instant-view multi-drug screen urine test … · the instant-view multi-drug screen urine test...
TRANSCRIPT
INSTANT-VIEW Multi-Drug Screen Urine Test
33-2896 REV F 112204 Page 1
INSTRUCTIONS FOR USE One Step Assay Rapid Visual Results For Professional, Qualitative In Vitro Diagnostic Use INTENDED USE AND SUMMARY OF TESTS
The INSTANT-VIEW Multi-Drug Screen Urine Test is a qualitative immunoassay intended to be used to detect the presence of drugs and/or drug metabolites in human urine at their specified cutoff levels, in a single assay. It is intended for health care professional use only. The INSTANT-VIEW Multi-Drug Screen Urine Test provides only a preliminary analytical test result. A more specific alternate chemical method must be used to obtain a confirmed analytical result. Gas Chromatography / Mass Spectrophotometry (GC/MS) is the preferred confirmatory method. Clinical consideration and professional judgment should be applied to any drug of abuse test result, particularly when preliminary positive results are used.1
Immunoassay urine-based testing for drugs of abuse has become one of the most accepted methods of preliminary screening. These assays allow laboratories to eliminate a large number of negative specimens and focus on the smaller number of initially positive samples.
PRINCIPLE OF THE PROCEDURE The INSTANT-VIEW assay is a one-step lateral flow chromatographic immunoassay with test strips which include 1) a burgundy-colored conjugate pad containing colloidal gold conjugated to anti-drug antibodies and 2) a nitrocellulose membrane containing a test line (T line) and a control line (C line). The T line is coated with the drug antigen; and the C line is coated with goat anti-mouse IgG antibody. This test is a competitive binding immunoassay. The drug or drug metabolite in the urine specimen competes with the antigen coated on the nitrocellulose membrane for the limited binding sites of the conjugated antibodies. When an adequate amount of urine specimen is applied to the sample pad of the device, the urine migrates by capillary action through the test strips. If the drug level in the specimen is below the cutoff level, the burgundy-colored gold-antibody conjugate will bind to the antigens coated on the nitrocellulose membrane, and form a burgundy T line, indicating a negative result. If the drug in the urine specimen is at a test strip’s cutoff level or higher, it will bind to conjugated antibodies, so that no T line develops, indicating a positive result. The colored gold-antibody conjugate should bind to the C line and form a burgundy-colored band regardless of the presence of the drug.
REAGENTS & MATERIALS SUPPLIED • 25 test devices each sealed in a foil pouch with a desiccant and a dropper
pipette (20 devices, if 7-12 test panel) • 1 Instructions for Use
MATERIAL REQUIRED BUT NOT PROVIDED • Specimen Collection Containers • Timer
STORAGE AND STABILITY Store the kit at room temperature 15-30°C (59-86°F). Each device may be used until the expiration date printed on the label if it remains sealed in its foil pouch containing desiccant. Do not expose the kit to temperatures over 30°C (86°F).
SPECIMEN COLLECTION AND STORAGE Each urine specimen must be collected in a clean container. Do not combine specimens. Specimens may be kept at room temperature for 8 hours, at 2-8°C for up to 3 days and at -20°C or lower for long term storage. Urine samples exhibiting visible precipitates should be filtered or centrifuged and allowed to settle. Use only clear aliquots for testing.
PRECAUTION 1. Instructions must be followed to obtain accurate results. 2. Do not open the sealed pouch, unless ready to conduct the assay. 3. Do not use expired devices. 4. Dispose of all specimens and used assay materials as potentially
biohazardous
ASSAY PROCEDURE 1. Refrigerated specimens and other test materials, including devices,
must be equilibrated to room temperature before testing. 2. Remove the test device from the pouch and label it with specimen
identification. 3. Perform assay:
DIP METHOD a) Remove the cap and dip the device into the specimen for at
least 10 seconds. The surface of the sample must be above the sample well and below the level of the arrowheads in the window. b) Remove the device from the specimen after 10 seconds.
OPTIONAL PROCEDURE: (Recommended for small sample volumes.) a) Remove the cap. Take the pipette from the pouch. b) Press bulb to fill the pipette with the sample specimen up to the
line on the barrel. Add all the specimen into the sample well. For 2-sided panels (7-12 test), repeat sample addition by pipette on side 2.
4. Put the cap back on the device and place it on a flat dry surface. 5. Read the test result between four (4) to seven (7) minutes after adding
the specimen. IMPORTANT: Do not read test results after seven (7) minutes.
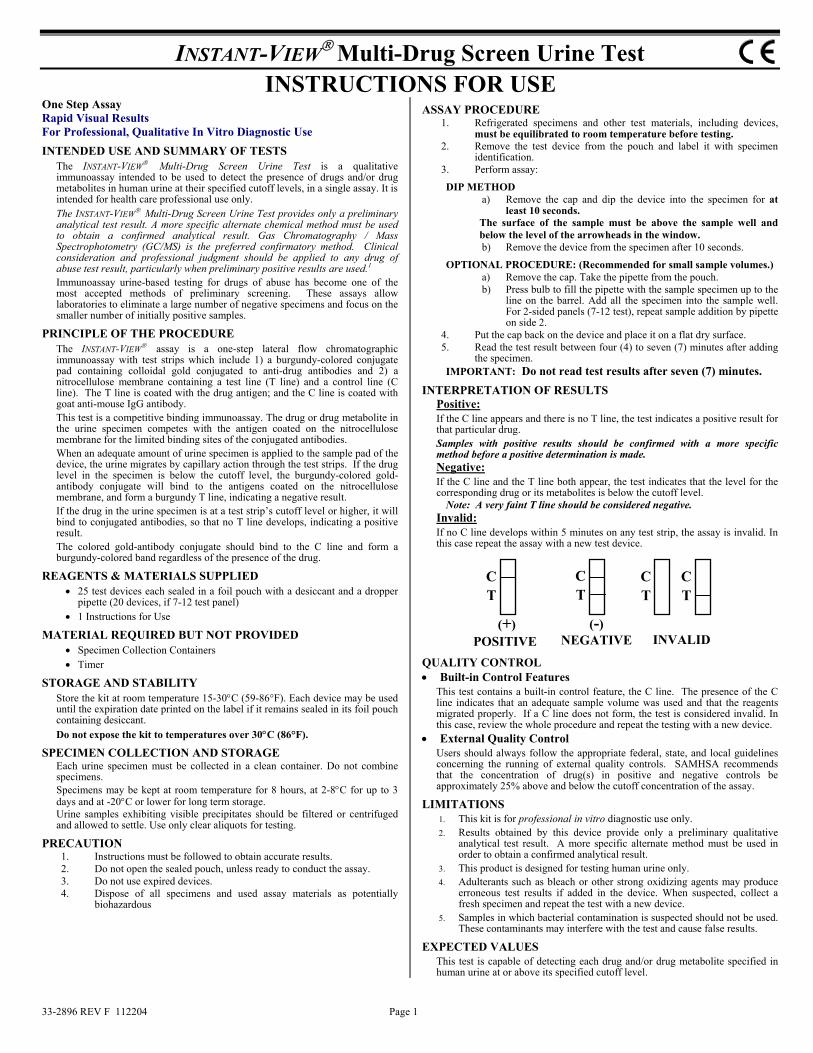
INTERPRETATION OF RESULTS Positive: If the C line appears and there is no T line, the test indicates a positive result for that particular drug. Samples with positive results should be confirmed with a more specific method before a positive determination is made. Negative: If the C line and the T line both appear, the test indicates that the level for the corresponding drug or its metabolites is below the cutoff level.
Note: A very faint T line should be considered negative. Invalid: If no C line develops within 5 minutes on any test strip, the assay is invalid. In this case repeat the assay with a new test device.
QUALITY CONTROL • Built-in Control Features
This test contains a built-in control feature, the C line. The presence of the C line indicates that an adequate sample volume was used and that the reagents migrated properly. If a C line does not form, the test is considered invalid. In this case, review the whole procedure and repeat the testing with a new device.
• External Quality Control Users should always follow the appropriate federal, state, and local guidelines concerning the running of external quality controls. SAMHSA recommends that the concentration of drug(s) in positive and negative controls be approximately 25% above and below the cutoff concentration of the assay.
LIMITATIONS 1. This kit is for professional in vitro diagnostic use only. 2. Results obtained by this device provide only a preliminary qualitative
analytical test result. A more specific alternate method must be used in order to obtain a confirmed analytical result.
3. This product is designed for testing human urine only. 4. Adulterants such as bleach or other strong oxidizing agents may produce
erroneous test results if added in the device. When suspected, collect a fresh specimen and repeat the test with a new device.
5. Samples in which bacterial contamination is suspected should not be used. These contaminants may interfere with the test and cause false results.
EXPECTED VALUES This test is capable of detecting each drug and/or drug metabolite specified in human urine at or above its specified cutoff level.
CT
C T
C T
CT
POSITIVE NEGATIVE INVALID(+) (-)

INSTANT-VIEW Multi-Drug Screen Urine Test
33-2896 REV F 112204 Page 2
PERFORMANCE CHARACTERISTICS INSTANT-VIEW Multi-Drug Screen Urine Test devices are qualitative immunoassays intended for use by health care professionals to screen for potential abuse of one or more drugs in a single assay. Different devices are made to screen for different numbers and combinations of drugs. Performance attributes of the individual tests that may be in a given INSTANT-VIEW device panel are summarized herein.
SENSITIVITY (CUTOFF): Each assay is developed to detect the presence of a drug of abuse or metabolite(s)* thereof at or above a specified cutoff level. For all assays, tests of patient’s samples should consistently indicate negative results for specimens below concentration of 75% of the cutoff and positive results above 125% of the cutoff. The drugs and their cutoff levels are listed below:
AMP - Amphetamine…… 1000 ng/ml MOR - Morphine……… 2000 ng/ml BAR - Barbiturates……… 200 ng/ml MTD - Methadone……… 300 ng/ml BZD - Benzodiazepines… 300 ng/ml PCP - Phencyclidine…… 25 ng/ml COC - Cocaine………… 300 ng/ml PPX - Propoxyphene… 300 ng/ml MET - Methamphetamine** 500 ng/ml TCA - Tricyclics……… 1000 ng/ml MET - Methamphetamine… 1000 ng/ml THC - Marijuana/Hashish 50 ng/ml MOR - Morphine**……… 300 ng/ml XTC - MDMA or Ecstasy 500 ng/ml
*Metabolites detected in the above tests are listed in the sections below: **Available but not SAMHSA levels.
INTERFERING SUBSTANCES: Interfering Substances: To determine the interference of structurally unrelated analytes, each test analyte was evaluated, using the analyte specific INSTANT-VIEW Urine Test device, in both drug free urine pools and urine pools spiked with the cutoff level of each analyte listed in the following table...
Common substances listed in this table were found not to interfere with the test results at the concentration of 100 µg/ml Acetaminophen Oxalic Acid Ethanol Acetylsalicylic Acid Caffeine Lidocaine Amikacin (+)-Chlorpheniramine Penicillin-G Amitriptyline Cocaine Phenylpropanalamine Ampicillin Codeine Ranitidine Arterenal Cortisone Salicyclic Acid Aspirin Methadone Thioridazine Atropine Methanol Trifluoperazine Benzoic Acid
Biological Analytes Concentration Biological Analytes Concentration Albumin 200 µg/ml pH 5.0 – 9.0 Bilirubin 100 µg/ml Specific Gravity 1.002 – 1.035 g/ml Creatine 100 µg/ml Uric Acid 100 µg/ml Glucose 200 µg/ml Hemoglobin 100 µg/ml
Vitamin C (L-Ascorbic Acid)
100 µg/ml
There is a possibility that other substances and/or factors not listed above may interfere with the test and cause false results.(e.g., technical or procedural errors)
A. Amphetamine (AMP) 1. Summary and Explanation of the Test
The detection of amphetamines in human urine has been widely used to assess the abuse of amphetamines. Amphetamines are central nervous system stimulating drugs. They may induce alertness, wakefulness, increased energy, reduced hunger and overall feeling of well-being. Overdose and extended usage of amphetamines may lead to substance abuse, which may cause severe and/or permanent damage to the human nerve system. Amphetamines appear in the urine within three hours after administration (any type), and may be present for about 24-48 hours after the last dose.2,3, 4
2. Accuracy A study was performed at three different Physician’s Office Laboratories (POL) and a Reference Laboratory. One hundred nineteen (119) clinical samples were blind labeled and tested. Each sample was tested at each site, with INSTANT-VIEW Amphetamine Urine Test, and compared with GC/MS results. The results from the INSTANT-VIEW Amphetamine Urine Test agreed 100% with the GC/MS data of specimens at levels below 75% of the cutoff (negative) and above 125% of the cutoff (positive). Thirty eight (38) discrepancies were observed on the specimens at the level between 75% and 125% of the cutoff. The overall agreement was 92.0%.
INSTANT-VIEW Test Positive Negative
Total
Agreement
Drug-free 0 176 176 100% <75% (0~750) 0 76 76 100% 75%~Cutoff (750~1000) 37 23 60 38.3% Cutoff~125% (1000~1250) 15 1 16 93.8%
GC/MS (ng/ml)
Positive (>1250) 148 0 148 100% Total 200 276 476 92.0%
3. Reproducibility Reproducibility was determined at three different POL locations, by persons with diverse educational backgrounds and work experience. Forty-pooled drug-free human urine specimens were spiked with amphetamine at different levels. All specimens were blind labeled and tested. The results are as follows:
POL 1 POL 2 POL 3 Amp. Conc. (ng/ml)
No of Samples + – + – + –
0 8 0 8 0 8 0 8 750 8 4 4 0 8 2 6 1000 8 8 0 8 0 8 0 1250 8 8 0 8 0 8 0 2000 8 8 0 8 0 8 0
The results indicate a 95.0% concordance with the expected results. 4. Cross-Reactivity
A study was conducted using amphetamine-related compounds to determine the cross-reactivity of the test.
Amphetamine related compounds showing the lowest concentration of the drug producing a positive response equivalent to the cutoff level. Compounds Concentration (ng/ml) Compounds Concentration (ng/ml) d-Amphetamine 1000 l-Amphetamine 20,000 d-,l-Amphetamine 1000
3,4- methylenedioxyamphetamine (MDA)
3000
B. Barbiturates (BAR) 1. Summary and Explanation of the Test
Barbiturates are central nervous system depressants and used as hypnotic sedatives. Overdose and extended usage of barbiturates may lead to severe and/or permanent damage to the human nervous system.2 Barbiturates are classified as (1) ultra-short, (2) short-intermediate, and (3) long-acting. The duration range of the ultra short-acting compounds, secobarbital, pentobarbital etc. is from fifteen (15) minutes to six (6) hours. The duration range of the intermediate acting compounds, amobarbital, etc. is from three (3) to twenty-four (24) hours. The duration range of the long-acting compounds, phenobarbital etc. is from fifteen (15) to forty-eight (48) hours.3, 5 The most commonly abused barbiturates are short- and intermediate-acting agents. The long-acting agents are rarely subject to abuse. Barbiturate derivatives are excreted into urine in varying amounts of unchanged drug and metabolites.5 Long-acting barbiturates are excreted with a higher percentage of unchanged drug in the urine, while shorter-acting barbiturates, secobarbital and amobarbital, are extensively metabolized and excreted in the urine with a smaller percentage of unchanged drugs.2, 3 The INSTANT-VIEW Barbiturate Urine Test is designated to detect unchanged secobarbital in the urine; however, as with some other analytical methods such as EMIT and RIA, this assay can also detect other commonly encountered barbiturates, depending on the concentration of drug present in the sample. Phenobarbital positives have been noted in chronic users up to several weeks after cessation of use. With standard single doses of secobarbital, pentobarbital, or amobarbital, positive results may be identified from 30 hours to 76 hours.2
2. Accuracy A study was performed at three different Physician’s Office Laboratories (POL) and a Reference Laboratory. One hundred (100) clinical samples were blind labeled and tested. Each sample was tested at each site, with INSTANT-VIEW Barbiturate Urine Test, and compared with GC/MS results. The results from the INSTANT-VIEW Barbiturate Urine Test agreed 100% with the GC/MS data of specimens at levels below the cutoff (negative) and above 125% of the cutoff (positive). One (1) discrepancies was observed on the specimens at the level between the cutoff and 125% of the cutoff. The overall agreement was 99.8%.
INSTANT-VIEW Test Positive Negative
Total Agreement
Drug-free 0 200 200 100% <75% (0~150) 0 12 12 100% 75%~Cutoff (150~200) 0 20 20 100% Cutoff~125% (200~250) 27 1 28 96.4%
GC/MS (ng/ml)
Positive (>250) 140 0 140 100% Total 167 233 400 99.8%
3. Reproducibility Reproducibility was determined by replicate assays of four different levels of samples with three different production lots. The devices were tested for five consecutive days five times each, for a total of 25 assays for each control. The results indicate 100% precision for the replicate within each lot and no appreciable inter-lot variation across the three different lots of devices.
4. Cross-Reactivity To determine the cross-reactivity of the structurally related compounds with the device, the following compounds were spiked into known drug-free urine pools and tested with the INSTANT-VIEW Barbiturate Urine Test. Those compounds showed a positive response at the concentration indicated in the following table:
Description Concentration (ng/ml) Description Concentration (ng/ml) Amobarbital 250 Phenobarbital 200
Barbital 250 Pentobarbital 250 Butabarbital 300 Secobarbital 200
Butalbital 200
C. Benzodiazepines (BZD) 1. Summary and Explanation of the Test
Benzodiazepines, including Alprazolam, Diazepam, Lorazepam, Triazolam, Chlordiazepoxide, Flurazepam and Temazepam are sedative, hypnotic and anti-anxiety drugs commonly being used as oral tranquilizers. Most benzodiazepine are extensively metabolized in the liver and excreted in the urine as metabolites.3 Benzodiazepines have a low potential for physical or psychological dependence. However, the same as other central nervous system stimulating drugs, they may induce drowsiness and muscle relaxation. Chronic abuse of benzodiazepine may result in intoxication, similar to drunken behavior. Overdose and extended usage of benzodiazepine may lead to coma and possibly

INSTANT-VIEW Multi-Drug Screen Urine Test
33-2896 REV F 112204 Page 3
death. Benzodiazepines may remain effective for 4-8 hours.3, 5 The members of the Benzodiazepine family are absorbed at different rates and their effects may vary with the absorption rate. They are excreted in the urine primarily as their parent compounds or an inactive metabolite, oxazepam glucuronide, that are only detectable for one (1) to two (2) days. Oxazepam, a common metabolite of many benzodiazepines, is also a marketed drug (Serax); it may remain detectable in urine for up to one week.3 That makes oxazepam a useful marker of benzodiazepine abuse.
2. Accuracy A study was performed at three different Physician’s Office Laboratories (POL) and a Reference Laboratory. One hundred (100) clinical samples were blind labeled and tested. Each sample was tested at each site, with INSTANT-VIEW Benzodiazepine Urine Test, and compared with GC/MS results. The results from the INSTANT-VIEW Benzodiazepine Urine Test agreed 100% with the GC/MS data of specimens at levels below 75% of the cutoff (negative) and above the cutoff (positive). Seven (7) discrepancies were observed on the specimens at the level between 75% of the cutoff and the cutoff. The overall agreement was 98.3%.
INSTANT-VIEW Test Positive Negative
Total
Agreement
Drug-free 0 168 168 100% <75% (0~225) 0 24 24 100% 75%~Cutoff (225~300) 7 25 32 78% Cutoff~125% (300~375) 32 0 32 100%
GC/MS (ng/ml)
Positive (>375) 144 0 144 100% Total 183 217 400 98.3%
3. Reproducibility Reproducibility was determined by replicate assays of four different levels of samples with three different production lots. The device was tested for five consecutive days five times each, for a total of 25 assays for each control. The results indicate 100 % precision for the replicate within each lot and no appreciable interlot variation across the three (3) different lots of devices.
4. Cross-Reactivity To determine the cross-reactivity of the structurally related compounds with the device, the following compounds were spiked into known drug-free urine pools and tested with the INSTANT-VIEW Benzodiazepine Urine Test. Those compounds showed a positive response at the concentration indicated in the following table:
Description Concentration (ng/ml) Description Concentration (ng/ml) Alprazolam 300 Lormetazepam 300 Bromazepam 500 Medazepam 300 Clobazem 1500 Nitrazepam 250 Chlonazepam 500 Nordiazepam 400 Diazepam 200 Prazepam 250 Desmethyldiazepam 300 Triazolam 300 Flurazapam 300 Oxazepam 300 Lorazepam 450
D. Cocaine (COC) 1. Summary and Explanation of the Test
Cocaine is one of the nervous system’s stimulating drugs with pharmacological properties, such as a local anesthetic. It has addictive effects leading to substance abuse. Cocaine may appear in urine for only few hours after use, whereas the benzoylecgonine, a hydrolytic degradation product of cocaine, may be detectable in urine over 2 days after taking cocaine. Therefore the detection of benzoylecgonine in human urine has been widely used to evaluate cocaine usage.2,3, 4
2. Accuracy A study was performed at three different Physician’s Office Laboratories (POL) and a Reference Laboratory. One hundred (100) clinical samples were blind labeled and tested. Each sample was tested at each site, with INSTANT-VIEW Cocaine (Benzoylecgonine) Urine Test, and compared with GC/MS results. The results from the INSTANT-VIEW Cocaine (Benzoylecgonine) Urine Test agreed 100% with the GC/MS data of specimens at levels below 75% of the cutoff (negative) and above the cutoff (positive). Nine (9) discrepancies were observed on the specimens at the level between 75% of the cutoff and the cutoff. The overall agreement was 97.8%.
INSTANT-VIEW Test Positive Negative
Total
Agreement
Drug-free 0 188 188 100% <75% (0~225) 0 4 4 100% 75%~Cutoff (225~300) 9 11 20 55% Cutoff~125% (300~375) 24 0 24 100%
GC/MS (ng/ml)
Positive (>375) 164 0 164 100% Total 197 203 400 97.8%
3. Reproducibility Reproducibility was determined at the three different POL locations by persons with diverse educational backgrounds and work experiences. Forty-pooled drug-free human urine specimens were spiked with benzoylecgonine at different levels. All specimens were blind labeled and tested. The result is as follows:
POL 1 POL 2 POL 3 Benz Conc. (ng/ml)
No of Samples + – + – + –
0 8 0 8 0 8 0 8 225 8 5 3 2 6 0 8 300 8 8 0 8 0 8 0 375 8 8 0 8 0 8 0 600 8 8 0 8 0 8 0
Results indicate an average concordance of 94.2 % with the expected results.
4. Cross-Reactivity A study was conducted using cocaine-related compounds to determine the cross-reactivity of the test.
Cocaine and its structurally related compounds showing the lowest concentration of the drug producing a positive response equivalent to the cutoff: Description Concentration (ng/ml) Description Concentration (ng/ml)Cocaine 300 Isoxsuprine 1500 Benzoylecgonine 300
E. Methamphetamine (MET500) 1. Summary and Explanation of Test
Methamphetamine in overdosage causes restlessness, confusion, anxiety, hallucinations, cardiac arrhythmias, hypertension, hyperthermia, circulatory collapse, convulsions, and coma.3 Methamphetamine has been implicated in fatal poisonings following both intravenous and oral administration. Chronic abusers may develop paranoid psychosis.1 D-Methamphetamine (d-desoxyephedrine, Desoxyn, Methedrine) is the N-methyl derivative of amphetamine. It is utilized in the treatment of obesity. Methamphetamine is administered by oral, nasal insufflation, or intravenous injection with duration of 2-4 hours.3, 5 Methamphetamine undergoes some N-demethylation to amphetamine, its major active metabolite. During normal conditions up to 43% of a dose is eliminated unchanged in the 24-hour urine, with about 4-7% as amphetamine. In acid urine, up to 76% is found as unchanged drug and 7% as amphetamine in 24 hours, whereas in alkaline urine the corresponding values are 2% and less than 0.1%. Methamphetamine urine concentrations of 0.5-4.0 mg/L are commonly observed during the first 24 hours after ingestion of 10 mg. Methamphetamine concentrations of 24-333 mg/L (average, 142) were observed in the urine of methamphetamine abusers.5
2. Accuracy A study was performed at three different Physician’s Office Laboratories (POL) and a Reference Laboratory. One hundred nineteen (119) clinical samples were blind labeled and tested. Each sample was tested at each site, with INSTANT-VIEW Methamphetamine Urine Test, and compared with GC/MS results. The results from the INSTANT-VIEW Methamphetamine(500) Urine Test agreed 100% with the GC/MS data of specimens at levels below 75% of the cutoff (negative) and above 125% of the cutoff (positive). Twenty two (22) discrepancies were observed on the specimens at level between 75% and 125% of the cutoff. The overall agreement was 95.4%.
INSTANT-VIEW Test Positive Negative
Total
Agreement
Drug-free 0 220 220 100% <75% (0~375) 0 36 36 100% 75%~Cutoff (375~500) 6 22 28 78.6% Cutoff~125% (500~625) 24 16 40 60%
GC/MS (ng/ml)
Positive (>625) 152 0 152 100% Total 182 294 476 95.4%
3. Reproducibility Reproducibility was determined at three different POL locations, by persons with diverse educational backgrounds and work experience. Forty-pooled drug-free human urine specimens were spiked with methamphetamine at different levels. All specimens were blind labeled and tested. The result is as follows:
POL 1 POL 2 POL 3 Methamp. Conc (ng/ml)
No of Samples + – + – + –
0 8 0 8 0 8 0 8 375 8 0 8 0 8 1 7 500 8 8 0 8 0 8 0 625 8 8 0 8 0 8 0 1000 8 8 0 8 0 8 0
The results indicate a 99.2% concordance with the expected results. 4. Cross-Reactivity
A study was conducted using methamphetamine-related compounds to determine the cross-reactivity of the test.
Methamphetamine related compounds showing the lowest concentration of the drug producing a positive response equivalent to the cutoff level. Description Concentration (ng/ml) d-Methamphetamine 500 l-Methamphetamine 25,000 d-Amphetamine 50,000 l-Amphetamine 10,000 3,4-methylenedioxyamphetamine (MDA) 50,000
F. Methamphetamine (MET1000) 1. Summary and Explanation of Test
Methamphetamine in overdosage causes restlessness, confusion, anxiety, hallucinations, cardiac arrhythmias, hypertension, hyperthermia, circulatory collapse, convulsions, and coma.3 Methamphetamine has been implicated in fatal poisonings following both intravenous and oral administration. Chronic abusers may develop paranoid psychosis.1 D-Methamphetamine (d-desoxyephedrine, Desoxyn, Methedrine) is the N-methyl derivative of amphetamine. It is utilized in the treatment of obesity. Methamphetamine is administered by oral, nasal insufflation, or intravenous injection with duration of 2-4 hours.3, 5 Methamphetamine undergoes some N-demethylation to amphetamine, its major active metabolite. During normal conditions up to 43% of a dose is eliminated unchanged in the 24-hour urine, with about 4-7% as amphetamine. In acid urine, up to 76% is found as unchanged drug and 7% as amphetamine in 24 hours, whereas in alkaline urine the corresponding values are 2% and less than 0.1%. Methamphetamine urine concentrations of 0.5-4.0 mg/L are commonly observed during the first 24 hours after ingestion of 10 mg.

INSTANT-VIEW Multi-Drug Screen Urine Test
33-2896 REV F 112204 Page 4
Methamphetamine concentrations of 24-333 mg/L (average, 142) were observed in the urine of methamphetamine abusers.5
2. Accuracy A study was performed at three different Physician’s Office Laboratories (POL) and a Reference Laboratory. One hundred (100) clinical samples were blind labeled and tested. Each sample was tested at each site, with INSTANT-VIEW Methamphetamine (1000) Urine Test, and compared with GC/MS results. The results from the INSTANT-VIEW Methamphetamine (1000) Urine Test agreed 100% with the GC/MS data of specimens at levels below 75% of the cutoff (negative) and above the cutoff (positive). Twelve (12) discrepancies were observed on the specimens at level between 75% of the cutoff and the cutoff. The overall agreement was 97%.
INSTANT-VIEW Test Positive Negative
Total
Agreement
Drug-free 0 200 200 100% <75% (0~750) 0 16 16 100% 75%~Cutoff (750~1000) 12 12 24 50% Cutoff~125% (1000~1250) 24 0 24 100%
GC/MS (ng/ml)
Positive (>1250) 136 0 136 100% Total 172 228 400 97%
3. Reproducibility Reproducibility was determined by replicate assays on four different concentrations (GC/MS) of methamphetamine in urine samples: 0ng/ml, 870ng/ml (within 25% below the cutoff), 1200ng/ml (within 25% above the cutoff), and 2000ng/ml (positive) with three different production lots. The devices were tested for five consecutive days five times each, for a total of 25 assays for each control. The results indicate 100% precision for the replicate within each lot and no appreciable inter-lot variation across the three different lots of devices.
4. Cross-Reactivity To determine the cross-reactivity of the structurally related compounds with the device, the following compounds were spiked into known drug-free urine pools and tested with the INSTANT-VIEW Methamphetamine Urine Test. Those compounds showed a positive response at the concentration indicated in the following table:
Description Concentration (ng/ml) d-Amphetamine 50,000 l-Amphetamine 10,000 3,4-methylenedioxyamphetamine (MDA) 50,000
G. Morphine (MOR300) 1. Summary and Explanation of Test
Morphine is a popular marketed drug (e.g. Serax) for treatment of moderate to severe pain.3
It is also a common metabolite of Opiates [morphine, codeine (methyl-morphine), and heroin (semi-synthetic derivatives of morphine)]. The opiates are administered either by smoking, intravenous injection, intramuscular injection or oral ingestion. Adverse or toxic effects of opiates usage include pupillary constriction, constipation, urinary retention, nausea, vomiting, hypothermia, drowsiness, dizziness, apathy, confusion, respiratory depression, hypotension, cold and clammy skin, coma, and pulmonary edema. Death may occur following an overdosage.3,4 The duration of effect of morphine is 3-6 hours.3 Morphine is metabolized extensively, with only 2-12% excreted as unchanged morphine in urine. Heroin is rapidly metabolized to morphine in the body; the pattern of urinary excretion of heroin is similar to that of morphine. Codeine is also extensively metabolized, 10-15% of the dose is demethylated to form morphine and norcodeine. It has been reported that the unchanged morphine may remain detectable in urine for up to one week,3 which make morphine a marker of opiates abuse.
2. Accuracy A study was performed at three different Physician’s Office Laboratories (POL) and a Reference Laboratory. Ninety four (94) clinical samples were blind labeled and tested. Each sample was tested at each site, with INSTANT-VIEW Morphine (300) Urine Test, and compared with GC/MS results. The results from the INSTANT-VIEW Morphine (300) Urine Test agreed 100% with the GC/MS data of specimens at levels below 75% of the cutoff (negative) and above the cutoff (positive). Thirteen (13) discrepancies were observed on the specimens at the level between 75% of the cutoff and the cutoff. The overall agreement was 96.5%.
INSTANT-VIEW Test Positive Negative
Total Agreement
Drug-free 0 180 180 100% <75%(0~225) 0 12 12 100% 75%~Cutoff(225~300) 13 11 24 45.8% Cutoff~125%(300~375) 24 0 24 100%
GC/MS (ng/ml)
Positive(>375) 136 0 136 100% Total 173 203 376 96.5%
3. Reproducibility Reproducibility was determined at three different POL locations, by persons with diverse educational backgrounds and work experiences. Forty-pooled drug-free human urine specimens were spiked with morphine at different levels. All specimens were blind labeled and tested. The results are as follows:
POL 1 POL 2 POL 3 Morphine Conc. (ng/ml)
No of Samples + – + – + –
0 8 0 8 0 8 0 8 225 8 3 5 3 5 1 7 300 8 7 1 8 0 7 1 375 8 8 0 8 0 8 0 600 8 8 0 8 0 8 0
The results indicate a 92.5% concordance with the expected results. 4. Cross-Reactivity
To determine the cross-reactivity of the structurally related compounds with the device, the following compounds were spiked into known drug-free urine pools and tested with the INSTANT-VIEW Morphine Urine Test. Those compounds showed a positive response at the concentration indicated in the following table:
Morphine structurally related compounds showing the lowest concentration of the drug producing a positive response equivalent to the cutoff level: Description Concentration (ng/ml) Description Concentration (ng/ml) Morphine 300 Morphine-glucuronide 500 Codeine 300 Meperidine 30000 Ethyl Morphine 300 Oxycodone 1000 Hydromorphine 400
H. Morphine (MOR2000) 1. Summary and Explanation of Test
Morphine is a popular marketed drug (e.g. Serax) for treatment of moderate to severe pain.3
It is also a common metabolite of Opiates [morphine, codeine (methyl-morphine), and heroin (semi-synthetic derivatives of morphine)]. The opiates are administered either by smoking, intravenous injection, intramuscular injection or oral ingestion. Adverse or toxic effects of opiates usage include pupillary constriction, constipation, urinary retention, nausea, vomiting, hypothermia, drowsiness, dizziness, apathy, confusion, respiratory depression, hypotension, cold and clammy skin, coma, and pulmonary edema. Death may occur following an overdosage.3,4 The duration of effect of morphine is 3-6 hours.3 Morphine is metabolized extensively, with only 2-12% excreted as unchanged morphine in urine. Heroin is rapidly metabolized to morphine in the body; the pattern of urinary excretion of heroin is similar to that of morphine. Codeine is also extensively metabolized, 10-15% of the dose is demethylated to form morphine and norcodeine. It has been reported that the unchanged morphine may remain detectable in urine for up to one week,3 which make morphine a marker of opiates abuse.
2. Accuracy A study was performed at three different Physician’s Office Laboratories (POL) and a Reference Laboratory. One hundred (100) clinical samples were blind labeled and tested. Each sample was tested at each site, with INSTANT-VIEW Morphine (2000) Urine Test, and compared with GC/MS results. The results from the INSTANT-VIEW Morphine (2000) Urine Test agreed 100% with the GC/MS data of specimens at levels below 75% of the cutoff (negative) and above the cutoff (positive). Two (2) discrepancies were observed on the specimens at level between 75% of the cutoff and the cutoff. The overall agreement was 99.5%.
INSTANT-VIEW Test Positive Negative
Total
Agreement
Drug-free 0 132 132 100% <75% (0~1500) 0 64 64 100% 75%~Cutoff (1500~2000) 2 30 32 93.8% Cutoff~125% (2000~2500) 28 0 28 100%
GC/MS (ng/ml)
Positive (>2500) 144 0 144 100% Total 174 226 400 99.5%
3. Reproducibility Reproducibility was determined by replicate assays of four different levels of samples with three different production lots. The device was tested for five consecutive days for a total of 25 assays for each control. The results indicate 100% precision for the replicate within each lot, and no appreciable inter-lot variation across the three (3) different lots of devices.
4. Cross-Reactivity To determine the cross-reactivity of the structurally related compounds with the device, the following compounds were spiked into known drug-free urine pools and tested with the INSTANT-VIEW Morphine Urine Test. Those compounds showed a positive response at the concentration indicated in the following table:
Description Concentration (ng/ml) Description Concentration (ng/ml) Codeine 2000 Morphine- glucuronide 3000 Ethyl Morphine 2000 Meperidine 30,000 Hydro morphine 2500
I. Methadone (MTD) 1. Summary and Explanation of the Test
Methadone, also called Dolophine, Methadose and Amidone, possesses many of the pharmacological properties of morphine and is approximately equipotent as an analgesic when administered parenterally. Unlike morphine, however, methadone produces marked sedative effects with repeated administration as a result of drug accumulation. Methadone has been used as a major substitute for opiates, such as heroin, morphine, and codeine in drug maintenance treatment clinics. It is administered either orally or by intravenous or intra-muscular injection.3 The duration of effect of methadone is 12-24 hours.5 Its major urinary excretion products are methadone, EDDP (2-ethylidene-1, 5-dimethyl-3, 3-diphenylpyrrolidine), and EMDP (2-ethyl-5-methyl-3, 3-diphenylpyrrolidine). The percentage of methadone excreted unchanged in urine is 5-50%, much higher than EDDP and EMDP, of the dose in 24 hours. Large individual variations in the percentage of unchanged methadone excreted in urine have been observed due to urine pH, urine volume, dose and rate of metabolism, etc. Methadone has been found remaining in urine for higher than 1,000 ng/ml 24 hours after overdose.5 Therefore the concentration of methadone in human urine has been used as a marker of methadone abuse.
2. Accuracy A study was performed at three different Physician’s Office Laboratories (POL) and a Reference Laboratory. One hundred (100) clinical samples were blind labeled and tested.

INSTANT-VIEW Multi-Drug Screen Urine Test
33-2896 REV F 112204 Page 5
Each sample was tested at each site, with INSTANT-VIEW Methadone (MTD) Urine Test, and compared with GC/MS results. The results from the INSTANT-VIEW Methadone Urine Test agreed 100% with the GC/MS data of specimens at levels below 75% of the cutoff (negative) and above the cutoff (positive). Ten (10) discrepancies were observed on the specimens at level between 75% of the cutoff and the cutoff. The overall agreement was 97.5%.
INSTANT-VIEW Test Positive Negative
Total
Agreement
<75% (0~225) 0 192 192 100% 75%~Cutoff (225~300) 10 18 28 64.3% Cutoff~125% (300~375) 36 0 36 100%
GC/MS (ng/ml) Positive (>375) 144 0 144 100%
Total 190 210 400 97.5%
3. Reproducibility Reproducibility was determined by replicate assays of four different levels of samples with three different production lots. The device was tested for five consecutive days, five times each, for a total of 25 assays for each control. The results indicate 100% precision for the replicate within each lot and no appreciable interlot variation across the three (3) different lots of devices.
4. Cross-Reactivity To determine the cross-reactivity of the structurally related compounds with the device, the following compounds were spiked into known drug-free urine pools and tested with the INSTANT-VIEW Methadone Urine Test. Those compounds showed a positive response at the concentration indicated in the following table:
Description Concentration (ng/ml) (-)-α-Methadol 800 (-)-α-Acetylmethadol (LAAM) 1000
J. Phencyclidine (PCP) 1. Summary and Explanation of the Test
Phencyclidine (PCP), also named as Angel Dust, Hog, and Killer Weed, is a popular drug of abuse as well as a legitimate veterinary tranquilizer. It is self-administered either by smoking, nasal insufflation, intravenous injection or oral ingestion.3 Its duration of effect is 2-4 hours, and psychosis may last for weeks. PCP has three major metabolites; however, the percentage of an intravenous dose excreted unchanged in urine is 30-50% in the 72 hours. Only 2% of a dose is excreted in feces. An average of 77% of an intravenous dose is excreted in urine and feces in 10 days.3, 5 Therefore, the PCP in human urine has been used as a marker of PCP abuse.4 Concentrations of unchanged drug in the urine of ambulatory users of PCP are most frequently between 0.04 and 3.4mg/L.3
2. Accuracy A study was performed at three different Physician’s Office Laboratories (POL) and a Reference Laboratory. One hundred (100) clinical samples were blind labeled and tested. Each sample was tested at each site, with INSTANT-VIEW Phencyclidine (PCP) Urine Test, and compared with GC/MS results. The results from the INSTANT-VIEW Phencyclidine Urine Test agreed 100% with the GC/MS data of specimens at levels below 75% of the cutoff (negative) and above the cutoff (positive). Eight (8) discrepancies were observed on the specimens at level between 75% of the cutoff and the cutoff. The overall agreement was 98%.
INSTANT-VIEW Test Positive Negative
Total
Agreement
<75% (0~18.75) 0 184 184 100% 75%~Cutoff (18.75~25) 8 16 24 66.7% Cutoff~125% (25~31.25) 32 0 32 100%
GC/MS (ng/ml)
Positive (>31.25) 160 0 160 100% Total 200 200 400 98%
3. Reproducibility Reproducibility was determined by replicate assays of four different levels of samples with three different production lots. The device was tested for five consecutive days for a total of 25 assays for each control. The results indicate 100% precision for the replicate within each lot and no appreciable interlot variation across the three (3) different lots of devices.
4. Cross-Reactivity To determine the cross-reactivity of the structurally related compounds with the device, the following compounds were spiked into known drug-free urine pools and tested with the INSTANT-VIEW Phencyclidine(PCP) Urine Test. Those compounds showed a positive response at the concentration indicated in the following table:
Description Concentration ( ng/ml) Description Concentration (ng/ml) Methylphenidate 25,000 Tenocyclidine 2,000 Pheniramine 25,000
K. Propoxyphene (PPX) 1. Summary and Explanation of the Test
Propoxyphene is a prescription drug for the relief of pain. Propoxyphene hydrochloride (Darvon, Dolene, and others) is available in 32mg and 65mg capsules; propoxyphene napsylate (Darvon-N) is available in 100mg tablets or as a suspension. It is structurally related to methadone. Overdose of the drug can affect the brain region and cause euphoria as many opioids do. The progressive symptomatology of propoxyphene includes analgesia, stupor, respiratory depression, and coma, etc. The half-life of propoxyphene is 8-24 hours. Following oral administration, propoxyphene reaches its peak in 1 to 2 hours. There is great variability between subjects in the rate of clearance. The percentage of excreted unchanged propoxyphene in urine is less than 1%. The major metabolite of propoxyphene is norpropoxyphene. Therefore, the detection of norpropoxyphene is widely used for the
testing of propoxyphene abuse. The half-life of norpropoxyphene is about 30 hours, and its accumulation with repeated doses may be responsible for some of the toxicity observed.5, 6
2. Accuracy The accuracy of this device was determined by a comparison study between the INSTANT-VIEW Propoxyphene (PPX) Urine Test and the GC/MS. This study was conducted in house, using one hundred (100) blind labeled clinical urine specimens. The detailed data is listed in this section. The results from the INSTANT-VIEW Propoxyphene (PPX) Urine Test agreed 100% with the GC/MS data of specimens at levels below the cutoff (negative) and above 125% of the cutoff (positive). Two (2) discrepancies were observed on the specimens at the level between the cutoff and 125% of the cutoff. The overall agreement was 98%.
INSTANT-VIEW Test Positive Negative
Total
Agreement
Drug-free 0 40 40 100% <75% (0~225) 0 10 10 100% 75%~Cutoff (225~300) 0 10 10 100% Cutoff~125% (300~375) 8 2 10 80%
GC/MS (ng/ml)
Positive (>375) 30 0 30 100% Total 38 62 100 98%
3. Reproducibility Reproducibility of the device was determined by replicate assays with three different lots. Specimens used in this study were the same as used in the accuracy study. The devices were tested for five consecutive days five times each, for a total of 25 assays for each control. The results obtained indicate 100% precision for the replicate within each lot and no appreciable inter-lot variation across the three different lots of devices.
4. Cross-Reactivity Cross-reactivity of the propoxyphene structurally related compounds were evaluated with this device. The following compounds were spiked into known drug-free urine pools and then tested with the INSTANT-VIEW Propoxyphene (PPX) Urine Test. Propoxyphene and its major metabolite, norpropoxyphene, have a similar positive response at the concentration of 300 ng/ml. Other compounds tested produced positive responses at a very high concentration: methadone at 1,350,000 ng/ml and the metabolite of methadone (EDDP) at 200,000ng/ml.
Drugs or compounds Concentration Propoxyphene 300 ng/ml Norpropoxyphene 300 ng/ml Methadone 1,350,000 ng/ml 2-ethyl-1,5-dimethyl-3,3-diphenylpyrroline (EDDP, Methadone Metabolite)
200,000 ng/ml
L. Tricyclics (TCA) 1. Summary and Explanation of the Test
Tricyclics (TCA) are a group of antidepressant drugs that contain three fused rings in their chemical structure.7 TCA can be taken orally or by intramuscularly (IM). The progressive symptomatology of TCA includes agitation, confusion, hallucinations, hypertonicity, seizures, and EKG changes. The half-life of TCA varies from a few hours to a few days. The commonly used tricyclic antidepressants are excreted with a very low percentage of unchanged drugs in the urine, less than 1%. Therefore, detecting the metabolites of TCA in human urine has been used for screening the abuse of TCA.3, 5 This test is able to detect amitriptyline, desipramine, Imipramine and nortriptyline at a cutoff level of 1,000 ng/ml.
2. Accuracy The accuracy was determined by comparing the results from the INSTANT-VIEW TCA Urine Test with the GC/MS data. This study was carried out in house, using eighty (80) blind labeled clinical urine specimens. The detailed data is shown in the table in this section. The results from the INSTANT-VIEW TCA Urine Test agreed 100% with the TCA GC/MS data of specimens at levels below 75% of the cutoff (negative) and above the cutoff (positive). Two (2) discrepancies were observed on the specimens with the GC/MS data between 75% of the cutoff and the cutoff. The overall agreement was 97.5%.
INSTANT-VIEW Test Positive Negative
Total
Agreement
Drug-free 0 40 40 100% <75% (0~750) 0 10 10 100% 75%~Cutoff (750~1000) 2 8 10 80% Cutoff~125% (1000~1250) 8 0 8 100%
GC/MS (ng/ml)
Positive (>1250) 12 0 12 100% Total 22 58 80 97.5%
3. Reproducibility Reproducibility was determined by replicate assays of four different levels of samples with three different production lots. The devices were tested for five consecutive days five times each, for a total of 25 assays for each control. The results indicate 100% precision for the replicates within each lot and no appreciable inter-lot variation across the three different lots of devices.
4. Cross-Reactivity To determine the cross-reactivity of the structurally related compounds with the device, the following compounds were spiked into known drug-free urine pools and tested with the INSTANT-VIEW TCA Urine Test. Those compounds showed a positive response at the concentration indicated in the following table:
Description Concentration (ng/ml) Description Concentration (ng/ml) Nortriptyline 1,000 Clomipramine 5,000 Amitriptyline 1,000 Doxepin 3,000 Imipramine 800 Protriptyline 2,000 Desipramine 800 Perphenazine 75,000 Nordoxepine 1,000 Promazine 15,000 Cycolbenzaprine 1,500 Trimipramine 2,000

INSTANT-VIEW Multi-Drug Screen Urine Test
33-2896 REV F 112204 Page 6
M. Marijuana (THC) 1. Summary and Explanation of the Test
Tetrahydrocannabinol (THC, ∆-9-THC, ∆-1-THC), is the most active of the principal constituents, as well as the major metabolite of cannabinoids, such as marijuana and hashish. Cannabinoids have been used as central nervous system depressants. Overdose and extended usage of cannabinoids may lead to substance abuse, which may cause severe and/or permanent damage to the human nerve system. The detection of THC in human urine has been widely used to assess the abuse of cannabinoids. 2,3, 4
2. Accuracy A study was performed at three different Physician’s Office Laboratories (POL) and a Reference Laboratory. Ninety nine (99) clinical samples were blind labeled and tested. Each sample was tested at each site, with INSTANT-VIEW Marijuana (THC) Urine Test, and compared with GC/MS results. The results from the INSTANT-VIEW Marijuana (THC) Urine Test agreed 100% with the GC/MS data of specimens at levels below 75% of the cutoff (negative) and above 125% of the cutoff (positive). Fourteen (14) discrepancies were observed on the specimens at the level between 75% and 125% of the cutoff. The overall agreement was 96.5%.
INSTANT-VIEW Test Positive Negative
Total
Agreement
Drug-free 0 160 160 100% <75% (0~37.5) 0 36 36 100% 75%~Cutoff (37.5~50) 11 13 24 54.2% Cutoff~125% (50~62.5) 17 3 20 85%
GC/MS (ng/ml)
Positive (>62.5) 156 0 156 100% Total 184 212 396 96.5%
3. Reproducibility Reproducibility was determined at three different POL locations, by persons with diverse educational backgrounds and work experiences. Forty-pooled drug-free human urine specimens were spiked with THC at different levels. All specimens were blind labeled and tested. The results are as follows:
POL 1 POL 2 POL 3 THC Conc. (ng/ml)
No of Samples + – + – + –
0 8 0 8 0 8 0 8 37.5 8 0 8 1 7 0 8 50 8 8 0 8 0 8 0
62.5 8 8 0 8 0 8 0 100 8 8 0 8 0 8 0
The results indicate a 99.2 % concordance with the expected results. 4. Cross-Reactivity
A study was conducted using THC-related compounds to determine the cross-reactivity of the test.
THC structurally related compounds showing the lowest concentration of the drug producing a positive response equivalent to the cutoff level: Description Concentration (ng/ml) 11-nor-∆-8-THC-9-COOH 50 11-nor-∆-9-THC-9-COOH 50 11-hydroxy-∆-9-THC 100 9-Tetrahydrocannabinol 10,000 Cannabonol 10,000
N. MDMA (Ecstasy, XTC) 1. Summary and Explanation of the Test
MDMA is an abbreviation for the chemical methylenedioxymethamphetamine. It has many street names including Ecstasy, X, XTC, E, Love Doves, Clarity, Adam, Disco Biscuits and Shamrocks. It is a stimulant with hallucinogenic tendencies described as an empathogen as it releases mood-altering chemicals, such as cartooning and L-dopa, in the brain and may generate feelings of love and friendliness. MDMA is a Class A drug, in the same category as heroin and cocaine. The adverse effects of MDMA use include elevated blood pressure, hyperthermia, anxiety, paranoia, and insomnia. Overdose of MDMA can be fatal, often resulting in heart failure or heat stroke.5, 8 MDMA belongs to a family of man-made drugs; its relatives include MDA (methylenedioxyamphetamine), the parent drug of MDMA, and MDEA (methylenedioxyethylamphetamine), also know as EVE. They all share the amphetamine-like effects. MDMA is administered either by oral ingestion or intravenous injection. MDMA tablets come in different sizes and colors, and often have logos such as doves on them. Its clinical dose is 50-100mg; the threshold toxic dose is 500mg. The effects of MDMA begin 30 minutes after intake. They peak in an hour and last for 2-3 hours. Sixty five percent (65%) of MDMA is excreted unchanged in urine: it is detectible in the urine for up to 3 days after use.5,8
2. Accuracy The accuracy was determined by comparing the results from the INSTANT-VIEW MDMA Urine Test with the GC/MS data. This study was carried out in house, using eighty (80) blind labeled clinical urine specimens. The detailed data is shown in the table in this sections. The results from the INSTANT-VIEW MDMA (Ecstasy, XTC) Urine Test agreed 100% with the MDMA GC/MS data of specimens at levels below 75% of the cutoff (negative) and above the cutoff (positive). Two (2) discrepancies were observed on the specimens with the GC/MS data between 75% of the cutoff and the cutoff. The overall agreement was 97.5%.
INSTANT-VIEW Test Positive Negative
Total
Agreement
Drug-free 0 40 40 100% <75% (0~375) 0 10 10 100% 75%~Cutoff (375~500) 2 9 11 82% Cutoff~125% (500~625) 9 0 9 100%
GC/MS (ng/ml)
Positive (>625) 10 0 10 100% Total 21 59 80 97.5%
3. Reproducibility The reproducibility study on this test was performed outside of Alfa facility, at three (3) Physician’s Office Laboratories (POL) and a clinical reference laboratory by personnel with diverse educational backgrounds and working experiences. One hundred and ten (110) MDMA-spiked urine samples containing six different levels of MDMA: 0, 257, 378, 615, 709, and 1417 ng/ml (determined by GC/MS), were used for this study. The results are summarized in the following table.
Samples Test Site I Test Site II Test Site III Test Site IV Total Number 15 15 15 15 60 0
ng/ml Result 15- 15- 15- 15- 60- Number 15 15 15 15 60 257
ng/ml Result 15- 15- 15- 15- 60- Number 25 25 25 25 100 378
ng/ml Result 25- 25- 25- 25- 100- Number 25 25 25 25 100 615
ng/ml Result 23+, 2- 23+, 2- 22+, 3- 24+, 1- 92+, 8- Number 15 15 15 15 60 709
ng/ml Result 15+ 14+, 1- 15+ 15+ 59+, 1- Number 15 15 15 15 60 1417
ng/ml Result 15+ 15+ 15+ 15+ 60+
At the four evaluation sites, two hundred and twenty (220) devices tested with samples containing less than 378 ng/ml MDMA (75% of the cutoff) were negative (100% agreement). Among the one hundred (100) devices tested with samples containing 615 ng/ml MDMA (125% of the cutoff), ninety two (92) were positive and eight (8) were negative (92% agreement). For the sixty (60) devices tested with samples containing 709 ng/ml MDMA (150% of the cutoff), fifty nine (59) were positive and one (1) was negative (98.3% agreement). The sixty (60) devices tested with samples containing 1417 ng/ml MDMA were all positive. No significant within-day, between-day, or between-assay discrepancy was observed. The results obtained from the four evaluation sites agreed 97.5% with each other, indicating a high reproducibility of the device.
4. Cross-Reactivity The cross-reactivity of the structurally related compounds with the device was studied. The following compounds were spiked into known drug-free urine pools and tested with the MDMA Urine Test. Compounds produced positive results at a concentration below 10µg/ml are indicated in the following table:
Description Concentration (ng/ml) methylenedioxyampphetamine (MDA) 2000 Methylenedioxyethylamphetamine(MDEA) 1000
Compounds that did not produce positive responses at a concentration of 100µg/ml are indicated in the following table:
Description Concentration (µg/ml) L-amphetamine 100 d-amphetamine 100 L-methamphetamine 100 d-methamphetamine 100 Hydroxymethamphetamine (HAM) 100 Dihydroxymethamphetamine (HMMA) 100 N-methyl-1-(1-3-benzodioxol-5-yl)-2-butanamine(MBDB) 100
REFERENCES 1. FDA Guidance for Labeling Urine Drugs of Abuse Screening Testing, Kshit Mohan, 7/21. 2. Urine Testing for Drugs of Abuse. National Institute on Drug Abuse (NIDA): Research
Monograph 73, 1986. 3. Baselt, R.C. Disposition of Toxic Drugs and Chemicals in Man, 4th ED., Biomedical
Publ., Davis, CA; p713-715, 1995. 4. Department of Health and Human Services, Mandatory Guidelines for Federal Workplace
Drug Testing Programs, Fed. Register. (69): 11970 (1988). 5. Wilson, John, Abused Drugs II, a Laboratory Pocket Guide., AACC Press. Washington,
DC; 1994. 6. Gilman AG, Rall TW, Nies AS, Taylor P eds., Goodman and Gilman’s the
Pharmacological Basis of Therapeutics, 8th ed., New York, Pergamon Press, 1990. 7. Dorland’s Illustrated Medical Dictionary, 26th Edition, W.B. Saunders Company,
Philadelphia, PA, pp89, 1981. 4Urine Testing for Drugs of Abuse, National Institute on Drug Abuse (NIDA): Research Monograph 73, 1986.
8. S-J. Peroutka ed. Ecstasy: The clinical, pharmacological and neurotoxicological effects of the drug MDMA. Kluwer Academic Publishers, 1990.
Manufactured for: CLIAwaived,Inc. SAN DIEGO, CA 92130 - USA MADE IN USA
WWW.DRUGTESTING-KITS.COM WWW.CLIAWAIVED.COM
INSTANT-VIEW Multi-Drug Screen Urine Test
Análisis de orina para la detección de diversas drogas
33-xxxx REV X XXXX Page 1
INSTRUCCIONES DE USO Análisis de un solo paso Rápidos resultados visuales Para uso diagnóstico cualitativo in vitro, por profesionales INDICACIONES DE USO Y RESUMEN DE LAS PRUEBAS
The INSTANT-VIEW Multi-Drug Screen Urine Test (análisis de orina para la detección de diversas drogas) es un inmunoanálisis cualitativo, cuyo empleo está indicado para detectar la presencia de drogas o de metabolitos de drogas en la orina humana, en sus concentraciones de corte especificadas, en un solo análisis. Su empleo está indicado únicamente para profesionales de la atención sanitaria. The INSTANT-VIEW Multi-Drug Screen Urine Test proporciona sólo un resultado analítico preliminar. Para confirmar este resultado analítico debe emplearse otro método químico más específico. El método confirmatorio preferido es la cromatografía de gases / espectrofotometría de masas. Al interpretar los resultados positivos preliminares de un análisis de drogas, deberá aplicarse el criterio clínico y profesional.1 El inmunoanálisis de drogas en la orina se ha convertido en uno de los métodos más aceptados de detección preliminar. Estos análisis permiten a los laboratorios eliminar una gran cantidad de muestras negativas y concentrarse en un número más pequeño de muestras inicialmente positivas.
PRINCIPIO DEL PROCEDIMIENTO El análisis INSTANT-VIEW es un inmunoanálisis cromatográfico de flujo lateral y de un solo paso, con tiras de pruebas que consisten en: 1) una compresa de conjugado, de color borgoña, que contiene oro coloidal conjugado con anticuerpos contra las drogas, y 2) una membrana de nitrocelulosa que contiene una línea de prueba (línea T) y una línea de control (línea C). La línea T está recubierta con el antígeno de la droga; la línea C está recubierta con anticuerpo IgG de antirratón de cabra. Este ensayo es un inmunoanálisis de unión competitiva. La droga o metabolito de droga presente en la muestra de orina compite con el antígeno recubierto de la membrana de nitrocelulosa por los sitios de unión limitados del anticuerpo de la compresa de conjugado. Si se aplica una cantidad suficiente de muestra de orina a la compresa para la muestra del equipo, la orina migra por capilaridad por las tiras de prueba. Si la concentración de droga en la muestra es inferior a la concentración de corte, el conjugado de color borgoña se unirá a los antígenos recubiertos de la membrana de nitrocelulosa (línea de prueba) y forma una línea T de color borgoña, lo que indica un resultado negativo. Si la droga está presente en la muestra de orina a una concentración de corte o más alta de la tira de prueba, se unirá a los anticuerpos conjugados, así que no se desarrolla una línea T, lo que indica un resultado positivo. El conjugado coloreado de oro-anticuerpo deberá unirse a la línea C y formar una banda de color borgoña, con independencia de la droga.
REACTIVOS Y MATERIALES SUMINISTRADOS • 25 equipos de análisis, cada uno de ellos sellado en una bolsa de papel de
aluminio, con desecante y una pipeta gotero (20 equipos, si se trata de un perfil de 7 a 12 pruebas)
• 1 Instrucciones de uso
MATERIAL NECESARIO PERO NO SUMINISTRADO • Recipientes para la recogida de muestra • Cronómetro
CONSERVACIÓN Y ESTABILIDAD Mantener el equipo a temperatura ambiente (15 a 30 ºC). Cada equipo puede utilizarse hasta la fecha de caducidad impresa en la etiqueta si se mantiene sellada en su bolsa de papel aluminio, que contiene desecante. No exponer el equipo a temperaturas superiores a 30 ºC(86°F).
RECOGIDA Y CONSERVACIÓN DE LAS MUESTRAS Cada muestra de orina debe recogerse en un recipiente limpio. No mezcle las muestras. Las muestras pueden mantenerse a temperatura ambiente durante ocho horas; a 2 a 8 ºC durante tres días como máximo, y a –20 ºC o más baja, para una conservación prolongada. No combinar las muestras. Las muestras de orina que presentan precipitados visibles deberán filtrarse o centrifugarse, y deberán dejarse asentar. Utilice sólo alícuotas transparentes para los análisis.
ATENCIÓN 1. Para obtener unos resultados exactos, deben seguirse las instrucciones. 2. No abra la bolsa sellada, a menos que esté listo para realizar el análisis.
3. No utilice equipos caducados. 4. Elimine todas las muestras y todos los materiales usados como
material con posible peligro biológico.
PROCEDIMIENTO DEL ANÁLISIS 1. Las muestras refrigeradas y otros materiales de análisis, incluidos los
equipos, deben equilibrarse a temperatura ambiente antes de los análisis.
2. Extraiga el equipo de análisis de la bolsa y etiquételo con la identificación de la muestra.
3. Realice el análisis:
MÉTODO DE INMERSIÓN a) Extraiga el tapón y sumerja el equipo en la muestra durante 10
segundos como mínimo. La superficie de la muestra debe quedar por encima del pocillo de la muestra y debajo del nivel de las flechas en la ventana. b) Extraiga el equipo de la muestra después de 10 segundos.
PROCEDIMIENTO OPTATIVO (recomendado para muestras de bajo volumen):
a) Extraiga el tapón. Retire la pipeta de la bolsa. b) Oprima el bulbo para llenar la pipeta con la muestra hasta la
línea del tambor. Coloque toda la muestra en el pocillo. En el caso de los paneles bilaterales (7 a 2 pruebas), repita la adición de las muestras por pipeta en la cara 2.
4. Vuelva a colocar el tapón en el equipo y colóquelo sobre una superficie plana y seca.
5. Lea el resultado de la prueba de cuatro (4) a siete (7) minutos después de colocar la muestra.
IMPORTANTE: No lea los resultados de la prueba después de (7) minutos.
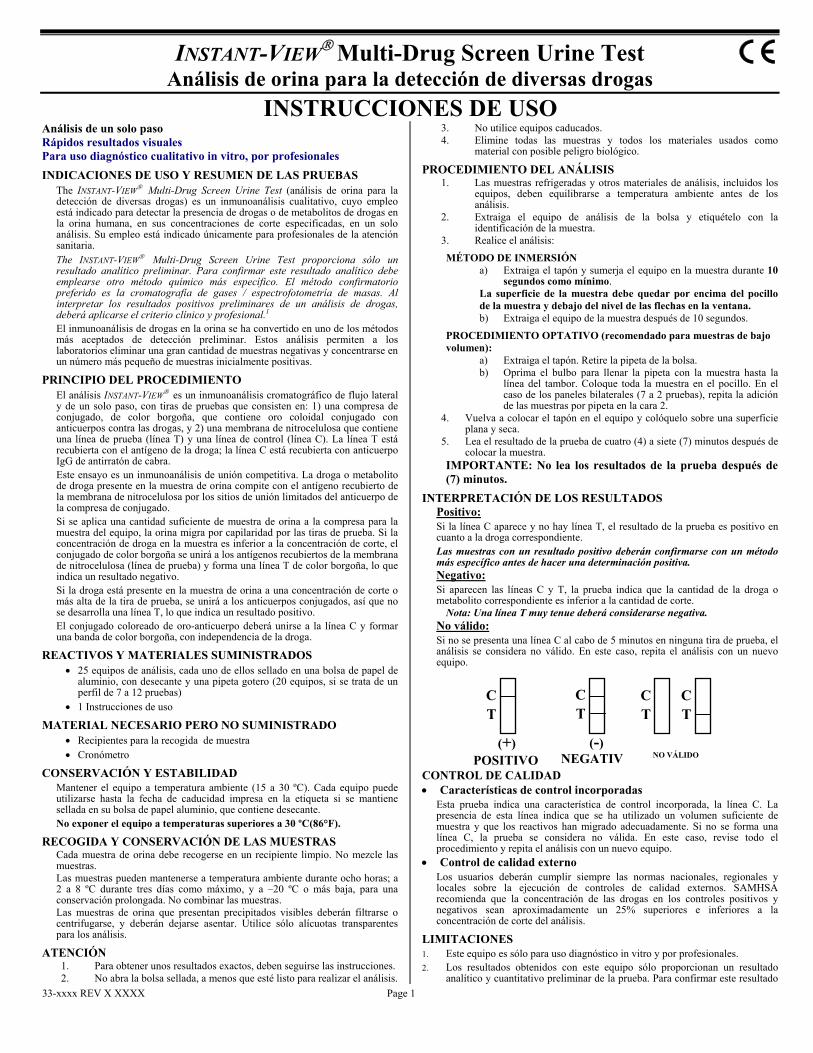
INTERPRETACIÓN DE LOS RESULTADOS Positivo: Si la línea C aparece y no hay línea T, el resultado de la prueba es positivo en cuanto a la droga correspondiente. Las muestras con un resultado positivo deberán confirmarse con un método más específico antes de hacer una determinación positiva. Negativo: Si aparecen las líneas C y T, la prueba indica que la cantidad de la droga o metabolito correspondiente es inferior a la cantidad de corte.
Nota: Una línea T muy tenue deberá considerarse negativa. No válido: Si no se presenta una línea C al cabo de 5 minutos en ninguna tira de prueba, el análisis se considera no válido. En este caso, repita el análisis con un nuevo equipo.
CONTROL DE CALIDAD • Características de control incorporadas
Esta prueba indica una característica de control incorporada, la línea C. La presencia de esta línea indica que se ha utilizado un volumen suficiente de muestra y que los reactivos han migrado adecuadamente. Si no se forma una línea C, la prueba se considera no válida. En este caso, revise todo el procedimiento y repita el análisis con un nuevo equipo.
• Control de calidad externo Los usuarios deberán cumplir siempre las normas nacionales, regionales y locales sobre la ejecución de controles de calidad externos. SAMHSA recomienda que la concentración de las drogas en los controles positivos y negativos sean aproximadamente un 25% superiores e inferiores a la concentración de corte del análisis.
LIMITACIONES 1. Este equipo es sólo para uso diagnóstico in vitro y por profesionales. 2. Los resultados obtenidos con este equipo sólo proporcionan un resultado
analítico y cuantitativo preliminar de la prueba. Para confirmar este resultado
CT
C T
C T
CT
POSITIVO NEGATIV NO VÁLIDO (+) (-)

INSTANT-VIEW Multi-Drug Screen Urine Test
33-xxxx REV x xxxxxx Page 2
analítico debe emplearse otro método químico más específico. 3. Este producto está destinado únicamente a los análisis en la orina humana. 4. Los adulterantes tales como lejía u otros agentes oxidantes fuertes pueden dar
unos resultados erróneos del análisis si se añaden al equipo. Si se sospecha su presencia, recoja una nueva muestra y repita la prueba con un equipo nuevo.
5. No deberán utilizarse muestras si se sospecha la presencia de contaminación bacteriana en las mismas. Estos contaminantes pueden interferir con la prueba y dar resultados falsamente negativos.
VALORES ESPERADOS Esta prueba puede detectar cada droga o metabolito de droga especificado en la orina humana a su concentración de corte especificada o superior a la misma.
CARACTERÍSTICAS DEL RENDIMIENTO Los equipos INSTANT-VIEW para el análisis de diversas drogas son inmunoanálisis cualitativos cuyo uso está indicado para profesionales de la atención sanitaria, con la finalidad de detectar el posible consumo abusivo de una o más drogas en un solo análisis. Se fabrican distintos equipos para detectar diferentes cantidades y combinaciones de drogas. A continuación, se resumen los atributos de rendimiento de cada una de las pruebas que puede haber en un perfil determinado del equipo INSTANT-VIEW.
SENSIBILIDAD (VALOR DE CORTE): Cada análisis se desarrolla para detectar la presencia de una droga o metabolito* de una droga a la cantidad de corte especificada o más. En todos los análisis, el resultado deberá considerarse claramente negativo si la muestra tiene una concentración de la droga inferior al 75% de la concentración de corte, y positivo si la concentración es superior al 125% del valor de corte. A continuación, se enumeran las drogas y sus valores de corte: AMP - Anfetamina…… 1000 ng/ml MOR - Morfina……… 2000 ng/ml BAR - Barbitúricos……… 200 ng/ml MTD - Metadona……… 300 ng/ml BZD - Benzodiazepinas… 300 ng/ml PCP - Fenciclidina…… 25 ng/ml COC - Cocaína………… 300 ng/ml PPX - Propoxifeno… 300 ng/ml MET - Metanfetamina** 500 ng/ml TCA - Tricíclicos……… 1000 ng/ml MET - Metanfetamina… 1000 ng/ml THC - Marihuana/Hachís 50 ng/ml MOR - Morfina**……… 300 ng/ml XTC - MDMA o éxtasis 500 ng/ml
*Los metabolitos detectados en estas pruebas se enumeran en los siguientes apartados:
**Pueden analizarse, pero no concentraciones SAMHSA.
INTERFERING SUBSTANCES: Sustancias que interfieren: Para determinar la interferencia de analitos estructuralmente no relacionados, se evaluó cada analito de prueba, con el equipo de análisis de orina Instant-View específico según el analito, tanto en muestras de orina mezcladas, sin drogas, como en muestras mezcladas a las que se añadió el valor de corte de cada analito enumerado en la siguiente tabla...
Se observó que las sustancias comunes enumeradas en esta tabla no interfieren con los resultados de análisis a la concentración de 100 µg/ml Paracetamol Ácido oxálico Etanol Ácido acetilsalicílico Cafeína Lidocaína Amikacina (+)-Clorfeniramina Penicilina G Amitriptilina Cocaína Fenilpropanolamina Ampicilina Codeína Ranitidina Arterenal Cortisona Ácido salicílico Aspirina Metadona Tioridazina Atropina Metanol Trifluoperazina Ácido benzoico
Analitos biológicos Concentración Analitos biológicos Concentración Albúmina 200 µg/ml pH 5.0 – 9.0 Bilirrubina 100 µg/ml Gravedad específica 1.002 – 1.035 g/ml Creatina 100 µg/ml Ácido úrico 100 µg/ml Glucosa 200 µg/ml Hemoglobina 100 µg/ml
Vitamina C (ácido L-ascórbico)
100 µg/ml
Existe la posibilidad de que otras sustancias o factores no enumerados interfieran con el análisis y den resultados falsos.
A. Anfetamina (AMP) 1. Resumen y explicación de la prueba
La detección de anfetaminas en la orina humana ha tenido un uso extendido para evaluar el consumo abusivo de anfetaminas, que son drogas que estimulan el sistema nervioso central. Pueden inducir un estado de alerta, falta de sueño, aumento de energía, disminución del hambre y sensación general de bienestar. La sobredosis y el consumo prolongado de anfetaminas pueden ser causantes del abuso de la droga, que puede causar un daño grave o permanente del sistema nervioso del ser humano. Las anfetaminas aparecen en la orina a las tres horas de su administración (cualquier tipo) y pueden estar presentes aproximadamente 24 a 48 horas después de la última dosis.2,3, 4
2. Exactitud Se realizó un estudio en tres laboratorios de distintas consultas de médicos y en un laboratorio de referencia. Ciento diecinueve (119) muestras clínicas se enmascararon y examinaron. Cada muestra se examinó en cada sitio, con INSTANT-VIEW Amphetamine, y se comparó con los resultados de cromatografía de gases y espectrofotometría de masas (CG/EM).
Los resultados obtenidos con el análisis de orina Amphetamine Urine Test INSTANT-VIEW tuvieron una concordancia del 100% con los datos obtenidos con la cromatografía de gases / espectrofotometría de masas, a concentraciones inferiores al 75% del valor de corte (negativo) y superiores al 125% del valor de corte (positivo). Se observaron 38 discrepancias en las muestras, a la concentración entre el 75% y el 125% del valor de corte. La concordancia total fue del 92,0%.
Análisis INSTANT-VIEW Positivo Negativo
Total Concordancia
Sin drogas 0 176 176 100% <75% (0~750) 0 76 76 100% 75%~ Corte (750~1000) 37 23 60 38.3% Corte ~125% (1000~1250) 15 1 16 93.8%
CG/EM (ng/ml)
Positivo (>1250) 148 0 148 100% Total 200 276 476 92.0%
3. Reproducibilidad Se determinó la reproducibilidad en tres laboratorios distintos de consultas (CONS), por personas con distintas formaciones y experiencias de trabajo. A 40 muestras de orina humana mezcladas, sin drogas, se añadió anfetamina a concentraciones distintas. Todas las muestras fueron enmascaradas y examinadas. Los resultados son los siguientes:
CONS 1 CONS 2 CONS 3 Conc. anf. (ng/ml)
Núm. de muestras + – + – + –
0 8 0 8 0 8 0 8 750 8 4 4 0 8 2 6 1000 8 8 0 8 0 8 0 1250 8 8 0 8 0 8 0 2000 8 8 0 8 0 8 0
Los resultados indican una concordancia del 95,0% con los resultados esperados. 4. Reactividad cruzada
Se realizó un estudio con compuestos relacionados con la anfetamina para determinar la reactividad cruzada de la prueba.
Compuestos relacionados con la anfetamina que muestran la concentración más baja de la droga que produce una respuesta positiva equivalente al valor de corte. Compuestos Concentración (ng/ml) Compuestos Concentración (ng/ml)
d-anfetamina 1000 l-anfetamina 20,000 d,l-anfetamina 1000
3,4- metilendioxianfetamina (MDA)
3000
B. Barbitúricos (BAR) 1. Resumen y explicación de la prueba
Los barbitúricos son depresores del sistema nervioso central y se emplean como sedantes hipnóticos. La sobredosis y el consumo prolongado de barbitúricos pueden ocasionar un daño grave o permanente del sistema nervioso del ser humano.2 Los barbitúricos se clasifican como: (1) ultracortos, (2) cortos-intermedios y (3) prolongados. La duración de los compuestos de acción ultracorta: secobarbital, pentobarbital, etc., es de quince (15) minutos a seis (6) horas. La duración de los compuestos de acción intermedia: amobarbital, etc., es de tres (3) a veinticuatro (24) horas. La duración de los compuestos de acción prolongada: fenobarbital, etc., es de quince (15) a cuarenta y ocho (48) horas.3,5 Los barbitúricos consumidos con mayor frecuencia como drogas son los de acción corta o intermedia; los de acción prolongada rara vez son consumidos de manera abusiva como drogas. Los derivados de los barbitúricos se excretan por la orina en cantidades variables del fármaco inalterado y los metabolitos.5 Los barbitúricos de acción prolongada se excretan en un porcentaje más alto de droga inalterada en la orina, mientras que los de acción más corta, secobarbital y amobarbital, se metabolizan de manera extensa y se excretan por la orina con un porcentaje más bajo de drogas inalteradas.2,3 INSTANT-VIEW Barbiturate Urine Test (análisis de barbitúricos en la orina) ha sido diseñada para detectar secobarbital inalterado en la orina; sin embargo, como ocurre con otros métodos analíticos tales como EMIT y RIA, este análisis también puede detectar otros barbitúricos encontrados con frecuencia, en función de la concentración del fármaco presente en la muestra. Se han observado resultados positivos a fenobarbital en consumidores crónicos hasta varias semanas después de interrumpir el consumo. Con dosis únicas estándar de secobarbital, pentobarbital o amobarbital, pueden identificarse resultados positivos desde 30 horas hasta 76 horas después.2
2. Exactitud Se realizó un estudio en tres laboratorios de distintas consultas de médicos y en un laboratorio de referencia. Cien (100) muestras clínicas se enmascararon y examinaron. Cada muestra se examinó en cada sitio, con INSTANT-VIEW Barbiturate Test, y se comparó con los resultados de cromatografía de gases y espectrofotometría de masas (CG/EM). Los resultados obtenidos con el análisis de orina Barbiturate Urine Test INSTANT-VIEW tuvieron una concordancia del 100% con los datos obtenidos con la cromatografía de gases / espectrofotometría de masas, a concentraciones inferiores al 75% del valor de corte (negativo) y superiores al 125% del valor de corte (positivo). Se observó una (1) discrepancia en las muestras, a la concentración entre el 75% y el 125% del valor de corte. La concordancia total fue del 99.8%.
Análisis INSTANT-VIEW Positivo Negativo
Total Concordancia
Sin drogas 0 200 200 100% <75% (0~150) 0 12 12 100% 75%~ Corte (150~200) 0 20 20 100% Corte ~125% (200~250) 27 1 28 96.4%
CG/EM (ng/ml)
Positivo (>250) 140 0 140 100% Total 167 233 400 99.8%
3. Reproducibilidad Se determinó la reproducibilidad mediante análisis repetidos en cuatro niveles distintos de muestras, con tres lotes de producción diferentes. Se examinaron los equipos durante cinco días consecutivos, cinco veces cada día, hasta un total de 25 análisis por cada control. Los resultados indican una precisión intralote del 100% de la repetición y ninguna variación apreciable entre lotes entre los tres lotes distintos de equipos.

INSTANT-VIEW Multi-Drug Screen Urine Test
33-xxxx REV x xxxxxx Page 3
4. Reactividad cruzada Para determinar la reactividad cruzada de los compuestos estructuralmente relacionados con el equipo, se añadieron los siguientes compuestos a muestras de orina mezcladas, sin drogas, y se examinaron con el análisis de orina INSTANT-VIEW Barbiturate Urine Test. Estos compuestos mostraron una respuesta positiva a la concentración indicada en la siguiente tabla:
Descripción Concentración (ng/ml) Descripción Concentración (ng/ml) Amobarbital 250 Fenobarbital 200
Barbital 250 Pentobarbital 250 Butabarbital 300 Secobarbital 200
Butalbital 200
C. Benzodiazepinas (BZD) 1. Resumen y explicación de la prueba
Las benzodiazepinas, entre ellas alprazolam, diazepam, lorazepam, triazolam, clordiazepóxido, flurazepam y temazepam son fármacos sedantes, hipnóticos y ansiolíticos que se emplean habitualmente como tranquilizantes orales. La mayoría de las benzodiazepinas se metaboliza ampliamente en el hígado y se excretan por la orina como metabolitos.3 Tienen un potencial bajo de dependencia física o psicológica. Sin embargo, lo mismo que otros estimulantes del sistema nervioso central, pueden inducir somnolencia y relajación muscular. El abuso crónico de benzodiazepinas puede producir una intoxicación similar a la conducta del alcohólico. La sobredosis y el consumo prolongado de benzodiazepinas pueden causar coma y, posiblemente, la muerte. Las benzodiazepinas pueden permanecer eficaces durante 4 a 8 horas.3,5 Los miembros de la familia de las benzodiazepinas se absorben a distintas velocidades y sus efectos pueden variar con la tasa de absorción. Se excretan por la orina principalmente como los compuestos originales o como un metabolito inactivo, glucurónido de oxazepam, que sólo son detectables durante uno o dos días Oxazepam, un metabolito común de muchas benzodiazepinas, también se comercializa como Serax; puede mantenerse detectable en la orina durante un período de hasta una semana.3 Ello hace que el oxazepam sea un marcador útil del abuso de benzodiazepinas.
2. Exactitud Se realizó un estudio en tres laboratorios de distintas consultas de médicos y en un laboratorio de referencia. Cien (100) muestras clínicas se enmascararon y examinaron. Cada muestra se examinó en cada sitio, con INSTANT-VIEW Benzodiazepine Test, y se comparó con los resultados de cromatografía de gases y espectrofotometría de masas (CG/EM). Los resultados obtenidos con el análisis de orina Benzodiazepine Urine Test INSTANT-VIEW tuvieron una concordancia del 100% con los datos obtenidos con la cromatografía de gases / espectrofotometría de masas, a concentraciones inferiores al 75% del valor de corte (negativo) y superiores al 125% del valor de corte (positivo). Se observaron siete (7) discrepancias en las muestras, a la concentración entre el 75% y el 125% del valor de corte. La concordancia total fue del 98,3%.
Análisis INSTANT-VIEW Positivo Negativo
Total Concordancia
Sin drogas 0 168 168 100% <75% (0~225) 0 24 24 100% 75%~Corte (225~300) 7 25 32 78% Corte~125% (300~375) 32 0 32 100%
CG/EM (ng/ml)
Positivo (>375) 144 0 144 100% Total 183 217 400 98.3%
3. Reproducibilidad Se determinó la reproducibilidad mediante análisis repetidos en cuatro niveles distintos de muestras, con tres lotes de producción diferentes. Se examinó el equipo durante cinco días consecutivos, cinco veces cada día, hasta un total de 25 análisis por cada control. Los resultados indican una precisión intralote del 100% de la repetición y ninguna variación apreciable entre lotes entre los tres lotes distintos de equipos.
4. Reactividad cruzada Para determinar la reactividad cruzada de los compuestos estructuralmente relacionados con el equipo, se añadieron los siguientes compuestos a muestras de orina mezcladas, sin drogas, y se examinaron con la prueba de orina INSTANT-VIEW Benzodiazepine Urine Test. Estos compuestos mostraron una respuesta positiva a la concentración indicada en la siguiente tabla:
Descripción Concentración (ng/ml) Descripción Concentración (ng/ml) Alprazolam 300 Lormetazepam 300 Bromazepam 500 Medazepam 300 Clobazem 1500 Nitrazepam 250 Clonazepam 500 Nordiazepam 400 Diazepam 200 Prazepam 250 Desmetildiazepam 300 Triazolam 300 Flurazapam 300 Oxazepam 300 Lorazepam 450
D. Cocaína (COC) 1. Resumen y explicación de la prueba
La cocaína es uno de los estimulantes del sistema nervioso que tiene propiedades farmacológicas, tales como anestésico local. Tiene unos efectos aditivos que se traducen en el abuso de la droga. La cocaína puede aparecer en la orina sólo unas horas después de su consumo, mientras que la benzoilecgonina, un producto de degradación hidrolítica de la cocaína, puede detectarse en la orina más de dos días después de su consumo. Por lo tanto, se ha empleado ampliamente la detección de benzoilecgonina en la orina humana para evaluar el consumo de cocaína.2,3,4
2. Exactitud Se realizó un estudio en tres laboratorios de distintas consultas de médicos y en un laboratorio de referencia. Cien (100) muestras clínicas se enmascararon y examinaron. Cada muestra se examinó en cada sitio, con INSTANT-VIEW Cocaine (Benzoylecgonine)
Test, y se comparó con los resultados de cromatografía de gases y espectrofotometría de masas (CG/EM). Los resultados obtenidos con el análisis de orina Cocaine (Benzoylecgonine) Urine Test INSTANT-VIEW tuvieron una concordancia del 100% con los datos obtenidos con la cromatografía de gases / espectrofotometría de masas, a concentraciones inferiores al 75% del valor de corte (negativo) y superiores al 125% del valor de corte (positivo). Se observaron nueve (9) discrepancias en las muestras, a la concentración entre el 75% y el 125% del valor de corte. La concordancia total fue del 97,8%.
Análisis INSTANT-VIEW Positivo Negativo
Total Concordancia
Sin drogas 0 188 188 100% <75% (0~225) 0 4 4 100% 75%~Corte (225~300) 9 11 20 55% Corte~125% (300~375) 24 0 24 100%
CG/E
M (ng/ml) Positivo (>375) 164 0 164 100%
Total 197 203 400 97.8%
3. Reproducibilidad Se determinó la reproducibilidad en tres laboratorios distintos de consultas (CONS), por personas con distintas formaciones y experiencias de trabajo. A 40 muestras de orina humana mezcladas, sin droga, se añadió benzoilecgonina a concentraciones distintas. Todas las muestras fueron enmascaradas y examinadas. Los resultados son los siguientes:
CONS 1 CONS 2 CONS 3 Conc. benzod. (ng/ml)
Núm. de muestras + – + – + –
0 8 0 8 0 8 0 8 225 8 5 3 2 6 0 8 300 8 8 0 8 0 8 0 375 8 8 0 8 0 8 0 600 8 8 0 8 0 8 0
Los resultados indican una concordancia del 94,2% con los resultados esperados. 4. Reactividad cruzada
Se realizó un estudio con compuestos relacionados con la cocaína para determinar la reactividad cruzada de la prueba.
Cocaína y sus compuestos estructuralmente relacionados que muestran la concentración más baja de la droga que produce una respuesta positiva equivalente al valor de corte: Descripción Concentración (ng/ml) Descripción Concentración (ng/ml) Cocaína 300 Isoxsuprina 1500 Benzoilecgonina 300
E. Metanfetamina (MET500) 1. Resumen y explicación de la prueba
La metanfetamina, en sobredosis, produce intranquilidad, confusión, ansiedad, alucinaciones, arritmias cardíacas, hipertensión, hipertermia, colapso circulatorio, convulsiones y coma.3 La metanfetamina se ha implicado en intoxicaciones mortales después de su administración tanto por vía intravenosa como oral. Los consumidores crónicos pueden presentar una psicosis paranoide.1 La D-metanfetamina (d-desoxiefedrina, Desoxyn, Methedrine) es el derivado N-metil de la anfetamina. Se utiliza en el tratamiento de la obesidad. La metanfetamina se administra por vía oral, insuflación nasal o inyección intravenosa, con una duración de dos a cuatro horas.3,5 La metanfetamina es sometida, en parte, a N-desmetilación y se convierte en anfetamina, su principal metabolito activo. En condiciones normales, hasta el 43% de la dosis se elimina inalterada en la orina de 24 horas, con un 4 a 7% aproximadamente de anfetamina. En la orina ácida, hasta el 76% se encuentra como droga inalterada, y el 7% como anfetamina en 24 horas, mientras que, en la orina alcalina, se encuentra el 2% como droga inalterada y menos del 0,1% como anfetamina. Con frecuencia, durante las 24 primeras horas de ingestión de 10 mg, se encuentran concentraciones de anfetamina en la orina de 0,5 a 4,0 mg/l. En la orina de consumidores de metanfetamina se observaron concentraciones de metanfetamina de 24 a 333 mg/l (promedio, 142 mg/l).5
2. Exactitud Se realizó un estudio en tres laboratorios de distintas consultas de médicos y en un laboratorio de referencia. Ciento diecinueve muestras clínicas analizadas mediante cromatografía de gases y espectrofotometría de masas en un laboratorio de toxicología fueron enmascaradas y examinadas. Cada muestra se examinó en cada sitio, con INSTANT-VIEW Methamphetamine Test, y se comparó con los resultados de cromatografía de gases y espectrofotometría de masas (CG/EM). La prueba demostró una concordancia total superior al 94,6%. Los resultados obtenidos con el análisis de orina Methamphetamine(500) Urine Test INSTANT-VIEW tuvieron una concordancia del 100% con los datos obtenidos con la cromatografía de gases / espectrofotometría de masas, a concentraciones inferiores al 75% del valor de corte (negativo) y superiores al 125% del valor de corte (positivo). Se observaron 22 discrepancias en las muestras, a la concentración entre el 75% y el 125% del valor de corte. La concordancia total fue del 95,4%.
Análisis INSTANT-VIEW Positivo Negativo
Total Concordancia
Sin drogas 0 220 220 100% <75% (0~375) 0 36 36 100% 75%~Corte (375~500) 6 22 28 78.6% Corte~125% (500~625) 24 16 40 60%
CG/EM (ng/ml)
Positivo (>625) 152 0 152 100% Total 182 294 476 95.4%
3. Reproducibilidad Se determinó la reproducibilidad en tres laboratorios distintos de consultas de médicos (CONS), por personas con distintas formaciones y experiencias de trabajo. A 40 muestras de orina humana mezcladas, sin drogas, se añadió metanfetamina a concentraciones distintas. Todas las muestras fueron enmascaradas y examinadas. Los resultados son los siguientes:
Conc. metanf. Núm. de CONS 1 CONS 2 CONS 3

INSTANT-VIEW Multi-Drug Screen Urine Test
33-xxxx REV x xxxxxx Page 4
(ng/ml) muestras + – + – + – 0 8 0 8 0 8 0 8
375 8 0 8 0 8 1 7 500 8 8 0 8 0 8 0 625 8 8 0 8 0 8 0 1000 8 8 0 8 0 8 0
Los resultados indican una concordancia del 99,3% con los resultados esperados. 4. Reactividad cruzada
Se realizó un estudio con compuestos relacionados con la metanfetamina para determinar la reactividad cruzada de la prueba.
Compuestos relacionados con la metanfetamina que muestran la concentración más baja de la droga que produce una respuesta positiva equivalente al valor de corte. Descripción Concentración (ng/ml) d-metanfetamina 500 l-metanfetamina 25,000 d-anfetamina 50,000 l-anfetamina 10,000 3,4-metilendioxianfetamina (MDA) 50,000
F. Metanfetamina (MET1000) 1. Resumen y explicación de la prueba
La metanfetamina, en sobredosis, produce intranquilidad, confusión, ansiedad, alucinaciones, arritmias cardíacas, hipertensión, hipertermia, colapso circulatorio, convulsiones y coma.3 La metanfetamina se ha implicado en intoxicaciones mortales después de su administración tanto por vía intravenosa como oral. Los consumidores crónicos pueden presentar una psicosis paranoide.1 La D-metanfetamina (d-desoxiefedrina, Desoxyn, Methedrine) es el derivado N-metil de la anfetamina. Se utiliza en el tratamiento de la obesidad. La metanfetamina se administra por vía oral, insuflación nasal o inyección intravenosa, con una duración de dos a cuatro horas.3,5 La metanfetamina es sometida, en parte, a N-desmetilación y se convierte en anfetamina, su principal metabolito activo. En condiciones normales, hasta el 43% de la dosis se elimina inalterada en la orina de 24 horas, con un 4 a 7% aproximadamente de anfetamina. En la orina ácida, hasta el 76% se encuentra como droga inalterada, y el 7% como anfetamina en 24 horas, mientras que, en la orina alcalina, se encuentra el 2% como droga inalterada y menos del 0,1% como anfetamina. Con frecuencia, durante las 24 primeras horas de ingestión de 10 mg, se encuentran concentraciones de anfetamina en la orina de 0,5 a 4,0 mg/l. En la orina de consumidores de metanfetamina se observaron concentraciones de metanfetamina de 24 a 333 mg/l (promedio, 142 mg/l).5
2. Exactitud Se realizó un estudio en tres laboratorios de distintas consultas de médicos y en un laboratorio de referencia. Cien (100) muestras clínicas se enmascararon y examinaron. Cada muestra se examinó en cada sitio, con INSTANT-VIEW Methamphetamine (1000) Test, y se comparó con los resultados de cromatografía de gases y espectrofotometría de masas (CG/EM). Los resultados obtenidos con el análisis de orina Methamphetamine (1000) Urine Test INSTANT-VIEW tuvieron una concordancia del 100% con los datos obtenidos con la cromatografía de gases / espectrofotometría de masas, a concentraciones inferiores al 75% del valor de corte (negativo) y superiores al 125% del valor de corte (positivo). Se observaron doce (12) discrepancias en las muestras, a la concentración entre el 75% y el 125% del valor de corte. La concordancia total fue del 97%.
Análisis INSTANT-VIEW Positivo Negativo
Total Concordancia
Sin drogas 0 200 200 100% <75% (0~750) 0 16 16 100% 75%~Corte (750~1000) 12 12 24 50% Corte~125% (1000~1250) 24 0 24 100%
CG/EM (ng/ml)
Positivo (>1250) 136 0 136 100% Total 172 228 400 97%
3. Reproducibilidad Se determinó la reproducibilidad mediante análisis repetidos en cuatro concentraciones distintas (CG/EM) de metanfetamina en muestras de orina: 0 ng/ml, 870 ng/ml (dentro del 25% por debajo del valor de corte), 1200 ng/ml (dentro del 25% por encima del valor de corte) y 2000 ng/ml (positivo) con tres lotes de producción distintos. Se examinaron los equipos durante cinco días consecutivos, cinco veces cada día, hasta un total de 25 análisis por cada control. Los resultados indican una precisión intralote del 100% de la repetición y ninguna variación apreciable entre lotes entre los tres lotes distintos de equipos.
4. Reactividad cruzada Para determinar la reactividad cruzada de los compuestos estructuralmente relacionados con el equipo, se añadieron los siguientes compuestos a muestras de orina mezcladas, sin drogas, y se examinaron con la prueba de orina INSTANT-VIEW Methamphetamine Urine Test. Estos compuestos mostraron una respuesta positiva a la concentración indicada en la siguiente tabla:
Descripción Concentración (ng/ml) d-anfetamina 50,000 l-anfetamina 10,000 3,4-metilendioxianfetamina (MDA) 50,000
G. Morfina (MOR300) 1. Resumen y explicación de la prueba
La morfina es un popular fármaco comercializado (p. ej., Serax) para el tratamiento del dolor moderado o grave.3 También es un metabolito común de los opiáceos [morfina, codeína (metilmorfina) y heroína (derivados semisintéticos de la morfina)]. Los opiáceos se administran por inhalación (fumados), por inyección intravenosa o intramuscular, o por vía oral. Entre los efectos adversos o tóxicos de los opiáceos se cuentan la miosis, estreñimiento, retención urinaria, náuseas, vómitos, hipotermia, somnolencia, mareos,
apatía, confusión, depresión respiratoria, hipotensión, piel fría y sudorosa, coma y edema pulmonar. Después de una sobredosis puede producirse la muerte.3,4 La duración del efecto de la morfina es de tres a seis horas.3 La morfina se metaboliza extensamente y sólo del 2 al 12% se excreta inalterada por la orina. La heroína se metaboliza rápidamente a morfina en el organismo; la pauta de excreción urinaria de la heroína es similar a la de la morfina. La codeína también se metaboliza extensamente, y del 10 al 15% de la dosis se desmetila para formar morfina y norcodeína. Se ha descrito que la morfina inalterada puede permanecer detectable en la orina durante un período de hasta una semana,3 lo que hace que sea un marcador del abuso de opiáceos.
2. Exactitud Se realizó un estudio en tres laboratorios de distintas consultas de médicos (CONS) y en un laboratorio de referencia. Noventa y cuatro (94) muestras clínicas se enmascararon y examinaron. Cada muestra se examinó en cada sitio, con INSTANT-VIEW Morphine (300) Test, y se comparó con los resultados de cromatografía de gases y espectrofotometría de masas (CG/EM). Los resultados obtenidos con el análisis de orina Morphine (300) Urine Test INSTANT-VIEW tuvieron una concordancia del 100% con los datos obtenidos con la cromatografía de gases / espectrofotometría de masas, a concentraciones inferiores al 75% del valor de corte (negativo) y superiores al 125% del valor de corte (positivo). Se observaron trece (13) discrepancias en las muestras, a la concentración entre el 75% y el 125% del valor de corte. La concordancia total fue del 96,5%.
Análisis INSTANT-VIEW
Positivo Negativo Total Concordancia
Sin drogas 0 180 180 100% <75%(0~225) 0 12 12 100% 75%~Corte(225~300) 13 11 24 45.8% Corte~125%(300~375) 24 0 24 100%
CG/EM (ng/ml)
Positivo(>375) 136 0 136 100% Total 173 203 376 96.5%
3. Reproducibilidad Se determinó la reproducibilidad en tres laboratorios distintos de consultas, por personas con distintas formaciones y experiencias de trabajo. A 40 muestras de orina humana mezcladas, sin drogas, se añadió morfina a concentraciones distintas. Todas las muestras fueron enmascaradas y examinadas. Los resultados son los siguientes:
CONS 1 CONS 2 CONS 3 Conc. morfina (ng/ml)
Núm. de muestras + – + – + –
0 8 0 8 0 8 0 8 225 8 3 5 3 5 1 7 300 8 7 1 8 0 7 1 375 8 8 0 8 0 8 0 600 8 8 0 8 0 8 0
Los resultados indican una concordancia del 92,5% con los resultados esperados
4. Reactividad cruzada Para determinar la reactividad cruzada de los compuestos estructuralmente relacionados con el equipo, se añadieron los siguientes compuestos a muestras de orina mezcladas, sin drogas, y se examinaron con la prueba de orina INSTANT-VIEW Morphine Urine Test. Estos compuestos mostraron una respuesta positiva a la concentración indicada en la siguiente tabla:
Compuestos estructuralmente relacionados con la morfina que muestran la concentración más baja de la droga que produce una respuesta positiva equivalente al valor de corte: Descripción Concentración (ng/ml) Descripción Concentración (ng/ml) Morfina 300 Glucurónido de morfina 500 Codeína 300 Merperidina 30000 Etilmorfina 300 Oxicodona 1000 Hidromorfina 400
H. Morfina (MOR2000) 1. Resumen y explicación de la prueba
La morfina es un popular fármaco comercializado (p. ej., Serax) para el tratamiento del dolor moderado o grave.3 También es un metabolito común de los opiáceos [morfina, codeína (metilmorfina) y heroína (derivados semisintéticos de la morfina)]. Los opiáceos se administran por inhalación (fumados), por inyección intravenosa o intramuscular, o por vía oral. Entre los efectos adversos o tóxicos de los opiáceos se cuentan la miosis, estreñimiento, retención urinaria, náuseas, vómitos, hipotermia, somnolencia, mareos, apatía, confusión, depresión respiratoria, hipotensión, piel fría y sudorosa, coma y edema pulmonar. Después de una sobredosis puede producirse la muerte.3,4 La duración del efecto de la morfina es de tres a seis horas.3 La morfina se metaboliza extensamente y sólo del 2 al 12% se excreta inalterada por la orina. La heroína se metaboliza rápidamente a morfina en el organismo; la pauta de excreción urinaria de la heroína es similar a la de la morfina. La codeína también se metaboliza extensamente, y del 10 al 15% de la dosis se desmetila para formar morfina y norcodeína. Se ha descrito que la morfina inalterada puede permanecer detectable en la orina durante un período de hasta una semana,3 lo que hace que sea un marcador del abuso de opiáceos.
2. Exactitud Se realizó un estudio en tres laboratorios de distintas consultas de médicos (CONS) y en un laboratorio de referencia. Cien (100) muestras clínicas se enmascararon y examinaron. Cada muestra se examinó en cada sitio, con INSTANT-VIEW Morphine (2000) Test, y se comparó con los resultados de cromatografía de gases y espectrofotometría de masas (CG/EM). Los resultados obtenidos con el análisis de orina Morphine (2000) Urine Test INSTANT-VIEW tuvieron una concordancia del 100% con los datos obtenidos con la cromatografía de gases / espectrofotometría de masas, a concentraciones inferiores al 75% del valor de corte (negativo) y superiores al 125% del valor de corte (positivo). Se observaron dos (2) discrepancias en las muestras, a la concentración entre el 75% y el 125% del valor de corte. La concordancia total fue del 99,5%.
Análisis INSTANT-VIEW
Positivo Negativo Total Concordancia

INSTANT-VIEW Multi-Drug Screen Urine Test
33-xxxx REV x xxxxxx Page 5
Sin drogas 0 132 132 100% <75% (0~1500) 0 64 64 100% 75%~Corte (1500~2000) 2 30 32 93.8% Corte~125% (2000~2500) 28 0 28 100%
CG/EM (ng/ml)
Positivo (>2500) 144 0 144 100% Total 174 226 400 99.5%
3. Reproducibilidad Se determinó la reproducibilidad mediante análisis repetidos en cuatro niveles distintos de muestras, con tres lotes de producción diferentes. Se examinó el equipo durante cinco días consecutivos, hasta un total de 25 análisis por cada control. Los resultados indican una precisión intralote del 100% de la repetición y ninguna variación apreciable entre lotes entre los tres lotes distintos de equipos
4. Reactividad cruzada Para determinar la reactividad cruzada de los compuestos estructuralmente relacionados con el equipo, se añadieron los siguientes compuestos a muestras de orina mezcladas, sin drogas, y se examinaron con la prueba de orina INSTANT-VIEW Morphine Urine Test. Estos compuestos mostraron una respuesta positiva a la concentración indicada en la siguiente tabla:
Descripción Concentración (ng/ml) Descripción Concentración (ng/ml) Codeína 2000 Glucurónido de morfina 3000 Etilmorfina 2000 Merperidina 30,000 Hidromorfina 2500
I. Metadona (MTD) 1. Resumen y explicación de la prueba
La metadona, también llamada dolofina, metadosis y amidona, posee muchas de las propiedades farmacológicas de la morfina y es aproximadamente equipotente como analgésico si se administra por vía parenteral. Sin embargo, a diferencia de la morfina, la metadona produce unos efectos sedantes marcados con la administración repetida, a consecuencia de la acumulación del fármaco. La metadona se ha empleado como principal sustituto de los opiáceos, tales como la heroína, la morfina y la codeína, en las clínicas de tratamiento de mantenimiento de drogas. Se administra por vía oral, o por inyección intravenosa o intramuscular.3 La duración del efecto de la metadona es de 12 a 24 horas.5 Sus principales productos de excreción urinaria son la metadona, EDDP (2-etildieno-1,5-dimetil-3,3-difenilpirrolidina) y EMDP (2-etil-5-metil-3,3-difenilpirrolidina). El porcentaje de metadona excretada inalterada en la orina es del 5 al 50%, mucho más que la EDDP y la EMDP, de la dosis en 24 horas. Se han observado grandes variaciones individuales en el porcentaje de metadona inalterada que se excreta por la orina, debido al pH y al volumen de la orina, a la dosis y la velocidad del metabolismo, etc. Se ha observado metadona presente en la orina a una concentración superior a 1000 ng/ml, 24 horas después de una sobredosis.5 Por lo tanto, se ha empleado la concentración de metadona en la orina humana como marcador del abuso de la metadona.
2. Exactitud Se realizó un estudio en tres laboratorios de distintas consultas de médicos (CONS) y en un laboratorio de referencia. Cien (100) muestras clínicas se enmascararon y examinaron. Cada muestra se examinó en cada sitio, con INSTANT-VIEW Methadone (MTD) Test, y se comparó con los resultados de cromatografía de gases y espectrofotometría de masas (CG/EM). Los resultados obtenidos con el análisis de orina Methadone Urine Test INSTANT-VIEW tuvieron una concordancia del 100% con los datos obtenidos con la cromatografía de gases / espectrofotometría de masas, a concentraciones inferiores al 75% del valor de corte (negativo) y superiores al 125% del valor de corte (positivo). Se observaron diez (10) discrepancias en las muestras, a la concentración entre el 75% y el 125% del valor de corte. La concordancia total fue del 97.5%.
Análisis INSTANT-VIEW Positivo Negativo
Total Concordancia
<75% (0~225) 0 192 192 100% 75%~Corte (225~300) 10 18 28 64.3% Corte~125% (300~375) 36 0 36 100%
CG/EM (ng/ml) Positivo (>375) 144 0 144 100%
Total 190 210 400 97.5%
3. Reproducibilidad Se determinó la reproducibilidad mediante análisis repetidos en cuatro niveles distintos de muestras, con tres lotes de producción diferentes. Se examinó el equipo durante cinco días consecutivos, cinco veces cada día, hasta un total de 25 análisis por cada control. Los resultados indican una precisión intralote del 100% de la repetición y ninguna variación apreciable entre lotes entre los tres lotes distintos de equipos.
4. Reactividad cruzada Para determinar la reactividad cruzada de los compuestos estructuralmente relacionados con el equipo, se añadieron los siguientes compuestos a muestras de orina mezcladas, sin drogas, y se examinaron con la prueba de orina INSTANT-VIEW Methadone Urine Test. Estos compuestos mostraron una respuesta positiva a la concentración indicada en la siguiente tabla:
Descripción Concentración (ng/ml) (-)-α-Metadol 800 (-)-α-Acetilmetadol (LAAM) 1000
J. Fenciclidina (PCP) 1. Resumen y explicación de la prueba
La fenciclidina (PCP), también llamada polvo de ángel o hierba asesina, es un a droga popular, así como un tranquilizante de uso veterinario. Se autoadministra fumado, por insuflación nasal, inyección intravenosa o ingestión.3 Su efecto tiene una duración de dos a cuatro horas y la psicosis puede durar varias semanas. La PCP tiene tres metabolitos principales; sin embargo, el porcentaje de una dosis intravenosa excretada inalterada por la orina es del 30 al 50% a las 72 horas. Sólo el 2% de una dosis se excreta por las heces. Un promedio del 77% de una dosis intravenosa se excreta por la orina y las heces en 10 días.3,5
Por lo tanto, se ha empleado la PCP en la orina humana como marcador del abuso de esta sustancia.4 La mayoría de las veces, las concentraciones de droga inalterada en la orina de los consumidores ambulatorios de PCP son de 0,04 a 3,4 mg/l.3
2. Exactitud Se realizó un estudio en tres laboratorios de distintas consultas de médicos (CONS) y en un laboratorio de referencia. Cien (100) muestras clínicas se enmascararon y examinaron. Cada muestra se examinó en cada sitio, con INSTANT-VIEW Phencyclidine (PCP) Test, y se comparó con los resultados de cromatografía de gases y espectrofotometría de masas (CG/EM). Los resultados obtenidos con el análisis de orina Phencyclidine Urine Test INSTANT-VIEW tuvieron una concordancia del 100% con los datos obtenidos con la cromatografía de gases / espectrofotometría de masas, a concentraciones inferiores al 75% del valor de corte (negativo) y superiores al 125% del valor de corte (positivo). Se observaron ocho (8) discrepancias en las muestras, a la concentración entre el 75% y el 125% del valor de corte. La concordancia total fue del 98%.
Análisis INSTANT-VIEW Positivo Negativo
Total Concordancia
<75% (0~18.75) 0 184 184 100% 75%~Corte (18.75~25) 8 16 24 66.7% Corte~125% (25~31.25) 32 0 32 100%
CG/EM (ng/ml)
Positivo (>31.25) 160 0 160 100% Total 200 200 400 98%
3. Reproducibilidad Se determinó la reproducibilidad mediante análisis repetidos en cuatro niveles distintos de muestras, con tres lotes de producción diferentes. Se examinó el equipo durante cinco días consecutivos, hasta un total de 25 análisis por cada control. Los resultados indican una precisión intralote del 100% de la repetición y ninguna variación apreciable entre lotes entre los tres lotes distintos de equipos.
4. Reactividad cruzada Para determinar la reactividad cruzada de los compuestos estructuralmente relacionados con el equipo, se añadieron los siguientes compuestos a muestras de orina mezcladas, sin drogas, y se examinaron con la prueba de orina INSTANT-VIEW Phencyclidine(PCP) Urine Test. Estos compuestos mostraron una respuesta positiva a la concentración indicada en la siguiente tabla:
Descripción Concentración (ng/ml) Descripción Concentración (ng/ml) Metilfenidato 25,000 Tenociclidina 2,000 Feniramina 25,000
K. Propoxifeno (PPX) 1. Resumen y explicación de la prueba
El propoxifeno es un fármaco de venta con receta médica para el alivio del dolor. El clorhidrato de propoxifeno (Darvon, Dolene y otros) se expende en cápsulas de 32 y 65 mg; el napsilato de propoxifeno (Darvon-N) se expende en comprimidos de 100 mg o como suspensión. Está relacionado estructuralmente con la metadona. La sobredosis del fármaco puede afectar ala región encefálica y causar euforia, al igual que muchos opiáceos. La sintomatología progresiva del propoxifeno consiste en analgesia, estupor, depresión respiratoria y coma, etc. La semivida del propoxifeno es de 8 a 24 horas. Tras la administración por vía oral, el propoxifeno alcanza un máximo en una a dos horas. Existe una gran variabilidad entre las personas en cuanto a la tasa de depuración. El porcentaje de propoxifeno inalterado que se excreta por la orina es inferior al 1%. El principal metabolito del propoxifeno es el norpropoxifeno. Por lo tanto, la detección de este metabolito se emplea extensamente para el análisis del abuso del propoxifeno. La semivida del norpropoxifeno es de aproximadamente 30 horas y su acumulación con dosis repetidas puede ser responsable de una parte de la toxicidad observada.5,6
2. Exactitud Se determinó la exactitud de este equipo mediante un estudio de comparación entre INSTANT-VIEWPropoxyphene (PPX) Urine Test y la cromatografía de gases / espectrofotometría de masas (CG/EM). El estudio se realizó en el laboratorio, con cien (100) muestras clínicas de orina enmascaradas. Los datos detallados se muestran en la tabla a continuación. Los resultados del análisis de orina INSTANT-VIEW Propoxyphene (PPX) tuvieron una concordancia del 100% con los datos obtenidos mediante cromatografía de gases y espectrofotometría de masas, a las concentraciones inferiores al valor de corte (negativos) y superiores al 125% del valor de corte (positivos). Se observaron dos discrepancias en las muestras a la concentración entre el valor de corte y el 125% del mismo. La concordancia total fue del 98%.
Análisis INSTANT-VIEW Positivo Negativo
Total Concordancia
Sin drogas 0 40 40 100% <75% (0~225) 0 10 10 100% 75%~Corte (225~300) 0 10 10 100% Corte~125% (300~375) 8 2 10 80%
CG/EM (ng/ml)
Positivo (>375) 30 0 30 100% Total 38 62 100 98%
3. Reproducibilidad Se determinó la reproducibilidad mediante análisis repetidos con tres lotes diferentes. Las muestras utilizadas en este estudio fueron las mismas que las del estudio de exactitud. Se examinaron los equipos durante cinco días consecutivos, cinco veces cada día, hasta un total de 25 análisis por cada control. Los resultados indican una precisión intralote del 100% de la repetición y ninguna variación apreciable entre lotes, en los tres lotes distintos de equipos.
4. Reactividad cruzada Se evaluó con este equipo la reactividad cruzada de los compuestos relacionados estructuralmente relacionados con el propoxifeno. Se añadieron los siguientes compuestos a muestras de orina mezcladas, sin drogas, y se examinaron con la prueba de orina INSTANT-VIEW Propoxyphene (PPX) Urine Test.

INSTANT-VIEW Multi-Drug Screen Urine Test
33-xxxx REV x xxxxxx Page 6
El propoxifeno y su principal metabolito, norpropoxifeno, presentan una respuesta positiva similar a la concentración de 300 ng/ml. Otros compuestos examinados dieron unas respuestas positivas a una concentración muy alta: metadona a 1.350.000 ng/ml y el metabolito de la metadona (EDDP) a 200.000 ng/ml.
Drogas o compuestos Concentración Propoxifeno 300 ng/ml Norpropoxifeno 300 ng/ml Metadona 1,350,000 ng/ml 2-etil-1,5-dimetil-3,3-difenilpirrolidina (EDDP, metabolito de la metadona)
200,000 ng/ml
L. Tricíclicos (TCA) 1. Resumen y explicación de la prueba
Los tricíclicos (TCA) son un grupo de fármacos antidepresivos que contienen tres anillos fusionados en su estructura química.7 Los TCA pueden administrarse por vía oral o intramuscular. La sintomatología progresiva de los tricíclicos consiste en agitación, confusión, alucinaciones, hipertonicidad, convulsiones y alteraciones electrocardiográficas. La semivida de los TCA varía entre unas horas y unos días. Los antidepresivos tricíclicos de uso habitual se excretan por la orina con un porcentaje muy bajo de fármaco inalterado, menos del 1%. Por lo tanto, se ha empleado la detección de los metabolitos de los tricíclicos en la orina humana para la evaluación del abuso de estos fármacos.3,5 Este análisis puede detectar amitriptilina, desipramina, imipramina y nortriptilina a una concentración de corte de 1.000 ng/ml.
2. Exactitud Se determinó la exactitud mediante la comparación de los resultados obtenidos con el análisis de orina TCA Urine Test INSTANT-VIEW con los datos obtenidos con la cromatografía de gases / espectrofotometría de masas. El estudio se realizó en el laboratorio, con ochenta (80) muestras clínicas de orina enmascaradas. Los datos detalladas se muestran en la tabla a continuación. Los resultados obtenidos con el análisis de orina TCA Urine Test INSTANT-VIEW tuvieron una concordancia del 100% con los datos obtenidos con la cromatografía de gases / espectrofotometría de masas, a concentraciones inferiores al 75% del valor de corte (negativo) y superiores al 125% del valor de corte (positivo). Se observaron dos (2) discrepancias en las muestras con cromatografía de gases / espectrofotometría de masas, a la concentración entre el 75% y el 125% del valor de corte. La concordancia total fue del 97.5%.
Análisis INSTANT-VIEW Positivo Negativo
Total Concordancia
Sin drogas 0 40 40 100% <75% (0~750) 0 10 10 100% 75%~Corte (750~1000) 2 8 10 80% Corte~125% (1000~1250) 8 0 8 100%
CG/EM (ng/ml)
Positivo (>1250) 12 0 12 100% Total 22 58 80 97.5%
3. Reproducibilidad Se determinó la reproducibilidad mediante análisis repetidos, en cuatro niveles distintos de muestras, con tres lotes de producción diferentes. Se examinaron los equipos durante cinco días consecutivos, cinco veces cada día, hasta un total de 25 análisis por cada control. Los resultados indican una precisión intralote del 100% de la repetición, y ninguna variación apreciable entre lotes, en los tres lotes distintos de equipos.
4. Reactividad cruzada Para determinar la reactividad cruzada de los compuestos estructuralmente relacionados con el equipo, se añadieron los siguientes compuestos a muestras de orina mezcladas, sin drogas, y se examinaron con la prueba de orina INSTANT-VIEW TCA Urine Test. Estos compuestos mostraron una respuesta positiva a la concentración indicada en la siguiente tabla:
Descripción Concentración (ng/ml) Descripción Concentración (ng/ml) Nortriptilina 1,000 Clomipramina 5,000 Amitriptilina 1,000 Doxepina 3,000 Imipramina 800 Protriptilina 2,000 Desipramina 800 Perfenazina 75,000 Nordoxepina 1,000 Promazina 15,000 Cicolbenzaprina 1,500 Trimipramina 2,000
M. Marihuana (THC) 1. Resumen y explicación de la prueba
El tetrahidrocannabinol (THC, ∆-9-THC, ∆-1-THC) es el más activo de los constituyentes principales, así como el principal metabolito de los cannabinoides, tales como la marihuana y el hachís. Los cannabinoides se han empleado como depresores del sistema nervioso central. La sobredosis y el uso prolongado de cannabinoides pueden ser causantes del abuso de la droga, que puede causar un daño grave o permanente del sistema nervioso del ser humano. La detección de THC en la orina humana ha tenido un uso extendido para evaluar el consumo de cannabinoides.2,3,4
2. Exactitud Se realizó un estudio en tres laboratorios de distintas consultas de médicos (CONS) y en un laboratorio de referencia. Noventa y nueve (99) muestras clínicas se enmascararon y examinaron. Cada muestra se examinó en cada sitio, con INSTANT-VIEW Marijuana (THC) Test, y se comparó con los resultados de cromatografía de gases y espectrofotometría de masas (CG/EM). Los resultados obtenidos con el análisis de orina Marijuana (THC) Urine Test INSTANT-VIEW presentaron una concordancia del 100% con los datos obtenidos con la cromatografía de gases / espectrofotometría de masas, a concentraciones inferiores al 75% del valor de corte (negativo) y superiores al 125% del valor de corte (positivo). Se observaron catorce (14) discrepancias en las muestras, a la concentración entre el 75% y el 125% del valor de corte. La concordancia total fue del 96.5%.
Análisis INSTANT-VIEW Positivo Negativo
Total Concordancia
Sin drogas 0 160 160 100% <75% (0~37.5) 0 36 36 100% 75%~Corte (37.5~50) 11 13 24 54.2% Corte~125% (50~62.5) 17 3 20 85%
Positivo (>62.5) 156 0 156 100% Total 184 212 396 96.5%
3. Reproducibilidad Se determinó la reproducibilidad en tres laboratorios distintos de consultas, por personas con distintas formaciones y experiencias de trabajo. A 40 muestras de orina humana mezcladas, sin drogas, se añadió THC a concentraciones distintas. Todas las muestras fueron enmascaradas y examinadas. Los resultados son los siguientes:
CONS 1 CONS 2 CONS 3 Conc. THC (ng/ml)
Núm. de muestras + – + – + –
0 8 0 8 0 8 0 8 37.5 8 0 8 1 7 0 8 50 8 8 0 8 0 8 0
62.5 8 8 0 8 0 8 0 100 8 8 0 8 0 8 0
Los resultados indican una concordancia del 98,8% con los resultados esperados. 4. Reactividad cruzada
Se realizó un estudio con compuestos relacionados con el THC para determinar la reactividad cruzada de la prueba.
Compuestos estructuralmente relacionados con el THC que muestran la concentración más baja de la droga que produce una respuesta positiva equivalente al valor de corte: Descripción Concentración (ng/ml) 11-nor-∆-8-THC-9-COOH 50 11-nor-∆-9-THC-9-COOH 50 11-hidroxi-∆-9-THC 100 9-Tetrahidrocannabinol 10,000 Cannabonol 10,000
N. MDMA (Éxtasis, XTC) 1. Resumen y explicación de la prueba
MDMA es una abreviatura del compuesto químico metilendioximetanfetamina, que tiene muchos nombres de uso coloquial, entre ellos, X, XTC, E, eva, adán, mitsubishi, píldora del amor, etc. Es un estimulante con tendencias alucinógenas, descrito como empatógeno, ya que libera sustancias químicas que alteran el humor, tales como la serotonina y L-dopa, en el cerebro y puede generar sentimientos de amor y amistad. La MDMA es una droga de clase A, en la misma categoría que la heroína y la cocaína. Entre las reacciones adversas de la MDMA se pueden el aumento de la presión arterial, hipertermia, ansiedad, paranoia e insomnio. La sobredosis con MDMA puede ser mortal y muchas veces ocasiona insuficiencia cardíaca o golpe de calor.5,8 La MDMA pertenece a la familia de las drogas sintéticas; entre las drogas emparentadas se cuentan la MDA (metilendioxianfetamina), droga originaria de la MDMA; y le MDEA (metilendioxietilanfetamina), también conocida como EVA. Todas comparten efectos de tipo anfetamínico. LA MDMA se administra por vía oral o inyección intravenosa. Los comprimidos de MDMA vienen en diferentes tamaños y colores, y muchas veces tienen logotipos tales como palomas. La dosis clínica es de 50 a 100 mg; el umbral de la dosis tóxica es de 500 mg. Los efectos de la MDMA comienzan 30 minutos después de la toma; presentan un pico al cabo de una hora y duran dos a tres horas. El 65% de la MDMA se excreta inalterada por la orina; permanece detectable en ésta hasta tres días después del consumo.5,8
2. Exactitud Se determinó la exactitud de este equipo mediante un estudio de comparación entre INSTANT-VIEW MDMA Test y la cromatografía de gases / espectrofotometría de masas (CG/EM). Este estudio se realizó en el laboratorio y se utilizaron 80 muestras clínicas de orina. Los datos detallados se muestran en la tabla a continuación. Los resultados del análisis de orina INSTANT-VIEW MDMA (Ecstasy, XTC) Urine Test tuvieron una concordancia del 100% con los datos obtenidos mediante cromatografía de gases y espectrofotometría de masas, a las concentraciones inferiores al 75% del valor de corte (negativos) y superiores al 125% del valor de corte (positivos). Se observaron dos discrepancias en las muestras a la concentración entre el 75% del valor de corte y el 125% del valor de corte. La concordancia total fue del 97.5%.
Análisis INSTANT-VIEW Positivo Negativo
Total Concordancia
Sin drogas 0 40 40 100% <75% (0~375) 0 10 10 100% 75%~Corte (375~500) 2 9 11 82% Corte~125% (500~625) 9 0 9 100%
CG/EM (ng/ml)
Positivo (>625) 10 0 10 100% Total 21 59 80 97.5%
3. Reproducibilidad El estudio de reproducibilidad de este análisis se realizó fuera de las instalaciones de Alfa, en tres laboratorios de consultorios médicos (CONS) y un laboratorio clínico de referencia, por personal con distintas formaciones y experiencias de trabajo. Para el estudio se utilizan 110 muestras de orina a las que se añadió MDMA en seis concentraciones diferentes: 0, 257, 378, 615, 709 y 1417 ng/ml (determinado mediante cromatografía de gases y espectrofotometría de masas). Los resultados se resumen en la siguiente tabla.
Muestras Lugar I Lugar II Lugar III Lugar IV Total Número 15 15 15 15 60 0
ng/ml Resultado 15- 15- 15- 15- 60- Número 15 15 15 15 60 257
ng/ml Resultado 15- 15- 15- 15- 60- Número 25 25 25 25 100 378
ng/ml Resultado 25- 25- 25- 25- 100- Número 25 25 25 25 100 615
ng/ml Resultado 23+, 2- 23+, 2- 22+, 3- 24+, 1- 92+, 8-

INSTANT-VIEW Multi-Drug Screen Urine Test
33-xxxx REV x xxxxxx Page 7
Número 15 15 15 15 60 709 ng/ml Resultado 15+ 14+, 1- 15+ 15+ 59+, 1-
Número 15 15 15 15 60 1417 ng/ml Resultado 15+ 15+ 15+ 15+ 60+
En los cuatro lugares de evaluación, 220 equipos examinados con muestras que contenían menos de 378 ng/ml de MDMA (75% del valor de corte) fueron negativas (concordancia del 100%). De los 100 equipos examinados con muestras que contenían 615 ng/ml de MDMA (125% del valor de corte), 92 fueron positivas y 8 fueron negativas (concordancia del 92%). De los 60 equipos examinados con muestras que contenían 709 ng/ml de MDMA (150% del valor de corte), 59 fueron positivas y una fue negativa (concordancia del 98,3%). Los 60 equipos examinados con muestras que contenían 1417 ng/ml de MDMA fueron positivos. No se observó ninguna discrepancia intradía, entre días ni entre análisis. Los resultados obtenidos de los cuatro sitios de evaluación tuvieron una concordancia del 97,5% entre sí, lo que indica una elevada reproducibilidad del equipo.
4. Reactividad cruzada Se estudió la reactividad cruzada de los compuestos estructuralmente relacionados con el equipo. Se añadieron los siguientes compuestos a muestras de orina mezcladas, sin drogas, y se examinaron con la prueba de orina MDMA Urine Test. Los compuestos que dieron resultados positivos a una concentración inferior a 10 µg/ml se indican en la siguiente tabla:
Descripción Concentración (ng/ml) Metilendioxianfetamina (MDA) 2000 Metilendioxetilanfetamina (MDEA) 1000
Los compuestos que no dieron un resultado positivo a una concentración de 100 µg/ml se indican en la siguiente tabla:
Descripción Concentración (µg/ml) L-anfetamina 100 d-anfetamina 100 L-metanfetamina 100 d-metanfetamina 100 Hidroximetanfetamina (HAM) 100 Dihidroximetanfetamina (HMMA) 100 N-metil-1-(1-3-benzodioxol-5-il)-2-butanamina (MBDB) 100
BIBLIOGRAFÍA 1. FDA Guidance for Labeling Urine Drugs of Abuse Screening Testing, Kshit Mohan, 7/21. 2. Urine Testing for Drugs of Abuse. National Institute on Drug Abuse (NIDA): Research
Monograph 73, 1986. 3. Baselt, R.C. Disposition of Toxic Drugs and Chemicals in Man, 4th ED., Biomedical
Publ., Davis, CA; p713-715, 1995. 4. Department of Health and Human Services, Mandatory Guidelines for Federal Workplace
Drug Testing Programs, Fed. Register. (69): 11970 (1988). 5. Wilson, John, Abused Drugs II, a Laboratory Pocket Guide., AACC Press. Washington,
DC; 1994. 6. Gilman AG, Rall TW, Nies AS, Taylor P eds., Goodman and Gilman’s the
Pharmacological Basis of Therapeutics, 8th ed., New York, Pergamon Press, 1990. 7. Dorland’s Illustrated Medical Dictionary, 26th Edition, W.B. Saunders Company,
Philadelphia, PA, pp89, 1981. 4Urine Testing for Drugs of Abuse, National Institute on Drug Abuse (NIDA): Research Monograph 73, 1986.
8. S-J. Peroutka ed. Ecstasy: The clinical, pharmacological and neurotoxicological effects of the drug MDMA. Kluwer Academic Publishers, 1990.