information standards governance process information ... resource grouper... · information...
TRANSCRIPT

INFORMATION STANDARDSGOVERNANCE PROCESS
INFORMATION STANDARDFINAL PROPOSAL
FOR NEW OR CHANGED INFORMATION STANDARD
Exploration of Updating the HRG Grouper fromversion 3.5 to version 4
16th April 2009

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 2 of 32
INFORMATION STANDARD FINAL PROPOSALFOR NEW OR CHANGED (INCLUDING RETIRED) INFORMATION STANDARD
This document should be completed using theGUIDANCE ON COMPLETING THE “INFORMATION STANDARDFINAL PROPOSAL NOTIFICATION” SUBMISSION TEMPLATE
REVISION HISTORYDate of this revision: 3rd April 2009
Versionno.
Revisiondate
Summary of Changes Changesmarked
1.0 03/04/09 First version N/A
SUBMITTED BY:
Document completed by: Mark Bowling
Role & organisation: Programme Manager, Financial Information Strategy (FIS),Programme Management Unit NHS Wales
FEEDBACK TO BE PROVIDED TO:Feedback will be provided on the Proposal within 10 days of the WIGSB meeting. If the feedback is to bedirected to another nominee please provide the name and contact details below.
Name: Mark Bowling
Email: [email protected]
SUBMISSION PURPOSEProposal submitted for: Formal Approval

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 3 of 32
SECTION 1: BACKGROUND
1. Information Standards Reference Number [From Information Services Division]IGRN 2008 / 021
2. Name of Information Standard
Exploration of Updating the HRG Grouper from version 3.5 to version 4
3. Type of changea) Introduction of new standard – as current version (HRG v3.5) predates the WIGSB process.
4. Type of standard [Select all that apply]a) Operational
5. IntroductionThe Healthcare Resource Grouping system is a type of classification with highly aggregatedcategories to which episodes of care may be assigned according to several attributes which havealready been classified, such as operation, disease, co-morbidity and age.
NHS Wales has used a grouping system since 1996, introducing HRGs in April 2000. The currentHRG version (v3.5) was introduced in October 2003, subsequently being used within Wales fromApril 2005. Since this time the Information Centre for Health and Social Care in England has workedwith various stakeholder groups (with significant clinical involvement) to fundamentally redesign theHRG approach, adopting their new version (v4) from April 2006, as did Northern Ireland.
This proposal is to explore and then, if justifiable, upgrade the HRG grouper to v4 within NHS Wales.Some of the key drivers from an information perspective will be explored further and evidenced as thereview progresses, these include:
o Procedure Coding. Despite NHS Wales updating to OPCS 4.4 the software to group for HRGv3.5 is based upon OPCS 4.2, hence OPCS codes get converted back two versions prior togrouping. Therefore the benefits (including 25% more codes and reflections of more recentclinical practice) are lost and could represent a significant wasted effort.
Following England’s development of OPCS to issue 4.5, Scotland and now Wales have alsoimplemented with effect 1st April 2009. During exploration it emerged that one encoding softwaresupplier (Simplecode) cannot provide a conversion back to OPCS 4.2, therefore at Trust level thesystem for two Trusts can no longer deliver HRG v3.5with effect from 1st April 2009. In light ofOPCS 4.5, further work is required at a national level to ensure that ePEDW can still deliver HRGv3.5 during 2009 / 10.
o Use of HRG data. Two complaints from the service in Wales have been a need to segregatespecialist from more routine activity and that, whilst modernised practice is moving away fromtraditional settings, reporting software can only describe the traditional Admitted Patient Caresettings.o HRGv4 has reportedly been developed to not only reflect complexity/specialist services, but
also provides a better reflection of age/complications and/or LOS which may address theformer. Some of the factors in increasing from around 600 to 1,400 codes.
o It has also developed the concept of ‘setting independence’ of the HRGs themselves, byreflecting care and not focusing upon the setting in which it takes place.
o Future updates to existing HRG grouping software. HRG grouping software is produced andmanaged by the Information Centre in England. As they have moved to HRG v4 their final v3.5reference cost grouper update was published January 2008. Therefore a method / mechanismwould have to be derived to implement any further grouper or coding (e.g. OPCS 4.5) changeswithin NHS Wales.
o Service Line Reporting / Patient Level Costing – whilst some organisations in Wales wereexploring developing these forms of system. The Director of Resources, WAG, wrote to all Trusts

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 4 of 32
and has since received plans detailing how each will deliver Service Line Reporting from the firstquarter of the 2009 / 10 financial year. All have noted Welsh Reference Cost data, includingHRGs, as a key source of benchmark to deliver these reports. A brief note of these projects isincluded at section 9.
o Generating Spell HRGs. An earlier project, Acute Activity Currencies for Commissioning /Costing was established to implement Hospital Spells as a commissioning currency. Theenvironment of NHS Wales has changed but that project has delivered the ability to generateFCEs, Campus Spells and Trust Spells from Welsh data. Two available methods to utilise thisand achieve HRGs at spell level are:o Additional grouping software for HRG v3.5. As the grouper was designed to group on the
basis of finished consultant episodes (FCEs) each FCE within a multi-episode spell will beindependently processed to generate an individual HRG. NHS England developed someexternal grouping software to then assign spell based HRG, based largely upon selecting thedominant FCE and based upon their definition of spell. In light of this the Acute ActivityCurrencies for Commissioning / Costing project recommended a review of HRG v4.
o Implement HRG v4. As it has been specifically designed around generating spells and cangenerate an appropriate spell HRG that may not appear within the underlying individual FCEHRGs, to better reflect the complexity and resource consumption of the overall spell.
6. SponsorSteve Elliot, DHSS Head of Finance (Hospital Resources), Department of Health and Social Services,WAGTel: 029 20823245 e:mail: [email protected]
7. Developer
Mark Bowling, Programme Manager, Financial Information StrategyTel: 029 20207604 e:mail: [email protected]
Project Team and other key support acknowledged at Appendix A
8. IImmpplleemmeennttaattiioonn DDaatteeThis project has been divided into two key phases. The first exploring the potential benefits of NHSWales upgrading to HRG v4, which this report concludes. If accepted the proposal is to implement at anational level during the summer of 2009. A further project to co-ordinate Trust level implementation maybe required – advice from the Board being specifically sought on this point.

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 5 of 32
SECTION 2: BUSINESS JUSTIFICATION
9. Purpose
The proposal seeks to evaluate an upgrade to HRG v4 from three perspectives and in doing so evidencea business need. The three perspectives are:
o Clinical. In exploring whether HRG v4 achieves a better reflection of modern medicine, identifyingbenefits to clinicians that could include benchmarking and evidencing individual’s consultant contractperformance.
o Acute activity currency. Contrasting the HRG v3.5 and HRG v4 methods of spell derivation asnoted above. As well as the potential to more accurately describe the care taking place.
o Performance Management. Acknowledgement that specialty itself is not an effective service lineand, specifically through link to clinical engagement, use of HRGs could help to drive efficiency. Thepotential expansion into other areas of clinical delivery beyond APC (acknowledging that this wouldrequire the capture and coding of activity in these areas). The requirements and links between HRGand Performance Management are becoming clearer, specifically as organisations move to developService Line Reporting for 2009 / 10.
Although all are at a project implementation stage is it clear that they share several factors:
All have a key focus in achieving clinical engagement, whilst still early all have clinicians engagedin the project to deliver this solution for the respective Trusts. One project being led by two seniorclinicians.
All will utilise the annual reference costs (including HRGs) at least in part, if not the whole of theirfinancial comparisons for benchmarking purposes.
Of those that have assisted with this project HRG version 4 has demonstrated a superior analysisof specialist and tertiary services (please refer to section 16).
Risks of not undertaking exploration. Please see drivers for change noted in Introduction sectionabove.
10. ScopeAssumptionso The use of a casemix tool in NHS Wales is desirable.
o A HRG v4 upgrade can be achieved through implementation at a national level, with or without localimplementation.
o There is an assumed desire to remain with HRG as the casemix tool, based upon:o Perceived cost, training requirements and possible resistance if changed.o As other home nations (England and Northern Ireland) utilise HRG and a key factor during the
Acute Activity Currencies for Commissioning / Costing review was to be able to benchmark, bothhistorically and within the UK.
NHS Service / Business Area CoveredAt present HRGs are specifically generated by HSW for WAG / NHS Wales corporate purposes and localTrust levels for annual costing returns and in some cases further utilised for benchmarking andcommissioning purposes #. Through Service Line reporting and Patient Level Costing projects it isexpected that both scope and usage at Trust level will significantly increase. Being principally utilised byservice planning, finance and information staff, although some clinical engagement/usage is present.
# The Acute Activity Currencies for Commissioning / Costing review found that in all cases the principlebasis for commissioning was at a specialty level –a simpler aggregation of patient data. Although specificreviews have then utilised HRGs to sub-analyse a particular issue.
Specific Exclusions from Scope

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 6 of 32
o This project is limited to exploring the benefits of upgrading the HRG version and will not explore therelative merits of other casemix grouping systems used internationally.
o The project will review the potential benefits upon existing data and hence range and method ofactivity coding within NHS Wales at present. Therefore specifically recognising the exclusion of anyfurther OPCS or ICD upgrades and any additional coding of activity in areas not presently covered ata Trust level.
11. FFuunnddiinngg
At a national level Health Solutions Wales participation was agreed via their 2008 / 09 service levelagreement with WAG. At this point in time, 2009 / 10 work has been submitted for their 2009 / 10 SLAagreement with WAG and is presently under consideration.
At a Trust level the impact assessment survey indicates a cost ranging from zero to £15,000 for localimplementation. Although it should be noted that a limited number of responses were received fromthose organisations included within the impact assessment process.
WIGSB Members should note that this proposal will deliver a robust national solution at no cost to Trusts,as they will merely be required to continue the same processes, and then the national solution will providethe derived version 4 HRG(s).
12. SupportLetters of support for the exploration of updating the grouper have been received from:
o Steve Elliot, Head of Finance, Department of Health and Social Services, WAG (Sponsor)o Kerry Ashmore, Information Modernisation and Development Manager, and Hywel Jones,
Principle Finance Manager – Costing and Benchmarking, both of Cardiff & Vale NHS Trust
These letters are attached at Appendix B. Representatives for each of these interested parties areinvolved in the project itself.

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 7 of 32
SECTION 3: HEALTH INFORMATION STRATEGIC AND OPERATIONAL FIT
13. Strategic FitThis proposal links to the wider NHS strategic aim of ensuring that there is consistency of data for costingand activity volumes. It will also facilitate the provision of analysis across the patient pathway, providingan opportunity to combine the information gleaned from various datasets. This will ensure a coherent longterm approach to information collection and provision.
Further, as per the drivers for this proposal noted in the introduction, some specific aspects for NHSWales include:o Costing – significant attention through Financial Information Strategy haso Service Line Reporting has been specified for all Trusts, HRGs underpin their proposed solutions but
there are notable risks in retaining version 3.5:o NHS Wales is reliant upon England who no longer support / upgrade version 3.5o Trusts have noted a desire to segregate specialist activity and expand into non-traditional
settings. Work on specialist data has proven elements of this segregation for both the Cardiff& Vale and Abertawe Bro Morgannwg NHSTs.
o An assumption that, whilst not specified at this point, spell and/or FCE based comparisonswould be required. One aspect of this project has been to prove that spell generation issuperior under version 4.
o OPCS upgrades have taken place but this is not reflected in the resultant HRGs.o NHS Wales already has version 3.5 and this is integrated into PAS systems, as well as being
submitted and generated nationally. In light of risks of remaining at version 3.5 as well as benefits ofmigrating to version 4 it is proposed that the upgrade to version 4 takes place.
With regard to the recent public engagement exercise around the future restructuring of the NationalHealth Service, it was considered relevant to continue exploration and development of this InformationStandard. The proposed data standards will not be affected by any organisational restructuring.
14. Operational FitHRG v3.5 is already populated by Trusts on local PAS systems. This data is then submitted to HSW,who independently generate a HRG v3.5 which is then utilised for the population of e-PEDW. Where aHRG v3.5 is not present in the submitted data the derived HRG is substituted for analytical purposes.The initial implications for upgrade to HRGv4 have been summarised via a project issue submission,attached at Appendix C. This highlights the differing data definitions between Wales and England and theimpact upon HRGv4.
Admission and Discharge differencesSources of admission and discharge errors were caused in the test data by the additional Welsh fieldsthat England do not have, many are related to the generation of Campus and Trust spells from Welshdata. A national solution to map and hence correct this in the data submitted to HSW has been proposedand agreed in principle by the Team. A summary of the differences and proposed action is attached atAppendix D.
There are two issues of note. Firstly the Welsh segregation of admissions from and discharges toanother hospital site within the same Trust (fields 55, 56 and 57). These have been segregated from theirrespective standard codes (51, 52 and 53) which relate to transfers to or from other Trusts and representapproximately 2% of all admissions and discharges. The use of this field in Wales would be to segregatehospital (or campus) from Provider spells. As the grouping software does not utilise any of these fields inSpell generation it is proposed that 55, 56 and 57 are mapped respectively to 51, 52 and 53 for groupingpurposes only.
The second issue relates to discharge field 98 – not applicable, hospital provider spell not yet finished.Whilst acknowledging only 14k of 1m entries, this is an issue as England do not use such a field and itappears at face value inappropriate to map elsewhere. Gwent Trust have over half of these entries so wepropose working with them in the first instance, during Phase 2, to understand the sue of this code andexplore potential solutions.

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 8 of 32
Specialty codesHRG version4 publications form the Information Centre had noted “Data quality checks have beenextended to administration data, such as treatment function code and main specialty code”. We haveexplored this with them and confirmed: Despite England upgrading their specialty code list the previous version, largely maintained within
Wales, remains valid. Further, and crucially, the specialty field is only utilised for unbundled HRGs in two areas;
rehabilitation (23 HRGs) and specialist palliative care (10 HRGs).
Further to this a number of supplementary questions were distributed to Trusts and HSW for completionin February 2009, along with the initial impact assessment undertaken November 2007 for the respectiveorganisation to validate their responses. This was also the opportunity for those organisations that didnot respond to the initial request to supply a completed impact assessment The results of both havebeen summarised for section 5.
Therefore the proposal at this point is to proceed with national generation via HSW for ePEDW data witheffect from the 1st April 2009. Therefore at a Trust level this project can have no impact during 2009 / 10unless they choose to utilise nationally generated data. We will then use this year to continue to workthrough additional implications of Trust level self generation of HRG v4.
15. Known standards in use nationally and internationallyThe table below summarises England’s development and introduction of HRG v4 in comparison withWales:
05 / 06 06 / 07 07 / 08 08 / 09 09 / 10England
OPCS 4 version used 4.2 4.3 4.4 4.4 4.5HRG vsn for Reference Cost collection 3.5 4 4 4 4HRG vsn for Payment by Results 3.5 3.5 3.5 3.5 4
WalesOPCS 4 version used 4.2 4.3 4.4 4.4 4.5HRG vsn for Reference Costcollection
3.5 3.5 3.5 3.5 3.5 &/ or4
To note Northern Ireland also implemented HRG v4 for Reference Costs with effect from April 2007,whilst Scotland remain on v3.5 at this time.

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 9 of 32
SECTION 4: THE PROPOSAL
16. Proposed Solution
It is proposed that NHS Wales upgrade the HRG version from 3.5 to 4.
In the first year (2009 / 10) it is proposed that this is done nationally, in recognition of bothnational organisational reforms and Trust level PAS system implications. It is then proposed thatTrust level implementation takes place during 2010 / 11, under the auspices of a separate project.
In support of this proposal the following summarises results of work to demonstrate the benefits of thisupgrade as well as noting some proposals to address necessary adaptation issues for the grouper’s usewithin Wales.
How spells are derived under HRG v4 and implications for WalesVersion 4 only utilises two fields within the data to define and generate spells. These are PROCODETand PROVSPNO fields, which in Wales deliver a Campus (Hospital) Spell. Once version 4 hasestablished the spell it takes all the appropriate fields, from the underlying FCEs, and begin the groupingagain (as if all the elements occurred within one episode) to generate one HRG for the whole spell.
We have confirmed with the Information Centre that specialty is neither generated nor perceived asmeaningful at a Spell level. The grouper therefore only shows specialty for an individual FCE.
Further there are admission and discharge fields within Welsh data, to generate spell activity for Welshdefinitions. These would trigger data validation errors, for further detail please see section 14(Operational Fit) which explains the proposed mapping to resolve this issue.
To conclude spell is therefore no longer considered to be an issue as the grouper will generate aconsistent spell that is already present in Welsh APC data. However if a future decision is made onwhich of two available spells (Provider and Campus (revised hospital spell)) then this may have to berevisited as an element of that review.
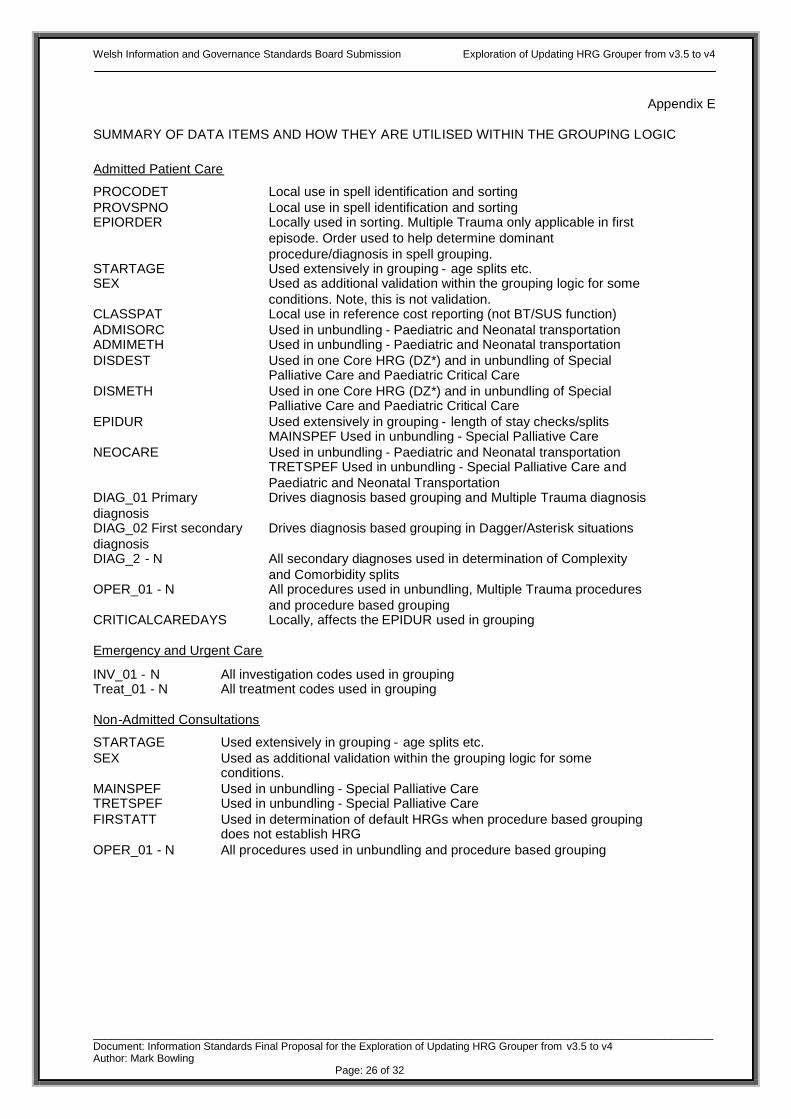
For information a list of data items and how they are utilised in the grouping logic, including those notedabove, has been included at Appendix E.
Trust level coding impact, if any, of introducing HRG v4 for existing activity capturedHSW completed an exercise for the group passing the same two years of national data through HRGversions 3.5 and 4. The first level of analysis is attached at Appendix C and contrasts how many FCEsfall into each chapter under both versions. The design of HRG v4 and expansion, including chapterdevelopments, meant that it was expected FCEs may move between areas and indeed this overallsummary shows similar patterns to English data, the initial cause for concern on this summary was thelevel of the U (undefined) codes. There are two key aspects to this that were explored further:
Genuine Data Quality issuesWe have confirmed with the creators of version 4, the Information Centre in England, that version 3.5 wasrelatively unconcerned with data quality, taking all fields presented, ignoring any that it did not recogniseand attempting to generate a grouping from the remainder. A Department of Health specified designcriteria for version 4 was data validation. The first step in grouping is for every field presented to bechecked against expected values, if any single field fails this process the record is rejected. Thisenforces data quality and the grouper supports this by producing very detailed data quality reportsspecifying how and why each record has failed. Further described at Appendix F.
Appendix G summarises and contrasts by chapter the number of FCEs for versions 3.5 and version 4.The first two tables giving the initial 2006 / 07 and 2007 / 08 results respectively and the third thenupdating the 2007 / 08 for data corrections between November and January as a result of thisinvestigation.

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 10 of 32
This improvement, to more than 10% of the FCEs that failed the initial data validation, was largelyachieved through correcting a few isolated anomalies. For example for the former Swansea NHS Trust afield (‘neonatal level of care’) had not been populated by their extract routine of their new PAS and also insome instances it was generating ‘OPCS’ rather than an actual code.
Errors caused by applying to data beyond the scope of HRGv4A further 17k records were rejected as Trusts, similar to England, are utilising ICD10 Classification ofMental and Behavioural Disorders which is slightly different to ICD10 Classification of Diseases andRelated Health Problems, and provides more specificity with some codes so that a 5th digit is required.HRG version 4 has been developed for Acute secondary care services, therefore the three mental health(chapter WD) HRGs merely distinguish based upon age. From discussions with the Information Centrewe confirmed that HRG version 4 is unlikely to be the vehicle to develop mental health classifications.Instead work in England is well advanced on developing ‘21 clusters’ to define mental health activity.Therefore proposed for Wales: For grouping purposes only the procedure code fields are limited to 4 characters (which would
truncate the additional 5th digit) Mental Health activity is not grouped using HRGs, this is consistent with HRG usage for reference
costs in Wales to date.
Additional Data Quality BenefitHRG version 4 generates specific data quality reports highlighting reasons that the record was deemed‘ungroupable’. These data quality reports have been shared with all Trusts via the CHIP Data QualityImprovement Manager for comment as part of their data quality requirements.
Further analysis has been requested by a number of Trusts to allow them to explore the issues. Thosedata quality issues identified during the development of the proposal are now in the process of beingintegrated within a monthly clinical data quality reporting mechanisms, which is subject to furtherdevelopment.
Segregation of Specialist ActivityIn support of one of the initial drivers good progress has been made in proving segregation of specialistactivity. Under available version 3.5 HRGs 606 are reached by Welsh data. Of the 1,400 version 4HRGs the same data generated 1,078 of them. The two years of data was further queried to separateany HRGs where 80% or more of the reported activity related to one organisation. This was utilised as acrude method of segregating potentially specialist and tertiary activity, for further analysis. The results,showing over three times as many potentially unique codes, are tabled below.
2006 / 07 2007 / 08 2006 / 07 2007 / 08Abertawe Bro Morgannwg 10 15 18 17Cardiff and Vale 10 5 53 53Cwm Taf 0 0 0 1Gwent Healthcare 0 0 3 4Hywel Dda 0 2 6 3North Wales 3 3 3 7North West Wales 0 0 2 2Powys LHB 0 0 0 0Velindre 8 5 9 11Total 31 30 94 98
HRG version 3.5 HRG Version 4
The detailed HRGs were then reviewed by the project team and the following actions taken:o For both Cardiff & Vale and Swansea HRGs that appeared to support the supposition of segregating
specialist activity for Spinal and Cardiac services were further analysed at Trust level. This identifiedthe specific cases which were then separately costed to see if it evidences distortions caused byspecialist activity. Two version 3.5 HRGs analysed in this way are noted below:
o E08 - Pacemaker Implant except for AMI, Heart Failure, or ShockAcross Wales there were 1,190 FCEs from 12 Trusts, with an average cost of £2,706 per FCE,ranging form £138 for Pontypridd & Rhondda to £8,200 for Cardiff & Vale. The Cardiff data had been

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 11 of 32
further analysed using version 4, which produced 17 individual HRGs ranging from 1 to 90 FCEseach, and having recalculated average unit costs of £2,395 to £35,101 per HRG.From the reasonably unique codes list two relating to implantation of defibrillators were in this datahaving an average cost of approximately £14,500 per procedure (43 FCEs).Whilst not possessing the defibrillator codes, an analysis of Swansea data for this version 3.5 HRGgave a range of £2,756 to £10,934 per HRG under version 4.
o R03 ‘Decompression and Effusion for Degenerative Spinal Disorders’Across Wales there were 654 FCEs from 5 Trusts, with an average cost of £5,523 per FCE, rangingfrom £635 for North West Wales to £8,525 for Cardiff & Vale. Again further analysis of the Cardiffdata showed 17 individual version 4 HRGs with recalculated average unit costs of £3,015 to £19,217per HRG.From the reasonably unique codes list two, relating to major extradural spinal and significant multipletrauma spinal, appeared in this data having an average cost of £11,769 and £19,217 respectively (79FCEs). Again Swansea recalculations broadly support the range of activity subsumed within oneFCE by HRG v3.5, having a range of £1,334 to £11,900 per FCE.
To summarise the average Cardiff & Vale cost for these procedures versus the overall Welsh averagecost under version 3.5 would indicate that the Trust are almost twice the average cost for Wales. Insegregating those aspects that are fairly unique to the Trust and recomparing shows the Trust asmore in line with overall Welsh performance for the comparable aspects. This will be a crucialdistinction in taking Service Level Reporting forward, firstly in segregating costs and activity for thespecialist providers but also to avoid distortions in the average unit cost that non-specialist providersmay be comparing themselves against.
o Some results did not accord with perceptions of specialist centres, for example ophthalmic treatmentsat the former Conwy & Denbighshire NHS Trust. These were segregated and the Trust approachedto assist in investigating the cause. It emerged that the ‘normal’ cataract procedure HRG (B13), thatthe majority of Trusts generate, needs an extraction as well as an insertion of lens procedure code.The extraction code was missing from the majority of the ePEDW data for Conwy & Denbighshire andit therefore generated a B15 code. However it was reportedly present on their local PAS, which thengenerated a B13 internally. This has identified a potential problem with the Trust’s extraction andsubmission routines which is being investigated further locally.
Clinical EngagementIn utilising the resultant output there will be a variety of users, from the WAG Performance Division at anational level through to the existing information and finance colleagues at Trust levels. The developmentof Service Line Reporting is expected to expand the users more generally into Trust management as wellas clinical engagement.
As part of the work to date some clinicians have been engaged. One orthopaedic consultant whospecifically approached colleagues as well as through feedback and testing of the resultant output e.g.respiratory consultants, anaesthetists and clinical coders have all been involved in a review of resultantHRGs for Chronic Obstructive Pulmonary Disease (COPD). As previously noted this didn’t evidence asegregation of non-invasive ventilation and intubations for English data, which was also reflected in theWelsh results. One key cause identified is the commencement of ventilation in an intensive careenvironment, i.e. generally outside of the COPD FCE where it appears not to be generally noted as it isalready in place for the patient. Investigation is ongoing at a patient record level with two Trusts to see ifprocess changes could be advised via the coding community.
In developing phase 2 for Trust level roll out opportunities will be sought to further pursue and evidenceclinical engagement opportunities.
Utilisation of OPCS versions 4.3 and 4.4 within WalesOne query during this process was the take up of OPCS 4.3 and 4.4 in Wales, as it underpins aspects ofversion 4 HRGs. We have investigated this from two angles, firstly HSW assisted in segregating thenumber of instances, by organisation, of either a 4.3 or 4.4 code in submitted data. A summary is shownbelow, all Trusts are utilising these codes and, as may be expected from the significant expansion tospecialist cancer coding in OPCS 4.3, Velindre have the majority of this increase.

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 12 of 32
Trust 4.3 codes 4.4 codes 4.3 codes 4.4 codesABM University NHS Trust 26,593 1,073 30,529 1,959Cardiff and Vale NHS Trust 46,522 968 41,544 2,364Cwm Taf NHS Trust 14,632 322 13,591 769Gwent Healthcare NHS Trust 23,524 639 20,434 1,982Hywel Dda NHS Trust 23,086 322 21,526 510North Wales NHS Trust 33,541 666 27,065 1,400North West Wales NHS Trust 10,938 325 11,643 734Powys Teaching LHB 660 13 438 33Velindre NHS Trust 108,860 26,895 55,552 29,687Grand Total 288,356 31,223 222,322 39,438
2008/09 (9 months)2007/08 (full year)
For the second step the Information Centre (England) assisted in providing a list of version 4 HRG codesthat can only be reached by OPCS 4.3 or 4.4 procedure codes, Appendix H gives the results for NHSWales which demonstrate over 2,500 FCEs. When added to the unbundled HRGs (noted below) that canonly be reached through the additional OPCS codes this demonstrates 127,000 codes generated throughthese new OPCS codes and a significant utilisation within Wales to date.
National implementation only for first yearThis decision was based upon: Re-organisation within NHS Wales having significant additional implications for organisations during
2009 / 10. Trust responses to the first Trust survey (Nov 07) indicated for some a six to nine month
implementation timescale (increase in number of characters and timescales for roll out of grouper inparticular).
The initial and follow up Trust Impact surveys. PAS supplier readiness, for example we have been informed that iSoft are not able to support HRGv4
from the 1st April 2009 and expect this development to take place during the latter part of 2009.
It is therefore proposed that Trust level implementation takes place during 2010 / 11 (at which point theywill be LHBs under the new organisational model)
Number of Fields, including ‘Unbundling’HRG version 3.5 only generates one code per FCE at present, PEDW then holding the Trust submittedHRG and it’s own derived HRG in two separate fields. Version 4 generates an FCE HRG and indicatesthe overall spell HRG for each record. Further it can generate ‘unbundled’ HRGs, to separate discrete orcostly elements including aspects such as high cost drugs, interventional radiology and chemotherapy.
This creates a problem for the national database in defining how many fields to set up to allow forunbundling. To resolve this we have: Investigated the number of unbundled fields generated by the test data, this is tabled at Appendix I.
Showing a maximum of 12 but 99% of those records having unbundled elements had 3 or lessunbundled codes. Although it should be noted that we are not using the system to it's potential.
Information Centre (England) colleagues noted that SUS set a limit for unbundled items at 12 Further they noted that the grouper produces a file that gives relational output. By noting a unique
spell reference it gives each unbundled record as a single line in an additional file. One solution forWales could therefore be some form of note on the main ePEDW record that unbundled element(s)do or don’t exist. Supplemented by a separate table containing this relational data.
In establishing how HRG version 4 can be introduced via HSW this summer we will investigate thisrelational file further as the preferred solution, as it would contain every unbundled item. If not feasible aconsistent limit of 12 unbundled fields would be proposed.

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 13 of 32
17. Fitness for PurposeThe standard outlined in this proposal will be achieved through the standard PAS functionality and APCstructure. To summarise the objectives identified for this phase of the project have largely been met,although more work to establish and evidence clinical engagement is required. This latter part will nowform a larger aspect of phase 2.
The following will be an indication of a successful implementation;o Health Solutions Wales will update the appropriate software packages to ensure that HRGv4 is
represented to Trust Information / Finance colleagueso All Trusts shall supply the information within their APC data set to HSW on a monthly basis, from
2010/11 onwardso Additional granularity would be able to be seen in the financial costing returns generated from
centrally held data.o All Trusts will be subjected to a data quality audit which will incorporate validations of the activity
which will be reconciled with the Trusts, as well as the data quality review processes already noted.
18. Testing / PilotHSW have assisted in piloting through a separate database, as noted in analysis thus far. Proving thatWelsh data can be grouped under HRG version 4.At a Trust level those Trusts represented in the project have been approached to test the output, e.g. forthe specialist activity noted above.Further Cardiff & Vale NHST have volunteered to pilot the implementation of HRG v4 at a Trust levelduring June 2009, to identify if any further / different issues emerge at Trust level..
19. Information GovernanceAs the proposed solution utilises the National Database infrastructure, which already has PIAG (PatientInformation Advisory Group) approval, there are no Information Governance issues.
20. Commercial Considerations
Two potential commercial issues were previously identified:o NHS England created and maintain the HRG software. To date Wales have received this and
upgrades free via download. It has been confirmed that this may continue.o Medicode underpins many PAS systems in Wales and would have to be upgraded to accommodate
version 4. Their project to deliver this has been successfully concluded and is being rolled out to theirWelsh Trusts. As noted other Trusts in Wales either utilise Simplecode, which has been upgraded forversion 4, or the Information Centre grouper itself.

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 14 of 32
SECTION 5: IMPACT ASSESSMENT
21. Impact Assessment
An Impact Assessment for HRG v4 had already been undertaken by CHIP in November 2007, prior to thisproject. The summarised results are included for reference below, and further detailed responses areincluded within Appendix J. Whilst this was felt to have not contained any major issues / stumbling blocksfor this project, a subsidiary version to this was being generated to update, clarify cost implications andaddress other areas of enquiry e.g. OPCS 4.4 take up. Following feedback at the Development Stagethis went out to Trusts and HSW in February 2009 to update the original review.
IMPACT ASSESSMENT 1Following the development of the recommendations outlined within the Acute Activity Currencies forCommissioning and costing, an Impact Assessment was developed with the aim of ascertaining theimpact on Trusts if HRGv4 was implemented locally. The following key headlines should be read in thecontext of Trusts being requested to populate a HRGv4 locally and then passed onto HSW for storagewithin the national database. Due to the elapsed time from the initial impact assessment, a copy of theoriginal impact assessment along with a number of supplementary questions were distributed to thoseorganisations previously surveyed for them to validate their previous responses and to supply responsesto the additional questions.
KEY HEADLINES FROM IMPACT ASSESSMENT 1Of the organisations included within the survey, nine organisations responded to the impact assessments,however, responses were received based upon the old Trust configuration for those Trusts that hadrecently merged.
WIGSB Members please note that impact assessments were not receivedfrom the following organisations;
Abertawe Bro Morgannwg University NHS Trust – former Swansea Cwm Taf NHS Trust – former Pontypridd and Rhondda Hywel Dda NHS Trust Health Solutions Wales
In view of the size of the impact assessments, the following key headlines will be split into the specificsections requiring a response;
SYSTEMS All Trusts confirmed that their PAS system would be affected by the proposed solution; also
highlight ing issues relating to engaging third party companies. Due to this reliance upon third party companies only 2 organisations would be able to independently
make the necessary changes, if the local option was explored.
PROCESSESS In terms of the impact upon the business processes, all organisations highlighted that there would be
slight impact upon the business process of the organisations. It was noted that due to the impactupon the clinical coders that dedicated protected time would be required by Trusts to ensure that allstaff are made aware of the new grouper.
RESOURCES Of the organisations surveyed, the costs ranged from £0k - £15.0k. The likely development time to implement the proposed solution would be 0-6 months. The majority of the costs were assigned to the requirement for additional training of clinical coding
and clerical staff to ensure that the proposed solution is implemented successfully.
PEOPLE The number of staff that would require training would be greater than 20, with an implementation
period of 6-12 months

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 15 of 32
To summarise, following the results of the above impact assessment a decision was made to explore thecurrently proposed solution of deriving the HRGv4 nationally. With this is mind a number ofsupplementary questions were asked of those organisations involved within the first impact assessment.
IMPACT ASSESSMENT 2 – SUPPLEMENTARY QUESTIONSFurther supplementary questions were sent to NHS Trust Information Managers, Business ServicesCentre, and Health Solutions Wales. The key questions asked were;
a) How does your Trust currently apportioned a HRG3.5 (e.g. Batch process, created from theencoding software, created on extract to PEDW, outside PAS within a warehouse etc)?
b) Is the current HRG3.5 stored within your PAS?c) What would be the required development time required to implement HRGv4?d) What approximately would be cost associated with this implementation?e) Would you be able to effect the change to the system, or are you reliant upon a third party?f) If a decision is made to apportion a HRGv4 nationally via Health Solutions Wales, would you
still require the ability to apportion locally? If so, how would achieve this?
KEY HEADLINES FROM IMPACT ASSESSMENT 2Detailed responses can be found in Appendix J. Disappointingly, and despite a number of follow upcommunications, there was a limited response from the service.
WIGSB Members please note that responses were not received from thefollowing organisations;
Abertawe Bro Morgannwg University NHS Trust Cwm Taf NHS Trust Hywel Dda NHS Trust North West Wales NHS Trust Health Solutions Wales North Wales NHS Trust
Of the organisations that responded they all stated that the assignment of HRG codes took placeduring the encoding process. This confirmed that there would be a requirement to ensure that afurther release of encoding software from those third party companies to allow HRGv4 to becreated. This would therefore result in a further requirement to modify the national infrastructureto then receive this modified data, if a decision is taken that a ‘submitted HRGv4 code’ field isrequired nationally (similar to the distinctions made in version 3.5 codes).
There was overwhelming feeling that although the proposed solution would be beneficial, locallyorganisations would like to implement HRGv4 for there own needs. Powys LHB conceded that ifthe data could be made available in a timely fashion nationally then there will less pressure uponthe LHB to implement HRGv4 locally.
In summary of those Trusts that responded to the supplementary questions agreed that, although theproposed solution is would be difficult to implement locally within the timescales the national solutionwould have no impact upon them as they would be expected to continue submitting data as per currentrequirements.
From an awareness perspective the following groups have been made aware of this project and are beingkept informed periodically of progress.o Clinical Coding User Groupo National costing groups – All Wales Costing Strategic Advisory Group and All Wales Costing
Technical Group (membership from information and finance, Trust, LHB, HCW and WAG)o Information Leadso Directors of Finance (both Trust and LHB)

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 16 of 32
To summarise impacts:o HSW – impact of changes to national database to generate and accommodate HRGv4 fields are
being discussed as part of the 2009 / 10 SLA.o Trust level:
no workload impact of phase 1, specifically APC submissions will remain as current. some Trusts may however have a HRG implication of migration to OPCS 4.5 (not an impact of
this project). For example 3M (supplier of majority of encoding software in Wales) have identifiedthat some PAS suppliers will not be able to cope with an HRGv4 code sent through their interfaceto the PAS system (e.g. iSoft have confirmed that they are not looking to support HRGv4 from the1st April 2009 and expect this development to take place during the later part of 2009).

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 17 of 32
SECTION 6: IMPLEMENTATION PLAN
22. Implementation planThe Implementation plan is outlined below.
Milestone Deadline Status
Phase 1
Final Proposal to be submitted to WIGSB April 2009 Pending
Ministerial Letter / Data Set Change Notification distributed tothe Service
April 2009 -
Health Solutions Wales (HSW) undertake necessarymodifications to the national infrastructure to allow HRGv4 tobe derived
June 2009 -
HSW to undertake retrospective population of HRGv4 in orderto provide analysis based upon first quarter of 2009/10 data
July 2009 -
HSW to provide HRGv4 via e-PEDW monthly from July 2009onwards
August 2009 -
Review the impact of the new standard upon corporate reportsand Welsh Costing Returns (WCR)
September 2009– December
2009
-
Production of the Data quality error reports in conjunction theemerging Clinical Coding Data Quality reporting mechanisms.
January 2010 –March 2010
-
Review submission to be submitted to WIGSB August 2010 -
Phase 2 – Trust level implementation:
Advice sort from the Board on this issue. Project group concluded that this would need to be subjectto a separate WIGSB submission and a separate sponsor for this aspect of the work would likely berequired.
23. Official Documentation
Advice also sought on this aspect. Project group have concluded:
Issue a Ministerial letter
Issue a DSCN (as HRGs are included within the data dictionary)

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 18 of 32
SECTION 7: MAINTENANCE AND REVIEW
24. Maintenance ProcessThe standard will be maintained, and monitored as per the arrangements included within Section 6:the Implementation Plan.Any further developments will be included within the work progressed by Directorate of Resources,under the auspices of the All Wales Costing – Strategic Advisory Group.All technical issues will be handled by Health Solutions Wales, and in liaison with Trusts. There may becircumstances when HSW escalates issues to the Project Sponsor where decisions are required.
Review to phase 1 may be required in light of lessons learnt from phase 2.
25. Planned review datesAs per the staged implementation plan included within Section 6 HSW will be expected to have thecapability to provide HRGv4 analyses by July 2009. The Phase 2, Trust level, project thenconcentrating on ensuring that Trusts will be able to supply HRGv4 episode data by April 2010.
A Review document will be prepared for submission to WIGSB in July 2010.

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 19 of 32
Appendix AAcknowledgements
Project Team:o Kerry Ashmore, Information Modernisation & Development Manager, Cardiff & Vale NHS Trusto Mark Bowling, Programme Manager, Financial Information Strategy (chair)o Jennifer Evans, Data Standards and Clinical Coding, HSWo John Evans, Costing (Finance), Hywel Dda NHS Trusto Sally Greenway, Head of Information Standards, WAGo Hywel Jones, Principle Finance Manager, Cardiff & Vale NHS Trusto Karen O’Doherty, Clinical Coding Advisor, NHS Waleso Lisa Powell, Costing (Finance), Cardiff & Vale NHS Trusto Denise Roberts, Project Manager, Financial Information Strategyo Helen Thomas, Information, ABMU NHS Trusto Helen Thomas, Finance, ABMU NHS Trusto Anthony Tracey, Project Manager, CHIP
I would also like to acknowledge assistance from:The NHS Information Centre (England), particularly Paula Monteith, Principal Casemix InformationDesign ConsultantPaul Kirkman, Key Account Executive, Health Information Systems, 3M (encoding software supplier)

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 20 of 32
Appendix B (1)

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 21 of 32

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 22 of 32
Appendix B (2)

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 23 of 32
Appendix C
Off-Specification Form - Number 001
PurposeTo document any situation where a product is failing, or may fai l, to meet its specification.
Issue Log No: 001
Date Raised: 11/09/2008
Status: Active
Description of Fault: The impact of differing data standards currently in place withinNHS England and NHS Wales, in particular Specialty Codes,Admission and Discharge Data Items.
Impact of Fault:In light of the analysis undertaken by Health Solutions Wales regarding HRGv4, the ProjectTeam are requested to consider the following;
The likely impact upon the implementation of HRGv4 within NHS Wales due to thediffering data standards
The inclusion of Critical Care Days which currently is not collected within the routineAPC submissions
In view of the above, there is a need to review the merit of continuing, stopping or changing thedirection of the HRG Project.
Proposed Way ForwardIt has become apparent that there are number of data items which are deemed mandatory andare required to be included within the input file for HRGv4. In summary they are;
The requirement to include a number of new fields, namely; Patient Classification,Discharge Destination, Source of Admission, Admission Method, Discharge Method,Neonatal Level of Care, and Critical Care Days.
As the HRG4 Grouper works upon definitions that have been agreed by England, where thereare Welsh variations, the grouper considers these as invalid values and will assign anungrouable code (UZ01Z. This would equate to approximately 97,000 records (based upon a 2year period)
A proposed way forward, in the short term, for these ungroupable cases could be to ensure thatmapping to existing codes is undertaken during the exporting of data for the input file from thecentral database.
However, this mapping will not be sufficient for the differences noted with the Specialty Codestructures. Due to their complexities, it would be difficult to undertake this mapping centrally.
It is proposed that further consideration is given to comply with the English Specialty codelistings.

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 24 of 32
The collection of Critical Care Days is used to ensure that the FCE length of stay has anycritical care days removed before grouping begins. Where there are no critical care dayspresent within the record a “0” can be placed within the record.
As NHS Wales does not have a critical element to its APC extract, HSW will be able to place azero within this field and these records will be passed through the grouper.
In summary the following are the proposed way forward; An investigation into whether in the short term, the mapping to existing codes could be
undertaken centrally. Further consideration is given in order to comply with the English Specialty code listings. Centrally a “zero” will be placed within the input file so that records can be passed
through the grouper.
Priority Assessment: Urgent
Decision: Project Team agreed with proposal
Date Completed: 09/10/2008

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 25 of 32
Appendix DData Field Differences in Welsh data that generate Grouping errors with ProposedMapping (for Grouping purposes only)
ePEDW data extract for 15 months (1st April 07 to 30th June 08)
Admission SourceNo of
records Proportion CauseProposed mapping for grouping
purposes
Valid and consistent withEngland
1,022,140 97.5% Nothing further required
Invalid entries 187 0.02% data qualitynone - leave to appropriately generatean invalid code
55, 56 & 57 - Hospitalsite within same Trust
22,934 2.2%
Introduced under DSCN 30/2001 toidentify patients admitted from ahospital in the same Trust. Utilised inWales to segregate Hospital (/Campus)from Provider spells.
map to 51, 52 & 53, their 'other NHSTrust' equivalents - in HRGv4 none ofthese fields utilised in generating Spell -thereby no impact upon grouping
85 non-NHS residentialcare home and 86 non-NHS nursing home
3,310 0.3%segregation occurred pre 1995, nohistory
map both to 85, which England definesas 'Non-NHS run care home', as noimpact upon grouping
Total 1,048,571
Admission MethodNo of
records Proportion CauseProposed mapping for grouping
purposes
Valid and consistent withEngland
1,046,734 99.8% Nothing further required
Invalid entries 51 0.005% data qualitynone - leave to appropriately generatean invalid code
14 - Second Offer 857 0.08%14 and 15 introduced under DSCN(2006) 03, one Trust (Gwent) submitted854 of these
Minor use and irrelevant to grouping -map to 13 Planned admission
25 Dom Visit and 27 viaNHS Direct
929 0.09%25 reinstated in 1998 (no DSCN), 27introduced by DSCN 38/2001
relatively small, irrelevant to groupingprocess, map to 28 'Other Means'
Total 1,048,571
Discharge DestinationNo of
records Proportion CauseProposed mapping for grouping
purposes
Valid and consistent withEngland
1,014,111 96.7% Nothing further required
Invalid entries 6 0.001% data qualitynone - leave to appropriately generatean invalid code
39 - Penal establishment,court or police station 288 0.03%
pre-1995. English code of 38 defined asPenal establishment or police station
Map to 38 due to similarity of code andpurpose
55, 56 & 57 - Hospitalsite within same Trust
17,278 1.6%
Introduced under DSCN 30/2001 toidentify patients discharged to ahospital in the same Trust. Utilised inWales to segregate Hospital (/Campus)from Provider spells.
map to 51, 52 & 53, their 'other NHSTrust' equivalents - in HRGv4 none ofthese fields utilised in generating Spell -thereby no impact upon grouping
85 non-NHS residentialcare home and 86 non-NHS nursing home
5,985 0.6%segregation occurred pre 1995, nohistory
map both to 85, which England definesas 'Non-NHS run care home', as noimpact upon grouping
98 - N/A hospitalprovider spell notfinished
10,903 1.0%Introduced 1st July 1997.Disproportionately 6,838 relate to oneformer Trust (NEW)
This is an issue, will work with Gwent inparticular to understand use andexplore possible solutions.
Total 1,048,571
Discharge MethodNo of
records Proportion CauseProposed mapping for grouping
purposes
Valid and consistent withEngland
1,045,199 100% Nothing further required
98 - N/A hospitalprovider spell notfinished
3,372 0.3% Introduced pre-1997.This is an issue, will work with Gwent inparticular to understand use andexplore possible solutions.
Total 1,048,571
Adm
issi
ons
Dis
char
ges
Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 26 of 32
Appendix E
SUMMARY OF DATA ITEMS AND HOW THEY ARE UTILISED WITHIN THE GROUPING LOGIC
Admitted Patient Care
PROCODET Local use in spell identification and sortingPROVSPNO Local use in spell identification and sortingEPIORDER Locally used in sorting. Multiple Trauma only applicable in first
episode. Order used to help determine dominantprocedure/diagnosis in spell grouping.
STARTAGE Used extensively in grouping - age splits etc.SEX Used as additional validation within the grouping logic for some
conditions. Note, this is not validation.CLASSPAT Local use in reference cost reporting (not BT/SUS function)ADMISORC Used in unbundling - Paediatric and Neonatal transportationADMIMETH Used in unbundling - Paediatric and Neonatal transportationDISDEST Used in one Core HRG (DZ*) and in unbundling of Special
Palliative Care and Paediatric Critical CareDISMETH Used in one Core HRG (DZ*) and in unbundling of Special
Palliative Care and Paediatric Critical CareEPIDUR Used extensively in grouping - length of stay checks/splits
MAINSPEF Used in unbundling - Special Palliative CareNEOCARE Used in unbundling - Paediatric and Neonatal transportation
TRETSPEF Used in unbundling - Special Palliative Care andPaediatric and Neonatal Transportation
DIAG_01 Primarydiagnosis
Drives diagnosis based grouping and Multiple Trauma diagnosis
DIAG_02 First secondarydiagnosis
Drives diagnosis based grouping in Dagger/Asterisk situations
DIAG_2 - N All secondary diagnoses used in determination of Complexityand Comorbidity splits
OPER_01 - N All procedures used in unbundling, Multiple Trauma proceduresand procedure based grouping
CRITICALCAREDAYS Locally, affects the EPIDUR used in grouping
Emergency and Urgent Care
INV_01 - N All investigation codes used in groupingTreat_01 - N All treatment codes used in grouping
Non-Admitted Consultations
STARTAGE Used extensively in grouping - age splits etc.SEX Used as additional validation within the grouping logic for some
conditions.MAINSPEF Used in unbundling - Special Palliative CareTRETSPEF Used in unbundling - Special Palliative CareFIRSTATT Used in determination of default HRGs when procedure based grouping
does not establish HRGOPER_01 - N All procedures used in unbundling and procedure based grouping

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 27 of 32
Appendix FExtract from Healthcare Financial Management Association HRG4 publication, March 2008 –explanation of Undefined Groups (U codes).Written by Steve Brown, editor, with support from Paula Monteith, principle information design consultantat the NHS Information Centre for Health and Social Care.

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 28 of 32
Appendix GTable 1: Annual Activity for All Wales 2006 / 07 grouped with HRG v3.5 & HRG4
Number of FCEsin HRG v3.5
Number ofFCEs in HRG4
% of FCEs inHRG v3.5
% of FCEsin HRGv4.0
A: Nervous System 38,939 68,699 4% 7%B: Eyes & Periorbita 29,875 29,126 3% 3%C: Mouth Head Neck & Ears 40,761 39,218 4% 4%D: Respiratory System 63,650 52,998 7% 6%E: Cardiac Surgery & Primary Cardiac Condition 78,536 71,492 8% 8%F: Digestive System 137,847 127,202 15% 14%G: Hepatobiliary & Pancreatic System 20,253 16,027 2% 2%H: Musculoskeletal System Including Spinal [R] 86,174 69,816 9% 8%J: Skin, Breast & Burns 62,103 54,180 7% 6%K: Endocrine & Metabolic System 11,433 9,473 1% 1%L: Urinary Tract & Male Reproductive System 87,096 80,119 9% 9%M: Female Reproductive System & Assisted Reproduction 43,126 39,715 5% 4%N: Obstetrics 73,584 61,052 8% 7%P: Diseases of Childhood & Neonates 53,271 67,304 6% 7%Q: Vascular System 11,898 16,775 1% 2%S / W: Immunology, Infectious Diseases & other contacts with healthservices, including Haematology & Mental Health
68,517 61,1217% 7%
T: Soft Tissue 12,704 1% 0%U: Undefined Groups 7,618 61,213 1% 7%V: Multiple Trauma - 1,855 - 0%
927,385 927,385 100%Source: PEDW (01-Apr-2006 to 31-Mar-2007)
Table 2: Annual Activity for All Wales 2007 / 08 grouped with HRG v3.5 & HRG4 (initial Oct 08)
Number of FCEsin HRG v3.5
Number ofFCEs in HRG4
% of FCEs inHRG v3.5
% of FCEsin HRGv4.0
A: Nervous System 37,073 33,453 4% 4%B: Eyes & Periorbita 30,843 25,814 3% 3%C: Mouth Head Neck & Ears 40,553 38,613 4% 4%D: Respiratory System 59,945 50,119 6% 5%E: Cardiac Surgery & Primary Cardiac Condition 76,954 61,248 8% 7%F: Digestive System 133,783 119,666 14% 13%G: Hepatobiliary & Pancreatic System 20,170 16,531 2% 2%H: Musculoskeletal System Including Spinal [R] 89,021 67,760 10% 7%J: Skin, Breast & Burns 50,684 46,820 5% 5%K: Endocrine & Metabolic System 10,600 8,035 1% 1%L: Urinary Tract & Male Reproductive System 83,737 77,113 9% 8%M: Female Reproductive System & Assisted Reproduction 42,203 37,163 5% 4%N: Obstetrics 68,423 54,256 7% 6%P: Diseases of Childhood & Neonates 51,439 52,756 6% 6%Q: Vascular System 12,540 15,353 1% 2%S / W: Immunology, Infectious Diseases & other contacts with healthservices, including Haematology & Mental Health
67,324 56,482 7% 6%
T: Soft Tissue 10,635 - 1% -U: Undefined Groups 32,904 156,065 4% 17%V: Multiple Trauma - 1,584 - 0%
918,831 918,831Source: PEDW (01-Apr-2007 to 31-Mar-2008)
Table 3: Annual Activity for All Wales 2007 / 08 grouped with HRG v3.5 & HRG4 (update Jan 09)
Number of FCEsin HRG v3.5
Number ofFCEs in HRG4
% of FCEs inHRG v3.5
% of FCEsin HRGv4.0
A: Nervous System 37,069 45,322 4% 5%B: Eyes & Periorbita 30,843 30,073 3% 3%C: Mouth Head Neck & Ears 40,553 44,053 4% 5%D: Respiratory System 59,944 53,571 7% 6%E: Cardiac Surgery & Primary Cardiac Condition 76,953 70,107 8% 8%F: Digestive System 133,782 129,686 15% 14%G: Hepatobiliary & Pancreatic System 20,170 18,101 2% 2%H: Musculoskeletal System Including Spinal [R] 89,020 78,097 10% 8%J: Skin, Breast & Burns 50,684 53,321 6% 6%K: Endocrine & Metabolic System 10,600 8,872 1% 1%L: Urinary Tract & Male Reproductive System 83,737 83,661 9% 9%M: Female Reproductive System & Assisted Reproduction 42,203 41,271 5% 4%N: Obstetrics 68,423 61,719 7% 7%P: Diseases of Childhood & Neonates 51,439 60,850 6% 7%Q: Vascular System 12,540 16,824 1% 2%S / W: Immunology, Infectious Diseases & other contacts with healthservices, including Haematology & Mental Health
67,324 62,716 7% 7%T: Soft Tissue 10,635 - 1% -U: Undefined Groups 32,913 58,748 4% 6%V: Multiple Trauma - 1,840 - 0%
918,832 918,832Source: PEDW (01-Apr-2007 to 31-Mar-2008)
Notes:
FCE's that have not yet been clinically coded were not included (Pdiag is blank)
Welsh Trusts - All Patients (Coded Data Only)

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 29 of 32
Appendix H (1)Version 4 HRGs generated exclusively by OPCS 4.3 or 4.4 codes in data submitted to ePEDW
HR
G4
Cha
pter
HR
G4
Labe
l
Nu
mbe
rof
FC
Esba
sed
on20
07/0
8da
ta
Core HRGs that can only be reached utilising OPCS 4.3 procedures codes, but can also be reachedthrough a diagnosis codingNervous System
Cerebral Degenerations or Miscellaneous Disorders of Nervous System 1,895
Core HRGs that can only be reached utilising OPCS 4.3 codesMouth, neck head and ears
Bone Anchored Hearing Aids 8
RespiratoryChest Physiotherapy 99
Simple Lung Function Exercise Testing 7
Hyperbaric Oxygen Treatment 7
Oxygen Assessment and Monitoring 7
Complex Gas Exchange Studies 4
Simple Gas Exchange Studies 2
TB Nurse Support 7
Respiratory Nurse and AHP education/support 1
Cardiac ProceduresPace 2 - Dual Chamber 407
Pace 3 - Biventricular and all congenital pacemaker Procedures - Resynchronisation Therapy 17
Percutaneous Congenital Interventions: Percutaneous transluminal ASD/VSD/PFO closure and valve insertion 2
Implantation of Cardioverter - Defibrillator only 66
Percutaneous Complex Ablation (includes Atrial Fibrillation or Ventricular Tachycardia) 45
Complex Echocardiogram (include Congenital, Transoesophageal and Fetal Echocardiography) 262
Simple Echocardiogram 710
BreastPedicled TRAM Reconstruction of Breast 2
Skin SurgeryPatch Tests 5
Investigative procedures 2 10
Urticaria tests 24
Minor Laser Therapy 5
Renal procedures and disordersKidney Transplant from Cadaver non-Heart beating donor 19 years and over 2
Live Kidney donor screening 1
Urological and male reproductive
Dynamic Studies of Urinary Tract 658
Treatment of Erectile Dysfunction 2
Female reproductiveVacuum Aspiration with Rigid Cannula for 9 weeks gestation or more 11
Vacuum Aspiration with Rigid Cannula for less than 9 weeks gestation 23
HaematologyPlasma Exchanges 2 to 9 11
Plasma Exchanges 10 to 19 1
Bone Marrow Transplant - Allogeneic Graft (Volunteer Unrelated Donor) 19 years and over 1
Non admitted care
Non-Admitted Face to Face Attendance - Follow-up 10
Multiprofessional Non-Admitted Face to Face Attendance - Follow-up 1
2,418

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 30 of 32
Appendix H (2)H
RG
4C
hap
ter
HR
G4
Lab
el
Nu
mb
erof
FC
Es
bas
ed
on
2007
/08
dat
a
Core HRGs that can only be reached utilising OPCS 4.4 codesRespiratory
Smoking Cessation Support 29
Respiratory Sleep Study 6
Skin SurgeryPhototherapy 5
Photochemotherapy 33
HaematologyPeripheral Blood Stem Cell Transplant - Autologous 19 years and over 20
Peripheral Blood Stem Cell Transplant - Autologous 18 years and under 4
Peripheral Blood Stem Cell Transplant - Syngeneic 19 years and over 1
Peripheral Blood Stem Cell Transplant - Allogeneic 19 years and older 11
109
In RC0809- 13 HRGs requiring the DGVP (or driving unbundled procedure) to be an OPCS-4.4 code (not present in4.3) - of these 11 are core, 2 unbundled- 196 HRGs requiring the DGVP (or driving unbundled procedure) to be an OPCS-4.3 code (not present in4.2) - of these 8 relate to outpatients, 62 are core, rest unbundled- 1 HRGs (AA18Z) is mixed medical/interventional HRGs where all OPCS codes are new to 4.3, but theHRG could be reached if grouping off primary diagnosis
This analysis comes with the following caveats:(1) No secondary procedure logic is used to resolve splits after the root HRG has been derived(2) There is no secondary procedure logic based on lists entirely composed of codes new to OPCS-4.3 orOPCS-4.4 (this assumption would not have been able to detect the now removed IR whose HRGs wereassigned on existing OPCS-4.2 codes with approach codes new to OPCS-4.3 - of course these HRGs wouldhave unreachable if the coder had only used 4.2)(3) The "OPCS version of a combination" is regarded as the highest version of its constituent codes e.g. anOPCS-4.2 code with an OPCS-4.4 site would be regarded as being "new to OPCS-4.4".(4) No lists used by the escalator in chapter H are composed entirely of new OPCS-4.3 or OPCS-4.4 codes.Not a problem because all affected HRGs can be reached directly by existing OPCS-4.2 codes as DGVP

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 31 of 32
Appendix IAnalysis of 2007/08 data having unbundled HRG
Trust 1st 2nd 3rd 4th 5th 6th 7th 8th 9th 10th 11th 12thABM University 7,147 819 262 72 22 10 7 6 5 5 3 1
Cardiff And Vale 12,313 3,225 820 284 78 23 10 3 1 1 1 1Cwm Taf 4,751 796 189 57 19 2 0 0 0 0 0 0Gwent Healthcare 7,770 1,473 382 114 25 6 2 1 1 0 0 0Hywel Dda 7,807 2,413 312 110 13 3 0 0 0 0 0 0North Wales 14,432 1,934 360 74 14 5 3 1 1 0 0 0North West Wales 3,703 614 150 56 13 1 0 0 0 0 0 0Powys LHB 184 0 0 0 0 0 0 0 0 0 0 0Velindre 66,439 10,348 557 382 26 18 9 4 2 1 1 0Total 124,546 21,622 3,032 1,149 210 68 31 15 10 7 5 2
Proportion 17.4% 2.4% 0.9% 0.2% 0.1% 0.02% 0.01% 0.01% 0.01% 0.004% 0.002%
Count of unbundled HRGs in each field
Proportion relates to those records having an unbundled HRG, e.g. of those records having an unbundledHRG 17.4% of them have two or more unbundled HRGs.

Welsh Information and Governance Standards Board Submission Exploration of Updating HRG Grouper from v3.5 to v4
_________________________________________________________________________________________________________Document: Information Standards Final Proposal for the Exploration of Updating HRG Grouper from v3.5 to v4Author: Mark Bowling
Page: 32 of 32
Appendix J
Gwent HealthcareNorth Wales Trust
(Conwy &Deinbighshire)
Velindre Powys LHB
Q1
How does your Trust currentlyapportioned a HRG3.5 (e.g. Batchprocess, created from theencoding software, created onextract to PEDW, outside PASwithin a warehouse etc)?
created from theencoding software
No responseInteractive encoder linked to ourEHR (PAS)
HRG processes happensautomatically as part of themandatory reporting process.
Q2Is the current HRG3.5 storedwithin your PAS?
Yes No response Yes
The HRG codes are closelyinterfaced with the PAS soassignment happens in thebackground and not visible to theuser.
Q3What would be the requireddevelopment time required toimplement HRGv4?
Sufficinet time to QAnew software
No responseApprox 40 days developmenteffort on EHR (PAS) plus discussionwith 3M regarding interfacing
Required changes would be carriedout within Hywel Dda NHS Trustand we would therefore beconstrained by their timescales.These have not been specified bythem to us.
Q4What approximately would be costassociated with thisimplementation?
Half Day awarenesssession for coders
No response
£8K plus the need to recruit extracoding resources As a specialistcancer centre radiotherapy,chemotherapy, specialistpalliative care and high cost drugsare a major part of our activity soall the benefits of unbundling keyelements will impact on coding(We will have to come back to youon this for details when our codingmanager returns from leave afteryour deadline).
Any system implementation costshave not been notified to us byHywel Dda NHS Trust. There willbe local staff training costs in theuse of episodes vs spells. We haveestimated these to be £15,000.
Q5Would you be able to effect thechange to the system, or are youreliant upon a third party?
Reliant upon a thirdparty
No responseYes in house system and interfaceto 3M
The system changes would becarried out by Hywel Dda NHSTrust.
Q6
If a decision is made to apportiona HRGv4 nationally via HealthSolutions Wales, would you stillrequire the ability to apportionlocally? If so, how would achievethis?
We would want to havelocal awareness of anygrouping applied to ourepisodes, and wouldimagine an update from3M would be available todo so
No response
I have doubts the HRG4“unbundling” could be donenationally so apportioning locallywould be required and it could beachieved via above
There would always be a need tocarry out local analysis of the databy HRGs therefore flexible accesswould be necessary. This could beby giving such access to a centraldatabase or HSW returning thedata with HRGs attached.
Trust
Questions