interdisciplinary treatment of patients with deep … treatment of patients with deep overbite and...
TRANSCRIPT

International Journal of Science and Research (IJSR) ISSN (Online): 2319-7064
Impact Factor (2012): 3.358
Volume 3 Issue 11, November 2014 www.ijsr.net
Licensed Under Creative Commons Attribution CC BY
Interdisciplinary Treatment of Patients with Deep Overbite and Parafunctional Activity
Miroslava Dinkova, DMD, PhD1, Greta Yordanova, DMD, PhD2
1,2Assistant Professor, Department of Orthodontics, Faculty of Dental Medicine, Medical University - Sofia, Bulgaria
Abstract: Bruxism is defined as parafunctional grinding of teeth and due to the excessive wear of the posterior teeth, patients with long-standing bruxism often have pathological deep overbite. For many decades, treatment of bruxism and deep overbite was focused on reshaping the bite for achieving an occlusion free of deviations. Despite large efforts, the management of bruxism and subsequent deepening overbite was not obtained. Keywords: overbite, bruxism, parafunction, adults 1. Introduction Deep overbite is one of the frequently seen malocclusions. It can occur isolated or along with other associated malocclusions [1]. It is thought to have a hereditary component. Deep overbite is said to be one of the most damaging malocclusions [1]. Graber has defined “Deep bite” as a condition of excessive vertical overlap between the maxillary and mandibular incisal margins when mandible is brought into habitual or centric occlusion [2]-[3]. It can be diagnosed when the lower incisors are overlapped by the upper incisors more than 2/3rd of the clinical crown height (fig. 1).
Figure 1: Virtual patient with deep overbite
The vertical overlap is either described in millimeters or as a percentage of mandibular incisor crown length overlapped by maxillary central incisors (1/3rd, 2/3rd and etc.). A notation of the overbite in percentage is stated as more descriptive and desirable since the measurement in millimeters does not give information about the degree of the overlap [1]. The deep overbite can be classified: • According to its origin – dental and skeletal deep bite. • According to the function – true and pseudo deep bite. • Depending on the extent of deep bite – incomplete and
complete overbite. • According to the dentition – deep overbite in primary,
mixed and permanent dentition. Of the above, the deep bite in adult non-growing patients is the most difficult and complex for treating. In such cases progressively with age a complicated pathology with breakdown of periodontal tissues, TMJ and teeth structures are observed [4]-[8]. Often deep overbite is related with increased muscular activity and persisting parafunctional
habits (bruxism, teeth clenching and etc.) [9]. Bruxism is defined as parafunctional grinding of teeth and oral habit consisting of involuntary rhythmic or spasmodic nonfunctional gnashing, grinding, or clenching of the teeth, in other than chewing movements of the mandible, which may lead to occlusal trauma [10]. American Academy of Orofacial Pain defined bruxism as “a diurnal (wake-time) and nocturnal (sleep-related) parafunctional activity” [11]. The prevalence of self-reported sleep bruxism is approximately 8% in the general adult population, in women and men alike [12]. According to Ricketts tooth wear is the most detrimental bruxism-related condition and as a side effect of it patients often have a deep overbite [13]. Due to the excessive wear of the posterior teeth, patients with long-standing bruxism have pathological overlap and affected facial esthetics and impaired dental health as a secondary consequence (fig. 2) [14].
Figure 2: Effects of bruxism - compared with healthy teeth
Furthermore the deep overbite malocclusion nowadays has been linked to the periodontal disease induction [15]. Occlusal, bruxism-related forces cause a stress in enamel and dentin structures and as a result a v-shaped cervical lesions, abfraction and teeth cracks can also be observed [16]. As a consequence for many decades, treatment of bruxism was focused on reshaping the bite as to achieve an occlusion and articulation that were free of deviations and interferences. Nevertheless and despite large efforts to optimize occlusal treatments effective, the management of bruxism and the
Paper ID: SUB14151 2920

International Journal of Science and Research (IJSR) ISSN (Online): 2319-7064
Impact Factor (2012): 3.358
Volume 3 Issue 11, November 2014 www.ijsr.net
Licensed Under Creative Commons Attribution CC BY
subsequent deepening overbite was not obtained. 2. Purpose The aim of the current study is to present a contemporary interdisciplinary treatment, including initial periodontal therapy, full orthodontic treatment for leveling, alignment and occlusion height recovery, non-invasive prosthodontic restorative therapy for the abraded teeth for achieving a full anatomy and functional integrity and myofunctional therapy for occlusal balance. 3. Case Report, Diagnosis. Treatment
planning, Treatment progress and Results 3.1 Case report A 21-year-old male patient was referred to our Orthodontic Clinic with chief compliant of pathological abrasion, increasing teeth sensitivity, jaw pain and frequent headaches. The medical family history of the patient revealed a hereditary deep overbirte and bruxism. The extraoral clinical examination displayed a brachycephalic and euryprosopic face, straight profile with a decreased lower facial height, hyperactive masticatory muscle and thin lips (fig. 3).
Figure 3: Extraoral view of the patient before the beginning
of the interdisciplinary treatment The intraoral clinical examination showed an expanded upper dental arch, flat palate, abrasion, teeth fractures, inverted curve of Spee in the upper dental arch and deep curve of Spee in the lower dental arch, impaired occlusal function (fig. 4).
Figure 4: Intraoral view of the patient before the beginning
of the interdisciplinary treatment
3.2 Diagnosis To support the orthodontic analysis a silicone impressions of both dental arches and bite registration were taken. The impressions were poured with stone plaster and the obtained casts were mounted into KaVo PROTARevo articulator using an individual face bow. For better visual control and treatment outcomes the casts were scanned and imported in Orapix software® (Orapix Co., Seoul, Korea). A 3D virtual set-up with final leveling and alignment was made (fig. 5). After the casts were dubbed, they were given to the prosthodontic specialist to make his treatment plan.
Figure 5: Orapix® set-up preparation
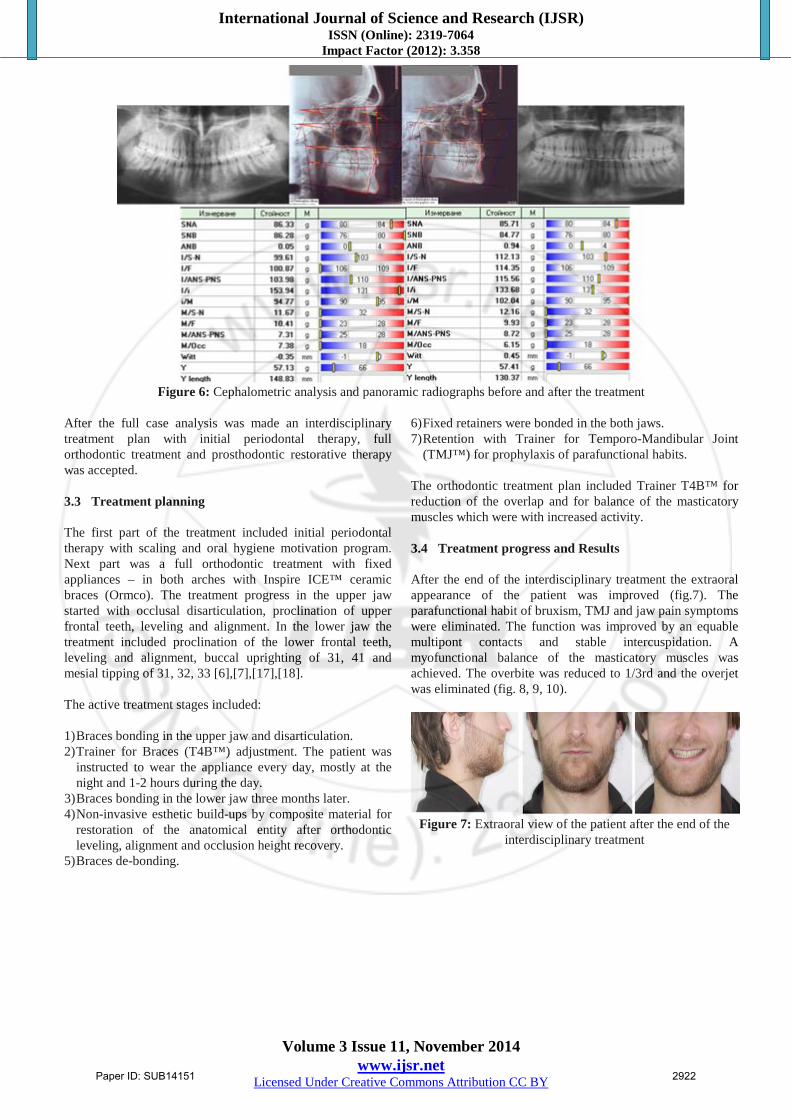
A full photo-documentation protocol was performed with Canon EOS – 550D Camera and Sigma EM-140 DG Ring Flash. The extraoral facial documentation included profile and frontal facial views of the patient. The intraoral documentation included occlusal (frontal and lateral) and dental arches photos. This protocol was performed in a 3-month period (fig. 3 and fig. 4). Panoramic radiographs and lateral cephalograms were taken before the beginning of the orthodontic treatment and after the end of it. The biometric orthodontic analysis showed: • Angle Class I molar and canine relationship. • 1 mm overjet. • >2/3rd overbite. • Expansion in both teeth arches. • Spaces. • Rotated and inclinated teeth. • Deviation of the lower midline. The Cephalometric analysis revealed a skeletal Class I with ANB angle of 0.7 degrees and skeletal Class I according to Wits analysis (-0.35), hypodivergent skeletal type, skeletal deep bite, parallelism of facial planes – FH, SpP, OcP, M (fig. 6). The panoramic radiograph revealed all the permanent teeth are existing. In some teeth a bone loss was established (fig. 6).
Paper ID: SUB14151 2921
International Journal of Science and Research (IJSR) ISSN (Online): 2319-7064
Impact Factor (2012): 3.358
Volume 3 Issue 11, November 2014 www.ijsr.net
Licensed Under Creative Commons Attribution CC BY
Figure 6: Cephalometric analysis and panoramic radiographs before and after the treatment
After the full case analysis was made an interdisciplinary treatment plan with initial periodontal therapy, full orthodontic treatment and prosthodontic restorative therapy was accepted. 3.3 Treatment planning The first part of the treatment included initial periodontal therapy with scaling and oral hygiene motivation program. Next part was a full orthodontic treatment with fixed appliances – in both arches with Inspire ICE™ ceramic braces (Ormco). The treatment progress in the upper jaw started with occlusal disarticulation, proclination of upper frontal teeth, leveling and alignment. In the lower jaw the treatment included proclination of the lower frontal teeth, leveling and alignment, buccal uprighting of 31, 41 and mesial tipping of 31, 32, 33 [6],[7],[17],[18].
The active treatment stages included:
1) Braces bonding in the upper jaw and disarticulation. 2) Trainer for Braces (T4B™) adjustment. The patient was
instructed to wear the appliance every day, mostly at the night and 1-2 hours during the day.
3) Braces bonding in the lower jaw three months later. 4) Non-invasive esthetic build-ups by composite material for
restoration of the anatomical entity after orthodontic leveling, alignment and occlusion height recovery.
5) Braces de-bonding.
6) Fixed retainers were bonded in the both jaws. 7) Retention with Trainer for Temporo-Mandibular Joint
(TMJ™) for prophylaxis of parafunctional habits.
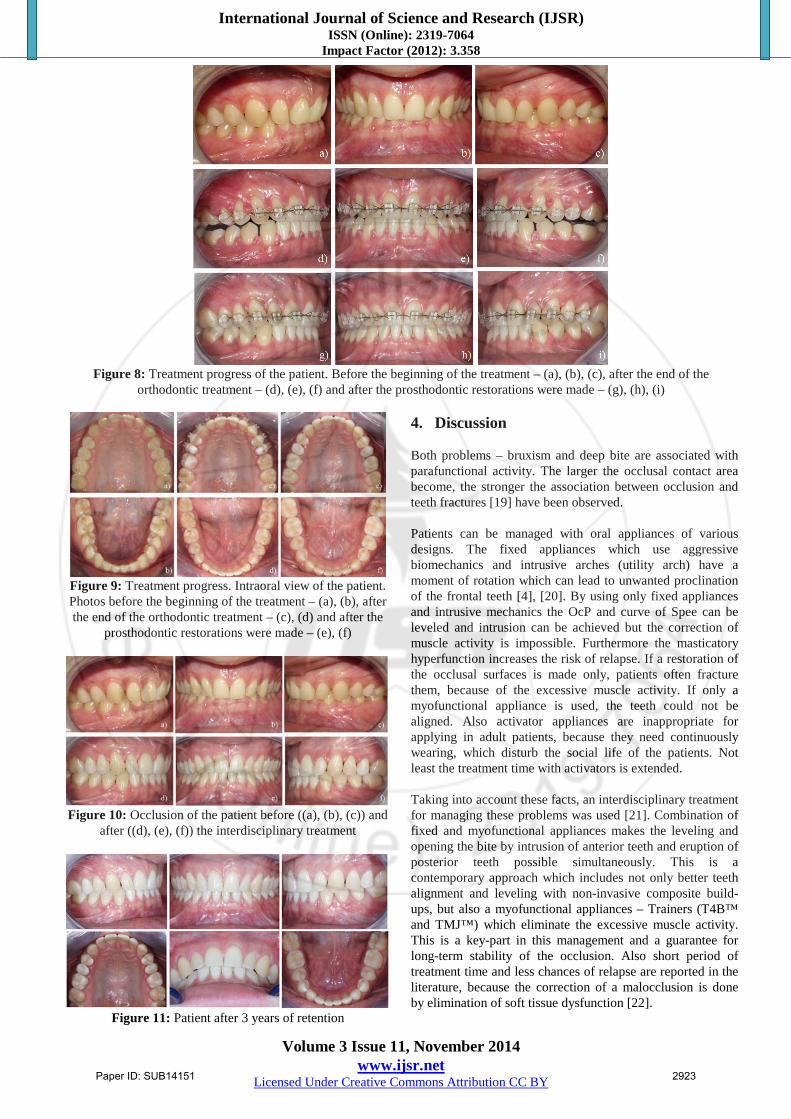
The orthodontic treatment plan included Trainer T4B™ for reduction of the overlap and for balance of the masticatory muscles which were with increased activity. 3.4 Treatment progress and Results After the end of the interdisciplinary treatment the extraoral appearance of the patient was improved (fig.7). The parafunctional habit of bruxism, TMJ and jaw pain symptoms were eliminated. The function was improved by an equable multipont contacts and stable intercuspidation. A myofunctional balance of the masticatory muscles was achieved. The overbite was reduced to 1/3rd and the overjet was eliminated (fig. 8, 9, 10).
Figure 7: Extraoral view of the patient after the end of the
interdisciplinary treatment
Paper ID: SUB14151 2922
International Journal of Science and Research (IJSR) ISSN (Online): 2319-7064
Impact Factor (2012): 3.358
Volume 3 Issue 11, November 2014 www.ijsr.net
Licensed Under Creative Commons Attribution CC BY
Figure 8: Treatment progress of the patient. Before the beginning of the treatment – (a), (b), (c), after the end of the
orthodontic treatment – (d), (e), (f) and after the prosthodontic restorations were made – (g), (h), (i)
Figure 9: Treatment progress. Intraoral view of the patient. Photos before the beginning of the treatment – (a), (b), after the end of the orthodontic treatment – (c), (d) and after the
prosthodontic restorations were made – (e), (f)
Figure 10: Occlusion of the patient before ((a), (b), (c)) and
after ((d), (e), (f)) the interdisciplinary treatment
Figure 11: Patient after 3 years of retention
4. Discussion Both problems – bruxism and deep bite are associated with parafunctional activity. The larger the occlusal contact area become, the stronger the association between occlusion and teeth fractures [19] have been observed. Patients can be managed with oral appliances of various designs. The fixed appliances which use aggressive biomechanics and intrusive arches (utility arch) have a moment of rotation which can lead to unwanted proclination of the frontal teeth [4], [20]. By using only fixed appliances and intrusive mechanics the OcP and curve of Spee can be leveled and intrusion can be achieved but the correction of muscle activity is impossible. Furthermore the masticatory hyperfunction increases the risk of relapse. If a restoration of the occlusal surfaces is made only, patients often fracture them, because of the excessive muscle activity. If only a myofunctional appliance is used, the teeth could not be aligned. Also activator appliances are inappropriate for applying in adult patients, because they need continuously wearing, which disturb the social life of the patients. Not least the treatment time with activators is extended. Taking into account these facts, an interdisciplinary treatment for managing these problems was used [21]. Combination of fixed and myofunctional appliances makes the leveling and opening the bite by intrusion of anterior teeth and eruption of posterior teeth possible simultaneously. This is a contemporary approach which includes not only better teeth alignment and leveling with non-invasive composite build-ups, but also a myofunctional appliances – Trainers (T4B™ and TMJ™) which eliminate the excessive muscle activity. This is a key-part in this management and a guarantee for long-term stability of the occlusion. Also short period of treatment time and less chances of relapse are reported in the literature, because the correction of a malocclusion is done by elimination of soft tissue dysfunction [22].
Paper ID: SUB14151 2923
International Journal of Science and Research (IJSR) ISSN (Online): 2319-7064
Impact Factor (2012): 3.358
Volume 3 Issue 11, November 2014 www.ijsr.net
Licensed Under Creative Commons Attribution CC BY
The Trainer for Braces™ (T4B™) is highly flexible, retrains the oral musculature (the Myofunctional Effect™) and treats the temporomandibular joint (TMJ) disorder (fig. 12). Braces Channels accommodate brackets and orthodontic archwire, and protect cheeks and gums, while lip bumpers discourage overactive lip muscle activity [23], [24].
Figure 12: Trainer for Braces (T4B™)
The TMJ Appliance™ relaxes the cranio-mandibular muscles – for extracapsular relief (Fig. 13). It treats symptoms by decompressing the joint through its aerofoil shaped base and eliminates the bruxism with its double-mouthguard effect. Further relief is provided by the change in the resting length of the muscles when the appliance is in place. This treatment assists in relieving TMJ and cranio-mandibular symptoms, limiting bruxing and grinding, and improves patient comfort [23], [24].
Figure 13: Trainer for TMJ (TMJ™)
5. Conclusion It is critical for successful dental therapy to understand the relationship between the parafunctional activity and subsequent formation of orthodontic malocclusions. The complexity of such cases needs comprehensive treatment plan and proper interdisciplinary management. The combination of different fields of dentistry makes the long-term stability of patients’ occlusion possible. References [1] C. Sreedhar, S. Baratam. Deep overbite – A review.
Annals and Essences of Dentistry; 1(1): pp. 8–25, 2009. [2] T.M. Graber, Current Orthodontic Concepts and
Techniques. Philadelphia, ISBN-10: 0721641873, W. B. Saunders Company, 1969.
[3] T.M .Graber, Orthodontics: Principles and Practice. 3rd ed. Philadelphia, ISBN 10: 0721641822 W. B. Saunders Company, pp. 740–789, 1972.
[4] C.J. Burstone, Biomechanics of deep overbite correction. Semin Orthod; 7 (1): pp. 26–33, 2001.
[5] C.J. Burstone, Deep overbite correction by intrusion. Am J Orthod; 72 (1): pp. 1–22, 1977.
[6] W.R. Proffit, H.W. Fields. Contemporary Orthodontics. 3rd ed. St Louis, Mosby; ISBN-10: 1556645538, 2000.
[7] M. Dinkova, Orthodontic treatment management in adult patients with periodontal problems in the frontal area. Dissertation in Sofia, Medical University of Sofia, Bulgaria, 2013.
[8] J.P. Goulet, J.P Lund, J. Montplaisir, et al, Daily clenching, nocturnal bruxism, and stress and their association with TMD symthoms. J Orofac Pain; 7: pp. 89, 1993.
[9] W. Jerjes, T. Upile, S. Abbas, P. Kafas, M. Vourvachis, J. Rob, E. Carthy, N. Angouridakis, C. Hopper, Muscle disorders and dentition-related aspects in temporomandibular disorders: controversies in the most commonly used treatment modalities. International Archives of Medicine; 1: pp. 23, 2008.
[10] Academy of Prosthodontics, The Glossary of Prosthodontic Terms. St. Louis, Mo.: Mosby; IBSN: 61265643; 94: pp. 10–92, 2005.
[11] R. De Leeuw, Orofacial Pain. Guidelines for Assessment, Diagnosis, and Management. Ed 4. Chicago: Quintessence, ISBN-10: 0867154136, 2008.
[12] G.J. Lavigne, S. Khoury, S. Abe, T. Yamaguchi, K. Raphael, Bruxism physiology and pathology: an overview for clinicians. Journal of Oral Rehabilitation; 35: pp. 476–494, 2008.
[13] R.M. Ricketts. Occlusion, the Medium of Dentistry. J. Prosthet. Dent.; 21: pp. 39–60. PubMed, 1969.
[14] N.D. Gupta, S. Maheshwari, K.C. Prabhat, L.A. Goyal, Critical review of the management of deep overbite complicated by periodontal diseases. Eur J Gen Dent; 1: pp. 2–5, 2012.
[15] J. Yardeni, Highlights of functional dental morphology: a brief survey. Dent Dig.; 75 (10): pp. 410–4, 1969.
[16] M.S. Sumanth, G. S. Rashmi, S.M. Noopur, A. Managoli, G. R. Surabhi, M. P.l Ashwini. No Carious Cervical Lesions: Abfraction. J Int Oral Health; 5(5): pp. 143–146, 2013.
[17] R. Nanda, Biomechanics in Clinical Orthodontics. Philadelphia; W. R. Saunders company, ISBN: 0721627846 9780721627847, 1996.
[18] R. Nanda, The Differential Diagnosis and Treatment of Excessive Overbite. – In: Nanda R. Symposium on Orthodontics; 69: pp. 82, 1981.
[19] J. Takehara, T. Takano, R. Akhter, M. Morita, Correlations of non-carious cervical lesions and occlusal factors determined by using pressure-detecting sheet. J Dent; 36 (10): pp. 774–779, 2008.
[20] B. Shroff, W.M. Yoon, S.J. Lindauer, C.J. Burstone. Simultaneous intrusion and retraction using a three-piece base arch. The Angle Orthodontist; 67: pp. 455–461, 1997.
[21] D. Mahony Combining functional appliances in the straightwire system. The Journal of Clinical Pediatric Dentistry; 26 (2), pp. 137–140, 2002.
Paper ID: SUB14151 2924

International Journal of Science and Research (IJSR) ISSN (Online): 2319-7064
Impact Factor (2012): 3.358
Volume 3 Issue 11, November 2014 www.ijsr.net
Licensed Under Creative Commons Attribution CC BY
[22] P. Pallavi, M.P. Suryakanth. Effect of Preorthodontic Trainer in Mixed Dentition. Case Reports in Dentistry, Article ID: 717435, 2013.
[23] G. Ramirez-Yañez, A. Sidlauskas, E. Junior, J. Fluter Dimensional changes in dental arches after treatment with a prefabricated functional appliance. J Clin Pediatr Dent.; 31 (4): pp. 279–83, 2007.
[24] Myofunctional Research Co: Trainer System™ DVD, 2008.
Author Profile
Miroslava Mileti Dinkova, DMD, PhD entered the field of dentistry in 1978 and specialized in Orthodontics, Pediatric Dentistry, Health Management and General Dentistry in 1987, 1993 and 2005, respectively at Faculty of Dental Medicine, Medical
University of Sofia, Bulgaria. In 2014 she received her PhD degree in Orthodontics. Since 1992 she is Assistant Professor at the Department of Orthodontics - Medical University of Sofia, Bulgaria. Her main interests are in adult orthodontics, interdisciplinary treatment approaches, lingual orthodontics and digital technologies in orthodontics. Dr. Dinkova is a member of WFO, EOS, SIDO, BaSS, BOS and President of BSCLO.
Dr. Greta Yordanova, DMD, PhD has completed a master's degree in dentistry in 1991. She has post-graduated in Orthodontics and developed dissertation entitled “Clinical results in treatments with Pendulum” and obtained PhD degree. Since 1995 she is Assistant Professor at the Department of Orthodontics at the
Medical University of Sofia. Her research interests are in the area of Non-extraction treatment and problems of ectopic and impacted teeth and working with 3D technology.
Paper ID: SUB14151 2925