
Source of variance SS DF MS F pBetween group 3.3333 2 1.6667Within group 413.65 57 7.257
Between group 82.633 2 41.316Within group 323.95 57 5.6833
0.7955
PLANTARFLEXION (ROM)Passive ROM
Pre Interventional0.2297
Post Interventional7.2698 0.0015
Table 9: Comparison of ankle ROM post- treatment inall the three groups.
Dorsiflexion(ROM) Plantarflexion( ROM)
Significant Significant
Not Significant Not Significant
Significant Significant
‘p' valueGROUPS
0.75483 0.6912
<0.0001 0.0263
Group A Vs.
Group B
Group A Vs.
Group CGroup B
Vs. Group C
<0.0001 0.0025
DISCUSSION AND CONCLUSION
This clinical trial was conducted to evaluate andcompare the immediate effectiveness ofmyofascial release technique, positional releasetechnique and passive stretching on pain andflexibility in subjects with chronic plantar fasciitisalong with therapeutic ultrasound. (Figure: 1)All the three groups had equal number ofparticipants and were well matched in term ofgender distribution. Age group of subjectsranged between 18 to 65 years. Majority of thepatients afflicted with subcalcaneal heel painare between 40 to 60 years of age, although therange has been reported to be 8 to 80 years ofage [21]. A similar study reported thatsubcalcaneal pain is a common orthopedicproblem that generally occurs in personsranging from 30 to 70 years of age [22].Mean body mass index (BMI) of the subjects inall the groups were 24.13 ± 2.21 for Group Aand 23.60 ± 2.99 in Group B and 23.37 ± 2.25 inGroup C. According to WHO standard ideal BMIis in the range of 18.5 - 24.9 [23]. The BMI in allthe three groups were well matched.Therapeutic ultra sound has shown to relievepain in plantar fasciitis, the results of which aresimilar to the present study. TherapeuticUltrasound refers to mechanical vibrationswhich are essentially the same as sound waves
but of a higher frequency. Therapeuticfrequencies of ultrasound range from 0.5 to 5MHz. It has been estimated that for an outputof 1W/cm2 there is a temperature rise of 0.8°C/min [24]. If local temperature is raised between40°C to 45°C hyperaemia will result [25]. Toachieve a useful therapeutic effect the tissuetemperature has tobe maintained betweenthesevalues for at least 5 mins [26]. Also heatingfibrous tissue structures such as joint capsules,ligaments, tendons and scar tissue may causea temporary increase in their extensibility, andhence a decrease in joint stiffness. Mild heatingcan also have the effect of reducing pain andmuscle spasm and promoting healing process[27]. Pain relief may also occur due to the nonthermal effects of pulsed ultrasound in the formof stimulation of histamine release from mastcells and factors released from macrophagesthat accelerate the normal resolution ofinflammation [26]. Therapeutic ultrasound hasthe potential to accelerate normal resolution ofinflammation provided that the inflammatorystimulus is removed [28]. The dosage fortherapeutic ultrasound used in the present studywas based on the evidence suggested by HanaHronkova et al [29]. Which has caused completedisappearance of pain in 50% of the subjectsPulsed Ultrasound was preferred for soft tissuerepair and 1 MHz frequency was chosen as it iscapable of reaching to deeper tissues [25].Myofascial release has also shown todecreasepain and improve functional foot indexin subjects with plantar fasciitis 30, the resultsof which are similar to the present study.Myofascial release technique and passivestretching with therapeutic ultrasound hasshown to relieve pain and normalize theconnective tissue by softening, lengthening andrealigns the fascia [31]. Patients with plantarfasciitis present with reduced ankle range ofmotion and great toe dorsiflexion due to painand a concomitant tight achilles.32 Restrictedmovement in ankle may also be due tohyperactivity of the myotatic reflex arc which iscaused by excessive gamma gain [33]. The goalof MFR is to release fascia restriction andrestore its tissue. This technique is used to easepressure in the fibrous bands of the connectivetissue function, or fascia. Gentle and sustained
Renu B.Pattanshetty, Amit S.Raikar. IMMEDIATE EFFECT OF THREE SOFT TISSUE MANIPULATION TECHNIQUES ON PAIN RESPONSE ANDFLEXIBILITY IN CHRONIC PLANTAR FASCIITIS: A RANDOMIZED CLINICAL TRIAL.

Int J Physiother Res 2015;3(1):875-84. ISSN 2321-1822 882
stretching of myofascial release is believed tofree adhesions and softens and lengthens thefascia. By freeing up fascia that may beimpending blood vessels or nerves, myofascialrelease helps in improving circulation andnervous system transmission. This technique hasbeen widely used in physical therapy treatmentsin the chronic conditions causing tightness andrestriction in soft tissues. It helps in change ofthe viscosity of the ground substance to a morefluid state which eliminates the fascia’sexcessive pressure on the pain sensitivestructure and restores proper alignment. Thereis sufficient evidence to support theeffectiveness of deep tissue procedures intreating strain/sprain injuries [34,35]. It has alsoshown to stimulate fibroblast proliferation,leading to collagen synthesis that may promotehealing of plantar fasciitis by replacingdegenerated tissue with a stronger and morefunctional tissue [36.37]. The reasons mentionedabove may explain the reason for relieving pain,improvement range of motion in myofascialrelease therapy group similar to the study [30].Direct MFR is a highly effective technique forsubjects with plantar fasciitis who need torecover quickly. All the treatment methods wereequally beneficial in relieving pain and improvingROM.Positional release therapy is a techniqueproposed to increase muscle flexibility byplacing the muscle in a shortened position topromote muscle relaxation in contrast to placingthe muscle in a lengthened or stretched position[20]. Also called as counter-strain therapy, it isan indirect myofascial technique focusing on theneurologic component of the neuro-vascularmyofascial somatic dysfunction. The use of bodypositioning, tender points to identify the lesionand to monitor the therapeutic intervention aresome of the Positional release therapy indirectapproaches with respect to tissue resistance[31]. The neurophysiologic rationale underlyingthe therapy is based on the fact that alterationin afferent neurons affect somatic jointdysfunction. Restricted movement may be dueto hyperactivity of the myotatic reflex arc, whichis caused by excessive gamma gain. Bypositioning the patient’s muscle in the positionof ease for a short period of time, the gamma
gain decreases, thereby allowing the hyperactivereflex arc to return to its original state and rangeof motion to increase. This technique has beenproposed for resolving dysfunction in chronic,subacute and acute condition [38]. The treatmentduration (90 sec) for Positional release therapyselected for this study produced immediatesignificant pain relief which further suggeststhat this time duration may be used in similarclinical set-ups in alleviating pain in chronicplantar fasciitis [33]. Pain relief may also occurdue to decrease in the intrafusal and extrafusalfiber disparity and reset of the inappropriateproprioceptive activity. Korr has provided aconceptual model how different manipulativetechniques like isometrics and stretching maybe effective in treatment of somatic dysfunction[39]. Wynne MM et al demonstrated reductionin pain and improvement in functional abilityusing positional release therapy results of whichare similar to the present study [23]. Use ofpositional release therapy normalizes myotaticreflex arc thus producing movement gains, whichmay explain the reason for improvement in ankleROM in the present study. But when comparedto MFR and Passive Stretching ROM gains wereto a lesser extent. Stretching is a term used todescribe any therapeutic maneuver designed toincrease mobility of soft tissue and subsequentlyimprove ROM by elongating structures that haveadaptively shortened and have becomehypomobile over time. When a muscle isstretched and elongated, the stretch force istransmitted to the muscle fibers via theconnective tissue (endomysium and perimysium)in and around the fibers. It is hypothesized thatmolecular interactions link these noncontractileelements to the contractile unit of muscle, thesarcomere. During passive stretch bothlongitudinal and lateral force transductionoccurs [40]. Since stretching is an integral partof treatment component of physical fitness andrehabilitation programmes, it is thought topositively influence performance and injuryprevention especially in the athletes. Shorteningand contracture of the plantar flexors may causelimitations in ROM that restrict the normal actionof muscle. This condition may be managed witha stretching program, which may decrease therisk of injury. Regardless of the type of program,the goal of stretching is to change the physical
Renu B.Pattanshetty, Amit S.Raikar. IMMEDIATE EFFECT OF THREE SOFT TISSUE MANIPULATION TECHNIQUES ON PAIN RESPONSE ANDFLEXIBILITY IN CHRONIC PLANTAR FASCIITIS: A RANDOMIZED CLINICAL TRIAL.

Int J Physiother Res 2015;3(1):875-84. ISSN 2321-1822 883
characteristics of connective tissue. Passivestretching along with therapeutic ultrasounddemonstrated marked reduction in pain andimprovement in range of motion in the presentstudy and it correlates well with the results ofstudy by CA Knight et al. The author suggestedstretching of the Achilles tendon and plantarfascia, performed 3-5 times daily, showedsignificant decrease in pain in plantar fascia [18].However, the present study aimed to evaluatethe immediate effectiveness of stretchingrather than a long term study. To conclude, thepresent study is the first to report the immediateeffectiveness of myofascial release technique,positional release therapy and passive stretchingon pain response and flexibility in chronicplantar fasciitis in all three groups. Futureresearch should consider using a larger samplesize in different populations like athletes andelderly population along with different electricalmodalities, more number of treatment sessionsand a follow-up.
CLINICAL MESSAGE:
Use of manual techniques like myofascialrelease therapy, positional release therapy orpassive stretching may be used along withtherapeutic ultrasound in the treatment ofchronic of plantar fasciitis instead of usingtherapeutic ultrasound in achieving immediaterelief of pain and improving ankle range ofmotion.
ACKNOWLEDGEMENTS:
We would like to mention a special thanks toM.D. Mallapur, Lecturer, Dept. of communitymedicine, JN Medical College, Belgaum,Karnataka for helping us with the analysis of thedata and also like to thank all the individualswho participated in the study.
REFERENCES
Conflicts of interest: None
[4]. Gorter K, De.Poels, De.Melker R, Kuyvenhoven M:Variation in diagnosis and management of commonfoot problems by GP’s. FamPract 2001; 18(06):569-573.
[5]. Whiting W.C, Zernicke R F, Roxas M; Plantar Fasciitis: Diagnosis and Therapeutic Considerations. Alt.Med Rev.2005; 10:83-93.
[6]. Kent K. Wu: Surgery of the foot. 3rd Ed. Philadelphia:Lea &Febiger; 1986.
[7]. American Podiatric Medical Association USA, citedin www.apma.org./topics/heel.htm / Nov 1st 2009.
[8]. Reid C. David: Sports Injury Assessment andRehabilitation. 1st Ed. New York: Churchill Livington;1992.
[9]. Singh D. , Angel J,. Trevino Bently Saul G. ForthrightlyReview: Plantar Fasciitis, BMJ,1997; 212-216.
[10]. Roberts Scott :Text Book on Plantar fasciitis, heelspurs and heel pain 8-25-2004, www.heel spurs.com/intro.html(Google) page 2 and 5/21st
Aug2009.[11]. Brotzman S.B, , Kevin M.D, Wilk E,: Text Book of
Clinical Orthopaedic Rehabilitation; 2nd Ed. NewYork: Churchill Living stone; 2001.
[12]. Rutherford Y.C , Niedfelat M.W: treatment of ChronicPlantar fasciitis. Am Fam pain. J. Foot Ankle Surg2001; 40:329-400.
[13]. American College of Foot and Ankle Surgeons: Thediagnosis and treatment of heel pain. J Foot AnkleSurg 2001; 40:329-40.
[14]. Hurtling D, Kessler RM: Management of CommonMusculoskeletal disorder. The lower leg, Ankle andFoot. 3rdEd. Philadelphia: Lippincott; 1995.
[15].Ravindra P, Prakash C: Degenerative Plantarfasciitis: A review of Current concepts. The Foot,vol17, issue 1, March 2007:3- 9.
[16]. Wapher K, Sharkey P: The use of right splints fortreatment of recalcitrant plantar fasciitis .FootAnkle; 1991; 12(3):135 - 137.
[17]. Draper DO, Castel JC, Castle D: Rate of temperatureincrease in human muscle during 1 MHz and 3 MHzcontinuous ultrasound. J Orthop Sports Phys.Ther.1995; 22:142-150.
[18]. CA Knight et al: Effect of Superficial heat, Deep heat,and Active Exercise, Warm up on the Extensibilityof the Plantar Flexors, PhysTher: Vol.81, No.6, June2001:1206 - 1214.
[19]. Carol M. 2001: The Myofascial release manual. 3rd
ed. Slack Inc 67.Walkier JM. Deep transversefrictions in ligament healing. J. Orthop SportsPhysther 1984; 6(2):89-94.
[20]. D’Ambrogio K J, Roth G B.: Text Book of PositionalRelease Therapy, Assessment and treatment ofmusculoskeletal Dysfuntion. Ed 2nd. Philadelphia:Mosby; 2002.
[21]. Gill LH: Conservative treatment for painful heelsyndrome. Proceedings of the third annual summermeeting. Foot ankle. 1987:8:122.
[22]. Lapidus P.W., Guidotti F.P., Painful heel: Report on232 patients with 364 painful heels. ClinOrtho.1965; 39:178.
[1]. Caillet R: Textbook of Foot and Ankle Pain. 2nd Ed.Philadelphia: FA Davis Company;1968.
[2]. S J. Bartold, Plantar heel pain syndrome: Overviewand management: Journal of Bodywork andmovement Therapies, 2004; 8: 214-226.
[3]. Footpain : A general description of the causes, http://www.docpods.com/foot pain.htm/Aug 16th 2005.
Renu B.Pattanshetty, Amit S.Raikar. IMMEDIATE EFFECT OF THREE SOFT TISSUE MANIPULATION TECHNIQUES ON PAIN RESPONSE ANDFLEXIBILITY IN CHRONIC PLANTAR FASCIITIS: A RANDOMIZED CLINICAL TRIAL.

Int J Physiother Res 2015;3(1):875-84. ISSN 2321-1822 884
[23]. Wynne M M. et al. Effect of Counterstrain on StretchReflexes, Hoffmann Reflexes, and Clinical Outcomesin subjects with plantar fasciitis. JAOA, January17, 2006; 106(9): 547-556.
[24]. Evans P. (1980): The healing process at cellularlevel: a review. Physiotherapy, 66, pg: 256-9.
[25]. Hronkova H, Navrtil L, , Skopek J and Kymplova J,Possibilities of the Analgesic therapy of Ultra soundand Non-Invasive therapy 19.02.2000,www.laserpartner.org. pg: 2.
[26]. Lehman J. F., De Lateur B. J: In Therapeutic Heat andCold, 3rd Ed, Baltimore: Williams & Wilkins;1982.
[27]. Young, S. ‘Ultrasound therapy’ in: Kitchen, S andBazin, S (eds) Claytons’sElectrotherapy, WBSaunders, Philadephia, 10th Ed, 1996,243-267.
[28].Young SR and Dyson: M. ‘Macrophagesresponsiveness to Therapeutic Ultrasound’.Ultrasound in medicine and Biology, 1990, (16) 261-269.
[29]. Evans P. The healing process at cellular level: areview. Physiotherapy, 1980: 66,: 256-259.
[30]. Leadhetter W. Cell matrix response in tendon injury.Clin Sports Med 1997; 11(3) ; 533-579.
[31]. Meseguer AA, et al. Immediate effects of the Strain/counterstrain technique in local pain evoked bytender points in the upper trapezius muscle. 2006;9(3):112-118.
[32]. Racette SB et al. Obesity: Overview of Prevalence,Etiology and Treatment. Physical therapy 2003; 83:276-288.
[33]. De Deyne, PG: Application of passive stretch andits implication for muscle fibres .Phys Ther. 2001:81(2): 819-827.
[34]. Richie D , AAPSM (2003-2004), your podiatricsports Physician Talks about Plantar FasciitisTreatment Pearls., www.aapsm.org (Pub Med)/ 4th
Aug 2006.[35]. Walkier JM. Deep transverse frictions in ligament
healing. J. Orthop Sports Phys Ther 1984; 6(2): 89-94.
[36]. Kvist M, Jarvinen M. Clinical histochemical andbiomechanical features in repair of muscle andtendon injuries. Int J Sports Med 1982; (3Suppl1):12-14.
[37]. Dyck DD Jr, Boyajian-O’Neil LA. Plantarfasciitis. ClinJ Sports Med 2004; 14(5) : 305-309.
[38]. Travor B, Julie Kramer et al: Effect of a Positionalrelease therapy technique on Hamstring flexibility.PhysTher Can; 2004; 56:165-170.
[39]. Jones LH: Spontaneous release by positioning. TheDO. 1964; 4: 109-116.
[40]. Wayne Pugh, The efficacy of foot or those in thetreatment of plantar fasciitis: - A systemic review,Physical Therapy 2000; 43: 276-188.
How to cite this article:Renu B.Pattanshetty, Amit S.Raikar. IMMEDIATE EFFECT OF THREE SOFTTISSUE MANIPULATION TECHNIQUES ON PAIN RESPONSE AND FLEXIBILITYIN CHRONIC PLANTAR FASCIITIS: A RANDOMIZED CLINICAL TRIAL. Int JPhysiother Res 2015;3(1):875-884. DOI: 10.16965/ijpr.2015.101
Renu B.Pattanshetty, Amit S.Raikar. IMMEDIATE EFFECT OF THREE SOFT TISSUE MANIPULATION TECHNIQUES ON PAIN RESPONSE ANDFLEXIBILITY IN CHRONIC PLANTAR FASCIITIS: A RANDOMIZED CLINICAL TRIAL.