integrated care organization best outcome for every patient, every time 1
TRANSCRIPT
1
I N T E G R A T E D C A R E O R G A N I Z A T I O N
Best Outcome for Every Patient, Every Time
Agenda
• Today’s changing healthcare environment• Positioning IHS for success• The ICO’s role in the IHS ACO• Organizational structure of the ICO• ICO strategy
2

The Catalyst
• Patient Protection and Affordable Care Act (“health reform”)While important, health reform has acted as a
catalyst, bringing to the forefront issues we knew existed
With or without reform, the world as we know it will change
3

Ty p i ca l Re l ati o n sh i p Between th e Govern ment an d P hys i c i an s
4

5
The Real Issues
• What we can all agree onCosts for patients and employers increasingFederal and State Budget deficits immenseLack of affordable access to careIncreasing regulatory burdensDecreasing reimbursement for hospitals and
physicians

6
The Real Issues
• Patients are frustratedHigh costFragmentationLack of coordination and collaborationQuality not commensurate with cost

7
The Real Issues
• Physicians are frustratedDeclining reimbursementIncreasing regulatory burdensLack of coordinationVolume driven patient care“Being a physician isn’t what it used to be…”

8
Insanity?
9
A New Day
• Value will be rewarded over volume• Physicians and other clinicians will be able to
serve their patients • Hospitals, physicians and other providers will
be rewarded for managing the overall health of our communities
• Patients will receive coordinated and collaborative health care…not fragmentation

10
Integrated Care Organizati on
11
Positi oning for Success
• Physicians and hospitals are better off working togetherCollaborate on initiatives that make both clinical
and financial sensePreparation will require a well-organized, capable
provider network with supportive infrastructure for population management

12
Potenti al Payment Arrangements
Increasing Risk
Value-Based PaymentFee for Service

13
IHS Overview• Formed in December 1994• 15 hospitals and 800+ employed physicians practicing in more
than 76 Iowa and Illinois communities• 2,600+ affiliated physicians• $2.6 billion total operating revenue• 22,200+ employees• 4 Colleges of Nursing• 2.5 million patient visits annually• Mission: Improve the health of the people and communities
we serve• Vision: Best outcome for every patient every time

14
Physician Alignment
Create Value
Demonstrate Value
Value-Based Contracting
IHS Road Map
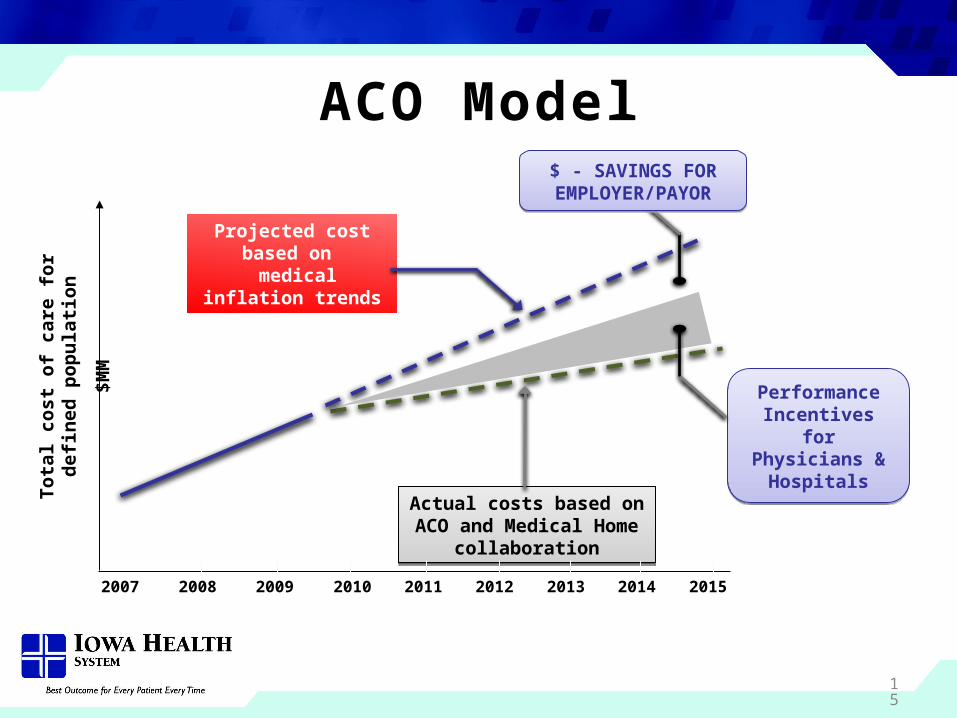
ACO Model
Performance Incentives for Physicians &
Hospitals
Performance Incentives for Physicians &
HospitalsTota
l cos
t of c
are
for d
efine
d po
pula
tion
$MM
Projected cost based on medical inflation trends
Actual costs based on ACO and Medical Home
collaboration
Actual costs based on ACO and Medical Home
collaboration
2007 2008 2009 2010 2011 2012 2013 2014 2015
$ - SAVINGS FOR EMPLOYER/PAYOR$ - SAVINGS FOR
EMPLOYER/PAYOR
15

16
Populati on Management
17
ICO Vision and Identi tyIHS Integrated Care Organization
About Us
The Integrated Care Organization (ICO) is our clinical integration platform for employed and independent physicians to work together to improve quality of care, enhance the patient experience and create more value in health care
Vision Statement
Best Outcome for Every Patient, Every Time
18
ICO Defi ned
• The ICO is a tax-exempt, nonprofit organization• Designed by independent and employed
physicians with multi-specialty group leaders from around the system
• Physicians intricately involved in governance and operations of the ICO
19
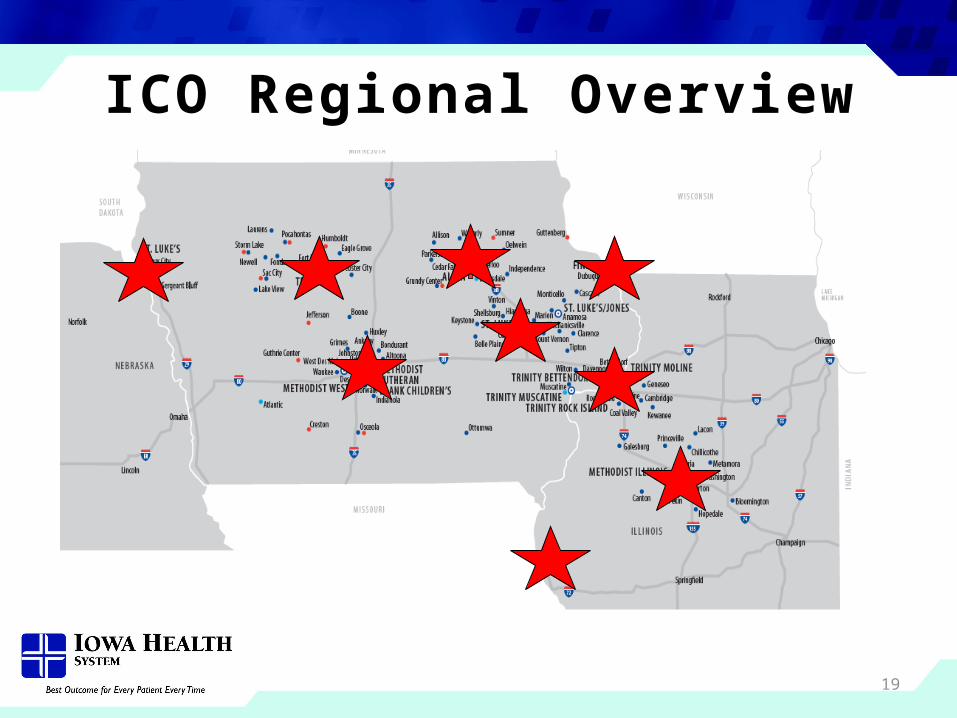
ICO Regional Overview
20
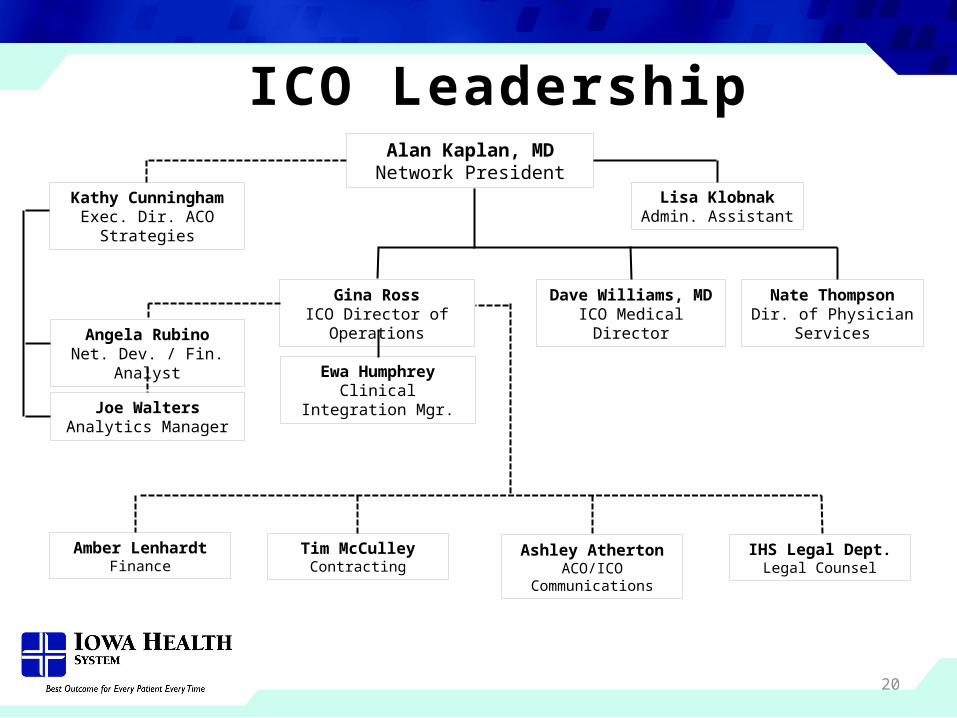
ICO LeadershipAlan Kaplan, MD
Network President
Nate ThompsonDir. of Physician Services
Dave Williams, MDICO Medical Director
Gina RossICO Director of Operations
Lisa KlobnakAdmin. Assistant
Angela RubinoNet. Dev. / Fin. Analyst
Tim McCulleyContracting
Amber LenhardtFinance
Ashley AthertonACO/ICO Communications
Ewa HumphreyClinical Integration Mgr.
IHS Legal Dept.Legal Counsel
Kathy CunninghamExec. Dir. ACO Strategies
Joe WaltersAnalytics Manager
21
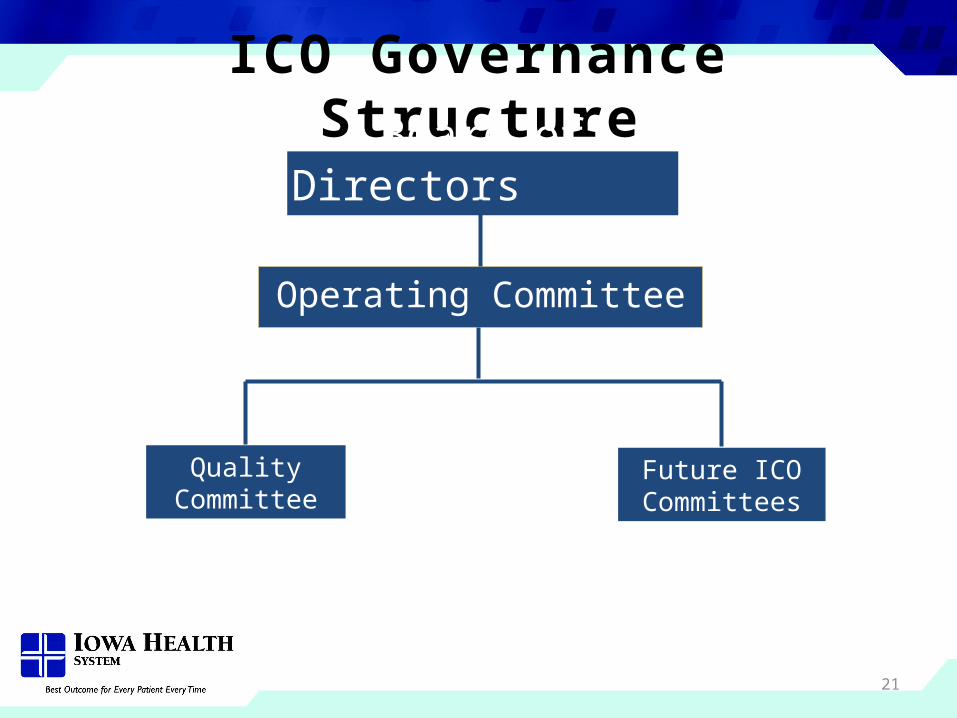
ICO Governance Structure
Operating Committee
Board of Directors
Quality Committee
Future ICO Committees
22
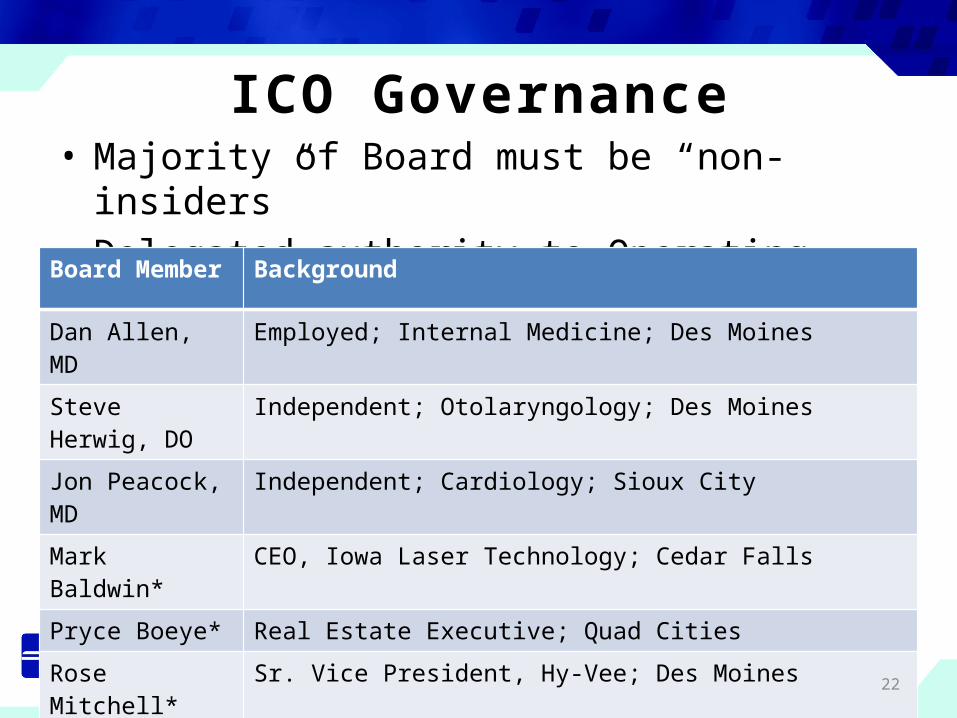
ICO Governance• Majority of Board must be “non-insiders” • Delegated authority to Operating Committee
Board Member Background
Dan Allen, MD Employed; Internal Medicine; Des Moines
Steve Herwig, DO Independent; Otolaryngology; Des Moines
Jon Peacock, MD Independent; Cardiology; Sioux City
Mark Baldwin* CEO, Iowa Laser Technology; Cedar Falls
Pryce Boeye* Real Estate Executive; Quad Cities
Rose Mitchell* Sr. Vice President, Hy-Vee; Des Moines
John Perkins* Attorney; Fort Dodge*Community Board Member
23
ICO Governance • Operating Committee
16 physician & 5 non-physician members Responsible for leading the operations of the ICO Gregory Johnson, MD, Chair (Peoria)
• Quality Committee 9 physician & 3 non-physician members Reports to the Operating Committee Responsible for development of the ICO Quality
Program Ron Iverson, MD, Chair (Dubuque)
24
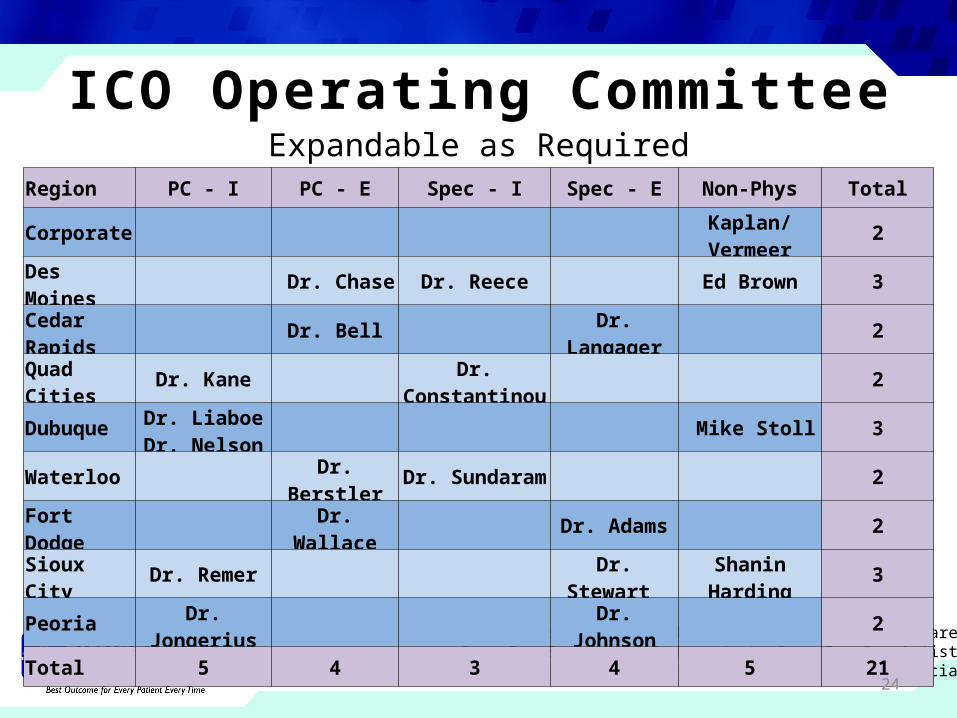
ICO Operati ng Committ eeExpandable as Required
PC-I = Primary care independent; PC-E = Primary care employedSpec-I = Specialist Independent; Spec-E = Specialist employed
Non-Phys = Medical group leaders, IHS Chief Medical Officer & IHS Chief Financial Officer
Region PC - I PC - E Spec - I Spec - E Non-Phys Total
Corporate Kaplan/Vermeer 2
Des Moines Dr. Chase Dr. Reece Ed Brown 3
Cedar Rapids Dr. Bell Dr. Langager 2
Quad Cities Dr. Kane Dr. Constantinou 2
Dubuque Dr. LiaboeDr. Nelson Mike Stoll 3
Waterloo Dr. Berstler Dr. Sundaram 2
Fort Dodge Dr. Wallace Dr. Adams 2
Sioux City Dr. Remer Dr. Stewart Shanin Harding 3
Peoria Dr. Jongerius Dr. Johnson 2
Total 5 4 3 4 5 21

25
ICO Quality Committ eeExpandable as Required
PC-I = Primary care independent; PC-E = Primary care employedSpec-I = Specialist Independent; Spec-E = Specialist employed
Region PC - I PC - E Spec - I Spec - E Non-Physician Total
Corporate Dr. Williams Gina Ross 2
Des Moines Dr. Schulte Wendt, Sander 3
Cedar Rapids Dr. Hodge 1
Quad Cities Dr. Raman 1
Dubuque Dr. Iverson 1
Waterloo Dr. Sampat 1
Fort Dodge Dr. Smith 1
Sioux City Dr. Brenner 1
Peoria Dr. Johnson 1
Total 1 4 3 1 3 12
26
ICO Strategy• Establish a clinically integrated network across IHS
Align independent and employed physicians on a common quality improvement platform
Pursue value-based contracts that reward performance on quality metrics which are meaningful to physicians, patients, families and our communities (i.e. shared savings)
Assist ICO physicians with the changing healthcare environment where quality, patient experience and value are recognized
27
ICO Engine
• Chronic Disease AnalyticsCreate disease registryAid in the management of chronically ill patientsEnhance physician-to-physician communicationProvide outcome measuresProvide actionable information to support
management of patient populations

28
ICO Engine

29
ICO Initi ati ves• Build system-wide primary care network
aligned on common set of metrics for 2012• Reward achievement of quality targets with
incentive dollarsIHS Self Funded Health PlanACO Shared Savings agreement with WellmarkRestructured Wellmark Pay for Performance
programsMedicare Shared Savings Program
30
Phases of Physician Engagement• Phase One: System wide network of primary
care physicians• Phase Two: Core specialty physicians required
for care of complex, chronically ill patientsCardiologyGastroenterologyEndocrinology
• Phase Three: Full spectrum of physicians
31
2012 Proposed ICO Metrics• Quality Program Measures
Chronic Care Management (Claims Data) Office visits within 30 days of hospital discharge 3 or more annual office visits for chronically ill
Primary Prevention (Claims Data) Mammography Colonoscopy Pediatric well visits
• Thresholds based on historical performance

32
Financial Drivers for Shared Savings
• Shared savings driven by:Avoidable ER visitsAvoidable admissionsReduction in pharmaceutical costsReduction in duplicative ancillary tests/proceduresEvidence based care guides

33
Timeline• January 1, 2012
Engage primary care physicians
• April 1, 2012IHS Self Funded Health PlanWellmark ACO Shared SavingsModified QIS ProgramEngage core specialty physicians
• July 1, 2012Engage full spectrum of physiciansMedicare Shared Savings Program

34
Ideal State
35
Summary• The ICO is the physician-driven quality improvement
platform within the IHS ACO• The ICO will create and demonstrate value through
physician collaboration around the “triple aim”: Improve quality outcomes Enhance patient experience Decrease overall cost of care
• ICO physicians will be positioned for long-term stability and success, regardless of what happens with healthcare reform
36