integrating data systems to support pi managing the...
TRANSCRIPT

Helen Macfie, Pharm.D., FABC
For IHI Leading Population Heath Transformation – February, 2017
Integrating Data Systems to Support PIManaging the Measurement
Madness

Alignment?
THE PROBLEM• Seen one ACO, seen one
– Over 100 unique metrics– Multiple definitions for “similar
indicators”
• Moving from designated to add attributed populations
• Original “P4P” measures we knew well, these are different
– Quality gates and shared savings thresholds vary
• Impact on the front line providers
• What about overdiagnosis?
H. Gilbert “Gil” Welch, M.D.
Author of “Overdiagnosed”

Metric mania
Here’s just one example for Depression Screening “NQF 0711, 0712”:• Boeing – get credit for >18yo with dx of
depression/dysthymia if have PHQ9 within 1 month of PCP visit AND, if score >9, meet the % target for depression remission to <5 within 6 months
• NextGen ACO – get credit if hit a different target for the % screened and then % in remission at 12 months
• Integrated Healthcare Association for CA Medical Groups/IPAs – 2017 measure under discussion for % assessed within defined 4 month measurement period, no target yet
Inclusions? Exclusions?*&^%$#!

SO FAR, SO GOOD…but a caution– We achieved 100% of Quality Gate scoring for Anthem ACO in
year 1 and 2…and 100% in Vivity for both MG & hospital scores
– Both the Next Gen & Boeing ACOs are “pay for reporting” in Year 1, then it gets tougher … both in metrics and thresholds
The easy stuff
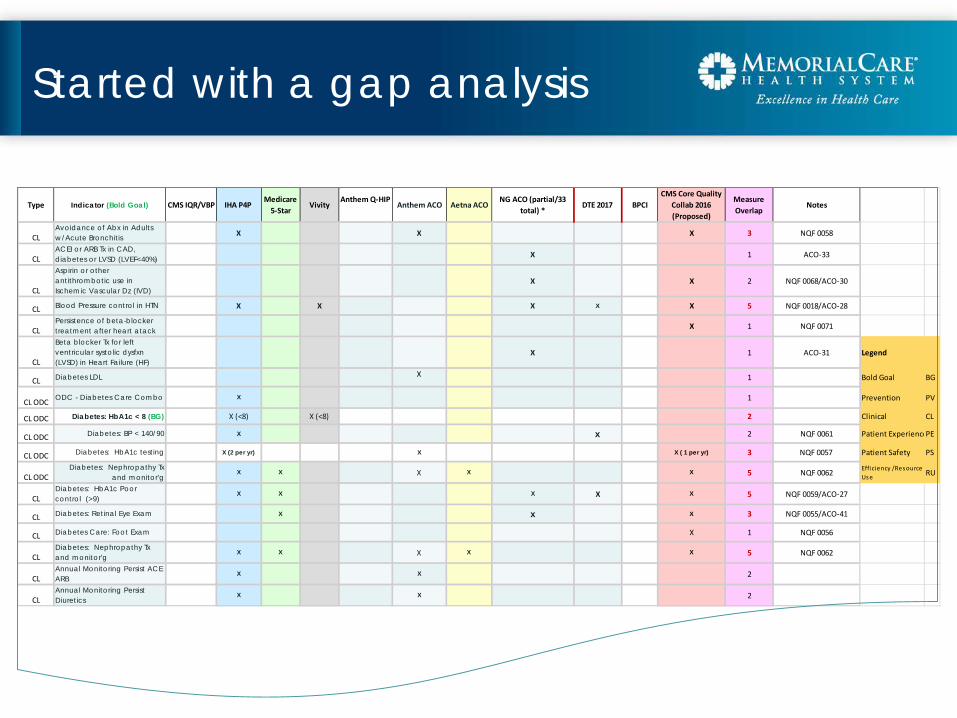
Started with a gap analysis
Type Indicator (Bold Goal) CMS IQR/VBP IHA P4P Medicare
5-StarVivity
Anthem Q-HIPAnthem ACO Aetna ACO
NG ACO (partial/33 total) *
DTE 2017 BPCICMS Core Quality
Collab 2016 (Proposed)
Measure Overlap
Notes
CLAvoidance of Abx in Adults w/Acute Bronchitis X X X 3 NQF 0058
CLACEI or ARB Tx in CAD, diabetes or LVSD (LVEF<40%) X 1 ACO-33
CL
Aspirin or other antithrombotic use in Ischemic Vascular Dz (IVD)
X X 2 NQF 0068/ACO-30
CL Blood Pressure control in HTN X X X X X 5 NQF 0018/ACO-28
CLPersistence of beta-blocker treatment after heart atack X 1 NQF 0071
CL
Beta blocker Tx for left ventricular systolic dysfxn (LVSD) in Heart Failure (HF)
X 1 ACO-31 Legend
CL Diabetes LDL X 1 Bold Goal BG
CL ODC ODC - Diabetes Care Combo X 1 Prevention PV
CL ODC Diabetes: HbA1c < 8 (BG) X (<8) X (<8) 2 Clinical CL
CL ODC Diabetes: BP < 140/90 X x 2 NQF 0061 Patient Experience PE
CL ODC Diabetes: HbA1c testing X (2 per yr) X X ( 1 per yr) 3 NQF 0057 Patient Safety PS
CL ODCDiabetes: Nephropathy Tx
and monitor'gX X X X X 5 NQF 0062 Efficiency /Resource
Use RU
CLDiabetes: HbA1c Poor control (>9)
X X X X X 5 NQF 0059/ACO-27
CL Diabetes: Retinal Eye Exam X x X 3 NQF 0055/ACO-41
CL Diabetes Care: Foot Exam X 1 NQF 0056
CLDiabetes: Nephropathy Tx and monitor'g
X X X X X 5 NQF 0062
CLAnnual Monitoring Persist ACE ARB
X X 2
CLAnnual Monitoring Persist Diuretics
X X 2

Getting granular
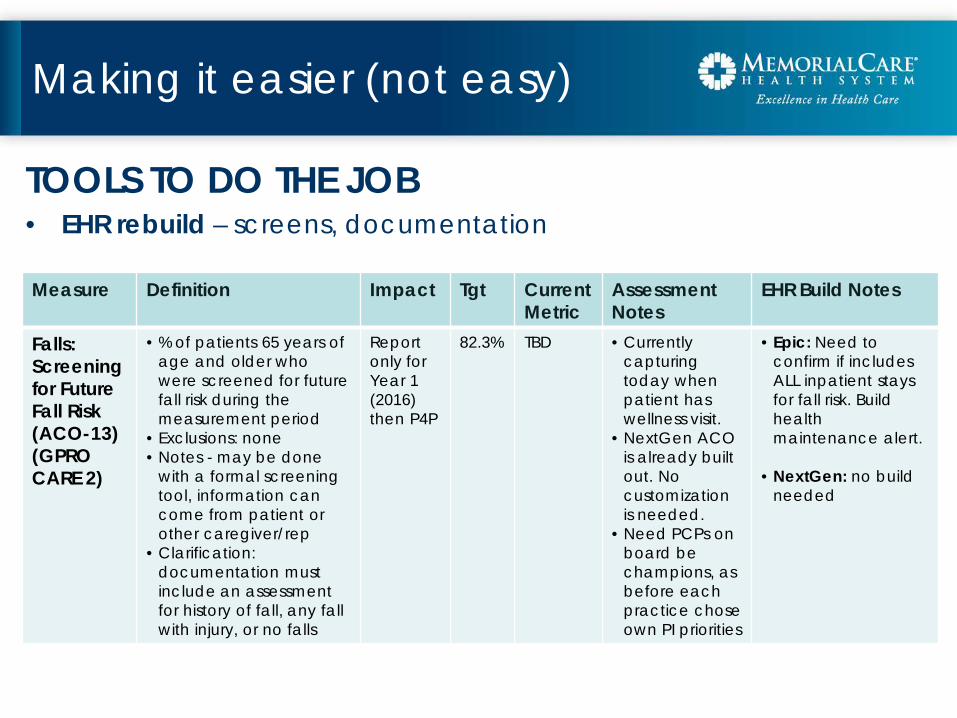
TOOLS TO DO THE JOB• EHR rebuild – screens, documentation
Making it easier (not easy)
Measure Definition Impact Tgt CurrentMetric
Assessment Notes
EHR Build Notes
Falls: Screening for Future Fall Risk (ACO-13) (GPRO CARE 2)
• % of patients 65 years of age and older who were screened for future fall risk during the measurement period
• Exclusions: none • Notes - may be done
with a formal screening tool, information can come from patient or other caregiver/rep
• Clarification: documentation must include an assessment for history of fall, any fall with injury, or no falls
Report only for Year 1 (2016)then P4P
82.3% TBD • Currently capturing today when patient has wellness visit.
• NextGen ACO is already built out. No customization is needed.
• Need PCPs on board be champions, as before each practice choseown PI priorities
• Epic: Need to confirm if includes ALL inpatient stays for fall risk. Build health maintenance alert.
• NextGen: no build needed

TOOLS TO DO THE JOB• Leveraging new “sit-on-top” tools - snapshots
Making it easier (not easy)

TOOLS TO DO THE JOB• Leveraging new “sit-on-top” tools – physician panel dashboards
Making it easier (not easy)

TOOLS TO DO THE JOB• Leveraging new “sit-on-top” tools– patient level drilldown
Making it easier (not easy)

TOOLS TO DO THE JOB• Understanding measure sampling and abstraction flow
Making it easier (not easy)

Creating sanity at the front line
LEVERAGING LEAN• Purpose – create an
organizational plan to develop, execute and manage the processes for improving quality measure results
• Assumption – data is valid, timely and accessible
• Pre-work: had already done the gap analysis on measures; EHR changes for documentation
Guiding Principles• Systemic thinking• Visibility of progress/
process• Single piece flow (avoiding
batches and silos)
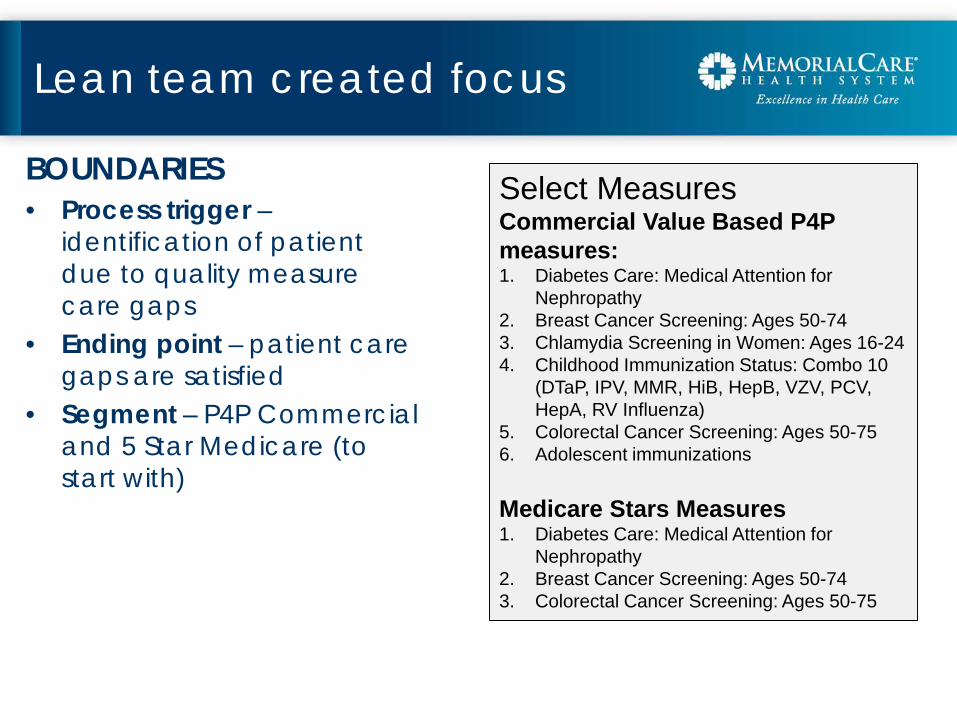
Lean team created focus
BOUNDARIES• Process trigger –
identification of patient due to quality measure care gaps
• Ending point – patient care gaps are satisfied
• Segment – P4P Commercial and 5 Star Medicare (to start with)
Select MeasuresCommercial Value Based P4P measures:1. Diabetes Care: Medical Attention for
Nephropathy2. Breast Cancer Screening: Ages 50-743. Chlamydia Screening in Women: Ages 16-244. Childhood Immunization Status: Combo 10
(DTaP, IPV, MMR, HiB, HepB, VZV, PCV, HepA, RV Influenza)
5. Colorectal Cancer Screening: Ages 50-756. Adolescent immunizations
Medicare Stars Measures1. Diabetes Care: Medical Attention for
Nephropathy2. Breast Cancer Screening: Ages 50-743. Colorectal Cancer Screening: Ages 50-75

Voice of the customer
SURVEY SAYS• Silos and inconsistency in practice
office workflow, missed opportunities• Numerous IT platforms on which
process measure display, confusing to staff, redundant messages to patient
• Inconsistent processes for communication between centralized and decentralized teams - misses
• Some providers who don’t choose to address care gaps during visit
• Staff don’t always see value of preventative screenings
• Patient understanding/”compliance”• Access to services (ex. colonoscopy)
Vision
SHARED FUTURE STATE• Process measure care gaps are addressed every time there is a
patient touchpoint• There is clear and consistent two-way communication between
care team and patient collaborative culture of prevention• Improvement doesn’t exclusively rely on dedicated PCP time• The care gap plan is communicated to care team members
within PCP offices, specialist offices and ancillary services• Continuous and consistent patient outreach to address
preventative screening proactively throughout the year• The patient and his/her care team member understand process
care gaps, have visibility on their care plan, see the value and actively participate in following through
• Care gap services are scheduled conveniently and easily by patients

Key Change!

Redesign plan
TEAMWORKIssue OutcomeConsistent process
• Standard work developed for to address care gaps at every visit
• Improved workflows for screening needs
Follow-up • Developed role of Quality Champions – clinic staff
Staff awareness • Created Tip Sheets for front office (scheduling) and practice staff
• Education and implementation plan
Patient activation • Screening fact sheets for patients• Colorectal screening tool for patients• Developed workflows for “noncompliant” patients
Visibility • Developed consistent reporting standards• Created template and guidelines for Visibility Board
for each practice/office site, easy to update• Communication paths between centralized and
decentralized teams
Accountability • Developed tiered accountability for metrics not met
Check-ins • Quarterly meetings with PI Team and Quality Champions
Recognition • Process for reward and recognition for high performing and most improved office

Making it visible
SURVEY SAYS• Developed a template for
visibility boards that gets updated regularly
• For all clinics (MCMG) and practice sites (IPA) so they can easily track their performance on process measures
• The template includes compliance information on the measure by physician with comparison to the group/practice and the 90th
%ile benchmark

Transparency & celebration
RECOGNITION• Awards are good!

Joy at work
ENTIRE CARE TEAM