information to users - digitool.library.mcgill.cadigitool.library.mcgill.ca/thesisfile36974.pdf ·...
TRANSCRIPT

INFORMATION TO USERS
This manuscript has been reproduced from the microfnm master. UMI films
the text directJy from the original or copy submitted. Thus, sorne thesis and
dissertation copies are in typewriter face, white ethers may be from any type of
computer printer.
The quality of this reproduction Is dependent upon the quallty of the
copy submitted. Broken or indistinct print, colored or paer quality illustrations
and photographs, print bleedthrough. substandard margins, and improper
alignment can adversely affect reproduction.
ln the unlikely event that the author did not send UMI a complete manuscript
and there are missing pages, these will be noted. Aise, if unauthorized
copyright material had to be removed, a note will indicate the deletien.
Oversize materials (e.g., maps, drawings, charts) are reproduced by
sectioning the original, beginning at the upper left-hand corner and continuing
from left to right in equal sections with small overfaps.
Proauest Information and Leaming300 North Zeeb Road, Ann Arbor, MI 48106-1346 USA
800-521-0600

Genetie Epidemiology and Phenotypie Resolution ofComplex Traits: Studies in Specifie
Language Impainnent and A1coholism
Mr. Dija Kovac
Department ofBiology
MeGill University~ Montreal
A thesis submitted to the Faeulty ofGraduate Studies and Research in partial fulfillment
of the requirements ofthe degree ofPh.D.
Copyright © Ilija Kavac 2000

1+1 Nationallibraryof Canada
AcQuisitions andBibliographie Services
385 W"'tgIDn Str.-t0Iawa ON K1A 0N4CIn8da
BiIUoIhèQue nationaledu Canada
Acquisitions etservices bibliographiques
385. rue wlllingtanoa-aON K1ACN4CIMda
The autbor bas granted a nonexclusive licence alloWÎDg theNational Library ofCanada toreproduce, lolD, distnDute or sencopies ofthis thesis in microform,paper or electronic formats.
The author retains ownership ofthecopyright in tbis thesis. Neither thethesis nor substantial extracts trom itmay he printed or otherwisereproduced without the author'spermission.
0-612-70064-X
Canadl
L'auteur a accordé une licence nonexclusive permettant à laBibliothèque nationale du Canada dereproduire, prêter, distrIbuer ouvendre des copies de cette thèse sousla forme de microfiche/film, dereproduction sur papier ou sur formatélectronique.
L'auteur CODSeIVe la propriété dudroit d'auteur qui protège cette thèse.Ni la thèse ni des extraits substantielsde celle-ci ne doivent être imprimésou autrement reproduits sans sonautorisation.

Mojlm roditeljima, Mlrjani i Petru KovaC
To my parents, Mirjana and Petar KovaC

TABLE Of CONTENTS
List ofFigures vii
List ofTables and Appendices viii
Abstraet Xl
Résumé xiii
Preface xv
Acknowledgements xv
Con~butionofAu~oΠ~
Major Contributions to Original Knowledge XIX
Prologue XXI
1. Introduction 1
Rationale and Objectives 1
1.1. Genetic Analysis ofComplex Traits 3
1.1.1. Charaeteristics ofComplex Traits 3
1. 1.2. Major Approaches to Genetic Analysis ofComplex Traits 5
1.1.2.1. Major Methods in Human Statistical Genetics 5
1.1.2.2. Biological Approaches 8
1.2. Phenotype Definition in Genetic Analysis ofComplex Traits 9
1.3. Summary 17
iii
2. Phenotype Dermition iD Specifie Language Impairment (SU) 17
2.1. The Diagnosis and Etiology ofSLI 17
2.2. Potential for Improvement ofPhenotype Definition in SLI 24
2.3. Specific Components ofthe Grammatical Phenotype in SLI 26
2.4. The SLI Phenotype and Attention DeficitIHyperactivity 29
2.5. Summary 34
2(8). Sibling Resemblance for Specifie Components 01Linguistie
Competence in Families 01 Speecb/Language Impaired Cbildren 35
Abstraet 37
Introduction 38
Subjeets and Methods 40
Results 48
Discussion 58
Appendix 64
Bridging Commentary 65
2(b). Attention DefieitlHyperaetivity in SLI Children lDereases Risk of
Speecb/Language Disorden in Fint-Degree Relatives:
A Preliminary Report 66
Abstract 68
iv
Introduction 69
Method 71
Results 7S
Discussion 84
Appendix 89
Commentary 90
3. Phenotype Definition in Alcoholism 92
3.1. The Diagnosis and Etiology ofAlcoholism 92
3.2. Phenotypes in Molecular Genetic Studies ofAlcoholism 9S
3.3. Major Aspects ofPhenotypic Heterogeneity in Alcoholism 97
3.3.1. Early Onset and Late Onset Alcoholism 100
3.3.2. Alcoholism and Antisocial Personality Disorder 106
3.4. Summary 112
3(8). Exploring Phenotypes in Alcobolism: Unrestricted Latent Class Analysis of
Antisocial Behaviors in Alcobol Dependent Males and Females witb Divene
Social AdjustmeDt 113
Abstract IlS
Introduction 117
Subjeets and Methods 119
v

Results 128
Discussion 142
AppendixA 148
AppendixB 149
Bridging ComlDentary ISO
3(b). ExploriDg the Impact of Extended Phenotype in Stratified Samples 158
Copyright Notice IS8
Introduction 1S9 (S211)
Methods 160 (S212)
Results 161 (8213)
Discussion 164 (S216)
4. Final Summary and Conclusions 165
References 178
VI
List ofFigures
Copter %(b).
Attention DefieitIHyperadivity in SU Children lDereases Risk of SpeecbJLanguage
Disorden in Fint-Degree Relatives: A PreliDliDary Report 66
Figure 1. Selection and Subgrouping ofSLI Families 72
Cbapter 3(a).
Exploring Pbenotypes in Aleobolism: Unrestrieted Latent ClaIS Analysis of
Antisocial &ehavion in A1eohol Dependent Males and Females with Divene Social
Adjutment 113
Figure 1. Observed Gender and Symptom Endorsement Probabilities in ASPD Symptom
Based Latent Classes (N = 236, 121 male, 115 female) 130
Figure 2. Observed Gender and Symptom Endorsement Probabilities in CD Symptom
Based Latent Classes (N = 236, 121 male, 115 female) 134
VII
List ofTables and Appendices
ChapterZ.
Phenotype Definition in Specifie Language Impairment (SLI) 17
Table 1. Proportions ofAffeeted First-Degree Relatives in SLI Probands and Control
Subjects 20
Chapter 2(a).
Sibling Resemblance for Specifie Components of Linguistic Competence in F.milies
ofSpeecb/Language Impaired Children 35
Table 1. Language Tests 43
Table 2. Age and Sex Matched Case-Control Comparison ofTest Scores 50
Table 3. Test and Age at Testing Correlations in the English Test Group 52
Table 4. Test and Age at Testing Correlations in the French Test Group 53
Table 5. Sibling Correlations for Specific Components ofLinguistic Competence 55
Table 6. Partial Sibling Correlations Controlling for Age at Testing 57
Appendix. Analyzed Subjects by Test Language and Familial Relationships 64
Chapter 2(b).
Attention DeficitIHyperactivity in SLI Cbildren Increases Risk of SpeecblLanguage
Disorden in Fint-Degree Relatives: A Preliminary Report 66
viii

Table 1. Family History Report for First-Degree Relatives 79
Table 2. Classification ofFirst-Degree Relatives by Family History Report 80
Table 3. Risk by Type ofFirst-Degree Relative 82
Appendix. Family History Questionnaire 89
Chapter 3(a).
Exploring Phenotypes in Alcobolism: Unrestrieted Latent ClaIS Analysis of
ADtisocial Bebavion in Alcobol Dependent Males and Females witb Divene Soeial
Adjustment 113
Table 1. Adult and Childhood Antisocial Behaviors 122
Table 2. Prevalence ofAntisocial Behaviors by Gender 123
Table 3. LCA Model Fitting for ASPD Symptoms in Alcohol Dependent
Males and Females 129
Table 4. LCA Madel Fitting for Conduct Disorder Symptoms in Alcohol Dependent
Males and Females 133
Table 5. Cross-tabulation of ASPD and CD Symptom Based Latent Classes
Stratified by Gender 136
Table 6. Comparison ofLatent Classes Derived from ASPD Symptoms: Alcohol
Dependent Males 137
Table 7. Comparison ofLatent Classes Derived from ASPD Symptoms: Alcohol
Dependent Females 138
Table 8. Psychiatric Co-morbidity in ASPD Symptom Based Latent Classes 141
ix
Appendix A. Symptom Endorsement Probabilities Observed in Latent Classes ofAlcohol
Dependent Individuals Derived ftom Behavioral Symptoms ofASPD
(After 15yr ofAge) 148
Appendix B. Symptom Endorsement Probabilities Observed in Latent Classes ofAlcohol
Dependent Individuals Derived ftom Behavioral Symptoms ofCD
(Before 15yr ofAge) 149
Chapter 3(b).
Exploring the Impact of Extended Phenotype iD Stntified SaDlpies 158
Table 1. Nominally Significant ÙlCi in the Early Subgroup at p < 0.01 162 (S214)
Table 2. Nominally Significant Loci in the Late Subgroup 163 (S215)
Table 3. Allele Sharing in Full Sib Pairs and Sample Sîzes at the ADH3 Functional
Candidate Gene on Chromosome 4 164 (S216)
x
ABSTRACT
Rationale. Definition ofcomplex bebavioral disorders is generally phenomenological in
nature and guided by pragmatic~ rather than genetic, concems. Consequently, important
aspect ofgenetic analysis is the search for novel phenotypic definitions from the
familial/genetic perspective. SU Study 1. SLI denotes an inability to acquire normal
language in the absence ofPeripheral hearing impairmen~ neurological disorder. and
mental retardation. Sibling resemblance for several theoretica11y derived specific
components of the SLI phenotype was examined in families ofSLI children. In 38 sib
pairs from 10 French-speaking pedigrees, Verb Tense Morphology sulrtests (Real and
Non-real Words) showed nonparametric correlations of0.39 and 0.35, respectl\'el~'
(p<O.05, 2-tailed). In a densely atTccted Anglophone pedigree~ 41 sib-pair showed
familial resemblance with reSPect to Derivational Morphology (F 0.52.. p<O_OI )
SLI Study 2. Family history study in 27 families examined the relationship bet\\'CCn
attention deficit/hyperactivity in SLI children and familial risk ofspeech/language
disorders. Higher odds ofspeech/language disorders were ohserved in first-degree
relatives of 13 SLI children who also had a Medical record ofattention
deficit/hyPeractivity (15/27 vs. 4/46, p=O.OOI). Alcobolism Study 1. Latent class analysis
(LCA) including gender and IS antisocial behaviors (> 15yr) was perfonned in 236
broadly ascenained alcohol.clependent subjects (121 males~ 115 females). Evidence for 3
qualitative behavioral classes was obtained: Socially Adjusted Adults, SAA; Antisocial
xi

Non-Aggressive Adults, ANAA; and Antisocial Agressive Adults, AAA In both
genders, the AAA class had the earliest age ofonset for alcohol dependence (p=O.OO1),
more alcoholic first-degree relatives and more ofother psychopathology. In females, the
ANAA class was intermediate. In the ANAA males, socially adjusted childhood behavior
ditTerentiated the late onset ftom the intermediate onset subgroup. A1coholism Study 2.
Initial sib-pair genome scans were performed in Pedigrees with the pedigree Mean carly
(N=52) and late-onset (N=S3) ofalcoholism from the COGA data set distributed for
GAWIl. Traits ofalcoholism, smoking, and addiction (either alcoholism or smoking)
were examined Subgroups and phenotypes influenced results, the interpretation ofwhich
is a1so discussed in view ofmethodological issues. Conclusion. Complexity ofSLI and
alcoholism is used to derive phenotypes that cao potentially increase the power of
statistical genetic mapping.
XII

RÉsUMÉ
RaisonnelDent. La définition des troubles bébavioraux complexes est généralement de
nature phénoménologique et guidée par des intérêts d'ordre pratique plutôt que
génétique. Par conséquent, la recherche de rlé+1"itions phénotypiques nouvelles dans une
perspective familiale/génétique constitue un aspect important de l'analyse génétique.
Étude SLI no 1. SLI (Specifie Language Impainnent) dénote l'incapacité d'acquérir un
langage nonnal en l'absence d'une atteinte à l'audition périphérique, d'un trouble
neurologique, ou de retard mental. Est examinée la ressemblance entre frères et/ou soeurs
de familles comportant des enfants atteints de SU, en ce qui a trait à un certain nombre
de composantes particuliéres du phénotype Su, dérivées théoriquement. Parmi 38
couples de frères et/ou soeurs chez 10 familles de pedigree francophone, des sous-tests
portant sur la morphologie verbe-temps (mots réels et nOD réels) ont démontré des
corrélations nonparamétriques de 0.39 et 0.35, respectivement (p<O.OS, 2 queues). Chez
un pedigree anglophone densément affecté, 41 couples de frères et/ou soeurs ont
démontré une ressemblance familiale en termes de morphologie dérivationnelle (r=O.52,
p<0.01). Étude SLI no 2. Une étude sur les antécédents familiaux portant sur 27 familles
examine la relation entre le défici de l'attention/hyperactivité chez des enfants atteints de
SLI et le risque, relié à la famille, de développer des troubles du langage. On a observé
une plus grande probabilité de développer des troubles du langage chez les parents de
premier degré de 13 enfants atteints de SLI, qui avaient également des antécédents
xiii
médicaux de déficit de r'attention/hyperactivité (15/27 contre 4/46, p=O.OOI). Étude sur
sujets alcooliques no 1. Une analyse de classe latente incluant le sexe et IS
comportements antisociaux (>lS ans) fut effectuée chez 236 sujets classés comme
alcooliques d'apres des critères généraux (121 hommes, 115 femmes). Des données
sur 3 catégories bébaviorales qualitatives furent obtenues: Adultes Socialement Adaptés
(ASA); Adultes Antisociaux non Agressifs (AANA); et Adultes Antisociaux Agressifs
(MA). Chez les deux sexes, la catégorie MA révélait la manifestation la plus précoce
de déPelldence alcoolique (p=O.OOI), ainsi qu'un plus grand nombre de paents de premier
degré alcooliques et un plus grand nombre de psychopathologies. Chez les femmes, la
catégorie AANA était intermédiaire. Chez les hommes AANA, un comportant
socialement adapté dès l'enfance différenciait le sous-grope au développement tardifde
celui ayant un développement plus précoce. Étude sur sujets alcooliques no 2. Des scans
initiaux de génomes appartenant à des couples frères et/ou soeurs ont été effectués chez
les pedigrees, la moyenne des pedigrees à manifestation d'alcoolisme précoce (N=S2) et
tardive (N=3) de l'ensemble des données COGA étant distribuée pour le GAWII. Les
traits suivants ont été examinés: alcoolisme, tabagisme, et dépendance (soit alcoolisme ou
tabagisme). Les sous-groupes et les phénotypes ont influencé les résultats, don't
l'intepretation fait l'objet d'une discussion portant, en autres, sur des questions de
méthodologie. Conclusion. La complexité du SU et de l'alcoolisme est utilisée pour
dériver des phénotypes pouvant accroître la puissance des statistiques appliquées à la
cartographie de gênes.
xiv
PREFACE
Acknowledgements
The work presented in this thesis is multidisciplinary and was made possible by
contributions ofMany people ofdifferent backgrounds!t too numerous to Imow and
mention aIl in this space. 1have benefited greatly from intellectual exchanges with Dr.
Roberta Palmour, my thesis supervisor. In addition, Dr. Palmour generously agreed to my
pursuit of research that is congruent with my interests, and this is much appreciated.
Other stimulating intellectual contacts, that 1can recall at this time, include Dr. Ken
Mor~ Dr. Clarke Fraser (ret), and also Dr. Guy Rouleau. Particular mention goes to Or.
Chantal Mérette, whose hospitality and cooperativeness introduced me funher to the first
band research experience. Radha Allard and Berdj Garabedian were very helpful in the
course of consolidating data from various sources in the Genetic Language Impainnent
Project. Finally, during my training Many fellow students ofDr. Palmour made the lab
environment and my experience a positive one.
xv

Contribution ofAuthors
This thesis includes 4 co-authored scientifie manuscripts, submitted to or
published in scientifie joumals. These manuscripts, copyrights where applicable~ and
contnbutions of individual co-authors are listed below. Ali manuscripts were also co
authored by my thesis supervisor, Dr. Roberta Palmour.
Chapter 2(a)
'~Sibling Resemblance for Specifie Components ofLinguistic Competence in Families of
SpeechlLanguage Impaired Children"; co-authored with Or. Myrna Gopnik, and
submitted to the Journal ofNeurolinguistics.
1have designed and implemented data analysis, and interpreted results. Dr Myrna
Gopnik, Dept. Linguistics, was the Principal Investigator in the McGill Genetic Language
Impainnent Project (GLIP). Dr. Gopnik designed the criteria according to which her
research group selected families for language testing in the GLIP projeet. Dr. Gopnik also
designed the language test instrument and supervised aetual testing, which was performed
by her linguistic research group.
XVI

Chapter 2(b)
«Attention DeficitIHyperactivitt in SU Children Increases Risk ofSpeechlLanguage
Disorders in First-Degree Relatives: A Preliminary Report"; co-authored with Berdj
Garabedian and Cbristele Du Souich, and submiued to the Journal ofCommunication
Disorders.
1have designed and implemented inclusion/exclusion criteria for specific
language impainnent (SLI) in this particular study, data analysis, and interpreted results.
Berdj Garabedian examined original Medical records, mostly in French language, and
prepared summarized Medical record information that was used in this study. Christele du
Souich condueted family history telephone interviews.
Chapter 3(a)
~'Exploring Phenotypes in Alcoholism: Unrestrieted Latent Class Analysis ofAntisocial
Behaviors in Alcohol Dependent Males and Females with Diverse Social Adjustment";
co-authored with Dr. Chantal Merette, Mireille Cayer, Lucie Legault, and Dr. Maurice
Dongier, and submitted to Alcoholism: Clinical and Experimental Research.
1have designed and implemented data analysis, and interpreted results. Dr
Chantal Merette reviewed statistical analyses, provided useful input on presentation of
results and, with the help ofMireille Cayer, independently repeated presented statistical
analyses. Dr Merette also POinted out a statistical issue in the analysis of the relationship
between childhood and adult latent classes, which 1corrected. Or. Maurice Dongier and
Lucie Legault actively participated in the recruitment ofsubjects, data collection and
xvii

•
preparatio~ within the Montreal centre ofthe International WHOIISBRA Study ofState
and Trait Markers ofAlcoholism.
Chapter 3(b)
"Exploring the Impact ofExtended Phenotype in Stratified Samples"; ~authored with
Eric Rouillard and Dr. Chantal Merette. This manuscript is published in Genetie
Epidemiology 17(Suppll), S211-S216 (1999). Copyright@ Wiley-Liss, Inc. The
Collaborative Group for Research 00 Genetics ofAlcoholism (COGA) distnbuted the
analyzed data set to participants ofthe Genetic Analysis Workshop Il held in Arcachon,
France, 1998, where a part ofthis study was presented as a poster.
1have designed and implemented data analysis, and interpreted results. Eric
Rouillard provided helpful advice in mastering teehnical aspects ofcomputer-based
linkage analysis. Dr. Merette provided her expertise in examinatioo of my study proposaI,
and generaI supervision ofstatistical analyses.
xviii

•
Major Contributions to Original Knowledge
Cbapter 2(a)
Included manuscript, in submissioD, examined sibling resemblance for various
theoretically derived specifie components oflinguistie competence in anglophone or
francophone families ofSLI children. Among these varied components, Verbal Tense
Morphology and Derivational Morphology showed greatest sibling resemblance. These
phenotypic components May therefore he ofpartieular interest for further familiaVgenetic
studies.
Chapter 2(b)
Included !!!a!l'lSCrip~ in submission, provides preliminary evidence of increased
risk ofspeechllanguage disorders in first-degree relatives ofSLI children who also have
attention deficit and/or hyperactivity behavioral problems. In addition, the evidence
Persists when relatives with leaminglreading disorders, often associated with
speech/language disorders, are counted as unaffected, making for a more robust result.
These findings merit further investigation ofthe relationship between SLI and attention
deficitlhyperactivity, which is ofpotential interest for genetic studies in SLI.
xix

Chapter 3(a)
Ineluded manuscript, in submission, provides evidence for qualitative
differentiation ofalcohol dependent individuals with respect to patterns ofspecifie
antisocial bebaviors, rather than continuous variation along the single dimension of
"severity". This result is ofpotential interest for genetic mapping studies, which are
currently focused on less precisely defined antisocial alcoholism.
Cbapter 3(b)
Included manuscript, published in a scientific journal, explores the impact of
phenotype-based stratification in statistical genetic analysis ofalcoholism as a complex
trait (an initial genome scan), and provides opportunity to compare results with
statistically identical analysis ofthe same, but unstratified, data set reported by original
investigators. In addition, potential impact ofphenotype definition that encompasses
alcoholism and/or smoking, a genetically correlated trait, is explored The results suggest
that, under certain conditions, these phenotype-based approaches may he heneficial for
identification of some genetic risk factors in complex traits.
xx
PROLOGUE
The ingenious discovery of laws according ta which genes, unobserved at the
time, are transmitted from parents ta otIspring was possible only because Gregor Mendel,
unknowingly, studied a particular class ofphenotypes. These phenotypes were
determined entirely by the information content ofthe DNA sequence al single genetic
loci, regardless ofthe variable ontogenetic context ofother genetic and environmental
factors. Not surprisingly, developmentaI biologists were among the first to articulate an
organismic perspective, which recognizes that biological organisms belong to the more
general class ofself-organizing systems, characterized by the emergence ofnovel
properties from interactions ofmultiple system elements (Von Bertalanffy, 1933, and
references therein). Likewise, experimental geneticists have long known that the
Mendelian concept ofthe phenotype applies only ta some and not a1l phenotypes
(Dobzhansky, 1937). During the past two decades, the organismic view ofthe path from
genes to phenotypes and a public sense ofurgency have forcefully converged ooto
genetics ofdevelopmental bebavioral disorders.
XXI

1. INTRODUCTION
RATIONALE AND OBJECTIVES
Rationale
The genetic basis ofMany disorders showing Mendelian inheritance has bccn
identified in the past decades. Complex disorders by definition do not show Mendehan
inheritance, and require more elaborate approaches to genetic analysis. In panlcular.
phenomenological clinical diagnoses ofcomplex behavioral disorders are poorly sUltcd
for genetic studies. The derivation ofnovel, more homogenous phenotypes. from the
familiaVgenetic perspective holds the potential to improve the power for statlstlcal
identification ofgenetic risk factors. In this work, we focus upon two eomplex bcha\'loral
disorders [specifie language impairment (SLD and alcoholism], ta which these
generalizations apply.
Objectives
1. To examine which ofa variety ofdifferent, theoretically derived components ofthe
SLI phenotype May show the greatest sibling resemblance.
1
2. To examine whether the risk ofspeecb/language disorder in first-degree relatives is
greater in 811 children who also bave attention deficitlhyperaetivity bebavioral
problems.
3. To examine whether subgroups ofalcohol-dependent individuals \vith distinctive
patterns ofspecific antisocial behaviors cao he empirically defined using a
multivariate statistical approach.
4. To examine the impact ofstratification inta the early and late-onset subgroups on the
results from the initial genome scan ofalcohol dependence, performed on the COGA
data set from the Genetic Analysis Workshop Il.
Details ofthe background pertinent to the aixl";e rationale and objectives are
presented further in this chapter.
2
1.1. GENETIC ANALYSIS OF COMPLEX 1RAITS
1.1.1.Cbaracteristics ofComplex Traits
In the field ofgenetics, the term "complex trait" is commonly taken to denote any
trait that does not show simple mendelian inheritance. Following are sorne characteristic
ofsuch traits:
• No specifie genetie allele is either neeessary nor sufficient
• Common genetie aileles with low penetrance
• Genetic locus and/or allelic heterogeneity
• Pleiotropy (a gene influences multiple traits)
• Multiple genes (locus heterogeneity, additive, threshol<L inter-genic interactions or
epistasis)
• Environmental effeets
• Gene(s) x environment(s) interactions
• SPecial modes ofinheritance (imprinting, dynamic mutations, mitochondrial genes)
• Phenocopies
• Ambiguous boundaries of phenotype definition
In principle, a complex trait can show any combination, or ail ofthe above
complexities. An important premise that allows for the 44rule of thumbn inferences of
relative trait complexity is that the traits at the higher hierarchicallevel ofdevelopmental
3

•
•
organization are directIy influenced by a larger number ofgenetie and environmental
factors, and are therefore expected to he etiologically more complex (Sehork, 1997).
Accordingly, behavioral traits are expected to he the most complex because the greatest
proportion ofgenes per organ are expressed in the brain, roughly estimated at -30.000
(NINDS, 1990; SutclitTe, 1988), and their highly concerted action is constantly
influenced by interactions with the environment (Eisenberg, 1995). In agreement with
this expeetation, psychiatrie disorders are especially notorious for ambiguous boundaries
ofphenotype definition and. failure to replieate findings ofgenetic vulnerability lOCI
(Craddoek & Jones, 1999; De Lisi, 2000; Kidd, 1997; Portin & Alanen, 1997. Runer et
al. 1999).
The foundations ofcurrent, widely used DSM-IV (APA, 1994) c1assifieatlon ln
psychopathology, as weIl as problems and approaches, are reviewed in Nathan and
Langenbucher (1999). Nosologieal problems include unknown etiology9 comorbldlty and
unclear boundaries between disorders; diagnostic validity; diagnostic stability o\'er ume:
and diagnostic reliability (partieularly for schizophrenie speetrurn disorders. personahty
disorders, and sorne childhood and adolescent disorders). Andreassen (1995) proposed a
"gold" standard for validation that ineludes laboratory tests derived from
multidisciplinary approaches, in addition to traditional approaches such as cl mlcal
description and family studies; these new approaches would "link a psychiatnc dlagnosis
to its underlying abnormalities in DNAn. The latter, however, may be an overly
reductionistic statement, unlikely to hold given the ineffieiency ofaccumulated genetic
analyses which have otherwise successfully revealed DNA abnormalities in many
relatively simple disorders. Because many behavioral disorders arise from complex
4

developmental processes spanning several hierarchicallevels oforganization above the
DNA sequence, common functional genetic polymorphisms, rather than traditional rare
mutant alleles, may act as risk factors that put individuals on the probabilistic
developmental path towards a psychiatric diagnosis (Rutter et al. 1999). In agreement
with Andreassen7 s recommendation, contemporary efforts emphasize the search for
neurobiological and genetie-familial validators that eould inform etiology and treatment
ofbehavioral disorders, although perhaps in a more complex manner than traditionally
envisaged. Approaehes to identification ofgenetically relevant phenotypes, which often
do not correspond to phenomenological diagnostic categories, are outlined further in this
chapter.
1.1.2. Major Approaehes to Genetic Analysis ofComplex Traits
In this briefoverview, major methodological approaches will be provisionally
grouped on the basis of predominantly statistical versus predominantly biological
perspectives, although these arbitrary groups are necessarily more or less related.
1. 1.2.1.Major Methods in Human Statistical Genetics
Linkage Analyses
Following the notion that human DNA polymorphisms can he used as markers for
closely linked genes (Botstein et al. 1980), the genes which cause many rare Mendelian
human diseases were identified, using the classical LOD score method of linkage analysis
5

•
in large pedigrees or sets ofpedigrees (Antonarakis &. McKusick, 2000). The power of
this method depends on the correct specification ofthe genetic model of inheritance,
which usually cannot he determined in complex traits (Risch, 1992). The development of
more robust, non-parametric (genetic model-Cree) linkage methods that use only affected
pairs ofrelatives circumvented this problem (Haseman &. Eiston, 1972; Kong and Cox,
1997; Kruglyak et al. 1996; Weeks & Lange, 1988; Weeks &, Lathrop~ 1995). The basic
assumption is that, if the genetic locus is etiologically important, pairs ofatTected
relatives will share alleles in that region to a greater extent than is expected by chance.
While this strategy is less powerful than the classical LOD score analysis with the
correctly specified model, it is more robust to etiological complexity (Lander &, Schork,
1994). It is therefore frequendy applied to genetic analysis ofcomplex traits, in particular
using affected sib-pairs (Field &, Tobias, 1997; Lander &. Schork, 1994; Ott, 1999;
Tomlinson &, Bodmer, 1995; Weeks &, Lathrop, 1995).
Association Studies
Traditionai association studies compare the frequency ofaileles or genotypes
among affected individuals (cases) with those found in unaffected individuals (controls).
Particular care in case~ontrol association studies needs to he taken to avoid factors that
could cause spurious positive or negative results, such as inappropriate choice ofcontrois
which can introduce population admixture (Commings, 1998). A useful strategy in this
respect is the transmission disequilibrium test or TOT, which detects linkage as weil
(reviewed in Spielman &, Ewens, 1996). The TOT is based on the premise that a parent
heterozygous for a trait-associated ailele should more often transmit that particular aIlele
6

to an atTected child The control group is not required in TDT analysis because the
untransmitted allele is used as a controL It is argued tbat association studies are more
powerful for identification ofgenes with small effects than linkage studies, making them
suitable for detection ofvulnerability genes in complex disorders (Comings, 1998; Risch
& Merikangas, 1996).
Some Issues in Statistical Significance
Statisticallinkage analyses ofmany marker loci across the genome (genome
scans) are frequently conducted in genetic analysis ofcomplex traits. An obvious
advantage ofthis approach is coverage ofthe genome. However, multiple tests at
individual marker loci pose a particular problem with respect to statistical interpretation
of results. There are differences in opinion regarding the appropriate correction ofthe
significance criteria (Ott, 1999), with sorne authors providing statistical guidelines based
on simulation studies and others preferring judicial reporting ofuncorrected p-values
(Curtis, 1995; Lander & Kruglyak, 1995; Witte et al. 1995). In principle, empirical p
values for any study can be obtained by computer simulation under the assumption ofno
linkage, for example Brzustowicz et al. (1997) determined empirical p-values to account
for testing ofmultiple markers and multiple phenotypes in a genome scan of
schizophrenia. Other authors do not correct for multiple phenotypes, e.g. Fisher et al.
(1999) in a study ofdyslexia. Regardless of the initial p-value, the standard for declaring
statistical genetic linkage is independent replication (Lander & Kruglyak, 1995), which
however becomes progressively more difficult with the increased dependence of the
genetic locus effect on the unobserved variability among atTected individuals. The latter
7

MaY in part account for frequent non-replication oflinkage results in psychiatrie disorders
(De Lisi, 2000). Beyond statistical evidence, the 'gold" standard for declaring a gene
etiologically relevant also requires a demonstration of funetional influence on the disease
phenotype; c.g., the Apo E4 allele ofthe Apo E gene, encoding a protein that binds to P
amyloid, is one ofetiological factors in Alzheimer's disease (reviewed in Rubînsztein.,
1997).
Other Statistical Methods
In addition to the frequently used methods notOO above, there are alternatives, e.g.
models based on variance components (Amos et al. 1994; Schork, 1993; Blangero &
Almasy, 1997). A novel method based on pattern recognition in neural networks detects
contribution of individualloci as a deviation from the Mean contribution ofail marker
loci in the genome (Lucek &~ 1997). For a comprehensive overview ofstatistical and
other methods and problems in human genetic analysis, the reader is referred to Ott,
1999.
1.1.2.2. Biological Approaches
[n human genetic analysis, it cao he advantageous to use isolated populations
which may be genetically and environmentally more homogenous due to their
evolutionary history (Jorde, 1995). Moreover, animal models including various
inbreeding techniques offer experimental advantages to identifying quantitative trait loci
(QTL), each ofwhich accounts for sorne small percent ofthe variance in complex
8

disorders (Lander & Schork, 1994). The extent ta which results ftom animal studies are
relevant to humans depends on the evolutionary conservation ofthe gene and gene
fonction, and is somewbat more limited in psychiatrie disorders because corresponding
end-point phenotypes cannot readily be diagnosed in animais (Flint & Corley, 1996).
However, functional studies in humans or animais can identify a priori candidate genes
relevant to the trait in question (Hill, 1998; Lander & Schork, 1994). One problem in the
candidate gene approach to complex behavioral disorders is the large number ofpotential
candidate genes expressed in the brain, an organ characterized by highly inter-related
functional processes.
1.2. PHENOTYPIC DEFINITION IN GENETIC ANALYSIS
OF COMPLEX TRAITS
Ali ofthe statistical methods for the identification ofgenes predisposing to
complex traits lose more or less power when the effects ofvulnerability loci are sensitive
to unobserved variability among afIected individuals, so that these loci are neither
necessary nor sufficient for the expression ofthe phenotype. It is therefore important to
ineorporate additional information pertaining to tbis unobserved variability ioto the
design ofgenetic mapping studies, in order to improve the power for detection ofspecifie
genetic effeets. In addition to previously noted approaches based on multilocus methods,
special more homogenous populations, or animal inbred strains, an important strategy in
this respect is the derivation ofmore homogenous phenotype definitions (Lander &
Sehor~ 1994; Ott & Bbat, 1999; Schor~ (997). Major approaches to the definition of
9
more homogenous phenotypes can he heuristically outlined onder the themes ofclinical
characteristics, severity~ developmental chronology, family history, comorbidity, specifie
associated traits or specifie components ofthe diagnostic phenotype, and the use of
multivariate statistically derived phenotypes.
Clinical Characteristics
Many complex disorders have variable clinical characteristics that can he used to
identify more homogenous phenotypes. In the example ofdiabetes, genetie analyses of
Type 1or insulin-dependent diabetes mellitus (IDDM) identified multiple susceptibility
loci in mice and humans (reviewed in Field & Tobias, 1997; Todd, 1999). The Type 2 or
non-insulin dependent diabetes mellitus (NIDDM) is both clinically and genetically
distinct from the Type 1 diabetes (permutt et al. 1998). Neurofibromatosis Type 1 is
linked to chromosome 17 (Goldgar et al. 1989), while clinically distinct
neurofibromatosis Type 2 is Iinked to chromosome 22 (Rouleau et al. 1993). Sometimes,
as in autosomal dominant cerebellar ataxias, clinical heterogeneity is extensive even
within famiIies, 50 that disease classification requires knowledge of the underlying
genetic locus, several of which were identified in different families (reviewed in Muller
& Graeber, 1996).
Severity
For traits measured directly on the continuous scale, i.e. hypertensio~ it is
obvious that individuals at the extreme ofthe affected phenotype can he considered more
severely affected. An example ofgene mapping using this strategy is linkage ofthe
10
angiotensin gene to essential hypertension (Jeunemaitre et al. 1992). A population based
and a clinically ascertained sample were studied. In the population based sample, linkage
was observed only in the subset ofextremely hypertensive subjects, while in the clinical,
more severely affected sample, linkage was observed in the total sample. When extremely
hypertensive subjeets from both samples were pooled, the evidence for linkage was
further improved. The angiotensin gene remains a strong candidate gene for essential
hypertension, not considering rare mendelian syndromes for which single gene mutations
are shown to increase blood pressure (Dominiczak et al. 2000). In other comple" traits,
quantitative measures ofseverity cao be constructed. For example, a recent linkage study
ofschizophrenia utilized a number ofphenotypes: categorical definitions of
schizophrenia, positive-symptom (psychotic), negative-symptom (deficit) and general
psychopathology-symptom scales as quantitative traits (Brzustowicz et al. 1997).
Significant genetie linkage to chromosome 6 was observed only for the positive-
symptom..score phenotype that was interpreted as the measure ofseverity for these
symptoms. Clinical observations can also he interpreted in the conteX! ofseverity. For
eKalllple, Kendler et al. (2000) reported that affected individuals from families in which
schizophrenia was linked to chromosome 8p had significantly more affective
deterioration, poorer outcome, and more thought disorder.
Developmental Chronology
It is known that the expression ofmany genes is dependent on the stage of
development, including those expressed in the brain (e.g. Tice et al. 1996). Accordingly,
the effects ofdifferent genes predisposing to complex disorders may he expressed at
Il

different stages ofdevelopment. Consequently, the age ofonset ofcomplex disorders can
he useful for the identification ofmore homogenous phenotypes. In familial Alzheimer
disease (AD), which accounts for ....5% ofail AD cases, difTerent genetic loci are mapped
to the early onset and Jate onset AD, otherwise neuropathoJogically indistinguishable
phenotypes (reviewed in: RubinszteiD., 1997; Shastry &, Giblin, 1999). The research in
early anset forms ofbreast cancer allowed identification ofvulnerability genes (Hall et al.
1990; Sellers, 1997; Wooster et al. 1995). In diabetes, genetic mutations were identified
in the analyses ofthe maturity onset diabetes in the young (MOOY) phenotype
(Yamagata et al. 1996).
Family Historv
The requirement for multiple affected relatives is a common method of
identifying families that are more likely ta segregate susceptibility genes in complex traits
(Lander & Schork, 1994; Hill, 1998), because sporadic cases are considered less likely to
have a substantial genetic component. This approach may not he always optimal as the
power ofspecifie pedigree structures can vary dramatically among models producing
identical population prevalence and sibling recurrence rate, while random ascertainment
typically involves a modest loss ofpower (McCarthy et al. (998).
Comorbidity
Comorbidity denotes co-occurrence ofdisorders in the same individual. At the
population level, co-occurrence ofbehavioral disorders above the frequency expected by
chance is often encountered. Comorbidity has notable adverse physical, psychological
12

•
and social consequences, prompting substantial research ïnterest. Several recent reports
review findings and approaches to comorbidity in the field ofpsyehopathology (Angold et
al. 1999; Clark et al. 1995; Klein &. Riso, 1993; Nathan &. Langenbucher, 1999; Sher &,
Trull, 1996), where substance related disorders, personality disorders, depression and
anxiety show highest levels ofcomorbidity. In an influential report, Klein and Riso
(1993) outlined Il pltential causes ofcomorbidity, Many ofthose methodological
artifacts, and suggested approaches to distinguishing these models, developed further by
Neale and Kendler (1995). With familial data, sorne models ofcomorbidity can he
resolved by examining risks to relatives ofprobands with and without comorbid disorder,
e.g. Biederman et al. (1992), or by a multivariate pedigree analysis, e.g. Stallings et al.
e1997). A powerful approach to study ofcomorbidity is multivariate analysis of twin data,
whieh can disentangle relative contnbutions ofgenetic and environmental factors to
disorder speeific and comorbid variation (Kendier et al. 1987; Kendler et al. 1995;
Slutske et al. 1998). For example, Kendler et al. (1995) reported that, in female twins,
genetic influences on phobia, generalized anxiety disorder, Pallie disorder, bulimia, major
depression and alcoholism are neither highly disorder specifie (except for alcoholism) nor
highly nonspecific. Patterns ofpsychiatrie symptoms, rather than diagnostic categories,
can also be analyzed in this manner; Kendler et al. (1987) reported that genetie influences
on symptoms ofdepression and anxiety aet in a largely non-specifie way on the overall
level ofsymptoms, while some environmental factors showed a more disorder-specific
influence.
In genetic mapping studies, comorbidity could he exploited by requirement for
dual diagnosis in affeeted individuals, for example in alcoholism with antisocial
13

personality disorder (Lappalainen et al. 1998). The association ofalcoholism and
antisocial personality disorder, for which there is evidence ofcommon genetic factors, is
presented in more detail in the Chapter 3. Another approach may he to use severa!
phenotype definitions that eneompass increasing number ofdiagnostic categories, some
ofwhich May represent diagnostic sub-threshold syndromes for the disorder of interest.
Forexample, Straub and coworkers (1995) used 4 increasingly broad phenotype
definitions in the study ofschizopbrenia. These definitions were: narrow - schizophrenia,
poor outcome schizophrenie affective disorder, and simple schizophrenia; intennediate
narrow plus schizotypal personality disorder, and non·affective psychotic disorders; broad
- intermediate plus pgychotic affective illness, paranoid, avoidan~ and schizoid
personality disorder; and ail psychiatric diagnoses. Evidence for linkage to chromosome 6
was maximal using intennediate phenotypic definition and decreased when this definition
was either narrowed or broadened.
Specifie Associated Traits and Soecifie Components of the Diagnostic Phenotype
Specifie traits that are associated with complex disorders, as weil as specifie
symptoms, are potentially useful in mapping ofgenetic loci with specifie etfects. This
strategy May be particularly important for disorders that are most complex, i.e. behavioral
disorders. An example ofthe associated trait May he the decrease in normal inhibition of
the P50 auditory evoked response to the second ofpaired stimuli, which is associated
with attention disturbances in sehizophrenia, and oceurs also among non-schizophrenie
relatives in a distribution consistent with inherited vulnerability ta the illness (Freedman
14

et al. 1997). These authors reported linkage ofthis neurophysiological phenotype to
chromosome 15 at the site ofthe a7-nicotinic receptor gene.
Analysis ofsPeCific theoretically derived components ofthe diagnostic phenotype
is the current approach ofchoice for genetic analysis ofdyslexia or specific reading
disability (Fisher et al. 1999; Gayan et al. 1999; Grigorenko et al. 1997). Reading
Performance, the principal impairment in dyslexia, can he decomPOsed into several
component processes including word recognition, orthographic coding, phonological
decodin& and phonological awareness (Gayan et al. 1999). Severallinkage studies of the
chromosome 6p region found evidence ofvarYing strength for sPecifie phenotYPlc
components; strongest evidence was found for phonological and orthographie skills. and
weaker evidence was obtained for word recognition or single word reading (Fisher et al.
1999; Gayan et al. 1999; Grigorenko et al. 1997). Phonological and orthographie
processing are individually heritable, with behavioral genetic evidence for bath eommon
and independent genetic factors (Oison et al. 1994). Above noted linkage evidencc
suggests that common genetic factors rnight include a locus on chromosomc 6p
Ultimately, genetic analysis might identify genes with comPOnent-specifie efTect.
although such a conclusion requires elimination ofmethodological explanatlons. sueh as
differences in accuracy ofassessment ofdifferent phenotypes, or marker informat1\'cness
(pennington, 1997).
Multivariate Phenotype Definitions
Novel phenotype definitions for genetic mapping studies can he obtained using
some ofnumerous formai multivariate statistical methods, i.e. factor analysis, principal
IS
component analysis, etc., to combine information trom multiple variables in a composite
phenotype. This cm he advantageous because it uses information from multiple data
items typically collected in studies ofpoorly defined complex phenotypes (McCIeam,
1993), and because it circumvents prohibitively expensive corrections for multiple
comparisons with univariate analyses ofManY variables (Ott and Rabinowitz, 1998).
Common criteria for a priori selection ofthe useful multivariate phenotype are increased
heritability (Grove, 1994; McClearn, 1993; Ott and Rabinowitz, 1999), or the best fit to a
major gene transmission (Goldin et al. 1980; Zlotnik et al. 1983), a1though these criteria
might not he optimal for mapping ofail loci (Allisson et al. 1998). An example for the
use ofa priori defined multivariate phenotype in linkage analysis ofa complex trait is a
genome scan ofa1coholism phenotype (Foroud et al. 1998), derived from the latent class
analysis (categorical analog offactor analysis) ofsymptoms ofa1coholism. Sorne
statistical methods combine information from multiple phenotypes in the course of
linkage analysis to improve power (reviewed in Allison et al. 1998).
1.3. SUMMARY
Increasing phenotypic information from the familial/genetic perspective is an
important approach to genetic dissection ofcomplex traits.
16

2. PHENOTYPE DEFINITION
IN SPECIFIC LANGUAGE IMPAIRMENT (SLI)
2.1. nIE DIAGNOSIS AND ETIOLOGY OF SLI
Diagnosis of SLI
Specific language impainnent (SLI) is a recognized disability characterized by
failure to develop language at an expected rate (Tager-Flusberg and Cooper, 1999).
Accordingly, the onset ofSLI is during the preschool years. The best estimate of
population prevalence for SLI is 7.4%, with 8% in boys and 6% in girls in the USA
(Tomblin et al. 1997). This disorder is also known as developmental aphasia (rarely used
Iately), developmental dysphasia, or developmentallanguage disorder (DLD), with the
DLD and SLI being the most popular terms in the UK and USA (Bishop et al. et al. 1992).
SLI is similar to other complex behavioral disorders in that there is no '~goldn standard for
diagnosis. The diagnosis in adults is particularly problematic (plante et al. 1996; Tomblin
et al. 1992), as is the case in other developmental childhood onset disorders (Smalley,
1997), because the impairment is generally less overt in adulthood. In addition, there is
no generally accepted test or structured interview to he used in arriving at a diagnosis of
SLI (Aram et al. 1993; Dunn et al. 1996; Plante, 1998).
The diagnosis of SLI is based on exclusionary and/or discrepancy criteria and is a
matter ofongoing debate (Tager-Flusberg and Cooper, 1999). Exclusionary criteria
commonly include mental retardation, peripheral hearing 1055 and neurological disorder,
17
although more subtle auditory, neurological, cognitive, and behavioral deficits remain
associated with the SU category (Bishop, 1992; Gauger et al. 1997; Goorhuis-Brouwer
& Wijnberg-Williams, 1996; Labey" Edwards, 1995; Lewis et al. 1993; Lubert, 1981;
Neils &~ 1986; Powell & Bishop, 1992; Plante et al. 1991; Plante, 1998; Redmond
and Rice, 1998; Tallai et al. 1991; Tomblin, 1989; Wright et al. 1997). Therefore"
notwithstanding the application ofthese exclusionary criteri~ the boundaries of the SLI
phenotype remain decidedly unclear, and uniform operational measures for these
exclusionary criteria are not established. With resPect to mental retardation" many studles
have accepted the nonverbal IQ criterion of 8S points or greater, using diverse
instruments, sorne ofwhich show different results when administered to the samc set of
subjects (Cole et al. 1994; Plante, 1998; Swisher et al. 1994). The cut-ofTvaluc of 85
points is debated on various grounds, including that it was originally proposcd not ~ a
nonverbal IQ criterion per se but to compensate for the expected low verbal IQ WhlCh
would otherwise result in a general IQ of 70 points or less, meeting the excluslona~
criterion ofmental retardation (Gopnik and Goad, 1997; Plante, 1998; Tager-Flusherg
and Cooper, 1999). For issues regarding the use ofIQ in discrepancy criteria. sc:e the next
paragraph. Because most studies with reported IQ values used a cut-otTof 85. therc IS
presently insufficient data to evaluate with any certainty the inf1uence~ or lack thc:rcof. of
nonverbal IQ below 8S in SLI (plante, 1998).
Discrepancy criteria are more controversial than exclusionary criteria (Aram et al.
1993; Dunn et al. 1996; Plante, 1998). The principal notion is that SLI can be diagnosed
in tenns ofa discrepancy between receptive and/or expressive language function and
sorne other cognitive fonction, i.e. discrepancy between language test score and mental or
18

chronological age. This rationale bas been adapted to a variety ofmeasures ofnonverbal
performance and language, with diverse operational criteria (plante, 1998). The major
issues regarding discrepancy criteria concem the psychometrie and statistical
shortcomings ofthose language tests which are presently use~ and the corresponding
paucity ofoperational definitions of language impairment (ASHA, 1989; Aram et al.
1993; Ounn et al. 1996; Plante, 1998). The rationale behind the concept ofcognitive
referencing often used in discrepancy diagnoses bas been questioned on various grounds.
These include weak conceptual rationale for the direct influence ofcognition, as
measured by IQ, on language skills, psychometrie issues regarding the significance of the
discrepancy, lack ofdifferences in treatment outcome stratified by IQ status, and
variation in cognitive ability, as measured by IQ scores, over lime (Casby, 1992; Cole et.
aL 1990; Francis et al. 1996; Krasowski and Plante, 1997). Discrepancy constructs can
show low sensitivity and Low specificity with respect to clinical diagnosis (Aram et al.
1992; Aram et al. 1993; Dunn et al. 1996).
In summary, the most widely used definition of SLI pertains, for the most part, to
overt exclusionary aspects, while the commonality with respect to the inclusion is largely
limited to the fact that subjects have received clinical treatment. Limitations of this
imprecision, and the need for additional multidisciplinary work on the fonnulation of
more precise SLI criteria, are recognized (Tager-Flusberg and Cooper, (999).
Etiology of SLI
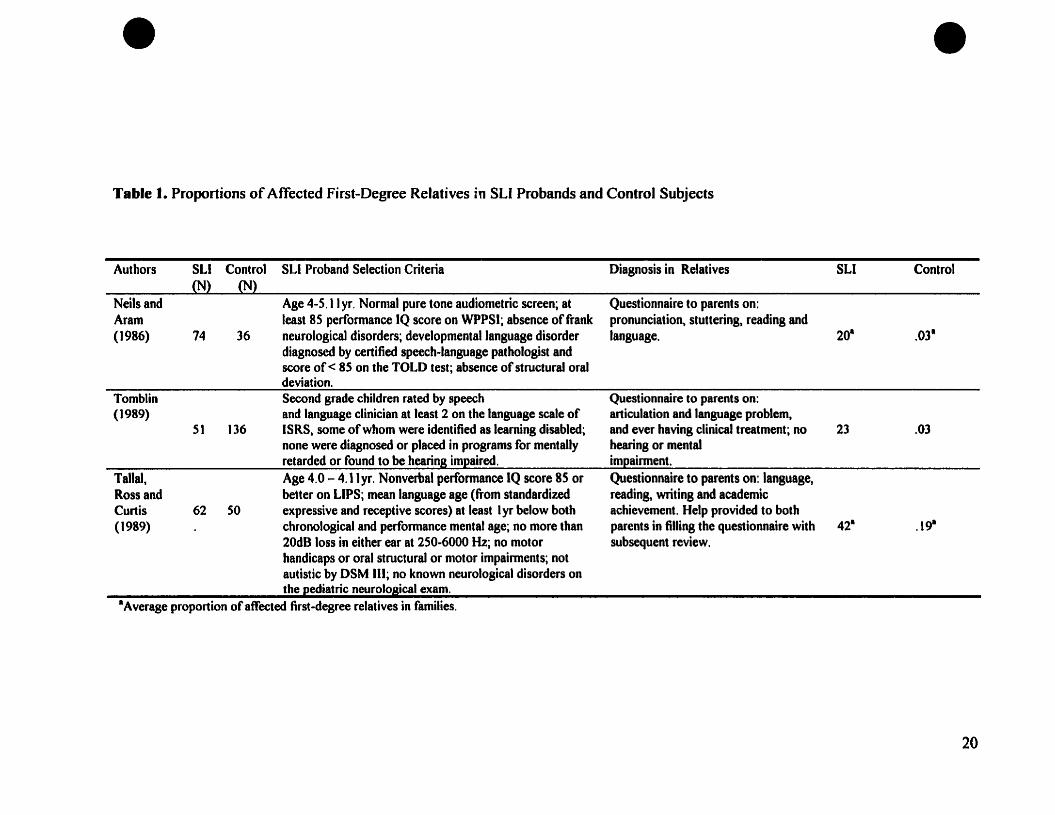
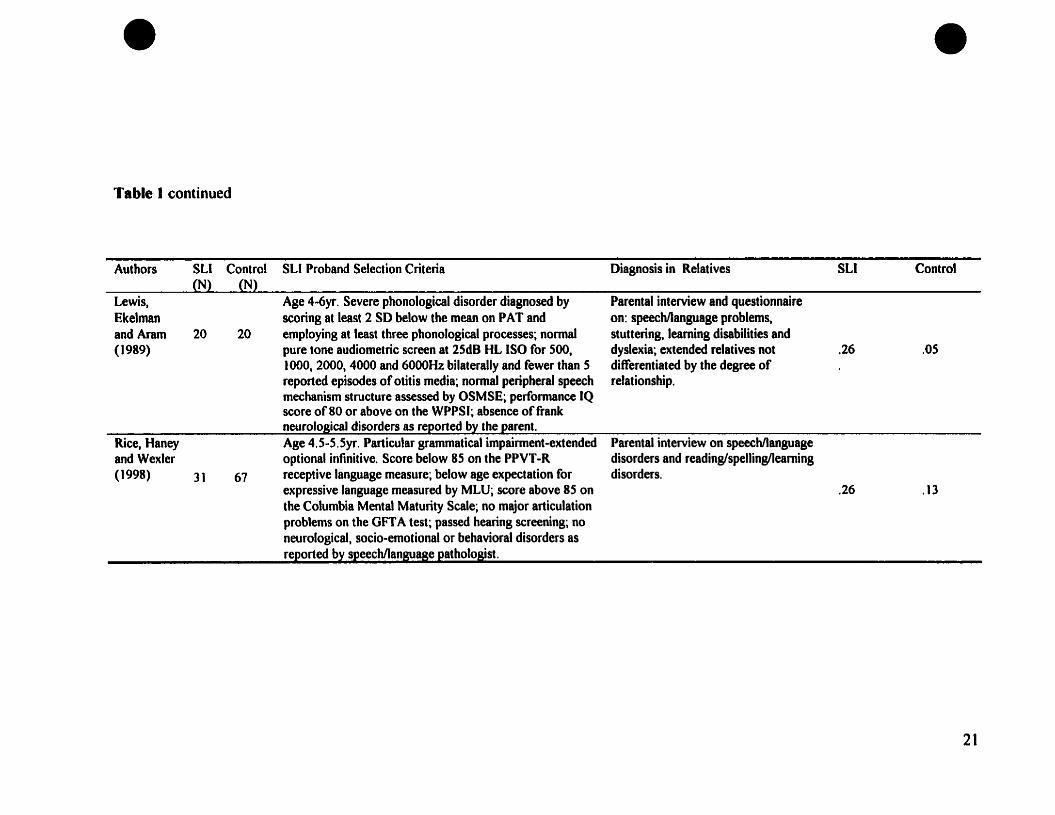
Family history studies comparing the risk to relatives ofSLI probands and
contrais, which utilize defined inclusion and exclusion criteria, are presented in Table 1.
19
e
Table 1. Proportions ofAffected First-Degree Relatives in SLI Probands and Control Subjects
e
Authors SLI Control SLI Proband Selection Criteria(N) (N)
Diagnosis in Relatives SLI Control
Neils and Age 4-5.1Iyr. Normal pure tone audiornetric sereen; at Questionnaire to parents on:Ararn least 85 performance IQ score on WPPSI; absence offrank pronunciation, stunering, reading and(1986) 74 36 neurological disorders; developrnentallanguage disorder language. 20' .03'
diagnosed by certified speech~language pathologist andscore of< 85 on the TOLD test; absence ofstructural oraldeviation.
Tornblin Second grade children rated by speech Questionnaire to parents on:(1989) and language clinician al least 2 on the language seale of articulation and language problern.
51 136 ISRS, sorne ofwhorn were identified as learning disabled; and ever having clinicat treatment; no 23 .03none were diagnosed or placed in programs for rnentally hearing or mentalretarded or round ta he hearing impaired. impainnent.
Tallal, Age 4.0 - 4.11yr. Nonverbal perfonnance IQ score 8S or Questionnaire to parents on: language.Ross and better on LIPS; mean language age (trom standardized reading, writing and academicCurtis 62 50 expressive and receptive seores) at least Iyr below both achievement. Help provided to both(1989) chronological and performance mental age; no more than parents in filling the questionnaire with 42' .19'
20dB loss in either ear at 250~6000 Hz; no motor subsequent review.handicaps or oral structural or motor impainnents; notautistic by DSM III; no known neurological disorders onthe pediatrie neurological exam.
•Average proportion ofaffected first-degree relatives in families.
20
e
Table 1 continued
e
Authors Stl Control Stl Proband Selection Criteria Diagnosis in Relatives Stl Control(N) (N)
Lewis, Age 4..(jyr. Severe phonological disorder diagnosed by Parental interview and questionnaireEkelman scoring at least 2 SD below the Mean on PAT and on: speech/langu8ge problems,and Aram 20 20 employing at least three phonological processes; nonnal stuttering, leaming disabilities and(1989) pure tone audiometric screen at 25dB HL ISO for 500, dyslexia; extended relatives not .26 .05
1000, 2000, 4000 and 6000Hz bilaterally and fewer than 5 differentiated by the degree ofreported episodes ofotitis media; normal peripheral speech relationship.mechanism structure assessed by OSMSE; performance IQscore of80 or above on the WPPSI; absence offrankneurological disorders as reported by the parent.
Rice, Haney Age 4.S-S.5yr. Particular grammatical impainnent-extended Parental interview on speech/languageand Wexler optional infinitive. Score below 85 on the PPVT-R disorders and readingfspellinglleaming(1998) 31 67 receptive language measure; below age expectation for disorders.
expressive language measured by MLU; score above 85 on .26 .13the Columbia Mental Maturity Scale; no major articulationproblems on the GFTA test; passed hearing screening; noneurological, socio-emolional or behavioral disorders asreported by speech!language pathologist.
21

The phenotype in relatives is often broadly defined, including learning disorders and
other communication disorders, ail ofwhich are ofte~ due to their striking associations
and the lack ofclear phenotype bounclaries, referred to as language..leaming disorders
(AACAP, 1998). Despite this problem and the concomitant methodological heterogeneity
that can explain some discrepant results, the principal overall conclusion ftom these
studies is that the proportion ofaffected first-degree relatives is consistently higher in SLI
probands than in control subjects.
However, familial aggregation does not constitute genetic etiology; as potential
environmental familial influences must also he considered. One way ofdoing this is to
conduet twin studies, on the rationale that MZ and DZ twins share similar environments,
but differ in genetie relatedness. A receot English language twin study reponed pair-wise
Ml concordance of0.54 and DZ concordance of0.30, for DSM..ill-R developmental
language or articulation disorder (Bishop et al. 1995). Proband-wise concordances were
0.70 (68/97) and 0.46 (16/35) respectively. In the cited study, parental report and medical
records yielded no evidence ofmental retardation, sensorineural hearing loss, structural
abnormality ofarticulators, serious visual impairment or a medical sYndrome. Therefore
this sample is comparable to other SLI samples. Another recent English language study
reported proband-wise concordance for test..based poor language status of 0.96 (82/85) in
Ml and 0.69 (24/35) in Dl twins (Tomblin & Buckwalter, 1998). These subjects passed
a hearing screening, and did not show mental retardation or other developmental and
behavioral disorders. Prior twin studies ofspeechllanguage measures were less
informative for the SLI category due to diagnostic limitations (Lewis and Thompson,
1992; reviewed in Bishop et al. 1995; Tomblin and Buckwalter, 1998).
22

•
Environmental influences, other than parental language input (Kuhl et al. 1997),
mayalso he important in SU Differences between SU children and controls were found
for parental tobacco smoking and breast feeding (Tomblin et al. 1997a).
Genetic Mapping Srumes and SL!. A segregation analysis ofSLI failed to
distinguish between a major gene and a multifaetorial transmission (Lewis et al. 1993),
in a sense confinning complex etiology that could have been hypothesized from the
general absence ofMendelian inheritance patterns in this poorly defined diagnostic
category. Tomblin and Zhang (1999) briefly noted that a major dominant locus model
was supported in the segregation anaIysis ofSLI in 58 families. A fully penetrant
autosomal dominant genetic locus in the 7q31 region was mapped to the phenotype of
severe speech/language impairment with speech and orofaciaI dyspraxia in a lΠfamily,
where sorne ofaffected individuals aIso had nonverbal IQ <85 but>70 points (Fisher et
aI. 1998; Vargha-Khadem et al. 1995). This family is clearly not representative ofmost
SLI families, because most families do not show simple Mendelian inheritance. However,
a recent report descnoes two different apparently balanced chromosome rearrangements
in the same region, one in the subject with specifie language impairment (and Iacking
reliable confirmation ofspeechllanguage impairment in extended relatives), and the other
in a different subject with autism (Warburton et al. 2000). The 7q31 region May therefore
harbor a gene, or genes, that are involved in bath autism and SLl, although the possibility
ofdifferent genes for different phenotypes cannot he excluded. Molecular genetic
mapping studies ofSLI are yet to be reported.
23
•
2.2. POTENTIAL FOR IMPROVEMENT
OF PHENOTYPIC DEFINITION IN SU
The clinical phenotype ofSLI is both poorly defined and at the high hierarchical
level ofdevelopmental organization, quite distant trom the level ofnucleotide sequences
in the genetic material. Consequently, different genes may he associated with ditIerent
components ofthe SLI phenotype. It is therefore important to define more homogenous,
precisely specified phenotypes within the overall SLI category in arder to facilitate
genetic and other research ofthis complex phenotype.
Many, but not ail, clinicians distinguish afIeeted individuals by clinicai SYndromes
more detailed than the basic expressive/receptive distinction in the diagnosis of SL!
(Rapin & Allen, 1983; Rapin, 1996). The DSM-IV defines expressive, mixed expressive
receptive, and phonologicallanguage disorder (APA, 1994). The ICD-I 0 defines
expressive language disorder and receptive language disorder. These categories, however,
are not widely used in research, but are only similar to the common definition ofSLI
described previously. Dysarthria denotes impaired speech articulation caused by motor
muscular deficit (Rapi~ 1996), and children diagnosed with this impairment are
generally not considered to be SLI children, although motor speech impairment does not
necessarily account for language deficits (Rice, 1999). The most common mixed
expressive/receptive language disorder in SLI is syntactic-phonological syndrome,
denoting poor phonology, syntax, and morphology (Rapin, 1996). Expressive language
disorders are: verbal dyspraxia, a severe expressive language problem with sparse output
and very poor phonology; and speech-programming deficit disorder, fluent with jargon
24
(Rapin, 1996). Disorders considered to he ofhigher arder processing nature are: lexical
deficit disorder, with ward finding and comprehension problems; and semantic-pragmatic
syndrome, with correct phonology and syntax accompanied by inappropriate use of
language, indicating difficulties with social aspects of language (Rapin, 1996). There May
he transition between these syndromes over time (Ramsden & Botting, 1999),
emphasizing the complex developmental character ofSU. In a single study, SU children
with expressive language deficit had a higher proportion ofaffected family members then
children with expressive and receptive language deficit (Lahey & Edwards, 1995).
In addition to clinical speech/language syndromes that May potentially be used to
increase homogeneity among affected individuals, there are more "molecular''l
phenotypes associated with SLI which may facilitate identification ofvulnerability genes
in this complex disorder. For example, auditory event related potentials, and phonological
processing deficits, are associated with both SLI and dyslexia (Fletcher et al. 1999;
Leppanen & Lyytinen, 1997; Riee, 1999). Distinct morphological strueture of language
related brain areas is associated with SLI (plante, 1996). Moreover, more specifie
linguistic components, or non-linguistic abnormalities present in SLI children, could in
principle he used to improve phenotype definition in SL!. Various hypotheses conceming
the "core" nature ofSLI were proposed on the basis of linguistic and non-Iinguistic facets
of the SLI phenotype. These include deficits in grammatical neural substrates, subtle and
multiple infonnation processing defieits, generalized intellectual defieit in conceptual
development or leaming strategies (Bishop, 1992; Clahsen, 1989; Curtîss and Tallai,
1991; Gopnik & Goa~ 1997; Leonard, 1989). However, recent views of SLI are more
oriented towards heterogenous etiology influenced by different factors that are neither
25

necessary nor suffieient for expression ofthe elinical SLI phenotype, rather than the
single '~core" explanation for the majority ofSLI cases (Bishop et al. 1999; Rice, 1999;
Tager-Flusberg and CooPer, 1999). For the purpose ofdetining more homogenous
phenotypes in SLI, the present work concems specifie components of impaired
grammatical competence, an~ in a separate study, the presence ofattention
defieitlhyperactivity behavioral problems in SU ehildren. These aspects ofSLI are
descnèed in more detail, below.
2.3. SPECIFIe COMPONENTS OF THE GRAMMATICAL
PHENOTYPE IN SLI
Although there is no consensus on partieular etiological hypotheses, numerous
studies coDSistently demonstrate that impainnent in the domain ofgrammatical
morphology represents a predominant aspect oflinguistie Performance in SLI ehildren
(Gopnik, 1999; Leonard et al. 1999; Oetting & Horohov, 1997; Rice, 1999; Rice &
Oetting, 1993; Riee & Wexler, 1996; Rose & Doyle, 1999). Until recently, there was no
substantial evidenee for a specifie grammatical marker that would accurately diseriminate
SL! children from controls (reviewed in Rice, 1999), leading to a proposition that SLI
essentially represents a developmental delay that falls within a broad range oftypical
language development in children (Leonard, 1987). More recent studies, however, have
identified finite verb morphology, in particular Tense marking, as a promising clinical
Marker in English speaking SLI children (Bedore & Leonard, 1998; Leonard et al. 1999;
26
Oetting & Horohov, 1997; Rice, 1999; Rice et al. 1995; Rice et al. 1998; Rice & Wexler,
1996).
Finiteness is a property marked on verbs, which can appear in finite and infinite
forms: finite forms are those marked for Tense and grammatical agreement (Rice, 1999).
In a study ofchildren receiving preschool intervention services, and meeting aIl inclusion
and exclusion criteria for SLI, Rice & Wexler (1996) found two types ofevidence which
argue in favor ofverb Tense marking (morphemes -s third person singular, -ed regular
past, BE, and 00 ) as a specific clinical marker for SLI children. Fi~ 37 ofthese 5yr old
SLI children showed low levels ofaccuraey for morphemes that mark Tense in relation to
45 age matched controls, and aIso in relation to 40 of3yr old controls matched for MLU
(the Mean length ofutterance). The latter control group was thereçore at an equivalent
language level as the SLI children on MLU (Riee & Wexler, 1996). This finding argues
against the view ofSLI as a developmentallanguage delay without qualitative
grammatical distinctions. Second, SLI children were impaired specifically on a set of
grammatical morphemes defined by the linguistic fonction ofTense, but not for
grammatical morphemes unrelated to Tense, including regular is plurals, the prepositions
in and on, and the progressive -ing on the verbs (Riee & Wexler, 1996). This result
suggests that the impairment ofgrammatical Tense marking function May he a relatively
specifie distinguishing factor contributing to the overall SLI phenotype. Auditory
processing-deficit was inconsistent with specific errors restricted to Tense marking in
these SLI children. Children with the Williams syndrome display a nearly adult level of
Tense marking, although their intellectual competencies are far below SLI children.
27
(Ricet 1999). These observations raise the possibility that specifie neural substrates
related to grammatical aptitude May contribute to the impainnent in Tense marking.
The status ofverb Tense marking as a clinicaI Marker was also examined by
Bedore & Leonard (1998}t in a discriminant function analysis ofSU children, ages 3.7yr
- 5.9Yft diagnosed sirnilarly with respect to inclusion and exclusion criteria. Linguistic
constructs including a finite verb morpheme compositet a noun morpheme composite,
and the Mean length ofutterance in morphemes, were used to discriminate 19 LI children
from 19 age-matched controls in a first study, and 6 additional SLI children and 6 novel
controls in a second experiment (Bedore & Leonar<l 1998). The finite verb morpheme
composite (regular past tense intlectionst regular third persan singular present inflections,
and copula and auxiliary be forms) showed the best combination ofsensitivity (>84%)
and specificity (100%), which was not substantially improved by the addition ofother
two variables. Tempered by the small number ofsubjects, these results indicated that
verb Tense marking may be an optimal clinical Marker among different components of
impaired language which were examined.
While the verb Tense marking is best documented, it may not he the ooly relevant
grammatical marker phenotype in SLI (Rice & WexIer, 1996). Overall grammatical
competence is a complex phenotype that comprises a number oftheoretically different
aspects of language comprehension and production (Gopni~ 1999). Accordingly, it is
recognized that global characterizations of language aptitude May not be as
neurologically and genetically illuminating as are carefully and precisely specified
distinctions, which may in tum provide the framework for relating linguistics to a more
molecular level of investigation (Rice, 1999). In the previously noted twin study ofSLI
28

children, Bishop and coworkers (1995) reported high heritability estimates for Word
Finding, for a Test for Reception ofGrammar, and for the Comprehension test (ail
estimates -1). Substantially lower heritability (-0.56) was reported for Repeating
Sentences, suggesting that sorne specifie aspects of linguistie competence May be under
greater genetic control than other aspects.
The above considerations suggest that the analysis ofmore specifie aspects of
linguistic competence can he a promising strategy for identification ofmore homogenous
phenotypes in SLI, which might eventually facilitate both the multifaceted understanding
ofthe complex end-point behavioral phenotype and the identification ofpotcnllal gcncuc
vulnerability loci. With this rationale, the present manuscript examines sibling
resemblance for specifie theoretically derived components ofgrammatical com~tcnce ln
families of SLI children, including competence in verb Tense marking, among olhcrs
The manuscript, submitted to the Journal ofNeuro1inguistics, is entitled ··Sibhng
Resemblance for Specifie Components ofLinguistics Competence in Famihes of
Speech/Language Impaired Children".
2.4. THE SLI PHENOTYPE
AND ATTENTION DEFICITIHYPERACTIVITY
Attention deficitlhyperactivity disorder (ADHD) is a common childhood onset
disorder with a population prevalence of2-12% (reviewed in Greenhill, 1998). and
substantial evidence of familial and genetic etiology (family, m'in and molecular genetic
studies reviewed in Rutter et al. 1999). Tbere are a variety ofoperational procedures for
29
arriving at diagnosis ofADHD (Conners~ 1998; Greenhill, 1989). DSM...IV (APA, 1994)
provides two sets ofoperational criteria, corresponding to inattention and
hyperaetivity/impulsivity~ to define a combined subtype~ predominantly inattentive
subtype~ and a subthreshold category. Comorbidity ofADHD with other psychiatric
disorders is notable~ including oppositional defiant disorder or conduct disorder~
depressive disorders~ anxiety~ bipolar disorder, and leaming disorders, with reading,
spelling, and arithmetic being studied most often in the latter category (reviewed in:
Angold et ai. 1999; Pliszka, 1998).
Attention DeficitIHyperactivity in SpeechlLanguage Impaired Children
The comorbidity between speechlIanguage disorders~ not defmed with respect to
SLI criteria, and attention deficit/hyperactivity disorder bas been documented in several
studies. For example~ Beitcbman and coworkers (1986) found that 30.4% of 135 children
in a population-based sample with speechllanguage disorders and 4.5% of 137 control
children had Attention Deficit Disorder by OSM-ID criteria. In the same study, 15.7% of
134 speech/language impaired children and 9.4% of 138 controls had a hyperactivity
score>2SD above the nonn on the Conners Teachers Questionnaire. Cantwell and Baker
(1987) studied clinically identified children with a) "pure~' speech disorder(voice,
articulation, fluency disorder), b) speech and language (expressive~ receptive or
processing) disorder, and c) language (expressive, receptive, or processing) disorder. The
proportions ofchildren in each of these three groups who aIso met criteria for attention
deficit disorder (based on interviews and behavior rating scales) were 10%, 23%~ and
33%, respectively, suggesting that attention deficit was not strongly associated with
30

Upure,t speech disorders as defined in the study. Conversely, language disorders are
among the major comorbid conditions in attention deficit disorder (Cantwell, 1996;
Cohen et al. 1993; Love et al. 1988). Love and coworkers (1988) found that two-thirds of
clinically identified children with DSM-m attention deficit disorder aIso had a language
disorder. Cohen and coworkers (1993) reported that bath children with previously
identified and unsuspected language impairments had symptoms associated with ADHD.
Attention DeficitIHyperactivity in SLI Children
Aram, Ekelman and Nation (1984) reported a longitudinal study ofEnglish
speaking language impaired children who passed a pure tone audiometric test, and did not
have neurological or craniofaciai abnormalities. Among 20 subjects, 15 had nonverbal IQ
>85 points. The 14 clinically diagnosed speecbllanguage imPaired boys, ages 13-16yr,
were rated by parents as more hyperactive than expected for a nonnative control group
(P<O.OI).
Goorhuis-Brower and Wijnberg-Williams (1996) reported that Il of 14 Dutch
speaking children, ages 6.7-9.7yr, showed attention problems based on questionnaires for
parents and teachers. These children were clinically diagnosed with SLI 4 years earlier,
having no hearing loss, mental retardation, neurological disorder, general medical
problem, or any psychiatrie disorder including AOfID. It is not clear, however, that these
children did not have any subclinical symptoms associated with attention
deficitlhyperactivity at the time of SLI diagnosis.
Redmond and Rice (1998) studied 17 English-sPeaking SLI children (11 boys and
6 girls) and 20 age-matched controls at ages of -6yr and -7yr. SLI children were
31

clinically diagnosed, had normal intellectual fonction, normal hearing, and no major
articulation problems. The Achenbach Child Behavior Checklist and the Teacher Report
Form were used to obtain ratings fram parents and teachers. At both ages, only the
teachers reported more attention problems in SLI children. At first rating, the T-scores
and SO (in brackets) for attention were 58(9) in SLI children versus 53(4) in controls~ as
rated by teaehers. At the second rating a year later, these values were 57(7) versus 53(4).
Taken together, evidence noted so far suggests that the association of
speechllanguage disorders with attention deficitlhyperactivity May persist when the: SLI
criteria are employed.
Attention DeficitIHyperactivity in SL! Cbildren and Familial Aggregation
Ofparticular further interest is the study ofTaIlal and coworkers (199 J ). who
rePOrted that SLI probands who had at least one affected parent were more oftcn ralcd as
having attention/hyperactivity behavioral problems. The SLI probands were dlagnosed
using the discrepancy ofat least 1yr between language age computed from standardazed
scores, and performance mental age and chronological age. They also had performance
IQ ~ 85, normal hearing acuity, no motor imPairment of articulators~English language
background, and were not autistic by OSM-ill-R criteria. The SLI probands wcre deemed
ta be family history positive ifat least one parent reported having had one or more of
following problems: a) below average or impaired school achievement in reading or
writing, b) placement in a remedial class for reading or writing, c) kept back a grade or
having failed a class, d) below average or impaired language development as a child, or
d) speech therapy. Among 23 SLI probands, 16 were family history positive and 7 were
32
family history negative. Scales developed trom factor analysis ofAchenbach parent and
teacher ratings showed that family history positive probands were more often rated as
"hyperactive" by parents (p<O.OO1) and more often rated as "inattentive" by teachers
(p<O.OS). Except from Donverbal auditory processing and attention, family history did Dot
differentiate between other profiles, including degree or Pattern oflanguage deticit,
general intelligence, academic performance measures, visual-spatial skills, speech-oral
motor abilities, and auditory competence as per audiological exam and brain stem evoked
auditory responses.
Notwithstanding the small sample size and ambiguous phenotypes inherent in the
current SL! diagnosis and the family history method, this study suggests the hypothesis
that anention/hyperactivity behavioral problems may provide a basis for delineating a
more familial phenotype within the SLI category. Based on these results, it can be
hypothesized that the risk to relatives ofSLI children with ADHD symptoms or diagnosis
May be higher than the risk to relatives of SLI children without these behavioral
problems. The Iogical next step is therefore ta compare these risks; the evidence in
support of this hypothesis would provide impetus for further familiaVgenetic studies of
the relationship between SLI an ADHD. This analysis is perfonned in the manuscript
entitled "'Attention DeficitIHyperactivity in SLI Children Increases Risk of
SpeechlLanguage Disorders in First-Degree Relatives", submitted ta the Journal of
Communication Disorders .
2.5. SUMMARY
Specific Language Impairment (SU) is a complex bebavioral disorder tbat is
gaining attention as a candidate for genetic mapping studies. The power ofthese studies
to identify correct linkage localization, and thence to detect specific genes, can be
enhanced by the use ofprecisely defined phenotypes that can alleviate ambiguities ofthe
clinical SLI diagnosis. The goal ofpresent studies is to explore phenotypes that May show
increased familial aggregation, using a) theoretically derived specific components of
grammatical competence; or, b) presence ofattention deticitihyperactivity behavioral
problems in SLI children. More familial phenotypes May eventually prove useful for
genetic mapping studies.
34

2(8). SIBLING RESEMBLANCE FOR SPECIFIC COMPONENTS OF
LlNGUISTIC COMPETENCE IN FAMILlES OF SPEECRILANGUAGE
IMPAIRED CIIILDREN
The present chapter consists ofthe following manuscript in submissio~ entitled
as above.
35
Sibling Resemblance for Specifie Components ofLinguistie Competence in Families of
Speech/Language Impaired Children
ILUA KOVAC1, MYRNA GOPNIK3
•ROBERTA M. PALMOUR1.2,·
Departments ofBiologyl, Human Geneties2, Psychiatrr, and Linguisties3 (ret.), McGill
University, Montreal, Quebec, Canada
1.2·Department ofPsychiatry, McGill University
Allan Memorial Institute, Research and Training Building Room 307
1033 Pine Avenue West, H3A lAt, Montreal, Quebec::, CANADA
Tel. (514) 398-7303; Fax (514) 3984370
E-mail: [email protected]
3Department ofLinguistics, McGill University
1085 Dr Penfield Avenue IDA lA7, Montreal, Quebec, CANADA
36

Abstraet
We examioed performance 00 specific linguistic tests in 23 English and French
speaking familles, recruited from clinical and other sources, ofchildren who met
following criteria for specifie language impairment (SLI): clinically diagnosed language
impairment without peripheral hearing 105s, mental retardation (nonverbal IQ~70),
neurological disorder, schizopbrenia or autisme Subjects, at least 9 years old, completed a
battery ofFrench or English language tests, including Derivational Morphology, Verb
Tense Morphology, Grammaticality Judgement, Syntaetic Comprehension., and Pointing.
Listening Comprehension and WUG pluralization test were analyzed ooly in the English
group. The Verb Tense Morphology(Real Words) and Verb Tense Morphology (Non-real
Words), respectively, showed non-parametric sibling correlations of0.39 and 0.35
(p<O.OS, 2-tailed) in 38 pairs (mixed gender) from 10 French test Pedigrees. In the
English group, Derivational Morphology showed significant 0.52 correlation in 41 sibling
pairs frorn the densely affected FE pedigree. After controlling for age, sibling correlation
for Verb Tense Morphology (Real Words) remained significant, and Derivational
Morphology correlation in the FE pedigree was borderline (p=O.OS). Impaired
grammatical morphology is a predominant aspect of SLI., and the present study, which
requires independent replicatio~ suggests that Verb Tense Morphology and Derivational
Morphology warrant particular attention in future familial and genetic studies.
Keywords: Verb tense, Familial resemblance, Specifie phenotype
37
1. Introduction
Children diagnosed with speechllanguage impairment and lacking peripheral
hearing loss, mental retardation, or neurological disorder are commonly referred to as
having specifie language impainnent (SLI), or developmentallanguage disorder, although
more subtle auditory, neurological, cognitive and behavioral deficits remain associated
with the SLI category (Lubert, 1981; Neils &, Aram, 1986; Tomblin, 1989; Tallai et al.
1991; Bishop, 1992; Powell &, Bishop, 1992; Lewis et al. 1993; Labey &, Edwards, 1995;
Goorhuis-Brouwer &, Wijnberg-Williams, 1996; Tomblin et al. 1997a; Wright et al. 1997;
Redmond &, Riee, 1998; Plante, 1998). The SLI is a complex disorder with documented
familial aggregation, influeneed by bath genetic and environmental factors (Lewis et al.
1993; Labey &, Edwards, 1995; Bishop, North, &, Donlan, 1995; Tomblin et al. 1997b;
Riee, Haney, &, Wexler 1998). Recently, a fully penetrant autosomal dominant genetic
locus was mapped in a single pedigree characterized with severe speeeManguage
impainnent accompanied by orofacial dyspraxia in ail atTected individuals (Vargha
Khadem et al. 1995; Fisher et al. 1998). However, SLI families typically do not show
simple Mendelian inheritance (Lewis et al. 1993).
Different factors, including output mechanisms, information processing,
grammatical mechanisms, and generally impaired conceptual developmen~ were
proposed as separate "core"" explanations of SLI (reviews in Bishop, 1992; Gopnik &,
Goad, 1997). However, because the phenotype ofgrammatical behavior is at a highly
complex hierarchicallevel ofdevelopmental organization, is likely to he influenced by
Many factors. It is increasingly recognized that there May he multiple synergistic fac~ors
38

which are neither necessary nor sufficient for expression ofthe phenotype ofSLI, i.e.
subde auditory processing deficits, or a nonverbal IQ between 70 and 85 points (Gopnik
&. Goad, 1997; Plante, 1998; Bishop et al. 1999; Tager.Flusberg &. Cooper, 1999; Rice,
1999). Accordingly, the analysis ofempirical data collected with test batteries designed
to probe theoretically derived linguistic components ofthe SLI phenotype could lead to
the development ofmore specific phenotypes. Ifthese phenotypes were etiologically
more homogenous they might increase the power to detect genes with more specifie
effects (Lander &. Sehor~ 1994). An example ofthis strategy is genetie research in
dyslexia (specifie reading disability), another complex disorder with ratber similar
exclusionary aspects ofphenotype definition (Fisher et al. 1999; Gayan et al. 1999;
Grigorenko et al. 1997; Penningto~ 1997). Component skills, such as phonological
decoding and orthographie coding, generally showed stronger evidence for linkage to
chromosome 6 than word recognition or reading performance, which are higher order
processes influenced by other factors in addition to these component skiUs (Fisher et al
1999).
The multidisciplinary Genetie Language Impairment Project (GLIP) at the McGill
University (Myrna Gopnik, PI) included a battery oftests designed to evaluate specifie
theoretically derived components of linguistic competence in families with SLI children
(Gopnik, 1999; Rose & Doyle, 1999). These linguistic tests were adapted for English,
French., Greek, and Japanese, so that overall results could he comparable across
languages. The purpose ofthe present study is to examine sibling resemblance for
specifie components of linguistic competence assessed by the English and French GLIP
39
test batteries. This examination may indicate specifie phenotypes of interest for further
familial and genetic studies.
2. Subjects and Metbods
2.1. Subjects
The present study included 23 families selected for direct language testing,
accordingto the criteria Iisted below, within the McGill University Genetie Language
Impairment Project (GLIP, Myrna Gopnik, PI). Ofthese 23 famifies, 14 families were
from the pool of 156 families initially identified through parental response to an
announcement in the newsletter ofthe Association ofQuebec Dysphasie Children
(AQEA). The AQEA comprises families ofchildren elinically diagnosed with
speechllanguage disorder. Ofthe remaining Il families, 9 were identified through
elinician's (from the Montreal Children's Hospital, or the Children's Hospital ofEastern
Ontario in Ottaw~ or the Vanguard Sehool in Montreal) referral of9 cases meeting the
selection criteria listed below, while 2 families were self-referred.
As reported previously (Gopni~ 1999; Rose & Doyle, 1999) information from
clinicians and Medical records was used to identify probands based on following criteria:
a) confirmed diagnosis of language impainnent by a speech/language pathologist, b)
normal hearing (25db), c) performance IQ of 70 and over, d) no presence offrank
neurological signs, e) no evidence ofautism or schizophrenia by the DSM m-R criteria.
40
Probands did not bave other serious Medical conditions tbat might have caused
speecb/language impairment.
At least one impaired first-degree relative as judged by clinical diagnosis7present
or past family history report ofspeechllanguage problem, speech therapy7 readinglwriting
problem, or an ongoing educational/school problem was generally required for enrolment
ofthe family for language testing. One family with 6 children and no first-degree
relatives of the SLI proband known to he impaired was a1so enrolled.
Healthy controls with no known family history ofspeech/language impairment
were also recruited for both English (N =22) and French (N = 8) language testing
(Gopnik, 1999; Rose & Doyle71999).
2.2. Methods
2.2./. Direct Linguistic Testing
Comprehensive linguistic accounts ofthe testing procedure and perfonnance of
these English and French speakïng subjects are reported elsewhere (Gopni~ 1999; Rose
& Doyle, 1999, and references therein). Here we provide a briefsummary. The GLIP
Linguistic Profile Test Battery was adapted from the Bilingual Aphasia Test (paradis,
1987) for the English and French subjeets examined in this report, and for the Greek and
Japanese subjects not examined here. The test battery was constructed to address a
number ofhypotheses about the nature and cause ofSLI (Gopnik, 1999). Sorne ofthe
linguistic tasks required an understanding ofabstract concepts such as grammaticality.
Subjects under the age of9 yr. were not always able to complete aU sections ofthe test
41
•
battery (Gopnik, 1999; Rose &, Doyle, 1999). Therefore, thase subjects whose test scores
are analyzed in this paper were at least 9 years old at the time oftesting. Within both the
English and French Linguistic Profile Battery, some families were identified through the
AQEA and some were identified in other ways. In the English test group, 55 of71 tested
subjects were included in the analysis, and in the French test group 67 of79 tested
subjects were included Excluded were subjects younger than 9yr at testing, 1 adoptive
father from the extended family in the English test group, and 1second-degree relative in
the French test group because of unusual response to testing, for example always giving
an affirmative answer to 29 Grammaticality Judgement questions (data trom Rose &,
Doyle, 1999). The analysis included 12 probands from Il ofthe 14 families identified
through the AQE~ and 4 probands from the 9 other families noted in the subjects
section. Many families used both French and English language in communication as
commonly found in Quebec, and in some families test languages ditTered among family
members, while 4 subjects, including 2 probands, participated in both test languages.
Further details conceming the structure ofthis analyzed sample by family, test language
and degree of relationship among tested family members are provided in the Appendix.
Table 1 briefly summarizes the tests provided for this report, including the
relevant language, areas ofcompetence that were targeted, and the test stratification into
sub-tests with respect ta types of input, as described more extensively elsewhere (Gopnik
1999; Rose & Doyle, 1999). Each test was explained to subjects before the aetual scored
trial began; subjects were also given trial examples that were not scored.
Grammaticality Judgment. Subjects were asked ta judge whether a sentence read
by the examiner was a correct sentence, and to verbally correct the sentence ifnecessary.
42

•
Table 1
Language Tests
Test (Language) Area ofCompetenœ Sub-tests
Derivational Morphology producing derivation ofword
(English and French) morphology in a sentence no sub-tests
Verb Tense Morphology producing change ofverb tense in a Real Word Sentences
(English and French) sentence Non-word Sentences
Grammatical Sentences
Grammaticality Judgement and recognition ofgrammatica1ly correct Ungrammatical Sentences
Correction sentences and producing correction of Correct Jud~ement
(English and French) ungrarnmatical sentences (English onl)·,
Correct Correction
{English onl~ •
Syntactïc Comprehension comprehension ofsyntaetically CanonicaJ Senlences
(English and French) complex sentences Non-canorncal Sentences
WUGTest Real Ward Sentences
(English ooly) producing noun pluralization Non-word ScnlcncO
Painting comprehension ofplural and singular
(English and French) no sub-tests
Listening Comprehension comprehension of temporal sequence
(English ooly) eventsy causal relations no sub-lests
43
Both ofthese responses were required to he correct for a positive score with
ungrammatical sentences. An English language example ofa grammatically incorrect
sentence is "Yesterday 1walk home"" and the French language example is "Le garçon
sourit la fille." There were 32 sentences in the English test and 30 sentences in the French
test, balfofwhich in either language were grammatically incorrect. In the French
language" 1 ungrammatical sentence was removed from score calculations by GLIP
testers because it was a problem for most speakers (data from Rose & Doyle" 1999). The
test score was the number ofcorrect responses. In the English language" scores for
Correct Judgement out ofaU 32 sentences and Correct Correction out of 16
ungrammatical sentences were also obtained
Derivationa/ Morph%gy. Subjects were asked to verbally complete taped
sentences using a ditTerent morphological forro ofthe word from the preceding complete
sentence. The English language example is "That makes a lot ofnoise. It is very __
(noisy). The French language example is "Mes amis font de la magie. Ce sont des __
(magiciens). There were 10 items in the English language and 12 items in the French
language. The test score was the number ofcorrect responses.
Verb Tense Morph%gy. Subjects were asked ta verbally complete taped
sentences by changing the tense of the verb. The English language example is '~very day
he plays bail. Yesterday he (played bail). The French language example is "Le
bébé a pleuré toute la nuit. Encore maintenant il (pleure). In both languages some
sentences contained non-words and subjects were asked to complete the sentence as if
those were real words" as in the English language example "Yesterday he [dizd] the
cookies. Right DOW he (is dizing).n The rationale for this stratification here, and in
44

the WUG test (see below)~ was that Real Words cao he memorized over time as a whole
and correctIy produced in the appropriate form without implicit knowledge of
grammatical rules; hence Non-real Words might reveal the lack ofgrammatical
competence more successfully (Gopnik, 1999; Rose & Doyle~ 1999). There were 12
sentences with the existing verbs and Il sentences with non-existing verbs in the English
language. In the French language there were 12 ofeach such sentences respectively. The
test score was the number ofcorrect responses.
Syntactic Comprehension. Subjects were asked to touch or say the number ofa
picture depicting the meaning ofa sentence read by the examiner. There were 8 canonical
and 14 non-canonical sentences in the English language, and 9 and 16 ofthese sentences
respectively in the French language. The test score was the number ofcorrect responses.
The English language example of the canonical sentence is "The girl washes the woman",
and the example of non-canonical sentence is "ft's the girl who the woman washes." The
French example of non-canonical sentence is "C'est la fille que le garçon pousse. (It is
the girl whom the boy pushes)".
The WUG Test. This test was administered only in the English group. Subjects
were shown a picture and told the name ofan object in the picture, repeated once, i.e.
"This is a chair. Chair." The next picture showed two ofthese objects and subjects were
asked to name them in plural~ i.e. "These are chairs". Some non-existing words were also
used and subjects were asked to respond as if those were rcal words~ i.e. "This is a wug.
Wug." "These are wugs." There were 10 items with existing words and 10 items with
non-existing words. The test score was the number ofcorrect responses.
45
•
Listening Comprehension. In this test from the English group, subjects were read
a short story and were then asked five questions about what bappened in the story. The
questions were: (1) Where were the boy and bis sister? (2) Wbat day ofthe week was it?
(3) What did the boy buy her? (4) Why did the boy buy an ice cream for bis sister? (5)
Why dido't the girl eat the ice cream? The test score was the nomber ofcorrect responses.
Pointing. In this test, subjects were asked to point to the pieture representing a
ward spoken by the examiner, either in singular or plural form. There were 24 items in
.the English and 16 items in the French language. The test score was the number ofconeet
responses.
2.2.2. S/atistica/ Methods
Properties of the scale measured by the administered language tests are not weil
understood. Therefore, the primary methods ofdata analysis were robust non-parametric
methods that require ordinal rather than interval scale ofmeasurement. The Wilcoxon
Signed Rank test for paired samples (Snedecor, 1956) was used to compare language test
scores in cases and controls, individually matched for age and sex without reference to
test scores. Due to the small number ofcontrols, particularly in the French b'fouP. some
reportedly normal subjects from families with SLI children were used as age- and sex-
matched controls. The potential drawback ofthis approach is that sorne of thc:se subJects
May have subtle language difficulties that could emerge at testing, making for a more
conservative comparison. Spearman's rho test was used to examine correlations between
test scores within the English and French test battery. Test score relationships with age
and gender were examined excluding probands, who were young and predominantly
46
males, and would tberefore bias these relationships. Speannan's rho test was used to
examine the correlations oftest scores with age, and Mann-Whitney U test was used to
compare age and test scores by gender.
2.2.3. Sib/ing Resemb/ance
Sibling resemblance for language test scores was evaluated using the Speannan's
rho correlation. A nonparametric method was chosen because it does not depend on the
assumption of interval seale ofmeasurement, and therefore allows for robust
interpretation ofresults. Moreover, we used ail possible sibling pairs in order to
maximize the utility ofthis data set through increased sample size, while acknowledging
that obtained correlations may he overestimated in comparison to statistically correct use
ofonly independent sibling pairs (Neale & Kendler, 1995).
There were 47 and 43 possible sibling pairs in the English and the French group
respectively, not counting 1 twin pair (purportedly MZ) in the French group. In the
English group, 41 of47 pairs were from the single extended FE pedigree known to he
densely affected and hence not representative ofSLI famifies. Because the remaining 6
sibling pairs contribute little information, and on the other hand might potentially
confound the interpretation of results, only the 41 sibling pairs ftom the FE pedigree were
analyzed in the English group. Moreover, 5 other sibling pairs ftom the FE pedigree that
were tested in the French language were excluded ftom the French group, for the reasons
noted above. Therefore, a total of41 and 38 sibling pairs were analyzed, originating
respectively ftom a single FE pedigree tested in English and 10 pedigrees tested in French
test.
47

•
The power for detecting a correlation with an etfect size of0.30 or 0.40,
conventionally referred to as medi~ was -50% and -7()oA. respectively, calculated for
the significance level of0.05 in 2-tailed tests with 41 sibling pairs in the English group
(Welkowîtz et al. 1991). For the 38 sibling pairs in the French group, the corresponding
power values were -45% and -7()oA.. Because the available sample sizes for other types of
relative pairs provided little statistical power, only sibling pairs are included in the
present study. In order to examine whether sibling correlation for age at testing might
potentially account for significant Don-parametric sibling correlations, in those instances
partial correlations using normalized Z scores (necessarily assuming interval scale of
measurement) were also computed
Although this report includes multiple statistical tests, most of the tested variables
are partly correlated, reducing the rate of inflation offalse positive results. As the
intention ofthis study is to provide hypotheses for further confirmatory research, we
consider as significant ail comparisons at the 2-tailed 0.05 level and discuss them in view
of relevant literature.
3. Resulu
3.1. The Population
The age at testing of 14 probands (the oldest affected child, in the case offamilies
with multiple clinically diagnosed siblings) trom 14 AQEA families ranged from 6.16 to
22.1yr (mean 12.11, SO = 3.98). This calculation included only 1 of2 MZ twins in one
48

family, both ofwhich were otherwise taken as probands. The age at testing of7 probands
from the 7 clinically referred families ranged from 4.72 to 17.95yr (mean 8.51, SO =
4.88). Ages at testing of2 self-referred probands were 9.6 and 21.35yr. The male-female
ratios in these recruitment-based subgroups ofprobands were 13/1,6/1 and 2/0
respectively. None ofclinically diagnosed children bad a language disorder cbaracterized
by fluent communication with inappropriate use of language, also referred to as the
semantic-pragmatic syndrome (Rapin & Allen, 1983; Rapin, 1996). Many ofthe 3S
clinically diagnosed children had additional non-exclusionary anomalies, most ofwhich
were related to motor fonction (motor problems, axiallbody coordination, cerebral
dysfunction); also noted were a medicai record reference to attention deficit and/or
hyPeractivity (12 children), and a record ofcentral auditory processing deficits (3
children).
3.2. Case-Control Comparison ofLanguage Test Scores
Table 2 presents comparison of language test scores between SLI subjects and
controls individually matched for age and gender. Differences in particular tests or sub
tests (Table 2) were consistent with previous case-control comparisons in these subjects
(Gopnik, 1999; Rose & Royle, 1999), except for the Pointing task in the French group
that did not show significant difference trom controls in the previous study, which was
not matched for age and gender (Rose & Rayle, 1999). The tests that showed significant
difference between cases and controls (Table 2) were selected for further analysis; when
only 1 sub-test and the overall test showed significant result, then only the sub-test was
49

Table 2
Age and Sex Matched Case-Control& Comparison ofTest Scores
p (Englishl p <Frenchl
Derivational Morphology'
Verb Tense Morphology'
Verb TenseMorphology (Real Wordsf
Verb Tense Morphology (Non-real Words)'
Grammaticality Judgement'
Grammatica1ity Judgement (Grammatical Sentences)
Grammaticality ludgement (Ungrammatical Sentences)
Grammaticality Judgement (Correct Judgement)
GrammaticaIity Judgement (Correct Correction)'
Syntaetic Comprehension'
Syntactic Comprehension (Canonical Sentences)
Syntaetic Comprehension (Non-canonical Sentences)'
WUG Test (Real Words)
WUG Test (Non-real Wordsf
Pointing'C
Listening Comprehension
0.025 0.020
0.013 0.015
0.018 0.027
0.037 0.034
0.035 0.011
0.018 0.017
0.068 not scored
0.028 not scored
0.027 0.027
lb 0.180
0.018 0.027
0.043 not tested
0.066 not tested
0.042 not tested
0.157 0.026
0.48 not tested
'p < O.OS, Wilcoxon Signed Ranks test, 2-tailed. --rhere were 9 case control pairs in the French group (8male, 1 female) and 9 pairs in the English group (5 male, 4 female), except for the WUG test and WUG subtests in the latter group with 8 pairs (5 male, 3 female). Cases were SLI subjects meeting study criteria. Theage and sex matched controls were extemal contrais (8 in the English and 3 in the French group) or subjeetsunaffected as per family history report (l in the English and 6 in the French group). In the English group,ages ofall subjeets ranged trom 9.6Oyr to 22.1Oyr with maximal ditrerenœ of 1.54yrbetween the case andmatched control and the mean differenœ ofO.017yr; in the French group corresponding figures were 9.5Syr,2l.35yr, l.42yr and .024yr. b l , equal ranks, not significant. .:pointing was significant ooly in the Frenchgroup.
50
entered into the analysis. Ofthe entire test battery, only the Verb Tense Morphology test
showed significant differentiation from controls for both the overall test and ail sub-tests,
(Real Words and Non...real Words), across both language groups (Table 2). In this case,
based on the distinct theoretical foundation ofthese sub-tests as descnbed in the present
methods section (see alsoGop~ 1999; Rose &. Doyle, 1999) we analyzed further only
the sub-test scores, as per our goal to identify specifie components of linguistic
perfonnance which show familial resemblance. The 7 scores analyzed further in the
English group were Derivational Morphology, Verb Tense Morphology (Real Words),
Verb Tense Morphology (Non...real Words), Grammaticality Judgment (Ungrammatical
Sentences), Grammaticality Judgment (Correct Correction), Syntactic Comprehension
(Non-canonical Sentences), and WUG Test (Non...real Words). The 6 scores analyzed
further in the French group were Derivational Morphology, Verb Tense Morphology
(Real Words), Verb Tense Morphology (Non-real Words), Grammaticality Judgment
(Ungrammatical Sentences), Syntactic Comprehension (Non-canonical Sentences), and
Pointing.
3.3. Corre/ational Structure olTest Batteries and Relationship with Age and Gender
Tables 3 and 4 show, within the English and the French batteries respectively,
correlations between language test scores and correlations of test scores with age at
testing. In both languages, an ofthe test scores targeting specific theoretically derived
components ofPerfonnance were panly correlated among each other, exeept for the
WOG Test (Non-real Words) and Grammaticality Judgment (Correct Correction) in the
51

Table 3
Test and Age at Testing Correlations in the English Test Groupa
Test' DM VTMR VTMNR GJUNGR OJCC SCNC WUGNR.
DM
VTMR 0.60··
VTMNR
OJUNOR
GJCC
SCNC
WUGNR
0.44·· 0.59··
0.30· 0.44··
0.57"
0.31·. 0.20
Age Tested 0.44·· 0.22 0.16 0.15 0.13 0.14
•p < 0.05; iap < 0.01, Spearman's rho, 2-tailed. ~or the language tests, ail ofthe 55 tested subjects areanalyzed, except for the OJeC with 54 and WUGNR with 53 subjects. For the age at testin& 6 probandswere excluded and remaining 49 subjects were included, with 48 subjects for the osce and the WUGNRtest. bSymbols: DM, Derivational Morphology; VTMR, Verb Tense Morphology (Real Words); VTMNRVerb Tense Morphology (Non-real Words); OJUNGR, Grammaticality Judgement (UngrammaticalSentences); GICC, Grammaticality Judgement (Correct Correction); SCNC, Syntactic Comprehension (Noncanonical Sentences); WUGNR, WUO Test (Non-real Words).
52

•
Table 4
Test and Age al Testing Correlations in the French Test Groupa
Tesé DM VTMR VTMNR. GJUNR SCNe POINT
DM
VTMR 0.58··
VTMNR 0.60·· 0.67··
GJUNGR 0.63·· 0.73·· 0.64··
SCNC 0.42·· 0.39·· 0.3"· 0.44··
POINT 0.43" 0.47·· 0.38·· 0.43·· 0.39"
Age Tested 0.44·· 0.60·· 0.46·· 0.45" -0.01 0.38··
.p < 0.05; ••p < 0.01, Spearman's mo. 2-tailed. aAll ofthe 67 subjects are presentai, except for age at testÏDgwhere 12 probands were excluded and remaining 55 subjects were included. bSymbols: D~ DerivationalMorphology; VTMR, Verb Tense Morphology (Real Words); VTMNR. Vero Tense Morphology (Non-realWords); GJUNG~ Grammaticality Judgement (Ungrammatical Sentences); SCNC. SyntacticComprehension (Non-canonical Sentences); POINT. Pointing.
S3

English group. Derivational Morphology and Grammatical Judgment (Ungrammatical
Sentences) test scores were significantly correlated with age in the English group. In the
French group, most test scores showed similar and significant correlation with age except
for the Syntactic Comprehension (Non-Canonical Sentences). Gender comparisons for
age at testing and test scores, excluding probands, were made between 31 males and 24
females in the French test group offamilies, and between 23 males and 26 females in the
English test group offamilies. The only significant gender ditTerence, within the power
limits of the sample sizes, was found for Derivational Morphology test in the French test
group, with males showing poorer performance (p = 0.028, two-tailed, Mann-Whitney U
test).
3.4. Sib/ing Resemblance for Specifie Components ofLinguistic Competence
As described in the methods section, in the English group 41 sibling pairs from
the densely affected extended FE pedigree were analyzed. In the French group, 38 sibling
pairs from 10 families were analyzed, with 15 pairs from the single nuclear family.
Table 5 presents correlations for language test scores in sibling pairs from the
English test FE pedigree, and the French test group ofpedigrees. In the FE pedigree,
performance on the Derivational Morphology test showed significant sibling correlation.
In the French test group ofpedigrees, performance on the Verb Tense Morphology (Real
Words), as weil as the Verb Tense Morphology (Non-real Words), showed significant
sibling correlation. In order to examine whether a correlation between age at testing in
sibling pairs might potentially account for observed significant correlations in language
S4

Table 5
Siblinga Correlations for Specifie Components ofLinguistie Competence
French Pedigrees
Test English FE Pedigree lN =10)
~ If Il Nœm ~ Il
Derivational Morphology 41 0.52" 0.001 38 0.27 0.10
Verb Tense Morphology (Real Words) 41 -0.02 0.90 38 0.39· 0.02
Verb Tense Morphology (Non-reaI Words) 41 0.24 0.14 38 0.35· 0.03
Grammaticality Iudgement
(Ungrammatica1 Sentences) 41 0.06 0.72 38 0.21 0.21
Grammaticality Iudgement
(Correct Correction)b 41 -0.16 0.31
Syntactîc Comprehension
(Non-canonica1 Sentences) 41 -0.04 0.80 38 0.19 0.25
WUG Test (Non-reai Wordst 36 0.02 0.92
Pointingd 38 -0.04 0.80
'p < 0.05; "p < 0.01, 2-tailed, Spearman's ma coefficient ofcorrelation (r,). anere were 10 male and 12female pairs in the English speaking FE pedigree, and 21 male and 4 fema1e pairs in the French group of 10pedigrees. Remaining sibling pairs were ofdifferent sexes. ~ot scored in the French language group.eAdnûnistered only in the English language. dpointing is not aoalyzed in the English language because it didnot differentiate cases from controls.
55
test scores, we computed partial correlations controlling for age at testing (Table 6). The
sibling correlation for performance on the Verb Tense Morphology (Real Words) in the
French language group remained significant ailer controlling for age. The sibling
correlation for performance on the Derivational Morphology test in the English FE
pedigree remained substantial after controlling for age, although with borderline
statistical significance (p = 0.05), perbaps due to power limitations.
56

Table 6
Partial Sibling Correlations Controlling for Age at Testing
Lanauaae ]§ ~ r R ~.LI!IIIIIIJ
English
FE Pedigree Derivational Morphology 3S 0.3ge
0.02 034 005
Frencb
Pedigrees Verb Tense Morpbology (Real Words) 34 0.42e
0.01 0."- 001
(N = 10) Verb Tense Morphology (Non-real Words) 34 0.40e
0.02 0:7 o 14
•P < 0.05; liP< 0.0l, 2-tailecL df=N - 2 for Pearson's rand df= N - 4 for panial correlation ·Pan.alcorrelations, controUing for Slbling correlations for age al testing, were computed using normal Z scores inmore numerous SlDling pairs from the age group younger than 2Syr at testing.
57
4. Discussion
We examined specifie theoretically derived components ofperformance on the
English or French Linguistie Test Profile Battery in families ofSLI children, recruited
ftom various sources within each language group, and most ofwhich were known to bave
al least one impaired first-degree relative. The examined test scores differentiated SLI
cases from age and sex matched controls, and were general1y partIy correlated.
Significant sibling correlations were found for performance on tests that involve
production ofgrammatical morphology. These include Derivational Morphology in the
English language (N =41 sibling pairs from the single densely affected FE pedigree), and
Verb Tense Morphology (Real Words) as weil as Verb Tense Morphology (Non-real
Words) in the French language group (N = 38 sibling pairs from 10 pedigrees). The
observed correlation oftest scores with age may be related, in part, to therapeutic effects
and the use of leamed strategies for compensation of language impainnent (paradis &
Gopnik, 1997; Kehayia, 1994; Kehayia., 1997). Sibling correlation for Verb Tense
Morphology (Real Words) in the French group remained significant after controlling for
age. The sibling correlation for Derivational Morphology in the English speaking FE
pedigree was borderline (p =0.05) after controlling for age.
Independent studies demonstrate that impaired grammatical morphology is a
predominant aspect ofSL!, notwithstanding the lack ofconsensus regarding particular
etiological hypotheses (Rice & Oetting, 1993; Rice & Wexler, 1996; Oetting & Horohov,
1997; Leonard et al. 1999; Riee, 1999). A series ofGLIP reports based on the analysis of
English and French speaking subjects from the present study, as well as Greek and
58

Japanese speakers, advanced a cross-linguistic hypothesis of impaired ability ta construet
morphological rules in SLI (summarized inGo~ 1999; Rose &. Doyle, 1999). Within a
somewhat different grammatical account, a set ofgrammatical morphemes for Tense
marking (-s third persan singular, -ed regular past, BE, and 00) was proposed as a
clinical marker for English sPeaking SLI children (Rice &. Wexler, 1996; Bedore &.
Leonard, 1998).
The present study provides no information that could distinguish between the
relative contributions ofgenetic and environmental factors to observed sibling
resemblance. A recent twin study reported heritability of0.45 for extreme, composite
English language scores where at least one twin bad poor oral language status without
other developmental or sensory impairments; sunilar results were obtained when the
required minimal nonverbal IQ was either 70 or 85 points (Tomblin &. Buckwalter,
1998). The composite language score in the Tomblin study comprised 4 receptive and 4
expressive test measures often used in clinical praetice. Neither the composite language
score nor individual tests targeted Derivational Morphology or Verb Tense Morphology
as specifically as tests examined in the present report. Another English language twin
study ofSLI (Bishop et al. 1995) reported high heritability estimates for Word Finding,
for a Test for Reception ofGrammar, and for the Comprehension test from the WISC-R
intelligence test. A lower heritability was reported for Repeating Sentences, suggesting
that sorne specifie aspects of linguistic competence could he onder greater genetic
influence then others. Again, none ofthese tests specifically targeted Derivational
Morphology or Verb Tense Morphology. The hypothesis ofsubstantial heritability for
59

these particular components ofthe SLI phenotype awaits further specifica1ly targeted
studies.
4./. Pedigree Structure for Sihling Pairs in the English and French Test
AlI sibling pairs tested in English originate from the single extended FE pedigree
which is densely atTected Ce.g. 14/34 atTected cousins) and therefore not representative of
SLI pedigrees. A high proportion ofatTected relatives is the reason that this particular
pedigree was selected for extensive testing, and this could also he positively related to
willingness to participate in the project. These circumstances might have a priori reduced
the generalizability offindings to the larger SLI population. This might potentially relate
to the lack ofsibliog resemblance for Verb Tense Morphology, proposed to he a clinical
marker for English speaking SLI children (Riec & Wexler, 1996). The proband in the FE
kindred had a recorded nonverballQ of71, and evidence ofa central auditory processing
defieit, with normal audiogram as per SLI criteria in this study. Regarding the density of
impaired individuals and nonverbal IQ, the FE pedigree is similar to the K family where a
fully penetrant autosomal dominant gene was mapped to severe speechllanguage
impairment with speech and orofacial dyspraxia (Vargha-Khadem et al. 1995; Fisher et
al. 1998). However, the FE pedigree does not show the same Mendelian pattern of
inheritance or orofacial dyspraxia in affected memhers. It might he hypothesized that
pedigrees which segregate larger numher ofspecifie risk factors, i.e. defieits in nonverbal
IQ, auditory processing, etc., are more Iikely ta he densely affected, but this hypothesis
requires more research ioto the effects ofparticular factors.
60

In contrast, sibling pairs tram the French group in the present study originate from
10 pedigrees, none ofwhich were denselyatTected. The differences in both the test
language and pedigree structures make it difficult to interpret the observed ditTerences in
sibling correlations between the English and French test subjects. Tbese familial
considerations may underscore the etiological complexity ofimpaired grammar which is
on the surface rather similar aeross languages and pedigree structures (including the FE
and the K families), featuring a prominent deficit in morphological produetîon (Gopnik,
1999).
4.2. Limitations
The test-retest reliability ofadministered language tests is not known. It is aIso
clear that the present study was underpowered, and is thus wlnerable to both Type 1and
Type II statistical errors. The smalt sample size also precluded stratification ofsibling
pairs by gender. It is not known whether the assumption ofan interval scale of
measurement for language test scores, which underlies the computation ofpartial
correlations controlting for age at testing, is valid. The exclusionary nonverbal IQ
criterion was 70., rather than 85 points as suggested in sorne ofthe Iiterature. However.,
reeent views (Gopnik & Goad, 1997; Plante, 1998; Tager-Flusberg & Cooper, 1999)
conceptuaIize a nonverbal IQ between 70 and 85 as a potential risk factor, rather than
exclusionary condition for SLI.
61
4.3. Conclusion
We approacbed familial study ofgrammati~impainnent in SLI from the
perspective ofa complex phenotype with theoretica11y distinct components which may he
partially decomposed by test design and statistical analysis. The results, which require
independent replication, suggest that Derivational Morphology and Verb Tense
Morphology production, independently documented as predominant aspects ofSLL
warrant particular attention in future familial and genetie studies of this important
communication disorder. More sensitive measurements, sueh as psychometrie on-line
task-processing time (Kebayia, 1994; Kehayia, 1997) could he developed to deteet
impaired adults who may score at high levels on the present test battery due to correlation
with age. Analogous to the example ofdyslexia, these specifie components ofthe SLI
phenotype could potentially he useful for geoetic studies, perhaps eventually providing
molecular elues to underlying influences of infonnation processing, linguistic neural
substrates or other etiological processes that are oot weil understood at present.
62

Aeknowledgement
This work within the multidisciplinary MeGill University Genetic Language
Impainnent Projeet (MyrnaGo~ PI) was supported in part by an Intercouneil Group
Grant from the Medical Researeh Couneil ofCanada and the Social Sciences and
Humanities Researeh Couneil (M. Gop~Principal Investigator). Additional support
from the Medical Researeh Couneil (MA...11663 t GR...14501) is aclmowledged. This work
is in partial fulfillment ofthe requirements ofthe Ph.D. degree (Ilija Kovac).
63

•
AppeDdix
Analyzed Subjectg& by Test Language and Familial Relationships
Test Language
Family
~ ~
Family Members Family Members
Nuclear ~ ~rd Other Nuclear ~Dd tJ:lrd Other
AI - - - - 4 - - -AR - - - - 5 - - -BC - - - - 2 - - -CA - - - - 4 - - -CG - - - - S - - -CT - - - - 5 - - -CX - - - - 4 - - -DP - - - - 4 1 2 -DS - - - - 4 2 2 le:
EA - - - - 8 - - -FE 3 4 14 - 3 1 3 r:FG 1 - - - 1 - - -FX - - - - 2 - - -LB 4 1 3 ICI - - ICI
SB 2 - - - 2 - - -DA 1 - - - - - - -HA 4 - - - - - - -HB 3 1 - - - - - -
He 1 - 1 - - - - -lA 3 - - - - - - -JO 3 - - - - - - -LA 1 - - - - - - -SA 4 - - - - - - -I: 30 6 18 1 S3 4 7 3
~cluded subjects not shawn, (N = 16 and 12 in the English and French test group respectively, as notOO inthe methods section).~ee ofrelationship ta the proban~ who is included here among nuclear familymembers. ~arried-in. ~ounh-degree relative.
64

Bridging CommeDtary
Like the preceding one, the following manuscript, entitled "Attention
Defieit/Hyperaetivity in SLI Children Inereases Risk ofSpeecblLanguage Disorders in
First Degree Relatives: A Preliminary Report"t is based on the data gathered within the
McGill University Genetie Language Impairment projeet (Myrna Gopnik, PI). However~
this report is based on Medical records offamilies identified through the Association of
Quebec Dysphasie Children, without regard ta familial aggregation ofthe disorder. This
design allows for a different approaeh to potentially defining a more familial form ofthe
SLI phenotype, by examining the influence ofattention deficit/hyperactivity in SLI
children on familial aggregation ofspeecbllanguage disorders. Among 27 anal~ozed
families, 8 families also completed language test battery in the course of research
analyzed in the preceding manuscript. In these 8 families, 4 adults who were reponedly
impaired achieved test scores similar to contrais; however, this does not invalidate family
history information because these adults might have compensated for potential language
impainnent. Remaining test scores in these 8 families were unremarkable with respect to
family history information. Because Most offamilies analyzed in the following repon
were not tested on the language test batteryt it is not possible to evaluate the relallonshlp
between findings from these two manuscripts.
65
2(b). AITENTION DEFICITIRYPERACTIVITY IN SU CllILDREN INCREASES
RISK OF SPEECBlLANGUAGE DISORDERS IN FlRST-FEGREE RELATIVES:
A PRELIMINARY REPORT
The present chapter consists ofthe following manuscript in submission, entitled
as above.
66
Increased Risk
Running head: INCREASED FAMILIAL RISK IN SU
Attention Deficit/Hyperactivity in SLI Children Increases Risk ofSpeech/Language
Disorders in First-Degree Relatives: A PreJiminary Report
llija Kovac1, Berdj Garabedian2
, Christele Du Souich2,4, Roberta M. Palmourl,2.3
Departments ofBiologyl, Human Genetics2 and Psychianyl, McGill University,
Montreal, Québec~ CANADA
4Present address: Department ofMedical Genetics3, University ofBritish Columbi~
Vancouver, British Columbia, CANADA
Address for correspondence:
Roberta M. Palmour, Ph.O.
Department ofPsychiatry, McGill University
1033 Pine Avenue West., Room 307
Montréal, Québec, H3A lAI
CANADA
Tel. (514) 398-7303
Fax (514) 398-4370
E-mail: [email protected]
67

Increased Risk
Abstraet
Specific language impainnen~ or developmental dysphasia, denotes the inability
to acquire normal expression and/or comprehension of language in the absence of
peripheral hearing impairmen~ neurological disorder, and mental retardation. The
presence ofattention deficit/hyperactivity in sorne SLI children has previously been
documented. This family history study used 27 SLI families, identified through the
parents from the dysphasia association, to examine the relationship between anention
deficit/hyperactivity in SLI children and the risk to first-degree relatives. Ail SLI chlldren
were clinically diagnosed with speech/language disorder; Medical records were scarched
for the presence ofany ofthe exclusion criteria noted above. Higher odds of
speech/language disorders were observed in first-degree relatives of 13 SLI children \\1th
Medical record ofattention deficitlhyperactivity, than in relatives of 14 SLI chlidren
without such record (15/27 and 4/46 respectively, p=O.OOI). This preliminary repon
warrants additional study to investigate the relationship between speech/language
disorders and attention deficitlhyperactivity in families of SL! children.
Educationa/ Objectives: The reader ofthis article will: 1) leam about the definltlon.
prevalence and cornplexity ofthe SLI phenotype 2) learn about the relation bc:tween co
morbid attention-deficit/hyperactivity in SLI children and the risk of speech.language
disorder in their relatives.
68

Increased Risk
KEY WORDS: communication disorder~ attention deficit, hyperactivity, phenotype,
familial
Introduction
Specifie language impainnent (SLI), or developmental dysphasia, denotes the
inability to acquire correct expression and/or comprehension oflanguage and is usually
diagnosed at preschool or early school age. The diagnosis ofSLI requires bath positive
identification ofspeech/language impairment, as weil as exclusionary and/or discrepancy
criteria comparing speech-language ability to some other cognitive measure (Aram,
Morris, & Hall, 1993; Dunn et aL 1996; Plante, 1998). Exclusion criteria commonly
include mental retardation, peripheral hearing impairment and overt neurological
disorder; operational measures of these parameters vary from parental/clinician's
descriptions to formai evaluations (Lahey & Edwards, 1995; Lewis, Ekelman, & Aram,
1989; Lewis, Cox, & Byard, 1993; Neils & Aram, 1986; Redmond & Rice, 1998; Rice,
Haney, & WexIer, 1998; Tallai, Ross, & Curtis, 1989; Tomblin, 1989; Tomblin et al.
1997). Children diagnosed with SLI in accordance with these exclusion criteria often
have milder behavioral, neurological, auditory and cognitive deficits (Goorhuis-Brouwer
& Wijnberg-Williams, 1996; Lubert, 1981; Powell & Bishop, 1992; Redmond & Rice,
1998; TallaI et al. 1991; Wright et al. 1997). Positive operational criteria for
speech/language impairment also vary among studies, but a commonality is that probands
are generally impaired enough to warrant clinical treatment. The best estimate ofthe
population prevalence (USA) for SLI is 7.4% in preschool children (Tomblin et al. 1997).
69

•
Increased Risk
The familial aggregation ofSLI bas been repeatedly documented, and twin data suggest
that genetic factors May he etiological (Bishop, North, &. DonIan, 1995; Lewis, Ekehnan,
&. Aram, 1989; Neils &, Aram, 1986; Rice, Haney, &, Wexler 1998; Tallai, Ross, &
Curtis, 1989; Tomblin. 1989).
Attention deficit/hyperactivity behavioral problems are observed in SLI children
(Aram, Ekelm~ &, Nation, 1984; Goorhuis-Brouwer &. Wijnberg-Williams, 1996;
Redmond and Riee, 1998; Tallai et al. 1991), raising the question ofthe relationship
between attention deficitlhyperactivity disorder (ADHD) and SLI. ADHD is another
eommon childhood onset disorder with a population prevalence of3·10% (Cantwell,
1996), and substantial evidence of familial aggregation with genetie etiological factors
(reviewed in Rutter et al. 1999). According to the OSM-IV criteria, sorne individuals May
predominantly show either attention deficit or hyperactivity, but MOst show a combined
ADHD phenotype (APA, 1994). There cao be developmental transition between these
symptoms. Co-morbidity between ADHD and other psychiatrie disorders is weil
documented (pliszka, 1998), and perhaps 2/3 ofchildren with ADHD show speech and
language disorders (Cantwell, 1996; Love & Thompson, 1988; Smalley, 1997).
Conversely, children with speech/language problems, but undefined with respect to the
exelusionary SLI criteria, show co-morbidity with other psychiatrie disorders, including
ADHD (Beitchman et al. 1986).
The rationale for the present study is that a comprehensive description ofthe
phenotype in individuals with a panicular complex disorder May allow discrimination of
clinical subtypes, which May in turn improve the power to identify etiological factors or
processes. A useful component in validating potential etiological subtypes is an
70

•Increased Risk
investigation ofthe familiality of the different phenotypes. Labey and Edwards (1995),
following this rationale, reported an increased risk to relatives ofSU children with
expressive, as compared to SLI children with mixed expressive-receptive language
disorder. Tallai and coworkers (TallaI et al. 1991) found tbat SLI children who had at
least one impaired parent had more attention/hyperactivity behavioral problems as rated
by parents and teachers. In view ofthe latter result, it cao he hypothesized that the risk to
relatives ofSLI children with attention/hyperaetivity behavioral problems might he higher
than the risk to relatives ofSLI children without such problems. In this study we
compared the risk to first-degree relatives in subgroups ofSLI children ditTerentiated by
the presence or absence ofthe Medical record ofattention deficitlhyperactivity.
Method
Participants
Recruitment. French speaking families with speech/language impaired children
were initially approached for the McGill University Genetic Language ImPainnent
Project (Myrna Gopnik, Ph.D., PI) by announcement in the newsletter of the Association
ofQuebec Dysphasie Children (AQEA). Infonnants from the total of 156 responding
families were contacted by telephone (Figure 1) to canfion their interest in participating
in the projec!, and family history infonnation (described in detail below) was obtained.
Upon consent, a systematic review ofthe clinical records of language impaired children
was conducted. The hospital and/or school records for speech/language imPaired children
from 76 families were available (Figure 1). Participants were treated in accordance with
71

Increased Risk
Telephone Interview
(N= 156)
No Medical
RecordsMedical Records Review
(N =80, excluded)(N=76)
SLI(N=27)
SLIadlh)'P- (N = 14)
SLIadlhyp+ (N = 13)
~on-SLI (N =24, excluded)
bundefined (N = 25, excluded)
Figure 1. Selection and Subgrouping ofSLI Families. Symbols: N, number offamilies~
SLIadlh~'P-' no medical record ofattention deficitlhyperactivity in the SLI proband;
SLIadlhyp+. Medical record ofattention deficit/hyperactivity found in the SLI proband.
aNon-SLI families are those in which Medical records documented exclusionary
condition(s) in the speech/language impaired children. tundefined families are those in
which medical records did not contain ail information pertinent to exclusionary criteria.
72

Increased Risk
the "Ethical Principles ofPsychologists and Code ofConduct" (American Psychological
Association, 1992).
Inclusion and exclusion criteria The inclusion criterion in the present study was
the diagnosis ofspeecbllanguage disorder by a certified speecbllanguage pathologist. By
virtue ofAQEA membership, ail families had speecb/language-impaired children who
met this criterion. The presence ofone SLI proband in the family was sufficient for
inclusion ofthe family in the study, regardless ofthe status ofother speech/language
impaired children, ifany, in the same family. Exclusion criteria in the present study were:
(1) no peripheral hearing impairment, as per Medical record ofa formal audiological test
such as audiogram or tympanogram, depending on examining physician, or the
improvised audiological exam (2 probands); (2) no mental retardation, as per medical
record ofa nonverbal or perfonnance IQ score ~85, formai psychological testing, or
clinical psychological reports; (3) no overt neurological disorder, as per Medical records
ofa neurological exam and/or EEG, MRI or CT scan; and (4) no developmental
syndromes or serious medical conditions (one child had a coloboma and was excluded).
Retention ofSLI families. Speechllanguage impaired children whose Medical
records did not contain sufficient information pertaining to exclusionary criteria were
classified as "undefinedn and excluded from the present study, as were the children
whose medical records documented exclusionary conditions (Figure 1). The 27 families
with speecManguage impaired children whose medical records documented absences of
exclusionary conditions were retained as SLI families (Figure 1).
73

Increased Risk
Family Historv
Family bistory interview. A semi-struetured family history (FH) interview
(questionnaire in the Appendix), with infonnants who responded to the recruiting
announcemen~ was conducted over the telephone by a trained genetie counselor.
Information on sex, birth date, degree ofrelation, general health (medical problems,
mental retardation, hearing, or psychological problems), speechllanguage problems,
speech therapy, readiog/writing problems and educationaVschool problems was collected
Family history information pertaining to first, second and third degree relatives of
speeeh/language impaired children was obtained Most ofthe infannants from the initial
156 families, and all informants in the 27 SLI farnilies presented in this report (Figure 1),
were mothers.
Family history based classification of relatives. Here we initially use phenotype
definition similar ta that used by Tallai and coworkers (Tallai et al. 1991). Family
members were classified as affeeted if they have a present or past report of
speechllanguage problem, reading/writing problem, received speech therapy, and/or
oogoing educational or school problems. We have also used an alternative phenotype
definition, where individuals with reported ooly learning or ooly readingl writing problem
are classified as unaffected. This alternative definition was used exclusively in the event
of initially significant difference in the risk ta relatives between SLI subgroups, to assess
whether this difference persists when the affected phenotype is restricted to those reports
that refer specifically ta the speech/language problem. Relatives younger than 3yr were
excluded from the analysis ofFH da~ because speech/language impairment May not be
reliably observed at younger ages.
74

•
Increased Risk
Statistical Analysis
The Pearson's X2 test was used to test the hypothesis that the odds ratio for having
an atfeeted first-degree relative, calculated for the subgroups ofSLI probands in 2 x 2
contingency tables, is significantly different ftom 1 (Fleiss, 1981). When any ofexpeeted
cell counts was ~5, the Fisher's exact test was used The tests and odds ratio estimates
were performed using the SPSS 8.0 statistical software. Statistical significance in this
report was generally determined at the 0.05 level in 2..tailed tests.
Results
As described in the Recruitment section, the selection ofSLI families was a
multistage process incorporating a number offactors, such as family membership in
AQEA, awareness of recruiting announcement, participation in family history interview,
and completed review ofMedical records. While we do not have enough information to
examine potential biases with respect to the sampling offamilies at most stages, we have
compared 76 families in which the Medical records ofspeech/language impaired children
could be reviewed with 80 families for which only the family history interview was
completed (Figure 1). These two groups were not significantly different with respect to
the proportion ofaffected first-degree relatives [0.16 or 42/261, and 0.21 or 58/282
respectively, ('x.2 = 1.81, P=0.18, 2-tailed)]. The groups were also similar in the
male/female ratio ofclinically diagnosed speech/language...impaired children (3.1: 1or
65/21 and 3.7:1 or 70/19 respectively). In order to examine whether the absence of
pertinent data in the Medical records might bias the retention of SLI families, we
75

•Increased Risk
compared the "undefined" families~ excluded due to the lack ofda~ to the pooled
uexcluded'" (due to exclusionary conditions) and SLI groups (Figure 1). There were no
significant ditTerences~ with proportions ofaffected first-degree relatives of0.15 (12179)
vs. 0.17 (30/182), respectively, and malelfemale ratios ofclinically diagnosed children of
3.1:1 (22/7) vs. 3.1:1 (43114). Hence the stratification associated with availability and
completeness ofmedical record information did not appear to have introduced bias, at
least with respect to familial incidence and sex ratio~ ioto the pool of families
investigated further.
The SLI families
ln 27 SLI families (Figure 1), identified as described in the method section, there
were 28 SLI probands among 32 clinically diagnosed speechllanguage impaired children.
ln one family, there were male twin (purportedly MZ) SLI probands, and in 3 other
families there were clinically diagnosed speechllanguage impaired children in addition to
the SLI proband. The Mean age of SLI probands in these 27 SLI families (excluding 1 MZ
twin proband) was 8.10 ± .75 years, ranging from 3-18 years. The male-female ratio of
SLI probands was 23:4 (not counting one reportedly MZ male twin)~ and 25:6 when aH
clinically diagnosed speechllanguage impaired children are considered.
Of the 28 SLI probands, 22 (79%) had Medical records evidence of non
exclusionary anomalies such as mild neurological symptoms (fine motor problems,
coordinationlbalance problems, immaturity, motor delay, minimal cerebral dysfunction,
slight hypotonia) and/or behavioral problems (attention deficitlhyperactivity, mild autistic
signs~ unspecified behavioral problems). The fact that we required ail probands to have a
neurologjcal evaluation in Medical records probably contributed to the identification of
76

Increased Risk
mild neurological signs, which could he under-reported ifonly the report ofa parent or
speech pathologist was used. AIl ofthe S SU probands with Medical record references to
mild autistic signs were diagnosed with semantic-pragmatic syndrome, which often
appears to he similar to the communication ofautistic children (Rapin & Allen, 1983);
i.e., these children may speak about themselves in the third persan. No SLI probands in
our study were diagnosed with sensory...motor disorder ofSPeech production (dysarthrîa),
although some investigators think ofverbal dyspraxia (diagnosed in some children) as a
severe speech production disorder rather than a language disorder, dePending on
unresolved models of language reception/production (Rapin, 1996).
Clinical Subgroups
The 13 families in which Medical records for 14 SLI probands (including 2 twins)
contained any reference to attention deficit and/or hyperactivity (not necessarily a DSM
diagnosis) in psychological or neurological evaluations, referred ta hereafter as the
medical record ofattention deficit/hyperaetivity (ad/hyp), constituted the SLladlhyp+
subgroup (Figure 1). The remaining 14 families, with no Medical record ofattention
deficitlhyperactivity in the SLI proband, constituted the SLIadJbyp- subgroup (Figure 1).
The difference in ages of 13 SLI probands from the SLladlhyp+ subgroup and 14 SLI
probands from the SLladJhyp- subgroup did not reach statistical significance (9.58 ± 1.14
vs. 6.71 ± .87 years respectively, p = 0.06, t-test, 2-tailed), however this small sample had
little statistical power. One ofthe 2 MZ twin SLI probands from the SLladIhyp- subgroup
was excluded from this age comparison because his age is correlated with the age ofbis
twin SLI brother, confounding the comparison. The male-fernale ratios of SLI probands
in the SLladlbyp+ subgroup and SLIadlbyp'" subgroup were 12:1 and Il:3, respectively. We
77

Increased Risk
note that the reportedly MZ twin SU probands were together in the SLIadlhyp+category,
a1though one was diagnosed with syntactic-phonological syndrome and verbal dyspraxia,
while the other was diagnosed with syntactic-phonological syndrome alone (diagnostic
definitions given further, below).
Family Historv in Clinical Subgroups
Table 1presents family history information for first-degree relatives ofthe
SLladlhyp- and SLladlhyp+ subgroup, where subgroups are defined respectively by the
absence or presence ofthe Medical record ofattention deficit/hyperaetivity as described
above. In addition, exclusively in the SLladlhyp+ subgroup we found 4 clinicaUy diagnosed,
speech/language impaired siblings ofSLI probands from 3 families. Together with Il
relatives affected by FR criteria (Table 1), these 4 children malee a total of 15 affected
first-degree relatives in the SLIadIbyp+ subgroup, as compared to 4 affected first-degree
relatives in the SLladIbyp- subgroup.
Table 2 shows that SL! probands with a Medical record ofattention
deficit/hyperactivity have higher odds ofhaving an affected first-degree relative then SLI
probands without a record ofad/hyp. Due to the moderate sample size, the estimate of the
odds-ratio value is imprecise as shown by a broad 95% confidence interval (Table 2).
Following this significant resul~ we have also tested the odds-ratio difference using an
alternative phenotypic definition, whereby 4 individuals with a report of isolated learning
or readinglwriting problems (Table 1) are classified as unaffected for speech/language
disorder. This alternative odds-ratio difference remained statistically significant [4/46 vs.
11/31 in the SLladlhyp- and SLladIhyp+ subgroup respectively (X2 = 5.54, df= 1, P=0.019,
Pearson's X2 test, 2-tailed; OR = 4.08, 95%CI = 1.19 - 13.98).
78

Increased Risk
Table 1
Family History Report for First-Degree Relatives
Family History Report
Language problem
Language and leaming problem
Expressive problem
Expressive and leaming problem
Learning problem
Pronunciation problem
Articulation problem
Stuttered when young
Reading and writing problem
1
1
1
1
3
.,-
Note. Symbols: aSLI probands without medical record ofattention deficit'hyperacu\'ny. N
= 50 first-degree relatives in 14 families; bSLI probands with medical record ofattention
deficit/hyperactivity, N = 42 first-degree relatives in 13 families. COashes denote absence
ofthe corresponding family history report in a given subgroup ofSLI children.
79
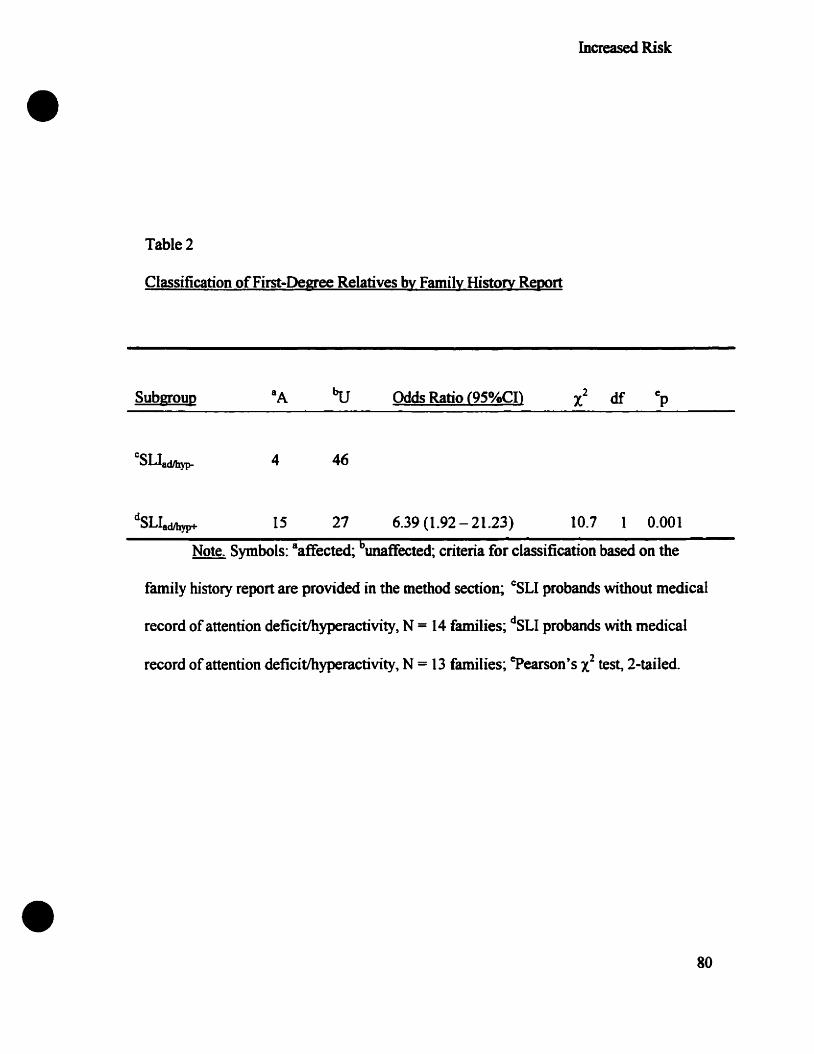
Increased Risk
Table 2
Classification ofFirst-Degree Relatives by Family Historv Report
Subgroup
4 46
Odds Ratio C95%Cn
dSLIadlhyp+ 15 27 6.39 (1.92 - 21.23) 10.7 1 0.001
Note. Symbols: aaffected; bunaffected; criteria for classification based on the
family history report are provided in the method section; cSLI probands without medical
record ofattention deficitlhyperactivity, N = 14 families; dSLI probands with medical
record ofattention deficitlhyperactivity, N = 13 families; epearson's X2 test, 2-tailed.
80

•Increased Risk
Table 3 summarizes the proportions ofvarious classes ofaffected first-degree
relatives in the SLIadIhyp- and SLIadtbyp+ subgroups. We note that the reported proportions
ofaffected second-degree relatives in the SLIadJhyp-and SLladIhyp+subgroup were 0.03
(5/177) and 0.11 (19/166), respectively. The reported proportions ofaffeeted third-degree
relatives (first cousins) were 0.07 (13/197) and 0.08 (17/201), respectively. The FR report
for extended relatives is expeeted to he less reliable than for first-degree relatives, and
less sensitive in particular, thus underestimating the risk to these relatives (Andreassen et
al. 1977). It is also subject to the reporting bias where relatives tram the informant's
lineage (maternai relatives in the present study) are more often reported as affected, as is
generally observed in the present study.
There were 5/14 families in the SLIadIhyp- subgroup and 5/13 families in the
SLIadlhyp+ subgroup in which clinically treated, speechllanguage-impaired children were
first-bom. Because the presence ofa clinically diagnosed speech/language...impaired child
may confer closer scrutiny to subsequently barn childre~ such stratification by birth
arder, when present, could contribute to differences in the proportion ofaffected siblings.
Another factor POssibly contributing to increased risk to first-degree relatives might be
increased assortative mating. There were 1114 and 1/13 families with bath parents
affected in the SLIadlbyp- and SLIadlbyp+ subgroups, resPectively. This is inconsistent with
the notion that attention deficit/hyperactivity mediated increase in assonative mating for
communication disorders (possibly as an etiologically independent modifier that
increases severity) might explain observed difference. The male-ta-male transmissio~
reported in sorne nuclear families from the SLladlbyp+ subgroup, would argue against a
simple X-linked pattern ofgenetic inheritance in this subgroup.
81

Increased Risk
Table 3
Risk by Type ofFirst-Degree Relative
First-Degree Relative aSLIlIdIhyp- bSLIadJhyp+
Parents 4/28 (0.14) 9126 (0.35)
Fathers 2114 (0.14) 4c113 (0.31 )
Mothers 2/14 (0.14) Sc,d /13 (0.3QI
Siblings 0/22 6c/16 (0.38)
Brothers 0/14 3c/I0 (0.3)
Sisters 0/8 3/6 (0.5)
4150 (0.08) 15/42 (0.36)
Note. Truncated at the age 3yr (n = 3 siblings from each subgroup). The I\\,n SLI
proband in 1 family from the SLIadlhyp subgroup was not counted as the first--deb-rree
relative because he was reportedly a MZ twin. Symbols: aSLI probands without medlcal
record ofattention deficitlhyperactivity, N = 14 families; bSL1 probands ";th medlcal
record ofattention deficitlhYPeractivity, N = 13 families; cincludes 1 person "1th a
report of learning problem; dincludes 1 person with a report ofreading/writing problem.
82

•
•
Increased Risk
Heterogenous Speech/Language Phenotype in SLI Probands
Heterogeneity in the speech/language phenotype could potentially confound
observed SLladl11yp+ vs. SLIadIbyp- ditTerence in the risk to first-degree relatives. A clinical
diagnosis of semantic-pragmatic syndrome was round in the MediCal records of 8
probands. Other probands were diagnosed with semantic-pragmatic syndrome and
dyspraxia (2), syntactic-phonological syndrome (8), syntactic-phonological syndrome and
developmental verbal dyspraxia (8), syntactic and semantic deficit (1), or developmental
verbal dyspraxia (1). Semantic-pragmatic syndrome denotes correct phonology and
syntax accompanied by inappropriate use of language, indicating difficulties with
semantic and social aspects of language (Rapin & Allen, 1983; Rapin, 1996; Snow &
Swisher, 1996). Syntactic-phonological syndrome denotes poor phonology, syn~ and
morphology (Rapin & Allen, 1983; Rapin, 1996; Snow & Swisher, 1996). Verbal
dyspraxia denotes severe expressive language problem with sparse output and very poor
phonology (Rapin, 1996). We compared the odds ofhaving an affected first-degree
relative in the 8 SLI probands diagnosed with semantic-pragmatic sYndrome alone
("fluent" SLI, N = 3 probands in the SLIad/hyp+ subgroup), and the remaining 19 SLI
probands with documented problem in the domain ofsYntax-phonology r~non-fluenf'
SLI). The atTectedlunaffected ratio, including leaming and reading/writing problem as
affected, was 2/24 in the "fluent" vs. 17/49 in the "non-fluent" SLI subgroup (p = 0.08,
Fisher's exact test, 2-tailed; OR = 4.16, 95%CI = 0.89 - 19.51).
83
Increased Risk
Discussion
In this study we found significantly higher odds ofhaving an affected first-degree
relative in 13 families ofSL! probands with concomitant Medical evidence ofattention
deficitlhyperactivity in the proband, than in 14 families of SL! probands whose Medical
records showed no evidence ofattention deficit/hyperactivity. Tallai and coworkers
(Tallai et al. 1991) reported that family history positive SLI probands (defined as having
at least one affeeted parent) were more likely ta have attention/hyperaetivity behavioral
problems, as reported by parents and teachers on the Achenbach's Child Behavior
Checklist. The present study therefore extended this finding by providing independent
data on familial ris~ including parents and siblings, which shows that the converse
relationship May also hold true.
The phenotypic definition ofaffected first-degree relatives employed in the
present study was similar to that employed by Tallai and coworkers for the classification
ofaffected parents of SLI probands (TallaI et al. 1991), including a report of learning and
reading/writing problems in addition ta the speech/language problems. Due to the
association ofcommunication and learning disorders, MOst family studies ofSLI used
sorne fonn ofbroader phenotype definition based on FH information (Lahey & Edwards,
1995; Lewis, Ekelman, & Aram, 1989; Neils & Aram, 1986; Rice, Haney, & Wexler
1998; TallaI, Ross, & Curtis, 1989; Tomblin, 1989). In the present study we also
examined an alternative phenotypic definition, whereby individuals with a report of
isolated leaming problems or isolated reading/writing problems were classified as
unaffected The increased risk to first-degree relatives from the SLIadlbyp+ subgroup
84
Increased Risk
persisted under this alternative phenotypic definition, providing more confidence that the
observed diiferentiation May relate to speech/language disorders. Labeyand Edwards
(1995) did not find ditIerences in family history with respect to parent-reported
behavioral problems in SL! probands. However, few SL! probands in their study were
reported to have behavioral problems, and not ail ofthose were rePOl1ed as attention
related problems.
The present study is not informative with respect to the nature ofthe relationship
between speech/language disorders and attention deficitlhyperaetivity in famifies ofSLI
children. It could he speculated that attention deficitlhyperactivity, whether etiologically
independent or not, might hinder the improvement ofspeech/language performance over
time, facilitating the reporting ofspeech/language impaired individuals in the SLladIhyp+
subgroup. Language irnpaired individuals rnay use pragmatic eues and strategies, similar
to leaming ofthe second language, to improve their observable perfonnance over time
(paradis & Gopnik, 1997). Nevertheless, it remains a possibility that the SLladl1lyp+
phenotype may represent an etiological subtyPe of SLI, cbaracterized by familial factors
common to attention deficitlhyPeractivity and speechllanguage disorders. This
hypothetical commonality could relate attention defieit and SLI through information
processing, as TallaI and coworkers (TallaI et al. 1991) also reported differences in
nonverbal auditory attention and processing, in addition to attention/hyperactivity
behavioral problems, between family history positive and negative SLI probands. It bas
been suggested that infonnation-processing deficits can eontribute to language
impairment in sorne children (Curtiss & Tallai, 1991).
85

•Increased Risk
The following limitations contribute to the preliminary character ofthis report.
Family history information is known to underestimate the rate ofaffected relatives
(Andreassen et al. 1977). First, our findings are based on the FH report on first-degree
relatives, which is generally more reliable than for extended relatives. Nonetheless, sorne
true cases might not have been reporte<!, and these cases might have been difTerentially
clustered in adlhyp negative families. Second, the presence or absence ofattention
deficitlhyperactivity in SLI children was based on the review ofMedical records
containing psychological and neurological evaluations, which is inferior to direct
examination. Thini, the consequence of increasing the stringency ofexclusionary criteria
by a requirement for pertinent medical record infonnation, which presumably improved
the reliability ofdiagnosis in SLI probands, was a reduction in sample size. The diagnosis
ofSLI was based on Medical records from difTerent clinicians with varying operational
measures, although major forms ofexclusionary conditions were absent in SLI children.
There was insufficient information to evaluate potential confounding effects ofage (the
SLIadlhyp+ probands tended to be older than the SLladlhyp- probands) or ofdifferent
speech/language phenotypes in SLI probands.
Conclusion
The present study, using 27 families identified through the parents from the
dysphasia association, provides preliminary evidence ofa higher risk ofspeech/language
disorders to first-degree relatives of SLI probands with attention deficit/hyperactivity
behavioral problems, than to first-degree relatives ofSLI probands without these
problems. Further study in a larger number offamilies, using direct assessment and
0Perational criteria for both speech/language disorders and attention deficitlhyperactivity
86
Increased Risk
is needed to corroborate this finding, and to examine the relationship between SU and
attention deficitlhyperactivity. Potential benefits offurther research on this aspect ofSLI
May include improved intervention strategies for this important common disorder~ and an
increase in power for genetic mapping studies, given the hypothesis that SLI with
attention deficitlhyperactivity might prove to he a more homogenous etiological
subgroup. The power for genetic mapping would he increased by the potentially higher
population relative risk Â. [the risk to relatives ofa given degree ofrelationship divided by
the population prevalence (Risc~ 1990a; Risch, 1990b)] for the first-degree relatives in
the SLIadJhyp+ subgroup than in the SLladlhyp· subgroup.
87
Increased Risk
AuthorNote
This work occurred within the multidisciplinary McGill University Genetic
Language Impairment Project (Myrna Gopni~PI) and was supported in part by an
Intercouncil Group Grant from the Medical Research Council ofCanada and the Social
Sciences and Humanities Research Council (M. Gopnik, Principal Investigator). Martha
Crago, Ph.D. and JoséeFo~ Ph.D. were co-investigators in the recruitment of families
described in this report. Additional support trom the Medical Research Council (MA
11663, GR-14501) is acknowledged. This work is in partial fulfillment ofthe
requirements of the Ph.O. degree (llija Kovac).
88
•
•
Increased Risk
APPENDIX
Family History Questionnaire
Is (s)he generally healthy? (Any Medical problems, mental retardatio~ hearing, or
psychological problems?)
At what age did (5)he start talkinglspeak tirst words?
Did/does (s)he have problems sayinglpronouncing words?
Did/does (s)he have difficulty pronouncing sounds?/mixes up sounds?/changes sooods?
Didldoes (s)he make shorter sentences than other persons hislher age?
Did/does (s)he speak slowly (<SO wordslmin)?
Didldoes (s)he have difficulty finding the right word to express hislher ideas (uses words
such as 'stuff', 'thing')?
Did/does (s)he have problems with plurals and the past tense?
Did/does (s)he have reading or writing problems?
Did/does (s)he have problems in school (needs special tutor or special education)?
If yes, since what age and for how long?
Didldoes (s)he have difficuIty pronouncing long words (>3 syllables, e.g. )?
Didldoes (s)he mix up sounds or syllables in long words?
Didldoes (s)he receive speech therapy?
Ifyes, what type, for how long, and since what age?
89

Commentary
Here we recapitulate some important issues, noted previously, that may influence
the ÏDterpretation ofthe data collected in the McGill University Genetic Language
Impairment Project These issues relate to the method for diagnostic assessment ofSLI
children, and bilinguality, which is commonly observed in examined families.
The diagnosis ofSLI in probands was indirect, based on the review ofMedical
records obtained from various hospitals and/or schools. Medical records originated from
different clinicians, which have used ditTerent diagnostic instruments and practices.
Consequently, variation in the phenotype ofSU probands is likeJy to he increased. This is
not the case in Many other studies ofStI, which report direct examination ofSU
probands with the single set ofoperational instruments and criteria, although, as noted
previously, these instruments and criteria vary somewbat between different studies (Rice,
Haney, & WexIer, 1998; Tomblin et al. 1997). We cao not detennine how much ofan
effec~ ifany, this limitation might have on presented results. However, the requirement
for specifie Medical record information regarding major exclusionary criteria provides
some assurance that the children who were retained cao he classified as SLI children.
Bilingualism was common in families recruited for presented studies, whereas in
other SLI studies families are often required to he monolingual (Riec & Oetting, 1993;
Oetting & Horohov, 1997). In part due to lack ofresearch, currently there is Jack of
diagnostic norms for bilingual SLI children comparable to those for monolingual SLI
90
children. Besicles ofadding some uncertainty in Medical record diagnoses, tbis might
pose an issue ofits own ifwe were in a position to perfonn direct diagnostic assessment
ofSLI children. With regards to direct linguistic testing performed in the present study of
sibliDg resemblance for specifie test components, native French speakers administered
French test battery to primarily francophone families, and native English speakers
adrnioistered English test battery to primarily anglophone families (Gopnik, personal
communication). Therefore, variation in test performance that might bave been caused by
unequal matching ofexaminer's and subject language between two language groups is
prevented. More generally, there is evidence that bilingual context does not impede
language therapy, and provides the advantage ofbroader social adaptation (Bruck, 1982).
ft is therefore ofboth practical and theoretical interest to add emphasis to research on
bilingual children with language disorders. Particularly, in areas such as Quebec where
bilingualism is the rule it May he difficult to gather a reasonable sample of language
impaired children from monolingual families; more importantly, bilingual children with
language disorders must not he neglected in research efforts that May facilitate more
appropriate treatments.
91

3. PHENOTYPE DEFINITION IN ALCOHOUSM
3.1. THE DIAGNOSIS AND ETIOLOGY OF ALCOHOLISM
Diagnosis ofAlcoholism
Alcoholism is a common disorder with substantial negative effects on individuals
and the society (Merikangas, 1990) and is therefore a subject ofextensive research. The
term "alcoholism" is widely used by the general public to denote repeated drinking of
ethanol-containing beverages followed by disruptive effects on individual and social
functioning. The DSM-IV makes a distinction between the alcohol dependence and
alcohol abuse (APA, 1994). The alcohol dependence category is focused on alcohol
seeking behavior, craving, tolerance and withdrawal. The alcohol abuse category is
focused on maladaptive alcohoI use manifested in adverse social consequences or
dangerous behaviors, i.e. driving while intoxicat~ without meeting the criteria for
diagnosis ofalcohol dependence. In addition ta DSM-IV, several other diagnostic systems
are used in recent alcoholism research, i.e. DSM-m-R, Feighner, ICD-IO (APA, 1987;
Feighner et al. 1992; WHO, 1992), resulting in partly concordant but partly discordant
diagnostic classifications (Schuckit et al. 1994). Calculation of the Iifetime prevalence of
alcoholism in the general population depends in part on the diagnostic system and
category, and estimates range from 5-14% in the United States (Kessler et al. 1994;
Myers et al., 1984; Robins et al., 1984). The National Comorbidity Study in the United
States reports lifetime general population prevalence ofDSM-m-R alcohol dependence
92
•
of 14.1%, with 20.1% in males and 8.2% in females (Kessler et al. 1994). Alcoholism is
comorbid with many other psychiatrie disorders, most notably antisocial personality
disorder and drug dependence, but also major depression, panic disorder, mania,
schizopbrenia (Heltzer" Pryzbeck, 1988; Kessler, 1997; Ross, 1995; Tomasson &
Vaglum, 1995).
Etiology ofAlcoholism
Family, adoption and twin studies suggest the importance ofboth genette and
enviromnental factors in the etiology ofalcoholism (reviewed in: Cotto~ 1979: Goldman~
1993; Merikangas, 1990; Prescott et al. 1994; Waldman & Slutske, 2000). Merikangas
(1990) reports, on average, a 7-fold increase in the risk to tirst-degree relatives of
alcoholic probands as compared to controls. While genetic influences in the nsL. for
alcoholism among women were initially not as clear as those for men (Preseau et al.
1994), more recent twin studies find evidence for substantial genetic influences on the
risk for alcoholism in women as well (Heath et al., 1997; Kendler et al., 1992) ThiS
could in part he related to the secular trend towards an increased frequency ofalcohollsm
in women (Reich et al. 1988; Stoltenberg et al. 1999), that might potentially contnbute to
increased expression ofvulnerability genes. In their review, Waldman and SIutsl~ (2000)
conclude that about 60% ofthe variation in risk ofalcoholism is due to genetlc
influences. Typical ofcomplex disorders, the mode of inheritance ofalcoholism 15 not
Mendelian.
Recent human and animal molecular genetic studies in alcoholism were reviewed
by Foroud and Li (1999). Genetic factors coosistently shown to influence alcoholism in
93
humans include polymorphisms in the ADH (alcahol dehydrogenase) and ALDH
(aldehyde dehydrogenase) genes, which are protective for alcoholism in Asian
populations. Most ofthe consumed alcohol is metabolized ta acetaldehyde, in part by
ADH, and the aceta1dehyde is then metabolized to acetate by ALDH The ALDH2*2
allele canfers a very low level ofaetivity ta the enzyme, and elevated levels of
acetaldehyde in carriers ofthis a11ele cause the aversive tlushing reaction whic~ at least
in some individuals, is a deterrent to excessive a1cohol consumption. Studies ofthe
ADH2*2 ailele also support the notion that this marker exerts a protective etTect (Foroud
& Li, 1999).
The implication ofADH and ALDH genes in alcoholism was facilitated by their
immediate funetional relationship to alcohol metabolism. This is not likely to he true for
most ofother susceptibility genes, whose effect may follow a more circuitous,
developmental pathway. Methodological advances in the genetic analysis ofcomplex
traits have facilitated numerous receot slodies. The most frequent analytical strategy by
far was the association study ofcandidate genes. The abstract search ofhuman studies in
the MEDLINE database (keywords "alcoholism" or "alcohol dependence" or "alcohol
abuse", and "gene") for the period January 1993-May 2000 identified 88 molecular
association studies using 28 candidate genes other than ADH or ALDH. Several, mostly
nonparametric linkage slodies ofcandidate genes were also identified in this search, sorne
ofwhich report association analyses as weil. Three studies from two whole genome scans
were identified (Foroud et al. 1998; Long et al. 1998; Reich et al. 1998). There is no
robust evidence identifying susceptibility loci for alcoholism, in contrast to the discussed
protective effects ofthe ADH and ALDH loci. The most promising candidate genes
94
modulate neurotransmission and are involved in other psychopathology as weil, i.e.
serotonin S-HTIB receptor (Lappalainen et al. 1998), tryptopban hydroxylase, TPH
(Nie1sen et al. 1998), GABA receptors (Buck et al. 1997), and the dopamine receptor,
DRD2. Evidence for the implication ofthis last locus is highly controversial, perhaps in
part due 10 an etfect that is restrieted to particular subsets ofalcoholics (Hill et al. 1999;
Noble, 1998). Candidate genes, Many ofwhich are indicated by QTL mapping in animal
models, are reviewed in Crabbe et al. (1999) and Goate & Edenberg (1998).
3.2. PHENOTYPES JN MOLECULAR GENETIC STUDIES OF ALCOHOLISM
Similar to other complex disorders, and behavioral disorders in particular,
defining the phenotype precisely is important for the statistical identification ofgenetic
risk factors in alcoholism (Foroud & Li, 1999; Hill, 1998; Schork & Schork, 1998). For
this purpose, the generic approaches outlined in Chapter 1 are applied in a1eoholism
research as weil. Following are sorne examples that illustrate phenotypie aPPl'oaches to
genetie analysis in alcoholism.
The P300 eomponent ofthe event-related brain potential bas been targeted in
genetie studies as a lower order phenotype, more umoleeular" than a clinical diagnosis,
and implicated in vulnerability to alcoholism as well as comorbid psychiatrie conditions
(Begleiter &, Porjesz, 1999; Begleiter et al. 1998). Another lower arder phenotype in
alcoholism May he a reduced level of response to alcohol, which implicated the 5HTI
and GABAA alpha 6 genes in a recent pilot study (Schuckit et al. 1999). Severity is also
used to narrow the phenotype definition for genetic studies. There is some evidence that
9S

part ofthe controversy surrounding the intensely studied DRD2 gene MaY relate to the
greater mIe ofthis gene in severe alcoholism, and the failure ta take this into account in
some studies (Noble~ 1998). Severe alcoholism with withdrawal seizures or delirium
tremens was associated to DATI and SHIT gene (Sander et al. 1997a, Sander et aL,
1997), and alcoholism with delirium tremens was associated with the CCK gene
polymorphism (Okubo et al. 1999).
Subtypes ofAlcoholism in Molecular Genetic Studies
Regarding subtypes ofalcoholism, discussed in more detail in the section 3 3 ln
this chapter, molecular genetic studies are presently focused on the early onset. antisocial
form ofalcoholism (Hallikainen et al. 1999; Kono, 1997; Lappalainen et al. 19Qq.
Lappalainen et al. 1998; Nielsen et al. 1998; Parsi~ 1999; PesoDen et al. lQ98.
Samochowiec et al. 1999; Sander et al. 1998). The rationale for this strategy stems from
the extensive literature documenting higher heritability ofthis pbenotype~ discussed
further below. A significant part ofthis research is conducted using the sample based on
Finnish violent., early onset (Virkkunen &. Linnoila, 1997) alcoholic male cnmmal
offenders (Hallikainen et al. 1999; Lappalainen et al. 1999; Lappalainen et al 1998.
Nielsen et al. 1998; Pesonen et al. 1998). Lappalainen et al. (1998) defined antisocial
alcoholism as DSM-ill-R alcohol dependence or abuse with a concomitant diagnosis of
antisocial personality disorder or intermittent explosive disorder. In the same study"
linkage to antisocial alcoholism (defined by antisocial personality disorder and alcohol
dependencelabuse) was alsa evaluated in the population ofSouth American Indians. In
both populations, linkage ofthe serotonin receptor fITR lB gene to antisocial alcoholism
96
was observed; there was no linkage ofthis gene to either non-antisocial alcoholism or the
combination ofantisocial and non-antisocial alcoholism (Lappalainen et al. 1998),
suggesting specificity ofthis genetic etTect. Nielsen et al. (1998) observed linkage of
tryptophan hydroxylase (TPH) to OSM-ID-R alcoholi~ although not in atTected sib
pairs; the evidence became stronger when alcoholics without ASP were analyzed. Other
studies used carly onset alcoholics, < 25 Yr. (Kono et al. 1997; Parsian, 1998), or
alcoholics with the ICD-I0 diagnosis ofASPD (Samochowiec et al. 1999; Sander et al.
1998). Candidate genes involved in neurotransmission (often involved in aggressive
behavior as weil) are putatively implicated in these studies, mostly by association:
monoamine-oxidase A, MAO-A (Parsian 1998; Samochowiec et al. 1999), serotonin 5
RTf transporter (Hallikainen et al. 1999), serotonin SLC6A4 transporter (Sander et al.
1998), dopamine receptor DRD2 (Kono et al. 1997). The late onset, less heritable subtype
ofa1coholism is not 50 intensely studied, i.e. Tiihonen et al. (1999) reported association
ofthe COMT gene with this subtype ofa1coholism.
Alcoholism and Phenotype in Genome Scans
The genome scan in the COGA subset ofdensely affected families (Reich et al.
1998) defined alcohol dependence requiring bath the DSM-III-R and the Feighner et al.
(1972) criteria. A genome wide study in an American Indian population (Long et al.
1998), environmentally and genetically more homogenous, and with a very high
incidence ofalcoholism (perhaps up to 80% in men and 50% in women) defined alcohol
dependence according to OSM-m-R criteria. A multivariate, statistically derived
phenotype was used in one analysis ofa recent genome scan within the Collaborative
97

Study ofthe Genetics ofAlcoholism, COGA (Foroud et al. 1998). The latent class
analysis, using Il symptoms ofalcoholism in families ofhigh-risk alcoholic probands,
identified 4 p(ogressively more severe classes, where class 4 was exclusively
charaeterized with withdrawal symptoms. The two MOst severe classes were combined ta
provide sufficient sample size for sib-pair linkage analysis, in which the strongest
evidence for a potential suscePtlbility locus was found on chromosome 16 (Foroud et al.
1998). These subjects were a subset ofthose ftom the previously noted genome-wide
study ofalcohol dependence (Reich et al. 1998). In the COGA sample, Begleiter et al.
(1998) condueted genome scan ofthe P3 event-related brain potential amplitude, a lower
order phenotype associated with alcoholism as ootOO in the beginning ofthis section.
3.3. MAJOR ASPECTS OF PHENOTYPIC HETEROGENEITY IN ALCOHOLISM
Subtypes ofAlcoholism
The variable presentation ofalcoholism bas been recognized for a long time,
resulting in attempts to classify alcoholics into more homogenous subgroups. Historical
review of39 typologies from the early scieotific literature in the period 1850-1941 cao he
found in Bahor and Lauennan (1983). Bahor and Dolinsky (1988) published a
comprehensive review ofthe typology literature since 1941. The eaclier typologies were
more intuitive, rather than resulting from systematic study. Sioce the 1950's, empirically
derived typologies based on statistical comparisons ofa priori tbeoretically derivOO
subgroups, or the a posteriori statistical derivation ofhomogenous subgroups in
multivariate analysis, have become common in the literature (Bahor & Dolinsky, 1988;
98

•
Hesselbroc~ 1983). Numerous variables ofdifferent types were used 10 classify
alcoholics, i.e. age, gender, patterns ofalcohol consumptio~ psychological measures
such as personality or cognitive ability, family history, psychiatrie comorbidity, biological
findings, educatio~ income, ete.
An overlap between classifications derived from different variables and
methodological approaches is noted (Bahor & Dolinsky, 1988; Hesselbroek, 1983). This
situation can he expected when alcoholism is viewed as a complex etiologica1 system
integrated by overlapping genetic and environmental etTects. A reœnt study reported
numerous cross.correlations hetween subgroups based on Il representative typologies of
alcobolism (penick et al. 1999). Ali typologies showed a degree ofclinical validity and
no one typology was clearly superior. Hence different typologies may he useful to a
degree, while remaining at least partly distinct, consistent with the view that ditTerent
classifications may need to he developed to tap information pertinent to different
purposes (Bahor & Dolinsky, 1988; Hesselbrock, 1983), i.e. various aspects oftreatment,
prevention, and researcb.
A widely accepted consensus from the extensive typologicalllterature is that two
broad categories ofalcoholics can be identified, with one showing earlier onset of
alcoholism, more psychiatrie comorbidity, increased frequency ofalcoholism and
comorbid psychopathology in biological relatives, greater severity, and poorer prognosis
(Bahor & Dolinsky, 1988; Penick et al. 1999). An overview ofMOst influential recent
typology research is presented below.
99

3. 3. 1. Early Onset and Late Onset Alcoholism
The age ofonset maintains a central position in delineating two broad subgroups
ofalcoholics throughout the past century ta present. An early typology, proposed by
Knight in 1937, descnbes the Essential and Reactive alcoholism (penick et al. 1990). The
Essential alcoholism had an earlier age ofonset ofabusive drinkïng, more severe
alcohoiism, no relation to environmental stressorslt and was linked 10 a positive family
history ofalcoholism, while the opposite pattern characterized Reactive alcoholism. This
broad distinction remains largely unchanged in various more recent fonnulations.
OperationaI Classification by the Age ofOnset
A particularly influential classification ofalcoholism was initially proposed in a
study ofadopted men by Cloninger et al. (1981), in a series ofmultivariate statistical
analyses. The more heritable Type 2 alcoholism showe~ in the biological father,
extensive treatment and characteristic combination ofearly-onset severe alcohol abuse
and severe criminality, no postnatal environmental effect on the frequency ofalcoholism
in sons, more severe alcoholism, and no alcohol abuse in biological mothers (Cloninger
et al. 1981). This etiological typology ofalcoholism from the adoption study was
subsequently transfonned into a proposai for explicit diagnostic Type 1 and Type 2
criteri~ to be applied to alcoholic individuals (Gilligan et al. 1988). Proposed criteria
included two elements: 1) age ofonset > 2S YT. for Type 1 alcoholism, or < 25 YT. for
TyPe 2 alcoholism; 2) two or more symptoms characteristic ofTyPe 1(benders, guil~
loss ofcontrol, cirrhosis) or Type 2 (inability to abstai~ fights while drinking, drunken
100

•
driving, treatment for alcohol use) alcoholism. In contrast ta this dichotomous proposai,
the same group also stated that Type 1and Type 2 should not he considered discrete
entities because many a1cohol abusers have some features ofeach type (Cloninger, 1987;
Sigvardsson et al. 1996). The latter view was supported in subsequent failures to classify
MOst alcoholics into either Type 1or Type 2 as per proposed criteria, due ta the presence
ofboth Type 1 and Type 2 features (Glenn & Nixon, 1996; Penick et al. 1990; Sannibale
& Hall, 1998). However, the 25 yr. age ofonset cutoft: without symptomatic criteria,
differentiated alcoholics along a variety ofclinical and biochemical measures (Glenn &
Nixon, 1991; Glenn & Nixon, 1996; Pennick et al. 1990; Von Knorring et al. 1985),
leading to the conclusion that Cloninger's classification primarily reflects the age ofonset
(Pennick et al. 1990).
The proportion ofsubjeets classified as early onset « 2S Yf.) can vary depending
on the theoretical construct whose onset is defined, i.e. 44% for "regular drunkenness
began" to 20% for "realized own problem" (parella & Filstead, 1988). These are
primarily self-reported constructs whose definition varies between studies. For example,
Glenn and Nixon (1996, 1991) used the age ofonset for the majority of7 symptoms,
Pennick et al. (1990) used reported age at which problems with alcoholism first began,
Von Knorring et al. (1985) used reported age ofonset ofsubjective drinking problems. In
addition, sorne investigators choose a different age cutot[ Buydens-Branchey et al.
(1989a, 1989b) defined early onset as excessive drinking before 20 yr., and Pennick et al.
(1999) defined early anset as the first experience ofany problems associated with
drinking before 24 yr. ofage. The onset ofalcoholism is a developmental sequence rather
than a discrete even~ and the earlier cutoff for excessive drinking might he comparable to
101
the later cutofffor subjective drinking problems, as the fonner stage precedes the latter
stage (Buydens-Branchey et al. 1989a; Parella & Fillstead, 1988). In summary, the
developmental nature ofalcoholism allows for varied conceptual and numerical criteria
for defining early and late onset alcoholism (parella &, Fillstead, 1988), within which two
broadly different subgroups ofalcoholics can he identified.
Age ofOnset and Major Recent Classifications ofAlcoholics
The MOst influential recent classifications (pennick et al. 1999) include
Cloninger's Type 1and Type 2 alcoholism (Cloninger et aL 1981), primary versus
secondary classification based on comorbid disorders (Schuckit, 1985), and a multivariate
empirical classification based on indices ofvulnerability and severity (Babor et al. 1992).
Cloninger incorporated bis original proposai ofType 1, late onset and Type 2,
early onset alcoholism (Cloninger et al. 1981), noted previously, into a more
comprehensive neurobiological theory ofalcoholism, including dimensions of
temperament (Cloninger, 1987; Cloninger, 1995). According to Cloninger (1987),
Novelty Seeking (NS) distinguishes individuals who are impulsive, exploratory,
excitable, distractible (high NS) and those who are rigid, refleetive, and attentive to
details (Iow NS). Harm Avoidance (HA) differentiates apprehensive, inhibited, shy,
cautious, pessimistic (high HA) from the confident, relaxed, optimistic, uninhibited and
energetic (low HA). Reward Dependence (RD) differentiates empathie, emotionally
dependent, sentimental, sensitive to social eues, and persistent (high RD) from the
socially detached, emotionally cool, praetical, tough-minded and independently self
willed (Iow RD). The Type 2 (early onset) alcoholies were proposed to he high in Novelty
102
•
Seeking, low in Harm Avoidance and Reward Dependence, and associated with antisocial
personality, while Type 1 alcoholies were proposed to show the opposite temperamenta1
pattern and an association with depression and anxiety (Cloninger, 1987; Cloninger,
1995). The Type 1 and Type 2 were not viewed as discrete entities, but as polar
prototypes on the continuum, acknowledging that combinations ofabove discussed
independently inherited temperament dimensions provide extensive heterogeneity in
behavioral predisposition to alcoholism (Cloninger, 1987; Cloninger, 1987b; Cloninger et
al. 1991; Sigvardsson et al. 1996; Svrakïe et al. 1993). In agreement with this complexity,
only high Novelty Seeking was consistently shown to prediet early onset abusive drinking
and discriminate antisocial alcoholies and persons with ASPD ftom their non-antisocial
counterparts (reviewed in Howard et al. 1997).
Schuckit (1985) detennined primary psychiatrie diagnoses in 541 men entering
alcohol treatmentpro~ ofwhom ail but two met criteria ofalcohol abuse and/or
dependence as per DSM-m and ROC. A primary diagnosis ofASPD (7.3%) was made
when individual met both the DSM-m and ROC criteria for definite or probable ASPD
before the age offirst major life problems due to alcohol or drugs. A primary diagnosis of
drug abuse (Il. 1%) was made when the first major life problem due to drugs preceded
the tirst major life problem due to alcohol. Primary affective disorder (1.7%) was
diagnosed when criteria for major affective disorder were met prior to the first major life
problem due to alcohol, or following an abstinence ofthree or more months. The
remaining 79.9% ofsubjeets were primary alcoholies. The age ofonset ofalcoholism was
defined as the age at which individual first met the alcoholism criteria stated above. The
age ofonset was lowest in primary drug abusers and primary ASPD subgroups (24.5 ± 5
103
•
and 25.0 ±6.8 yr. respectively), as opposed ta 36.6 ± 12.4 and 35.0 ± 10 yr. in primary
alcoholics and primary affective disorder subgroup, respectively. The early onset
subgroups had more depressioD and a higber frequency ofalcoholism, depression and
drug abuse among first-degree relatives.
Bahor and coworkers (1992) used cluster analysis to derive subtypes among 228
males and 85 females who met OSM-ID criteria for alcohol dependence (96%) or abuse
(4%). A total of 17 variables were used in the analysis. Premorbid risk factors were:
familial alcoholisrn, childhood disorder, bipolar character dimensions, and the onset of
problem drinking. Indices ofalcobol and other substance use were: quantity ofalcohol,
reliefdrinking, alcohol dependence severity, benzodiazepine use, and polydrug use.
Variables descnbing chronicity and consequences ofaIcoholism were: physical
conditions, physical consequences, social consequences, lifetime severity, and years of
heavy drinking. Psychiatrie symptoms were depression symptom count, antisocial
personality symptom count (DSM-llI), and severity ofanxiety. The 2-eluster solution,
Type A and Type B, was identified for bath genders (N = 107 and 121 respectively in
males, versus 53 and 32 in females). These types were differentiated on ail entered
variables in males and on 13117 variables in females (no difference for benzodiazepine
use, reliefdrinking, depressive symptoms and anxiety), as expected because c1uster
solutions were derived from these variables. Except for the age ofonset and years of
heavy drinking, the Type B had higher values ofditTerentiating variables (more
pathology) in bath males and females. The age ofonset ofproblem drinking for Type A
was 30.34 ± 9.80 yr. in males and 34.20 ± 10.50 in females, and for Type Bit was 21.70
± 5.36 in males and 21.46 ±4.59 in females. These authors have also validated obtained
104

•
elusters by examining variables that were not entered in the eluster analysis, namely
personality measures, drinking history, a1cohol..related consequences, and clinical ratings,
showing substantial differentiation betweeo the Type A and Type B (Babor et. al 1992).
In summary, the similarity between methodologically diverse classifications of
alcoholies a100g a number ofparameters ioeluding early onset ofalcoholis~antisocial
behavior and polysubstance abuse is striking, notwithstanding sorne differeoces in other
psyehopathology. For example, Penniek et al. (1984) found an association ofASPD and
depression in a study ofmale aleoholics, Babor et al. (1992) found an association
between depression and ASPD in male but not fernale alcoholics, and Hesselbrock et al.
(1984) did not find this association in either gender. These discrepancies cao he expected
because alcoholics with ASPD differ with respect to the presence ofother psychiatrie
disorders (Liskow et al. 1991). Overall, in both genders there is a subgroup associated
with the earlier onset ofalcoholism, childhood and adult antisocial behaviors,
polysubstance abuse, higher frequency ofalcoholism and comorbid psychopathology in
biological relatives, greater severity ofalcoholism and poorer prognosis, al least with
conventional treatments (Babor et al. 1992; Cloninger et al. 1981; Cloninger, 1995; Glenn
& Nixon, 1991; Hesselbrock et al. 1984; Kendler et al. 1998; Longabaugh et aL 1994;
McGue et al. 1997; Penick et al. 1984; Schuckit, 1985). Results ofthe exploratory factor
analysis in the comparative study of Il alcoholism typologies (Pennick et al. 1999) are in
agreement with these data. The following 3 dimensions, explaining 35°At ofvariance,
were suggested to account for significant overlap between alcoholism typologies: a) age
and age correlates including the age ofonset; b) "pure" versus psychiatrically
lOS

heterogenous alcoholism that encompasses antisocial personality disorder; c) current
severity ofpsychiatrie distress, impairment and dysfunction.
3. 3. 2. Alcoholism and Antisocial Personality Disorder
Association ofA1coholism and ASPD
In the Epidemiological Catchment Area (ECA) study in the United States,
antisocial personality disorder was the disorder most strongly associated with alcoholistn,
with the estimated odds ratio of21 (Helzer & Przybeck, 1988). The 15% ofmen and 10%
ofwornen with a lifetime diagnosis ofDSM-ID-R alcohol abuse or dependence a1so met
the diagnostic criteria for ASPD, compared to general population ASPD rates of4% in
men and 1% in wornen. Conversely, lifetime prevalence ofalcohol abuse of74% was
found among those with ASPD, compared to 14% in the general population (Regier et al.
1990). Similar results were obtained in the National Comorbidity Study, where only drug
disorders were more strongly associated with alcohol disorders (Kessler et al. 1994;
Kessler et al. 1997), as weil as in the epidemiological study conducted in Canada (Ross,
1995). Generally, the rates ofASPD are higher among alcoholics receiving treatment than
among those identified in the general population, i.e. ranging from 25-56% for men and
19-30% for women (Penick et al. 1988; Ross, 1989; Ross et al. 1989; Thomasson &
Vaglum, 1995). This is consistent with previously noted greater severity ofalcoholism
with comorbid ASPD, and the ASPD might a1so he a factor that facilitates identification,
and institutionalization in particular, for treatment ofalcoholism.
106

Longitudinal Studies
In accordance with the strong association between alcoholism and ASPD, which
by diagnostic definition includes childhood antisocial behavior, longitudinal studies have
found that childhood antisocial behavior prediets abusive drinking (reviewed in Zucker &.
Lisansky.<Jomberg, 1986). More specific longitudinal studies found that childhood
antisocial behavior predicts an earlier onset ofa1coholism (Cloninger et al. 1988~ Jessor
&, Jessor, 1975), consistent with the previously noted association between ASPD and
early onset alcoholism. Jessor and Jessor (1975) followedjunior high school students
(grades 7, 8 and 9) for 4 years, and found that generally deviant behavior (lying. stealing.
cheating, aggression) predieted an earlier onset ofdrinking in both boys and girls
Cloninger et al. (1988) followed 233 boys and 198 girls from a detailed behavloral
assessment at Il yr. to the age of27 yr., when abusive drinkers were identified from
Temperance Boards, drunken driving or other drinking arrests, treatment for alcohohsm
or its complications, or a psychiatric diagnosis ofalcoholism. Novelty seeking. raled
using teacher's interview report ofchildhood antisocial behaviors (e.g. overaCllvc.
disorderly, excitable, violent temper tantrums, obtrusive/disruptive... ) predicted abUSive
drinking in boys. The relative risk ofabusive drinking was 2.4 for boys high ln no\(el~'
seeking as compared to the total population. The faet that only 21198 girls were .denttfied
as abusive drinkers may relate to secular trends, which increase prevalence ofalcoholism
in more recent generations (Reich et al. 1988; Stoltenberg et al. 1999). Currently in
progress is a Michigan State University Longitudinal Study (Zucker et al. 1994)~ however
these subjects were only 9-11 years old at the last, wave 3 assessment (Leonard et al.
2000).
107
Family, Twin and Adoption Studies
Family studies examining the rates ofantisocial behavior in relatives ofalcoholic
adults (Amarlc~ 1951)~ the rates ofalcohol dependence in parents ofchildren with conduct
disorder (Stewart et al. 1980)~ or the rates ofconduet disorder in the otfspring of
aleoholic parents (Lynskey et al. 1994)~ found evidence for cross-transmission of
alcoholism and antisocial behavior. Twin studies provide evidence for common genetic
factors in alcoholism and conduct disorder or ASPD (Grove et al. 1990; McGue et al.
1992; Pickens et al. 1995; Slutske et al. 1998). Slutske et al. (1998) examined OSM-m...R
Iifetime diagnoses ofconduct disorder and alcohol dependence assembled from the
telephone interview in a sample of2682 twin pairs~ including males and females. Genetic
influences common to conduet disorder and a1cohol dependence accouoted for 17% and
35% ofthe genetic variation in Iiability to alcohol dependence in men and women,
respectively~ and for 11% and 23% of the totalliability variation in men and women~
respectively. On the other han~ adoption studies generally suggest that alcoholism and
antisocial behavior are genetically independent~ because there is no cross-trait association
between biological parents and their adopted away offspring (Cadoret et al. 1985;
Cadoret et al. 1987; Cadoret et al. 1995). This discrepancy could in part result from the
diminished power ofadoption studies to detect genetic covariation between traits in
comparison to twin studies (Slutske~ 1998; Waldman & Slutske~ 2000).
Symptomatic Behavioral Complexity ofthe Earlr Onset Antisocial Alcoholism
The data thus far suggest that alcoholism and ASPD share some proportion of
underlying genetic variance. Translation ofthis findiDg towards a phenotypic definition
108

useful for genetie mapping studies in alcoholism, however, is complicated by the
complex developmental nature ofthese disorders al the diagnostic level.
Variation along broad, genetically influenced Personality dimensions of
neuroticismlemotionality, extraversionlsociability and, especially,
impulsivity/disinhibition is related in various degrees to bath alcoholism and ASPD
(reviewed in Sher & Troll, 1994). Both ASPD and alcoholism are thought 10 he
composed ofat lcast two broad subtypes, the more psychopathie (impulsiveldisinhtbited)
and the more neurotie subtyPes (Sher & Trull, 1994), although individuals ean show
extreme levels ofboth impulsivity and neurotieism (MeGue et al. 1997). Loeher (1990)
distinguished the "Aggressivelversatile" Path leading to wide-ranging antisocial behavior,
with the onset in preschool years, and the '~onaggressive antisocial" l'8th leading ta
more specialized offending, with the onset in adolescence. At present, the DSM-IV
indirectly aeknowledges the heterogeneity ofASPD by subtyping conduct disorder (CD),
which is required for the diagnosis ofASPD, into the early onset «10 yr.) often
aggressive subtype, and the adolescent onset subtype (APA, 1994).
Failure to account for likely heterogeneity within the diagnostic category ofASPD
might hinder identification ofgeoetic risk factors whose common effect on ASPD and
abusive drinking is mediated by more specifie phenotypie components. Thus far, Most
studies examining the relationship between alcoholism and ASPD were oot designed to
take iota account potential heterogeneity with respect 10 the pattern ofspecifie antisocial
behaviors, employing instead piecemeal records information (e.g. Cloninger et al. 1981),
diagnosis ofASPD (e.g. Schuckit, 1985), or ASPD symptom count (e.g. Bahor et al.
1992; Zucker et al. 1994). A recent latent class analysis of38 ASPD and CD symptoms
109

was perfonned in a sample ofbigh-risk (strong family history ofa1coholism) alcoholic
probands (19.4%), their relatives (71.1%), and controls (9.5%) ftom the Collaborative
Study on the Genetics ofAlcoholism (COGA) group (Bucholz et al. 2000). Latent class
analysis is a categorical analog offactor analysis that identifies unobserved classes which
MaY he interpreted as discrete or as parts ofthe continuum, dePending on whether class
prevalences ofspecifie symptoms change abruptly or not (McCutcheon, 1987). The study
asked whether there are subtypes ofASPD with distinct symptom patterns.. and whether
certain ASPD symptoms are particularly strongly associated with alcohol dependence.
The results from both males and females supported the interpretation ofthe disorder
distributed on a continuum ofseverity (Bucholz et al. 2000). Among females. a 4-class
solution was obtained with OSM-ill-R lifetime conduet disorder and ASPD round almost
exclusively in the·most severe elass. Among males, a S-class solution was obtalned wilh
the highest prevalence ofASPD in the most severe class. The relationship of latent
classes to alcoholism, i.e. the age ofonset and prevalence ofOSM-m...R lifetime alcohol
dePendence, was largely consistent with generally observed carlier onset and Increased
prevalence ofabusive drinking in antisocial individuals. The non-representauvc
character ofthe analyzed population, intended to maximize the potential for genetlc
studies in alcoholism (requiring at least two affected first-degree relatives. among other
criteria), limits the generalizability ofresults (Bucholz et al. 2000). Moreover. a critlcal
assumption of latent class analysis is that within each class symptom frequencies are
statistically indePendent; therefore ail individuals are assumed to have an equal
probability ofshowing a certain symptom pattern calculated by multiplyjng symptom
frequencies (McCutcheon, 1987). In view of the familial charaeter and covariation of
110

•
ASPD and alcohol~ this assUlDption is ignored as Most ofthe analyzed individuals
were family memhers ofaIcoholic probands; they might therefore he more likely to show
a symptom pattern similar ta tbat found in the proband Also, family members are
expected to he similar but not identical ta the proband, and might therefore bias the
results towards a continuous solution by diminishing potential distinctions between
probands.
Kendler et al. (1998) applied latent class analysis to data from Temperance Board
Registrations in a sample of2505 male twins from the population-based Swedish Twin
Registries. Among other variables, the data included drunkenness, drunken driving, and
crime, and were thus less informative for specific patterns ofantisocial behaviors than the
data from above discussed COGA study (Bucholz et al. 2000). In contrast ta the COGA
study, the results showed qualitative ditTerences, particularly in causes of registration
noted above. The latent class with early onset o( and multiple, TBR registrations
(prevalence 30%), showed a distinctly strong endorsement for drunkenness, drunken
driving, and crime, as compared to 3 classes that strongly endorsed either drunkenness, or
drunken drivin& or crime.
The COGA study was not designed to examine the latent structure ofantisocial
behaviors among alcohol-dependent individuals. By definitioo, individuals affected with
a complex disorder such as alcohol dependence have a constellation ofrisk factors and
potential modifiers sufficient for the expression ofthe phenotype. This constellation may
influence antisocial behavior via the impact ofalcohol dependence, via the presence of
common genetic factors and lor through other means, 50 that the latent structure of
antisocial behaviors in alcohol-dependent individuals might not he the same as that found
111
in other populations. This latent structure is investigated in the present manuscript in
submission, entitled "Exploring Phenotypes in A1coholism: Unrestrieted Latent Class
Analysis ofAntisocial Bebaviors in Alcohol Dependent Males and Females with Diverse
Social Adjustment'7.
3. 4. SUMMARY
A1coholism is a complex and heterogenous behavioral disorder, sharing genetie
risk factors with antisocial personality disorder, among other phenotypes. Phenotypes,
and by extension molecular genetie mapping studies, in alcoholism did not take ioto
account potential differentiation with respect to the pattern ofantisocial bebavioral
symptoms amoog alcoholics, although some studies focused 00 violent alcoholics. The
literature documents substantial clinical and biochemical heterogeneity between the
early- and late-onset subgroups ofalcoholics. The first study in the present work explores
whether subgroups ofalcohol.dependent individuals with distinct patterns ofspecifie
antisocial behaviors can be empirically defined. The second study explores the impact of
stratification into the early- and the late-onset subgroups ofalcoholies on results ofthe
initial genome scan. These phenotype-oriented approaches might ultimately increase the
power for identification ofspecifie genetic effects.
112

3(8). EXPLORING PHENOTYPES IN ALCOROLISM: UNRESTRIcrED
LATENT CLASS ANALl'SIS OF ANTISOCIAL BEHAVIORS IN ALCOHOL
DEPENDENT MALES AND FEMALES WITR DIVERSE SOCIAL
ADJUSTMENT
The present chapter coosists ofthe following manuscript in submission, entitled
as above.
113
Exploring Phenotypes in Alcoholism: Unrestrieted Latent Class Analysis
ofAntisocial Bebavion in Aleobol Dependent Males and Females with
Divene Social Adjustment
ILUA KOVAC·, CHANTAL MERETI'E2, MIREILLE CAYER2
, LUCIE LEGAULT3,
MAURICE OONGIER3•4 and ROBERTA M. PALMOUR1.J.4,5
McGill University
Supported in part by grants from the Medical Research Council ofCanada, the National
Health Development Research Program and the Réseau Santé Mentale of the Fonds de
Recherché en Santé du Québec. This work is in partial fulfillment ofthe requirements for
the Ph.D. degree (I1ija Kovac).
Departments ofBiologyl, Human Genetics4, and Psychiatry5 , MeGiIl University,
Montreal, Quebec, Canada; Centre de Recherché Université Laval Robert-Giffard2,
Québec, Canada; Douglas Hospital Centre de Recherche3, Verdun, Québec, Canada
Correspondence to:
Dr Roberta Palmour
Department ofPsychiatry, McGill University, Allan Memorial Institute, Research and
Training Building Room 307,1033 Pine Avenue West, IDA lAI, Montreal, Quebec,
Canada. Tel. (514) 398-7303; Fax (514) 398-4370; E-mail: [email protected]
114

•
ABSTRACf
Backgroud. Perhaps the best accepted distinction with respect to helerogenous
suhtypes ofalcoholism is the early onset and antisocial alcoholism versus late onset
alcoholism. The present study, in the Montreal sample ofthe WHO-/SBRA Study ofState
and Trait Markers ofAlcoholism, formally examines whether subgroups ofalcohol
dependent individuals with distinctive patterns ofspecific antisocial behaviors can be
empirically dejined Metbods. An unrestricted latent class ana/ysis (LCA), inc/uding
gender and 15 antisocial behaviors expressed after 15yr ofage, was perjOrmed in 236
subjects (121 males and 115fema/es) with D8M-/Vdiagnosis ofa/cohol dependence;
subjects were ascertainedfrom clinica/ (690/6 ofmales, 30% offema/es) and general
population sources, andshowed a wide range ofsocial adjustment. Latent classes were
validated by comparing age ofonset fOr a/cohol dependence, frequency ofalcoho/icjirst
degree relatives, and other psychopalhology, us;ng a multivariate index ofchildhood
behavior obtained by independently conducting an LCA of12 conduct disorder
symptoms. Results. Evidence fOr 3 qualitative behavioral classes with potenlial
interpretative value was obtained: Social/y Adjusted Adu/ts (SM, N = 62, 23 males, 39
jema/es), Antisocial Non-Aggressive Adu/ts (ANAA, N = 138, 77 ma/es, 61 jémales), and
Antisocial Aggressive Adu/ts (MA, N = 36, 21 male, 15tema/es). The LCA ofchildhood
behaviors identified 3 classes comparable 10 adu/t classes. In bath ma/es and[ema/es, the
AM c/ass had the ear/iest age ofonsetfor a/cohol dependence (p=O.OOI), an increased
proportion ofalcoho/icfirst-degree relatives and an increasedprevalence ofo/her
psychopathology, whi/e the SM c/ass showed the opposite pattern. ln féma/es. the ANAA
115
c/ass was intermediate. ln ma/esfrom the ANM c/ass. socially adjusted chi/dhood
behavior differentiated the /ale onset subgroupfrom the intermediate onset subgroup.
CODelusions. The present multivariate exploration suggests a comp/ex structure of
qualitative hehaviora/phenotypes rather than continuous variation ofantisocial
behaviors among alcoho/-dependent individua/s. A bener understanding ofthe types of
heterogeneity in a/coho/ism mayfacilitate the identification ofrisklactors.
Keywords:
alcohol abuse, alcohol dependence, antisocial bebaviors, latent class analysis
RUDDing bead:
Latent Structure ofAntisocial Behaviors in Alcoholism
116

INTRODUCTION
There is presendy a broad consensus that elinically diagnosed a1coholism
represents a heterogenous condition (Bahor, 1994). Heterogeneity among alcoholic
individuals is likely to hinder not ooly treatment efforts (Longabaugh et al. 1994), but
also the detection ofspecifie geoes which might increase vulnerability 10 the disorder
(Lander and Sehor~ 1994). Alcoholism overail May he viewed as a complex etiological
system integrated by overiapping actions and interactions ofvarious genetie and
environmental effects. In this integrated eontext it is not surprising that altemate
typologies ofalcoholism variously based on parameters such as drinking patterns, family
history, PSychiatrie co-morbidity, psychological and physiological measurements, show
significant cross.correlations when relatively simple or multivariate empirical approaches
are employed (penick et al. 1999).
One ofthe best accepted facets ofdiiTerentiation (peniek et al. 1999) is
alcoholism associated with antisocial behaviors, i.e. criminal records, diagnoses ofASPD
(Antisocial Personality Disorder), and/or ASPD symptom count (Cloninger et al. 1981;
Peniek et al. 1984; Hesselbrock et al. 1984; Cloninger 1995; Schuckit, 1985; Schuckit et
al. 1986; Hesselbrock et al. 1985; Bahor et al. 1992; Longabaugh et al. 1994; McGue et
al. 1997; Kendler et al. 1998). This broad type ofalcoholism is charaeterized by an earlier
age ofonset, an increased ftequeney ofalcoholism in first-degree relatives, increased
rates ofdrug use and childhood behavioral problems, more severe alcoholism and
differenl treatment outcome. Although il was suggested that this type ofalcoholism, also
tenned Type 2 alcoholism, might he limited to males (Cloninger et al. 1981; Bohman et
117

al. 1981), early onset and antisocial alcoholism is found in females as weil (Hesselbrock
et al. 1984; Glenn and Nixon, 1991; Babor et al. 1992).
A recent study in a large sample oftwins suggested that genetic factors common
ta alcohol dependence and conduct disorder (a precursor ofASPD) account for 11% and
23% ofthe total variation in liability ta alcohol dependence in males and females,
respectively (Slutske et al. 1998). Struetured exploration ofspecifie signs and symptoms
may suggest distinct phenotypes whieh will ultimately permit detection ofmore specifie
vulnerability genes. The diversity ofspecifie antisocial behaviors is reflected in the
operational DSM·IV coding ofdifferent higher order criteria for ASPD, ineluding
unIawful behavior, deceitfulness, impulsivity or failure to plan ahead, irritability and
aggressiveness, recldess disregard for the safety ofselfor others, consistent
irresponsibility, and laek of remorse (APA., 1994). Neither the threshold diagnosis nor the
symptom count score capture the potential for ditTerentiation of individuals based on
variable patterns ofantisocial behaviors. Rather, a fonnal multivariate statistical model
that explicitly postulates such differentiation can he used to investigate novel phenotypie
definitions ofalcoholism with increased dimensionality, potentially allowing for more
meaningful interpretation.
In the present study, we use the information from the Montreal arm ofthe WHO.
ISBRA Study ofState and Trait Markers ofAlcoholism (Tabakoffet al. 1996) to conduct
exploratory analyses ofsubtypes ofalcohol dependent individuals derived from ASPD
symptoms, using the multivariate categorical technique of latent class analysis (LCA).
The LCA is intuitively similar to a quantitative factor analysis and postulates mutually
exclusive classes of individuals which best account for the observed frequencies of
118

•
bebavioral symptoms (McCutcheon, 1987). Under this assumption, we examined the
latent structure ofdiverse antisocial bebaviors among alcohol dependent males and
females showing a wide range ofsocial adjustment
SUBJECrS AND METHODS
Subjects
The WHO-ISBRA Study ofState and Trait Markers ofA1coholism is a
multinational investigation carried out in Australia, Brazil, Canada, Finland, Ja~
Sweden and the United States. Montreal is one of5 clinical centres in this project
(Tabakoffet al. 1996). Ali participating centres recruited approximately equal numbers of
male and female non-drinkers, light drinkers, heavy drinkers (reflecting alcohol
consumption in the last 3 months) and alcoholics in treatment in three equally
represented age groups: 18-29, 30-44 and 45-60. A total of297 females and 310 males
were reeruited in Montreal. Ali of these subjects were in good physical and mental health,
apart from possible alcohol problems, as determined by interview and physical
examination. Subjects sutfering trom major medical or psychiatrie disorders, and those
with a history of intravenous drug abuse were excluded. Written informed consent was
obtained from each subject.
The present exploratory analysis includes 121 male and 115 female subjects
recruited in the Montreal centre who met DSM-IV criteria for alcohol dependence in the
past year, regardless oftheir age group or drinking group. Among the 121 male subjects,
83 (69%) were recruited from a1cohol and/or drug treatment facilities (28 from the
119

detoxification clinic, 30 ftom the rehabilitation program and 25 ftom the combined
detoxificationlrehahiütation program) and 38 (31%) were identified ftom the general
population tbrough newspaper advertising. Among the 115 female subjects, 35 (30%)
were recruited ftom treatment settings (4 ftom the detoxification clinic, 11 ftom the
rebabilitation program, 20 ftom the combined program) and 80 (70%) ftom the general
population through newspaper advertising. Other diagnostic aspects ofaIcoholism and
demographic information are presented in the results.
Data collection
An initial telephone screening was carried out with subjects who had answered a
newspaper advertisement. The subjects considered suitable were given an appointment
for the interview, at which time a physical examination was perfonned and blood and
urine samples were callected. The subjects, except the alcoholics in treatment, were
provided with a 540 (eN) stipend at the end ofthe session.
Interviewers were trained in the use ofan instrument (The WHo-lSBRA
Interview Schedule), developed especially for this study by Bridget Grant and Boris
Tabakoff. Dr. Grant trained the initial group ofMontreal interviewers. A summary
description ofthe WHO/ISBRA Interview Schedule can he found in Tabakoffet al. 1996.
The kappa values for making a OSM-IV diagnosis ofalcohol abuse and dependence with
this instrument ranged from 0.60 to 0.80 (TabakotI: 1996). Overall, this struetured
interview instrument cantains 8 sections: Intake Screening, Recruitment Setting,
Background Information, Medical Conditions, Alcohol Consumption, Alcohol
Experiences, Substances and Personal History, and Family History section, with the latter
120
two sections including information on other psychopathology. The instrument required
between 30 minutes and 2 hours for completio~ depending on the subject's profile. A
diagnosis ofDSM-IV alcohol dependence in the past year was recorded by the selection
ofappropriate questions from the A1cohol Experiences section ofthe WHO/ISBRA
Interview Schedule.
Variables
Two sets ofbehavioral variables were used in latent class analyses (LCA).
Symptoms occurring after 15yr ofage (abbreviated here as ASPD symptoms) Of, ln a
separate LCA, before 15yr ofage (CD or conduct disorder symptoms) are described in
Table 1, and prevalence ofthese behaviors by gender is shown in Table 2. Thcsc
bebaviors were coded in the "Substances and Personal History" section ofthe
WHO/ISBRA Interview Schedule. Among ASPD symptoms, 3 variables pertalnlng to
childcare (not shown in Table 1) were not included in LCA because ofextremely low
frequencies « .01). In order to assess whether the ASPD symptom-based latent classes of
alcohol-dePendent subjects differ in other relevant aspects, we have contrasted extemal
variables (not included in the LCA ofASPD symptoms) between these classes. The
extemal variables we examined were: age, age ofonset for alcohol dependence.
proportion ofalcoholic first-degree relatives, childhood behavioral problems.. drug use.
lifetime depression, and anxiety. The age ofonset ofalcohol dependence was considered
to he the age at which symptoms first began to appear. First-degree relatives were
considered to be alcoholic ifthe infonnant could report that 80y of 18 alcohol-related
experiences had happened MOst days for at least a month, or intermittently for a few
121

•
•
Symptom
Adult behaviors(> IS yr.):
not working
absent from workquit jobtraveledno homeliedbillsstoledamagebun persanweaponscamunfaithfuIarrestcould he arrested
Childhoodbehaviors« 15 yr.):
hooky
suspendednmawayliedstoledamagefightsweaponhurt personhurt animaltirearrest
Table 1. Adult and Childhood Antisocial Behaviors
Description
were unemployed or out of school for 6 montbs or longer wben you shouJd bave beenworking or in schaolwere often absent from work or school for no goOO reasonquit 3 or more jobs without makïng plans to find other jobstraveled around from place ta place without making plans ahead oftimehad no reguJar place to live for a month or longertold a lot oflies or used a false name or aliasfailed to pay your bills or other financial obligations on a regular basismore than once stole things from your family or others (mcluding stores)damaged anotber persan's property on purposeinjured or burt ancther persan on purposeother than in combaty used a weapoo lite a ciuby knife or sun. in a fightscammed or conned someone for money or just for funnever remained faithfuI ta the same penon for longer than a yearwere arrested by the police for anything other tban a traffic violationdid anything you could have been arrested for even though you weren't caught (notincluding drunk driving)
did not go to schaol (played hooky) without a medical or other good reason for anentire day at least twice during one yearwere suspended or expeUed from schaolran away from home ovemight or longertold a lot ofliesmore tban once stole things from your family or others (including stores)damaged another persan's property 00 purposestarted physical fights with non-relatives 3 or more timesused a weapon (like a club, knife or gun) in a fightoutside offighting, injured or hun another persan on purposeinjurecl or hurt an animal on purposestarted a tire on purpose ta injure another penon's propeny or just to see it bumdid anything you were arrested for (mcluding going ta juvenile detention) or could havebeen arrested for even though you weren't caught
122
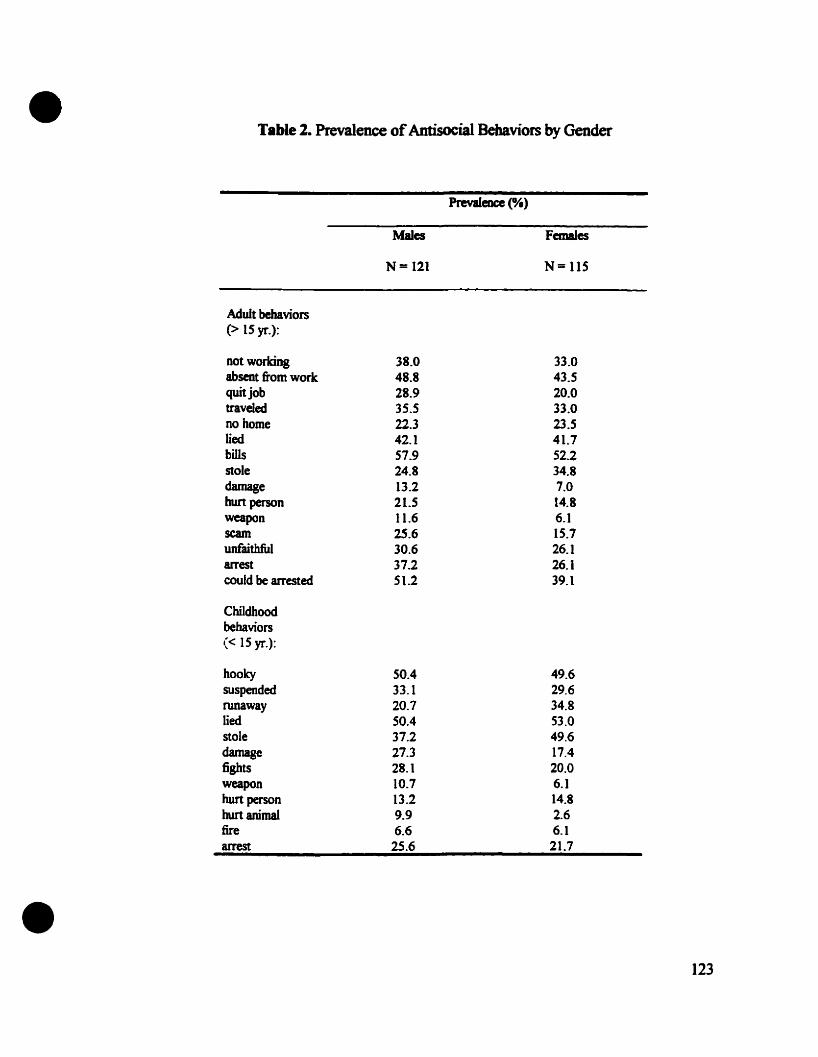
Table 2. Prevalence ofAntisocial Bebaviors by Gender
Prevaleoce (%)
Males Females
N= 121 N=1l5
Adultbehaviors(> 15 yr.):
ootworking 38.0 33.0absent from work 48.8 43.5quit job 28.9 20.0ttaveled 35.5 33.000 home 22.3 23.5lied 42.1 41.7bills 57.9 52.2stole 24.8 34.8damage 13.2 7.0hunperson 21.5 14.8weapoo 11.6 6.1seant 25.6 15.7unfaithful 30.6 26.1arrest 37.2 26.1could be arrested 51.2 39.1
Childhoodbehaviors« 15 yr.):
hooky 50.4 49.6suspended 33.1 29.6runaway 20.7 34.8lied 50.4 53.0stoIe 37.2 49.6damage 27.3 17.4fights 28.1 20.0weapoo 10.7 6.1OOn persan 13.2 14.8hunanimal 9.9 2.6fire 6.6 6.1arrest 25.6 21.7
123
months or longer. A multivariate index ofchildhood behavioral problems was obtained
by the LCA ofCD symptoms, conducted independently ftom the LCA ofASPD
symptoms. Drug use was defined as either psychoactive drug use (other than tobacco) in
the last 30 clays or having lifetime drug related problems. These variables were selected
because they can differentiate alcoholism associated with antisocial behaviors~ as
descnbed in the introduction. Wc bave also examined the distnbution of lifetime
depression and anxiety among latent classes, as potentially relevant ta suh-classification
(Del Boca, 1994}, as weil as the distribution of individuals with 3 or more CD ~mptoms.
Lifetime depression was coded positive ifsubject was 50 depresse~almost ail day cvery
day for 2 weeks or longer, that helshe couldn't carry on usual daily activities. Lifetlme
anxiety was coded positive ifsubject 50ugbt help for anxiety.
Latent C/ass Analyses (LCA)
The LCA is a multivariate statistical method for the analysis ofcategoncal data in
multi-way contingency tables. The latent class model postulates that observed symptom
frequencies can he explained by the categorical latent variable with mutually exclusive
classes~ within which observed variables are statistically independent (assurnpuon of
local independence). Parameter estimates of the latent class Madel include: class
membership probabilities at the level of the observed population which can he IOterpreted
as class frequencies; class membership probabilities at the level of individuals
conditiona] on the membership in a given class; and symptom endorsement probabilities
(SEPs) that reflect the probability of individual endorsing a SYmptom conditional on class
membership. The overall profile ofSEPs is characteristic for each class. The LCA
124
classification assigns the individual to the class for which hislher conditional probability
ofmembership is greatest. The model estimates oflatent class prevalences and SEPs
were very similar to the values observed on the basis ofLCA classification, bence only
the latter are presented in this report. Depending on whether SEPs change gradually or
abruptly across latent classes, the classes tan he respectively interpreted as pans ofthe
continuum or discrete, qualitatively ditTerent classes (McCutcheon, 1987). The relative
goodness-of-fit ofnested latent class models can he compared by a likelihood ratio 1: test
(McCutcheoD, 1987). While the use ofthis asymptotic chi-squared test is optimal when
expected cell counts are large, standard statistical method for sparse contingency tables is
not developed at present. The Akaike information criterion (AlC) was also used.
Exploratory latent class models, whereby all model parameters are estimated
without a priori restrictions, were fitted to 15 behavioral symptoms ofASPD and 12
behavioral symptoms ofCD (Table 1) in separate analyses using the LEM software
package for categorical data analysis (Vermunt, 1997). The LEM program uses the EM
algorithm to estimate latent class model parameters. The LCA ofCO symptoms was
performed to provide multivariate index for childhood behavior among ASPD symptom
based classes. We comPal'ed the relative fit of2· and 3 class models for ASPD or CD
symptoms in a sample of236 subjects (121 males and 115 females) who met OSM-IV
criteria for a1cohol dePendence in the past year, and showed a wide range ofsocial
adjustment. Geoder was included as a variable in the LCA. 80th 2 and 3-class models for
either ASPD or CD symptoms exhibited stable maximum likelihood solutions. Models
with more than 3 classes were not examined because the ftequency ofclass membership
in our moderate sample would decrease in the event ofa better model fi~ limiting the
125

•
ability ta examine further and interpret all classes. Usually, the structure investigated with
smaller data sets may he more complex than indicated even by the best-fitting model, and
large samples require more complex models to provide the best fit because they can
deteet smalt statistical effects which May, however, he oflittle practical importance
(Agresti, 1990). Therefore, interpretation oflatent classes need not always he based on
the absolute goodness-of-fit, but may consider the practical relevance ofrelative
goodness-of-fit in view ofpertinent knowledge (Bucholz et al. 1996). The 3-class
solutions in the present study provided the opportunity ta explore the latent structure of
antisocial behaviors in this manner.
Relationship ofLatent Classes to Alcoho/ism
Latent classes derived from ASPD symptoms were compared for extemal
variables relevant to alcoholism and described above. An overall association between
latent classification based on ASPD and CD symptoms was tested with the Pearson X2 test
for independence in a 3x3 contingency table. The linear association between CD and
ASPD symptom-based classes was tested using the Mantel-Haenszel X2 test for linear
association (Armitage & Berry, 1994). Due to unequal variances between classes, overall
tests across 3 ASPD symptom based classes for quantitative variables were done using
the X2 based Median test (Snedecor, 1956). Pair-wise comparisons between classes for
quantitative variables were done using the t-test, assuming equal or unequal variances as
determined by the 2-tailed f-test at the 0.05 significance level. Dichotomous variables
were generally tested using the Pearson 1: test, except where expeeted ftequencies
smaller than 5 were encountered; for these cases, Fisher's exact test was used. Most of
126

the pair-wise tests were performedpost hoc after the overall test was detennined to he
significant The exceptions were pair-wise comparisoDS for age, age ofonset ofalcohol
dependence, and proportion ofa1coholics first-degree relatives between male latent
classes characterized by non-aggressive and aggressive antisocial behaviors. These
comparisons were performed a priori because ofthe well-documented association of
violent behavior with male gender and Type 2 or highly heritable early onset alcoholism
(Virkkunen and Linnoila, 1997). In order to take into 8CCOWlt potential gender effects, ail
statistical tests were initially performed separately within the male and female subgroups.
Those variables that showed different results between gender categories are presented
separately for males and females, and remaining variables are presented in the pooled
sample.
A statistical examination ofmultiple latent classes necessitates multiple
comparisons. To reduce the inflation in the rate offalse positive results, we have limited
comparisons ofASPD symptom-based latent classes to several extemal variables deemed
MOst relevant from review ofthe literature as described in the variables section.
Furthennore, Many ofseleeted variables are correlated and hence the Bonferroni type
correction ofthe significance level would he too conservative. In this exploration we
opted to note ail results significant at the 2-tailed 0.05 level and discuss them in view of
relevant literature, referring to the 0.051evel as a tendency towards significance and 0.01
level as a significant difference.
127
•
RESULTS
AlI ofthe 121 male and 115 female subjects met DSM-IV criteria for alcohol
dependence in the past year. Most participants also met the DSM-IV criteria for alcohol
withdrawal (93% ofmales and 95% offemales) and alcohol abuse (86% ofmales and
79% offemales) in the past year. The DSM-m-R criteria for past alcohol dependence
(APA, 1987) were met by 89% ofmales (106/119) and 90% offemales (98/109). Male
and female subject groups were ofsimilar Mean age (males 36.1 yr, SD = 11.2; females
36.9 yr, SD = 11.9). The racial composition ofthe male and female groups was alsa
similar: predominantly white (94%), 2% black and 4% other. The distribution ofsocial
class based on the Hollingshead-Redlich index (Hollingshead & Redlich, 1958), recorded
in 106/121 males was 1-3%, II-Il%, m-270ÂI, IV-53%, and V-6%. Distribution ofmarital
status in males was 17% married, 12% living with a partner, 8% separated, 15%
divorced, and 49% never married. Similar distributions of social class and marital status
were observed in females.
LCA ofAdu/t Antisocial Behaviors
The latent 3-class model provided the best fit to the data on 15 symptoms of
ASPD in alcohol dependent males and females, among examined models (Table 3). The
observed Symptom Endorsement Probabilities (SEPs) in cach of3 latent classes are
graphically presented in Figure 1 (numerical values in the Appendix A). Class 1showed
either 0 or very low SEPs for ail symptoms, the highest being 0.07 for ubills'" and Unot
working" variables, and bence overall this class was tenned Socially Adjusted Adults
128

Table 3. LCA Model Fitting for ASPD Symptoms in Alcohol Dependenf
Males and Females
Madel -2 log-likelihood Ukelibood ratio 12 test
l-class 4377.26
p
2-class
3-class
3870.52
3675.79
506.74
194.73
17 (33 - 16) < 0.0000
10 (43 - 33) < 0.0000
-rndividuals who met OSM-IV criteria for alcobol dependence in the last 12 months. bNumber ofdegrees oftreedom equals the difference in the number ofparameters estimated by the n+1 class and the n-elass model;the number ofparameters estimated in the 3-c1ass model was reduced by the number ofconditionalprobabilities estimated at zero value (McCutcheon, 1987). The Aie aIso resulted in the 3-class solution.
129

0.0
..5 .6Eu~oe .4
UJESCo .2
~CI'.)
po
f
1 t
1
t1 ! l l~ 1 1.
0Class 1
(26.3%)
cClass2
(58.5%)
Class 3~
(15.2%)
Gender and Symptoms ofAntisocial Personality Disorder
Figure 1. Observed Gender and Symptom Endorsement Probabilities in ASPD Symptom
Based Latent Classes (N =236, 121 male, 115 female). Symbols (circles, squares, and
triangles) represent observed proportions of individuals who endorsed a particular
symptom in a given class. These observed symptom endorsement probabilities were very
similar to those estimated by the latent 3-class model, as noted in the methods section.
Horizontal reference lines are drawn at probabilities of0.25 and 0.75 for the sole purpose
ofvisual aid.
130
(SM). Relative to the SAA class, Class 2 bad higher SEPs for ail symptoms, the highest
SEPs in this class being for variables "absent from work" (0.55), "bills" (0.67) and "could
be anested" (0.52). While the SEPs for aU behaviors increased further in the Class 3, only
certain behaviors exlubited an abrupt increase ftom the Class 2 to Class 3. Specifically,
SEPs for variables "damage" and "weapon" increased from 0.05 and 0.04 in Class 2 to
0.47 and 0.42 in Class 3. The SEP for the variable "hurt person" increased from a low of
0.15 in the Class 2 to 0.58 in Class 3. Moreover, SEP for the variable "scam" a1so showed
an abrupt increase trom Class 2 (0.12) to Class 3 (0.92). In view ofthese SEP profiles,
Class 2 was termed Antisocial Non-Aggressive Adults (ANAA) and the Class 3 was
termed Antisocial Aggressive Adults (AAA). The frequencies oftheS~ ANAA and
AAA class were respectively 26% (62/236), 58% (138/236) and 15% (36/236). The SEP
values for male gender in the SM, ANAAA and AAA class were respectively 0.37, 0.56
and 0.58 (Appendix A). The rates ofalcoholics recruited from treatment (as opposed to
newspaper adds from the general population) in male SM, ANAA and AAA classes
were 87% (20/23), 71% (55/77), and 38% (8/21), respectively. Corresponding rates
among females were 44% (17/39), 26% (16/61), and 13% (2/15). These data in both
gender categories are consistent with the possibility that the most antisocial alcoholics
(MA c1ass) were less likely ta view their condition as socially undesirable and seek
treatmen~ instead being motivated to participate when otTered financial compensation.
LCA ofChildhood Antisocial Behaviors
The LCA ofCD symptoms~ conducted independently from the LCA ofASPD
symptoms, provided a multivariate index ofchildhood behavioral problems. Among the
131

•
examined models, a 3-class model again sbowed the best fit to 12 symptoms ofCD in
alcohol dependent males and females (Table 4). The highest SEPs observed in Class 1
were 0.15 and 0.18 for the behaviors "hook.y" and "lied" respectively (Figure 2,
numerical values for ail SEPs in the Appendix B). The SEPs for remaining bebavioral
symptoms ofconduct disorder in this class were either 0 or very low. The Class 1 overall
was hence similar ta the SAA class derived from ASPD symptoms, and was tenned
Socially Adjusted Children (SAC). As observed in the LCA ofASPD symptoms, the SEPs
for all symptoms were higher in each subsequent class. An abrupt increase in the SEP for
the variable "stole" was noted between the Class 1(O.OI) and either Class 2 or Class 3
(0.78 and 0.77 respectively). The variables "fights", "weapon" and "hurt persan" showed
an abrupt increase in SEPs between Class 2 (0.29, 0.08 and 0.15 respectively) and Class 3
(1,0.50, and 0.77 respectively). The SEPs for "damage" and, less frequent, "burt animal"
and "tire" symptoms also showed a greater iDcrease from Class 2 to Class 3 than from
Class 1 to Class 2. With respect ta the differences in SEPs for aggressive behaviors, these
two classes were broadly similar ta the ANAA and the AAA class derived from ASPD
symptoms. Therefore, Class 2 was termed Antisocial Non-Aggressive Children (ANAC)
and Class 3 was tenned Antisocial Aggressive Cbildren (AAC). The frequencies ofthe
SAC, ANAC and AAC class were respectively 45% (106/236), 46% (108/236) and 9%
(22/236). The SEP values for male gender in the SAC, ANAC and AAC class were
respectively 0.59,0.43 and 0.59.
132

Table 4. LCA Model Fitting for Conduet Disorder Symptoms in Alcohol Dependent
Males and Females
Madel -2 log-Iikelihood Likelihood ratio i test
l-class 3197.58
p
2-class
3-class
2737.55
2642.48
460.03
95.07
13 (26 - 13) < OOסס.0
8 (34 - 26) < OOסס.0
amdividuals who met OSM-IV criteria for alcohol dependence in the Iast 12 months. 'Number ofdegrees offteedom equals the difference in the number ofparameters estimated by the n+1 class and the n-class Madel;the number ofparameters estimated in the 2 and 3-c1155 models was reduced by the number ofconditionalprobabilities estimated at zero value. The Ale also resulted in the 3-class solution.
133

0Class 1
(44.901'0)
0Class 2
(45.8%)
.:. Class 3
(9.3%)
.l1
l(
j
1
( >0 ~
--.- --.-
·~- .8:Eas.&Je
Q..- .6clUelU~..0"0 .4c~
egc. .2e>.
ri)
0.0
1.0
Gender and Symptoms ofConduct Disorder
Figure 2. Observed Gender and Symptom Endorsement Probabilities in CD Symptom
Based Latent Classes (N = 236, 121 male, 115 female). The meaning ofsymbols is
explained in Figure 1.
134
Cross-tabulation ofAdult and Childhood Latent Classes
Cross-tabulation ofthe independently obtained latent 3-ciass solutions for
antisocial bebaviors after (ASPD) and before (CD) lSyr ofage, stratified by gender, is
shown in Table S. As might have been expeded, in bath male and female individuals
there was a significant overall association between these latent classifications. However,
only among females was there a significant linear association between adult and
childhood behavioral classes. The lack ofIinear association in males was main]y due to
the fact that most males in the adult ANAA elass (52%) belonged ta the SAC c1ass in
ehildhood (Table 5). Ofthese 40 males, 60% (24/40) had at least one behavioral
symptom ofconduet disorder. More than halfofmembers ofthe AAA class in elther
males or females did not belong to the analogous childhood AAC class, probabl~· due to
the small total number of individuals in the AAC class (Table 5).
Phenomenology ofAlcoholism in the SAA. ANAA and the MA C/ass
We compared adult latent classes for age, age ofonset for alcohol dependcnce.
and frequency ofalcoholic first-degree relatives. For all ofthese variables. difTerent
results were obtained in male and female subgroups and therefore results are presenled
separately by gender.
Tables 6 and 7 present comparisons ofthe SAA, ANAA and AAA class for age
and age ofonset for alcohol dependence, in alcohol dependent males and females
respectively. Age and age ofonset for alcohol dependence showed significant overall
association with latent classification in both males and females~ however the pattern of
ditTerentiation between latent classes within gender categories was somewhat different.
135

Table S. Cross-tabulation ofASPD and CD Symptom Based Latent Classes
Stratified by Gender
Percent (N) of Subjects in
ASPD Latent CI,,'''· (>1Syr)
Gender CD Latent Classes «15yr) SAA ANAA AAA X2 df p
Male SAC 83 (19) 52(40) 14(3)
ANAC 17 (4) 43 (33) 43 (9) 38.03b 4 < 0.0001
AAC 0(0) 5 (4) 43 (9) 3.421: 0.064
Female SAC 74 (29) 2S (15) 0(0)
ANAC 23 (9) 70(43) 67 (10) 46.9Sb 4 <0.0001
MC 3 (1) S (3) 33 (5) 22.901: <0.0001
·Symbols: SAA, Socially Adjusted Adults; AN~ Antisocial Non-Aggressive AduJts; AM.. AntisocialAggressive Adults; SAC, Socially Adjusted Children; ANAC. Antisocial Non-Aggressive Children; AAC,Antisocial Aggressive Children. bpearson X2 test for independence in the presented lx3 contingency table. 2-taiIed. 'Mantel-Haenszel X2 test for linear association between ASPD and CD latent classes, 2..tailed.
136

e
Table 6. Comparison ofLatent Classes Derived from ASPD Symptoms: Alcohol Dependentl Males
e
Variable
SAA
(N = 23)
ANAA
(N = 77)
AAA
(N = 21) Overall Test Statistic
n Mean sn n Mean sn n Mean sn x'1. df p
Age
Age of Onset for
23 39.74" 11.89 76 37.I3-c 10.87 20 26.9C 4.94 16.41 2 < 0.001
AJcohol Dependence 22 28.32" 8.32 71 25.2111.C 7.26 20 19.15e' 3.48 13.19 2 0.001
Due to unequal variances between groups. overall comparisons for quantitative variables were made with the non-parametric X2based median test. Pair..wisequantitative comparisons were made using the 2-tailed t..tests at the O.OS significance level. assuming equal or unequal variance as determined by the F tests at the0.05 significance level. For these pair..wise comparisons. in each group where applicable subjects outside of2SD trom the mean were excluded. Identical super..'script in a descriptive statistic for any two latent classes for a given variable denotes pair..wise comparison. Bold superscripts denote a priori pair..wise tests.performed before the overall test across 3 classes. Symbols: 81ndividuals who met DSM-IV criteria for alcohol dependence within the last 12 months. "Latentclasses: SM Socially Adjusted Adults; ANM Antisocial Non..Aggressive Adults;~ Antisocial Agressive Adults. "not significant at the 2..tailed 0.05 level.e'p < 0.001. t..test. 2-tailed.
137
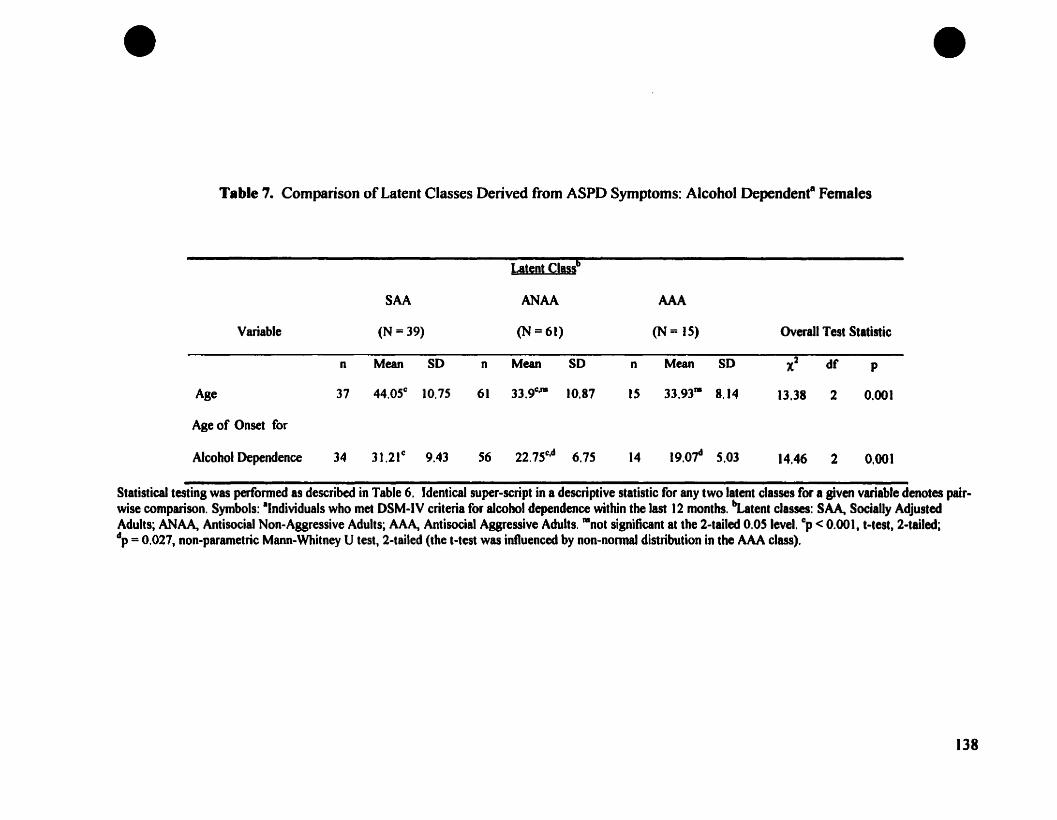
e
T.ble 7. Comparison oC Latent Classes Derived from ASPD Symptoms: Alcohol Dependent· Females
e
Variable
Age
Age of ORset for
Latent Classb
SAA ANAA AAA
(N =39) (N =61) (N = 15) Overall Test Statistic
n Mean SO n Mean SD n Mean SD x2 df P
37 44.05c 10.75 61 33.9c,- 10.87 IS 33.93- 8.14 13.38 2 0.001
)UcoholDependence 34 31.21c 9.43 S6 22.75c•d 6.75 14 19.0~ 5.03 14.46 2 0.001
Statistical testing was performed as described in Table 6. Identical super-script in a descriptive statistic for any two latent classes for a given variable denotes pairwise comparison. Symbols: Ilndividuals who met OSM-IV criteria for alcohol dependence within the last 12 months. butent classes: SM Socially AdjustedAdults~ ANM Antisocial Non-Aggressive Adults~ MA, Antisocial Aggressive Adults. Rlnot significant at the 2-tailed O.05level. cp < 0.001, t-test, 2-tailed;dp =0.027, non-parametric Mann-Whitney U test. 2-tailed (the t-test was influenced by non-nonnal distribution in the AM clus).
138

•
In males, the AAA class was younger and bad the carlier age ofonset ofalcohol
dependence (Table 6). As noted previously, in males 52% ofindividuals ftom the ANAA
class were members ofthe childhood SAC class, contnbuting ta the lack oflinear
association between childhood and adult classes. To investigate these individuals further,
we examined the ANAA class after stratification iota those who were members ofthe
childhood SAC class, N = 40, and the remainder, N = 37. The former subgroup was more
similar to the SAA class: the Mean age was 40.9 yr, SO = 10.8, and the Mean age ofonset
for alcohol dependence was 29.3 yr, SO =9.7. The latter subgroup had the Mean age of
33.7 yr, SO = 10.3, and the Mean age ofonset for alcohol dependence of24.2 yr, SO =
8.2. In females, but not males, the ANAA class was younger and had the earlier age of
onset ofalcohol dependence as compared to the SAA class (Table 7). A small nomber of
females from the AAA class showed a tendency (p < 0.05) towards lower age ofonset for
alcohol dependence than the ANAA class, notwithstanding similar corrent age (Table 7).
The respective proportions ofmales from the SM, ANAA and the MA class
who completed the FR report regarding first-degree relatives were 12/23,58/77 and
16/21. The frequencies ofalcoholic first-degree relatives ofmales from the SAA, ANAA,
and the AAA class were 0.31, (27/86), 0.26 (90/341) and 0.41 (23/56). There was no
significant overa11 association between the frequency ofalcoholism in first-degree
relatives and ASPD symptom based latent classification <X2 = 5.33, df= 2, p =0.07,2·
tailed). Ali ofthe 12/23 males from the SAA class who completed the FH report had at
least one alcoholic first.degree relative, and therefore the FH report for the SAA class is
biased towards higher frequency ofalcoholic relatives, contributing to the lack of
significant overall association. However, apriori comparison ofthe ANAA and the AAA
139

class showed a tendency towards a greater ftequency ofalcoholism among first-degree
relatives ofmales ftom the AM class (X2=5.09, df= 1, P = 0.024, 2-ta11ed).
The respective proportions offemales ftom the SAA, ANAA and the AAA class
who completed the FH report were 28139, 43/61, and 13/15. The frequencies ofalcoholic
first-degree relatives offemales trom these classes were respectively 0.27 (421158), 0.38
(73/193) and 0.44 (30/68). Overall, there was a tendency towards a significant association
between the ftequency ofa1coholism in first-degree relatives and latent classification (1..2
= 8.10, df= 2, P =0.017, 2-tailed). The increase in the ftequencyofalcoholic first-degree
relatives between the SM and the ANAA class approached significanœ <'1.2 = 4.98, df=
l, P= 0.026, 2-tailed); there was no significant difference between the ANAA class and
the small AAA class in this respect <1..2 = 0.83, df= 1, P = 0.36, 2-tailed).
Psychopathology in the SM, ANM, and the MA C/ass
Table 8 presents psychopathology in latent classes derived from ASPD symptoms.
Similar statistical results were obtained within gender categories and in the pooled
sample, and therefore only the pooled sample is presented. The strong association with
membership in the childhood MC class further supports distinct character ofthe AAA
class, which is not apparent when only the count of3 or more CD symptoms is
considered (Table 8). The frequency ofdrug use behavior increased progressively across
latent classes. Depression and anxiety were not significantly associated with the present
latent classification, suggesting that these factors do not account for observed differences
between latent classes. The overall proportions ofmales and females with lifctime
depression were respectively 40% and 57%, and overall proportions ofthose with anxiety
140

Table 8. Psychiatrie Co-morbidity in ASPD Symptom Based Latent Classes
Perœnt (N) of Subjects in
ASPP Latent a,,'O· (>1Sm
Variable
SAA
(N = 62)
ANAA
(N= 138)
AAA
(N=36) df
CD 3+ symptoms 19 (12) 54 (74) 89 (32) _c
AAC d 2 (1)- 5 (7)fa.e 39 {14t 44.54 2 <0.001
DrugUsl 31 (19)' 67 (92r 100 (36)b 49.35 2 <0.001
Lifetime Depression S5 (34) 43 (60) 53 (l9) 2.62 2 0.27
80ugbt Help for Anxiety 31 (19) 32 (44) 47 (l1) 3.40 2 0.18
AlI statistical tests used ratios '''yeslno'' and were initially performed in males and females separately withresuJts similar to those presented here in the pooled sample. Identical superscript for any two latent classesfor a given variable indicates pairwise comparison, performed after the significant overall test. lLatentcla.;ses: SAA, Socially Adjusted Adults; ANAA, Antisocial Non-Aggressive Adults; AM AntisocialAggressive Adults. bpearson X2 test ofindependence in 2x3 contingency table (variable yes/no x latentclassification). cnus variable is shown for descriptive purposes. dAntisocial Aggressive Children from theLCA ofCD symptoms. "not significant at the 2-tailed O.OS leve~ FlSher's exact test. cp < 0.001, Fisher'sexact t~ 2-tailed; fUsed drogs in the last 30 days and/or had lifetime problems with drugs. 'x2 = 22.48. df=l, P < 0.001, 2-tailed; bX:Z = 16.3, df= l, P < 0.001, 2-tailed.
141

were 21% and 47010 respectively. This is consistent with higher prevalence ofthese
disorders in alcoholic women (De1Boca, 1994).
DISCUSSION
The latent class analysis ofASPD symptoms (behaviors after 15 yr ofage) among
alcohol-dependent individuals, showing a wide range ofsocial adjustment, provided
evidence for 3 qualitative behavioral classes [Socially Adjusted Adults (SAA. N =62.
37% males), Antisocial Non-Aggressive Adults (ANAA, N = 138,56% males), and
Antisocial Aggressive Adults (AM, N = 36,58% males)], ratherthan continuous
variation along the severity dimension. Male and female subgroups were similar "1th
respect to size, demographic characteristics and present and past diagnoses ofalcohol ism.
The increased proportion ofmales in the ANAA and the AAA class is consistent Wlth the
well-established higher prevalence ofASPD in alcoholic males (Hesselbrock et al 1984:
Babor et al. (992). Failure to find a Iinear association between analogous. independently
obtained childhood « 15 yr) and adult classes was observed only in males. and 15
discussed below in greater detail.
While the AAA class showed higher symptom endorsement probabilitles (SEPs)
for ail antisocial behaviors than did the ANAA class, the endorsement ofoven a~'1'e5sive
behaviors increased abruptly, suggesting that aggressive behaviors may he substanuvely
independent from other antisocial behaviors. An abrupt increase in the endorsement of
certain behaviors is more consistent with the presence ofqualitative ditTerences between
classes rather than purely continuous variation (McCutcheon, 1987). The distinctive
142

character ofthe MA class is further supported by the strong association with
membership in the aggressive childhood (AAC) class, in agreement with the DSM-IV
recognition ofthe aggressive early onset subtype ofCD (APA, 1994). These tindings are
consistent with the view that aggressive bebavior may he an important indicator of
heterogeneity within the ASPD diagnostic category (Byudens-Branchey et al. 1989;
Loeher, 1990; Sher and Trull, 1994). In addition, the endorsement ofscamming bebavior
also increased abruptly from the ANAA to the MA class, suggesting some commonality
between this trait and overt aggressive behaviors. The ANAA class had the greatest
endorsement for being repeatedly absent from work for no good reason, regularly failing
to pay bills, and exhtbiting behaviors that are grounds for arrest. The antisocial latent
classes obtained might therefore also he interpreted to be largely congruent with the
DSM-IV ASPD criterion of"consistent irresponsibility" for the ANAA class, and most of
the DSM-IV ASPD criteria including "irritability and aggressiveness" and "deceitfulness"
for the AAA class (APA, 1994).
To our knowledge, the present study is the first to ask whether there were
subtypes ofalcohol-dependent individuals based on the LCA ofspecific sytnptom data
for ASPD. The recent LCA ofASPD symptoms conducted in the COGA sample asked
different questions, including whether there are subtypes ofASPD, and whether specific
s}'mptom patterns are associated with alcohol dependence (Bucholz et al. 2000). The
COGA population, which was analyzed, comprised high-risk alcoholic probands
identified from treatment (19.4%), their biological relatives (71.1%), and controls (9.5%).
The COGA sample is not representative, which limited the generalizability ofthe results
(Bucholz et al. 2000). Moreover, inclusion offamily members in the LCA could
143
presumablyobscure potential distinction between probands, thus introducing a bias
towards the concluded continuum ofseverity for ASPD symptoms. Because the latent
structure ofASPD symptoIDS among alcohol-dependent individuals is not necessarily the
same as in other populations, the differences in questions posed and populations analyzed
limit the comparison ofthe present latent class solution with that presented in the COGA
study. Nevertheless, it is ofinterest ta note that the COGA male class D bas a mild
childhood behavioral profile, but an antisocial adult profile, and is thus similar to the late
onset subgroup ofmales from the ANAA class in the present report Although this
subgroup ofANAA males showed milder childhood and adult behavioral profiles than
did the COGA class D, both results support the nosological separation ofchildhood and
adult antisocial behaviors. The category ofprimarily adult antisocial behavior is not an
unexpected finding in populations with substantial substance abuse (Cottier et al. 1995),
due to the negative impact of this behavior on social adjustment.
Compared to the LCA oftemperance board registrations in male twins that
included drunkenness, drunken driving and crime (Kendler et al. 1998), the slodies cited
above used bath males and females and a richer range ofbehavioral infonnation. Kendler
and colleagues found evidence for qualitative latent classes, as did the present study. The
LCA ofsymptoms ofalcohol dependence in the COGA sample ofrelatives produced a
continuum ofseverity (Bucholz, 1996). The exception was the most severe class 4,
which was characterized by withdrawal syndrome as per OSM-ill-R criteria for
withdrawal, requiring shakes and one other withdrawal symptom (Bucholz, 1996).
Almost all ofpresent subjects displayed a1cohol withdrawal by OSM-IV criteria, which
144
•
•
do not obligatorily require shaking (APA, 1994). These subjects might therefore ditTer
somewbat ftom the class 4 subjects in the COGA population.
In the present study, adult behaviorallatent classes were validated in relation ta
alcoholism by contrasting variables that were not iDCluded in the LCA. Barly onset
alcoholism is associated with antisocial behavior in both males and females, and is alsa
characterized by a lower age ofonset for a1cohol dePendence, more frequent and
aggressive problem behaviors in childhood, increased drug use, and an increased
frequency ofalcoholic first-degree relatives (Cloninger et al. 1981; Penick et al. 1984.
Hesselbrock et al. 1984; Cloninger 1995; Scbuckit,.1985; Hesselbrock et al. 1985. Glenn
and Nixon, 1991; Bahor et al. 1992; McGue et al. 1997; Kendler et al. 1998). In bath
males and females, the AAA class had the cbaracteristics ofthe early onset alcohol tsm.
while the SAA class had the characteristics ofthe late onset alcoholism. Current age dld
not account for other charaeteristics ofearly onset alcoholism in sorne studies (Babor ct
al. 1992; McGue et al. 1997), and there was insufficient statistical power for analysas
stratified by corrent age in the present study. Although there is heterogeneity ln the
criteria used by different investigators to identify early and late onset alcoholics. the
intensely studied sample ofFinnish male aggressive alcoholics is similar in many respects
to the male AAA class identified in the present report (Virkkunen and Linnoila. 1997)
The present exploration could therefore he interpreted as providing sorne addluonal
support for the utility ofthis Finnish subgroup in alcohol research. ln females. bUI nol in
males, the ANAA class aiso displayed an early anset aicoholism in cornparison to the
SAA class~ although to the less extreme extent than the AAA class. ln males~ rnembers of
the ANAA who belonged to the sociaUy adjusted chiidhood class had the late onset of
145
•
•
alcohol dependence, presumably in part mediating exhibited adult antisocial behavior,
while the remaioing ANAA males had intermediate onset. This is consistent with
longitudinal studies linking childhood antisocial behavior ta an earlier onset of
alcoholism (Jessor and Jessor, 1975; Cloninger et al. 1988). The facilitation ofantisocial
behavior by drinking could contribute to documented higher frequency ofthese behaviors
in male alcoholics, noted before, and the overrepresentation ofmales in treatment, as the
rate ofASPD is higher among alcoholics ascertained from tteatment (Waldman and
Slutske, 2000).
There are a number of limitations to the present study. Although collected using a
carefully prepared interview instrumen~ the data represent self-reports rather than
objective measures and have substantial retrospective charaeter. The sampling ofequally
represented age, drinking and gender categories in the WHO-ISBRA project might have
influenced the generalizability of results. The family history report was not completed by
aIl subjects. The population was predominantly white, providing little information
pertaining to other races. The moderate total sample size required that a joint LCA of
males and femaIes he condueted, including gender as a variable, in order to accommodate
a relatively large number ofanalyzed symptoms, and bas limited comparative analysis to
3 latent classes. The total sample size, however, is comparable to that used in the bulk of
alcoholism research to date, hence the observed variation could perhaps he MOst readily
related to accumulated knowledge. The size of latent classes, particularly the AAA class,
decreased after stratification by gender. Nevertheless, we deemed it useful to retain the
AAA class because of important features (i.e., aggressive behaviors), distinguishing these
subjects from the socially maladjusted subjects in the ANAA class. In view ofstatistical
146

power, we were only able to use those secondary variables deemed highly relevant to
validate latent classes in relation ta subtypes ofalcoholism reported by others, rather than
perform more extensive exploratory analyses. Moreover, multivariate analyses with a
single data set provide a broader margin for statistical artifacts. Tbese limitations
underline the requirement for the replication ofthe PreSent LCA solution in an
independent sample.
In conclusion., the present empirical analysis identified discontinuous latent
classes in a broadly ascertained sample ofalcohol-dependent individuals, evaluated from
a multidimensional behavioral perspective. These potential discontinuities MaY he of
particular interest for genetic mapping studies, which are currently focused around the
concept ofearly onset antisocial alcoholism (parsian 1999; Nielsen et al. 1998;
Lappalainen et al. 1998). In future studies, attention to patterns ofalcohol consumption
and to genetically intluenced personality and character traits that May constitute risk
factors common to antisociality and alcoholism, [e.g., behavioral disinlubition., novelty
seeking, uncooperativeness, etc. (Cloninger, 1987; Sher and Trull, 1994; Cloninger, 1995;
Howard et al. 1997; Waldman and Slutske, 2000)], as weil as to other symptoms of
psychopathology, cao provide better insight ioto the phenotypes suggested in the present
exploration. It will he possible to address some ofthese issues, as weIl as sorne of present
limitations, in the large international WHO/ISBRA sample (n - 3000), ofwhich alcohol
dependent subjects from the Montreal centre studied here are a part. However, an
independent replication study in a representative sample ofalcobol dependent individuals
is needed to confinn the present findings.
147

Appendix A. Symptom Endorsement Probabilities Observed in Latent Classes ofAlcohol
Dependent Individuals Derived ftom Behavioral Symptoms ofASPD
(After 15yr ofAge)
Symptom SAA- ~ AAA
N=62 N=138 N=36
male gender 0.37 0.56 0.58
Dot working 0.07 0.34 0.92
absent from work 0.06 0.55 0.83
quit job 0 0.23 0.72
traveled 0 0.40 0.72
no home 0 0.28 0.44
lied 0.02 0.48 0.89
bills 0.07 0.67 0.94
stole 0.02 0.28 0.83
damage 0 0.05 0.47
hurt persan 0.02 0.15 0.58
weapon 0 0.04 0.42
scam 0 0.12 0.92
unfaithful 0.03 0.32 0.58
arrest 0.05 0.30 0.83
could be arrested 0 0.52 0.97
-Utent classes:S~ Socially Adjusted Adults; ANAA. Antisocial Non-Aggressive Adults; AMAntisocial Aggressive Adults. Behavioral symptoms ofASPD are descnDed more extensively in Table 1.
148

AppeDdiI B. Symptom Endorsement Probabilities Observed in Latent Classes ofAlcohol
Dependent Individuals Derived from Behavioral Symptoms ofCD
(Before ISyr ofAge)
Symptom SAC- ANAC MC
N== 106 N= 108 N=22
malegender 0.59 0.43 0.59
hooky 0.15 0.74
suspended o.os 0.44
runaway 0.07 0.40 0.68
lied 0.18 0.75
$laie 0.01 0.78 0.77
damage 0.04 0.28 0.86
fights 0.04 0.29
weapon 0 0.08 0.50
hurt person 0 0.15 0.77
hurt animal 0.01 0.07 0.27
tire 0 0.08 0.26
arrest 0.01 0.35 0.77
-Latent classes: SAC, Socially Adjusted Children; ANAC, Antisocial Non-Aggressive Children; AAC,Antisocial Aggressive Children. Behavioral symptoms ofconduet disorder are described more extensively inTable 1.
149

BridgiDg CommeDary
Regarding the preœding manuscri~ a very recent report including latent class
analysis ofantisocial behaviors in the sample of7326 male and fernale subjects from the
National Longitudinal Survey ofYouth (Muthen &. Muthe~ 2000) may be relevant. The
analysis identified 4 classes, in which SEPs for "tÏghting" were 0.09, 0.53, 0.20, and 0.74,
trom class 1 to 4 respectively. Because the SEPs did not increase gradually aeross classes
as they did for sorne other symptoms, e.g. shoplifting, the authors suggest that the results
May ref1ect different kinds ofantisocial behaviors, rather than a single dimension of
increasing severity. However, the differences between the population anaIyzed in this
paper, and our own population, preclude direct comparison ofthese results with the study
presented here.
In view ofthe frequent use ofbasic latent class analysis with likelihood ratio
testing to evaluate the number of latent classes in psychiatrie research, for instance
Bucholz et al. (1996) or Sullivan et al. (1998), it is of interest to note pertinent views
from the perspective ofstatistical theory. White latent class models cao he viewed as
nested models, they are nested in a way that does not meet certain assumptions ofthe
likelihood ratio test statistics (Vermunt, 1997a; Uebersax, 2000). Rather, the use ofmore
"heuristic" approaches, such as the model parsimony measure Akaike Information
Criterion (AIC), is more appropriate (Uebersax, 2000). In the present study, the AIC,
calculated as -2 log likelihood plus 2 tintes the number ofparameters, resulted in the
latent 3-class solutions as did the likelihood ratio test: the AIC value decreased from the
150

l-class to 3-class solution for both the ASPD and CD symptom based analyses. An
alternative, computation...intensive approach involves simulation ofdata sets by Monte
Carlo, bootstrapping, or sunilar methods (Aitken et al. 1981; Langeheine et al 1996).
Rejection ofmodels in which sorne latent classes have low prevalences, which is often
necessary to allow interpretation of latent classes, cao also he viewed as a criterion for
model selection (Uebersax, 2000). This often occurs when a relatively large number of
indicator variables (symptoms) are analyzed in a comparatively small sample, as is the
case in the present study or the study ofBucholz et. al. (1996). In addition to removing
indicators ofvery small frequency, as was done in the present study, another option for
improved overall model fitting might he to remove indicators that are conceptually
redundant. However, this would invariably involve a degree ofarbitrariness, because a set
ofad hoc criteria for redundancy would need to he devised in the absence offonnal rules.
For a complex behavioral disorder ofunknown. etiology, it is particularly difficult to
decide which symptoms to retain. Indee~ one ofthe important goals is to identify
relationships between symptoms that might not he self-evident. Additionally, like any
other classification, modal classification (assignment of individuals to the MOst probable
latent class membership) is subject to some enar; here this occurs because ofnon-zero
probabilities for alternative class membership. In the present study, the expeeted
proportion ofclassification errors due to modal assignment (Vermunt, 1997) for the LCA
ofASPD symptoms was -0.05, and -0.04 for the LCA ofCD symptoms.
The present, exploratory latent class analysis specifically examined whether
variation in symptom patterns can he viewed as continuous or discrete in arder ta infonn
genetic studies in this particular regard, and it is therefore a descriptive study. More
151

elaborate~ explanatory questions can also he examined in multivariate categorical data
sets. Where this is the~ a study design can include a derivation ofthe meaningful
explanatory hypothesis prior to testing it in multivariate models; alternatively, the study
May generate an explanatory hypothesis from the multivariate analysis. Multivariate
hypothesis-generating design may be a valuable option for complex disorders in
particular, where simple research designs may he poorly suited to capture underlying
complex relationships. Sorne madeling possibilities include using gender as a grouping
variable to examine causal hypotheses, using properly justified a priori model restrictions
rather than exploratory estimation ofail parameters, and simultaneously USiDg separate
latent variables for childhood and adult symptoms where data cao support the iDCrease in
the number ofparameters. For example, the logliDear modeling capabilities ofthe LEM
software allow for direct modeling of latent class parameters and the use oflatent classes
as response or predictor variables, without the use ofmodal classification (Vermun~
1997). A major statistical development that allowed examination ofnumerous
explanatory hypotheses, enabling incorporation ofexternal variables into causal models
with categoricallatent variables, was a "modified LISREL approach" (Hagenaars, 1993).
This method is named after the LISREL model that brings together factor analysis and
regression analysis into one structural model for continuous data. Presentation of
structural-modeling techniques is outside ofthe scope ofthis wor~ but is explicated in
the references herein, particularly Hagenaars (1993), and Uebersax (2000) for cunent
developments in latent class modeling, and additionalliterature.
152

The following manuscript is based on the data from to Collaborative Research
Group on Genetics ofAlcoholism (COGA), wbich were distributed ta participants orthe
Genetic Analysis Workshop (GAW) Il, held in Arcacho~France, 1998. The GAW is
held at regular interva1s with the goal ofaddressing methodological issues in genetic
epidemiology. On each occasion a different theme is chosen, with an appropriate
simulated or real data set to stimulate participants contributions.
The manuscript explores the eifect ofstratification into early- and late-onset
subgroups ofalcoholics on results from the initial genome scan. It is not directly related
to the preceding manuscript, except that the early-onset subgroup is likely to have
charaeteristics sunilar to those round in the socially maladjusted classes. Agam, because
comparable data are not available, precise comparisons cannot he made.
In addition, this manuscript explores the impact ofphenotype definition that
includes either alcoholism or smoking, or both, in the '~affeeted" category. Besides ather
substance abuse, a strong association exists between alcoholism and smoking. The
incidence ofsmoking among alcoholics in treatment often exceeds 70% (Bobo, 1992;
Gulliver et al. 2000). The population prevalence ofsmoking is declining (Bobo, 1992;
Bergen & Caporaso, 1999), and the 1987 National Health Survey suggested prevalences
of31.7% for men and 26.8% for women in the United States (Fiore et al. (989). Twin
studies document genetic influences on smoking behavior in bath genders, with
heritability ofabout 50% (reviewed in Rossin& 1998). Twin studies have also suggested
presence ofgenetic factors common to alcoholism and smoking (Swan et al. 1996; True
et al. 1999). This finding is weil supported by extensive human and animalliterature
documenting commonality in physiologjcal pathways ofaddictions to different
153
substances ofabuse; i.e. the activation ofthe dopaminergic mesolimbic pathwayand the
increase in brain dopamine levels are reward mecbanisms common to alcobol7 nicotine7
cocaine7 amphetamines (reviewed in Koob7 2000). However, the researcb interest in the
genetics ofsmoking bas lagged behind the interest in the genetics ofalcoholism
(Kozlowski, 1991). There are some controversial reports about the potential role ofthe
dopamine DRD2 receptor gene variants in smoking (Bierut et al. 2000; Spitz et al. 1998).
Potential candidate genes for smoking are reviewed by Rossing (1998)7 and Many of
those are also candidates for alcohol related phenotypes.
The following is a description ofthe COGA data set relevant to the present
manuscri~ which was provided by COGA investigators to participants ofthe GAWI1 7
and May help familiarize the reader with the study background
"Description ofCOGA Data for GAW Il:
The Collaborative Study on the Genetics ofAlcobolism (COGA) is a six--center
program to identify and map genes that increase susceptlbility to develop Alcohol
Dependence and related phenotypes. In order to ascertain infonnative families for the
study ofgenetic linkage, approximately 1261 probands with alcohol dependence were
selected from inpatient and outpatient treatment units. Families were required to have
three or more available sibs (including the proband) ifboth parents were a1so available.
Four or more sibs were required ifone or both parents were missing or unavailable. The
proband could belong either to the otIspring or parental generation. At least two relatives
were required to live in the catchment area ofa COGA center. Probands were not
included in the study ifthey were uncooperative, were positive for the mv virus, were
intravenous drug users, had a fatal iUness or were unable to participate in the protocol.
154
•
•
First-degree relatives were personally interviewed and administered a personality trait
inventory (N-8996 adult interviews) and families with three or more affected members
(alcohol dependence) were selected for genetic linkage studies. Bilineal families were not
included Children age seven and older were interviewed (N-1309) as weil as adults.
Nuclear families were extended either by ascertaining second and third-degree
relatives through affected members ofthe primary family or by leapfrogging over an
unaffected individual into a branch ofthe family tbat included affected members
(ascertained by history). Members ofthe extended branches ofthe families were
measured with the same protoeol that was used to cbaracterize the densely atTected
nuclear families. Bilineal branches were not ascertained
The data set to he distnbuted for GAWll ineludes 105 pedigrees with 1214
members. Nine...hundred and ninety-two members have been genotyped and ofthese 970
have been interviewed using the adult assessment protoeol. A subset ofthe interviewed
adults (813) also successfully completed the personality trait assessment. Twenty-two
individuals have been genotyped and did not receive the adult assessment protocol and 13
individuals have been assessed but were not genotyped. Six hundred and seven
individuals in103 families were assessed in COGA neurophysiology laboratories.
Two hundred and ninety-six markers, with average heterozygosity of0.73, have
been typed at an average intermarker distance of 13.6 centimorgans. Allele frequencies
have been estimated with the USER MI3 program (M. Boenke) and the program
CRIMAP (p. Green) bas been used ta estimate marker arder and distances. The affected
status ofAlcohol Dependence requires a positive diagnosis ofAlcohol DePendence by
the DSM m-R criteria ofthe American Psychiatrie Association and definite Alcoholism
155

by the Feighner Criteria This is referred to as the COOA criterion for alcohol
dependence.
A semi-structured interview for the lifetime assessment ofpsychiatric and alcohol
related psychopatbology was developed for this program. The SSAGA (Semi-Structured
Interview for the Assessment ofthe Genetics ofAlcoholism) makes diagnoses in multiple
diagnostic systems, assesses alcohol consumptio~ enquires about hannful use ofalcohol
and enables age-at-onset to he measured. Lifetime cigarette smoking is also measured. A
test-retest reliability study conducted betwecn and within COGA sites attested to the
reliability ofthe lifetime diagnosis ofalcohol dependence.
Personality traits are assessed with the Tridimensional Personality Questionnaire
(TPQ) developed by Cloninger and associates. It bas been found to he heritable and its
scales have been correlated with the lifetime diagnosis ofalcohol dependencc.
There are 228 independently counted alcohol dependent affected sibpans ID these
data using COGA criteria. Individuals are categorized as unaffected if they dnnk but have
no symptoms ofalcohol dependence or abuse (Number of unaffected sibpairs = 30)
The Collaborative Study on the Genetics ofAlcoholism (COGA) (H. Beglelter~
SUNY HSCB, Principal Investigator, T. Reich, Washington University~ Co-Princlpal
Investigator) includes six ditferent ecnters where data collection takes place. The six
sites and Principal Investigator and Co-Investigators are: Indiana University (l
Numherger Jr., T.-K. Li, P.M. Conneally, H. Edenberg); University of Iowa (R. Crowe9
S. Kuperman); University ofCalifornia at San Diego and Scripps Institute (M. Schuckit't
F. Bloom); University ofConnecticut (V. Hesselbrock); State University ofNew Yor~
Health Sciences Center at Brooklyn (B. Porjesz, H. Begleiter); Washington University in
156

St Louis (T. Reic~ C.R. Cloninger, J. Rice). This national collaborative study is
supported by the National Institute on Alcohol Abuse and Alcoholism (NIAAA) by
U.S.P.H.S. grants NIAAA UIOAA08401, UIOAA0S402, UIOAA08403."
157

3(b). EXPLORING THE IMPACf OF EXTENDED PHENOTYPE
IN STRAID1ED SAMPLES
Aeknowledgement
The following manuscript, entitled "Exploring the Impact ofExtended Phenotype
in Stratified Samples" by Dija Kovac, Eric Rouillard, Dr. Chantal Mérette, and Dr.
Robena Palmour, is published in the journal Genetic Epidemiology 17(Suppl 1): S211
8216, 1999. Copyright © (1999 Wiley-Liss, IDe.). Reprinted by permission ofWiley-Liss,
me., a subsidiary ofJohn Wiley &. Sons, Ine.
158