inservice_postrel_acl outcomes & return to sport
TRANSCRIPT

Tina Postrel, SPT
University of Central Florida
Spring 2015 Inservice

Incidence: re-injury & return to sport
Risk factors
Key concepts of rehab
Early phase
Late phase
Return to sport outcome measures
Objective measures
Subjective/psychosocial
Biomechanical screens
Time vs. functional tests
Return to practice
Clinical Recommendation
Summary

@ 2 yrs:
Study overview:
return to pivoting/cutting sport
N=78
C=47
LOE=2 cohort study
Overall: 30% of athletes sustained 2nd ACL injury
21% contralateral
9% ipsilateral
Females: 2x more likely for contralateral injury
vs ipsilateral

@ 10 yrs:
Study overview:
systematic review
N=2682
LOE=2
Overall: 20.5%
8% ipsilateral, 12.5% contralateral
contralateral tear 1.63x greater

20113 2014 4 20115
Achieve successful knee function 90% ----- ------
Return to ANY sport 82% 81% 67%
Return to PRE injury level 63% 65% ------
Return to COMPETITVE sport 44% 55% 33%
Study size N=5,770 N=7,556 N=503
(athletes)
Study design MA & SR MA & SR Case
series
Mean F/U time 3.5 yrs N/A 12 mo

Effusion
Extension

Proprioception
Stability
Hip & glut strength
control medial collapse
Power
Contralateral limb training too!

Running Progression
Trace or less effusion, >80% strength, >8-16wks


Quad Strength
MVIC: Max Voluntary Isometric Contraction
>90% contralateral strength
similar hop test scores compared to uninjured athletes
<85% = ↓ self reported fxn, impaired performance (hop tests)
Hamstring/Quad Ratio
>60% H:Q ratio
Clinical Application:
Biodex Isokinetic machine OR Dynamometer @ 60° Flex

Hop Testing >16-22 weeks
Test dynamic knee stability, agility
≥ 90% limb symmetry index
Instructions: 2 practice trials ea LE→2 measured trials →avg & compare involved to
uninvolved

Subjective /psychosocial
IKDC
International Knee Documentation Subjective Knee Form
High Specificity (SP= 84.8% @ 6mo, 91.9% @ 12mo)
Athlete low score = indicative of failing fxnal tests
Low Sensitivity (SN= 62% @ 6mo, 37% @ 12mo)
High/normal score = better symmetry on hop test, but
doesn’t correlate w/passing
IKDC > KOOS
Knee Injury & OA Outcome Score
TSK
Tampa Scale for Kinesiophobia
good to ID fear of reinjury
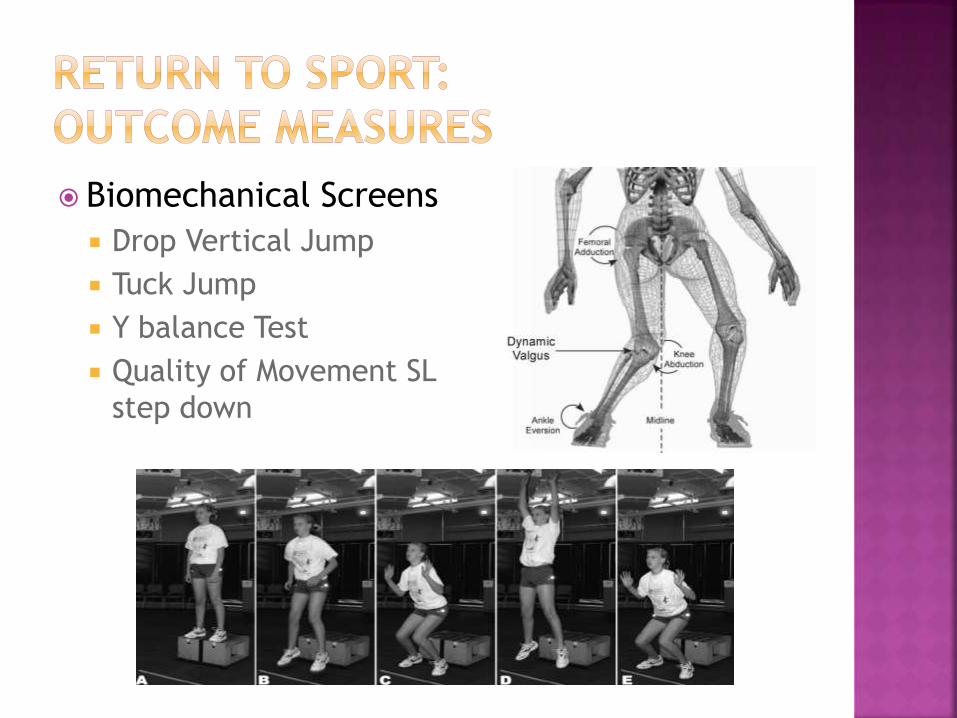
Biomechanical Screens
Drop Vertical Jump
Tuck Jump
Y balance Test
Quality of Movement SL
step down

Rate of Force Development (RFD)
Way to compare neuromuscular control vs max strength
RFD: Measures quick accelerations & power
RFD vs MVIC: Max Voluntary Isometric Contraction (@ 60° Flex)
• MVIC 97% pre-injury level
@ 6 mo
• RFD≥ 90% pre-injury level
@ 12 mo
• Subjects required +20wks
rehab c power focus

Time vs Functional Measures?
Most recommendations ≥ 6 months
However… time does not correlate c functional abilities
20149 201011
Pass Fxnal outcomes @ 6 mo 30% 48%
Pass Fxnal outcomes @ 12 mo 52% 78%
Fxnal outcomes tested: Quadriceps
index, hop tests
Quadriceps index, hop
tests, KOS-ADLS,
Global Rating Scale of
Overall Knee Function
Study design Prospective
Cohort
RCT
cohort N=141 N=40


Objective Tests: Absence of knee effusion and pain
Full knee AROM/PROM
Quad Strength ≥ 90% contralateral quad strength
Subjective: Athlete Perception via IKDC
Functional & Biomechanical Screens: ≥ 90% bilat symmetry c SL hop tests
Quality test: Vertical drop jump test (consider contralateral too)
Overall Time:≥ 12 mo 0-6 mo: strength, balance, proprioception
6-12 mo: power/explosive strength, sport specific, return to practice
*risk of re-injury is significant and return to sport % is low so multiple measures needed. Single measures may be inadequate to ID deficiencies.


Incidence of Re-injury Contralateral ACL tear 1.6x > ipsilateral
Athletic population > general
Women > men
Incidence of Return to Sport Only ½ return to competitive sport
Comprehensive testing needed before clearance for return to sport Subjective, objective, functional & biomechanical screens
Don’t forget about power!
“Gold Standard” for return to sport No effusion
>90% quad MVIC
SL hop test
IKDC
Quality of Movement: Vertical Drop Jump
Functional Milestones > Time Milestones

1. Paterno M, Rauh M, Schmitt L, Ford K, Hewett T. Incidence of second ACL injuries 2 years after primary acl reconstruction and return to
sport. The American Journal Of Sports Medicine. 2014;(7):1567.
2. Magnussen R, Meschbach N, Kaeding C, Wright R, Spindler K. ACL graft and contralateral ACL tear risk within ten years following
reconstruction: a systematic review. JBJS Reviews. 2015; 3(1):e3.
3. Ardern C, Webster K, Taylor N, Feller J. Return to sport following anterior cruciate ligament reconstruction surgery: a systematic review and
meta-analysis of the state of play. British Journal Of Sports Medicine. 2011;45(7):596-606.
4. Ardern C, Taylor N, Feller J, Webster K. Fifty-five per cent return to competitive sport following anterior cruciate ligament reconstruction
surgery: an updated systematic review and meta-analysis including aspects of physical functioning and contextual factors. British Journal Of
Sports Medicine. November 2014;48(21):1543-1553.
5. Ardern C, Webster K, Taylor N, Feller J. Return to the Preinjury Level of Competitive Sport After Anterior Cruciate Ligament Reconstruction
Surgery. American Journal Of Sports Medicine. March 2011;39(3):538-543.
6. Adams D, Logerstedt DS, Hunter-Giordano A, Axe MJ, Snyder-Mackler L. Current concepts for anterior cruciate ligament reconstruction: a
criterion-based rehabilitation progression. J Orthop Sports Phys Ther. 2012 Jul;42(7):601-14. doi: 10.2519/jospt.2012.3871.
7. Schmitt L, Paterno M, Hewett T. The impact of quadriceps femoris strength asymmetry on functional performance at return to sport following
ACL recostruction. JOPST. 2012; 42(9):750-759.
8. Reid A, Birmingham B, Stratford P, Alcock G, Giffin R. Hop testing provides a reliable and valid outcome measure during rehabilitation after
anterior cruciate ligament reconstruction. Phys Ther. 2007; 87:337-349.
9. LOGERSTEDT D, Dl STASI S, SNYDER-MACKLER L, et al. Self-Reported Knee Function Can Identify Athletes Who Fail Return-to-Activity Criteria
up to 1 Year After Anterior Cruciate Ligament Reconstruction: A Delaware-Oslo ACL Cohort Study. Journal Of Orthopaedic & Sports Physical
Therapy. December 2014;44(12):914-923.
10. Angelozzi M, Madama M, Cacchio A, et al. Rate of Force Development as an Adjunctive Outcome Measure for Return-to-Sport Decisions After
Anterior Cruciate Ligament Reconstruction. Journal Of Orthopaedic & Sports Physical Therapy. Sept 2012 ;42(9):772-780.
11. Hartigan E, Axe M, Snyder-Mackler L. Time Line for Noncopers to Pass Return-to-Sports Criteria After Anterior Cruciate Ligament
Reconstruction. JOSPT. 2010;40(3):141-154.
12. Hu F, Chmieleski T, Spindler K, Wilk K, Swiontkowski M, Marx R. Return to Sport after ACL Reconstruction. JOSPT & JBJS Webinar. Nov 2014.
13. Mueller L, Bloomer B, Durall C. Which Outcome Measures Should Be Used to Determine Readiness to Play After ACL Reconstruction?. Journal
Of Sport Rehabilitation. May 2014;23(2):158-164.

