integrative treatments in cancer patients: case … · integrative treatments in cancer patients:...
TRANSCRIPT

INTEGRATIVE TREATMENTS IN CANCER PATIENTS: CASE STUDIES
Massimo Bonucci M.D.
first ISS-ARTOI CONFERENCE oN INTEGRATIVE oncology November 6/7 - 2013 Rome
President A.R.T.O.I.Chief of surgical pathology department
And Oncology outpatientSan feliciano hospital - rome

INTEGRATIVE ONCOLOGY IN ITALY
Massimo Bonucci M.D.
ITALIAN –ISRAELI-US WORKSHOP CLINICAL oncology November 8-2013 Rome
President A.R.T.O.I.Chief of surgical pathology department
Oncology outpatientSan feliciano hospital - rome
In Italy In Italy we do not have public facilities where you can practice the Integrated Oncology. There are two realities hospital for Integrative Medicine in Italy: 1 - Hospital of Pitigliano in Tuscany 2 - Hospital of Merano in South TyrolIn both structures are practiced complementary therapies such as acupuncture, homeopathy, osteopathy, shiatsu massage and other practices to reduce pain, fatigueBut in none of these structures is administered antitumor therapy

In Italy In some Regions as Marche, Friuli
Venezia Giulia, Umbria, Emilia Romagna, were made proposals by law for the assessment of the use of Complementary Medicine.
In this last year through the
collaboration of some colleagues in the Public Facilities are going to
start the assessments for integrative observational studies.

In Italy
In some Private Hospital instead you can take advantage of
integrative treatments: chemotherapy, homeopathy,
herbal medicine, hyperthermia and other treatments.
Often, however, patients are treated with chemotherapy in a Public Hospital and then arriving
in the private practices of physicians who practice
integrative therapy, primarily homeopathy, acupuncture, herbal
medicine.

In Italy
But even in this case there are not many doctors who treat cancer patients with all complementary therapies, but are limited to their specific knowledge: homeopathy, herbal medicine, and so on.
The integrative treatments are mainly the reduction of side effects: effects of chemo and radiation therapy.
There are also economic reasons of the patients for this type of choice.

The information derived from the census EPAAC:
• Patients in the public arena are mainly sent from the
Departments of Oncology
• The CM most commonly used are:
• 1 – acupuncture; 2 -MTC; 3 - herbal medicine; 4- homeopathy;
5 – homotossicology; 6 - anthroposophy ;

1- reduction of adverse effects from CT and RT with particular reference to nausea and vomiting
2- management of pain3- reduction of adverse effects
due to iatrogenic menopause4- improvement in QoL5- resolution anxiety, depression,
fatigue, supportive treatment CT and RT, perioperative noise reduction
6- gastrointestinal disorders, sleep disorders
7- prevention of relapse8- reduction of muscle disorders,
palliative care, reduction of neuropathy
The main clinical indications for which is used in Integrative Oncology IN ITALIAN CENTRES are in order of frequency

In Italy In my case, or in that of some other
collegues, as oncologists, the treatment concerns not only in research the
reduction of side effects but also the ability to associate natural substances
with the intent to increase positive feedback.
My patients are sent also to other colleagues for complementary
treatments: hyperthermia, acupuncture, psycho-oncology, nutrition.

Questions1- Patient who is interested to receive nutritional supplements before or during chemotherapy (clinical dilemma: Is there sufficient evidence to support the use of herbs and dietary supplements during chemotherapy for QOL improvement? How do you ensure safety in regard to supplement-chemotherapy interaction?
2- Improving patient's quality of life during radiation treatment (clinical dilemma: In which cases integrative medicine is indicated during radiation treatment? How do you provide complementary medicine in clinical radiation setting if evidence-based medicine is lacking?)

ABSORPTION: ALTERATION OF ORAL BIOAVAILABILITY
DISTRIBUTION : ALTERATION OF PROTEIN TRANSPORT Phase IMETABOLISM: INTERATION METABOLISM Phase II
EXCRETION: ALTERATION EXCRETION URINARY/LIVER
INTERACTION OF PHARMAKOCYNETICS

Induction Rapid metabolis short time/plasma concentration REDUCED EFFECT
Inhibition Reduced metabolis More time/plasma concentration
INCREASE ACTION INCREASE TOXIC EFFECTS
FACTORS: INDUCTORS - INHIBITORS

CYP 1A1-2CYP 2 B6CYP 2 C8-9-19CYP 2D6CYP 2E1CYP 3A4 35 % OXIDATION
EsterasiUGT
CYP Family

Anastrozole CYP2C9/ CYP 3A4Bleomycin N/A
Busulfan CYP 3A4
Capecitabine Carbossilesterasi/Citidinesterasi
Cisplatin OCT2/ABCC2
Cyclofosfamide CYP2B6/CYP2C9/ CYP3A4
Docetaxel CYP 3A4/5 – ABCB1Doxorubicine CYP 3A4 /CYP2D6- ABCB1
Epirubicine CYP 3A4Erlotinib CYP3A4 /CYP1A2
Etoposide CYP3A4 /ABCB1/ABCC1-2
Fluorouracile Diidropirimidin deidrogenasi
Gefitinib CYP3A4 /ABCG2
Gemcitabine Deamminasi
Ifosfamide CYP2B6/ CYP3A4
Imatinib CYP2C9/ CYP 3A4 Irinotecan CYP 3A4 /UGT1A1 Methotrexate ABCC1/ABCG2 Mytomicine C N/A Oxaliplatin OTC2 Paclitaxel CYP 3A4 /CYP2C8 Tamoxifene CYP2D6/ CYP 3A4 Teniposide CYP 3A4 – ABCB1 Topotecan CYP 3A4 - ABCB2 Vimblastine CYP 3A4 – ABCB1 Vincristine CYP 3A4/5 - ABCB1 Vinorelbine CYP 3A4

• Panax ginseng Inhib. CYP2D6/CYP3A4 •Citrus aurantium no az. CYP2D6/CYP3A4
• Black pepper Inhib. CYP3A4/ABCB1
• Scutellaria Inib. CYP3A4/ABCB1
• Echinacea Induct. CYP3A4
• Garlic Inhib CYP3A4/CYP2E1
• Ginger no act CYP2C9
• Grapefruit strong inhib. CYP3A4
• Ginkgo strong induct. CYP2C19 Inhib CYP3A4
• Vitis Vinifera induct. CYP3A4
• Tea no act CYP2D6/CYP3A4 Green Induct. CYP1A2
• Kava Kava strong inhib. CYP2E1
• Licorice inhib. CYP3A4
• Silibum mariano no act CYP1A2/CYP2D6 /CYP3A4
• Peppermit Inhib. CYP3A4
• Panax quinq no az CYP2D6/CYP3A4
• S. Jont W strong induct. CYP1A2/CYP2C8 CYP2C9/CYP2E1/CYP3A4
• Turmeric no act CYP3A4
• Valerian no act CYP1A2/CYP2D6 /CYP3A4• Alfa glucan no act CYP1A2/CYP2D6 /CYP3A4

- ECHINACEA Attention with Camptothecins,Cyclophosphamide TK inhibitors,Epipodophyllotoxin,Taxans,Vinca (inductor CYP3A4)- GINKGO Attention with Camptothecins,Cyclophosphamide Taxans,Vinca(inhibitor CYP3A4/CYP2C19) Discourage Alkylanting agents,Cancer Antibiotics, platinum derivates (scavenger with free radicals)- GINSENG Discourage Estrogen receptor positive breast and endometrial (stimulus to growth)- GREEN TEA Discourage with Erlotinib ( CYP1A2 inductor)-SOY Avoid withTamoxifen (antagonist in inhibiting
growth), Estrogen receptor positive, breast- endometrium (stimulus to growth)
- S.JHON W Avoid with all drugs (inductor all CYP)- VALERIAN Attention withTamoxifen,Cyclophosphamide,Teniposide (CYP2C19 inhibitor)- VITIS VINIFERA Attention with Camptothecins,Cyclophosphamide TK inhibitors,Epipodophyllotoxins,Taxans,Vinca,Platinum (inductor CYP3A4 e scavenger with free radicals)

- Cisplatin Quercitin Coriolus versicolor Astragalo mebr. Silibum mariano AHCC AHCC Aloe vera Ginkgo biloba- Cyclophosphamide Astragalo membr. AHCC Withania Somnif. Coriolous Versic.- Adriamycin/Idarab Green Tea Green Tea AHCC
- Fluorouracil/Il-2 Turmenic AHCC Green Tea/Astragalo Panax ginseng- Tamoxifen Green Tea/Panax quinqu.- Mitomycin C Panax ginseng- Taxol AHCC
DRUGS increased reduction antineoplastic action
toxicity


Cancer Res. 2010 October 1; 70(19): 7392–7399. Published online 2010 September 14. Clinical Pharmacology of Resveratrol and its Metabolites in Colorectal Cancer
Patients Ketan R Patel,1* Victoria A Brown,1* Donald JL Jones,1 Robert G Britton,1 David
Hemingway,1 Andrew S. Miller,1 Kevin P. West,1 Tristan D Booth,2 Marjorie Perloff,3 James A Crowell,3 Dean E Brenner,4 William P Steward,1 Andreas J Gescher,1 and Karen Brown1
Levels of resveratrol and its metabolites were consistently higher in tissues originating in the right side of the colon compared to the left. Consumption of resveratrol reduced tumor cell proliferation by 5% (P=0.05).
The results suggest that daily oral doses of resveratrol at 0.5 or 1.0 g produce levels in the human gastrointestinal tract of an order of magnitude sufficient to elicit anti-carcinogenic effects.
Resveratrol merits further clinical evaluation as a potential colorectal cancer chemopreventive agent





Antiossidanti, Vitamina ASelenio, Folati, PolifenoliCarotenoidi
Ac grassi Omega-3, Curcumina,riduzione di peso
Restrizione caloricaBassa insulinemiaFibre e Frutta
Enzimi Induttori Fase I° e II°Isotiocianati
Alimenti ricchi diantiossidanti, Vitamina E
Fibre, riduzione di pesoSulforafano, Soia
Grasso, Dieta Americana, Bassi folati, basso introduzionevegetali e frutta
Grasso, Ac grassi Omega-6, Obesità
Vitamina A, Ac. Grassi Omega-3, Carotenoidi, Polifenoli, Isotiocianati
Ac grassi Omega-6, grasso,eccesso alimentare, cibi che alzano Insulina
Saccarina, nitrosammine, amineEterocicliche, muffe
Ferro, Ac grassi Omega-6, acido Arachidonico
Grasso, obesità
DannoDNA
Infiammazione
Apoptosi
Prolifer. Cellulare
Esposizione ai carcinogeni
Stress ossidativo
Ormoni

Patient who is interested to receive nutritional supplements before or during chemotherapy (clinical dilemma: Is there sufficient evidence to support the use of herbs and dietary supplements during chemotherapy for QOL improvement? How do you ensure safety in regard to supplement-chemotherapy interaction?

-43 cancer patients (median age 66,3 – range 35-85 years) were selected and divided into two groups
-A group (31) will take 3 gr/day patients after surgery/chemotherapy in absence of desease-A group (12) will take 6 gr/day patients with desease or in progression
Parameters evaluated:-Blood count, liver function, inflammatory state, Ferritin, LDH, lipid profile, Immunoglobulins, Dhea-s, lymphocytic typing.
All patients were evaluated at time 0-1-2 and 3 months and evaluated parameters and health status

Patients n. 43 %
with mts 12 16
no desease 31 84
reduction 3 7
stable 7 16
progression 2 4
12 pt with mts

- The results that we are noticing in a group with desease:
Almost all patients (about 80%), reported a general improvement of their condition.
-10 patients showed an increase of lymphocytes and neutrophyls.
- 10 patients showed an increase of Th4, reduction of Th8 and normalization of NK
-Three patients in particular showed a further reduction in size of lesions after a two months of integrative treatment.
-All the patients reported mild difficulty in taking the capsules, especially those who assume 12 per day

- Health spending cuts (short, medium and long term) - Reduction in hospitalization- Reduced costs for home care- Reduction of working days lost- Reduced costs for Companies- Increase in activities related to the well-being
EFFICIENCY OF EXPENSE

Of the 49 patients who used the Polydatin and of the 43 patients who used the Glucan-AHCC we can estimate a calculation to reduce health care spending
- Less use of pain medication and / or antiemetics A - Less use of stimulators of hematopoiesis (granulopoiesis and / or hematopoiesis) B- Reduction of blood tests C- Reduction of working days lost D
Calculated for the 14 patients in remission / reduction of injuries- A Euro 1.500- B “ 25.200- C “ 1.000- D “ 2.800Total “ 30.000

IJACM 2013“Effect of AHCC in women receiving adjuvant chemotherapy for
breast cancer: a retrospettive study” Dep. Hemat. And Oncol. University of Tokio
….we calculated the number of G-CSF usage per taxane infusion weekly (paclitaxel)….the AHCC group had significantly lower usage of G-CSF per administration of taxane therapy that did the control group (0.14 in the AHCC group and 0.41 in the control group , p=0.008)
Conclusions: AHCC has the potential to reduce the severity of neutropenia induced by breast cancer chemotherapy and the use of G-CSF during chemotherapy

after 6 mo from Rt.; with Xeloda and Boswellia- Curcumin- Polidatin- Lactofer- Oncophyt 8 and diet
Pz. 54 aa. mts. breast ca: protocol FEC and RT

70 year old man with Glioblastoma.
Radiotherapy and Temodal on April 2011
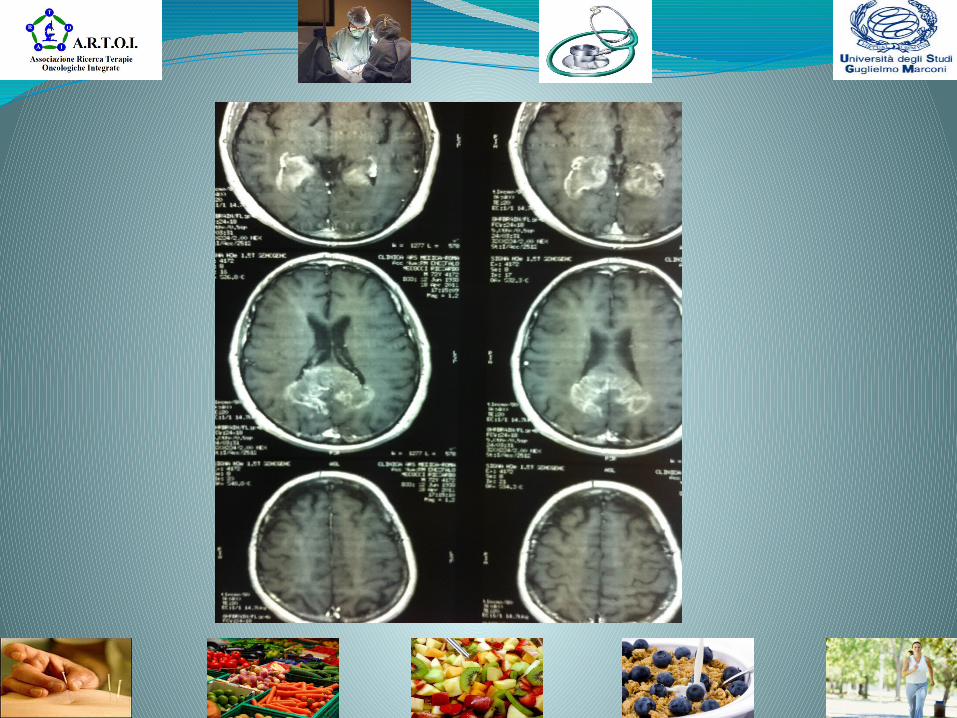

Temodal weekly; July 2011

20 months after Boswellia Serrata, Ruta 6 CH, Calcarea Solforica D7, Polydatin and Curcumin regimen and nutrition. Very good regression on December 2012

Clinical evidence with Lactoferrin
Experimental Study
Lactoferrin in Patient with higth risk of cancer or colon relapse (post polipectomy/after neoplasia)
-20 patients without ill after surgery-20 patiebts with intestinal polips-10 patients ttreated with surgery, chemotherapy e/o radiotherapy
Valutation at 0, 3, 6 e 12 mounth:
- Colonscopy, blood tests of the inflammation, lymphocyte immunophenotyping; DHEA-S; Ferritin; Fibrinogen; Cortisol.

Safety study with
- Mangostano
- Colostro di capra
- Ossigeno in gocce