innovations in treatment of perianal crohn disease ... · pdf fileof perianal crohn disease...
TRANSCRIPT

Dipartimento di Scienze Mediche e Chirurgiche Istituto di Clinica Chirurgica
Prof. Aroldo FianchiniAncona
INNOVATIONSIN TREATMENT OF PERIANAL
CROHN DISEASE combined therapy
Cristina Marmorale

PERIANAL CROHN DISEASE
22-23% occurence of perianalcrohn disease
12% AT 1 YEAR15% AT 5 YEARS21% AT 10 YEARS26% AT 20 YEARS
12% WITH ISOLATED ILEAL DISEASE15% WITH ILEOCOLONIC DISEASE 41% WITH COLONIC DISEASE AND RECTAL SPARING92% WITH COLONIC DISEASE INVOLVING THE RECTUM
Perianalfistulae
LOW QUALITY OF LIFE
54 % perianal complications in Crohn disease
Digestive and Liver Disease 39 (2007) 959–962 & ECCO Consensus on CD 2010 : Special situations

CLASSIFICATION OF PERIANAL LESIONS
• FISSURES
• SKIN TAGS E HEMORROID DISEASE
• PENTRATING ULCERS
PRIMITIVE SECONDARY
• FISTULAS
• ABSCESSES
• STENOSIS
• CANCER

PATHOGENESIS OF FISTULAE
ANAL GLAND INFECTION TRACKS ALONG INTERSPHINCTERIC SPACE
PENTRATING ULCERS (primary lesions) EXTEND WITH FORMATION OF ABSCESSES AND FISTULAS (secondary lesions)

PARK’S Classification
(1) SUPERFICIAL
(2) INTER-SPHINCTERIC
(3) TRANS-SPHINCTERIC
(4) SUPRA-SPHINCTERIC
(5) EXTRA-SPHINCTERIC FISTULAS
Parks AG, Gordon PH, Hardcastle JD. A classification of fistula-in-ano. Br J Surg 1976;63:1–12

AGA 2003CLASSIFICATION
SIMPLE
COMPLEX
Gastoenterology 2003; 125:1508–1530
- PHISICAL ISPECTION OF PERIANAL AREAS
- RECTOSIGMOIDOSCOPY
THIS CLASSIFICATION IS THE MORE USED IN CLINICAL PRACTICE. SIMPLE FISTULAS ARE MORE RESPONSIVE TO TREATMENT , INSTEAD COMPLEX FISTULAS ARE OFTEN REFRATTARY AND SURGERY CAN CAUSE INCONTINENCE IN SOME CASES


DIAGNOSIS AND EVALUATION OF PERIANAL CROHN DISEASE

ASSESS THE NUTRITIONAL STATUS OF THE PATIENT
LOCATE THE ORIGIN OF THE FISTULA AND ITS ANATOMY
EVALUATE THE ORIGINATING INTESTINAL LOOP (INFLAMMATION OR STENOSIS)
IDENTIFY OR EXCLUDE LOCAL SEPSIS (ABSCESS)
DETERMINE WHICH ORGANS ARE AFFECTED AND THEIR CONTRIBUTION TO SYSTEMIC SYMPTOMS OR IMPAIRMENT OF THE QUALITY OF LIFE
OBBIECTIVE

PELVIC MAGNETIC RISONANCE

EXAMINATION UNDER ANAESTHESIA

ANORECTAL ULTRASOUND

PROCTOSIGMOIDOSCOPY

CONVENTIONAL TREATMENT APPROACH FOR CROHN DISEASE

SURGICAL PROCEDURES FOR PERIANAL CROHN'S DISEASE
EMERGENCY TREATMENT OF SEPSIS INCISION AND DRAINAGE OF ABSCESS
DAMAGE LIMITATION SETON DRAIN “BRIDGING “ DEFUNCTIONING STOMA
DEFINITIVE TREATMENT FISTULOTOMY FISTULECTOMYFLAP REPAIR OF FISTULAINTERNAL SPHINCTEROTOMY
INTESTINAL RESECTION PROCTECTOMY OR PROCTOCOLECTOMYPROXIMAL RESECTION
British journal of surgery 2004; 91: 801–814
Dis Colon Rectum 2005; 48: 1337–1342

TREATMENT OF FISTULATING DISEASE
SIMPLE PERIANAL FISTULAE

EMERGENCY TREATMENT OF SEPSIS
INCISION AND DRAINAGE OF ABSCESES
INSERTION OF SETON DRAIN

“BRIDGING PERIOD”
Non cutting SETON OOSTOMY
The Management of Perianal Crohn’s DiseaseAm J Gastroenterol 2007;102:S85–S87
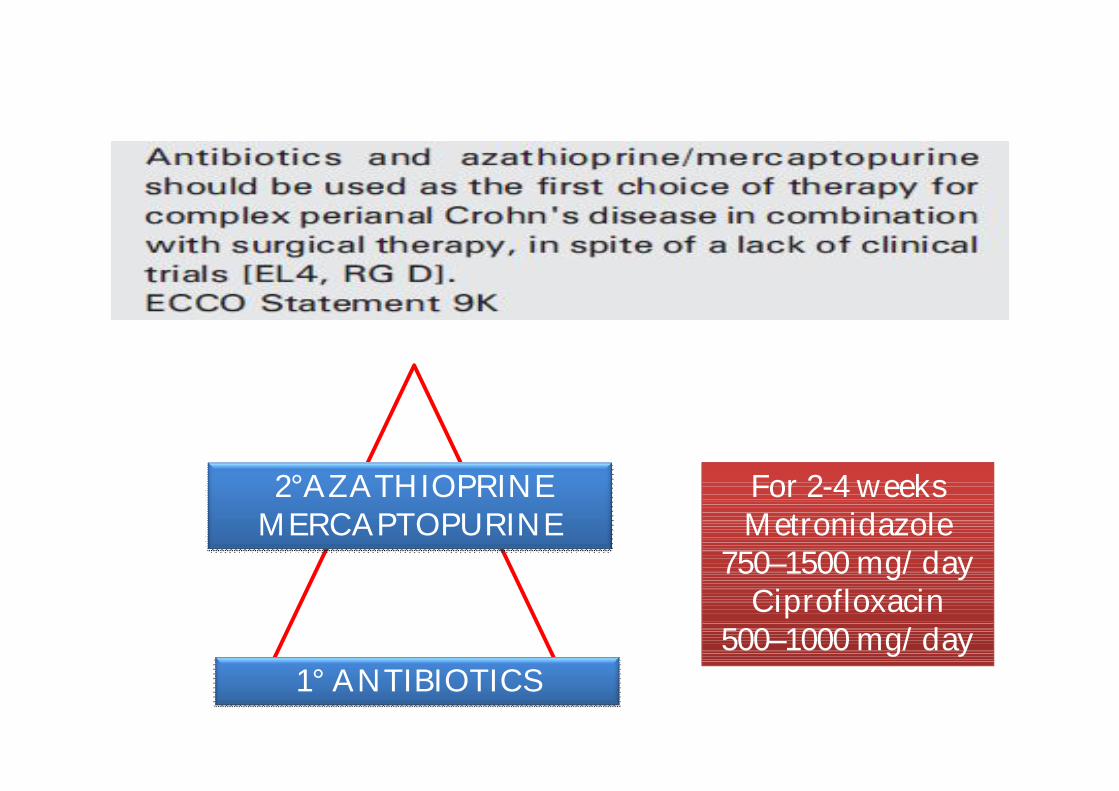
1° ANTIBIOTICS
For 2-4 weeksMetronidazole
750–1500 mg/dayCiprofloxacin
500–1000 mg/day
2°AZATHIOPRINEMERCAPTOPURINE

COMPLEX PERIANAL FISTULAE
It Will be a difficulOperation?
Don’t worryI have a calculator…

3° INFLIXIMABADALIMUMAB
2°AZATHIOPRINEMERCAPTOPURINE
1° ANTIBIOTICS
FAIL
FAIL
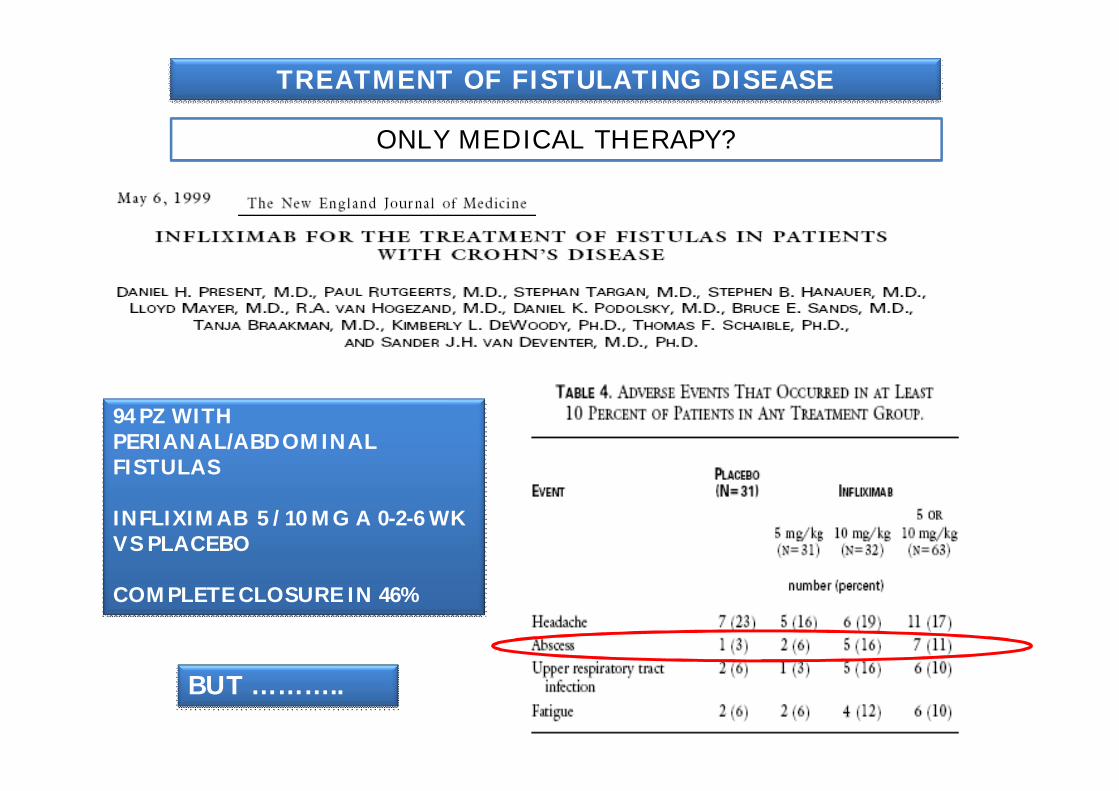
94 PZ WITH PERIANAL/ABDOMINAL FISTULAS
INFLIXIMAB 5 / 10 MG A 0-2-6 WK VS PLACEBO
COMPLETE CLOSURE IN 46%
BUT ………..
TREATMENT OF FISTULATING DISEASE
ONLY MEDICAL THERAPY?
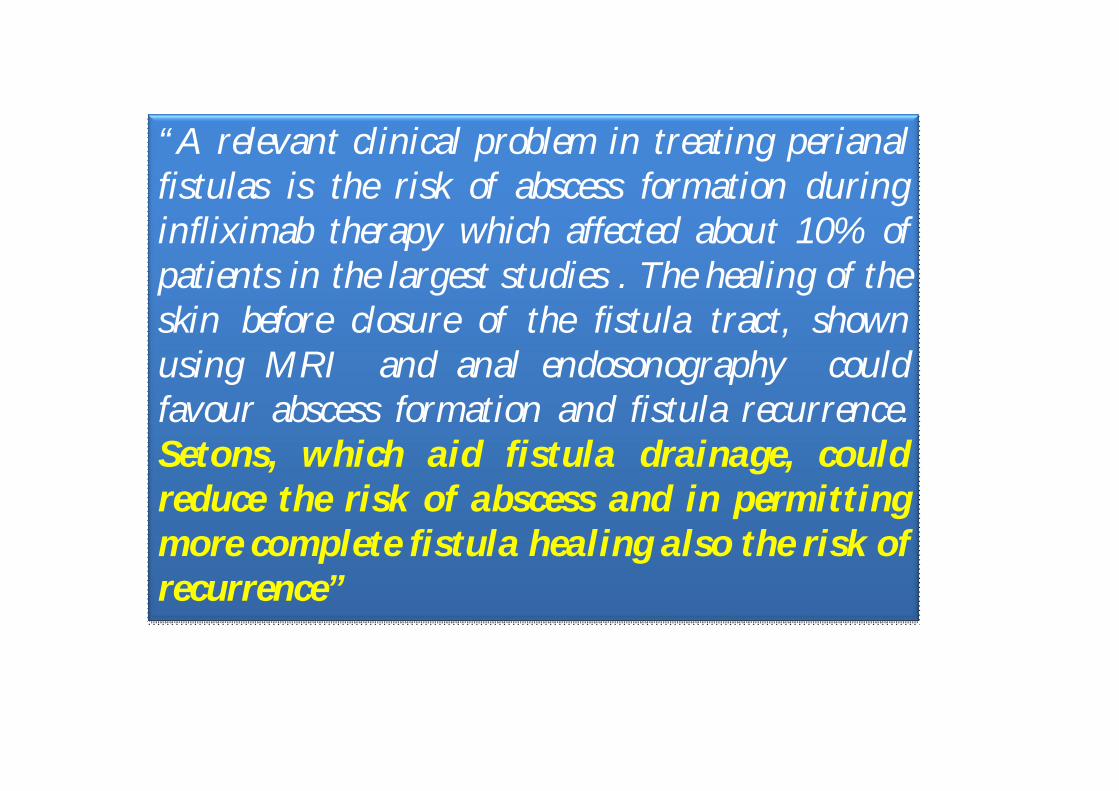
“A relevant clinical problem in treating perianalfistulas is the risk of abscess formation duringinfliximab therapy which affected about 10% ofpatients in the largest studies . The healing of theskin before closure of the fistula tract, shownusing MRI and anal endosonography couldfavour abscess formation and fistula recurrence.Setons, which aid fistula drainage, couldreduce the risk of abscess and in permittingmore complete fistula healing also the risk ofrecurrence”

3° INFLIXIMABADALIMUMAB
2°AZATHIOPRINEMERCAPTOPURINE
1° ANTIBIOTICS
SURGERY

Hippocrates, great Greek physician of the fifth century B.C., is pictured palpating a young patient. Kindliness and concern, embodied in his aphorism, “Where there is love for mankind, there is the love for the art of healing,” are reflected in Hippocrates’ face. This revered practitioner, scientist, and teacher, well deserved the title, “Father of medicine,” which has been associated with his name for more than 2,000 years.
COMBINED THERAPY

Inflamm Bowel Dis. 2003 Mar;9(2):98-103Treatment of perianal fistulizing Crohn's disease with infliximab alone or as an adjunct to exam under anesthesia with seton placement.Regueiro M, Mardini H.University of Pittsburgh School of Medicine, Presbyterian Hospital, Pittsburgh, Pennsylvania 15261, USA.
Colorectal Disease, 2004 ; 7: 164–168Infliximab in the surgical management of complex fistulating anal Crohn’s diseaseC. Talbot*, P. M. Sagar*, M. J. Johnston*, P. J. Finan* and D. Burke**Division of Colon and Rectal Surgery, The General Infirmary at Leeds, United Kingdom
Tech Coloproctol (2008) 12:111–117Combined therapy with infliximab and seton drainagefor perianal fistulizing Crohn’s disease with anal endosonographic monitoring: a single-centre experienceL. Guidi C. Ratto S. Semeraro I. Roberto I. De Vitis A. Papa M. Marzo A. Parello G. Foglietto G.B. Doglietto G.B.Gasbarrini G.FedDipartimento di Scienze Chirurgiche Università Cattolica del Sacro Cuore, Roma, Italy
COMBINED THERAPY
Dis Colon Rectum. 2003 May;46(5):577-83. Combined seton placement, infliximab infusion, and maintenance munosuppressives improve healing rate in fistulizing anorectal Crohn's disease: a single center experience.Topstad DR, Panaccione R, Heine JA, Johnson DR, MacLean AR, Buie WD.Department of Surgery, Foothills Hospital, University of Calgary, Calgary, Alberta, C
Dis Colon Rectum 2006; 49: 1837–1841Fistulating Anal Crohn’s Disease: Results of Combined Surgical and Infliximab TreatmentSyed A. Hyder, F.R.C.S.,1 Simon P. L. Travis, F.R.C.P.,2 Derek P. Jewell, F.R.C.P.,2 Neil J. McC. Mortensen, F.R.C.S.,1 Bruce D. George, F.R.C.S.,1
Dig Dis Sci (2009) 54:1746–1752Predicting Factors of Fistula Healing and Clinical Remission After Infliximab-Based Combined Therapy for Perianal FistulizingCrohn’s DiseaseDavid Tougeron Guillaume Savoye Ce´line Savoye-Collet Edith Koning Francis Michot Eric LereboursDepartment of Surgery, Rouen University Hospital C Nicolle,1 rue de Germont, 76031 Rouen, France

INFLIXIMAB
COMBINED THERAPY

COMPLEX PERIANAL FISTULAE
CONSERVATIVE TREATMENT
SURGERON GASTROENTEROLOGIST


Dig Dis Sci (2009) 54:1746–1752
INTRALESION INFLIXIMAB
Dis Colon Rectum, April 2005
Scand J Gastroenterol. 2006 Sep;41(9):1064-72.Treatment Of Perianal Fistulas In Crohn's Disease By Local Injection
Of Antibody To Tnf-alpha Accounts For A Favourable ClinicalResponse In Selected Cases: A Pilot Study.
Asteria Cr , Ficari F , Bagnoli S , Milla M , Tonelli F.

LOCAL THERAPY: WILL BE THE FUTURE?
TOPICAL TACROLIMUS
FIBRIN GLUE
INTRALESION INFLIXIMAB
ADIPOSE DERIVED STEM CELL TERAPY
FISTULA PLUG