integrated cancer services action plan colchester hospital ...€¦ · action plan colchester...
TRANSCRIPT

Integrated Cancer Services Action Plan
Colchester Hospital University
NHS Foundation Trust 31 May 2014
KEY
Implemented, clearly evidenced and externally approved
On Track to deliver
Some issues – narrative disclosure
Not on track to deliver
1

Colchester Trust - Our improvement plan & our progress
What are we doing?
• The Trust entered Special Measures following concerns about the standard of cancer care being delivered by the Trust.
• The Trust has been given a variety of recommendations which have come from CQC visit report, the Intensive Support Team report, External Review Visit (published 19
December) focussed on Cancer Services. The recommendations covered the following areas of concern:
• Failsafe paper processes
• Audit of cancer waiting times data
• Review of Cancer Services workload (including Oncology Consultants)
• Cancer Pathways – Urology (bladder and prostate), Brain & Central Nervous System, Cancer of Unknown Primary Origin and Sarcoma
• Governance arrangements
• Safeguarding Adults & Children
• The Trust has amalgamated the 331 recommendations from the reviews (set out above) into a Cancer Remedial Action Plan. All recommendations have been recognised
and accepted by the Trust. The actions within the Cancer Remedial Action Plan address all issues, with the overall aim to improve the quality of cancer services. We
envisage that improvements will be largely complete by 31 December 2014. The Trust will set out a longer-term plan to maintain progress and ensure that the actions lead to
measurable improvements in the quality and safety of care for patients.
• The Trust established that there were a number of themes which encompassed all the recommendations
• Governance structures and processes for managing patients on a cancer pathway
• Data Collection & Data Governance
• Management of patients on a Cancer pathway
• Safeguarding Adults and Children
This document provides a high level summary of the ‘urgent actions’ under these themes but is not a comprehensive list of all actions or other actions being taken to improve.
We have set out our progress in making improvement against these actions. While we take forward our plans to address the 331 recommendations, the Trust will remain in
‘special measures’.
• To ensure appropriate oversight and rapid improvement in cancer services the Trust has implemented the following changes:
• Reconstitution of the Trust Cancer Board to include Multi-disciplinary Clinical Leads to oversee the decisions made relating to Cancer Services . The Trust Cancer
Board reports to the Trust Quality and Patient Safety Committee., a sub-committee of the Trust Board.
• Appointment of Cancer Programme Director and Project Manager to drive the required improvements reporting to a Cancer Steering Group
• A Project Management Office and Turn Around Director to oversee and give assurance to the delivery of the action plan.
2

Colchester Trust- Our improvement plan & our progress
Who is responsible?
• Our actions to address the NHS England Cancer Services review report recommendations have been agreed by the Trust Board.
• Our Chief Executive, Lucy Moore is ultimately responsible for implementing actions in this document. Sean MacDonnell, Medical Director, is the Executive Lead for delivery
of improvements in Cancer.
• The Improvement Director assigned to Colchester Hospitals NHS Foundation Trust is Mark Davies, who will be acting on behalf of Monitor and in concert with the relevant
Regional Team of Monitor to ensure delivery of the improvements and oversee the implementation of the action plan overleaf. Should you require any further information on
this role please contact [email protected]
• Ultimately, our success in implementing the recommendations of the Trust’s Cancer Action Plan will be assessed by the Chief Inspector of Hospitals, who will re-inspect our
Trust within 12 months after entering the Special Measures programme.
• If you have any questions about how we’re doing, contact Mark Prentice, Head of External Relations, [email protected] , 01206 742752.
How we will communicate our progress to you
• We will update this progress report every month while we are in special measures.
• There will be regular updates on NHS Choices and subsequent longer term actions may be included as part of a continuous process of improvement.
• The Trust Board receives monthly updates in its public meeting.
Chair / Chief Executive Approval (on behalf of the Board):
Chair Name: Sally Irvine Signature: Date 31st May 2014
Chief Executive Name: Lucy Moore
Signature:
Date: 31st May 2014
3

Colchester Trust - Our improvement plan Governance Structures and Processes for managing patients on a cancer pathway
Summary of Urgent Actions Required Action Owner
Agreed Timescale for Implementation
External Support/ Assurance
Progress Revised deadline (if required)
We will: • Ensure key roles responsibilities and
accountabilities are defined and appointed to (e.g. Lead Cancer Clinician, Lead Cancer Nurse, Executive Lead for Cancer)
Medical Director Director of Nursing
Lead Cancer Clinician/Executive Lead for Cancer – 31 January 2014 Lead Cancer Nurse by 28 February 2014
Monitor Clinical Commissioning Group
Red Key roles have been defined in line with national role descriptions as detailed in the Manual of Cancer Standards. Roles have been appointed to with the exception of the Lead Cancer Nurse. Lead Cancer Nurse Interviews being carried out on 6th May. Lead Cancer Nurse role not appointed to. Post has been re-advertised. Closing date 6th June with interviews set for 30th June. The Royal Marsden is supporting us to find a suitable candidate for this role.
• Review of all MDTs to ensure they are effective (using National Cancer Action Team published "Characteristics of an Effective MDT" Feb 2010).
Medical Director
31 December 2014 Strategic Clinical Network
Green Review Programme is being developed – to be presented at Cancer Board May 14. MDT-fit tool presented at Cancer Board May 14. We are seeking to identify suitable clinical resource to take this very important action. At present we are still on track to deliver by end December 14.
• Ensure that the appropriate Governance Committees provide assurance to the Board of the quality of care delivered
Medical Director
31 March 2014 Monitor Blue Cancer Board meeting monthly, with clear Agenda and Minutes. Agreed Terms of Reference in place. Well attended by Clinical Leads. The work programme of the Cancer Board in 2014 is to monitor the delivery of the Cancer Remedial Action Plan. Monthly update of progress to the Quality & Patient Safety Committee.
• Review the workload of all Cancer Services workforce
Medical Director (Clinicians) Director of Nursing (Nurses) Chief Operating Officer (Administrative Staff)
31 March 2014 National Peer Review Programme
Red A Summary of vacancies recruited to, and additional posts identified through external review has been completed. All remaining vacancies have been advertised and are being actively recruited. Clinical workload review is incorporated into annual joint planning cycle commencing 1st April 14. MDT Co-ordinator workload being assessed using IST Workload Tool commencing 13th May 14 completion date 31st May 14. Clinical Nurse Workload review terms of reference to be agreed at June Cancer Board. Work on Medical workforce has commenced with risks identified in Lower Gi, Head & Neck, and Dermatology.
4
Colchester Trust - Our improvement plan
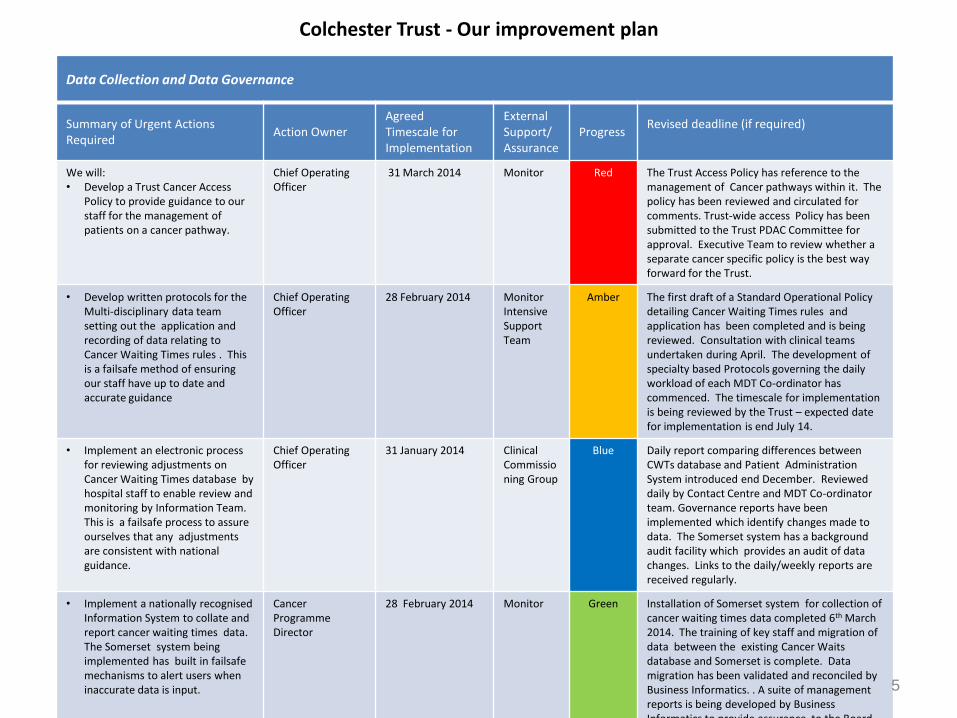
Data Collection and Data Governance
Summary of Urgent Actions Required
Action Owner Agreed Timescale for Implementation
External Support/ Assurance
Progress Revised deadline (if required)
We will: • Develop a Trust Cancer Access
Policy to provide guidance to our staff for the management of patients on a cancer pathway.
Chief Operating Officer
31 March 2014 Monitor Red The Trust Access Policy has reference to the management of Cancer pathways within it. The policy has been reviewed and circulated for comments. Trust-wide access Policy has been submitted to the Trust PDAC Committee for approval. Executive Team to review whether a separate cancer specific policy is the best way forward for the Trust.
• Develop written protocols for the Multi-disciplinary data team setting out the application and recording of data relating to Cancer Waiting Times rules . This is a failsafe method of ensuring our staff have up to date and accurate guidance
Chief Operating Officer
28 February 2014 Monitor Intensive Support Team
Amber The first draft of a Standard Operational Policy detailing Cancer Waiting Times rules and application has been completed and is being reviewed. Consultation with clinical teams undertaken during April. The development of specialty based Protocols governing the daily workload of each MDT Co-ordinator has commenced. The timescale for implementation is being reviewed by the Trust – expected date for implementation is end July 14.
• Implement an electronic process for reviewing adjustments on Cancer Waiting Times database by hospital staff to enable review and monitoring by Information Team. This is a failsafe process to assure ourselves that any adjustments are consistent with national guidance.
Chief Operating Officer
31 January 2014 Clinical Commissioning Group
Blue Daily report comparing differences between CWTs database and Patient Administration System introduced end December. Reviewed daily by Contact Centre and MDT Co-ordinator team. Governance reports have been implemented which identify changes made to data. The Somerset system has a background audit facility which provides an audit of data changes. Links to the daily/weekly reports are received regularly.
• Implement a nationally recognised Information System to collate and report cancer waiting times data. The Somerset system being implemented has built in failsafe mechanisms to alert users when inaccurate data is input.
Cancer Programme Director
28 February 2014 Monitor Green Installation of Somerset system for collection of cancer waiting times data completed 6th March 2014. The training of key staff and migration of data between the existing Cancer Waits database and Somerset is complete. Data migration has been validated and reconciled by Business Informatics. . A suite of management reports is being developed by Business Informatics to provide assurance to the Board. The Somerset system feeds Qlikview, the management tool used by the Trust to track its performance at specialty level.
5

Colchester Trust - Our improvement plan
Data Collection and Data Governance (continued)
Summary of Urgent Actions Required
Action Owner
Agreed Timescale for Implementation
External Support/ Assurance
Progress Revised deadline (if required)
We will: • Make improvements to our
weekly cancer escalation processes ensuring there is a failsafe method for escalating patients treatment pathways.
Chief Operating Officer
31 January 2014
Clinical Commissioning Group
Green Review of weekly escalation processes has been completed. Changes to the process have been implemented. A weekly Action Log has been implemented which identifies constraints which may delay patient pathways – this is reviewed by Service Managers weekly . Detailed Terms of Reference for escalation processes presented to Cancer Board in April 14. Comments from clinical teams being collated. Consideration is being given to merging the 18 week and Cancer weekly meetings to improve service management representation.
• Implement an electronic system of single point of receipt for GP Suspected Cancer Referrals, and referrals to and from other hospitals for cancer pathways. This is a failsafe method of capturing referrals which will replace paper referrals into the Trust.
Chief Operating Officer
31 March 2014
Clinical Commissioning Group
Green The Contact Centre commenced on 23rd December for internal referrals. External (2ww) referrals are timetabled to commence via Choose & Book at end March (in conjunction with North East Essex CCG). An operational policy has been developed, which details how referrals are managed with detailed timeframes and presented at Cancer Board (April 14). GP two week wait referrals moved to Choose & Book from 31st March 14 (with an nhs.net email as a failsafe if Choose & Book slot not available). Practices are able to set up a delivery/read receipt for these referrals to provide assurance of receipt. The Inter-Trust Referral policy is in development in partnership with other Essex Hospitals with whom cancer pathways are shared. Anticipated date for completion of the inter-trust referral policy is end July 14 but is dependent on other external organisations. 6

Colchester Trust - Our improvement plan
Data Collection and Data Governance (continued)
Summary of Urgent Actions Required Action Owner
Agreed Timescale for Implementation
External Support/ Assurance
Progress Revised deadline (if required)
We will: • Develop a programme of regular and
continuous training for our MDT Co-ordinator team which will provide us with a failsafe method of ensuring our staff are up-to date.
Chief Operating Officer
28 February 2014
Monitor Intensive Support Team
Green Initial training commenced Dec 13. Further training day for Root Cause Analysis undertaken mid February 14. Training relating to the new data information system (Somerset) completed (7th & 14th February).. Regular training updates on issues identified through the Weekly Escalation Processes continue to be delivered through Team Meetings for the MDT Co-ordinator & Data Clerk Team. Team Meetings are taking place weekly with a standard item on CWTs guidance – topics for discussion/training are identified by the MDT Co-ordinator & Data Clerk Team.
• Improve support and advice to MDT Co-ordinator Team including standard operating procedures to support MDTCs/Data Clerks roles/functions, including escalation processes This is a failsafe method of ensuring our staff are following consistent and accurate guidance.
Chief Operating Officer
28 February 2014
Monitor Intensive Support Team
Green
The Cancer Services Standard Operational Policy details the Cancer Waiting Times guidance and protocols outlining the standard processes required to support each MDT on a daily basis has been completed and is being reviewed. This document details how data is to be recorded on the Somerset cancer data information system. Policy presented to Cancer Board April 14. The Operational Policy has been submitted to the Trust PDAC Committee May 14. Awaiting confirmation from PDAC that the Policy has been approved.
• Develop an electronic failsafe competency framework to ensure MDTC/Data Clerks knowledge and skills are maintained (similar to that used for IT Governance) which will be tested annually.
.Cancer Programme Director
31 March 2014
Monitor Intensive Support Team
Amber Discussions have commenced to develop an e-learning tool and competency framework for annual assessment of data collection staff. Cancer Services Standard Operational Policy encompasses competency framework. This action has slipped due to implementation of Somerset system. The Trust is reviewing the options for delivering the e-learning tool and will be confirmed by end June 14.
• Implement Inter-Trust Referral policy (recommended by Midlands & East of England Strategic Clinical Network).
Medical Director 31 January 2014
Strategic Clinical Network
Amber Communication with external trusts advising of the adoption of this policy established - an Essex wide meeting took place end April with Trusts, the Strategic Clinical Network (SCN) and the Cancer Registry. The aim was to reach agreement by end May 2014 but this timetable has slipped. The Trust anticipated date for completion, subject to external organisations is end July 2014, Currently awaiting confirmation of date for teleconference from the SCN and Cancer Registry to finalise the policy.
• Establish regular failsafe monitoring programme to ensure all referrals are made by Day 42 and tracked appropriately
Medical Director 31 March 2014
Clinical Commissioning Group
Amber Somerset implemented with data migration completed. Monitoring of incoming and outgoing tertiary referrals was expected to be monitored via Somerset from 1 April 2014. Release of Somerset module for inter-trust referrals has slipped to Autumn 2014 by Somerset Cancer Registry and is outside of the control of the hospital. The deadline for completion to be reviewed.
7

Colchester Trust - Our improvement plan Management of patients on a cancer pathway
Summary of Urgent Actions Required Action Owner
Agreed Timescale for Implementation
External Support/ Assurance
Progress Revised deadline (if required)
We will • Ensure that patients referred through
18 weeks are upgraded onto a Cancer Pathway (if there is a suspicion of Cancer) . Ensure trust-wide Access Policy for Cancer has a clear definition of Consultant Upgrades
Chief Operating Officer
31 March 2014
Monitor Green Development of a dedicated Trust Cancer Access Policy to encompass when it is appropriate for MDT Clinical Teams to upgrade patients onto a 62 day cancer pathway is under development. Clarification relating to Consultant Upgrade discussed at Cancer Board Feb 14. All Consultant Upgrades will be recorded on Somerset through the Contact Centre (single point of referral) from 1 April 14. All Consultant upgrades are recorded on Somerset. Number of consultant upgrades being monitored monthly through Cancer Hub. Numbers of consultant upgrades are reported monthly to the Cancer Board as part of the regular performance report. There is increasing level of confidence by the Trust Executive that the previous level of under-reporting is being addressed and monitored.
• Ensure that all recommendations from peer review are implemented
Divisional Clinical Directors
31 December 2014
Strategic Clinical Network .
Green The Cancer Action Plan incorporates all recommendations from previous peer reviews and has clear actions and timescales. The Cancer Board is responsible for ensuring delivery of all peer review remedial actions and this is encompassed in its Terms of Reference. Timetable for peer review and requirements of each MDT team to be confirmed at June Cancer Board.
• Ensure that the Anal Cancer Pathway is implemented and is IOG compliant
Medical Director
30 September 2014
Specialised Commissioning Group
Blue Discussions are continuing with Specialised Commissioning and the Strategic Clinical Network to ensure compliance with Improving Outcomes Guidance (IOG) is in line with agreed timetable. CHUFT are referring all Anal Salvage Surgery patients to Norfolk & Norwich hospital (upto 12 patients per year) as an interim measure agreed with Specialised Commissioning. There is a separate additional piece of work which will be led by NHS England, Specialised Commissioning Team to confirm an IOG compliant solution for all hospitals in Essex.
• Ensure Gynaecology MDT has cover for Consultant Oncologist
Medical Director
30 June 2014 Strategic Clinical Network
Green Recruitment commenced December 13. Consultant Oncologist appointed – commences June 14. Following induction, MDT cover will be in place by end June 14.
• Ensure Urology service has sufficient capacity to treat patients
Chief Operating Officer
31 March 2014
Monitor Green All actions to increase capacity are completed or on course for completion. Additional clinics commenced mid December; additional theatre capacity, including weekend working, has been in place since January 14; recruitment for additional medical and nursing staff has commenced. Additional consultant commenced early March; additional nursing posts have been advertised and shortlisted. Interviews successful – CNS post appointed to – start date to be confirmed.
8

Colchester Trust - Our improvement plan
Management of patients on a cancer pathway (continued)
Summary of Urgent Actions Required Action Owner
Agreed Timescale for Implementation
External Support/ Assurance
Progress Revised deadline (if required)
We will • Ensure there a re clear documented
pathways for Urology (prostate and bladder)
Multi-disciplinary Team Clinical Lead
30 December 13
External Visit Review Team
Blue Prostate and Bladder cancer pathways have been revised and assured by the visiting External Review Clinical Lead. The Clinical Team are regularly auditing this pathway and is part of the regular programme of pathway audits to be presented at Cancer Board. External revisit of prostate, bladder and renal pathways (28th April) confirmed pathways assured. No immediate risks or serious concerns identified.
• Ensure the Skin pathway is compliant with cancer waiting times guidance.
Medical Director
31 January 2014
Strategic Clinical Network
Green Pathway has been reviewed by visiting External Consultant and compliance with Cancer Waiting Times guidance has been received. Pathway audit will be undertaken to ensure compliance. Awaiting date for revisit of pathway from Strategic Clinical Network.
• Ensure there is a clear documented pathway for suspicious lesions
Medical Director
31 January 2014
Strategic Clinical Network
Blue A process for the management of the pathway for patients with suspicious lesions has been developed and is incorporated within the Contact Centre Operational Policy7. Discussed and agreed at Cancer Board March 14. External pathway revisit (14th April) confirmed process assured.
• Ensure there are robust tracking methods for Sarcoma patients
Medical Director
31 March 2014
Strategic Clinical Network
Blue A Standard Operational policy for the management of Sarcoma patients has been developed and is being implemented. Sarcoma pathways (bone and soft tissue) ratified at Cancer Board March 14. Pathway audit to be presented at Cancer Board. External pathway revisit (14th April) confirmed pathway assured.
• Ensure there is a clear documented pathway for Brain/Central Nervous System patients
Medical Director
28 February 2014
Strategic Clinical Network
Blue Revised pathway completed 16th December. Agreed at Cancer Board Feb 14. Pathway revisit took place 20th May – pathway assured.
• There is a clear MDT structure and pathway for Cancer of Unknown Primary
Medical Director
31s March 2014
Strategic Clinical Network
Blue Standard operational policy has been developed for the management of patients who present with Cancer of Unknown Primary. MDT structure reviewed – anticipated to be in place mid April 14. The external pathway revisit has confirmed assurance of the Cancer Unknown Primary pathway.
9

Colchester Trust - Our improvement plan
Management of patients on a cancer pathway (continued)
Summary of Urgent Actions Required
Action Owner Agreed Timescale for Implementation
External Support/ Assurance
Progress Revised deadline (if required)
• Ensure all Cancer pathways are regularly audited . This is a failsafe process to ensure that patients are treated in line with agreed pathways.
Medical Director
31 December 2014 Strategic Clinical Network
Green A programme of regular clinical audit of cancer pathways is being presented to Cancer Board . The outcome of the first pathway audit (Urology) was presented at the March Cancer Board. Audit programme agreed at Cancer Board March 14 covering all tumour site pathways. Relevant pathway audits presented at each Cancer Board.
• Develop a continuous quality improvement programme for cancer specialties, to encompass clinical peer review visit recommendations
Trust Clinical Cancer Lead
31 May 2014 Strategic Clinical Network
Green A draft document detailing each of the components of the continuous quality improvement programme presented to Cancer Board May 14. The key components identified as contributing towards a continuous quality improvement programme are in place and are being regularly monitored. Implementation is in progress and being monitored by the Cancer Board and Quality & Patient Safety Committee. The Royal Marsden is providing additional support to the hospital to develop a Strategy for Cancer. The Continuous Quality Improvement Programme to be submitted to Quality & Patient Safety Committee June 14.
10

Colchester Trust - Our improvement plan
Safeguarding Adults and Children
Summary of Urgent Actions Required
Action Owner Agreed Timescale for Implementation
External Support/ Assurance
Progress Revised deadline (if required)
We will • Confirm the Non-Executive Director
lead and ensure all board members receive training
Director of Nursing End December 2013 Monitor Blue Non-Executive Director for Safeguarding confirmed . Safeguarding training completed .
• Ensure that there are policies and procedures in place to protect vulnerable adults and children
Director of Nursing End December 2013 Monitor Clinical Commissioning Group
Blue Policies and procedures completed and presented to Trust Board.
• Ensure the internal Trust intranet has an e-training module
Director or Nursing
End December 2013 Clinical Commissioning Group
Blue E-training module for Safeguarding In place mid December.
• Develop a communications plan for
contacting all patients (to convey outcome) following clinical-notes review (duty of candour).
Medical Director 31 July 2014 NHS England Green It has been agreed with NHS England that this will be incorporated into Retrospective Review programme timetable under Duty of Candour.
11

Colchester Trust - How our progress is being monitored and supported
12
Oversight and improvement action Agreed Timescale for Implementation
Action owner Progress
Outline details of how the progress is being monitored and supported during the Special Measures programme. e.g. the appointment of an Improvement Director by Monitor; the identification of a Buddy Trust to help support the Special Measures Trust implement its Action Plan.
Confirm whether the action has been started – its due date or completed date (detail month and year.)
Confirm who is responsible for making sure each task is actioned.
Provide a brief summary of why the
RAG colour was picked for each particular
action
• There is a multidisciplinary led external review structure, which is overseeing the development and implementation of the Trust Cancer Action Plan, comprising a clinical oversight group, an operational group and an Executive Assurance Group. These groups encompass NHS England Clinical Commissioning Group, Trust representatives, Essex County Council , health regulators (Monitor) and Health Watch (which represents patients views).
Mid December 13 Chief Executive Blue The Trust is
represented with excellent attendance
on all groups
• In addition to the above, there are regular Clinical Commissioning Group oversight and assurance groups which meet weekly. These include :
a) Review of the weekly process for reviewing patients on the cancer waiting times database
b) Weekly unscheduled visits/walkabouts by the Commissioners
c) Weekly clinical scrutiny by GP partners –review of patient pathways
December 13 Cancer Programme Director Blue All groups are being regularly attended
• Trust Cancer Board has been reconstituted to include Multi-disciplinary Team Clinical Leads , Clinical Nurse Specialists, and Service Managers, to oversee the decisions made relating to Cancer Services . The Trust Cancer Board reports to the Trust Board through the Quality and Patient Safety Committee. The Cancer Board oversees and monitors the implementation of the Trust Remedial Cancer Action Plan.
Mid December 13
Clinical Lead for Cancer Services Blue Reconstituted Board
commenced mid December.
Effectiveness of the Group to be monitored throughout the year by the Quality & Patient
Safety Committee
• Appointment of Cancer Programme Director and Project Manager to drive the required improvements.
Beg December 14 Sean MacDonnell, Medical Director Blue Cancer Programme
Director took up post 2nd December 13
Project Manager in post from 27th February
2014

Colchester Trust - How our progress is being monitored and supported
Oversight and improvement action Agreed Timescale for Implementation
Action owner Progress
Outline details of how the progress is being monitored and supported during the Special Measures programme. e.g. the appointment of an Improvement Director by Monitor; the identification of a Buddy Trust to help support the Special Measures Trust implement its Action Plan.
Confirm whether the action has been started – its due date or completed date (detail month and year.)
Confirm who is responsible for making sure each task is actioned.
Provide a brief summary of why the
RAG colour was picked for each particular
action
• A Cancer Service s Steering Group to oversee and drive the implementation of the Trust Cancer Action Plan has been established to ensure progress against the Cancer Action Plan. This Group reports to Trust Board through the Quality & Patient Safety Committee and the Trust Turnaround Board. The Steering Group monitors the progress of the Cancer Remedial Action Plan.
January 2014 Medical Director Blue Steering Group has commenced and is
meeting weekly
• A Programme Management Office has been implemented to provide structure to the improvement programmes at the Trust including Cancer. This includes the Cancer Services Steering Group which reports to the Quality & Patient Safety Committee and Turnaround Board chaired by the CEO.
January 2014 Chief Executive Blue Programme
Management Office commenced January 14
• Appointment of Improvement Director (by Monitor) to work with and support the Trust to deliver the Cancer Action Plan.
Completed 20th January 2014
Chief Executive Blue Improvement Director
took up post week commencing 20th
January
13