international atomic energy agency (iaea) human resources...
TRANSCRIPT

International Atomic Energy Agency (IAEA)Human Resources Development in Radiation Oncology in the Context of Cancer Control
Programmes in Latin America
International Atomic Energy Agency (IAEA)Human Resources Development in Radiation Oncology in the Context of Cancer Control
Programmes in Latin America
Buenos Aires, 23 a 27 de abril de 2007
Luiz Antonio Santini
National Cancer Institute (INCA)
Brasil
Buenos Aires, 23 a 27 de abril de 2007
Luiz Antonio Santini
National Cancer Institute (INCA)
Brasil


Hospital Complex Hospital Complex
HC IIHC II HC IIIHC III
HC IVHC IVHC I e CEMOHC I e CEMO

AttributionsAttributions
a) Assist the Health Minister in the design of the Na tional Policies for Oncologic care;
b) Conduct national actions of prevention, diagnosi s and treatment of malign neoplasia and its correlated disord ers;
c) Provide medical assistence;
d) Conduct clinical, epidemiological and experimenta l research;
e) Provide formal education, training and developmen t of human resources.
a) Assist the Health Minister in the design of the Na tional Policies for Oncologic care;
b) Conduct national actions of prevention, diagnosi s and treatment of malign neoplasia and its correlated disord ers;
c) Provide medical assistence;
d) Conduct clinical, epidemiological and experimenta l research;
e) Provide formal education, training and developmen t of human resources.

ScreeningScreening

Model of the Natural History of the DiseaseModel of the Natural History of the Disease
STAGES OF ONCOLOGIC CAREOPPORTUNITY EFECTIVENESS
TIME
DiagnósticoTratamentoReabilitação
Sintomase sinais no início
da fase clínica
Sintomas e sinais comdiagnóstico
tardio
Palliative care
Signs and
symptoms
Earlydetection
Research
Genetic predisposition
Information /Communication
Exposure to risk factors
Biological onset
of the disease
ScreeningDiagnosisTreatment
Rehabilitation
Signs and symptoms
on the clinicalphase outset
Signs and symptoms
with latediagnosis

Source: National Cancer Control Programmes. Policie s and managerial guidelines.WHO, 2002. p.59Source: National Cancer Control Programmes. Policie s and managerial guidelines.WHO, 2002. p.59

Location Population screeningBreast YesCervix YesProstate NoIntestines NoSkin NoOral cavity No
Actions for Early DetectionActions for Early Detection
Source: National Cancer Control Programmes. Policies a nd managerial guidelines.WHO, 2002.Source: National Cancer Control Programmes. Policies a nd managerial guidelines.WHO, 2002.

Cancer of the Cervix ScreeningCancer of the Cervix Screening

Incidence in WomenIncidence in Women
Female breast Cervix Colon and rectum
48930
1926013970
Women
Can
cer
Typ
es -
Wom
en

World distribution of incidence coefficientsfor cancer of the cervix in women, 2002
World distribution of incidence coefficientsfor cancer of the cervix in women, 2002
Source: Globocan 2002, IARCSource: Globocan 2002, IARC
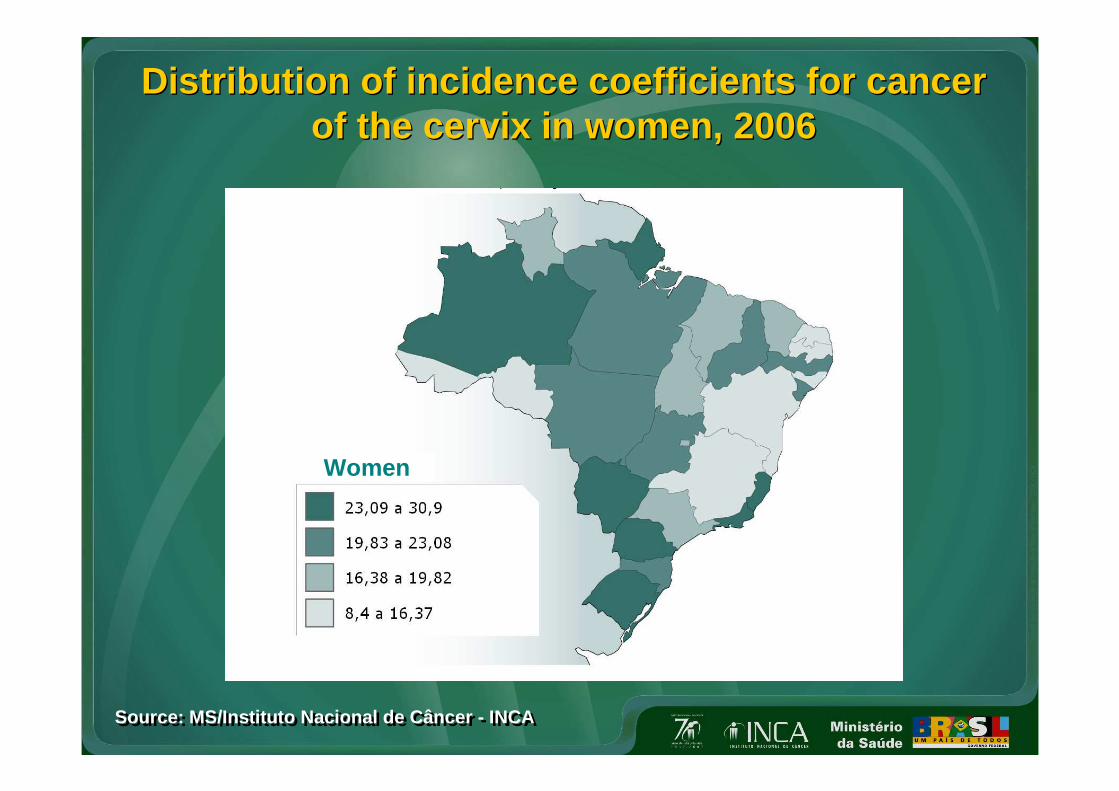
Distribution of incidence coefficients for cancerof the cervix in women, 2006
Distribution of incidence coefficients for cancerof the cervix in women, 2006
Source: MS/Instituto Nacional de Câncer - INCASource: MS/Instituto Nacional de Câncer - INCA
Women

Source: National Cancer Control Programmes. Policies a nd managerial guidelines.WHO, 2002. p.60Source: National Cancer Control Programmes. Policies a nd managerial guidelines.WHO, 2002. p.60
Natural History of Cancer of the Cervix
Natural History of Cancer of the Cervix

Cancer of the Cervix Control in Brazil: History
Cancer of the Cervix Control in Brazil: History
PAISM
Pró-Onco
Viva Mulher1st National Campaign
1984 1987 1997/98 1999-2002
Intensification of Viva Mulher -
2nd National Campaign
PCCU –Strategic
GuidelinesViva Mulher
(pilot)
2006
Pacto pela vida
2005
PHASE IPHASE I PHASE IIPHASE II PHASE IIIPHASE III PHASE IVPHASE IV

Phase I - Before 1997Phase I - Before 1997
Proposition of PoliciesReality• Isolated actions • Lack of continuity• Lack of articulation• Non guaranteed treatment • No evaluation
Proposition of PoliciesReality• Isolated actions • Lack of continuity• Lack of articulation• Non guaranteed treatment • No evaluation

PHASE II-a.Viva Mulher pilot project (1997 - 1998 )5 municipalities + 1 state
PHASE II-a.Viva Mulher pilot project (1997 - 1998 )5 municipalities + 1 state
• Development of a model for early detection • Standardization of procedures
– Technical procedures for specimen collection and sl ide examination
– Quality and treatment monitoring – Incorporation of new technologies
• Definition of the referral flow• Conduct qualitative research;• Partnership with NGOs, universities, and scientific
societies; • Humanization of health care;• Design of a model for political-managerial articulati on;• Development of a computer system to monitor actions
(SISCOLO).
• Development of a model for early detection • Standardization of procedures
– Technical procedures for specimen collection and sl ide examination
– Quality and treatment monitoring – Incorporation of new technologies
• Definition of the referral flow• Conduct qualitative research;• Partnership with NGOs, universities, and scientific
societies; • Humanization of health care;• Design of a model for political-managerial articulati on;• Development of a computer system to monitor actions
(SISCOLO).

PHASE II-b. National Implementation Phase (Aug/ Sep 1998)
PHASE II-b. National Implementation Phase (Aug/ Sep 1998)
• Implementation of the National Programme for Cancer of the Cervix Control (PNCCCU) on 06/21/98;
• Implementation of actions in all states, with adher ence of 98% of municipalities from August to September 1998.
MAIN ACHIEVEMENTS:– Standardization of screening, diagnosis and treatme nt actions – Extension of actions to all states – Test of the network’s capacity– Doubling of the number of cytology tests – Strengthening of partnerships– Availability of treatment through CAF in the public health care
network – Financing guaranteed
• Implementation of the National Programme for Cancer of the Cervix Control (PNCCCU) on 06/21/98;
• Implementation of actions in all states, with adher ence of 98% of municipalities from August to September 1998.
MAIN ACHIEVEMENTS:– Standardization of screening, diagnosis and treatme nt actions – Extension of actions to all states – Test of the network’s capacity– Doubling of the number of cytology tests – Strengthening of partnerships– Availability of treatment through CAF in the public health care
network – Financing guaranteed

PHASE III. Consolidation Phase (1999-2002)
PHASE III. Consolidation Phase (1999-2002)
OBJECTIVE
Increase access to actions on cancer of the cervix earl y detection for Brazilian women, specially those in the high-risk age group, and guarantee appropriate treatment for the disease and its precursor lesions.
Main strategies: – Consolidation of a geopolitical managerial base, – Articulation of a communication network for women, – Reevaluation of the actual technology availability for diagnosis and
treatment, – Training human resources, and – Designing an evaluation plan
OBJECTIVE
Increase access to actions on cancer of the cervix earl y detection for Brazilian women, specially those in the high-risk age group, and guarantee appropriate treatment for the disease and its precursor lesions.
Main strategies: – Consolidation of a geopolitical managerial base, – Articulation of a communication network for women, – Reevaluation of the actual technology availability for diagnosis and
treatment, – Training human resources, and – Designing an evaluation plan

Phase IV. Populacional Strategy: Cytopathologic screening within primary care
(Strategic guidelines and Pacto pela vida )
Phase IV. Populacional Strategy: Cytopathologic screening within primary care
(Strategic guidelines and Pacto pela vida )
Qualification of diagnosis and treatment:� Quality control of cytopathology testing – specific l egislation for internal and
external control; ME module implemented at SISCOLO
� Terminology based on 2001 Bethesda Consensus (compa rability)-implementation of the new Brazilian version – July 2 006
� Standardized clinical conduct (manual of recommenda tions)
� Technology for clinical treatment implemented: “see and treat” method
Network organization:� Decentralized control actions: municipal sphere
� Activities based on the natural history of the dise ase: from primary prevention to palliative care
� Organization based on the oncologic care network str ucturing
� Expansion of oncologic care based on coverage parame ters
Qualification of diagnosis and treatment:� Quality control of cytopathology testing – specific l egislation for internal and
external control; ME module implemented at SISCOLO
� Terminology based on 2001 Bethesda Consensus (compa rability)-implementation of the new Brazilian version – July 2 006
� Standardized clinical conduct (manual of recommenda tions)
� Technology for clinical treatment implemented: “see and treat” method
Network organization:� Decentralized control actions: municipal sphere
� Activities based on the natural history of the dise ase: from primary prevention to palliative care
� Organization based on the oncologic care network str ucturing
� Expansion of oncologic care based on coverage parame ters

Cancer of the Cervix Control in Numbers
Cancer of the Cervix Control in Numbers
• Pilot Project (5 municipalities + 1 state; 1997/98)– 124.440 Women
• Intensification Phase of the Programme (Brazil; August/September 1998)– 3.177.740 women
• Consolidation Phase of the Programme – ROUTINE -(Brazil; since 1999)– Until 1998 - 6 million cytology tests per year– 1999 to 2002 – 8 million cytology tests per year – After 2002 – 11 million cytology per year
• Pilot Project (5 municipalities + 1 state; 1997/98)– 124.440 Women
• Intensification Phase of the Programme (Brazil; August/September 1998)– 3.177.740 women
• Consolidation Phase of the Programme – ROUTINE -(Brazil; since 1999)– Until 1998 - 6 million cytology tests per year– 1999 to 2002 – 8 million cytology tests per year – After 2002 – 11 million cytology per year

Number of cervical cytopathologic Tests Brazil, 1995 to 2006
Number of cervical cytopathologic Tests Brazil, 1995 to 2006
0
2.000.000
4.000.000
6.000.000
8.000.000
10.000.000
12.000.000
14.000.000
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006
1998 and 2002 campaign
Routine

0
2.000.000
4.000.000
6.000.000
8.000.000
10.000.000
12.000.000
14.000.000
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006
Year
Num
ber
of T
ests
North Northeast Southeast South Central Total for Brasil
Number of Cervical Cytopatologic Tests per Year in Brazil and Brazilian Regions,
from 1995 to 2006 *
Number of Cervical Cytopatologic Tests per Year in Brazil and Brazilian Regions,
from 1995 to 2006 *
•Projection for 2006 (data for 11 months)
Source: Datasus (www.datasus.gov.br , access on 02/02/2007)
•Projection for 2006 (data for 11 months)
Source: Datasus (www.datasus.gov.br , access on 02/02/2007)

0,00
10,00
20,00
30,00
40,00
50,00
60,00
70,00
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
Year
Am
ount
(R$)
Expenditure for Cervical CytopathologicTests. Brazil, 1995 to 2006 *
Expenditure for Cervical CytopathologicTests. Brazil, 1995 to 2006 *
* Until November 2006; Expenditure in millions (Reais)
Source: Datasus (www.datasus.gov.br , access on 02/02/2007)
* Until November 2006; Expenditure in millions (Reais)
Source: Datasus (www.datasus.gov.br , access on 02/02/2007)

4,9%
31,2%
40,8%
16,4%
6,6%
North Northeast Southeast South Central
Proportion of Expenditure for Cytopathologic Tests per Region.
Brazil, 1995 to 2006
Proportion of Expenditure for Cytopathologic Tests per Region.
Brazil, 1995 to 2006
Source: Datasus (www.datasus.gov.br , access on 02/02/2007)Source: Datasus (www.datasus.gov.br , access on 02/02/2007)

Sources: Dados dos Registros de Câncer Base Populac ionalMP/Fundação Instituto Brasileiro de Geografia e Est atística – IBGEMS/INCA/Conprev/Divisão de Informação
Sources: Dados dos Registros de Câncer Base Populac ionalMP/Fundação Instituto Brasileiro de Geografia e Est atística – IBGEMS/INCA/Conprev/Divisão de Informação
Specific Rates for Cancer of the Cervix Incidence, Salvador, 1998 - 2002
Specific Rates for Cancer of the Cervix Incidence, Salvador, 1998 - 2002
0,0
10,0
20,0
30,0
40,0
50,0
60,0
70,0
80,0
Age group
Spe
cific
rat
e
C53 - Cervix malign neoplasia D06 - Cervix carcinoma “in situ”
0-4
5-9
10-1
415
-19
20-2
425
-29
30-3
435
-39
40-4
445
-49
50-5
455
-59
60-6
465
-69
70-7
475
-79
80-8
4 85,
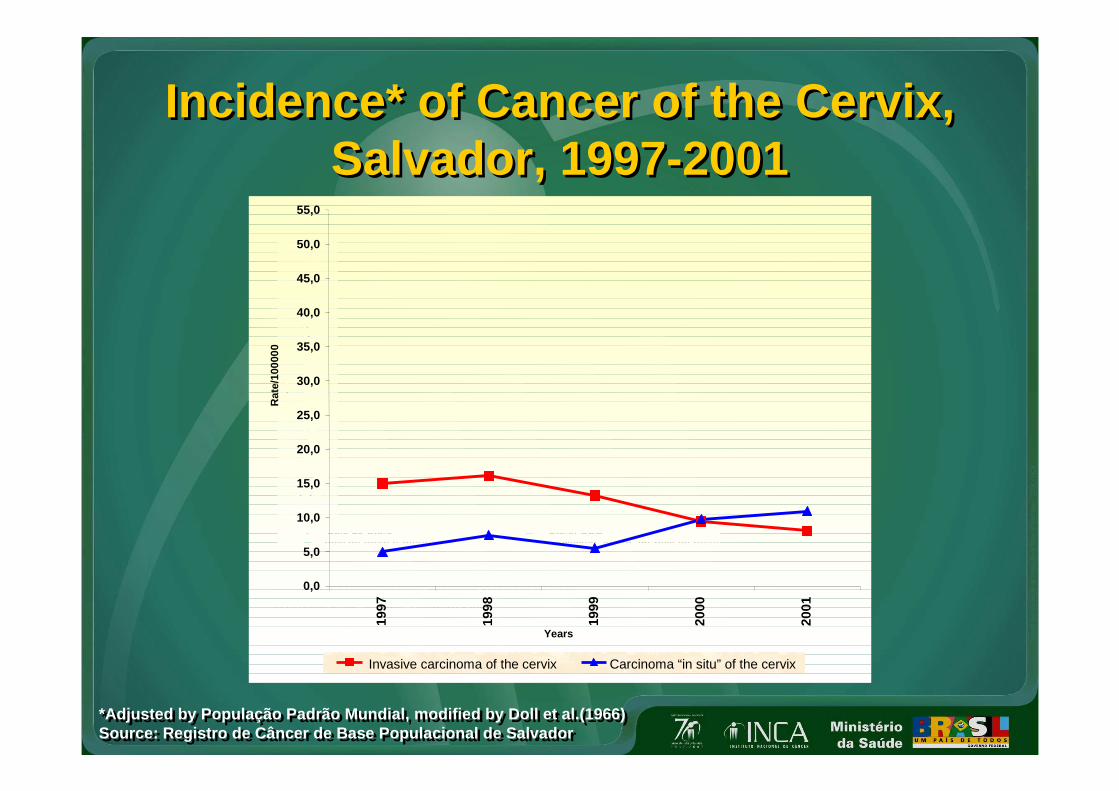
*Adjusted by População Padrão Mundial, modified by Doll et al.(1966)Source: Registro de Câncer de Base Populacional de Salvador*Adjusted by População Padrão Mundial, modified by Doll et al.(1966)Source: Registro de Câncer de Base Populacional de Salvador
Incidence* of Cancer of the Cervix, Salvador, 1997-2001
Incidence* of Cancer of the Cervix, Salvador, 1997-2001
(1) População Padrão Mundial, modificada por Doll et al.(1966)
(2) População de Salvador, 1997-2001 - IBGE
Fontes: Fundação Instituto Brasileiro de Geografia e Estatística - IBGE
Divisão de Informção - CONPREV/INCA/MS
Registro de Câncer de Base Populacional de Salvador
Taxas de Incidência por
câncer do Colo do Úter o,
Útero, SOE e Carcinoma "in si tu",
ajustadas por idade
pela população mundial,
por 100.000 mulheres,
Salvador, entre 1997 e
2001.
0
2
4
6
8
10
12
14
16
18
20
Anos
Colo do Útero Útero, SOEColo do Útero e Útero, SOE Carcinoma "in situ" do Colo do Útero
0,0
5,0
10,0
15,0
20,0
25,0
30,0
35,0
40,0
45,0
50,0
55,0
1997
1998
1999
2000
2001
Years
Rat
e/10
0000
Invasive carcinoma of the cervix Carcinoma “in situ” of the cervix

Sources: Dados dos Registros de Câncer Base Populac ionalMP/Fundação Instituto Brasileiro de Geografia e Est atística – IBGEMS/INCA/Conprev/Divisão de Informação
Sources: Dados dos Registros de Câncer Base Populac ionalMP/Fundação Instituto Brasileiro de Geografia e Est atística – IBGEMS/INCA/Conprev/Divisão de Informação
Specific Rates for Cancer of the Cervix Incidence, Porto Alegre, 1997- 2001.
Specific Rates for Cancer of the Cervix Incidence, Porto Alegre, 1997- 2001.
Age group
0,0
10,0
20,0
30,0
40,0
50,0
60,0
70,0
Spe
cific
rate
C53 - Cervix malign neoplasia D06 - Cervix carcinoma “in situ
0-4
5-9
10-1
415
-19
20-2
425
-29
30-3
435
-39
40-4
445
-49
50-5
455
-59
60-6
465
-69
70-7
475
-79
80-8
4 85,

Sources: Dados dos Registros de Câncer Base Populacio nalMP/Fundação Instituto Brasileiro de Geografia e Estatís tica – IBGEMS/INCA/Conprev/Divisão de Informação
Sources: Dados dos Registros de Câncer Base Populacio nalMP/Fundação Instituto Brasileiro de Geografia e Estatís tica – IBGEMS/INCA/Conprev/Divisão de Informação
*População Padrão Mundial*População Padrão Mundial
Specific Rates for Cancer of the Cervix Incidence, Age Adjusted*.Porto Alegre,1997- 2001.
Specific Rates for Cancer of the Cervix Incidence, Age Adjusted*.Porto Alegre,1997- 2001.
1997 1998 1999 2000 2001
C53 - Cervix malign neoplasia D06 - Cervix carcinoma “in situ
0,0
Spe
cific
rate
10,0
20,0
30,0

Current NecessitiesCurrent Necessities
• Increase quality of cytopathology test
• Increase quality of specimen collection
• Guarantee patient follow-up
• Increase quality of cytopathology test
• Increase quality of specimen collection
• Guarantee patient follow-up

Main ChallengesMain Challenges
• Organization of Services
• System of Information
• Permanent Education
• Process and Results’ Evaluation
• Organization of Services
• System of Information
• Permanent Education
• Process and Results’ Evaluation

Cancer in Numbers WorldwideCancer in Numbers Worldwide
Source: 2005 UICC ReportSource: 2005 UICC Report
2006
11 million new cases
7 million deaths
2020
16 million new cases
12 million deaths
60% OF NEW CASES IN LESS DEVELOPED COUNTRIES
60% OF NEW CASES IN LESS DEVELOPED COUNTRIES

New Cancer Cases per YearNew Cancer Cases per Year
WHO (2003)WHO (2003)
3
4
5
6
7
8
9
10
1990 1995 2000 2005 2010 2015 2020
new
can
cer
case
s (m
illio
ns)
year
developingcountries
industrializedcountries
10 million in 2000
16 million in 2020
50% more
16 million in 2020
50% more

Brazilian Plan of Action Cancer of the Cervix Control 2005 – 2007
Brazilian Plan of Action Cancer of the Cervix Control 2005 – 2007
Strategic Guidelines• Increase coverage for target population • Guarantee quality of tests• Develop human resources • Strengthen systems of information • Conduct research • Mobilize society
Strategic Guidelines• Increase coverage for target population • Guarantee quality of tests• Develop human resources • Strengthen systems of information • Conduct research • Mobilize society

International CongressInternational Congress