infectious complications in pd – peritonitis and exit site...
TRANSCRIPT

1
AL05182
Infectious Complications in PD Infectious Complications in PD ––Peritonitis and Exit Site InfectionsPeritonitis and Exit Site Infections
Beth Piraino, MDProfessor of Medicine
Assistant Dean of AdmissionsUniversity of Pittsburgh
Chicago NAC-ISPDApril 2005
AL05182
Baxter Healthcare is not responsible for the material in this presentation and does not endorse the opinions or advice of the author.
It is the responsibility of the health care practitioner to determine diagnosis and appropriate treatment for their patients.
AL05182
2
AL05182
--Covered in talkCovered in talk--
• Exit site infections• Peritonitis• Structure and monitoring outcomes
related to PD infections.
AL05182
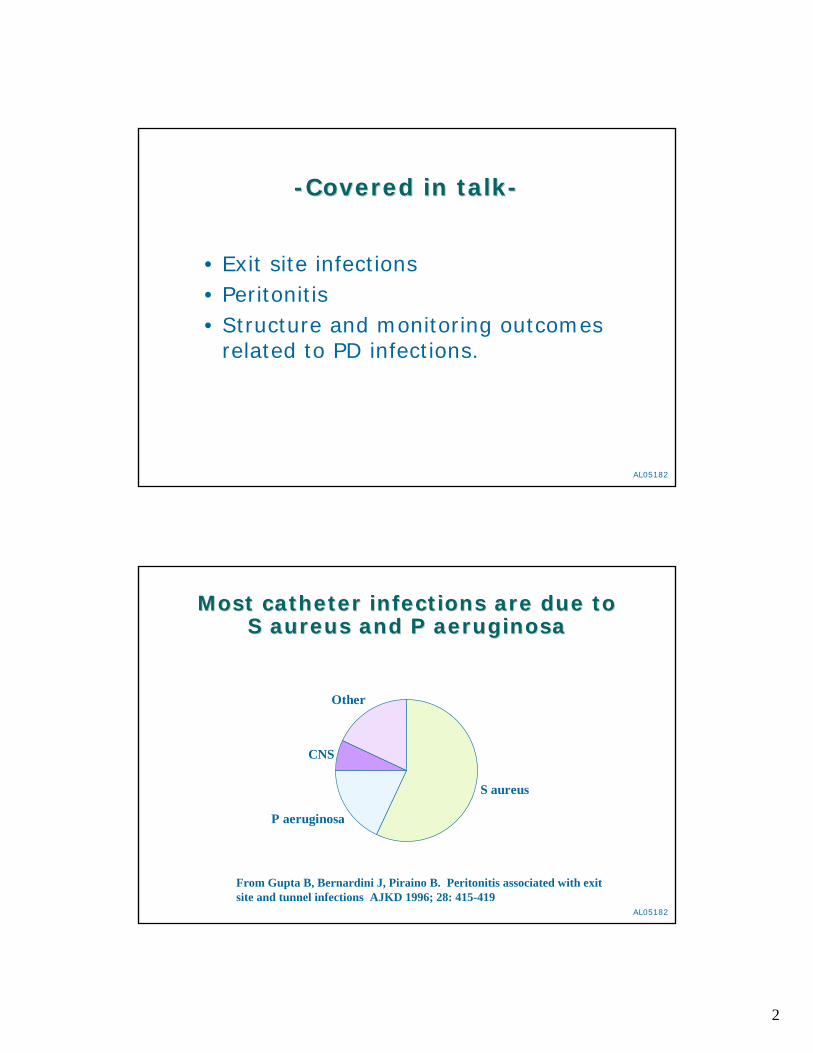
Most catheter infections are due to Most catheter infections are due to S S aureusaureus and P and P aeruginosaaeruginosa
S aureus
P aeruginosa
CNS
Other
From Gupta B, Bernardini J, Piraino B. Peritonitis associated with exit site and tunnel infections AJKD 1996; 28: 415-419

3
AL05182
00.10.20.30.40.50.60.7
'83 '84 '85 '86 '87 '88 '89 '90 '91 '92 '93 '94 '95 '96 '97 '98 '99 '00 '01
YEAR
catheter infections peritonitis
S. aureus episodes / patient - year
Piraino B, Bernardini J, Fried L. S aureus prophylaxis and Trends in GN infections in PD Patients PDI 2003; 23: 456-459
MUPIROCIN PROPHYLAXIS given throughout 1990’s
Trend of S. aureus PD related infections over the years of the Pittsburgh PD Registry
AL05182
00.10.20.30.40.50.60.7
'83 '84 '85 '86 '87 '88 '89 '90 '91 '92 '93 '94 '95 '96 '97 ;98 '99 '00
YEAR
catheter infections peritonitis
But….Mupirocin has no impact on P. aeruginosaepisodes / patient - year
Clearly no change over time!Piraino B, Bernardini J, Fried L. S auresu prophylaxis and Trends in GN infections in PD Patients PDI 2003; 23: 456-459

4
AL05182
So we did a randomized trial comparing So we did a randomized trial comparing gentamicin cream to gentamicin cream to mupirocinmupirocin at the at the
exit site, beginning in 2001exit site, beginning in 2001
Our hypothesis–Gentamicin cream at the exit site would be as
effective as mupirocin in preventing S aureusinfections
–Gentamicin cream at the exit site would reduce P aeruginosa exit site infections by 50%
Since baseline P aeruginosa exit site infection rate was 0.11/year, the study was powered for 140 dialysis years f/up
Bernardini….Piraino JASN 2005; 16: 539-545.
AL05182
MethodsMethods
• Randomized, double-blinded at 3 centers• Prevalent and incident patients• Central drug preparation and blinding by
the Investigational Drug Service at Pittsburgh.
• Prospective data collection of all catheter infections and peritonitis.–Rates expressed as episodes per year at risk
Bernardini….Piraino JASN 2005; 16 539-545.

5
AL05182
Patient characteristics of the Patient characteristics of the randomized groups were similarrandomized groups were similar------
Mupirocin Gentamicin
Number patients 66 67Patient years follow-up 54 64Age 51 54Diabetic, insulin dependent 41% 40%Male 58% 51%White 88% 93%Incident to PD 59% 46%
No difference in the two groups for any of these variables.
AL05182
0.000
0.200
0.400
0.600
0.800
1.000
0.0 3.0 6.0 9.0 12.0 15.0 18.0 21.0 24.0 27.0 30.0Months
Sur
vivo
rshi
p: S
(t)
gentamicin cream
mupirocin cream p=0.03
Results: the group on gentamicin cream had a longer time to first exit site infection
Bernardini….Piraino JASN 2005
6
AL05182
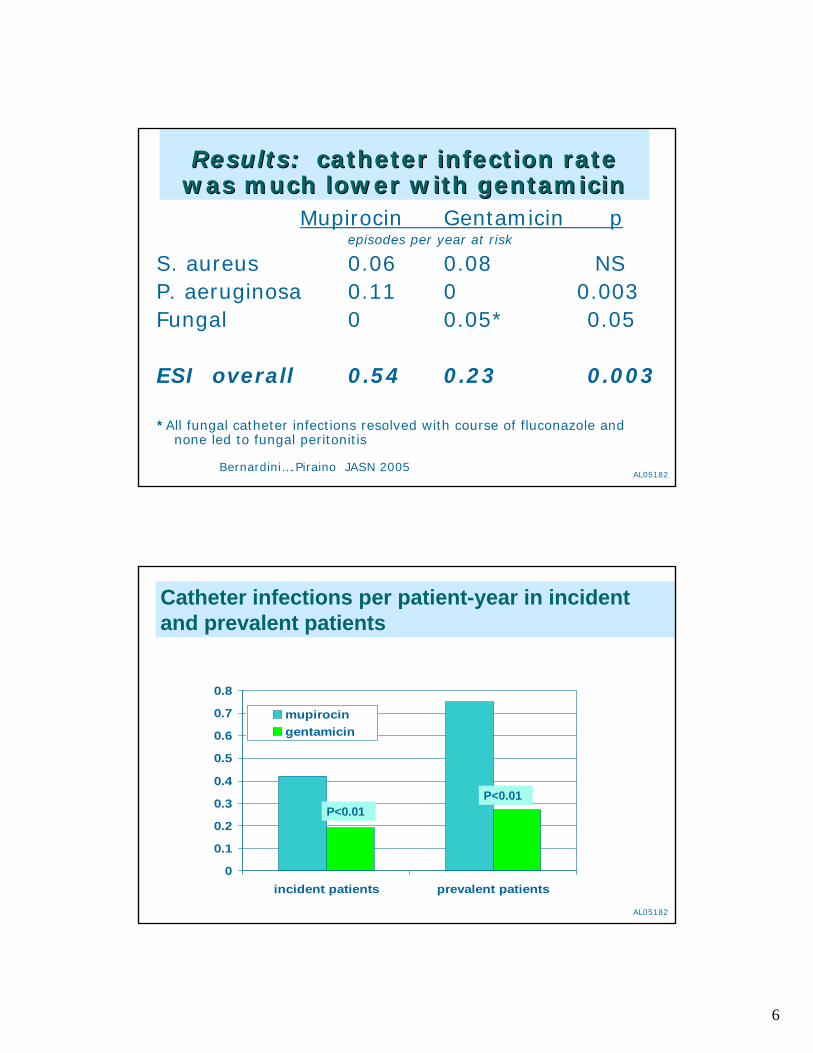
Results:Results: catheter infection rate catheter infection rate was much lower with gentamicinwas much lower with gentamicin
Mupirocin Gentamicin pepisodes per year at risk
S. aureus 0.06 0.08 NSP. aeruginosa 0.11 0 0.003 Fungal 0 0.05* 0.05
ESI overall 0.54 0.23 0.003
*All fungal catheter infections resolved with course of fluconazole and none led to fungal peritonitis
Bernardini….Piraino JASN 2005
AL05182
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
incident patients prevalent patients
mupirocingentamicin
Catheter infections per patient-year in incident and prevalent patients
P<0.01P<0.01

7
AL05182
To our surprise, To our surprise, peritonitis ratesperitonitis rates were were also lower in the gentamicin groupalso lower in the gentamicin group
Mupirocin Gentamicin p valueepisodes per year at risk
P aeruginosa 0.04 0 0.14Other Gram negative 0.11 0.02 0.02S aureus 0 0.03 NSFungal 0.04 0.03 NS
Peritonitis overall 0.52 0.34 0.03Bernardini….Piraino JASN 2005
AL05182
SummarySummary of the randomized trial of the randomized trial findingsfindings
Gentamicin cream applied daily to the exit site compared to mupirocin significantly reduced:
exit site infections (57%)and peritonitis (35%)
Funded by Paul Teschan and NKF Bernardini….Piraino JASN 2005; 16: 539-545

8
AL05182
How to determine if an exit site How to determine if an exit site infection is present? infection is present?
Exit site scoring systemExit site scoring system
• Swelling• Crust• Redness• Pain• Drainage
Each scored 0-3If score >3 than an ESI present.
Schaefer et al JASN 1999;10: 136-145
AL05182
Replacing the catheter for refractory Replacing the catheter for refractory ESIESI
• S aureus and P aeruginosa exit site infections may prove refractory or relapsing.
• Catheter change highly effective in resolving.
Finkelstein AJKD 2002;39:278-1286
GUIDELINE: For refractory exit site infections, catheter replacement should be done and can be done
as same day procedure

9
AL05182
Summary: exit site infectionsSummary: exit site infections
1.Catheter placement to prevent trauma
2.Protocol to reduce risk of ESI3. If infection occurs, culture exit site
drainage and treat until completely resolved
4.Replace catheter as simultaneous procedure if refractory
AL05182
PeritonitisPeritonitis
PD patients presenting with abdominal pain OR cloudy effluent should be presumed to have peritonitis.
Diagnosis is confirmed with cell count and culture.1. ≥100 WBC per mcL with more than 50% polys2. Positive culture (approximately 80%) will depend
on culture technique

10
AL05182
Structured approach to training Structured approach to training improves outcomes on PDimproves outcomes on PD
• Tells the learner what they will learn• What the teacher will do• What the learner needs to do• How teacher and learner will recognize
when learning has occurred.
Hall et al Nephr Nursing J 2004; 31: 149-163
AL05182
Example of learning Example of learning outcomes/objectivesoutcomes/objectives
Memory: The learner will gather supplies for exchange
Concept: The learner will differentiate between sterile and not sterile.
Principle: The learner will recognize and state the principles: if something sterile touches something not sterile, it is contaminated; if contamination occurs, peritonitis may result
Judgment: The learner will recognize situations that may lead to peritonitis and appropriate action to prevent
Problem solving: The learner will recognize contamination and demonstrate action to take.
11
AL05182
Preventing peritonitis Preventing peritonitis
Every effort should be made to preventperitonitis in PD programs.
This involves emphasis on – training and connection methods–exit site care and appropriate prophylaxis– timely replacement of the catheter
2005 ISPD PD Related Infections Recommendations are in the most recent issue of Peritoneal Dialysis International and emphasize these points
[Piraino B, et al PDI 2005; 25: 107-131]
AL05182
What organisms do we expect to see in PD related peritonitis?

12
AL05182
ORGANISMS causing peritonitis:ORGANISMS causing peritonitis:149 patient years, 110 incident PD patients149 patient years, 110 incident PD patients
Organism episodes per year
S aureus 0.04CN Staph 0.03 37%Other GP 0.04Pseudomonas 0.05 33%Other GNR 0.05Polymicrobial <0.01Culture negative 0.07AFB 0.02TOTAL 0.30
or 41 months per episodeLi et al AJKD 2002;40:373-380
AL05182
What should we use as empiric What should we use as empiric therapy of peritonitis?therapy of peritonitis?
2000 ISPD Guidelines:
CefazolinAnd
Ceftazidime

13
AL05182
However,However,
Methicillin resistance in coagulase negative Staphylococcal infections is very high in many programs.
In addition, MRSA peritonitis is an extremely serious infection, even life threatening and certainly a risk to the peritoneal membrane.
AL05182
Empiric therapyEmpiric therapy------2005 Guidelines2005 Guidelines
Cefazolinor
Vancomycin
Ceftazidime
or
Gentamicin
AND

14
AL05182
Considerations for making the Considerations for making the decisiondecision
• Each center must know its own history regarding organisms and resistance patterns
• Practicality must also be considered—– In particular in patient vs out patient
treatment– Insurance coverage for meds– CAPD versus CCPD
AL05182
Dosing of antibioticsDosing of antibiotics
• IP dosing is preferred; absorption enhanced with peritonitis (“high transporter”)
• Drug may be given in each exchange or intermittently. Dwell time must be 6 hours minimum
• Little data on drug dosing in APD– Can switch to around the clock cycles with dwell of
3-4 hours– Alternatively, switch patients to CAPD

15
AL05182
Why switch to CAPD when an APD Why switch to CAPD when an APD patient gets peritonitis?patient gets peritonitis?
• IP cephalosporin levels will not be adequate in APD unless the antibiotic is given in all exchanges.
• Guidelines and most of the data are for CAPD with continuous administration.
However, it is not always possible to switch the patient to CAPD.
AL05182
AlternativeAlternative
If vancomycin being used, an alternative is to place the antibiotics in the long dwell.
However, it still may be difficulty to achieve adequate levels in all exchanges if rapid exchanges on the cycler are being done.
MORE DATA NEEDED!!

16
AL05182
Subsequent therapySubsequent therapy
• Tailor choice of drug to sensitivities
• Use least toxic antibiotic (that is, avoid long courses of aminoglycosides)
• Treat for 2-3 weeks.
AL05182
Case of the 28 year old man on Case of the 28 year old man on CAPD 13 yearsCAPD 13 years
• Previously one mild episode of peritonitis [CNS] that resolved readily and one severe episode due to E coli [also resolved].
• Several episodes of S aureus ESI successfully treated with oral antibiotics
• Presents with severe abdominal pain, clear fluid, hypotension, no fever.

17
AL05182
ContinuedContinued
• Exit site looks fine• Fluid quickly becomes cloudy• Given vancomycin and gentamicin• Fluid by day 3 begins to clear• 4th day, increase in cloudiness, increase in
pain, and increase in cell countWhat would you do now?
AL05182
Management of peritonitisManagement of peritonitis------refractory peritonitisrefractory peritonitis
• About 5% patients with peritonitis die• 18% of episodes of peritonitis resulted in
transfer to HD.• If the fluid was still cloudy after 5 days,
failure rate was 46%.ISPD guideline: remove catheter if
effluent fails to clear by 5 days.
Krishnan PDI 2002;22: 573-581.

18
AL05182
Results of waiting 10 days to remove Results of waiting 10 days to remove catheter in refractory peritonitiscatheter in refractory peritonitis
died <4 wks catheter removal
7%
replacement successful
subsequent PD failure32%
died during treatment
28%
Szeto JASN 2002;13:1040-1045
AL05182
Note indications for catheter Note indications for catheter removalremoval
• Refractory peritonitis
• Fungal peritonitis
• Relapsing peritonitis
• Refractory exit site infection
• Should be considered for mycobacterial
peritonitis and multiple enteric

19
AL05182
Summary: Treatment of peritonitisSummary: Treatment of peritonitis• Choose empiric therapy for program
based on sensitivities• Always examine exit site/tunnel—
preferably replace catheter for refractory exit site infection before peritonitis.
• If no response in 5 days, remove catheter• If relapse, treat and replace catheter• Avoid extended use of aminogylcosides
AL05182
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
'98 '99 '00 '01 '02 '03
YEAR
Monitoring peritonitis in a PD program Should always be expressed as rates[episodes per year at risk]
PD Registry Data--DCI Oakland
One episode per 75 months
NO national data on peritonitis rates
7 episodes in 6 patients in a program with 70 patients
20
AL05182
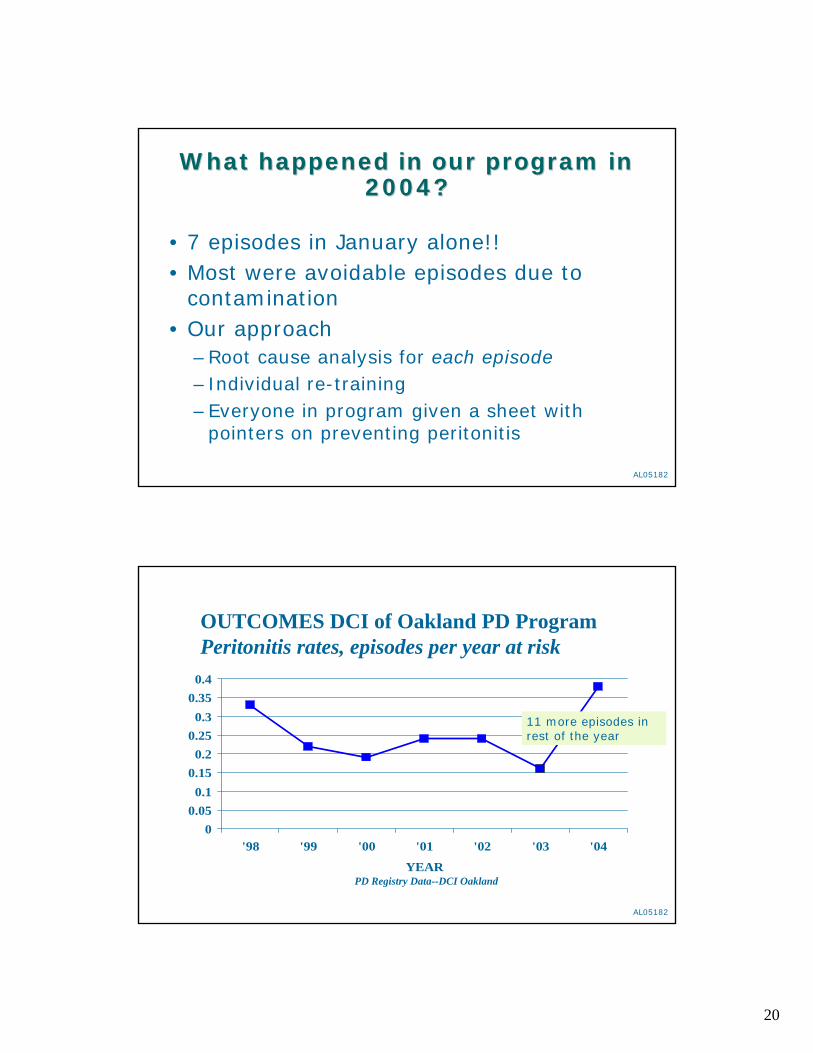
What happened in our program in What happened in our program in 2004?2004?
• 7 episodes in January alone!!• Most were avoidable episodes due to
contamination• Our approach
–Root cause analysis for each episode– Individual re-training–Everyone in program given a sheet with
pointers on preventing peritonitis
AL05182
00.050.1
0.150.2
0.250.3
0.350.4
'98 '99 '00 '01 '02 '03 '04
YEAR
OUTCOMES DCI of Oakland PD ProgramPeritonitis rates, episodes per year at risk
PD Registry Data--DCI Oakland
11 more episodes in rest of the year

21
AL05182
00.050.1
0.150.2
0.250.3
0.350.4
'98 '99 '00 '01 '02 '03 '04 '05
YEAR
OUTCOMES DCI of Oakland PD ProgramPeritonitis rates, episodes per year at risk
PD Registry Data--DCI Oakland
This year (3 months data) our rates are back down to one episode per 50 months
AL05182
Final pointFinal point
Dialysis Patient Mortality
22
AL05182
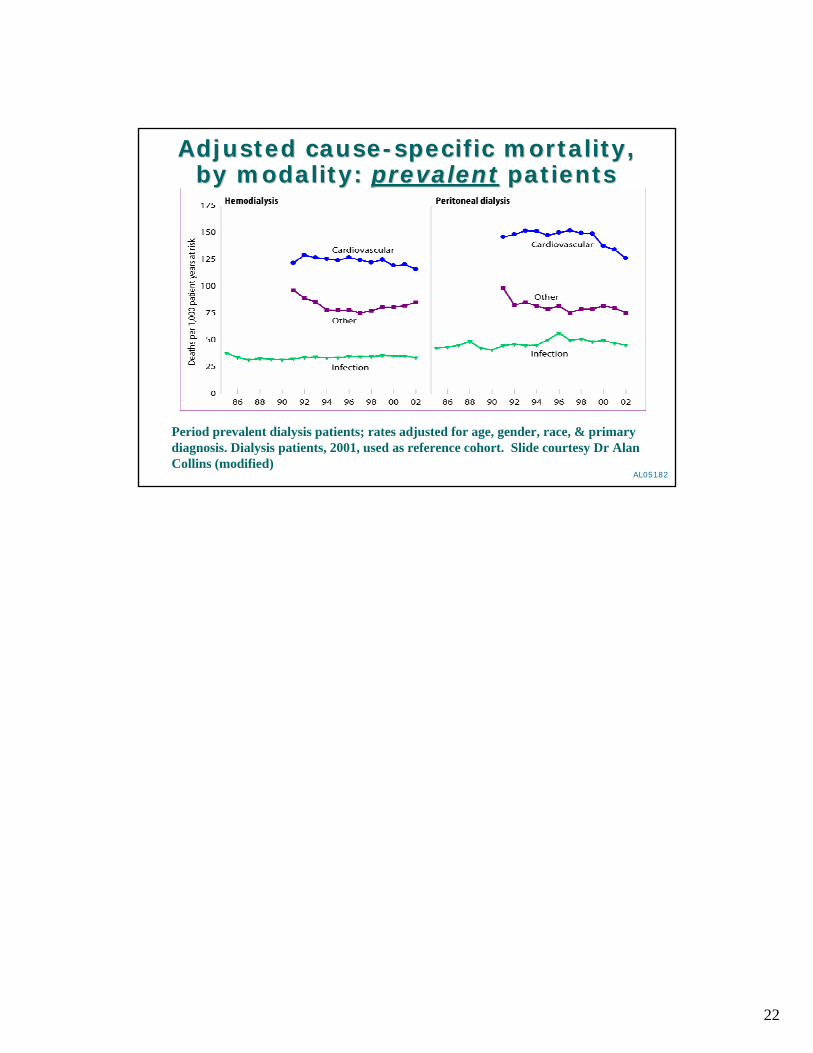
Period prevalent dialysis patients; rates adjusted for age, gender, race, & primary diagnosis. Dialysis patients, 2001, used as reference cohort. Slide courtesy Dr Alan Collins (modified)
Adjusted causeAdjusted cause--specific mortality, specific mortality, by modality: by modality: prevalentprevalent patients patients