international journal of physiotherapy and research, int j … · · 2014-12-11int j physiother...
TRANSCRIPT

Int J Physiother Res 2014;2(6):757-61. ISSN 2321-1822 757
Case Report
REHABILITATION OF A QUADRIPERETIC PATIENT: A SINGLE CASESTUDYKaur Harmandeep *1, Bhardwaj Meenu 2, Dadia Sadbhawna 3.
*1 College of Physiotherapy, Adesh University, Bathinda, Punjab, India.2 College of Physiotherapy, Adesh University, Bathinda, Punjab, India.3 Assistant professor College Of Physiotherapy, Adesh University Bathinda, Punjab, India.
Background: Physical activity and exercise following a spinal cord injury is a central part of the rehabilitationprogramme for everyone with a spinal cord injury. However, the level and extent of the injury as well as howmuch time has passed since the injury is of even greater importance. Patients should be mobilised as soon asmedically possible after a spinal cord injury.In the present study, during the active rehabilitation phase, emphasises of treatment was on maximisingfunctional independence (transfers, self-care including- bathing, toileting, dressing); and later on emphasiswas on general fitness, co-ordination and balance.Outcomes: Level of functional independence was improved i.e. the patient was able to transfer from bed tochair; he was able to stand and walk with the help of walker. He was able to do his self-care, i.e. bathing,toileting, dressing, eating, which was not possible earlier.KEYWORDS: Cervical spinal cord injury, Quadriparesis, Rehabilitation.
Quick Response code
Access this Article online
International Journal of Physiotherapy and ResearchISSN 2321- 1822
www.ijmhr.org/ijpr.html
ABSTRACT
INTRODUCTION
Address for correspondence: Kaur Harmandeep , BPT Intern, College of Physiotherapy, AdeshUniversity, Bathinda, Punjab. VPO Behmana, Distt Patiala Punjab(147101), India.E-Mail: [email protected]
International Journal of Physiotherapy and Research,Int J Physiother Res 2014, Vol 2(6):757-61. ISSN 2321-1822
DOI: 10.16965/ijpr.2014.649
The spinal cord is the long cylindrical lowest partof central nervous system. It occupies uppertwo-thirds of vertebral canal. It gives rise to 31pairs of spinal nerves. Spinal cord extends fromupper border of atlas vertebra to the lower bor-der of first lumbar or second lumbar in an adult.Superiorly it continues with the medullaoblongata, inferiorly it terminates as conusmedullaris. It is surrounded by three meninges.Outer most Dura mater, middle arachnoidsmater and innermost is the pia mater. Spinal cordpresents cervical enlargement for supply ofupper limb muscles. This extends from C4 to T2spinal segments with maximum diameter at the
level of C6 segment. Another enlargement is thelumbar enlargement for supply of muscles oflower limb. 1
Spinal injuries can be classified on the basis ofmechanism of injury. These are flexion,compression, hyper extension and flexiondistraction. Spinal cord injuries typically dividedinto two broad functional categories:quadriplegia and paraplegia. Quadriplegia refersto complete paralysis of all four extremities andtrunk, including respiratory muscles, and resultsfrom lesions of the cervical cord 2. Spinal cordinjury is a low incidence, high cost disabilityrequiring tremendous change in an individual’slifestyle. This type of injury mostly occurs from
Accepted : 25-07-2014Published (O): 23-11-2014Published (P): 11-12-2014
Received: 27-05-2014Peer Review: 27-05-2014Revised: 16-06-2014DOI: 10.16965/ijpr.2014.649

Int J Physiother Res 2014;2(6):757-61. ISSN 2321-1822 758
Kaur Harmandeep, Bhardwaj Meenu, Dadia Sadbhawna. REHABILITATION OF A QUADRIPERETIC PATIENT: A SINGLE CASE STUDY.
indirect forces produced by movement of thehead and trunk and less often from direct injuryto a vertebra. A fall from height is thecommonest mode of sustaining a spinal injuryin developing countries. Other modes may beroad traffic accidents, sport injuries.3
The treatment of spinal cord injuries can be donein the three phases. Emergency care, definitivecare and rehabilitation. Emergency care will bedone at the site of the accident and in theemergency department. Definitive care dependsupon the stability of spine. And rehabilitationprotocol will make the individual independent. 4
REHABILITATIONManagement of the patient with SCI is a complexand challenging task in which continuity of careis critical to achieving the overall goals ofrehabilitation. Frequent and open communi-cation among team members, patient, familyand care givers is vital to maintaining anorganised and highly individualized approach toboth rehabilitation and reintegration of thepatient into the community. 2
Rehabilitation has been defined by the WorldHealth Organisation as a progressive, dynamic,goal-oriented and often time –limited process,which enables an individual with impairment toidentify and reach his/her optimal mental,physical, cognitive and social function level.Rehabilitation after spinal cord injuries seeksthe fullest possible physical and psychologicalreadjustment of the injured person to hispermanent disability with a view to restoring hiswill to live and working capacity.GOALS OF THE REHABILITATION 4
1. Rehabilitation continues with planning fordischarge back to community and finallyreintegration into the former or new roles andactivities within the community.2. Family and peers have an important rolethroughout the rehabilitation process and mustbe initiated and integrated into this processplanning.The initial treatment is passive stretching, e.g.stretching muscles, mobilising joints and tonormalise the muscle tone. This is followed byan active training programme that incorporatesindividual training for the purpose of improving
aerobic fitness, muscle strength, co-ordinationand balance. Both the spinal cord injury patientand the Physiotherapists managing his or herrehabilitation must know how to avoid andprevent complications during training.Physiotherapists must also be fully aware of thepossibilities available to spinal cord injurypatients so as to be able to help the patient toimprove his or her health and physical fitness.Consequently, it is vital to acquire newknowledge on how these individuals can besttrain, not just for the purpose of improvingaerobic fitness and muscle strength, but also tolearn how to do “old activities with newmuscles.”During the active rehabilitation phase, theemphasis of treatment is on maximizingfunctional independence. Initially this includesbasic skills such as bed mobility, transfers andwheelchair mobility skills. As the patientprogresses, these interventions are expandedto include skills necessary for work, home, andcommunity re-entry. Rehabilitation programmeemphasises on neuromuscular facilitation/spasticity, independence level, and to A.D.L’s. 5
A 44 year old male patient presented tophysiotherapy department of college ofPhysiotherapy, Adesh University, Bathinda withcomplaint of inability of standing and walkingsince 3 years. There was a history of fall thatled to spinal cord injury 3 years ago. MRI findingwere consistent with Spinal Cord Compressioninjury at C5-C6, C6-C7 level. The patientunderwent surgery after 3 days of injury. Aftersurgery, he had not taken any Physiotherapytreatment and was totally dependent on hisfamily members for his all A.D.L’s.
Mode of ambulation: wheelchairBody built : MesomorphicAttitude of limb :Upper limb: Left Hand and wrist: flexion at PIPand DIP joint of index and middle fingerLower limb: Hip joint – externally rotated (B/L)Knee joint – flexed (Right - 10p left - 4p )Feet – inverted and plantar flexed (B/L)
ON OBSERVATION
CASE DESCRIPTION

Int J Physiother Res 2014;2(6):757-61. ISSN 2321-1822 759
Kaur Harmandeep, Bhardwaj Meenu, Dadia Sadbhawna. REHABILITATION OF A QUADRIPERETIC PATIENT: A SINGLE CASE STUDY.
Upper limb (left): Grade 1 (According toAshworth’s scale)Lower limb (Right & left): Grade 2 (According toAshworth’s scale)
MUSCLE TONE
REFLEXES
RIGHT LEFT
Knee Exaggerated Exaggerated
Ankle Exaggerated Exaggerated
SENSORY EXAMINATION: Intact
MOTOR EXAMINATION: ROM was measuredwith goniometer in supine lying. The active painfree ranges available were as follows:
ROM RIGHT LEFTHip flexion 0⁰-40⁰ 0⁰
Knee flexion 10⁰-100⁰ 4⁰-100⁰
Shoulder flexion 0⁰-180⁰ 0⁰-120⁰Shoulder abduction 0⁰-170⁰ 0⁰-110⁰
Elbow flexion 0⁰-110⁰ 0⁰-110⁰
MUSCLE STRENGTH: Muscle testing wasperformed and scoring was based on ManualMuscle Testing. 6
RIGHT LEFTUpper Limb Grade 4 Grade 3Lower LimbHip flexors Grade 2 Grade 2Abductors Grade 2 Grade 2
Knee flexors Grade 3 Grade 3Dorsiflexors Grade 3 Grade 3
FINDINGS: Physiotherapy evaluation revealeddecrease functional mobility such as ambula-tory status such as transfers, bathing, eating,dressing standing, walking, gripping with lefthand, weight transfers in sitting, decreasemuscle strength, decrease ROM.
ROM RIGHT LEFTKnee flexion (in supine)
8⁰-100⁰ 2⁰-112⁰
Hip flexion 0⁰-40⁰ 0⁰-10⁰
PLAN OF CARE DESIGN: The rehabilitationprogram focuses on Functional independence,ROM, flexibility, strength, endurance, proprio-ception, gait training and fitness of patient.
PHYSIOTHERAPY PROTOCOLGOALSTo achieve the functional level of independence.To make patient ambulatory with or withoutassistance.To normalise the muscle toneTo improve muscle strength.To increase range of motion.DAY 1 TO DAY 5Cryotherapy for 5 minutes to decrease themuscle tone.Active assisted ROM exercises of both upperlimb and lower limb (10 repetitions)Stretching of hamstrings, quadriceps, calfmuscles, adductors, (3 repetitions with 30second hold)Stretching of muscles of hand (intrinsic muscles).Sustained stretch in prone lying with weight of2 kg on each ankle [Fig. 1].Transfer techniques (lying to side lying, side lyingto sitting, sitting to wheel chair, wheel chair tobed.)Foot correction with pillow placement in supinelying.
Fig. 1: Sustained stretch in prone lying.
DAY 6 TO DAY 10Cryotherapy, active ROM exercises, stretchingis continued.Strengthening exercises of quadriceps, calfmuscles, hip flexors, and abdominals.Bridging.Gripping exercises of hand.

Int J Physiother Res 2014;2(6):757-61. ISSN 2321-1822 760
Kaur Harmandeep, Bhardwaj Meenu, Dadia Sadbhawna. REHABILITATION OF A QUADRIPERETIC PATIENT: A SINGLE CASE STUDY.
Self-made splint for extension of PIP and DIPjoints [Fig. 2 (a), Fig. 2 (b)].
Fig. 2(b) Dorsal view
Mat exercises (side rolling, side rolling to pronelying, prone on elbow, prone on hand)Weight transferring in sitting.Self-made splint for right leg was given toprevent further deformity.
REASSESSMENTSUBJECTIVEHe was able to extend his fingers of left sidewhich was not possible earlier.Able to extend his left knee fully.
OBJECTIVE
ROM RIGHT LEFTKnee flexion (in supine)
8⁰-100⁰ 2⁰-112⁰
Hip flexion 0⁰-40⁰ 0⁰-10⁰
Fig. 2(a) Ventral view
DAY 11- DAY 15Standing with supportMat exercises (prone on elbow, prone on hand,quadripud, kneel sitting).Weight transferring during mat exercises.Swiss Ball exercises, with patient sitting on chair[pushing away the ball with both feet, to improvethe strength.Balancing exercises with Swiss ball were started
for balancing [jogging, weight shifting].Tilt table (for 10 minutes) (Fig. 3).Sustained stretch was given after the treatment.
Fig .3: Prone on tilt table.
DAY 16- DAY 20Active ROM exercises of both upper and lowerlimb.Stretching continuedStrengthening continued with weight bands ofhalf kg.Bridging on one leg.Sit to stand (on chair).Swiss ball exercises were continued [progressionin jogging and weight shifting by placing handsacross chest, trunk rotation, knee extension,forward and backward bending].Reach out activities were started on Swiss ball.Standing with support of walker.Weight transfer through one leg standing.Mat exercises were continued.Weight shifting in quadriped position and oneleg raising in this position to strengthen themultifedus muscle and for balancing.Balance exercises in kneel sitting.Co-ordination exercises of both upper and lowerlimb.Tilt table in prone lying.Walking started with support of walker (Fig. 4)Foot exercises [plantar and dorsiflexion].Dynamic quads with PRE programme.
Int J Physiother Res 2014;2(6):757-61. ISSN 2321-1822 761
RIGHT LEFT1 RM 1 kg 1kg
10 RM 0.5 kg 0.5kg
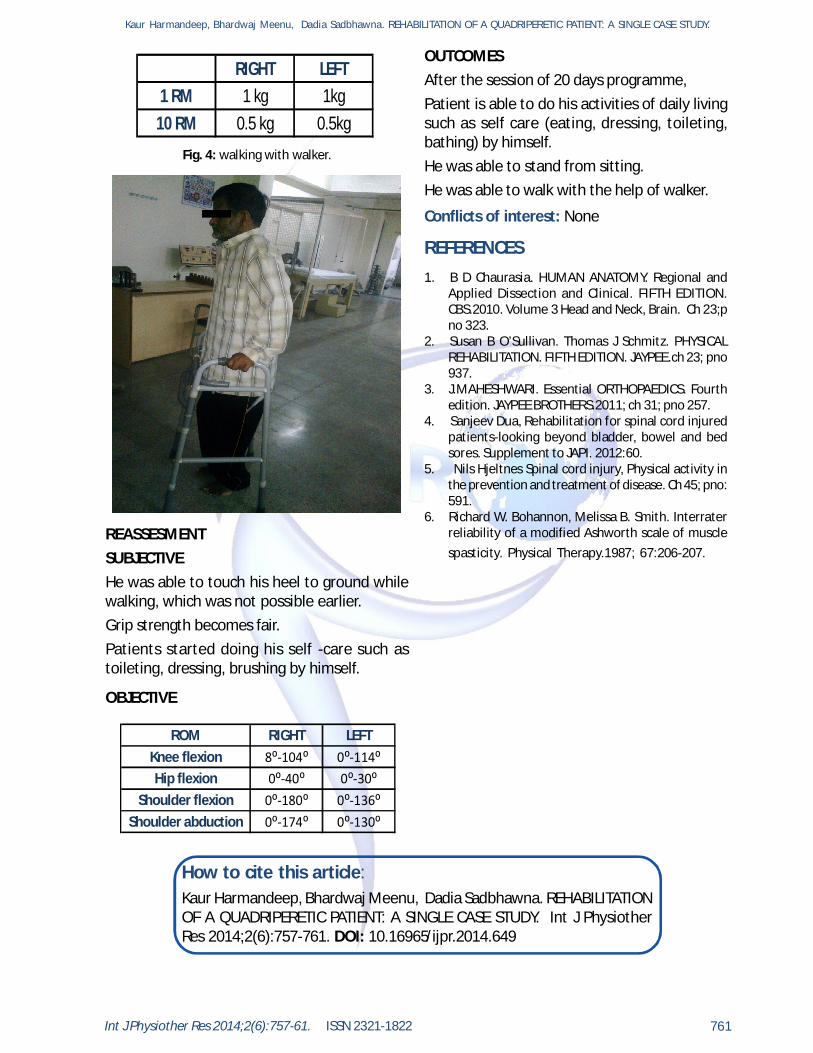
Fig. 4: walking with walker.
REASSESMENTSUBJECTIVEHe was able to touch his heel to ground whilewalking, which was not possible earlier.Grip strength becomes fair.Patients started doing his self -care such astoileting, dressing, brushing by himself.
OBJECTIVE
ROM RIGHT LEFTKnee flexion 8⁰-104⁰ 0⁰-114⁰Hip flexion 0⁰-40⁰ 0⁰-30⁰
Shoulder flexion 0⁰-180⁰ 0⁰-136⁰Shoulder abduction 0⁰-174⁰ 0⁰-130⁰
REFERENCES
Conflicts of interest: None
1. B D Chaurasia. HUMAN ANATOMY. Regional andApplied Dissection and Clinical. FIFTH EDITION.CBS.2010. Volume 3 Head and Neck, Brain. Ch 23;pno 323.
2. Susan B O’Sullivan. Thomas J Schmitz. PHYSICALREHABILITATION. FIFTH EDITION. JAYPEE.ch 23; pno937.
3. J.MAHESHWARI. Essential ORTHOPAEDICS. Fourthedition. JAYPEE BROTHERS.2011; ch 31; pno 257.
4. Sanjeev Dua, Rehabilitation for spinal cord injuredpatients-looking beyond bladder, bowel and bedsores. Supplement to JAPI. 2012:60.
5. Nils Hjeltnes Spinal cord injury, Physical activity inthe prevention and treatment of disease. Ch 45; pno:591.
6. Richard W. Bohannon, Melissa B. Smith. Interraterreliability of a modified Ashworth scale of musclespasticity. Physical Therapy.1987; 67:206-207.
OUTCOMESAfter the session of 20 days programme,Patient is able to do his activities of daily livingsuch as self care (eating, dressing, toileting,bathing) by himself.He was able to stand from sitting.He was able to walk with the help of walker.
How to cite this article:Kaur Harmandeep, Bhardwaj Meenu, Dadia Sadbhawna. REHABILITATIONOF A QUADRIPERETIC PATIENT: A SINGLE CASE STUDY. Int J PhysiotherRes 2014;2(6):757-761. DOI: 10.16965/ijpr.2014.649
Kaur Harmandeep, Bhardwaj Meenu, Dadia Sadbhawna. REHABILITATION OF A QUADRIPERETIC PATIENT: A SINGLE CASE STUDY.