interaction of two lipid disorders in a large french-canadian...
TRANSCRIPT

Interaction of Two Lipid Disorders in aLarge French-Canadian Kindred
Jean Davignon, Suzanne Lussier-Cacan, Antoine Gattereau,Patricia P. Moll, and Charles F. Sing
This study investigates the pedigree of 508 individuals over five generations identi-fied by an individual with hypertriglyceridemia, familial hypercholesterolemia, and alib llpoprotein electrophoretlc phenotype. The sample of 378 living individuals studiedextensively for risk factors and disease status was distributed among maternal (170)and paternal (176) relatives and the codescendants (32) of the index case. It was foundthat the distributions of the plasma lipid and lipoprotein abnormalities in the differentsubsets of the kindred were consistent with the presence of two separate hereditarylipid disorders: familial hypercholesterolemia on the paternal side and familial hyper-prebetallpoproteinemia on the maternal side. This combination of disorders with apossible contribution from factors influencing glucose metabolism was associatedwith a high frequency of hypercholesterolemia and its clinical manifestations and ofcardiovascular morbidity among the codescendants. An interaction effect is suggest-ed as an explanation for the unusually high prevalence of hyperlipidemia among thecodescendants and for the presence of a Mb phenotype in the index case.(Arteriosclerosis 3:13-22, January/February, 1983)
Familial hypercholesterolemia (FH) is character-ized by a very high plasma low density lipopro-
tein (LDL) cholesterol level, the presence of tendonxanthomas in some affected subjects, prematureatherosclerosis, and a decreased number of cell sur-face LDL-receptors.1 Although plasma cholesterol inFH is always markedly elevated, plasma triglycer-ides and their major carrier, very low density lipopro-
From the Department of Lipid Metabolism and AtherosclerosisResearch, Clinical Research Institute of Montreal, and the Univer-sity of Montreal, Faculty of Medicine, Montreal, Quebec, Canada,and the Department of Human Genetics, University of MichiganMedical School, Ann Arbor, Michigan.
Address for reprints: Dr. Jean Davignon, Department of LipidMetabolism, Clinical Research Institute of Montreal, 110 PineAvenue West, Montreal, Quebec, Canada H2W 1R7.
This work was supported by grants from Health and WelfareCanada (604-7-759 and 6605-1658-53), the Medical ResearchCouncil of Canada (MT-5427), the Quebec Heart Foundation, andgrants US-DOE 2828 and NIH HL 24489.
This work was presented in part at the Fifth International Sym-posium on Athersclerosis, Houston, Texas, 1979. Dr. Lussier-Cacan was a fellow of the Canadian Heart Foundation during thecompletion of this study.
Received September 28, 1981; revision accepted August 31,1982.
See NAPS Document No. 04035 for nine pages of supplemen-tary material. Order from NAPS, c/o Microfiche Publications, P.O.Box 3513, Grand Central Station, New York, New York 10163.Remit in advance, in U.S. funds only, $7.75 for photocopies or$4.00 for microfiche. Outside the U.S. and Canada, add postageof $4.50 for photocopy and $1.50 for microfiche.
teins(VLDL), may be either normal (FH lla) or elevat-ed (FH lib). FH patients with the lib phenotyperepresent a heterogeneous group2'3 since both en-vironmental and genetic factors may be responsiblefor the superimposed hypertriglyceridemia. Thisstudy was initiated in an attempt to sort out thesevarious influences in a proband with typical FH andthe Mb phenotype and to establish the genetic etiol-ogy of the plasma lipid levels and lipoprotein patternsin a French-Canadian pedigree identified by such aproband.
This paper presents the description of the studyand the initial analyses carried out. We identified 508individuals in five generations and extensively stud-ied 379 (four generations) who were alive. Theseindividuals were distributed into four major subsetsdefined with respect to the index: 135 paternal rela-tives (P subset); 142 maternal relatives (M subset);26 codescendants (C subset) which included hisoffspring, his siblings, and all of their offspring; andfinally, 75 nonmembers who married into the pedi-gree (NM subset). The nonmembers were furthersubdivided according to the subset of the pedigreeinto which they married (i.e., P nonmembers).
We shall demonstrate in this paper that the adultsand children in the different subsets that composethe pedigree differed markedly in the frequencies oflipoprotein abnormalities and clinical manifestationsof atherosclerotic disease. It will be shown that the
13
by guest on June 30, 2018http://atvb.ahajournals.org/
Dow
nloaded from

14 ARTERIOSCLEROSIS VOL 3, No 1, JANUARY/FEBRUARY 1983
lib phenotype of the index case and the distributionof lipid phenotypes in the different subsets are con-sistent with the presence of two separate, hereditarylipid disorders in this pedigree that are distinct fromfamilial combined hyperlipidemia. This combinationof disorders is associated with an increased frequen-cy of hypercholesterolemia and its clinical manifesta-tions and of cardiovascular morbidity in the C subset.
Methods
Index Case
The index case was selected from 26 potentialprobands with a type lib electrophoretic phenotypeand a well documented diagnosis of xanthomatousFH. The criteria for selection included: the size of thepedigree, the availability of living relatives, the distri-bution of subjects between maternal and paternalrelatives, the number of codescendants, and thegeographic dispersion of the individuals of thekindred.
The index case selected (III-7 in figure 1) was aFrench-Canadian police officer, born in Saint-Andre,New Brunswick, who had moved to a Montreal sub-
urb at the age of 18, married at 23, and had sevenchildren. His father was discovered to be hypercho-lesterolemic shortly before his death at age 57 of amyocardial infarction. This event prompted a familysurvey which revealed the presence of hypercholes-terolemia in several of the index's siblings. Twomonths before his referral to our lipid clinic at age 36,the presence of hyperlipidemia (cholesterol, 365 mg/dl; triglycerides, 200 mg/dl) had been documentedduring hospitalization for atypical chest pain, anxiety,and gastrointestinal symptoms. Myocardial ischemiawas indicated by an ECG during a two-step Master'stest, and coronary atherosclerosis was demonstrat-ed by a coronary angiogram. Shortly before we be-gan to collect his genealogy in 1972, he sustained (atage 37) an acute anteroseptal myocardial infarctionfrom which he recovered uneventfully.
He was of normal weight (77.6 kg) for his height(1.83 m). Bilateral xanthelasma had been present forseveral years and were stable in size. He had arcuscorneae and xanthomas of the Achilles tendons bi-laterally and of the extensor tendon of the middleright finger. His plasma cholesterol level at entry intoour clinic in January 1971 was 370 mg/dl and histriglyceride level was 238 mg/dl. The plasma lipopro-
III
IV n + e> o B o2 3 4 5 6
• • €> D LJ14 12 13
o10
[+] DECEASED |_J NORMAL
O FEMALES B TYPE lie
| | MALES | TYPE lib
INDEX 3 TYPE IV
I MALE NOT EXAMINED
A ANGINA
A INFARCT
• DIABETES
O CHO-INTOL.
• CHOLELITHIASIS
X TENDON XANTHOMA
Xo XANTHELASMA
3 ARCUS CORNEAE
i ARTERIAL BRUIT
CHOLi
TG
120
74
AGE 6
DPEDIGREE 13
NO.
Figure 1 . Plasma lipids, age, and clinical manifestations of hyperlipidemia and atherosclerosis in the codescendants andtheir spouses. The frequency and severity of the hyperlipidemia and of its clinical consequences are higher than expectedfrom the inheritance of the two lipid transport disorders transmitted Independently and militate in favor of genetic interactions(CHO-intol = carbohydrate intolerance).
by guest on June 30, 2018http://atvb.ahajournals.org/
Dow
nloaded from
HYPERLIPIDEMIA IN A FRENCH-CANADIAN KINDRED Davignon et al. 15
tein cholesterol levels were 80 mg/dl for VLDL, 261mg/dl for LDL, and 29 mg/dl for high density lipopro-teins (HDL). He had an impaired glucose tolerance4
with a normal fasting glycemia of 102 mg/dl and val-ues at 60 minutes of 222 mg/dl and at 120 minutes of188 mg/dl. The major causes of secondary hyperlipi-demias were excluded by a thorough clinical andlaboratory evaluation.
Definition of the Pedigree
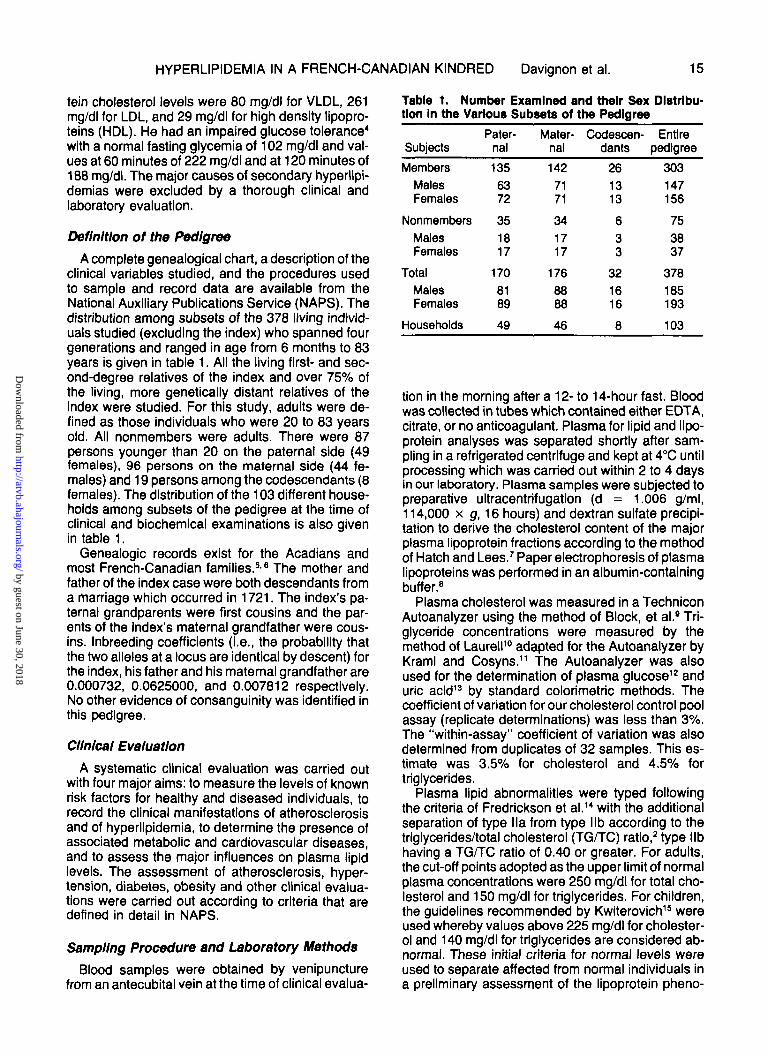
A complete genealogical chart, a description of theclinical variables studied, and the procedures usedto sample and record data are available from theNational Auxiliary Publications Service (NAPS). Thedistribution among subsets of the 378 living individ-uals studied (excluding the index) who spanned fourgenerations and ranged in age from 6 months to 83years is given in table 1. All the living first- and sec-ond-degree relatives of the index and over 75% ofthe living, more genetically distant relatives of theindex were studied. For this study, adults were de-fined as those individuals who were 20 to 83 yearsold. All nonmembers were adults. There were 87persons younger than 20 on the paternal side (49females), 96 persons on the maternal side (44 fe-males) and 19 persons among the codescendants (8females). The distribution of the 103 different house-holds among subsets of the pedigree at the time ofclinical and biochemical examinations is also givenin table 1.
Genealogic records exist for the Acadians andmost French-Canadian families.56 The mother andfather of the index case were both descendants froma marriage Which occurred in 1721. The index's pa-ternal grandparents were first cousins and the par-ents of the Index's maternal grandfather were cous-ins. Inbreeding coefficients (i.e., the probability thatthe two alleles at a locus are identical by descent) forthe index, his father and his maternal grandfather are0.000732, 0.0625000, and 0.007812 respectively.No other evidence of consanguinity was identified inthis pedigree.
Clinical Evaluation
A systematic clinical evaluation was carried outwith four major aims: to measure the levels of knownrisk factors for healthy and diseased individuals, torecord the clinical manifestations of atherosclerosisand of hyperlipidemia, to determine the presence ofassociated metabolic and cardiovascular diseases,and to assess the major influences on plasma lipidlevels. The assessment of atherosclerosis, hyper-tension, diabetes, obesity and other clinical evalua-tions were carried out according to criteria that aredefined in detail in NAPS.
Sampling Procedure and Laboratory Methods
Blood samples were obtained by venipuncturefrom an antecubital vein at the time of clinical evalua-
Table 1. Number Examined and their Sex Distribu-tion In the Various Subsets of the Pedigree
Subjects
Members
MalesFemales
Nonmembers
MalesFemales
Total
MalesFemales
Households
Pater-nal
135
6372
35
1817
170
8189
49
Mater-nal
142
7171
34
1717
176
8888
46
Codescen-dants
26
CO
C
O
6
CO
C
O
32
1616
8
Entirepedigree
303
147156
75
3837
378
185193
103
tion in the morning after a 12- to 14-hour fast. Bloodwas collected in tubes which contained either EDTA,citrate, or no anticoagulant. Plasma for lipid and lipo-protein analyses was separated shortly after sam-pling in a refrigerated centrifuge and kept at 4°C untilprocessing which was carried out within 2 to 4 daysin our laboratory. Plasma samples were subjected topreparative ultracentrifugation (d = 1.006 g/ml,114,000 x g, 16 hours) and dextran sulfate precipi-tation to derive the cholesterol content of the majorplasma lipoprotein fractions according to the methodof Hatch and Lees.7 Paper electrophoresis of plasmalipoproteins was performed in an albumin-containingbuffer.8
Plasma cholesterol was measured in a TechniconAutoanalyzer using the method of Block, et al.9 Tri-glyceride concentrations were measured by themethod of Laurell10 adapted for the Autoanalyzer byKraml and Cosyns.11 The Autoanalyzer was alsoused for the determination of plasma glucose12 anduric acid13 by standard colorimetric methods. Thecoefficient of variation for our cholesterol control poolassay (replicate determinations) was less than 3%.The "within-assay" coefficient of variation was alsodetermined from duplicates of 32 samples. This es-timate was 3.5% for cholesterol and 4.5% fortriglycerides.
Plasma lipid abnormalities were typed followingthe criteria of Fredrickson et al.14 with the additionalseparation of type lla from type Mb according to thetriglycerides/total cholesterol (TG/TC) ratio,2 type libhaving a TG/TC ratio of 0.40 or greater. For adults,the cut-off points adopted as the upper limit of normalplasma concentrations were 250 mg/dl for total cho-lesterol and 150 mg/dl for triglycerides. For children,the guidelines recommended by Kwiterovich15 wereused whereby values above 225 mg/dl for cholester-ol and 140 mg/dl for triglycerides are considered ab-normal. These initial criteria for normal levels wereused to separate affected from normal individuals ina preliminary assessment of the lipoprotein pheno-
by guest on June 30, 2018http://atvb.ahajournals.org/
Dow
nloaded from

16 ARTERIOSCLEROSIS VOL 3, No 1, JANUARY/FEBRUARY 1983
type, taking into account the clinical setting. Thisinitial classification into normals and hypertipidemicswas further documented by plasma lipoprotein anal-yses. A few adults whose lipid levels were above thecut-off points were later reclassified as unaffected asa result of the lipoprotein analyses. Indeed, in someinstances elevated HDL-cholesterol was responsiblefor the total plasma cholesterol exceeding the upperlimit of the normal range. Whenever there was adiscrepancy between the plasma lipids and lipopro-tein measurements (for instance, normal plasmatriglycerides and elevated VLDL-cholesterol) at-tempts were made to find the source of the discrep-ancy. In a few instances this led to including someindividuals in an "unclassifiable" category.
Urine samples were tested immediately after void-ing for the presence of blood, ketones, glucose, andprotein using a standard strip test procedure (Lab-stix, Ames Company, Rexdale, Ontario).
Hypotheses and Statistical Methods
The index was not included in any of the analysesreported here. We considered the distributions ofcontinuous variables and the class frequencies forthe categorical variables: 1) in the total sample ofindividuals, 2) within the subsamples of adults andchildren in the C, M and P subsets, and 3) in theadults who made up the NM subset. The first generalhypothesis tested was that the medians of eachcontinuous variable and relative frequencies of theclasses of each categorical variable were similar foradult members and for the nonmembers of the pedi-gree. Other analyses tested the hypothesis that theclass frequencies and the medians were the same:1) in the P, M and C subsets of adults and children, 2)in the three subsets of spouses who married thosemembers and 3) between hyperlipidemic and normalindividuals.
A two-way analysis of frequencies18 tested the in-dependence of subset assignment and each of thediscrete classifications: status of influences, electro-phoretic type, presence or absence of clinical mani-festations of hyperlipidemia, atherosclerosis, andrisk factors. The null hypothesis that two classifica-tions are independent in their effects on the frequen-cy of joint outcomes was tested by the likelihood ratioof the probability of observing the two-way table un-der the assumption of independence compared tothe probability of the observed table.
The null hypothesis that specified subsets haveequal medians against the alternative that at leastone of the subsets has a different median from atleast one other subset was also tested. If the nullhypothesis was rejected, multiple a-posteriori com-parisons were made to identify statistically signifi-cant contrasts. Because these data were not normal-ly distributed and because the variability amongindividuals was heterogeneous among the subsetscompared, we used the nonparametric Kruskal-Wal-lis test statistic.17
The tests using these nonparametric statistics areconservative in that the actual level of significance issmaller than the stated level when the variable isnormally distributed and there is homoscedasticityamong subsets. We chose the nonparametric ap-proach for the interpretation of the data realizing thatboth parametric and nonparametric approaches as-sume independence of observations which may beviolated when pedigrees are sampled. Unless other-wise noted, the statistical contrasts reported in theresults section were considered to be significantwhen the expected differences would have occurredby chance alone less than 5% of the time. Means,rather than medians, are reported for comparabilityto other studies.
Results
Among the 378 subjects examined, there were nocases of hypothyroidism, high fever within the weekbefore the examination, nephrosis, active hepatitis,obstructive liver disease, or uncontrolled diabetesmellitus that would have necessitated resampling.Among the 193 women, seven were pregnant, andthree of them were resampled at a later date whentheir normal menstrual cycle had resumed. One washyperlipidemic but could not be resampled. Her lipidvalues, as well as those of a child who did not fast,were excluded from the study.
Of the 108 individuals, besides the pregnant wom-en, who presented with one or more influencesknown to affect lipid levels, none was considered toneed resampling. Two persons had major surgeryapproximately 2 months before sampling but theirpreviously diagnosed hyperlipidemia persisted. Onesubject had had a partial ileal bypass operation sev-eral years earlier for the treatment of hypercholester-olemia but was still hypercholesterolemic. Four sub-jects were receiving a lipid-lowering agent, but thetherapy was not effective. One subject with doc-umented hypercholesterolemia had sustained arecent myocardial infarction within 1.5 months ofsampling and still had hypercholesterolemia. Of 34subjects on a low fat diet, only two reported a recentmoderate weight loss, and the influence of this onlipids was considered negligible. There were 19women on oral contraceptives, 14 on estrogens, andseven had had ovariectomies.
There were no differences between nonmembersand adult members of the pedigree in average age,height, weight, body mass index (BMI = weight overheight squared), blood pressure, glucose, and uricacid levels. Furthermore, the mean levels of thesemeasures for adult members and nonmembers wereindependent of the relationship of the subject to theindex. Similarly, when adjustments were made forvariations in age, there were no differences betweenchildren of the various subsets for the other varia-bles. The large number of children (53.3% of totalsample, 101 females and 101 males) accounted for
by guest on June 30, 2018http://atvb.ahajournals.org/
Dow
nloaded from

HYPERLIPIDEMIA IN A FRENCH-CANADIAN KINDRED Davignon et al. 17
a low mean age of 21.4 years for the total sample atthe time of examination.
The distribution of electrophoretic phenotypes ofthe 349 individuals who were typed is summarized intable 2. Among the 16 individuals not classified ashaving either a normal or a specific hyperlipidemictype, 14 had a VLDL cholesterol level higher thanexpected from their total triglyceride level and twohad a VLDL cholesterol level lower than expected.These individuals illustrate the difficulty in categoriz-ing subjects using primarily cut-off values. Of the 29individuals not typed, 26 were children under age 7.
None of the 89 individuals (26%) with hyperlipid-emia in this pedigree had a Type I or a Type IIIelectrophoretic pattern. Among nonmembers, thedistribution of lipid phenotypes was independent ofthe subset of the pedigree in which the marriageoccurred. However, the high frequency of hyperlipi-demia (19 of 73 tested) in the total NM subset wasunexpected. Type IV was predominant. For bothadults and children, the relative frequencies of lipidphenotypes were significantly different among the P,M, and C subsets (p < 0.001). The highest frequen-cy of hyperlipidemia in both adults and children wasobserved in the C subset. Only the Type II phenotypewas observed. In the P subset, l la was the mostfrequent type of hyperlipidemia, while IV was mostfrequent in the M subset.
The adults with Types lla, lib and IV hyperlipide-mia were significantly older (6.5 years), heavier (5.1kg) and had higher blood pressure levels (11 mm Hgsystolic and 6 mm Hg diastolic) than those with nor-mal lipid phenotypes (p < 0.01). The four Type Vadults were 16 kg heavier on the average than thenormal adults and had significantly higher mean uricacid levels (6.3 vs 4.9 mg/dl). On the other hand, themeans of age, height, weight, BMI, blood pressure,glucose levels, and uric acid levels were not sig-nificantly different in normal and hyperlipidemicchildren.
The means, standard deviations, and ranges oflipids and lipoproteins are given in table 3 for thenonmembers and the children and adults separatelyfor the three subsets. The mean levels of cholesteroland LDL were significantly higher in adult memberscompared to nonmembers. There were no signifi-cant differences in the levels of lipids and lipopro-teins among the various subsets of nonmemberswho married into the pedigree.
When all members were considered, the C subsethad significantly higher levels for cholesterol, LDL,and the ratios of these with HDL compared to the Pand M subsets, even though they had the lowestmean age. The adult members of the C subset hadsignificantly higher levels of all lipids, lipoproteins,and ratios except HDL compared to adult membersof the P and M subsets (table 3). Among the threesubsets of children, the C members had significantlyhigher levels for cholesterol, LDL, cholesterol/HDLand LDL/HDL. While not statistically significant, themean triglyceride level was approximately 10 mg/dlhigher for children in the C subset compared to the Pand M subsets. The P subset children had a signifi-cantly higher mean for VLDL which could not beaccounted for by the higher mean age of children inthis subset.
Among normal adults, females had significantlyhigher mean levels of HDL compared to males (39 vs34 mg/dl, respectively). Among both adults and chil-dren with normal electrophoretic types, there wereno statistically significant differences among subsetsfor any lipid or lipoprotein levels. However, amongnormal children, those in the C subset had the high-est mean levels of cholesterol and triglycerides.
Among adult hyperlipidemics, significant differ-ences were detected between the various subsets ofthe pedigree. The C subset adult hyperlipidemicshad the highest mean levels of cholesterol (357mg/dl) LDL (268 mg/dl) and cholesterol/HDL (10.3),while the P subset hyperlipidemics had the highest
Table 2. Distribution of Electrophoretic Phenotypes and Percentage of Hyperllpldemla In the Subsets for Adults(Distribution for Children Is in Parentheses)
Electrophoretic phenotypeNormalllalibIVV
Unclassified
HyperlipidemiaTotalPercent
Number not typed
Paternal
32(52)9(17)6(1)1(0)0(0)
0(9)
16(18)33.3(22.8)
0(8)
Members
Maternal
25(75)0(0)3(0)
13(2)0(0)
4(1)
16(3)35.6(3.7)
1(18)
Codescen-dant
1(9)3(9)3(1)0(0)0(0)
0(0)
7(10)85.7(52.6)
0(0)
Paternal
281041
0
617.6
1
Nonmembers
Maternal
211153
2
1030.3
1
Codescen-dant
30120
0
350.0
0
by guest on June 30, 2018http://atvb.ahajournals.org/
Dow
nloaded from

18 ARTERIOSCLEROSIS VOL 3, No 1, JANUARY/FEBRUARY 1983
Table 3. Summary Statistics for Plasma LIplds and LIpoprotelns (mg/dl)
Cholesterol
Triglycerides
VLDL-C
LDL-C
HDL-C
C/HDL-C
LDL-C/HDL-C
Nonmembers
189±40(100-334)
73
121 ±92(35-552)
73
25±15(2-73)
72
129±33(63-231)
72
36±7(23-58)
72
5.4 ±1.2(3.5-8.5)
72
3.7±1.0(1.9-7.0)
72
Paternal>20 years
226±90(126M56)
48
89 + 47(23-247)
48
21+12(4-66)
48
169±81(83-382)
48
36±9(20-76)
48
6.6 + 3.1(3.6-18.4)
48
5.0 ±2.8(2.2-15.5)
48
Maternalss20 years
202 ±38(146-300)
45
132±83(28-360)
46
31 ±21(6-108)
45
133±29(59-206)
45
39±7(27-57)
45
5.4±1.1(3.6-8.7)
45
3.5 ±0.9(1.4-6.4)
45
Codescen-dant
2s20 years
341 ±56(212-380)
8
162±107(58-370)
8
51 ±31(20-90)
8
252 ±47(149-299)
8
38 + 11(21-55)
8
9.9±3.7(4.9-16.7)
8
7.2 ±2.4(3.5-11.4)
8
Paternal<20 years
188±64(118-344)
79
55 ±24(14-141)
79
21 ±15(2-78)
72
131 ±61(45-281)
72
36±7(19-53)
72
5.3 ±1.7(3.0-9.6)
72
3.7±1.6(1.1-7.8)
72
Maternal<20 years
154 + 22(108-214)
79
56 + 40(16-254)
81
14 + 8(1-46)
61
108 + 20(70-149)
61
35 + 6(24-59)
61
4.5 + 0.7(3.1-6.8)
61
3.1+0.7(1.8-5.1)
61
Codescen-dant
<20 years
231 ±77(120-368)
19
65±30(28-146)
19
16 ± 6(8-30)
16
181 ±73(72-299)
16
38±8(29-55)
16
6.3±2.1(3.3-9.7)
16
4.8 ±2.0(1.9-8.3)
16
Values are mean ± SD. Range is given in parentheses. VLDL-C = very low density lipoproteln cholesterol; LDL-C = lowdensity lipoprotein cholesterol; HDL-C = high density lipoprotein cholesterol.
mean for LDL/HDL (8.0). The hypertipidemic mater-nal members had mean triglyceride levels 36 mg/dlabove the mean for all hyperlipidemic adults (p <0.001). Among hyperlipidemic children, the rankingof the C, P, and M subset means were similar to thatobserved for hyperlipidemic adult members.
In summary, these data suggest that the genea-logical relationship of members to the index case(i.e., the subset) was not independent of their llpidand lipoprotein levels. While all differences were notstatistically significant, all the lipid and lipoproteinlevels were highest among C subset members. Asimilar pattern of elevated levels was seen in boththe adults and children of the C subset. Likewise, forboth adult members and children, those in the Psubset had significantly higher mean cholesterol lev-els and significantly lower mean triglyceride levelsthan those in the M subset.
The distribution of lipid and lipoprotein levelsamong subsets was associated with the percent-ages of the individuals with major clinical manifesta-tions of hyperiipidemia and atherosclerosis (table 4).For adults, the members of the pedigree differedsignificantly from nonmembers only in the percent-age of tendon xanthomas (23.8% versus 0%). Thedistribution of clinical conditions among nonmemberadults (table 4) was independent of the subset of thepedigree in which the marriage occurred. Among
adults who were members, those in the C subset hadsignificantly higher percentages of arcus comeae,xanthelasma, tendon xanthomas, CHD, and anginapectoris compared to the M and P subsets. For all themanifestations mentioned just above, the P subsetmembers had higher relative frequencies than the Msubset members. For children, only the percentagesof cigarette and alcohol use varied significantlyamong subsets. No children in the C subset reportedthat they smoked and no children in either the P or Msubsets reported alcohol use. Although not shown intable 4, hyperlipidemic adults had significantly higherpercentages of arcus corneae, xanthelasma, tendonxanthomas, CHD, angina pectoris, Ml, and use ofalcohol (25%, 11%, 32%, 29%, 27%, 7%, 25%,respectively) compared to normolipidemic adults(5%, 2%, 0%, 4%, 4%, 1%, 12%, respectively).
Discussion
Typical cases of FH with tendon xanthomas, pre-mature atherosclerosis, and cell surface LDL-recep-tor deficit may or may not exhibit hypertriglyceride-mia. Although FH Ha shares many of the clinical andbiological features of FH Mb, some differences be-
by guest on June 30, 2018http://atvb.ahajournals.org/
Dow
nloaded from

HYPERLIPIDEMIA IN A FRENCH-CANADIAN KINDRED Davignon et al. 19
Table 4. Percentage of Individuals with Major Clinical Manifestations of Hyperllpidemla,Atherosclerosis, and Risk Factors for Coronary Heart Disease
Arcus corneaeXanthelasmaTendon xanthomasCoronary heart diseaseAngina pectorisMyocardial infarctionPeripheral atherosclerosisIntermittent claudicationObesityDiabetesHypertensionSmokingAlcohol use
Nonmembers(n = 75)
10.72.70.09.39.32.74.01.3
22.71.35.3
44.620.0
Members>20 years(n = 101)
11.95.9
23.813.912.93.03.02.0
16.83.08.9
38.612.9
All
Paternal(n = 48)
12.54.2
25.014.612.56.34.24.2
14.62.18.3
35.414.6
members >20
Maternal(n = 46)
4.32.20.06.56.50.02.20.0
21.74.38.7
41.310.9
years
Codescen-dant
(n = 7)
57.142.985.757.157.10.00.00.00.00.0
14.342.914.3
tween the two have been reported2'3 and some re-searchers have considered the Mb phenotype as aseparate disease entity.18 The issue has been obfus-cated by the finding that another distinct heritabledisease, familial combined hyperlipidemia,119 canalso harbor the Mb phenotype. The index of the pedi-gree under study presented all the currently accept-ed clinical and biochemical criteria of heterozygousFH.1 We also found that he had the expected partialdeficit in LDL-receptors, as measured in survivinglymphocytes by 12SI-LDL degradation.20 The study re-ported here was initiated to establish the geneticetiology of hypertriglyceridemia in this individual.
The overall relative frequencies of the Types lla,Mb and IV in adult relatives of the index case in theentire kindred are consistent with the expectationthat one-third of the affected relatives would be ofeach type in familial combined hyperlipidemia.119
However, there are several reasons to reject the hy-pothesis that the segregation of these phenotypes inthis pedigree is consistent with familial combined hy-perlipidemia. First, data from the M and P subsetsrepresent separate lipid disorders that are not typicalof familial combined hyperlipidemia. The distributionof electrophoretic phenotypes among the progeny of33 matings in the P subset (table 5) is explained
Table 5. Segregation of Phenotypes In Nuclear Families
Type of mating
Paternal subset (n = 33)Normal x normalNormal x hypercholesterolemlcNormal x not typedHypercholesterolemic x not typedNot typed x not typedTotal
Maternal subset (n = 27)Normal x normalNormal x hypercholesterolemlcNormal x not typedNormal x unclassifiedNormal x hypertrigryceridemicHypertrlglyceridemic x hypertriglyceridemicHypertrlglyceridemic x unclassifiedHypertrlglyceridemic x not typedTotal
Number
147651
—
71628111
—
Normal
2712850
52
17378
15153
59
Hyper-cholester-
olemic
012321
18
000000000
Offspringhyper-triglyc-
eridemic
000000
001000102
Unclas-sified
024309
001000001
Nottyped
421108
304360001
by guest on June 30, 2018http://atvb.ahajournals.org/
Dow
nloaded from

20 ARTERIOSCLEROSIS VOL 3, No 1, JANUARY/FEBRUARY 1983
entirely by familial hypercholesterolemia (FH) deter-mined by a dominant gene at a single locus. A ratio of14 to 17 (hypercholesterolemic to normal) observedfor the progeny of 12 matings in which one parentwas hypercholesterolemic does not deviate signifi-cantly from the 1 to 1 ratio expected for a trait deter-mined by a dominant gene. In contrast, none of themating types in the M subset produced hypercholes-terolemic progeny (table 5). The M subset gave amarkedly different pattern of lipid phenotypes; onlytwo children had abnormal electrophoretic pheno-types (table 2). We used an analysis of the continu-ous variability of lipid levels to test for the presence ofa major segregating locus for familial hyperprebeta-lipoproteinemia (FHPB). Elston et al.21 suggest fourcriteria necessary to infer segregation at a majorlocus. One is that continuously distributed data,when considered as a random sample from somedistribution, should fit a mixture of distributions sig-nificantly better than they fit a single distribution. Thetriglyceride values for all members of the M subsetand their spouses were standardized for age, sex,and use of hormones using the Lipid Research Clin-ics population as a standard.22 Using the method ofDay,23 we found that two normal distributions fit thestandardized data significantly better than one. Thispreliminary finding is consistent with the hypothesisthat genetic variability at one locus may contribute tothe distribution of triglyceride levels.
A second reason to presume the presence of twoheritable disorders in the M and P subsets is pro-vided by a detailed examination of the codescen-dants (figure 1). If we assume: 1) that the father ofthe index case transmitted the type Ha phenotype(tendon xanthomas, a high cholesterol level (425mg/dl), and premature CHD) from the P subset to hisoffspring; 2) that the mother of the index case trans-mitted the Type IV phenotype (high triglyceride lev-els, diabetes, and a milder form of CHD) to heroffspring; and 3) that these conditions are deter-mined by two unlinked and nonepistatic heritable dis-orders, we would expect an equal number of off-spring with Type lla hyperlipidemia with tendonxanthomas, Type IV with few clinical signs of hyper-lipidemia and atherosclerosis, a mixture of lla and IV(Type Mb with severe disease), and the normal lipidphenotype. Although there was an excess of theType II phenotype (7 of 8), the types of progenyobserved are consistent with the segregation of twoseparate loci. The normal individual (III-9, figure 1)represented the combination of normal genes at thetwo loci that were transmitted from each of the singlyheterozygous parents. The Type lla individuals rep-resented the combination of a mutant gene deter-mining hypercholesterolemia and a normal gene fortriglyceride levels from the father and the combina-tion of normal genes at the two loci from the mother.The Type Mb individuals were likely the double heter-ozygotes for the two mutants, one from the fatherand one from the mother.
Even more striking than the distribution of electro-
phoretic phenotypes, were the extreme levels of thelipids and lipoproteins and the high frequency of clini-cal manifestations and atherosclerotic complicationsamong these eight adults in the C subset who wereall under age 40 when examined. Taken in combina-tion with the data from the M and P subsets thatsupport two heritable disorders, these data furthersupport the hypothesis that the adults of the C subsetrepresented the interactions between the effects of agene determining hypertriglyceridemia and the ef-fects of a gene for hypercholesterolemia. In the nextgeneration in the C subset, one-half the children ofthe index case had normal triglycerides (three FH lla,one normal) even though the index's spouse hadhypertriglyceridemia with a Type IV pattern. Amongthe nieces and nephews of the index (IV, figure 1),Phenotype lla was present in nine of the 10 affectedchildren. Since the mean age at the time of samplingwas 9.5 years (No = 18) for this generation, it isprobable that the hypertriglyceridemia was not ex-pressed and that this trait perhaps exhibits low pene-trance as previously reported in FHPB.1 It is likelythat the hypertriglyceridemia would eventually be ex-pressed in children who had plasma triglycerides inthe upper normal range either as Type IV (IV-5, fig-ure 1) or as Type lib (IV-4, the twin of IV-3). It is alsopossible that the 2-year-old IV-19 with a cholesterollevel of 194 might be eventually affected (Type lla).
These interpretations of the distribution of informa-tion among the P, M, and C subsets are based on theassumptions that the father of the index who trans-mitted the hypercholesterolemia was not hypertri-glyceridemic, that no secondary causes accountedfor the hypertriglyceridemia in the index case, andthat the diabetic trait present on the maternal side didnot account for a major part of the hypertriglyceride-mia in the index. These assumptions are supportedby a number of considerations. First, although plas-ma triglyceride levels for the father of the index (11-1,figure 1) were not available, his plasma cholesterolwas very high, he had tendon xanthomas, he died atage 57 of a myocardial infarction, and most of hisaffected biological relatives had the lla phenotype(26 of 33, 79%). Therefore, it is reasonable to as-sume that he also had FH lla. Second, the index wasnot obese and he did not consume alcohol or largeamounts of simple sugar in his diet at the time of thesampling. Thyroid, liver, and renal functions werenormal and he was not taking any drugs or hor-mones. Third, only three of the 16 hypertriglyceride-mic adults in the maternal subset had fasting glucoselevels above 115 mg/dl, the level which is regardedby the National Diabetes Group4 as the limit definingimpaired glucose tolerance. Two of these individualshad values below 125 mg/dl and the third (an aunt ofthe index) was a possible diabetic with a fasting glu-cose of 158 mg/dl. Because the 59-year-old motherof the index had an adult-onset diabetes requiringinsulin, the index case could have inherited the dia-betic trait. This is unlikely because his fasting glyce-mia level was normal. Although he had an abnormal
by guest on June 30, 2018http://atvb.ahajournals.org/
Dow
nloaded from

HYPERLIPIDEMIA IN A FRENCH-CANADIAN KINDRED Davignon et al. 21
glucose tolerance, his normal fasting blood sugar inthe absence of excess body weight was not likely tobe the source of hypertriglyceridemia of the magni-tude noted after a 12-hour fast.
Indeed, it has been shown that plasma free fattyacids, the substrate for liver synthesis of triglycer-ides, are not increased in subjects with glucose intol-erance unless they are obese.24 Furthermore, nodeficit in plasma or adipose tissue-lipoprotein lipaseactivity (the major catabolic enzyme for plasma tri-glycerides) is found in lean individuals until plasmaglucose reaches or exceeds 150 mg/dl.25 This is notto say that glucose intolerance could not contributeto enhancing an inherited defect in triglyceride me-tabolism or increase the sensitivity of plasma triglyc-eride levels to dietary carbohydrates.2627 The highprevalence of abnormal glucose tolerance in pa-tients ascertained for hypertriglyceridemia is well es-tablished28'M and was to be expected on the mater-nal side where FHPB is present. On the other hand, ithas been shown that the prevalence of diabetes isthe same among normolipidemic and hypertriglyceri-demic first-degree relatives of individuals with famil-ial hypertriglyceridemia.30 This suggests that diabe-tes and hypertriglyceridemia have separateetiologies, although they may coexist in about 35%of subjects with familial hypertriglyceridemia.1130 Inconclusion, the mild carbohydrate intolerance in theindex case may have contributed in part, but notwholly, to his hypertriglyceridemia. There is no wayto determine whether it could have contributed toenhancing the severity of the cardiovascular abnor-malities in the codescendants by means other thanincreased plasma triglycerides (i.e., basement mem-brane changes, effect on collagen metabolism, orother mechanisms).
In conclusion, the distribution of lipoprotein pheno-types, as well as the concentrations of plasma lipidsand lipoproteins in the various subsets, corroboratesthe fact that there is aggregation specifically for hy-percholesterolemia (Type II, elevated LDL) on thepaternal side and aggregation specifically for hyper-prebetalipoproteinemia (Type IV, elevated VLDL) onthe maternal side. Adults with hypercholesterolemiain both the P and C subsets have children with ele-vated cholesterol levels. Matings of normals with hy-percholesterolemics in the P subset did not give riseto hypertriglyceridemic children, and matings of nor-mals with hypertriglyceridemics in the M subset didnot give rise to hypercholesterolemic children. Final-ly, the index case had an LDL receptor site deficien-cy. These observations all suggest that the distribu-tion of phenotypes in this pedigree is not consistentwith the criteria currently used to define familial com-bined hyperlipidemia.1'19 The nonrandom distribu-tion of lipid and lipoprotein measures and of clinicalmanifestations among the subsets of this pedigreeare more consistent, instead, with a hypothesis thatthe Mb phenotype in the index resulted from the com-bined inheritance of FH from the father and FHPBfrom the mother.
AcknowledgmentsThe generous collaboration of Christine Bertagna, Remi Collin,
Emmett Corbin, Marcel Fauconnier, Michel Langelier, Michel Le-llevre, Jacques LeLorler, Maurice A. Mishkel, Martine Ortin-Qeorge, Lewis D. Page, Elisabeth Reichel, and Fernand Robergeis gratefully acknowledged. The invaluable participation of DeniseBrossard, Use Demers, Use Dube, Gabrielle Fullum, Mireille Oliv-ier, and Suzanne Quidoz is deeply appreciated as well as thesecretarial help of Daniele Amaud, Rejeanne Ouellet, and AnnePreston and the technical assistance of Lucie Boulet, Diane Gir-oux, Murlelle Paquette, Nicole Patard, Stephen Rothwell, andMichel Tremblay.
References1. Fredrickson DS, Goldstein JL, Brown MS. The familial hy-
perlipoproteinemias. In: Stanbury JB, Wyngaarden JB, Fred-rickson DS, eds. Metabolic basis of inherited disease. NewYork: McGraw-Hill, 1978;604-655
2. Davignon J, Aubry F, Noel F, Laplerre Y, Lafortune M.Heterogeneity of familial hyperiipoprotelnemia type II on thebasis of fasting plasma triglyceride/cholesterol ratio and plas-ma cholesterol response to chlorophenoxyisobutyrate. Re-vue Can Blol 1971;30:307-318
3. Plchardo R, Boulet L, Davignon J. Pharmacoklnetlcs ofclofibrate in familial hypercholesterolemia. Atherosclerosis1977;26:573-582
4. National Diabetes Group. Classification and diagnosis ofdiabetes mellitus and other categories of glucose intolerance.Diabetes 1979;28:1039-1057
5. Arsenautt B. Histoire des Acadiens. Ottawa:Lemeac, 19786. Tanguay C. Dfctionnaire genealogique des families Canad-
lennes. Montreal:Elysee, 19757. Hatch FT, Lees RS. Practical methods for plasma lipoprotein
analysis. In: Paoletti R, Krltchevsky D, eds. Advances in lipidresearch, New York:Academic Press, 1968;6:16-18
8. Lees RS, Hatch FT. Sharper separation of lipoprotein spe-cies by paper electrophoresis in albumin-containing buffer. JLab Clin Med 1963:61:518-528
9. Block WD, Jarrett KJ Jr, Levlne JB. An improved automat-ed determination of serum total cholesterol with a single colorreagent. Clln Chem 1966;12:681-689
10. Laurell SA. A method for routine determination of plasmatriglycerides. Scand J Clin Invest 19€6;18:668-672
11. Kraml N, Cosyns L A semi-automated determination of se-rum triglycerides. Clin Biochem 1969;2:373-380
12. Glucose Procedure N-26. In: Autoanalyzer manual. Chaun-cey, New York: Technlcon Instruments Corporation, 1965
13. Uric Acid Procedure N-13b. In: Autoanalyzer manual.Chauncey, New York: Technicon Instruments Corporation,1965
14. Fredrickson DS, Levy Rl, Lees RS. Fat transport in lipopro-teins — An integrated approach to mechanisms and disor-ders. New Engl J Med 1967;276:32-44, 94-103, 148-156,215-226, 273-281
15. Kwtterovlch PP. Pediatric aspects of hyperlipoproteinemia.In: Rifkind BM, Levy Rl, eds. Hypeiiipidemia, diagnosis andtherapy. New York: Grune & Stratton, 1977;249-279
16. Mood AA, Grayblll FA. Introduction to the theory of statistics.New York: McGraw-Hill, 1963
17. Conover WJ. Practical nonparametrlc statistics. New York:John Wiley and Sons, 1971
18. Brown HB, Lewis LA, Page IH. Mixed hyperlipidemia, a sixthtype of hyperlipoproteinemia. Atherosclerosis 1973;17:181-196
19. Goldstein JL, Hazzard WR, Schrott HG, Blerman EL, Mo-tulsky AG. Hyperlipidemia in coronary heart disease. II- Ge-netic analysis of lipid levels in 176 families and delineation ofa new Inherited disorder, combined hyperiipidemla. J ClinInvest 1973;52:1544-1568
by guest on June 30, 2018http://atvb.ahajournals.org/
Dow
nloaded from

22 ARTERIOSCLEROSIS VOL 3, No 1, JANUARY/FEBRUARY 1983
20. Bilhelmer DW, Ho YK, Brown MS, Anderson RGW, Gold-stein JL. Genetics of the low density lipoprotein receptor. JClin Invest 1978;61:678-694
21. Elston RC, Namboodirl KK, Kaplan EB. Resolution of ma-jor loci for quantitative traits. In: Morton NE, Chung CS, eds.Genetic epidemiology. New York: Academic Press, 1978;223-240
22. The Lipld Research Clinics Program. Population studiesdata book. The prevalence study. Bethesda, Maryland: U.S.Department of Health, Education and Welfare, 1980;1 DHEWpublication no. (NIH) 80-1527
23. Day NE. Estimating the components of a mixture of normaldistributions. Biometrika 1969;56:463-474
24. Bagdade JD, Porte D, Blerman EL. The interaction of diabe-tes and obesity on the regulation of fat mobilization in man.Diabetes 1969;18:759-772
25. Brunzell JD, Porte D Jr, Bierman EL. Abnormal lipoprotein-
lipase-mediated plasma triglyceride removal in untreated dia-betes mellitus associated with hypertriglyceridemia. Metabo-lism 1979;28:901-907
26. Bierman EL, Porte D. Carbohydrate intolerance and lipemia.Ann Int Med 1968:68:926-933
27. Gries FA, Koschinsky T, Berchtold P. Obesity, diabetesand hyperlipoproteinemia. Atheroscler Rev 1979;4:71-95
28. Albrlnk MJ, Davidson PC. Impaired glucose tolerance inpatients with hypertriglyceridemia. J Lab Clin Med 1966;67:573-584
29. Glueck CJ, Levy Rl, Fredrlckson DS. Immunoreactive insu-lin, glucose tolerance and carbohydrate inducibility in types II,III, IV and V hyperlipoproteinemia. Diabetes 1969;18:739-747
30. Brunzell JD, Hazzard WL, Motulsky AG, Bierman EL. Evi-dence for diabetes mellitus and genetic forms of hypertriglyc-eridemia as independent entities. Metabolism 1975;24:1115-1121
Index Terms: Familial hypercholesterolemia • familial hyperprebetalipoproteinemia • plasma lipoproteinsxanthomas • atherosclerosis • field survey • genetics • cholesterol • triglycerides • diabetes
by guest on June 30, 2018http://atvb.ahajournals.org/
Dow
nloaded from

J Davignon, S Lussier-Cacan, A Gattereau, P P Moll and C F SingInteraction of two lipid disorders in a large French-Canadian kindred.
Print ISSN: 1079-5642. Online ISSN: 1524-4636 Copyright © 1983 American Heart Association, Inc. All rights reserved.
Greenville Avenue, Dallas, TX 75231is published by the American Heart Association, 7272Arteriosclerosis, Thrombosis, and Vascular Biology
doi: 10.1161/01.ATV.3.1.131983;3:13-22Arterioscler Thromb Vasc Biol.
http://atvb.ahajournals.org/content/3/1/13World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://atvb.ahajournals.org//subscriptions/
online at: isArteriosclerosis, Thrombosis, and Vascular Biology Information about subscribing to Subscriptions:
http://www.lww.com/reprints
Information about reprints can be found online at: Reprints:
document. Question and AnswerPermissions and Rightspage under Services. Further information about this process is available in the
which permission is being requested is located, click Request Permissions in the middle column of the Webthe Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service ofArteriosclerosis, Thrombosis, and Vascular Biologypublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on June 30, 2018http://atvb.ahajournals.org/
Dow
nloaded from