intensive risk factors management in diabetic subjects claramunt.pdf · intensive. risk factors ....
TRANSCRIPT

Intensive risk factors management in diabetic subjects
Yes: M. Khattab (Egypt) No: X. Cos Claramunt (Spain)
Intensive risk factors management in diabetic subjects
Francesc Xavier Cos Claramunt EAP Sant Martí de Provençals. SAP Litoral. Barcelona. ICS Grup d’Estudi de la Diabetis a l’Atenció Primària de Salut (RedGedapS) Executive member of Primary Care Diabetes Europe
Intensive risk factors management in diabetic subjects

Intensive risk factors management in diabetic subjects
Intensive risk factors management in diabetic subjects
YES / NO NO for all !

Intensive risk factors management in diabetic subjects
Duality of Interest
• XC: honoraria clinical trials, consultant and advisory board Boehringer Ingelheim, Lilly, MSD, Abbott, Novartis, Novo Nordisk, Sanofi-Aventis y Astra-Zeneca.

Intensive risk factors management in diabetic subjects
Agenda
Diabetes trials “real life” Explanations & Challenges Guidelines/recomendations Take-home messages

Intensive risk factors management in diabetic subjects
years
Postprandial glucose
Fasting glucose
0
100
200
Insulin Risk of diabetes
Impaired islet cell function
Insulin resistance
–10 0 10 15 20 25 30 5 –5
Diabetes
10 15 20
5
Glu
cose
mm
ol/l
Prop
ortio
nal a
mou
nt o
f ns
ulin
in in
rela
tion
to
norm
al (%
)
Pre diabetes (IFG / IGT) NGT
IFG: impaired fasting glucose; IGT: impaired glucose tolerance Adapted from International Diabetes Center. Type 2 Diabetes BASICS. Minneapolis, Minn: International Diabetes Center; 2000.
Intensive risk factors management in diabetic subjects
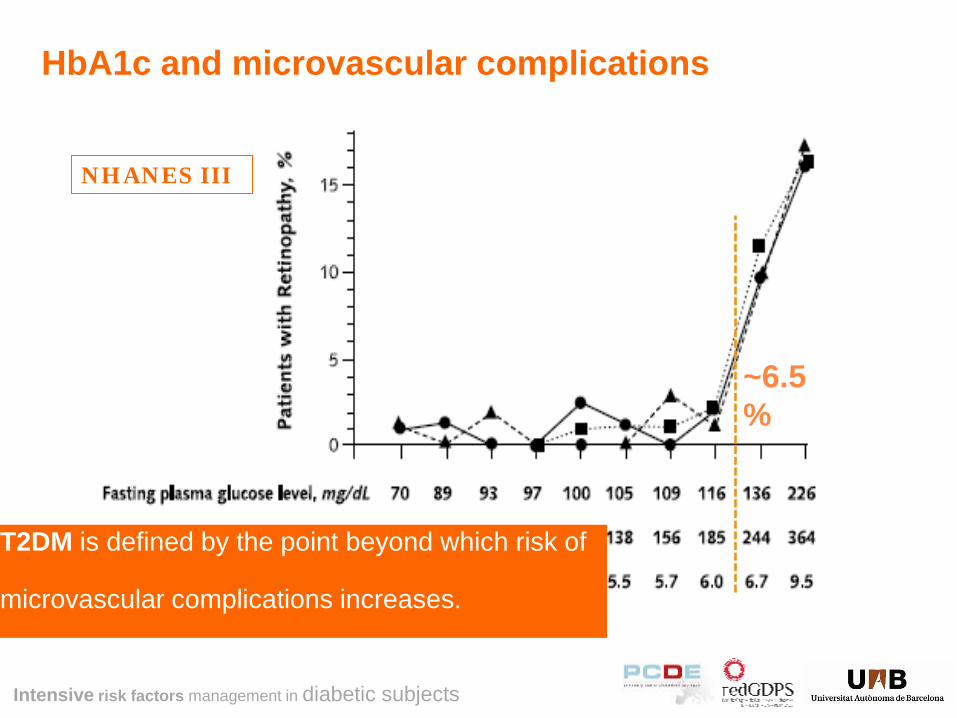
HbA1c and microvascular complications
NHANES III
~6.5%
T2DM is defined by the point beyond which risk of
microvascular complications increases.
Intensive risk factors management in diabetic subjects
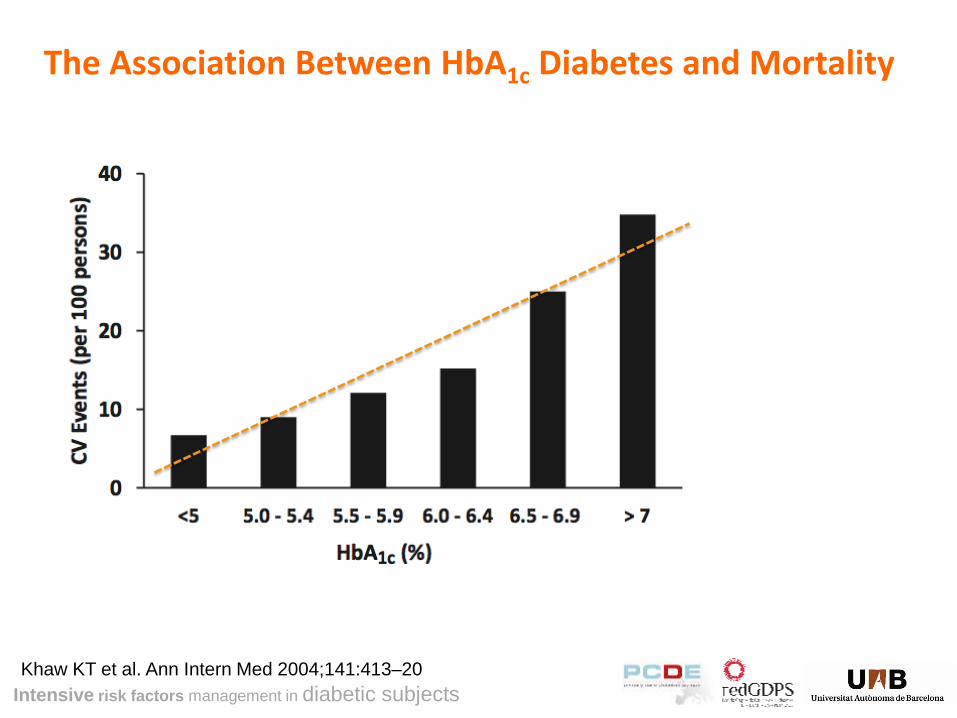
Khaw KT et al. Ann Intern Med 2004;141:413–20
The Association Between HbA1c Diabetes and Mortality

Intensive risk factors management in diabetic subjects
Glucose Lowering and CVD trials
Yrs from Dx 0 5 -10 -5 10 15
ACCORD
VADT
Eye, Kidney, Nerve Disease
CVD
IFG &/or IGT Type 2 Diabetes (T2DM) High
Dysglycemia - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
ADVANCE
UKPDS

Intensive risk factors management in diabetic subjects
UKPDS randomized years
0
6
7
8
9
0 5 10 15
Conventional
Intensive
6.2% = upper limit of normal range Med
ian
HbA
1C (%
) UKPDS Intensive control reduces complications in type 2 diabetes
–30
–25
–20
–15
–10
–5
0
Rel
ativ
e ris
k re
duct
ion
(%)
12%
25%
16%
6%
P = 0.029
P = 0.0099
P = 0.052
P = 0.44
Lancet 1998; 352:837–853.

Intensive risk factors management in diabetic subjects
–30
–25
–20
–15
–10
–5
0
Rel
ativ
e ris
k re
duct
ion
(%)
9%
24%
15% 13% P = 0.040
P = 0.001
P = 0.014 P = 0.007
UKPDS Long-term follow-up and legacy effect
10 9 8 7 6
0 5 10 15 5 10 1977 1997 2007 Years from randomization
UKPDS Active
Conventional
Intensive
Intervention ends UKPDS
Follow-up
Med
ian
HbA
1c (%
)
Biochemical data no longer collected

Intensive risk factors management in diabetic subjects
Glycemic control and CVD outcome
HbA
1c %
7
7.5
8
8.5
9
ACCORD 10.251
ADVANCE 11.140
VADT 1.791
UKPDS 3.867
STENO-2 160
Intervention studies in Type 2 Diabetes
Age 62y DM 10y
Age 66y DM 8y
Age 60y DM 12y
Age 54y DM 0y
Age 55y DM 6y

Intensive risk factors management in diabetic subjects
Meta-analysis: impact of intensive glucose control on coronary heart disease* events
Ray KK, et al. Lancet 2009; 373:1765–1772.
Intensive treatment/standard treatment
Odds ratio (95% CI)
Odds ratio (95% CI)
Participants Events
UKPDS 3,071/1549 426/259 0.75 (0.54–1.04)
PROactive 2,605/2633 164/202 0.81 (0.65–1.00)
ADVANCE 5,571/5,569 310/337 0.92 (0.78–1.07)
VADT 892/899 77/90 0.85 (0.62–1.17)
ACCORD 5,128/5123 205/248 0.82 (0.68–0.99)
Overall 17,267/15,773 1,182/1,136 0.85 (0.77–0.93)
0.4 0.6 0.8 1.0 1.2 1.4 1.6 1.8 2.0
Intensive treatment better Standard treatment better
*Included non-fatal myocardial infarction and death from all cardiac mortality.

Intensive risk factors management in diabetic subjects
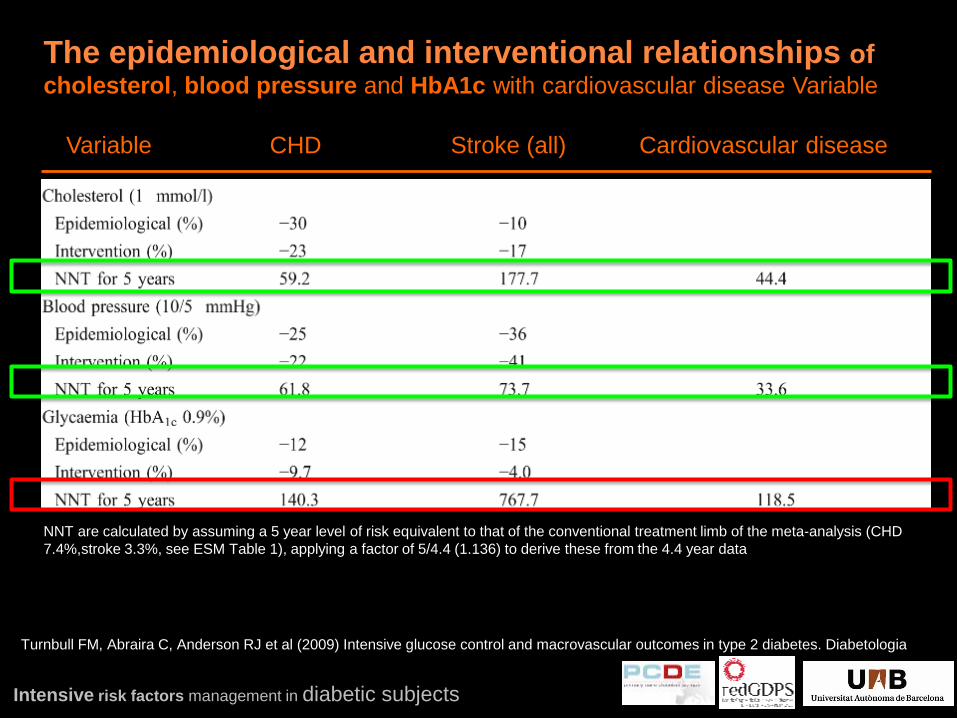
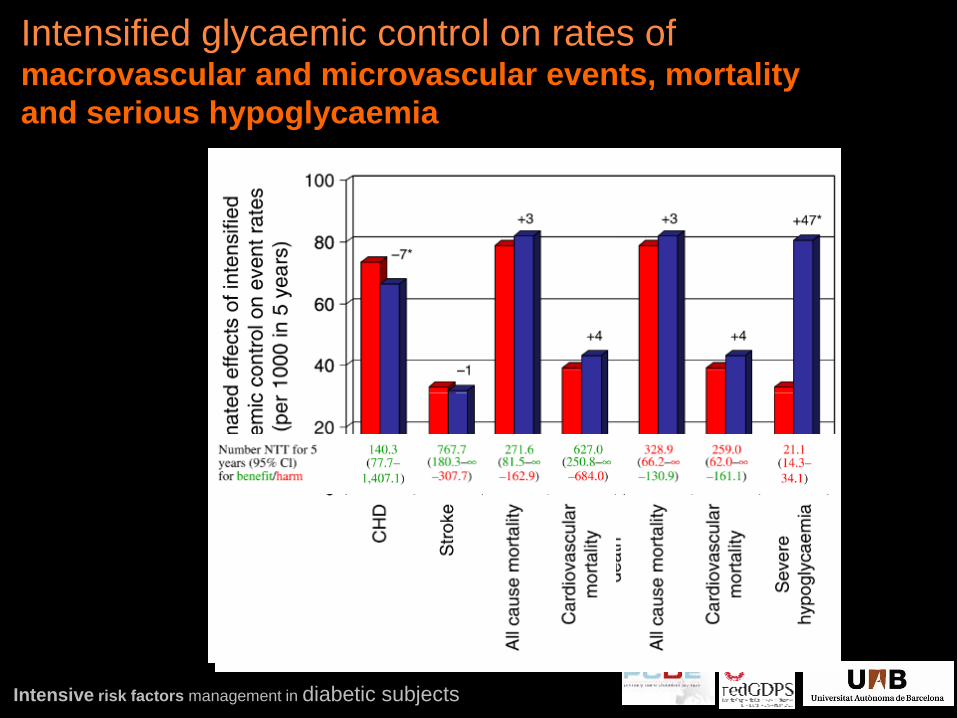
Variable CHD Stroke (all) Cardiovascular disease
The epidemiological and interventional relationships of cholesterol, blood pressure and HbA1c with cardiovascular disease
NNT are calculated by assuming a 5 year level of risk equivalent to that of the conventional treatment limb of the meta-analysis (CHD 7.4%,stroke 3.3%, see ESM Table 1), applying a factor of 5/4.4 (1.136) to derive these from the 4.4 year data
Turnbull FM, Abraira C, Anderson RJ et al (2009) Intensive glucose control and macrovascular outcomes in type 2 diabetes. Diabetologia
Intensive risk factors management in diabetic subjects
Variable CHD Stroke (all) Cardiovascular disease
The epidemiological and interventional relationships of cholesterol, blood pressure and HbA1c with cardiovascular disease Variable
NNT are calculated by assuming a 5 year level of risk equivalent to that of the conventional treatment limb of the meta-analysis (CHD 7.4%,stroke 3.3%, see ESM Table 1), applying a factor of 5/4.4 (1.136) to derive these from the 4.4 year data
Turnbull FM, Abraira C, Anderson RJ et al (2009) Intensive glucose control and macrovascular outcomes in type 2 diabetes. Diabetologia
Intensive risk factors management in diabetic subjects
Intensified glycaemic control on rates of macrovascular and microvascular events, mortality and serious hypoglycaemia

Intensive risk factors management in diabetic subjects
CHD Stroke
Intensified glycaemic control on rates of macrovascular and microvascular events, mortality and serious hypoglycaemia
Turnbull FM, Abraira C, Anderson RJ et al (2009) Intensive glucose control and macrovascular outcomes in type 2 diabetes. Diabetologia

Intensive risk factors management in diabetic subjects
CDC Diabetes Cost-effectiveness Group (2002) Cost-effectiveness of intensive glycemic control, intensified hypertension control, and serum cholesterol level reduction in type 2 diabetes. JAMA 287:2542–2551
The costs (per QALY based on UKPDS data and expressed in 1,997 US$) Ex: 65-year-old new-onset patient $154,376 for decreasing A1c about 8% to 7% $43,331 for cholesterol lowering –$413 for blood pressure lowering Glucose control Aged 75- 84 years rise to $401,883 Aged over 84 years $2.1 million; Blood pressure control is cost-saving at every age below 85 years

Intensive risk factors management in diabetic subjects
Despite advances in treatment, a significant proportion of patients with Type 2 diabetes still fail to reach target HbA1c levels
0102030405060708090
100
HbA1c checkedMet HbA1c target
Stone MA et al. Diabetes Care. 2013 April 23.
Per
cent
GUIDANCE Study 7,597 T2DM patients Gap exists between checking HbA1c and achieving target HbA1c <7%
HbA1c checked Met HbA1c target

Intensive risk factors management in diabetic subjects
Vinagre et al. Diabetes Care 2012;35.

Intensive risk factors management in diabetic subjects
Challenges associated with achieving optimal glycaemic goals
6,5
7,0
7,5
8,0
8,5
9,0
2001 2002 2003 2004 2005 2006 2007
3,5
4,0
4,5
5,0
5,5
6,0
2001 2002 2003 2004 2005 2006 2007
Type 1 diabetes
Type 2 diabetes + insulin
Year Year
Mea
n H
bA1c
(%)
Mea
n Tc
hol (
mm
ol/l
)
In patients with type 1 diabetes or type 2 diabetes on insulin, there was a 0.1% relative improvement in HbA1c vs. improvements in total cholesterol of 15% and
29%, respectively between 2001 and 2007
Currie et al. Diabetic Medicine 2010; 27:938-948

Intensive risk factors management in diabetic subjects
Comorbidity of top 10 common conditions
Guthrie B et al. BMJ 2012;345:e6341

Intensive risk factors management in diabetic subjects
Elderly patients
7
6
5
4
3
2
1
0 0 40 50 70 80 90 60
Age (yr)
Year
s of
Life
Los
t
Men 7
6
5
4
3
2
1
0 0 40 50 70 80 90 60
Age (yr)
Women
Death from unknown causes Noncancer, nonvascular deaths Cancer deaths Vascular deaths
ERFC (Emerging Risk Factor Collaboration). NEJM 2011;364:829-841.
Intensive risk factors management in diabetic subjects
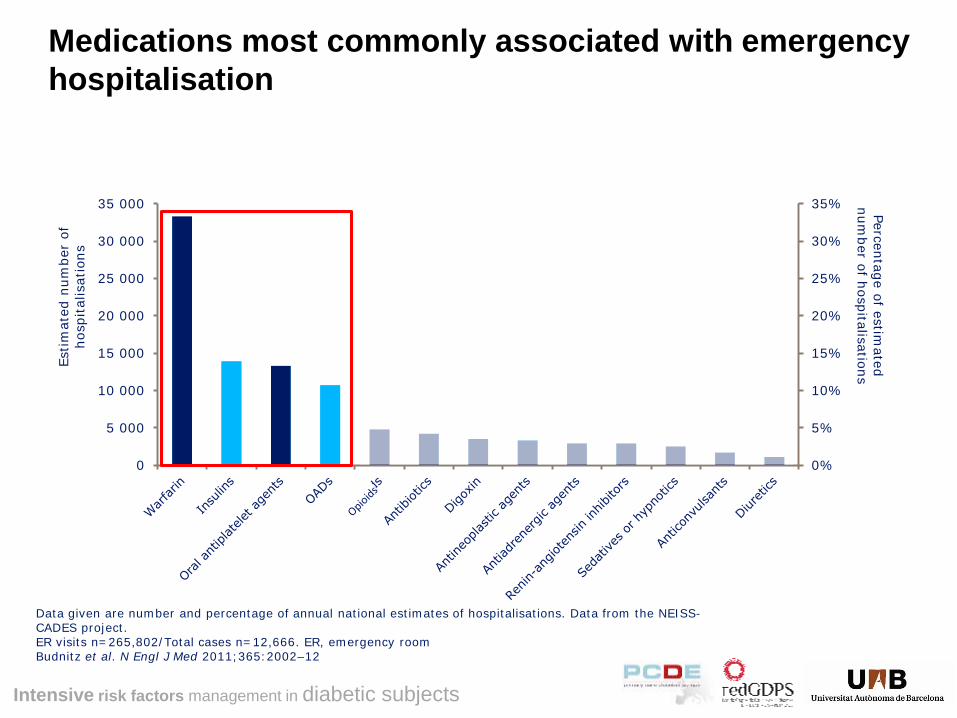
Medications most commonly associated with emergency hospitalisation
0%
5%
10%
15%
20%
25%
30%
35%
0
5 000
10 000
15 000
20 000
25 000
30 000
35 000 Percentage of estimated
number of hospitalisations
Estim
ated
num
ber
of
hosp
ital
isat
ions
Data given are number and percentage of annual national estimates of hospitalisations. Data from the NEISS-CADES project. ER visits n=265,802/Total cases n=12,666. ER, emergency room Budnitz et al. N Engl J Med 2011;365:2002–12
Intensive risk factors management in diabetic subjects
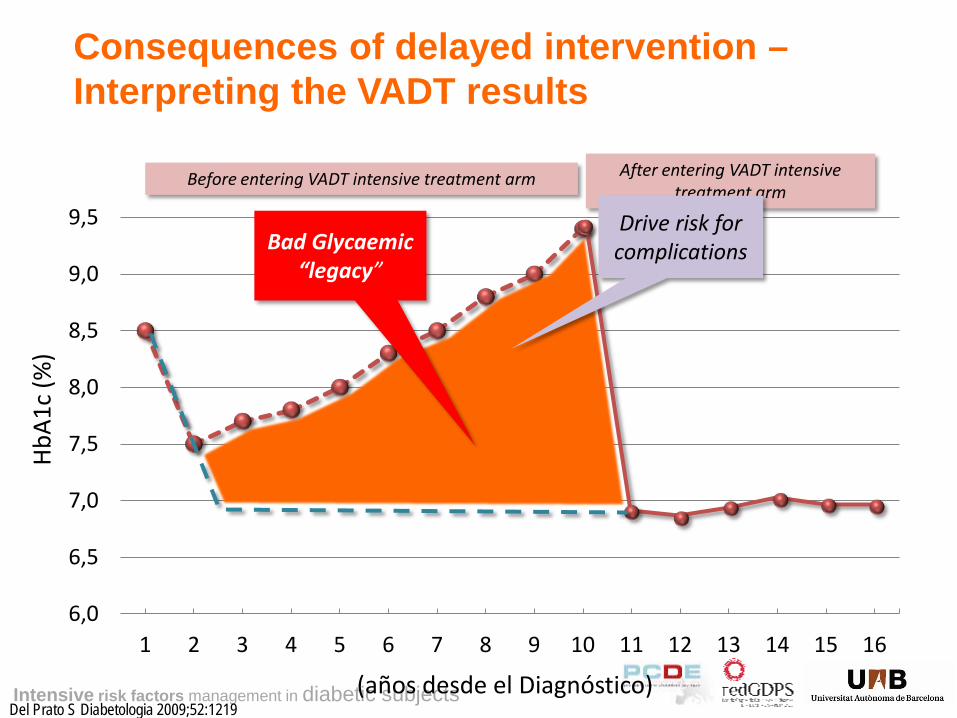
Consequences of delayed intervention – Interpreting the VADT results
6,0
6,5
7,0
7,5
8,0
8,5
9,0
9,5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
(años desde el Diagnóstico)
HbA1
c (%
)
Bad Glycaemic “legacy”
Del Prato S Diabetologia 2009;52:1219
Before entering VADT intensive treatment arm After entering VADT intensive treatment arm
Drive risk for complications
Intensive risk factors management in diabetic subjects
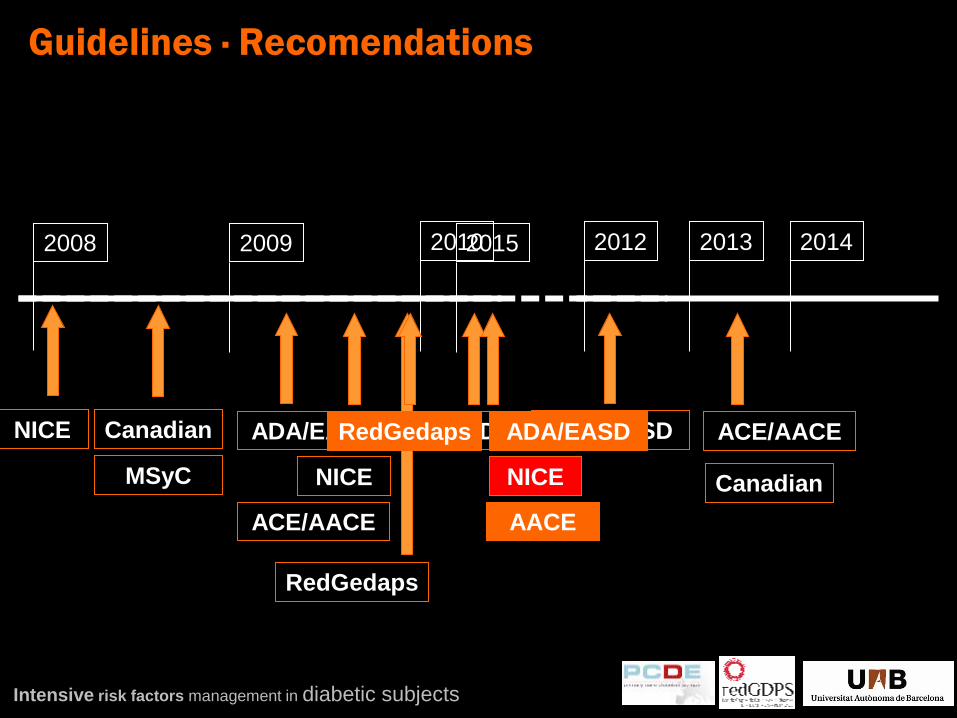
2008 2009
NICE Canadian ADA/EASD
Guias
RedGedaps
MSyC
2010
NICE
SED
ACE/AACE
2012
ADA/EASD
2013
ACE/AACE
Canadian
2014 2015
RedGedaps ADA/EASD
NICE
Guidelines · Recomendations
AACE

Intensive risk factors management in diabetic subjects
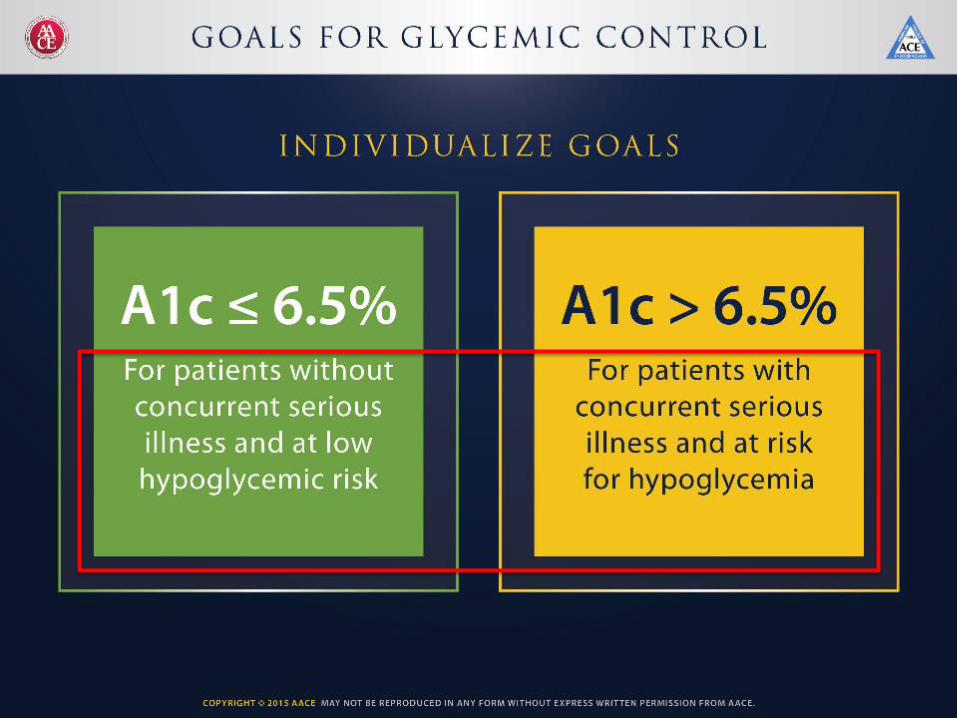
HbA1c targets generally 6.5–7% when safe and appropriate
ADA/EASD HbA1c < 7%
IDF (Europe)
HbA1c ≤ 6.5%
CDA (Canada)
HbA1c ≤ 7%
NICE (UK)
HbA1c 6.5%/7.5%
AACE (US)
HbA1c ≤ 6.5% ALAD (Latin America) HbA1c < 6–7%
APPG (Asia-Pacific)
HbA1c ≤ 6.5%
Australia
HbA1c ≤ 7%
ADA. Diabetes Care 2015; 32(Suppl 1):S13–S61; Endocr Pract. 2015;21: In Press.IDF. Global guideline for type 2 diabetes, IDF 2012. Available at: http://www.idf.org/sites/default/files/IDF-Guideline-for-Type-2-Diabetes.pdf JBS2. Heart 2005; 91(Suppl. V):1–52. European Diabetes Policy Group.
Diabet Med 1999; 16:716–730. CDA. Can J Diabetes 2008; 32(Suppl. 1):S1–S201. NICE. 2009. Available at: http://www.nice.org.uk/nicemedia/pdf/CG87ShortGuideline.pdf; ALAD. Rev Assoc Lat Diab 2000; Suppl. 1. Asian-Pacific Policy Group. Practical Targets and Treatments (3rd Edn). Available at: http://www.idf.org/webdata/docs/T2D_practical_tt.pdf. NSW Health Department. The Principles of Diabetes Care
and Guidelines for the Clinical Management of Diabetes Mellitus in Adults. NSW Health Department 1996.
Joint British Societies (JBS 2) HbA1c < 6.5%
Intensive risk factors management in diabetic subjects
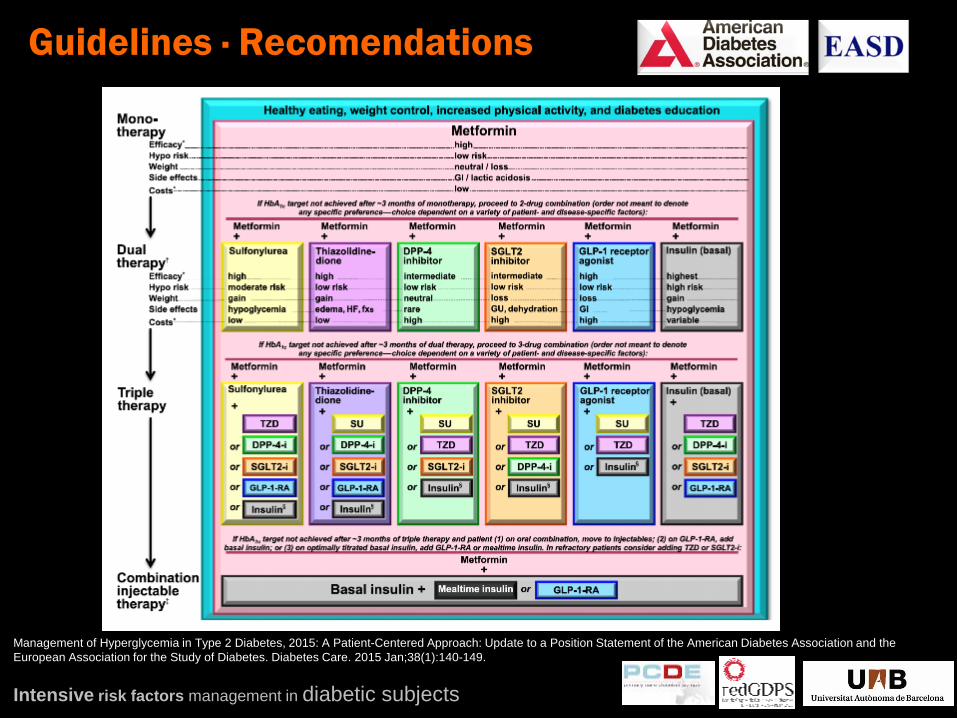
Management of Hyperglycemia in Type 2 Diabetes, 2015: A Patient-Centered Approach: Update to a Position Statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2015 Jan;38(1):140-149.
Guidelines · Recomendations

Intensive risk factors management in diabetic subjects
Based on an original figure by Ismail-Beigi et al. Management of Hyperglycemia in Type 2 Diabetes, 2015: A Patient-Centered Approach: Update to a Position Statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2015 Jan;38(1):140-149.
Guidelines · Recomendations


Intensive risk factors management in diabetic subjects
At diagnosis Treatment review Older patients
Clear guidance1
• Diet and exercise plan
• Metformin given • Avoid diabetes
complications
Complications arise1-3
• Complications such as CVD or renal impairment may become more frequent
• More individualised approach to treatment required
QoL becomes one of the most important considerations4
Management of T2D Becomes More Complex Over Time
Disease progression
1,2. Adapted from National Institute for Health and Clinical Excellence. Clinical Guideline 87. Type 2 diabetes – newer agents (a partial update of CG66): quick reference guide. NICE clinical guideline 66: Type 2 Diabetes Management. Available at: http://www.nice.org.uk/nicemedia/pdf/CG66NICEGuideline.pdf (accessed November 2012). 3. Go AS, et al. N Engl J Med. 2004;351:1296–1305; 4. Morley JE. Diabet Med. 1998;15 (Suppl. 4): S41–6.

Intensive risk factors management in diabetic subjects

Intensive risk factors management in diabetic subjects

Comparison of study populations
Lixisenatide ELIXA
Within 180 days of ACS
Alogliptin EXAMINE
Within 15–90 days of ACS
Aleglitazar ALECARDIO
Enrolled 2–6 wks after ACS; also other CVDs/RFs needed
Empagliflozin EMPA-REG OUTCOME
Enrolled >2 months after ACS, UA, PCI, stroke, PAD
Aleglitazar ALEPREVENT
≥40 y with prior MI or stroke ≥3 months OR ≥55 y and evidence of CVD
Sitagliptin TECOS
Pre-existing CVD
Linagliptin CAROLINA
CVD OR end-organ damage OR age ≥70 y OR ≥2 RFs
Saxagliptin SAVOR-TIMI 53
Established CVD or RFs
Liraglutide LEADER
≥50 y + CVD, cerebrovascular disease or PVD or CHF or CRF OR ≥60 y and RFs
Dulaglutide REWIND
≥50 y + established disease OR ≥55 y + subclinical disease
OR ≥60 y + ≥2 RFs
Exenatide QW EXSCEL With CVD
Dapagliflozin DECLARE-TIMI 58 High risk for CVD
Recent ACS Established disease DM with Risk Factors Post-ACS (<6 m)
Lessening risk
39
Semaglutide SUSTAIN 6
≥50 y + established disease OR ≥60 y + subclinical disease
Canagliflozin CANVAS/CANVAS-R
≥30 y and documented CVD OR ≥50 y and ≥2 RFs
Insulin degludec DEVOTE
≥50 y + CVD or renal disease OR ≥60 y and RFs
Linagliptin CARMELINA
Albuminuria + CVD ± impaired renal function
Ertugliflozin NCT01986881 Established disease

Intensive risk factors management in diabetic subjects
• Hyperglycaemia is a substantially weaker risk factor for CVD than
cholesterol or blood pressure.
• Good glucose control beneficial on microvascular complications,
cataracts and neuropathy, but the added benefits of an HbA1c of 7%,
as against 8%, diminish with age and life expectancy.
• Little attention to the unwanted effects of intensified therapy, and its
low utility in those with established complications or a limited life
expectancy.
• Challenge to translate RCT results on “real life” patients
• INDIVIALIZED approach in new Recommendation and GL
Take-home message

Intensive risk factors management in diabetic subjects
• Hyperglycaemia is a substantially weaker risk factor for CVD than
cholesterol or blood pressure.
• Good glucose control beneficial on microvascular complications,
cataracts and neuropathy, but the added benefits of an HbA1c of 7%,
as against 8%, diminish with age and life expectancy.
• Little attention to the unwanted effects of intensified therapy, and its
low utility in those with established complications or a limited life
expectancy.
• Challenge to translate RCT results on “real life” patients
• INDIVIALIZED approach in new Recommendation and GL
Take-home message
Intensive risk factors management in diabetic subjects
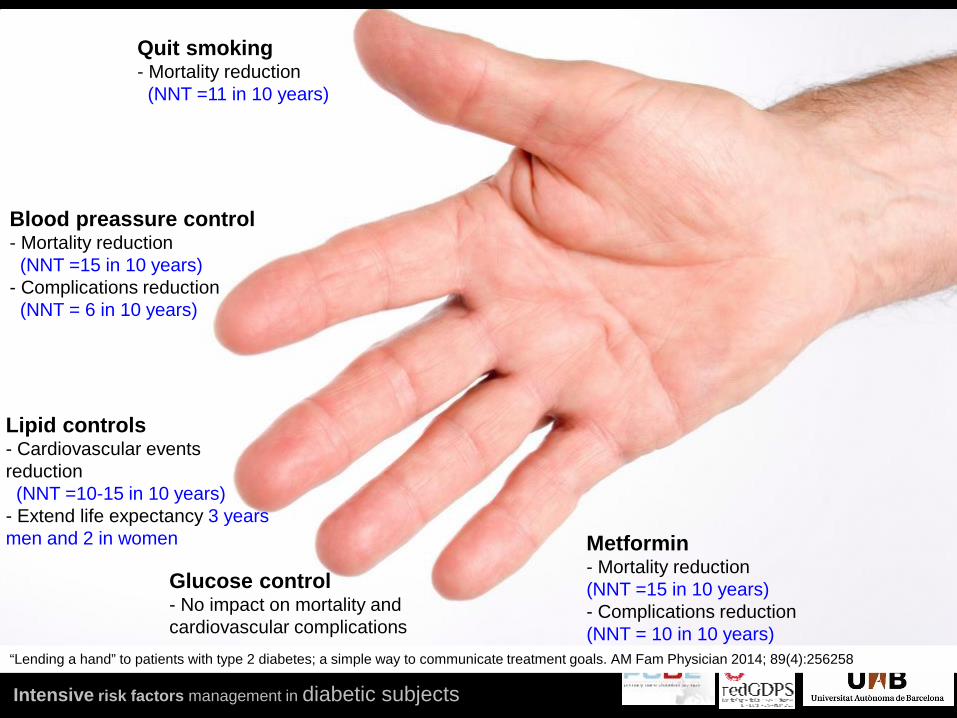
“Lending a hand” to patients with type 2 diabetes; a simple way to communicate treatment goals. AM Fam Physician 2014; 89(4):256258
Quit smoking - Mortality reduction (NNT =11 in 10 years)
Glucose control - No impact on mortality and cardiovascular complications
Blood preassure control - Mortality reduction (NNT =15 in 10 years) - Complications reduction (NNT = 6 in 10 years)
Metformin - Mortality reduction (NNT =15 in 10 years) - Complications reduction (NNT = 10 in 10 years)
Lipid controls - Cardiovascular events reduction (NNT =10-15 in 10 years) - Extend life expectancy 3 years men and 2 in women

Intensive risk factors management in diabetic subjects
@Xaviercos Thanks