informal consultation on scaling up health workforce production [pdf
TRANSCRIPT
Informal consultation on scaling up
health workforce production Geneva
15–16 November 2006
Evidence and Information for Policy, Department of Human Resources for Health

© World Health Organization 2006
All rights reserved. Publications of the World Health Organization can be obtained from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel: +41 22 791 2476; fax: +41 22 791 4857; email: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press, at the above address (fax: +41 22 791 4806; email: [email protected]).
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either express or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.
This publication contains the collective views of an international group of experts and does not necessarily represent the decisions or the stated policy of the World Health Organization.

Contents
Background - challenges for the health workforce ...........................................................................1
Why scale up health workforce production?.....................................................................................2
What to scale-up?.............................................................................................................................3
Case 1. Brazil - PROFAE .................................................................................................................3
Case 2: Kenya - AMREF ..................................................................................................................4
Case 3. Cuba and Venezuela ..........................................................................................................4
Case 4. E-health and ICT technologies for health workforce education and training ......................5
How to scale up health workforce production?.................................................................................6
Closing remarks................................................................................................................................8
Annex 1.............................................................................................................................................9
Informal Consultation on Scaling-up of Health Workforce Production.........................................9
Programme...................................................................................................................................9
Annex 2...........................................................................................................................................10
List of Participants......................................................................................................................10
Temporary Advisers ...................................................................................................................10


Informal consultation on scaling up health workforce production
Between 15 to 16th November 2006 WHO organized a two-day consultation on scaling up the production of the health workforce. Participants with different backgrounds and experiences were invited to present their point of view and contribute to the development of a concept paper highlighting the main challenges and some workable policy options for scaling up the production of the health workforce.
Background - challenges for the health workforce There is a chronic shortage of well-trained health workers worldwide, both in terms of numbers of clinical and non-clinical health workers, and the necessary administrative and logistics staff at all levels. There is increasing evidence that health worker shortages are interfering with efforts to achieve the internationally agreed-upon health-related development goals, including those contained in the Millennium Declaration and those of WHO's priority programmes (WHO, 2006). This health workforce crisis is severely hampering the ability of additional financial resources – made available through new modalities, such as debt alleviation or the Global Fund to Fight AIDS, Tuberculosis and Malaria, GAVI, PEPFAR etc – to attain their goals. In many countries, there is simply insufficient human capacity to absorb, deploy and use efficiently the new money offered by global health initiatives.
In poorer countries, while the population is increasingly ageing, rapidly urbanizing and still suffering from infectious diseases, the health services fail to respond to current and emerging needs. The chasm is widening between what is theoretically possible and what is actually being done. Success in bridging this gap will be determined in large measure by how well the workforce is developed in order to contribute towards more effective health systems (WHO, 2006). For these reasons, in recent years the issue of human resources for health has been catapulted on the top of the global health agenda.
The World health report 2006: working together for health estimated that 57 countries have an absolute shortage of 2.3 million doctors, nurses and midwives, which means that they don't have sufficient health professionals to deliver essential health interventions, such as skilled attendance at birth, and immunization programmes. The cost of training and deploying the needed workforce would require an increase in health spending of about USD 10 per capita per year in each of these countries by 2025.
Countries have already tried various strategies – over-production, importation, etc. – but the global environment and economic situation have put obstacles in their path. For instance, the developed world under-produces health workers and imports huge numbers, a policy that promotes poaching of health workers from developing world. Countries are now looking for clear, coherent, and coordinated technical advice to address this problem.
Responding to the needs expressed by its Member States, the World Health Assembly passed the Resolution WHA59.23 in May last year. The resolution calls for a rapid scaling up of the production of human resources for health, and for establishing and strengthening partnerships between institutions from developed and developing countries in the area of health workforce education and training.
A truly comprehensive response to the global human resources for health (HRH) crisis cannot be undertaken by any single entity. It calls for concerted, coordinated and sustained action from the multiple key players within sectors and institutions and across sectors, disciplines, countries and regions of the world. The Global Health Workforce Alliance (GHWA) was born out of this increasing interest in HRH in May 2006. It provides a forum for sharing and learning from each other' experiences, and for harnessing partnerships to address this complex yet essential component of health systems performance and social development. The GHWA is aimed at both the global and country level, and its main focus is the impact of the shortage and overall health systems crisis in Africa. The GHWA supports the development of strategies needed to solve the HRH crisis.
Informal consultation on scaling up health workforce production • Page 2
Recent reports from WHO showed that things are moving: awareness has been raised, especially in African countries. In many countries health sector budgets have increased, as has the focus on HRH, at least at Ministry of Health (MoH) level. But, there needs to be a change within many Ministries of Health structures so that HRH is given top priority – especially in terms of staffing, incentives and resources.
The aim of the consultation was to review the main challenges in scaling up the production of the health workforce and to propose some workable policy options. The consultation addressed three key questions: why scale up? what to scale up? and how to scale up?
Why scale up health workforce production? A first discussion during the meeting, was on the issue that new ideas were needed for a massive increase of HRH production in the regions and countries where the shortage of health workers is a prevailing problem. A revolution in thought is called for to deal with the HRH crisis: creative and innovative ideas on how to marshal the health workforce to address the shortage, since it is impossible to solve the current problems only by boosting existing educational models.
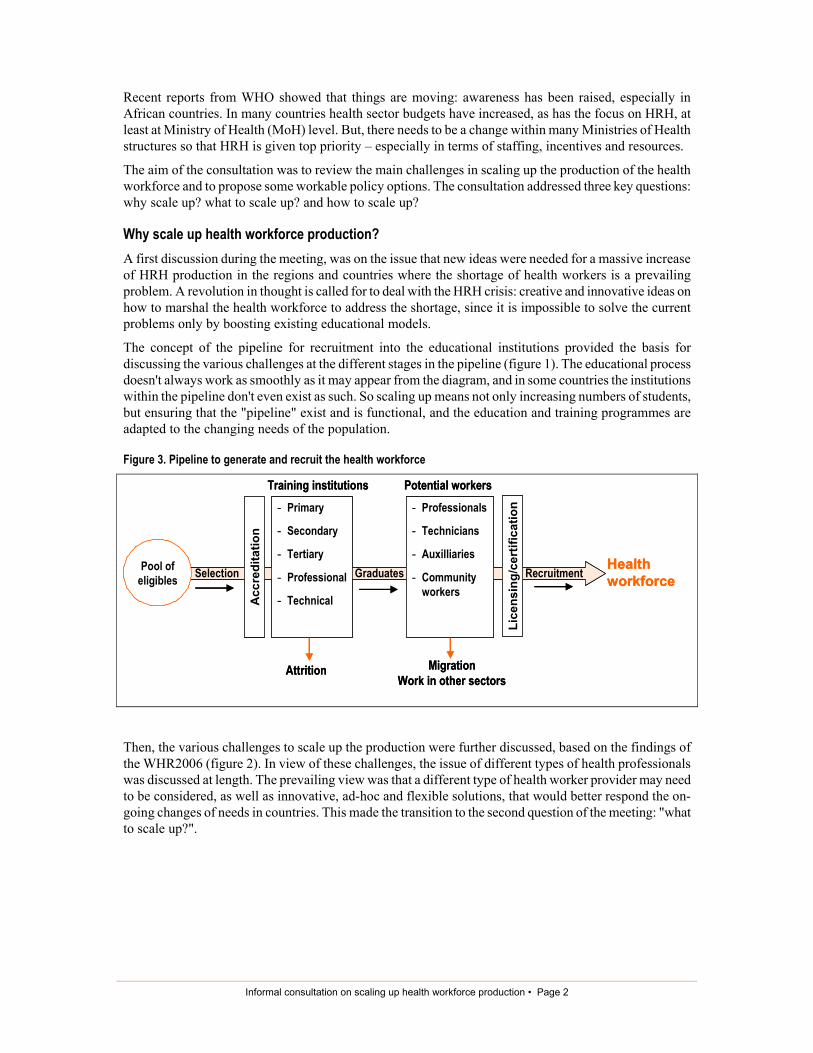
The concept of the pipeline for recruitment into the educational institutions provided the basis for discussing the various challenges at the different stages in the pipeline (figure 1). The educational process doesn't always work as smoothly as it may appear from the diagram, and in some countries the institutions within the pipeline don't even exist as such. So scaling up means not only increasing numbers of students, but ensuring that the "pipeline" exist and is functional, and the education and training programmes are adapted to the changing needs of the population.
Figure 3. Pipeline to generate and recruit the health workforce
Then, the various challenges to scale up the production were further discussed, based on the findings of the WHR2006 (figure 2). In view of these challenges, the issue of different types of health professionals was discussed at length. The prevailing view was that a different type of health worker provider may need to be considered, as well as innovative, ad-hoc and flexible solutions, that would better respond the on-going changes of needs in countries. This made the transition to the second question of the meeting: "what to scale up?".
Pool of eligibles
Acc
redi
tatio
n
- Primary
- Secondary
- Tertiary
- Professional
- Technical
- Professionals
- Technicians
- Auxilliaries
- Community workers
Lice
nsin
g/ce
rtifi
catio
n
Selection Graduates Recruitment
Training institutions Potential workers
Attrition MigrationWork in other sectors
Healthworkforce
Pool of eligibles
Acc
redi
tatio
n
- Primary
- Secondary
- Tertiary
- Professional
- Technical
- Professionals
- Technicians
- Auxilliaries
- Community workers
Lice
nsin
g/ce
rtifi
catio
n
Selection Graduates Recruitment
Training institutions Potential workers
Attrition MigrationWork in other sectors
Healthworkforce

Informal consultation on scaling up health workforce production • Page 3
Figure 2: Challenges to the health workforce production
What to scale-up? With respect to the type of worker to be scaled up and the length of preparation for the role, different experiences were analysed. From the maternal health area for example, two lessons were considered: first, the need to link training strategies to performance and service delivery considerations: "it is about real people in real situations" and secondly, "it's not only about supply: people have expectations, and responding to these is a political imperative". Increasingly, people are seeking out a higher level of professional care, even in a context where they may be losing trust in health professionals. Several case studies were presenting during the meeting, illustrating experiences on scaling up the production of the health workforce at various levels
Case 1. Brazil - PROFAE The Brazilian experience in significantly scaling up of nursing aids, the Programme of Education of Auxiliary Nurses (PROFAE), was presented. The coverage of this programme is national, based on a strong participation in decision making of the municipal and state level authorities. It is a federal initiative aimed at improving health care services at the three levels of the health care delivery system, through upgrading the qualification of nursing personnel.
Schools for these health workers were built in every state of Brazil, 70% of these schools belonging to the public sector. The implementation of this scale-up scheme was made possible by the Ministry of Health (MoH). The government spent USD 370 million, half of which was loaned by the Inter-American Development Bank. Some of the results of this program are presented in box 1.
According to estimates of the MoH, there were about 225,000 workers of medium or elementary levels performing nursing functions without the qualification required by the law, both in the public network and in the private one. PROFAE's goal was to upgrade the qualifications of this contingent in four years (2000-04). Out of these workers, it is estimated that about 46,000 (24%) have no elementary schooling degree, an imperative condition for professional certification as nursing aid. Many of these workers were called "nursing aids", a definition that is not legally acknowledged. Nursing aids and Auxiliary Nurses have a secondary education, i.e. at least 10-12 months training. To get to the next level (Technical Nurse), they needed an additional 12-months training.

Informal consultation on scaling up health workforce production • Page 4
Box 1. Some results of the PROFAE Programme
Case 2: Kenya - AMREF In Kenya, a long-standing NGO (AMREF) developed an important educational scale up operation1. Its purpose was to upgrade 22,000 community health nurses (KECHNs) from enrolled status to registered diploma (KRCHNs) level2. The rationale for the upgrading operation was that there is a chronic shortage of higher level skilled nurses in Kenya and that the majority of nurses at the enrolled level do not possess the necessary skills to effectively serve their communities. It was estimated that with traditional classroom methods it would take over 200 years and cost over USD 50 million at the current production rate of 100 students per year, whereas using e-learning would take 5-7 years at 5% of the cost, with no disruption of services nor impact on the nurses' family life.
In this project, training was delivered through distance education. It was anticipated that at the end of the project, Kenya will have developed a feasible e-Learning solution, designed and tested to upgrade the skills of Kenyan nurses, with a reduction in the time required training, and with the possibility of thus rapidly increasing their numbers. The project offered an enriched learning experience using ICT, and is expected to be a model for replication in other African countries, which are also experiencing chronic shortages of qualified health workers.
Progress to date includes the training of 100 mentors / course coordinators, the establishment of 71 training centres and the upgrading of 3,265 nurses since September 2005. The key challenges were: huge initial investment; obtaining critical 'buy in' by top management of the nursing profession; a shortage of approved sites to conduct clinical training and deployment upon completion is not guaranteed. Retention is a major issue in Kenya as there is no agreed framework for it; however, access to e-learning has helped to retain health workers in their home environment.
Case 3. Cuba and Venezuela Finally, the Cuban and Venezuelan experiences in scaling up the production of physicians was mentioned, although there is still a relative lack of information and evaluation of these experiences. In the 1960s Cuba started to double the number of their physicians. More recently, Cuba opened a Latin American School of Medicine, using existing buildings (a former Navy base), where 10,000 students from developing countries or underserved minorities from developed countries, are being trained as physicians. The aim is that these graduates will return to their communities and provide the much needed community health care
1 A private sector partner, Accenture, paid for the infrastructure, made some donations in kind and gave USD 2 million. 2 A PRN (professional Registered Nurse are also called licensed nurses -Infirmiers Diplome d'Etat. Their education last about 3,4 or more
years in nursing school and lead to a university degree. EN (Enrolled Nurse) also called nurse technician or associated nurse, its education las about 3 to 4 years and leads to an award not equivalent to a university first degree. AN (Auxiliary Nurse) also called assistants are trained in secondary schools, a period of on-the-job training may be included, and sometimes formalised in apprenticeships. The same can be aplayed to the different categories of Midwives.
• 218,244 students enrolled in the Auxiliary Nursing course, with 207,844 students graduated as Auxiliary Nurses • 82,029 enrolled in the Nursing Technician course, with 80,124 graduated as Nursing Technicians • Creation of Technical Professional and National Consulting Boards • Development of a methodology to identify professional competence profiles • Elaboration and agreement of norms to certify professional competence of the auxiliary nurses who completed PROFAE courses • Elaboration and validation of tools for competence evaluation, and performing a pilot-test of the professional competence
certification • Performing studies on health labour and education markets, including monitoring of the nursing labour market • Publication of eight issues of the "Education Journal" • Strengthening and modernization of the Technician Schools of the Brazilian Health System, including creation of 11 new ETSUS
(Technical Schools)

Informal consultation on scaling up health workforce production • Page 5
in these underserved areas. In Venezuela, more than 20,000 medical students receive medical education in micro-schools that are part of the "Barrio Adentro" health service program, which uses already existing physical and teaching resources located in areas that remained until recently underserved by the health system.
After reviewing those scaling-up actions it was evident that the shortage does not only refer to the number of health workers. The existing institutional educational capacity needs to be boosted, by the use of innovative technologies and technical resources that could facilitate more effective and efficient access to education of the targeted and bigger population groups. WHO e-Health experience on ICT for the health workforce was discussed since it is based on a paradigm shift, from health systems focused on curing disease in patients by health professionals in health care facilities, to a focus on the citizen – empowering him/her with information to maintain his/her health wherever (s)he may be.
Case 4. E-health and ICT technologies for health workforce education and training The e-Health experience identified the following priority action areas:
• Legal and ethical issues • e-Health norms and standards • Access to health information • Global Observatory for e-Health • Public private partnerships for ICT in health • ICT for health promotion • ICT for human resources for health • ICT for service delivery.
The last two areas are particularly relevant to this discussion on scaling up the health workforce. Examples of ICT projects like HINARI, the Health Academy and POHLN were presented.
The HINARI program (Health Inter Network Access to Research Initiative) was set up by WHO together with major publishers to enable developing countries to gain access to one of the world's largest collections of biomedical and health literature. Over 3,503 journal titles are now available to health institutions in 113 countries, benefiting many thousands of health workers and researchers, and thus contributing to improved world health.
The Health Academy is about investing in people, especially the younger generation. It brings together technology, health information, and education for the benefits of human development through eLearning. It is health promotion addressed to the population (currently only 1% of the population uses academic health centres) and starts in schools. Consortia are being created in each country to link the schools to the internet. Currently there are 21 schools in Jordan and 24 in Egypt that are part of this project. There are 4,152 students - 35% male, 65% female, from 12 to 17 years old - already enrolled in the project. The students have 1 male mentor and 1 female mentor per school. The interest of this experience is that it could be easily scalable and specific contents could be adapted. The eAfrica Commission through eSchools project is leading it.
POLHN (The Pacific Open Learning Health Net initiative) is aimed at meeting the continuing education needs and standards of practice of health professionals in Pacific Island countries, while remaining in their jobs due to staff shortages and/or overcome costly overseas training. The initiative was supported by the Western Pacific Regional Office of WHO. Learning centres equipped with computers and internet connections in ten Pacific countries enable health personnel, such as nurses, doctors, allied health workers and, health managers to be trained in basic information technology and computer skills so as to access or search for electronic health information or undertake online or distance learning courses. Specific health courses designed to meet training needs of health personnel are developed and delivered through distance learning online modality via interactive website: www.polhn.com or interactive CD-ROMS. Local trainers /mentors support course participants where needed. Self-directed learning contents/modules in print and CD-ROMS are distributed for use in countries without learning centres or to those that cannot access the learning centres. The Commonwealth of Learning maintains a primary site, or portal, for the

Informal consultation on scaling up health workforce production • Page 6
POLHN at http://www.colfinder.org/wolhn to facilitate easy access to relevant international publications and literature, including those on the Internet. POLHN has been a success according to an external evaluation conducted in 2004. There was a strong interest among the participating countries to contribute to its long-term sustainability; the courses were appropriate and useful; there was a desire for more accredited courses; and it contributed to the retention of significant number of workers at their workplaces.
Africa Union - Pan-Africa e-Network involves a collaboration between the Government of India through the African Union countries on the use of tele-education and tele-health. Tele-education is included in initial education and training, continuing professional development and support of the health personnel who was deployed in the service areas. Tele-health was used to provide services beyond the physical reach of employees.
After reviewing those experiences, some lessons and questions were considered:
• institutional capacity needs to be built, especially schools & labs; production capacity includes scaling up the physical bricks & mortar, administration, investing in infrastructure (particularly to support distance learning) and is key to enable scaling up;
• regulatory interventions are a prerequisite; • observatories are crucial: accurate data and information are needed for political decisions; • buy-in from the professional associations is very important; • health worker's career progression following the upgrading must be planned and embedded into the
Government's HRH/public service policy (not just the MoH's); • curriculum development is needed; • should there be more focus on the peoples (i.e. self-care) rather than professionals?
How to scale up health workforce production? A “vision” of scale-up production was exposed:
A health workforce which is matched in number, knowledge and skill sets to the needs of the population and which contributes to the achievement of health outcomes by utilizing a range of innovative methods.
Considering that the main goal for scaling up the production of health workers is the improvement of health outcomes, three possible lines of actions (technical, political and financial) where highlighted (figure 3).
Figure 3. Framework for scaling up the production of health workforce
ScaleScale--up frameworkup frameworkGOAL: HEALTH OUTCOMES
BASIC PACKAGE OF SERVICES
SKILL MIX
"CLOSE-TO-PATIENT HEALTH TEAMS(Defined within country/regional context)
Existing capacity Development of new capacities
-- ResourcesResources-- IncentivesIncentives-- PartnershipsPartnerships
-- AdvocacyAdvocacy-- LeadershipLeadership-- CommitmentCommitment-- LegislationLegislation-- PolicyPolicy-- PartnershipsPartnerships
-- TrainingTraining-- InstitutionsInstitutions-- InfrastructureInfrastructure-- Supportive environmentSupportive environment-- ConnectivityConnectivity-- PartnershipsPartnerships
FINANCIALFINANCIALPOLITICAL POLITICAL TECHNICALTECHNICAL
INDICATOR: MDGs

Informal consultation on scaling up health workforce production • Page 7
Technical component
A comprehensive situational assessment of training institutions is required to ascertain the resources required for training. Considerable technological opportunity exists: identify approaches which are highly efficient, low cost, accessible to population.
The elements for Health Education Institutions needs assessment comprise among other things: the volume /quality /capacity; a rapid time scale; and an evaluation of the local learning economy: where is new investment needed; what is the target of the investment; governance of this investment;
Political component
It is absolutely necessary to bridge health development and education development. The financing landscape is also very problematic, as there are different modalities of how higher education is financed and how graduates are hired into the sector. The regulatory system is non-existent or functioning poorly in many countries. In most countries, academic leadership doesn't have a health systems perspective.
A comprehensive inventory of the roadblocks is therefore needed, as well as to identify how to deal with them. As this is a multi-stakeholder process, it is thus crucial to generate 'buy in' to get the support from different leaders of institutions, and form the "heavyweights" of the political arena. Lastly, it is important to create coherence across governments with respect to foreign policy (migration) and national policy (work across sectors).
Finance component
Costing the scaling up requires a comprehensive analysis, as this must include pre-service and in-service, public and private sector financing, salaries and in-kind, national and international financing. The following diagram was presented, showing that there is a set of required interactions in order to produce a multi-purpose, multi-skilled health worker / team, according to each country policy decisions (figure 4).
In relation with the structure and content of the scaling-up process, the curriculum needed to be: of the highest quality to meet international accreditation standards; standardized and coordinated, i.e.: a common foundation year, problem based, lifelong learning, competency based outcomes patient-centred approach; adapted to meet local needs and issues; focused on range of health workers; using team-based teaching and learning; using an adult learning PBL/CBL designed approach; using substitute teachers, (i.e. seniors teach juniors, patients/ health workers teach students, ICT; developing leaders and managers).

Informal consultation on scaling up health workforce production • Page 8
Figure 4. A different type of health care provider?
The following points and issues were raised in the group feedback:
a. it is crucial to develop leadership programs in academic and health sectors, as well as to promote role models and champions;
b. put in place mechanisms to reduce student attrition, e.g. waive fees, provide food and housing, improve teaching and assessment, train new/existing teachers;
c. tap into the Diaspora; d. improve productivity of training/education – 2nd and 3rd shifts – in existing schools; using
distance education, e-learning; more preceptors/teachers; assess existing materials for use elsewhere; use secondary schools as training sites;
e. connectivity: bulk purchasing of hardware (by country/region); legislation for service providers to offer free bandwidth; offer local services/servers; partnerships with industry (not necessarily using their products) needs to be looked at carefully, go for open source solutions whenever possible.
Closing remarks Scaling up workforce production is a complex undertaking. This meeting brought together a number of specialists to lay out the challenges for rapidly increasing the numbers of health workers in countries with acute shortages, and to set the foundations for a global framework on scaling up health workforce production. The case studies presented served as a basis for discussing the challenges, and the potential options to overcome these challenges. The framework presented stressed out that a three -pronged approach in required, so that technical, political and financial issues are addressed in a cohesive manner.
No country can afford a health systems with insufficient numbers of, or poorly trained, health workers. But the education and training of these workers is an intersectoral business, which has to address in the same time issues related to education, health and the labour market. Therefore, a solution can only be found when all these actors are working together and agreeing on a common way forward. WHO is committed to work with its partners to provide the most-up-to-date policy options and recommendations on how to address the challenges of scaling up health workforce production, to build up national health workforces responsive to population needs.
Multi-purpose,
Close to client,
Multi-skilled, etc
= a person/team
Health Education Institutions
- Delivery models - Assessment - CE - QA
Health needs +
Client
expectations
Continuous Professional Development
- Support models - Career
motivation - Promotion
Certification
Board
- Multi-professional
- Performance
Country CONTEXT
Healthcare CONTEXT

Informal consultation on scaling up health workforce production • Page 9
Annex 1 Informal Consultation on Scaling-up of Health Workforce Production
Geneva, 15–16 November 2006 Programme
Day 1: November 15th Why Scale-Up? Chairperson: Helen McElroy What to Scale-Up? Chairperson: Ian Bates
900 Welcome, objectives and expected outcomes: a new paradigm. M. Dayrit, HRH , Director Advocacy and Partnership for HRH, Francis Omaswa, Director, Global Health Workforce Alliance
945 Discussion, Q & A 1000 Coffee Break
1030 Panel: Experiences in Scaling-up production of health workforce
• International Training Centre, ILO, Turin, Frans Lenglet • PROFAE (Brazil) – Maria Alice Roschke • AMREF, Kenya, Peter Ngatia
Discussion and summary 1145 Vision of a scaled-up health workforce: a new paradigm 1245 Lunch 1400 Conceptual base
Health systems and scaling up health workforce, W Van Lerberghe, WHO
Challenges to health workforce production, H. Mercer, WHO A conceptual framework, Peter Walker, University of Ottawa E-learning, Y. Kwankam, WHO
1530 Coffee Break 1545 Group work: Dimensions of the Scaling-up production framework
1800 Reception
Day 2: November 16 How to Scale-up? Chairperson: Valerie Fleming From framework to action Chairperson: Manuel Dayrit
0900 Summary of Day 1 0915 Presentation: WHA Resolution 59.23 on Rapid Scaling-up of health workers
Group Work: Developing the Framework elements, gaps, strategies, success indicators
1045 Break 1100 Group work 1200 Group Report 1245 Lunch 1400 Implementation Plan Advocacy and implementation strategies
technical working group? Next steps
1730 ADJOURNMENT
Meeting outputs:
Vision for scaling –up health workforce production Critical principles of scaling-up Framework for scaling-up Implementation Strategies
Informal consultation on scaling up health workforce production • Page 10
Annex 2 List of Participants
Temporary Advisers Professor Ian Bates Head of Education School of Pharmacy University of London 29/39 Brunswick Square London WC1N 1AX United Kingdom
Telephone: +44(0)207753 5866 Fax: +44(0)207753 5920 Email: [email protected]
Professor Valerie Fleming School of Nursing Midwifery and Community Health Glasgow Caledonian University Cowcaddens Road Glasgow G4 0BA United Kingdom
Telephone: +44 141 331 3473 Fax: +44 141 331 8399 Email: [email protected]
Dr Helen McElroy Manager, Health Care Professionals Unit Health Human Resources Strategies Division Health Canada Jeanne Mance Building Address Loc 1918C Tunney's Pasture, Ottawa ONK1A 0K9 Canada
Telephone: (613)954 8606 Fax: (613) 954 4994 Email: [email protected]
Dr Peter Ngatia Director for Training AMREF Regional Office P.O. Box 44675 Nairobi Kenya
Telephone: 254 733 696 372 Fax: 254 20 609 518 Email: [email protected]
Mrs Maria Alice Roschke Coordinator, Medical Education Ministry of Health Esplanada dos Ministérios Bloco G Ed. Sede Sala 725, Cep: 70 056 900 Brasilia Brazil
Telephone: +(61) 3315 2189 Fax: +(61) 3315 2862 Email: [email protected]
Dr Anne Snowdon Associate Professor Faculty of Nursing University of Windsor 401 Sunset Ave, Windsor, N9B 3P4 Ontario Canada
Telephone: +(519) 253-3000 Fax: +(519) 973 7084 Email: [email protected]
Dr Peter Walker Faculty of Medicine Dean's Office University of Ottawa 451 Smyth Road Ottawa Canada
Telephone: +(613) 247 0622 Email: [email protected] [email protected] (Dean's Office)

Informal consultation on scaling up health workforce production • Page 11
Other Organizations Dr Frans Lenglet Director of Training ILO International Training Centre Viale Maestri del Lavoro 10 Turin Italy
Telephone: +39-011-693-6651 Fax N°: +39-011-693-6348 Email: [email protected]
World Health Organization
Headquarters Secretariat Mr Jean-Marc Braichet Scientist Department of Human Resources for Health
Telephone: 41227912391 Email: [email protected]
Dr Mario Roberto Dal Poz Coordinator, TEP Department of Human Resources for Health
Telephone: 412213599/12551 Email: [email protected]
Dr Manuel Millar Dayrit Director Department of Human Resources for Health
Telephone: 41227912428/4713 Email: [email protected]
Dr Timothy Evans Assistant Director General Evidence & Information for Policy
Telephone:+4122 7912391 Email: [email protected]
Mr Pierre Benjamin Fouquet Department of Human Resources for Health
Telephone: 41227913554 Email : [email protected]
Ms Genevieve Gray WHO Consultant Department of Human Resources for Health
Telephone: +41227915482 Fax: +4122791 4747 Email: [email protected]
Dr Fatos Hande Harmanci Medical Officer Department of Human Resources for Health
Telephone: 41227913407 Email: [email protected]
Dr S. Kwankam Yunkap Coordinator, KMS Knowledge Management and Sharing
Telephone: 41227912527 Email :[email protected]
Dr Wim Van Lerberghe Coordinator, HSP Health Policy, Development & Services
Telephone: 41227913216 Email : [email protected]
Mr Hugo S. Mercer Scientist Department of Human Resources for Health
Telephone: 41227913749 Email : [email protected]
Dr Francis Gervase Omaswa Special Adviser Department of Human Resources for Health
Telephone: 41227915473 Email: [email protected]
Telephone: 41227911049 Dr Jean Yan Chief Scientist for Nursing & Midwifery Department of Human Resources for Health
Email: [email protected]