infective conjunctivitis its pathogenesis, management...
TRANSCRIPT
Chapter 2
Infective Conjunctivitis – Its Pathogenesis,Management and Complications
Adnaan Haq, Haseebullah Wardak andNarbeh Kraskian
Additional information is available at the end of the chapter
http://dx.doi.org/10.5772/52462
1. Introduction
The aims of this chapter are to briefly discuss infective conjunctivitis, its subtypes and itstreatment. Other forms of conjunctivitis will also be considered and discussed in this chap‐ter, namely, neonatal conjunctivitis, conjunctivitis in the immunocompromised. A compre‐hensive assessment of the various treatments of conjunctivitis will also be discussed.
Conjunctivitis is a term broadly used to describe an inflammation of the conjunctiva. Con‐junctivitis may be split into four main aspects; bacterial, viral, allergic and irritant. Infectiveconjunctivitis, namely bacterial and viral will be discussed in this chapter in details.
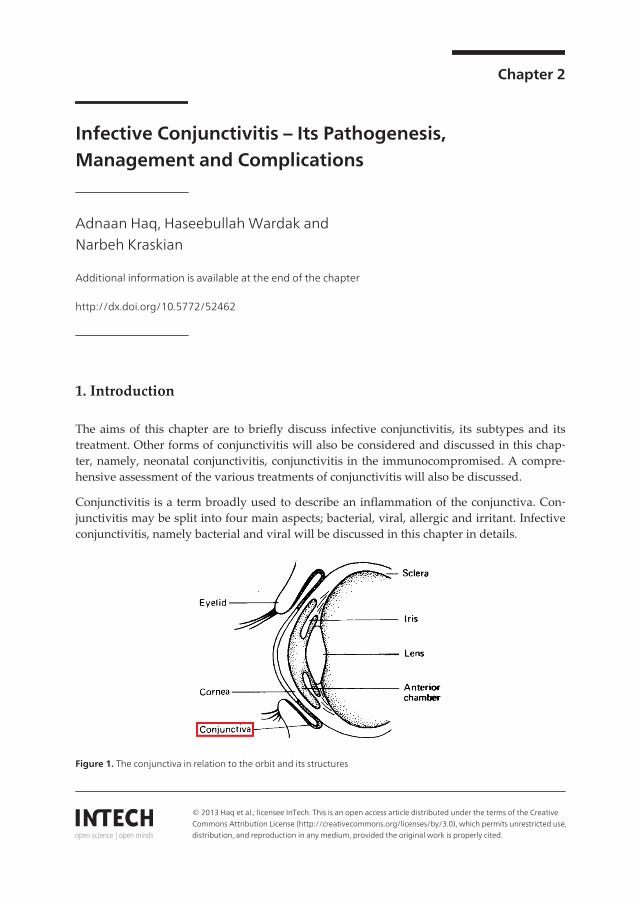
Figure 1. The conjunctiva in relation to the orbit and its structures
© 2013 Haq et al.; licensee InTech. This is an open access article distributed under the terms of the CreativeCommons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use,distribution, and reproduction in any medium, provided the original work is properly cited.
1.1. Anatomy of the conjunctiva
The conjunctiva is the fine mucous membrane which covers and joins the anterior surface ofthe eyeball to the posterior surface of eyelid. This translucent membrane lines the white part ofthe eye starting at the edge of the cornea (limbus) and runs behind the eye to cover the anteriorpart of the sclera. It then flows, loops forward, and forms the inside surface of the eyelids. Atthe medial canthus the conjunctiva fold thickens, which is called the semilunar fold.
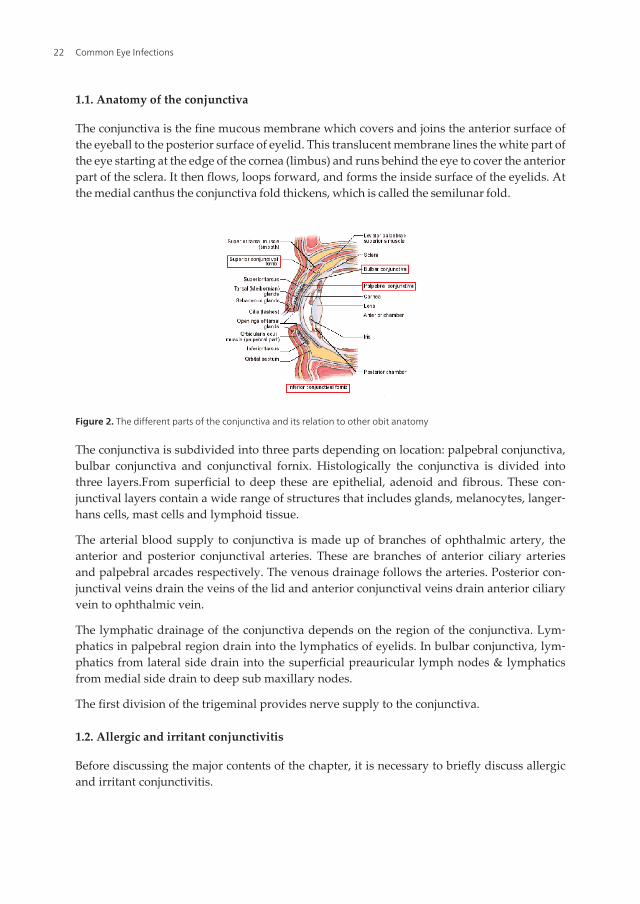
Figure 2. The different parts of the conjunctiva and its relation to other obit anatomy
The conjunctiva is subdivided into three parts depending on location: palpebral conjunctiva,bulbar conjunctiva and conjunctival fornix. Histologically the conjunctiva is divided intothree layers.From superficial to deep these are epithelial, adenoid and fibrous. These con‐junctival layers contain a wide range of structures that includes glands, melanocytes, langer‐hans cells, mast cells and lymphoid tissue.
The arterial blood supply to conjunctiva is made up of branches of ophthalmic artery, theanterior and posterior conjunctival arteries. These are branches of anterior ciliary arteriesand palpebral arcades respectively. The venous drainage follows the arteries. Posterior con‐junctival veins drain the veins of the lid and anterior conjunctival veins drain anterior ciliaryvein to ophthalmic vein.
The lymphatic drainage of the conjunctiva depends on the region of the conjunctiva. Lym‐phatics in palpebral region drain into the lymphatics of eyelids. In bulbar conjunctiva, lym‐phatics from lateral side drain into the superficial preauricular lymph nodes & lymphaticsfrom medial side drain to deep sub maxillary nodes.
The first division of the trigeminal provides nerve supply to the conjunctiva.
1.2. Allergic and irritant conjunctivitis
Before discussing the major contents of the chapter, it is necessary to briefly discuss allergicand irritant conjunctivitis.
Common Eye Infections22
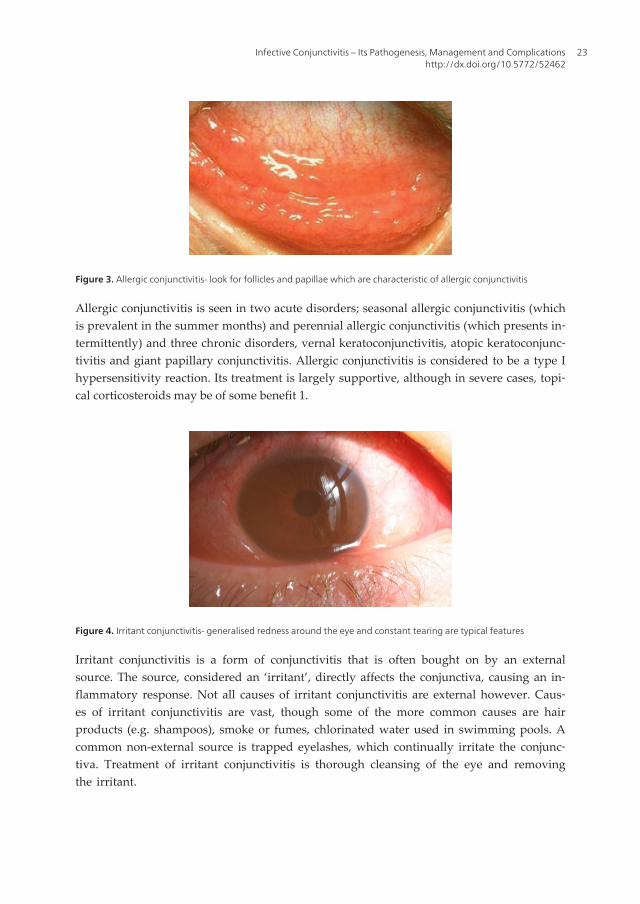
Figure 3. Allergic conjunctivitis- look for follicles and papillae which are characteristic of allergic conjunctivitis
Allergic conjunctivitis is seen in two acute disorders; seasonal allergic conjunctivitis (whichis prevalent in the summer months) and perennial allergic conjunctivitis (which presents in‐termittently) and three chronic disorders, vernal keratoconjunctivitis, atopic keratoconjunc‐tivitis and giant papillary conjunctivitis. Allergic conjunctivitis is considered to be a type Ihypersensitivity reaction. Its treatment is largely supportive, although in severe cases, topi‐cal corticosteroids may be of some benefit 1.
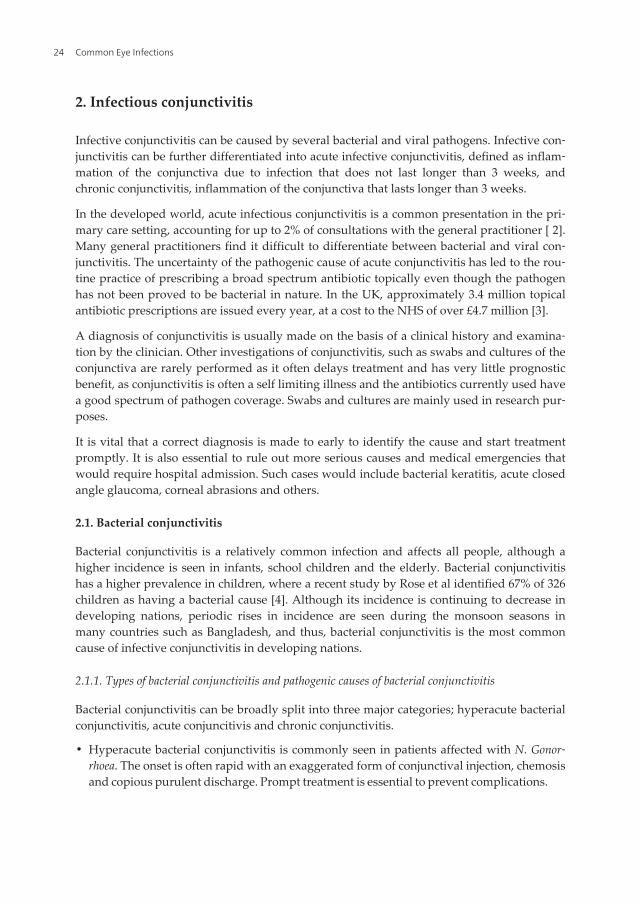
Figure 4. Irritant conjunctivitis- generalised redness around the eye and constant tearing are typical features
Irritant conjunctivitis is a form of conjunctivitis that is often bought on by an externalsource. The source, considered an ‘irritant’, directly affects the conjunctiva, causing an in‐flammatory response. Not all causes of irritant conjunctivitis are external however. Caus‐es of irritant conjunctivitis are vast, though some of the more common causes are hairproducts (e.g. shampoos), smoke or fumes, chlorinated water used in swimming pools. Acommon non-external source is trapped eyelashes, which continually irritate the conjunc‐tiva. Treatment of irritant conjunctivitis is thorough cleansing of the eye and removingthe irritant.
Infective Conjunctivitis – Its Pathogenesis, Management and Complicationshttp://dx.doi.org/10.5772/52462
23
2. Infectious conjunctivitis
Infective conjunctivitis can be caused by several bacterial and viral pathogens. Infective con‐junctivitis can be further differentiated into acute infective conjunctivitis, defined as inflam‐mation of the conjunctiva due to infection that does not last longer than 3 weeks, andchronic conjunctivitis, inflammation of the conjunctiva that lasts longer than 3 weeks.
In the developed world, acute infectious conjunctivitis is a common presentation in the pri‐mary care setting, accounting for up to 2% of consultations with the general practitioner [ 2].Many general practitioners find it difficult to differentiate between bacterial and viral con‐junctivitis. The uncertainty of the pathogenic cause of acute conjunctivitis has led to the rou‐tine practice of prescribing a broad spectrum antibiotic topically even though the pathogenhas not been proved to be bacterial in nature. In the UK, approximately 3.4 million topicalantibiotic prescriptions are issued every year, at a cost to the NHS of over £4.7 million [3].
A diagnosis of conjunctivitis is usually made on the basis of a clinical history and examina‐tion by the clinician. Other investigations of conjunctivitis, such as swabs and cultures of theconjunctiva are rarely performed as it often delays treatment and has very little prognosticbenefit, as conjunctivitis is often a self limiting illness and the antibiotics currently used havea good spectrum of pathogen coverage. Swabs and cultures are mainly used in research pur‐poses.
It is vital that a correct diagnosis is made to early to identify the cause and start treatmentpromptly. It is also essential to rule out more serious causes and medical emergencies thatwould require hospital admission. Such cases would include bacterial keratitis, acute closedangle glaucoma, corneal abrasions and others.
2.1. Bacterial conjunctivitis
Bacterial conjunctivitis is a relatively common infection and affects all people, although ahigher incidence is seen in infants, school children and the elderly. Bacterial conjunctivitishas a higher prevalence in children, where a recent study by Rose et al identified 67% of 326children as having a bacterial cause [4]. Although its incidence is continuing to decrease indeveloping nations, periodic rises in incidence are seen during the monsoon seasons inmany countries such as Bangladesh, and thus, bacterial conjunctivitis is the most commoncause of infective conjunctivitis in developing nations.
2.1.1. Types of bacterial conjunctivitis and pathogenic causes of bacterial conjunctivitis
Bacterial conjunctivitis can be broadly split into three major categories; hyperacute bacterialconjunctivitis, acute conjuncitivis and chronic conjunctivitis.
• Hyperacute bacterial conjunctivitis is commonly seen in patients affected with N. Gonor‐rhoea. The onset is often rapid with an exaggerated form of conjunctival injection, chemosisand copious purulent discharge. Prompt treatment is essential to prevent complications.
Common Eye Infections24
• Acute bacterial conjunctivitis is the most commonly seen bacterial conjunctivitis and oftenpresents with a typical presentation, time course and prognosis. In a study done by Weisset al, the most common pathogens in acute bacterial conjunctivitis were Staphylococcusaureus, Haemophilus influenzae, streptococcus pneumoniae, and Moraxella catarrhalis, whereasin an older study done by Gigilotti et al, Chlamydia trachomatis was also commonly foundin infected patients [5, 6].
• Chronic bacterial conjunctivitis, ie, red eye with purulent discharge persisting for longerthan a few weeks, is generally caused by Chlamydia trachomatis or is associated with anidus for infection such as in dacryocystitis [7].
In certain bacterial conjunctivitis, it is essential to identify a pathogen. As mentioned, mostcauses of conjunctivitis are diagnosed and treated on a clinical exam basis, but in patientswho are particularly susceptible such as neonates or immunodeficient patients, a microbio‐logical diagnosis must be made to exclude harmful pathogens such as N.gonorrheae, Listeriamonocytogenes, Corynobacterium diptheriae and certain members of the Haemophilus group.These pathogens contain proteolytic enzymes which may cause long term damage to the pa‐renchyma of the conjunctiva.
2.1.2. Signs and symptoms of bacterial conjunctivitis
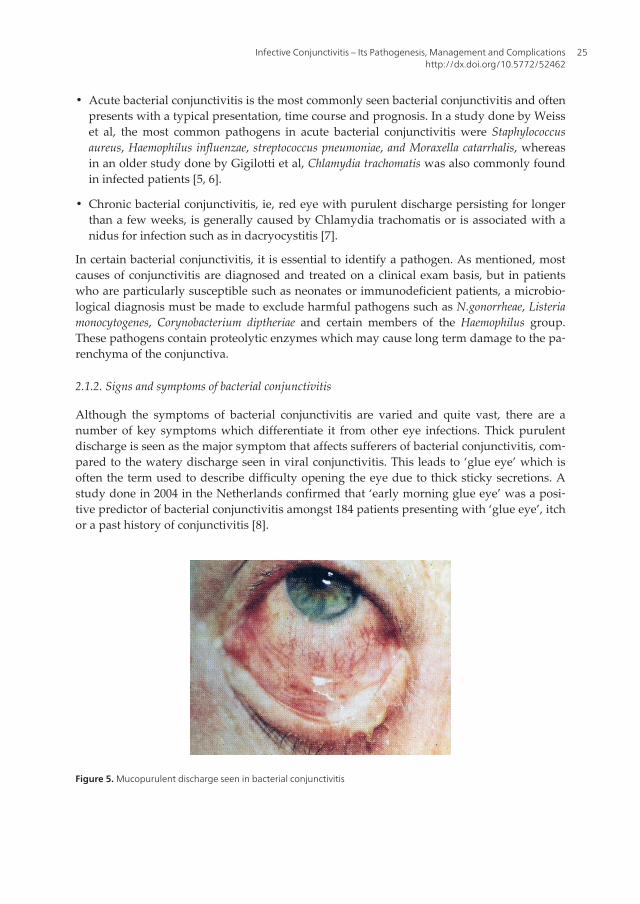
Although the symptoms of bacterial conjunctivitis are varied and quite vast, there are anumber of key symptoms which differentiate it from other eye infections. Thick purulentdischarge is seen as the major symptom that affects sufferers of bacterial conjunctivitis, com‐pared to the watery discharge seen in viral conjunctivitis. This leads to ‘glue eye’ which isoften the term used to describe difficulty opening the eye due to thick sticky secretions. Astudy done in 2004 in the Netherlands confirmed that ‘early morning glue eye’ was a posi‐tive predictor of bacterial conjunctivitis amongst 184 patients presenting with ‘glue eye’, itchor a past history of conjunctivitis [8].
Figure 5. Mucopurulent discharge seen in bacterial conjunctivitis
Infective Conjunctivitis – Its Pathogenesis, Management and Complicationshttp://dx.doi.org/10.5772/52462
25
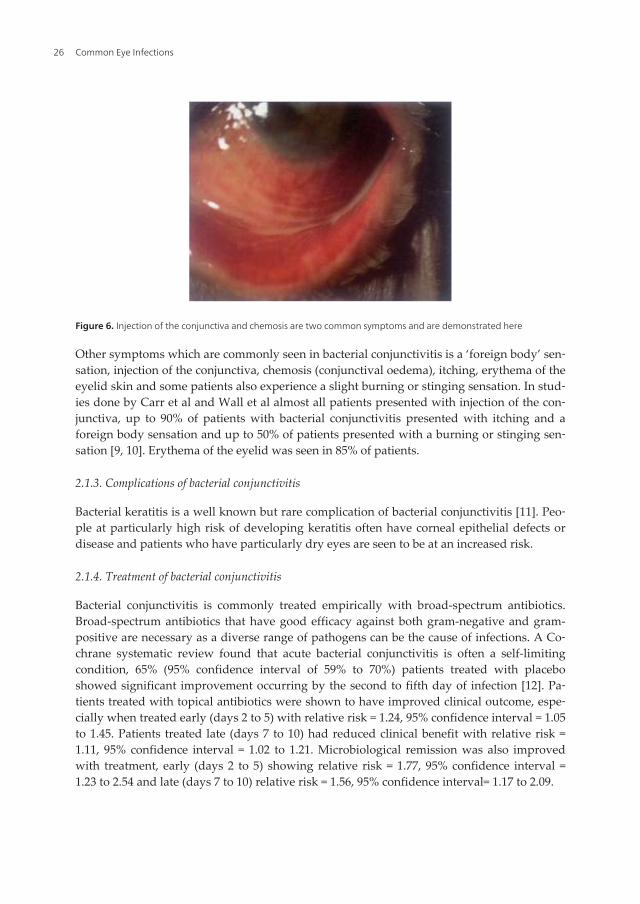
Figure 6. Injection of the conjunctiva and chemosis are two common symptoms and are demonstrated here
Other symptoms which are commonly seen in bacterial conjunctivitis is a ‘foreign body’ sen‐sation, injection of the conjunctiva, chemosis (conjunctival oedema), itching, erythema of theeyelid skin and some patients also experience a slight burning or stinging sensation. In stud‐ies done by Carr et al and Wall et al almost all patients presented with injection of the con‐junctiva, up to 90% of patients with bacterial conjunctivitis presented with itching and aforeign body sensation and up to 50% of patients presented with a burning or stinging sen‐sation [9, 10]. Erythema of the eyelid was seen in 85% of patients.
2.1.3. Complications of bacterial conjunctivitis
Bacterial keratitis is a well known but rare complication of bacterial conjunctivitis [11]. Peo‐ple at particularly high risk of developing keratitis often have corneal epithelial defects ordisease and patients who have particularly dry eyes are seen to be at an increased risk.
2.1.4. Treatment of bacterial conjunctivitis
Bacterial conjunctivitis is commonly treated empirically with broad-spectrum antibiotics.Broad-spectrum antibiotics that have good efficacy against both gram-negative and gram-positive are necessary as a diverse range of pathogens can be the cause of infections. A Co‐chrane systematic review found that acute bacterial conjunctivitis is often a self-limitingcondition, 65% (95% confidence interval of 59% to 70%) patients treated with placeboshowed significant improvement occurring by the second to fifth day of infection [12]. Pa‐tients treated with topical antibiotics were shown to have improved clinical outcome, espe‐cially when treated early (days 2 to 5) with relative risk = 1.24, 95% confidence interval = 1.05to 1.45. Patients treated late (days 7 to 10) had reduced clinical benefit with relative risk =1.11, 95% confidence interval = 1.02 to 1.21. Microbiological remission was also improvedwith treatment, early (days 2 to 5) showing relative risk = 1.77, 95% confidence interval =1.23 to 2.54 and late (days 7 to 10) relative risk = 1.56, 95% confidence interval= 1.17 to 2.09.
Common Eye Infections26

An open, randomized and controlled study by Everitt et al investigated 307 adults and chil‐dren with suspected infective conjunctivitis using three different treatment methods: notreatment, delayed topical treatment and immediate topical chloramphenicol treatment [13].The varying treatments did not affect the severity of symptoms experienced within the firstthree days of infection. However, patients with moderate symptoms who were treated im‐mediately with topical chloramphenicol had a reduced duration of symptoms with an aver‐age of 3.3 days whilst patients that received no treatment had 4.9 days duration.
Rietveld et al carried out a double-blind randomized and placebo controlled study in a pri‐mary care setting. The efficacy of fusidic acid gel was compared to a placebo gel in 163 adultpatients presenting with a red eye and mucopurulent discharge [14]. After 7 days the treat‐ments were evaluated with clinical cure being found in 62% of patients on fusidic acid geland 59% of patients on placebo gel. The study found that the severity of symptoms and theduration of symptoms were not significantly different in either group. In conclusion, withthe limited evidence the authors produced, they did not support the current practice of pre‐scribing empirical antibiotics.
The majority of doctors actively treat uncomplicated acute bacterial conjunctivitis with em‐pirical topical antibiotics at diagnosis. There are several other options available including:delaying treatment for 5 days and begin treatment if no sign of improvement and to treatpatients who have clinical features associated with a bacterial cause. Studies comparing theeffectiveness of different antibiotics recommended for use in suspected bacterial conjunctivi‐tis have shown similar levels of effectiveness. Therefore, it is important to consider local bac‐terial resistance and cost-effectiveness of the antibiotics being prescribed [15]. All antibioticcourses should be taken for 7-10 days. Compliance with the length of time the antibioticsareprescribed for is particularly important to help prevent resistance developing.
The first line treatment in mild to moderate bacterial conjunctivitis is either Trimethoprim-Pol‐ymyxin B (Polytrim) solution, Erythromycin 0.5% ointment, or Azithromycin drops. Alterna‐tives to these antibiotics are bacitracin ointment and sulfacetamide drops. In moderate tosevere infections, or antibiotic-resistant infections and in immunocompromised patients, fluo‐roquinolones are recommended. These include: ofloxacin, ciprofloxacin, levofloxacin, moxi‐floxacin and gatifloxacin. Chlamydial conjunctivitis requires oral antibiotics alongside atopical antibiotic to treat the systemic infection alongside the ophthalmic manifestation. Theoral antibiotic options include Azithromycin, doxycycline, or erythromycin. These are given incombination with Azithromycin or erythromycin drops for 2 to 3 weeks [16]. In addition, pa‐tients should be advised to take several precautions to help prevent spread of infection. Pa‐tients should wash their hands regularly and thoroughly, especially after touching anyinfected secretions. Furthermore, patients should avoid sharing towels, pillows, or utensils.
Studies have shown that treatment with topical antibiotics shortens the duration of disease,prevents spread of infection, reduces the rate of recurrence, and decreases the risk of com‐plications that effect vision [17].However, there has been controversy in recent years overthe use of empirical antibiotics and its role in an evidently self-limiting disease with the clin‐ical outcome being only marginally favourable to taking no antibiotics. There has been in‐creasing antibiotic resistance especially among the older class of antibiotics that have been
Infective Conjunctivitis – Its Pathogenesis, Management and Complicationshttp://dx.doi.org/10.5772/52462
27
used extensively such as chloramphenicol, sulphonamides, polymyxins, bacitracin, amino‐glycosides and early generation fluoroquinolones. The efficacy of these drugs has reducedto a combination of resistance and narrow spectrum of activity [18, 19].The newer genera‐tion of fluoroquinolones, such as gatifloxacin and moxifloxacin, have a greater range of ac‐tivity and efficacy against common pathogens of the eye [20].Specifically, they have better invitro efficacy over the older generation fluoroquinolones against gram positive pathogens.However, the efficacy was not greater with Haemophilus influenza isolates [21]. The OcularTracking Resistance in the U.S. Today (TRUST) initiative annually monitors the in vitro sus‐ceptibility of common ocular pathogens; Staphylococcus aureus, Streptococcus pneumonia,and Haemophilus influenzae. Between 2000 and 2005 there was a 12.1% increase in the inci‐dence of methicillin-resistant Staphylococcus aureus (MRSA). Moreover, greater than 80% ofthe MRSA strains were also resistant to fluoroquinolones [22, 23].
2.1.5. Prognosis of bacterial conjunctivitis
The prognosis of bacterial conjunctivitis is normally very good with the correct and prompttreatment of the infection. In many cases, spontaneous remission, without a cure, is seen. Ina study done by Sheikh and Hurwitz et al, spontaneous cure occurred in 60% of patientswithin 1-2 weeks [24]. However, with prompt antibiotic treatment, the treatment time is sig‐nificantly reduced.
2.2. Viral conjunctivitis
Viral conjunctivitis is a common infection amongst the Western population, and is often as‐sociated with other infections around the body. Due to the contiguity with the respiratorytract anatomy, viral upper respiratory tract infections are a common cause of secondary vi‐ral conjunctivitis.
Most cases of viral conjunctivitis are mild. Days 3-5 of infection are often the worst, but theinfection will usually clear up in 7–14 days without treatment and without any long-termconsequences. In some cases, viral conjunctivitis can take 2-3 weeks or more to clear up, es‐pecially if complications arise.
2.2.1. Pathogens causing viral conjunctivitis
Much unlike bacterial conjunctivitis, there are many pathogens associated with viral con‐junctivitis, although the majority of cases of viral conjunctivitis are encompassed by a fewcommon pathogens. The specific viruses are much dependant on the geographical area inthe world. In a study done in the Far East countries of Japan, Korea and Taiwan the mostcommon pathogens isolated from 1105 cases were adenovirus 8 and enterovirus 70. Other vi‐ruses also identified were adenoviruses 19 and 37 [25]. Similarly, the causes of viral conjuncti‐vitis in the Western countries are mainly adenoviruses, though adenovirus 13 seems to be thedominant strain in these countries.
Other rarer causes of viral conjunctivitis include herpes simplex virus, herpes zoster virus andthe measles virus. Although less commonly seen, it is essential to identify herpes and measles
Common Eye Infections28
viruses early to ensure prompt treatment, to prevent any long term complications associatedwith these viruses.
A recent study also showed outbreaks of the avian influenza viruses in patients, although thismay possibly be linked to the recent outbreaks of the virus in humans.
2.2.2. Signs and symptoms of viral conjunctivitis
As with bacterial conjunctivitis, a diagnosis of viral conjunctivitis is often made by the gen‐eral practitioner on the basis of a history and examination. However, due to the overlap insymptoms between viral and bacterial conjunctivitis, it is often difficult to ascertain viralfrom bacterial conjunctivitis.
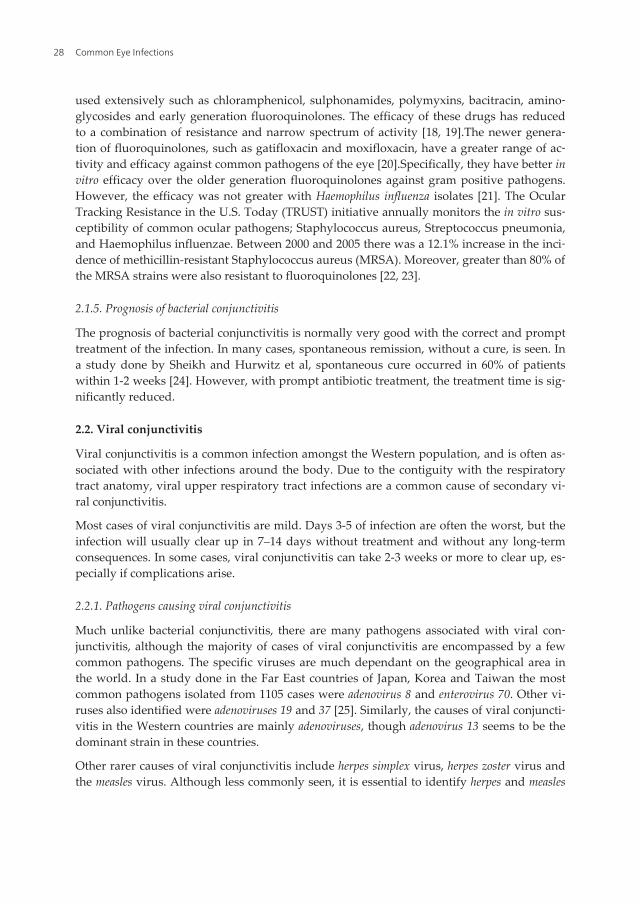
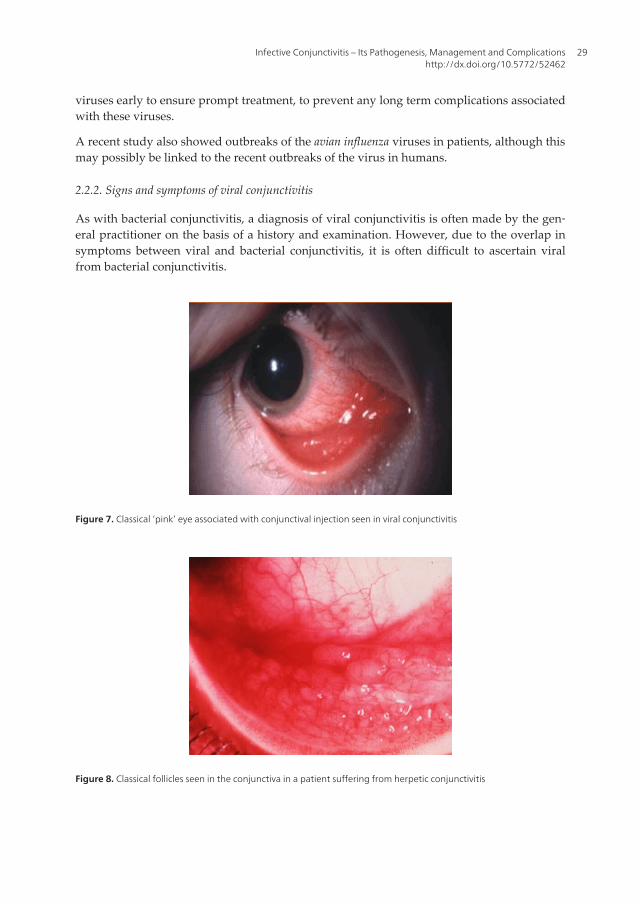
Figure 7. Classical ‘pink’ eye associated with conjunctival injection seen in viral conjunctivitis
Figure 8. Classical follicles seen in the conjunctiva in a patient suffering from herpetic conjunctivitis
Infective Conjunctivitis – Its Pathogenesis, Management and Complicationshttp://dx.doi.org/10.5772/52462
29
The key symptom of viral conjunctivitis is ‘pink eye’. This shows a fine, diffuse pinkness ofthe conjunctiva, which is often easily mistaken for the ciliary injection of iritis. Other symp‐toms associated with viral conjunctivitis include discharge which is often clear and watery.This is often the most discernible difference between bacterial and viral conjunctivitis.
A history of itchy eyes is also suggestive of viral conjunctivitis, although it is a symptom al‐so associated with irritant and allergic conjunctivitis. Rarer symptoms associated with sim‐ple adenovirus viral conjunctivitis include foreign body sensation, ocular discomfort,excessive tearing and sticky eyelids which are worse in the morning.
Herpes simplex conjunctivitis is usually unilateral. Symptoms include a red eye, photophobia,eye pain and mucoid discharge. There may be periorbital vesicles, and a conjunctivalbranching (dendritic) pattern of fluorescein staining makes the diagnosis.
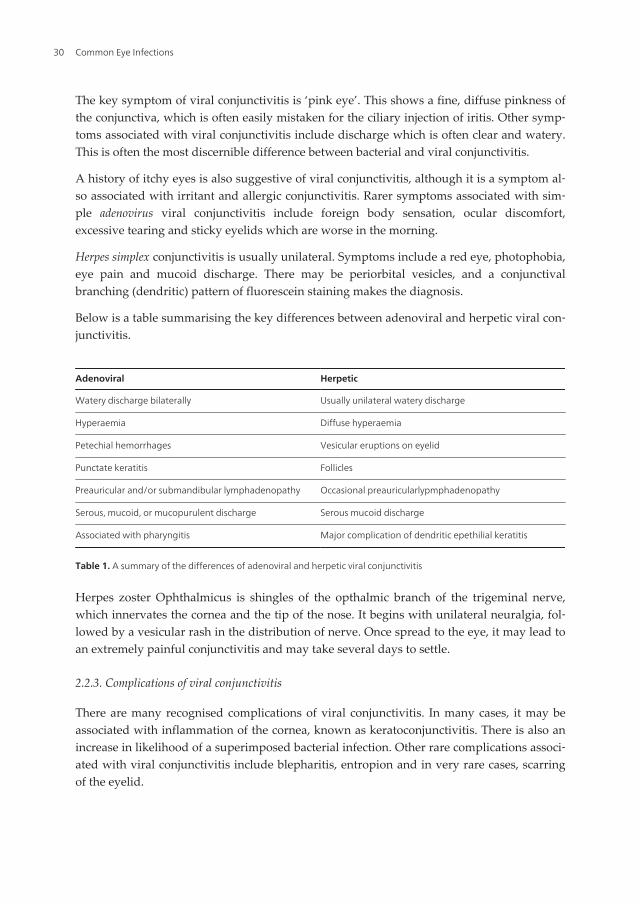
Below is a table summarising the key differences between adenoviral and herpetic viral con‐junctivitis.
Adenoviral Herpetic
Watery discharge bilaterally Usually unilateral watery discharge
Hyperaemia Diffuse hyperaemia
Petechial hemorrhages Vesicular eruptions on eyelid
Punctate keratitis Follicles
Preauricular and/or submandibular lymphadenopathy Occasional preauricularlypmphadenopathy
Serous, mucoid, or mucopurulent discharge Serous mucoid discharge
Associated with pharyngitis Major complication of dendritic epethilial keratitis
Table 1. A summary of the differences of adenoviral and herpetic viral conjunctivitis
Herpes zoster Ophthalmicus is shingles of the opthalmic branch of the trigeminal nerve,which innervates the cornea and the tip of the nose. It begins with unilateral neuralgia, fol‐lowed by a vesicular rash in the distribution of nerve. Once spread to the eye, it may lead toan extremely painful conjunctivitis and may take several days to settle.
2.2.3. Complications of viral conjunctivitis
There are many recognised complications of viral conjunctivitis. In many cases, it may beassociated with inflammation of the cornea, known as keratoconjunctivitis. There is also anincrease in likelihood of a superimposed bacterial infection. Other rare complications associ‐ated with viral conjunctivitis include blepharitis, entropion and in very rare cases, scarringof the eyelid.
Common Eye Infections30

Figure 9. Herpes simplex keratitis, demonstrated here via fluorescein staining
The most serious complication of viral conjunctivitis is herpes simplex keratitis, a corneal ul‐cer, which can ultimately lead to blindness. This is an extremely rare side effect of viral con‐junctivitis and requires immediate transfer to hospital and review by the ophthalmologists.
2.2.4. Treatment of viral conjunctivitis
Viral conjunctivitis is a self-limiting disease that usually resolves within two weeks of onset ofsymptoms and does not require treatment with antiviral medication. There is no evidence sup‐porting the use of anti-viral medication and their efficacy has not been proven. However, as ahighly contagious disease, there is a need to make infected patients aware of good hygienepractices to prevent further spread. Viral conjunctivitis is transmitted through direct contact,therefore, hands should be thoroughly washed regularly, and infected patients should notshare pillows, towels and other utensils [26].The highly contagious nature of viral conjunctivi‐tis, especially adenovirus, makes it necessary for infected patients to avoid going to work orschool for 5 days to 2 weeks. Contagiousness of adenovirus conjunctivitis has been shown to bereduced in an in vitro study using the topical anti-viral agent povidone-iodine. Povidone-io‐dine at a concentration of 1:10 (0.8%) is particularly effective against free adenovirus, eradicat‐ing all of them within 10 minutes with little cytotoxicity [27]. In addition, patients with contactlenses should avoid using them until the conjunctivitis resolves and last dose of any treatmenthaving been taken over 24 hours ago [28]. Treatment for viral conjunctivitis is supportive, in‐volving cold compresses, ocular decongestants, and artificial tears for symptomatic relief. Inpatients with high susceptibility of contracting bacterial infections an antibiotic may be givento prevent a bacterial superinfection occurring.If a pseudomembrane or corneal subepithelialinfiltrates develop then a topical corticosteroid may be given alongside the other non-pharma‐cological treatments outlined earlier. Immediate referral to an ophthalmologist should be con‐sidered in patients with a psuedomembrane or corneal subepithelial infiltrate. Immediatereferral is necessary in patients with hyperacute conjunctivitis or those who have corneal in‐volvement including ulceration and herpetic keratitis.
Infective Conjunctivitis – Its Pathogenesis, Management and Complicationshttp://dx.doi.org/10.5772/52462
31
2.2.5. Prognosis of viral conjunctivitis
Viral conjunctivitis is extremely contagious and remains so for 14 days, which also is oftenhow long the symptoms remain.
The prognosis is very good for viral conjunctivitis. It resolves completely within 2 weeks ofthe ‘pink eye’ onset and there are rarely any long term complications or problems associatedwith viral conjunctivitis [29].
3. Conjunctivitis in the immunocompromised
Conjunctivitis in the immunocompromised is something that is often overlooked by the gen‐eral practioner. However, it is essential to properly investigate conjunctivitis in immunodefi‐cient patients as they are more likely to suffer from long term complications such asdendritic ulcers and corneal damage.
3.1. Epidemiology and conjunctival microvascular disease associated with HIV
Up to 75% of HIV infected patients have suffered from conjunctivitis. Most will exhibit mi‐crovascular changes of the conjunctiva, often the inferior perilimbal bulbar conjunctiva.These changes are often seen as capillary dilations, short irregular vessels and a granular ap‐pearance of blood column within the vessels.
In some cases, there have been reports of direct infiltration of the vascular endothelial cellsof the conjunctiva being infiltrated by the HIV virus, which causes a deposition of immunecomplexes within the conjunctiva, causing conjunctivitis.
3.2. Infections causing conjunctivitis in the immunocompromised
Most conjunctivitis reports in the immunocompromised, especially HIV, have shown staphy‐lococci to be the main infective agent, with coagulase negative staphylococci (mostly staphylococ‐cal epidermidis the majority) accounting for most of the cases. The major other normal floraorganism which cause infection in immunocompromised patients include cornybacteriumpseudo/diphtherticum(found in the nasopharynx) and certain members of the Haemophilusgroup. Isolated cases of neisseriameningitidisand the measles virus have also been found in im‐munocompromised patients, although no study has yet shown a direct link between thesetwo organisms and conjunctivitis in the immunocompromised.
Opportunistic infections may also cause conjunctivitis. Below are common pathogens thathave been identified as opportunistic infections causing conjunctivitis:
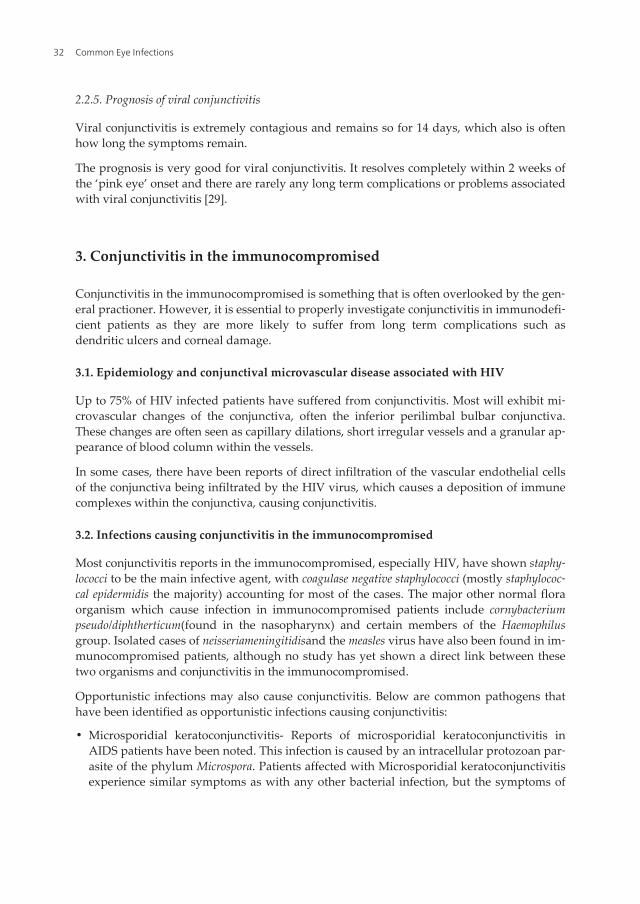
• Microsporidial keratoconjunctivitis- Reports of microsporidial keratoconjunctivitis inAIDS patients have been noted. This infection is caused by an intracellular protozoan par‐asite of the phylum Microspora. Patients affected with Microsporidial keratoconjunctivitisexperience similar symptoms as with any other bacterial infection, but the symptoms of
Common Eye Infections32
photophobia and extreme redness are also present. There may also be bilateral conjuncti‐val hyperaemia with diffuse coarse white infiltrates, conjunctival hypertrophy and ero‐sions of the corneal epithelium [30].
Microsporidial keratoconjunctivitis should not be overlooked in HIV patients because itrarely responds to conventional topical antivirals or antibacterials. In some cases, antiproto‐zoal medication has also been reported as ineffective. A recent study found that Fumagillin(Fumidin B) is the treatment with most positive outcome in HIV patients with Microspori‐dial keratoconjunctivitis [31].
Figure 10. Conjunctivitis in a patient suffering from AIDS
• Molluscum contagiosum-Although rarely affecting the conjunctiva even in immunocom‐promised individuals, molluscum contagiosum has been noted to primarily affect theconjunctiva and also cause secondary conjunctival inflammation during infection. In onecase report, a nodule of molluscum contagiosum was noted on the bulbar conjunctiva ona 34 year old man with AIDS [32]. However, in most cases of patients in an immunocom‐promised state with molluscum contagiosum, the conjunctiva is secondarily affected,causing an associated follicular conjunctivitis [33].
Treatment of primarily conjuctival infection of molluscum contagiosum is via cryotherapyand/or surgery, although this has shown to provide only limited long term correction inHIV patients.
• Fungal infections- Fungal infections affecting the conjunctiva are rare. In immunocompro‐mised patients, the cornea is often affected, causing a keratitis to develop. This can how‐ever, cause a secondary conjunctivitis. Studies have shown that Cryptococcus and Candidaalbicans are the most common pathogens affecting the cornea and conjunctiva in immuno‐compromised patients.
Infective Conjunctivitis – Its Pathogenesis, Management and Complicationshttp://dx.doi.org/10.5772/52462
33
Fortunately, the treatment is very effective for fungal infections. Although hospital admis‐sion is required in patients affected with keratitis, topical amphotericin B or natamycin, sub‐conjunctival miconazole and oral ketoconazole are proven effective antifungals.
4. Neonatal conjunctivitis
Neonatal conjunctivitis also known as ophthalmia neonatorum is inflammation of the con‐junctiva occurring in the first month of life. This condition is caused by a number of differ‐ent pathogens. These include bacteria, viruses and chemical agents. In recent timesprophylaxis has led to decreased morbidity in the developed world. However, it is still asignificant cause of ocular morbidity, blindness and even death in the developing world.
4.1. Epidemiology of neonatal conjunctivitis
The incidence of ophthalmia neonatorum is dependent on many different factors. The mainrisk factor for ophthalmia neonatorum of infective origin is the presence of a sexually trans‐mitted disease in the mother. The organism usually infects the neonate through direct con‐tact as it passes through the birth canal. Therefore, incidence is high in areas with highrates of sexually transmitted disease [34]. Prolonged rupture of membranes at the time ofdelivery is also thought to increase the risk of infection. It is also dependent on socioeco‐nomic factors; incidence varies in highly developed countries with good prenatal care com‐pared to the developing parts of the world [35]. The offending pathogens varygeographically due to the differences in the prevalence of maternal infection and the use ofprophylaxis. In US and Europe the incidence has been reported 1-2% depending on the so‐cioeconomic character of the area. However in other parts of the world the incidence is re‐ported to be as high as 17%. In recent studies in Pakistanthe incidence has been 17% and inKenya as high 23% [36, 37].
There has been a sharp decrease in the incidence of ophthalmia neonatorum in the past fewdecades in the developed countries due to many reasons. In 1800s, prophylaxis (silver ni‐trate) for ophthalmia neonatorum in the developed countries was used for the first time.Since then there has been gradual decrease in incidence. Better prenatal care has also led todetection and treatment of sexually transmitted diseases hence reduction in the risk of trans‐mission to new-borns during birth.
4.2. Aetiology of neonatal conjunctivitis
Ophthalmia neonatorum can be broadly divided into two types, septic and aseptic. Theaseptic type (chemical conjunctivitis) is generally secondary to the instillation of silver ni‐trate drops for ocular prophylaxis. Septic neonatal conjunctivitis is mainly caused by bacteri‐al and viral infections. Causes include [38]:
From maternal genital tract:
Common Eye Infections34
• Bacterial
◦ Neisseria gonorrhoeae
◦ Chlamydia trachomatis
◦ Group B beta-haemolytic streptococci
• Viral
◦ Herpes Simplex Virus (HSV)
From cross infection:
• Staphylococcus aureus
• Coliforms
• Pseudomonas aeruginosa
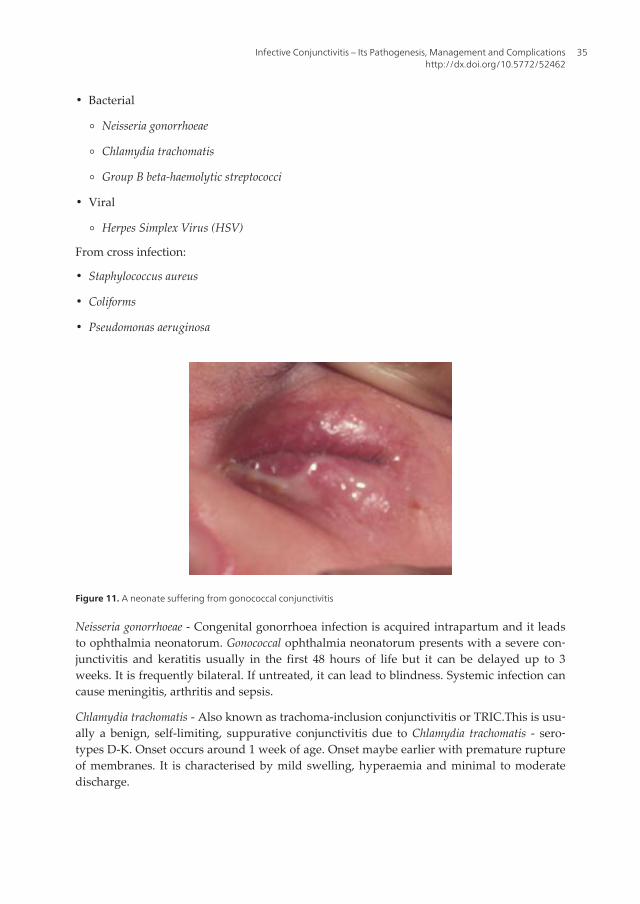
Figure 11. A neonate suffering from gonococcal conjunctivitis
Neisseria gonorrhoeae - Congenital gonorrhoea infection is acquired intrapartum and it leadsto ophthalmia neonatorum. Gonococcal ophthalmia neonatorum presents with a severe con‐junctivitis and keratitis usually in the first 48 hours of life but it can be delayed up to 3weeks. It is frequently bilateral. If untreated, it can lead to blindness. Systemic infection cancause meningitis, arthritis and sepsis.
Chlamydia trachomatis - Also known as trachoma-inclusion conjunctivitis or TRIC.This is usu‐ally a benign, self-limiting, suppurative conjunctivitis due to Chlamydia trachomatis - sero‐types D-K. Onset occurs around 1 week of age. Onset maybe earlier with premature ruptureof membranes. It is characterised by mild swelling, hyperaemia and minimal to moderatedischarge.
Infective Conjunctivitis – Its Pathogenesis, Management and Complicationshttp://dx.doi.org/10.5772/52462
35
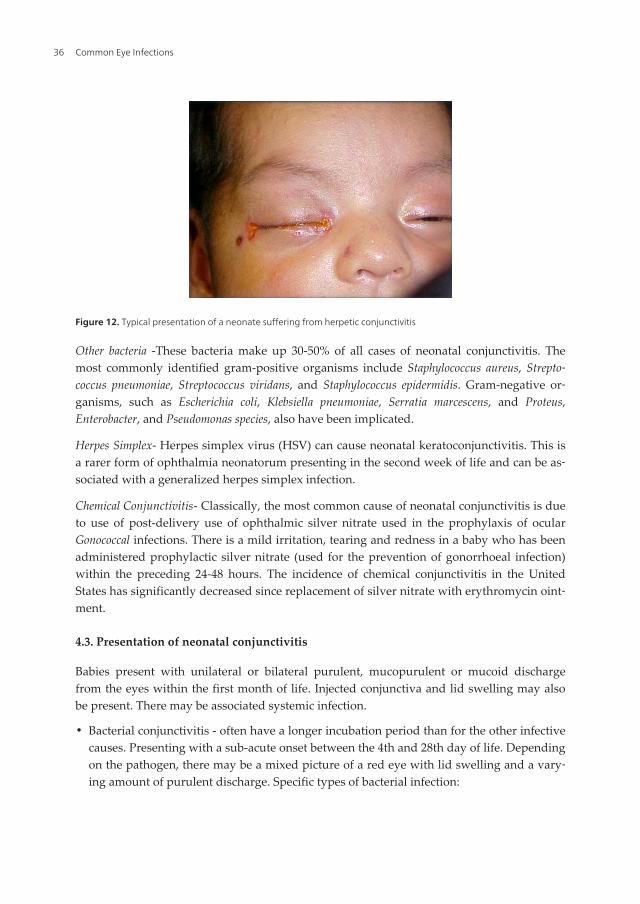
Figure 12. Typical presentation of a neonate suffering from herpetic conjunctivitis
Other bacteria -These bacteria make up 30-50% of all cases of neonatal conjunctivitis. Themost commonly identified gram-positive organisms include Staphylococcus aureus, Strepto‐coccus pneumoniae, Streptococcus viridans, and Staphylococcus epidermidis. Gram-negative or‐ganisms, such as Escherichia coli, Klebsiella pneumoniae, Serratia marcescens, and Proteus,Enterobacter, and Pseudomonas species, also have been implicated.
Herpes Simplex- Herpes simplex virus (HSV) can cause neonatal keratoconjunctivitis. This isa rarer form of ophthalmia neonatorum presenting in the second week of life and can be as‐sociated with a generalized herpes simplex infection.
Chemical Conjunctivitis- Classically, the most common cause of neonatal conjunctivitis is dueto use of post-delivery use of ophthalmic silver nitrate used in the prophylaxis of ocularGonococcal infections. There is a mild irritation, tearing and redness in a baby who has beenadministered prophylactic silver nitrate (used for the prevention of gonorrhoeal infection)within the preceding 24-48 hours. The incidence of chemical conjunctivitis in the UnitedStates has significantly decreased since replacement of silver nitrate with erythromycin oint‐ment.
4.3. Presentation of neonatal conjunctivitis
Babies present with unilateral or bilateral purulent, mucopurulent or mucoid dischargefrom the eyes within the first month of life. Injected conjunctiva and lid swelling may alsobe present. There may be associated systemic infection.
• Bacterial conjunctivitis - often have a longer incubation period than for the other infectivecauses. Presenting with a sub-acute onset between the 4th and 28th day of life. Dependingon the pathogen, there may be a mixed picture of a red eye with lid swelling and a vary‐ing amount of purulent discharge. Specific types of bacterial infection:
Common Eye Infections36
• Chlamydial infection - 5 to 14 days after birth (some report up to 28 days after birth): uni‐lateral/bilateral watery discharge which becomes copious and purulent later on. Theremay be associated preseptal cellulitis and, less commonly, rhinitis, otitis and pneumonitis.
• Gonorrhoeal infection - typically 1-5 days after birth but may occur later: hyper-acute con‐junctival injection and chemosis, lid oedema and severe purulent discharge. There may beassociated corneal ulceration and perforation.
• Viral conjunctivitis
• The onset is acute usually 1-14 days after birth: unilateral/bilateral serosanguinous dis‐charge ± vesicular skin lesions. Uncommonly it can also lead to systemic infection.
4.4. Differential diagnosis of neonatal conjunctivitis
Every other potential cause of red eye needs to be excluded. The differentials include [39]:
• Dacryocystitis
• Congenital glaucoma
• Nasolacrimal duct obstruction
• Preseptal/Orbital cellulitis
• Congenital glaucoma
• Infectious keratitis
4.5. Investigations
A definitive diagnosis of the cause of ophthalmia neonatorum is dependent on laboratoryidentification of the offending organism. The speed of progression of some of the causativeagents makes it imperative to do a test which can identify the cause as soon as possible.Some of the laboratory tests that can be performed are as follows [40]:
• Culture on chocolate agar for N gonorrhoeae. Due to the rapid progression of N gonorrhoeaconjunctivitis, it makes it imperative to perform smears, as it may be possible to identifygram-negative diplococci and initiate proper treatment within hours.
• Conjunctival scraping with Gram stain and Giemsa stain for chlamydia. Conjunctivalspecimens for chlamydia testing must include conjunctival epithelial cells because C. tra‐chomatis is an obligate intracellular organism and exudates are not adequate for testing.Other non-culture methods such as direct fluorescent antibody testing, enzyme immuno‐assays and nucleic acid testing (NAT) may allow early detection of Chlamydia withinhours rather than several days, as required for culture methods.
• Culture on blood agar for other strains of bacteria. For other viral aetiology direct culturesof the HSV vesicles can be performed. Alternatively direct antibody testing or PCR can bedone. If symptoms worsen or symptoms recur after treatment cultures may have to be re‐peated.
Infective Conjunctivitis – Its Pathogenesis, Management and Complicationshttp://dx.doi.org/10.5772/52462
37
4.6. Management of neonatal conjunctivitis
Prophylaxis- In 1881 for the first time silver nitrate was used as prophylactic treatment toreduce the incidence of ophthalmia neonatorum. Silver nitrate is specifically more effectiveagainst gonorrhoeal conjunctivitis. It inactivates gonococci by agglutination. It is not effec‐tive against Chlamydial conjunctivitis. However silver nitrate use also led to mild conjuncti‐val inflammation, tearing and redness which typically resolved within 48 hours. Chemicalconjunctivitis is a self-limiting condition, therefore no treatment is required. However pres‐ervative artificial tears have been used in some cases.
In recent times povidone-iodine drops are used as prophylaxis instead of silver nitrate [41].These are shown to be more effective against gonococcal and chlamydial conjunctivitis and al‐so less toxic. In US, erythromycin is being used as alternative to silver nitrate and povidone-iodine [42]. This is also well tolerated and effective against TRIC and gonococci agents.
Treatment -Treatment of neonatal conjunctivitis should initially be based on the history,clinical presentation and results of smears. This can later be adjusted when laboratory re‐sults become available then specific therapy can be instituted.
The risk of transmission of chlamydial, gonococcal, herpetic, and streptococcal pathogens tothe foetus during the birth process should be considered. If necessary, cervical culturesshould be performed and managed appropriately. To confirm the presence of a sexuallytransmitted disease in the neonate, examine and treat the mother and her sexual partner. Ifnecessary, therapy can be modified when the results of culture and sensitivity are known.
Bacterial conjunctivitis- Chlamydial conjunctivitis is treated with fourteen day course oftwice daily oral erythromycin(50 mg/kg/d divided qid) [43, 44]. Systemic therapy is impor‐tant in Chlamydia conjunctivitis, due to the high incidence of extra-ocular infection in neo‐nates. It has shown to eliminate Chlamydial infection in 80-100% of patients. Topicalerythromycin can be used as adjunct with the oral therapy. If there is failure to respond tothis course the fourteen day course can be repeated before seeking alternative antibiotics[45].
Gonococcal conjunctivitis may be treated with intramascular or intravenous ceftriaxone 50mg/kg/day or as a single dose treatment of 125mg [46]. Alternatively, cefotaxime 100mg canbe given intramuscularly or 25 mg/kg given either intramuscularly or intravenously every12 hours for 7 days [47].
Neonates with conjunctivitis caused by herpetic simplex virus should be treated with sys‐temic acyclovir to reduce the chance of a systemic infection [48]. An effective dose is 60mg/kg/day IV divided.The recommended minimal duration is 14 days, but a course as longas 21 days may be required.Infants with neonatal HSV keratitis should receive a topical oph‐thalmic drug, most commonly 1% trifluridine drops or 3% vidarabine ointment.
4.7. Complications of neonatal conjunctivitis
Complications of neonatal conjunctivitis vary. There are two main types of complications,ocular and systemic complications. These can be prevented with prompt diagnosis and
Common Eye Infections38

treatment. Ocular complications include pseudomembrane formation, peripheral pannusformation, thickened palpebral conjunctiva, cornealoedema, corneal opacification, cornealperforation, staphyloma, endophthalmitis, loss of eye, and blindness [49].
Systemic complications of chlamydia conjunctivitis include pneumonitis, otitis, and phar‐yngeal and rectal colonization. Pneumonia has been reported in 10-20% of infants with chla‐mydial conjunctivitis. Complications of gonococcal conjunctivitis and subsequent systemicinvolvement include arthritis, meningitis, anorectal infection, septicaemia, and death.
Ophthalmia neonatorum is a preventable cause of childhood blindness and with prompt di‐agnosis, treatment and efforts on all levels, this can be eradicated.
5. Prevention of conjunctivitis
Infective conjunctivitis is a condition which affects people of all ages. Its spread is somethingthat can be effectively controlled via good personal hygiene and adequate education. Oncean individual is affected, rapid measures must be taken to ensure that the spread is limited.
Good personal hygiene is primarily achieved via effective hand washing and eye care.Where an outbreak of the highly contagious viral conjunctivitis has occurred, stringentmeasures to control the spread must be undertaken immediately. Simple measures such asremoval of possible contaminated materials (hand cloth, towels and face cloths) are very ef‐fective in reducing spread.
For specialist cases of conjunctivitis, i.e. neonatal conjunctivitis and conjunctivitis in the im‐munocompromised, immediate action must be undertaken to ensure no long term complica‐tions and quick recovery. Should there be any delay in treatment, the potential for long termdamage, and even blindness, is very high. Prevention of such conditions can be attained byimmediate and frequent treatment via hospital admissions, prophylactic medication andgood eye hygiene.
6. Conclusion
Conjunctivitis can be a very irritating and frustrating condition to suffer from. Not onlydoes it have profound social implications, it can also affect education and finances if socialexclusion is required. General practitioners must remain vigilant when diagnosing viralfrom bacterial conjunctivitis and try to ensure that patient education of the condition is at anoptimum level to prevent spread. Special care must also be taken into consideration in neo‐natal conjunctivitis and conjunctivitis in the immunocompromised.
Although conjunctivitis is mostly a mild condition, GPs must also be aware of other moreserious conditions and be able to differentiate mild conditions from more serious underlyingand emergency conditions. This is only achieved via being able to create a list of differentialsfrom a thorough patient history, examination and referral to an ophthalmologist if required.
Infective Conjunctivitis – Its Pathogenesis, Management and Complicationshttp://dx.doi.org/10.5772/52462
39
Author details
Adnaan Haq, Haseebullah Wardak and Narbeh Kraskian
St. George’s University of London, UK
References
[1] Santa JO, Mark BA. Allergic conjunctivitis: Update on pathophysiology and pros‐pects for future treatment. The Journal of Allergy and Clinical Immunology. 2004;115: 118-122.
[2] Sheikh A, Hurwitz B. Topical antibiotics for acute bacterial conjunctivitis: a systemat‐ic review. Br J Gen Pract. 2001; 51:473–7.
[3] Department of Health, Prescription cost analysis data. Leeds: Department of Health,1998.
[4] Rose PW, Harnden A, Brueggemann AB, Perera R, Sheikh A, Crook D, Mant D.Chloramphenicol treatment for acute infective conjunctivitis in children in primarycare: a randomised double-blind placebo-controlled study. Lancet. 2005; 366: 37–43.
[5] Weiss A, Brinser JH, Nazar-Stewart V. Acute conjunctivitis in childhood. J Pediatr.1993; 122: 10–14.
[6] Gigliotti F, Williams WT, Hayden FG, Hendley JO. Etiology of acute conjunctivitis inchildren. J Pediatr. 1981; 98: 531–536.
[7] Tarabishy BA, Jeng HB. Bacterial conjuntivitis: A review for internists. ClevelandClinic Journal of Medicine. 2008; 75: 508-512.
[8] Genees en hulpmiddelen Informatie Project. Annual report prescription data. Colle‐gevoorzorg verzekeringen, Amstelveen, 2001.
[9] Carr WD. Comparison of Fucithalmic® (fusidic acid viscous eye drops 1%) andChloromycetin Redidrops® (chloramphenicol eye drops 0. 5%) in the treatment ofacute bacterial conjunctivitis. J Clin Res. 1998; 1: 403–411.
[10] Wall AR, Sinclair N, Adenis JP. Comparison of Fucithalmic® (fusidic acid viscouseye drops 1%) and Noroxin (norfloxacin ophthalmic solution 0. 3%) in the treatmentof acute bacterial conjunctivitis. J Drug Assess. 1998; 1: 549–558.
[11] Schiebel N: Use of antibiotics in patients with acute bacterial conjunctivitis. AnnEmerg Med. 2003; 41: 407–409.
[12] Sheikh A, Hurwitz B. Topical antibiotics for acute bacterial conjunctivitis: Cochranesystematic review and meta-analysis update. British Journal of General Practice.2005; 55: 962-964.
Common Eye Infections40
[13] Everitt HA, Little PS, Smith PW. A randomised controlled trial of management strat‐egies for acute infective conjunctivitis in general practice. BMJ. 2006; 333: 321.
[14] Rietveld RP, Bindels PJE, Sloos JH, van Weert HCPM. The treatment of acute infec‐tious conjunctivitis with fusidic acid: a randomised controlled trial. Br J Gen Pract.2005; 55: 924–930.
[15] Cronau H, Kankanala RR, Mauger T. Diagnosis and management of red eye in pri‐mary care. Am Fam Physician. 2010; 81: 137-44.
[16] Anon. Acute Conjunctivitis. Best Medical Practice, BMJ [serial online]. Availablefrom:http://bestpractice. bmj. com/best-practice/monograph/68/treatment/details.html
[17] Sheikh A, Hurwitz B. Topical antibiotics for acute bacterial conjunctivitis: Cochranesystematic review and meta-analysis update. British Journal of General Practice.2005; 55: 962-964
[18] Fraunfelder FW. Corneal toxicity from topical ocular and systemic medications. Cor‐nea. 2006; 25: 1133-8
[19] Schlech BA, Blondeau J. Future of ophthalmic anti-infective therapy and the role ofmoxifloxacin ophthalmic solution 0. 5% (VIGAMOX) . SurvOphthalmol. 2005; 50:64-7.
[20] Kowalski RP, Dhaliwal DK, Karenchak LM, Romanowski EG, Mah FS, RitterbandDC, Gordon YJ. Gatifloxacin and moxifloxacin: an in vitro susceptibility comparisonto levofloxacin, ciprofloxacin, and ofloxacin using bacterial keratitis isolates. Am JOphthalmol. 2003; 136: 500-5.
[21] Kowalski RP, Yates KA, Romanowski EG, Karenchak LM, Mah FS, Gordon YJ. Anophthalmologist's guide to understanding antibiotic susceptibility and minimum in‐hibitory concentration data. Ophthalmology. 2005; 112: 1987.
[22] Asbell PA, Colby KA, Deng S, McDonnell P, Meisler DM, Raizman MB, Sheppard JDJr, Sahm DF. Ocular TRUST: nationwide antimicrobial susceptibility patterns in ocu‐lar isolates. Am J Ophthalmol. 2008; 145: 951-958.
[23] Asbell PA, Sahm DF, Shaw M, Draghi DC, Brown NP. Increasing prevalence of me‐thicillin resistance in serious ocular infections caused by Staphylococcus aureus inthe United States: 2000 to 2005. J Cataract Refract Surg. 2008; 34: 814-8
[24] Sheikh A & Hurwitz B: Topical antibiotics for acute bacterial conjunctivitis: a system‐atic review. Br J General Prac. 2001; 51: 473–477.
[25] Ishii K, Nakazono N, FujinagaK, Fujji S, Kato M, Ohtusaka H, Aoki K, Chen CW, LinCC, Sheu MM, Lin KH, Oum BS, Lee SH, Chun CH, Yoshii T, Yamazaki S. Compara‐tive Studies on Aetiology and Epidemiology of Viral Conjunctivitis in Three Coun‐tries of East Asia—Japan, Taiwan and South Korea. International Journal ofEpidemiology. 1986; 16: 98-103.
Infective Conjunctivitis – Its Pathogenesis, Management and Complicationshttp://dx.doi.org/10.5772/52462
41
[26] Donahue, S. P. , Khoury, J. M. , Kowalski, R. P. (1996) Common ocular infections: aprescriber's guide. Drugs. 52 (4) , pp. 528-529.
[27] Monnerat, N. , Bossart, W. , Thiel, M. A. (2006) Povidone-iodine for treatment of ade‐noviral conjunctivitis: an in vitro study. Klinische Monatsblätterfür Augenheilkunde.223 (5) , pp. 349-52.
[28] Cronau, H. , Kankanala, R. R. , Mauger, T. (2010) Diagnosis and management of redeye in primary care. American Academy of Family Physicians. 81(2) , pp. 137-44.
[29] Schueler, S. J. , Beckett, J. H. , Gettings, D. S. (2008) Viral Conjunctivitis: Outlook.Available: http://www. freemd. com/viral-conjunctivitis/outlook. htm. Last accessed8th August 2012.
[30] Chronister, C. L. (1996) Review of External Ocular Disease Associated with AIDS andHIV infection. American Academy of Optometry. 73 (4) , pp. 225-230.
[31] Diesenhouse, M. C. , Wilson, L. A. , Corrent, G. F. , Visvesvara, G. C. (1993) Treat‐ment of Microsporidial keratoconjunctivitis with topical fumagillin. American Jour‐nal of Ophthalmology. 115 (1) , pp. 293-298.
[32] Charles, N. C. , Freidberg, D. N. (1992) Molluscum Contagiosum in AIDS. Ophthal‐mology (Rochester) . 99 (7) , pp. 1123-1126.
[33] Kohn, S. R. (1987) MolluscumContagiosum in patients with AIDS. American MedicalAssociation: Archives of Ophthalmology. 105 (4) , p. 458.
[34] Schryver, A. D. , Meheus, A. (1990) Epidemiology of sexually transmitted diseases:the global picture. Bulletin of the World Health Organization. 68(5) , pp. 639–654.
[35] Verma, M. , Chaatwal, J. , Varughese, P. (1994) Neonatal Conjunctivitis: A Profile. In‐dian Paediatrics. 31(11) , pp. 1357-61.
[36] Jamal, L. , Khan, M. (2010) Ophthalmianeonatorum. Journal of College Physiciansand Surgeons Pakistan. 20(9) , pp. 595-8.
[37] Laga, M. , Plummer, F. A. , Nzanze, H. , Namaara, W. , Brunham, R. C. , Ndinya-Achola, J. O. , Maitha, G. , Ronald, A. R. , D'Costa, L. J. , Bhullar, V. B. , Fransen, L. ,Piot, P. , (1986) Epidemiology of Opthalmia Neonatorum in Kenya. The Lancet.328(8516) , pp. 1145-1149.
[38] Enzenauer R. W. , (2011) Neonatal Conjunctivitis. Available at: http://emedicine.medscape. com/article/1192190-overview(Accessed: 5th August 2012) .
[39] Scott, O. , (2011) OphtalmiaNeonatorum Available at: http://www. patient. co. uk/doctor/Ophthalmia-Neonatorum. htm(Accessed 5th August 2012) .
[40] Gregory, S. , Cantor, L. , Louis, B. , Weiss, J. S. , (2011) Paediatric Opthalmology andStrabismus. In The American Academy of Ophthalmology, ed, Basic and clinical sci‐ence course. 1st edn. Singapore: American Academy of Ophthalmology, pp. 186-188.
Common Eye Infections42
[41] Sherwin, J. , Isenberg, A. P. T. , Leonard, A. P. T. , Wood, M. , (1995) A ControlledTrial of Povidone–Iodine as Prophylaxis against OphthalmiaNeonatorum. The NewEngland Journal of Medicine. 332 (9) , pp. 562-566.
[42] Darling, E. , McDonald, H. , (2010) A meta-analysis of the efficacy of ocular prophy‐lactic agents used for the prevention of gonococcal and chlamydial ophthalmianeo‐natorum. Journal of Midwifery and Women's Health. 55(4) , pp. 319-27.
[43] Heggie, A. D. , Jaffe, A. C. , Stuart, L. A. , Thombre, P. S. , Sorensen, R. U. (1985) Topi‐cal Sulfacetamidevs Oral Erythromycin for Neonatal Chlamydial Conjunctivitis.American Journal of diseases of children. 139(6) , pp. 564-566.
[44] Zar H. J. , (2005) Neonatal Chlamydial Infections: Prevention and Treatment. Pedia‐tric Drugs. 7(2) , pp. 103-110.
[45] Stenberg, K. , Mardhip, A. , (1991) Treatment of chlamydial conjunctivitis in new‐borns and adults with erythromycin and roxithromycin. Journal of AntimicrobialChemotherapy. 28(2) , pp. 301-307.
[46] Laga, M. , Naamara, W. , Brunham, R. C. , D’Costa, L. , Nsanze, H. , Piot, P. , Kuni‐moto, D. , Ndinya-Achola, J. , Slaney, L. , Ronald, A. R. , Plummer, F. A. (1986) Sin‐gle-Dose Therapy of Gonococcal Ophthalmia Neonatorum with Ceftriaxone. TheNew England Journal of Medicine. 315(22) , pp. 1382-1385.
[47] Pierce, J. M. , Ward, M. E. , Seal, D. V. (1982) Ophthalmianeonatorum in the 1980s:incidence, aetiology and treatment. British Journal of Ophthalmology. 66 (11) , pp.728-731.
[48] Whitley, R. , (2004) Neonatal herpes simplex virus infection. Current Opinion in In‐fectious Diseases. 17(3) , pp. 243-246.
[49] Gogate, P. , Gilbert, C. , Zin, A. (2011) Severe Visual Impairment and Blindness in In‐fants: Causes and Opportunities for Control. Middle East African Journal of Ophthal‐mology. 18(2) , pp. 109-114.
Infective Conjunctivitis – Its Pathogenesis, Management and Complicationshttp://dx.doi.org/10.5772/52462
43
