infection control service annual report
TRANSCRIPT

1
Primary Care and Mental Health Partnership Trusts
INFECTION CONTROL SERVICE
ANNUAL REPORT
1 April 2008 – 31 March 2009
On behalf of
Worcestershire Primary Care Trust
The Worcestershire non acute NHS Infection Control Service Annual Report was presented at the April 2009
Worcestershire non acute Infection Control Committee and agreement was reached that the drafting of service objectives and agreement of the 2009/2010 service level agreement would be postponed until it could be
ascertained whether further funding for the service to meet demands would be available.
WPCT IC annual report – June 2009 2
Worcestershire non acute NHS Infection Control Service
Worcestershire Primary Care Trust Annual Report 1 April 2008 – 31 March 2009
1. Executive Summary This report aims to summarise the infection control activities carried out on behalf of the Worcestershire Primary Care Trust. The Worcestershire non acute Infection Control Service was originally established in September 1997. It was recognised in planning for the transfer of responsibilities to PCT that this service should be managed by one organisation on behalf of Worcestershire’s PCT and Mental Health Trust. Since October 2005, the service has been hosted by the Worcestershire Mental Health Partnership Trust; it operates across the two organisations and General Practices within Worcestershire. Over the last two years the service has also become involved in issues relating to the wider health economy. The infection prevention and control agenda is ever increasing with continued importance at all levels of the organisation which is supported by central publications requiring action, a need to provide assurance and also participation in national initiatives. Each NHS Trust is expected to have sufficient systems in place to apply evidence based protocols and to comply with each applicable aspect of The Health Act to minimise infection risks. A service level agreement exists that has been designed to ensure compliance with the requirements in The Health Act (2006) amended 2008, Essential Steps for Safe, Clean, Care, Standards for Better Health and more recently the nine key criteria required by the Care Quality Commission in it’s registration process. It acknowledges the importance of partnership working with the aim being to ensure that there is a managed environment, which minimises the risk of infection, to patients, staff and visitors. 2. Infection Control Team The team comprises 4 Infection Control Nurses (ICNs), (1 wte Nurse Consultant, 1.1 wte completed accredited training and 0.6 wte in training post). Medical/Microbiological support is provided as part of an SLA with Worcestershire Acute Hospitals Trust which provided Infection Control Doctor (ICD) support. This also ensures 24 hour access for staff requiring infection control advice. The ICNs work during office hours but advice is available to staff 24 hours a day, 365 days a year, through the on call arrangements as part of the Service Level Agreement for the ICD role. Within Worcestershire PCT an existing director has been appointed as Director with responsibility for Infection Prevention and Control (DIPC) - Sandra Rote. This provides a direct link to Trust Board. It is however acknowledged that the Infection Control Team, if necessary, can directly access the Chief Executive. The infection control framework within the policies and procedures binder details these relationships and communication lines for each organisation. 3. Service Remit The agenda for this is ever increasing with continued importance at all levels of the organisation. This is supported by central publications requiring action, a need to provide assurance and also required participation in national initiatives. Within Primary Care the service remit includes provider service, general practice and certain elements of commissioning. The Health Act highlights the importance of this stating that when a Trust is commissioning services they should satisfy themselves that contracted services have appropriate systems in place to minimise infection risks as far as is reasonably practical. 4. Description of Infection Control Arrangements Infection control service provision follows guidelines produced by the Department of Health (1995), HSC 2000/002 and the Health Act (2006, updated 2008). Service objectives are agreed annually and progress reviewed by the Worcestershire non acute Infection Control Committee, (WnaICC), which meets on a quarterly basis. Membership and terms of reference for this committee are in accordance with national recommendations. For a meeting to be quorate both the organisations included in the SLA need to be represented. The Infection Control Team meets

WPCT IC annual report – June 2009 3
monthly to discuss any ongoing or arising issues and meetings will occur on a minimum of a bi-monthly basis with the Director with Responsibility for Infection Prevention and Control. The Trust is represented on the Local Health Protection Unit Committee and Healthcare Associated Infection Group. Liaison with all other local Infection Control Nurses based in the Worcestershire Acute Hospitals Trust, other neighbouring NHS Trusts and the local Health Protection Unit clinical team also occurs on a regular basis. Infection Control Nurse representation is provided at various committees/meetings as requested, within client organisations. These include Community Hospital Infection Groups, Professional Nursing Advisory Groups, Patient Environment Action Teams (PEAT), Quality and Safety, Decontamination, Medical Devices Management and Health and Safety. There is a great number of publications that provide support and guidance on what is good practice in infection prevention and control and how it can be continually improved, this obviously includes the recommendations set out in The Health Act (2006) amended 2008 under the key headings of Management, Organisation and the Environment, Clinical Care Protocols and Health Care Workers which comprise of various duties. The national agenda aims to ensure that infection prevention and control issues are firmly placed at the heart of all NHS services, and that reducing healthcare associated infection is everyone’s business, but recognises the pivotal role that Infection Control Teams have in the process. The need for this has been further strengthened by the Care Quality Commission (2008) requirements which state that, The Trust must:
ο have in place and operate effective management systems for the prevention and control of HCAI that are informed by risk assessments and analysis of infection incidents
ο provide and maintain a clean and appropriate environment that facilitates the prevention and control of HCAI
ο provide suitable and sufficient information on HCAI to patients and the public and to other service providers when patients move to the care of another healthcare or social care provider
ο ensure patients presenting with an infection or who acquire an infection during treatment are identified promptly and receive appropriate treatment and care to reduce the risk of transmission
ο gain the co-operation of staff, contractors and others involved in the provision of healthcare in preventing and controlling infection
ο provide or can secure adequate isolation facilities ο secure adequate access to laboratory support ο adhere to, appropriate policies and protocols for the prevention and control of HCAI ο ensure so far as is reasonably practicable, that healthcare workers are free of and are protected from
exposure to communicable infections during the course of their work, and that all staff are suitably educated in the prevention and control of HCAI
In addition to this within the PCT: o Participated in the Clean, Safe Care and Saving Lives programmes which provide self
assessment tools and guidance on key clinical procedures, audit tools and help with action plans. These publications have informed practice and assisted in infection prevention and control
o Continue to participate in the National Patient Safety Agency cleanyourhands campaign. The Trust has also received a certificate noting its ongoing commitment to this scheme.
o Adopted specific guidance on reporting and management duties e.g. MRSA Screening – Operational Guidance, Going Further Faster etc.
o Can obtain support via the Department of Health and also Strategic Health Authority healthcare associated infection support teams if required
o Promote guidance from the Department of Health and Health Protection Agency pertaining to specific micro-organisms including PVL Staphylococci, Clostridium difficile associated diarrhoea etc.
o Successful registration in January with the Care Quality Commission. On www.worcestershirehealth.nhs.uk it is possible to view the infection control services position statements for key publications.

WPCT IC annual report – June 2009 4
5. Resources • Infection Control Nurses
• 1 wte Nurse Consultant - Carole Clive (CC) • 1.1 wte Completed Training - Cassie Gregory (CG) (0.5wte) and Karen Hall (KH) (0.6wte) • 0.6 wte Training Post Becky Davies (BD)
• Study Days Attended • Tuberculosis – Prevention of a Problematic Pathogen (CG/BD) • Seven C's of change (CG) • Root Cause Analysis training local (CC ) • Root Cause Analysis Toolkit (DH event) (CC) • Management of Automated Endoscopy Washer Disinfectors (KH) • Infection Control – Community (CG/KH) • Water Pathogens and their Management (BD) • Launch of ALERT for cleanyourhands campaign (CC) • Reducing Surgical Site Infections (BD) • ICNet training (CC, BD, CG, KH,GP) • Mentor Assessors Course – Update (BD, CG & KH) • SHA HCAI Forum (CC/BD) • Mandatory training attended by or completed on line by all ICNs.
• Infection Control Doctor Accessed through a Service Level Agreement (employed by Worcestershire Acute Hospitals
Trust). This post was shared between Dr Anne Dyas and Dr Jane Stockley, Consultant Microbiologists. Since October 2008 the service has been provided by Dr Jane Stockley.
• Other • In 2008/2009 the Infection Control Service was delivered within a defined pay and non pay
budget totalling £203,912. The cost of the service level agreement with Worcestershire Acute Hospitals Trust for Consultant Microbiologist support to the Infection Control Service is funded from this budget and in 2008/2009 cost £55,0000; £36,092 in 2007/2008.
• Office at Evesham Community Hospital with the following resources; o Mobile phone with message facility o Portable OHP o 2 Glow and Tell Light Boxes o LCD projector o Digital Camera
o Telephone/Ansaphone/Fax Unit o 3 lap top computers with docking stations o 2 Printers o Books, CD roms and teaching aids o Subscription to Journal of Hospital Infection
6. National initiatives The Infection Control Service has contributed to benchmarking against a number of initiatives detailed below and distributed position statements and educational information and guidelines from the Department of Health and Health Protection Agency as appropriate.
• The implementation of Saving Lives High Impact Interventions initiatives was commenced in March 2008. Within inpatient areas, Matrons, Managers and Infection Control Link Staff were invited to a two hour training session relating to the use of care bundles and high impact interventions. The session focused on the hand hygiene high impact intervention and included discussion as to the implementation of the standard and use of the observational tool. The tool is designed for Acute Trusts and discussion as to how this can be adapted for Primary Care areas was included within the session. Standard Operating Procedures were drafted and the tool has been in use although it is felt that the current audit programme provides a more reliable result. The Infection Control Team has also assessed compliance with appropriate Saving Lives requirements across the PCT. 28 staff from the PCT attended.

WPCT IC annual report – June 2009 5
• Member of clean safe care forum which enable direct access to resources to minimise the spread of infection in clinical practice.
• The PCT is participating in the community “cleanyourhands” campaign. The campaign went live in July 2008 and two series of posters and other awareness raising information was sent to all wards/units within the Trust and GP Practices. Between April 2008 and July 2008 the service campaigned for a cleanyourhands lead in each area. Stages 1, 2 and 3 resources have been distributed and a feedback day attended.
• Evidence gathering for the Healthcare Commissions Standards for Better Health and Special Data Collection exercise. Data has been added for Waste, Decontamination, Cleanliness and Infection Prevention and Control Standards.
• The Team has contributed to the development of action plans and risk registers acknowledging potential risks for decontamination, waste and infection control practices.
• A full review and position statement has been undertaken for compliance of the service with the Health Act (updated 2008) requirements and also Care Quality Commission (2009) requirements.
• Assistance is now provided to undertake a root cause analysis investigation. The Team was involved in the DH work group to review current national tools and have also attended an SHA training event. Cases followed up may relate to the wider health economy or customer organisations and include: • All MRSA bacteraemias diagnosed within the PCT or identified within 48 hours of
admission to another Trust. These are termed pre 48’s and are the responsibility of the previous healthcare provider to investigate. This may be a PCT responsibility if the patient was cared for by their GP prior to admission.
• Any deaths that occur within the PCT where Clostridium difficile associated diarrhoea is considered to be a causative or contributory factor or any deaths that occur within another NHS setting, from Clostridium difficile associated diarrhoea that was diagnosed within 48 hours of admission.
• When a patient has a serious confirmed infection which may be health care acquired and information is required.
• In addition to this, data has continued to be collected following the three month study that has been undertaken (separately) in the PCT which investigated any deaths that occur in patients who have at any time during their stay been diagnosed with Clostridium difficile associated diarrhoea.
• Provision of leaflets for distribution in PCT child development centres and Nursery relating to exclusion in relation to occurrence of childhood infections have been updated.
• Participation in Patient Environment Action Teams/Groups in compliance with the National Standards of Cleanliness in the NHS. Representation and involvement in PCT PEAT group and initiatives is ongoing.
• Decontamination of re-usable medical devices - It was anticipated by the Department of Health when work commenced in 1999 that all sterilization of instruments would occur in approved departments by March 2007. It is now widely recognised, particularly in primary care settings that this is difficult to achieve due to a lack of infrastructure (appropriate departments, huge range and volume of instruments, geographical spread and also availability of disposables). The guidance recommends local decontamination be undertaken as it would be within a sterile services department with all decontamination being carried out away from the patient treatment area and meeting the criteria set for Sterile Services Departments as a minimum. A scoping exercise and subsequent action plan to promote further compliance in the PCT were drafted and the decision made that all bench top steam sterilizers with the exception of those used in Dental be removed and a central contract put in place and where required additional instruments purchased. As an interim measure, the use of disposable instruments has occurred. Within dental, it was agreed that future surgery refurbishment projects would include the commissioning of a washer disinfector and facilitate decontamination practices in compliance with HTM 01 05.

WPCT IC annual report – June 2009 6
• Department of Health Posters in relation to coughs and sneezes, hand hygiene and appropriate use of antibiotics have been distributed across all clinical services.
• Further to recent Department of Health publications relating to Screening for Meticillin Resistant Staphylococcus aureus (MRSA) colonisation and also the Darzi report, it has been necessary for the PCT to review categories of screening prior to admission or surgery. Initially a scoping exercise was undertaken and a plan submitted to the SHA for approval for the Trust. To support this process attendance at Matron/Manager meetings and distribution of explicit information accompanied by training/presentations, securing of appropriate PGDs for suppression treatment in surgical areas, patient information leaflets and drafting of protocols, together with chief executive compliance statements, have ensured that this requirement has been successfully implemented. It is planned as part of the ongoing monitoring to calculate on a monthly basis the number of screens taken.
7. Achievements 2008/2009 In summary, it is accepted that there is no magic solution to tackle the challenge of Healthcare Associated Infection. On review of successes it is noted that these are achieved through a combination of constant vigilance and hard work. The Infection Prevention and Control Team work to approved objectives which facilitate compliance with central publications and the national agenda to ensure that sustained improvements in infection prevention and control are promoted and achieved throughout the health economy. It is recognised that this can be challenging but the embedding of robust infection control practices across customer organisation aims to bring sustained improvements, minimise infection rates and ensure compliance with standards reflecting evidence based best practice 7.1 Policies/Guidelines • Over 300 copies of the Infection Control Policies and Procedures binder have now been
distributed. The availability of this binder and compliance with the guidelines is investigated on each clinical audit that is carried out.
• Due to the volume of routine work it has not been possible to complete the planned update to the Infection Control Policies and Procedures Binder. This is now considered a high priority by the Team. Finalised guidance will also be available on the internet and is currently awaiting ratification.
• Contents of the current Policies and Procedures binder and an additional 26 leaflets on infectious conditions for use by patients, staff and the general public are still available on www.worcestershirehealth.nhs.uk or from the Infection Control Team.
• Ongoing distribution of posters to support a number of clinical practices including manual cleaning of instruments/equipment, cleaning of isolation areas, use of decontamination wipes, hand hygiene and action to take following a needle stick injury etc.
• Promotion of the Third Edition of the Countywide Antimicrobial Prescribing Guidance for Primary Care.
• Guidance has been provided for new build and refurbishment projects to highlight key requirements from an infection prevention and control perspective. Advice has been provided for the re-development and upgrade of wards at ECH, the new build Malvern Hospital, enhancements to the decontamination area at the Integrated Community Equipment Service, Farrier House and also for a number of GP practices, special schools and the lymphoedema services.
• Updating of the leaflet advising on management of childhood infections and appropriate exclusion guidance.
• Ongoing distribution of an A3 Visitors Charter (in poster format) to inpatient areas highlighting how to minimise infection risks and ways in which the Trust minimises these risks, in addition to ongoing distribution of posters detailing infection prevention and control measures. These have predominantly been displayed in health centre and clinic rooms. Leaflets relating to minimising infection risks are also available for use in both inpatient and community settings.
WPCT IC annual report – June 2009 7
• Worcestershire PCT has been acknowledged for partnership working by the pre school learning alliance due to the significant contributions made to their publication relating to good practice in infection control in early years and childcare settings.
7.2 Training and Education The Infection Control Team has continued to develop a range of training and education programmes. The methods of training vary from formal teaching to informal ward based interactive sessions. These are all publicised directly as well as through the Infection Control Training Directory. Attendance at training this year was much lower than in previous years and work is ongoing to ensure attendance is improved in 2009/2010. • During the course of 2008, the new waste management regulations HTM 0701 came into effect.
Over 500 members of staff throughout the county have been trained in the implementation of these new regulations. All Trust sites have been provided with bins, labels, posters and information to promote a smooth transition.
• In addition to the New Waste Regulation Training sessions, over 30 study days/teaching sessions have been provided. All sessions are aimed at raising staff awareness of Infection Control with reference to local and national guidelines and legislation. Some of the topics covered included management of various infections, bloodborne contamination incidents, safe working practices, care of invasive devices etc. Topics for education are related to audit outcomes.
• Teaching sessions have also been provided for the continence team at countywide training (4), Tissue Viability Study Days/Modules (8) Integrated Community Equipment Stores (2), CVC/Nursing Staff undertaking IV access (2), and GP practices (5).
• Presentations have also been provided for the neighbouring Acute Trust, Local Health Protection Unit and Strategic Health Authority.
• Two 2 day courses for Healthcare Assistants within both the PCT and MHPT have been coordinated and run jointly with the Acute Trust. The course attendance was significantly reduced from previous years but evaluated positively. Delegates from PCT detailed below:
DATE PCT HCAs MHPT HCA’s TOTAL
March/April 2008 0 6 6 Sept/Oct 2008 4 0 4 Feb/March 2009 2 4 6
TOTAL 6 10 16 • A Conference and Product Exhibition for Health Care Assistants who have attended a short
infection control course was provided to ensure an opportunity to update, maintain interest in infection control, network and view new products. This event evaluated well and was attended by a total of 16 PCT staff.
• A number of one day update course were provided for various groups of staff. All evaluated well and attendance is detailed below:
STAFF ATTENDING STAFF GROUP PCT MHPT TOTAL
Residential/Day Unit Staff 4 8 12 Healthcare Assistants in the Community 10 - 10 Therapy Staff 3 5 8
• It was necessary to cancel a day planned for qualified PCT staff due to a reduced uptake in the first instance and more latterly, forecasted poor weather conditions. Days have been rescheduled for 2009/2010.
• Five one hour updates on decontamination of re-usable medical devices have been provided in various locations throughout the year. Attendance has been variable with a total of 41 staff

WPCT IC annual report – June 2009 8
attending sessions. These are predominantly from General Practice settings and provider services dental areas.
• A DVD training programme for Pandemic Influenza has now been developed within the region. In addition to the training provided in 2007/2008 when 1034 staff were trained, a clinical refresher guide was developed and this has been updated following the publication of further infection control guidance in 2008.
• Additional teaching sessions have been provided for: • Local podiatrists on Infection Control in Practice. (1) • General Practitioners on Infection Control Risks in Minor Surgery (1) • Practice Nurses on maintenance of the cold chain (2) • Nursing Home staff on management on infection control (1) • Community Equipment Loans Service sessions for community staff and Nursing Homes
on decontamination practices (4) • Healthcare Staff working within Prison settings in conjunction with the local Health
Protection Unit (2).
7.2.1 Link Professionals • Link Professionals have been identified in the majority of clinical services/departments. Staff
are encouraged to complete the Developments in Infection Control course run by Worcester University College worth 20 CAT points at level 3. 13 members of staff successfully completed the course this year. Preparations for a further course later this year have already started. The course was entirely managed by the infection control team with support from the Infection Control Doctor. Up until this year, the course was jointly run with the Acute Trust.
• An eighth Infection Control study day and product exhibition occurred on 20 May 2008 entitled Clean, Safe Care. 68 PCT staff attended this day which acts as an update on current infection control issues and offers staff the opportunity to network and view new products that are displayed by sponsoring company representatives. Feedback from this event was positive and a further event is planned for 21 May 2009, over 120 people attended.
• Four Link Staff Half-Day Training Sessions have been provided to enable further knowledge on specific aspects of infection control practice to be gained. Although attendance is lower than the previous year, staff find these sessions beneficial, all evaluations have been positive. Two sessions were provided on change management within infection control for clinical staff and whilst staff who attended found the sessions worthwhile, it appears that many staff favoured a pure infection control topic.
DATE TOPIC PCT Staff MHPT Staff TOTAL 23 April Scabies/Head lice 10 5 15 16 July Navigating the Seven C’s 11 0 11 15 October Waste 17 2 19 28 January Seven C’s 5 0 5 43 7 50
7.2.2 Student Nurse Education • Five teaching sessions have been carried out for Student Nurses relating to infection prevention
and control practices at Worcester University College. Two of these sessions relate to the provision of basic microbiology and infection control principles which until this year were provided by the university.
• Two 6 week student nurse placements have occurred with the ICNS over the course of the year. This allows Student Nurses to gain insight into the work of Infection Control Nurses and act as a resource for their cohort and on subsequent placements.
WPCT IC annual report – June 2009 9
0
200
400
600
800
Jan Feb
March
April
May June
JulyAug
Sept
OctNov Dec
Month
No.
of c
onta
cts Contacts 1998
Contacts 2000Contacts 2002Contacts 2004Contacts 2006Contacts 2007Contacts 2008Contacts 2009
7.2.3 Online Training • Infection Control online training has been promoted by the team at all training sessions and in
Newsletters; cards have also been designed and distributed to provide information on accessing this module of e-learning. Figures relating to uptake are reviewed through each organisation and collated annually by the team. When this was reviewed in July over 100 staff had accessed the training but not all had completed the modules.
7.2.4 Countywide Induction Reducing the Risk Seminars • Infection Control is incorporated into the Countywide Induction and Update Refresher. 13 one
hour update sessions (2 more than in 2008) were provided over the course of the year in addition to 24 one hour induction sessions (6 more than in 2008). This equates to a total of 37 sessions being provided. Both sessions increased in length to 1 ¼ hours mid year. A number of additional sessions have also been provided when groups of staff clinical/non clinical want infection control updates within their own workplace. To date, this has been provided as requested when reasonable attendance is expected.
• One and one and a half hour Infection Control update sessions have been provided as follow: • 29 April – Speech and Language Therapy – 7 Primary Care Trust staff • 1 May – Speech and Language Therapy – 4 Primary Care Trust Staff • 2 June – Speech and Language therapy – Catshill Clinic – 16 Primary Trust staff • 19 June – Twilight DNs, Malvern Hospital – 8 WPCT staff • 24 June – District Nurses, Malvern GP Practices – 8 PCT staff • 13 August – Abottswood Surgery – 15 WPCT staff • 2 September – Speech and Language Therapy – 16 WPCT staff • 11 September – Speech and Language Therapy – 11 WPCT staff • 18 November – Staff at HMP Long Lartin – 9 PCT Staff
Total time spent teaching from 1 April 2008 – 31 March 2009 – 412 hours excluding preparation
5 Total time spent teaching from 1 April 2007 – 31 March 2008 – 410 hours excluding preparation Total time spent teaching from 1 April 2006 – 31 March 2007 – 399 hours excluding preparation Total time spent teaching from 1 April 2005 – 31 March 2006 – 291 hours excluding preparation
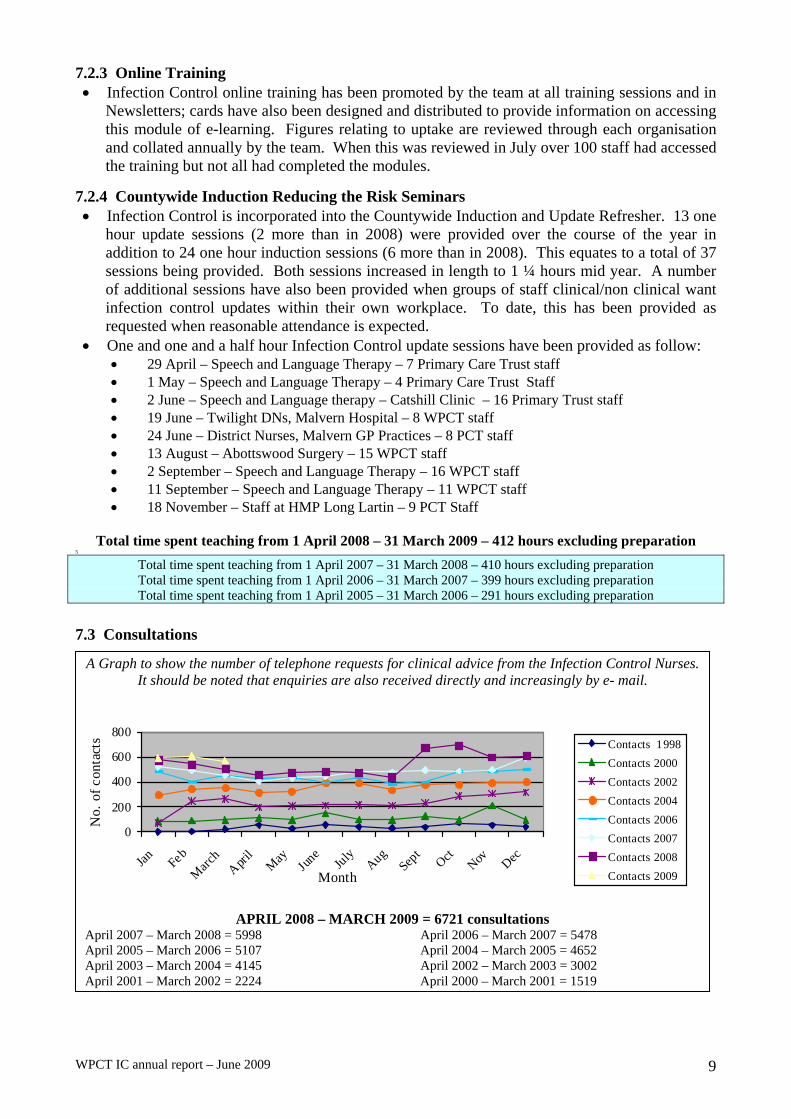
7.3 Consultations
A Graph to show the number of telephone requests for clinical advice from the Infection Control Nurses. It should be noted that enquiries are also received directly and increasingly by e- mail.
APRIL 2008 – MARCH 2009 = 6721 consultations April 2007 – March 2008 = 5998 April 2006 – March 2007 = 5478 April 2005 – March 2006 = 5107 April 2004 – March 2005 = 4652 April 2003 – March 2004 = 4145 April 2002 – March 2003 = 3002 April 2001 – March 2002 = 2224 April 2000 – March 2001 = 1519

WPCT IC annual report – June 2009 10
The higher rate of calls received by the Team during September and October and January and February are clearly attributable to the prevalence of viral gastroenteritis and it is estimated that in excess of 250 calls related to this. The increase in calls in March relates to the implementation of MRSA screening. It is hoped that the number of calls to the service can be kept at approximately 500 calls per month. Obviously the general increase relates to the increasing focus on infection prevention and control nationally and locally. 7.4 Audit An annual programme of Infection Control audit is planned and carried out in all in-patient/residential clinical areas. The Infection Control Nurses Association (2004) audit tool which is endorsed by the Department of Health has been adapted and used for all clinical audits across client organisations. This tool has undergone major revision this year to ensure continued relevance with all new guidance publications. Audits of other facilities, services and procedures have also been carried out as per service objective requirements. A major review of the scoring process to indicate requirements for action was undertaken this year and agreed. This increased the minimum accepted score to 75% from 70%, and altered the banding of red, amber and green scores although not significantly. In addition, an overall total score will be dictated by the lowest rating for an individual section of the audit. It is planned to include information on this in the next annual report.
Kitchens areas are audited on an annual basis with tool modification occurring each year to ensure promotion of standards. Any area/service where an audit score of less than 75% is achieved is re–audited within 3 months.
Between April 2008 and March 2009 the following services have been reviewed using a questionnaire approach to ascertain knowledge on infection control principles and current practices. Upon each review, the questionnaire is refined and updated ensuring promotion of increased, evidence based standards. A summary of the recommendations that have accompanied each review have been sent out routinely to all staff included in the questionnaire:
• 63 questionnaires were distributed to District Nurses working within the Primary Care Trust. A response rate of 48% was received which is below the 65% required to promote reliability and validity of a postal questionnaire. The overall score received was 85% which is 2% up from the overall score received in 2005.
• 50 questionnaires were distributed to Specialist Nurses working within the Primary Care Trust. Despite reminder letters being sent out a response rate of only 30% was received as against 59% in the 2005 study. This is well below the 65% required to promote reliability and validity of a postal questionnaire. The overall score received was 69% as against 77% in 2005.
• 118 questionnaires were distributed to Health Visitors; a response rate of 62% was received. The overall score achieved was 86%. This represents a significant improvement upon the 54% achieved in 2005. A presentation is also planned for this group of staff as part of the feedback from this review.
• The Orchard Service was reviewed for the first time with 39 questionnaires distributed to both qualified staff and healthcare assistants. Unfortunately despite reminders being sent out, only a 49% response rate was received with an overall score of 86%.
• A total of 37 questionnaires were sent out to main stream school nurses, 23 responses were received giving a response rate of 62%. An overall score of 78% was achieved. The section on hand hygiene scored 94% across the service and demonstrated an increase on the previous review in 2005.
• Audits were carried out in 8 Worcestershire schools where School Nurses – Special Needs were involved in an advisory and/or clinical role. The Audit Tool was based on the DH/ICNA (2004) tool and modified by the Infection Control Team to ensure relevant and appropriate criteria for

WPCT IC annual report – June 2009 11
use within this speciality. The range of scores achieved for each school was between 86 - 94% with an average score of 91%.
• Within Podiatry services, 54 observational audits and 7 domicilliary visits were carried out using a modified version of the DH/ICNA Audit Tool (2004). Hand Hygiene, Use of Disinfectants and Waste Regulation section scores were all up on 2005, with an 82% overall score achieved.
• Prisons within the county have all been audited in conjunction with the local health protection unit. As part of this process, infection prevention and control representation is now required at a prison environment work stream group to ensure that recommendations from the visits can be actioned. A re audit of one of these areas is planned for May 2009.
• Twenty-one health centres/clinics were visited in June/July 2008. Within each building, the rooms where direct care/treatment was provided to service users were reviewed. 77 rooms were assessed with regard to Environment, i.e., flooring, work surfaces, fixtures and fittings, overall appearance, availability of facilities, i.e., hand wash sink, deep sink, Methods of disposal used for laundry, sharps, offensive, hazardous and household waste and room usage including cleaning schedules.
• A review of the Lymphoedema Service was undertaken at its new base in Pershore, this was following advice which had been given prior to and during refurbishment work. The overall results demonstrated a good standard of infection prevention and control and it was advised that further consideration be given to enhancing the clinical area to ensure ease of effective cleaning.
• A review of CAMHS service was undertaken, which demonstrated a slight improvement from the previous visit and further recommendations were made to enhance infection prevention and control.
7.4.1 Clinical Programme • Audits have been completed in line with the formal audit programme and also at the request of
individual practitioners. The number of clinical areas audited within the service remit is detailed below. Reports are distributed to individual practitioners and their managers for action. All audit reports are copied to the Director of Infection Prevention and Control or a nominated colleague. Validation of areas is sought to confirm validity of the audit programme for individual organisations prior to the annual programme commencing.
April 2008 – March 2009 127 average score – 91% range 64 – 98% April 2007 – March 2008 112 average score - 91% range 79 – 99% April 2006 – March 2007 121 average score – 92% range 69 – 98% April 2005 – March 2006 117 average score – 80% range 59 – 98%
WORCESTERSHIRE PCT AVERAGE SCORE RANGE 2008/2009 93% 66-100% 2007/2008 93% 83-100% 2006/2007 89% 60 – 95% 2005/2006 90% 65 – 97%
7.4.2 Kitchen audits • Kitchens are audited on an annual basis by the Team this is generally done in conjunction with
the Facilities Department. • The tools used for ward, main and procedural kitchen audits were modified to include recent
legislation and build on existing standards. • The increase in the number of ward/procedural kitchens is due to re-audits following an agreed
increase to the score requirements which act as a precursor for re-audit.

WPCT IC annual report – June 2009 12
Total number of ward/procedural kitchens audited April 2008 – March 2009 = 69 Total number of ward/procedural kitchens audited April 2007 – March 2008 = 64 Total number of ward/procedural kitchens audited April 2006 – March 2007 = 82 Total number of ward/procedural kitchens audited April 2005 – March 2006 = 80 Total number of ward/procedural kitchens audited April 2004 – March 2005 = 68
Total number of ward/procedural kitchens audited 2008/2009 in WPCT = 28
Practices Environment Ward/Procedural Kitchens Average Range Average Range TOTAL
WPCT AREAS 08/09 83% 66 – 98% 88% 50-100% 85% April 2008 – March 2009 82% 56 – 100% 78% 40 – 100 80% WPCT AREAS 07/08 90% 69 – 100% 86% 63 – 100% 88% April 2007 – March 2008 85% 55 – 100% 86% 50-100 85% WPCT AREAS 06/07 89% 69 – 95% 88% 69 – 100% 88% April 2006 – March 2007 85% 48 – 100% 85% 43 – 100% 84% WPCT AREAS 05/06 87% 69 – 98% 80% 42 – 100% 84% April 2005 – March 2006 84% 48 – 100% 80% 42 – 100% 82%
Total number of main kitchens audited: April 2008 – March 2009 = 13 April 2007 – March 2008 = 14 April 2006 – March 2007 = 16 April 2005 – March 2006 = 15
Total number of main kitchens audited 2008/2009 in WPCT = 7
Main Kitchens Facilities Environment Decon. Practices Overall Average 08/09 93 89 88 94 94 Range 08/09 73-100 72-93 74-97 93-100 86-96 Average 07/08 97 82 89 92 91 Range 07/08 91-100 72-93 74-97 76-100 89-93 Average 06/07 86% 85% 87% 90% 87% Range 06/07 80 – 100% 72 – 100% 76 – 100% 80 – 100% 81 -97% Average 05/06 84% 91% 87% 96% 90% Range 05/06 70 – 100% 84 – 100% 75 – 100% 92 – 100% 83 -98% Average 04/05 94% 89% 94% 91% 92% Range 04/05 86 – 100% 75 – 100% 53 – 100% 77 – 96% 73 – 97% Average 03/04 88% 86% 90% 88% 88% Range03/04 50 – 100% 65 – 100% 66 – 100% 59 – 100% 66 – 100% 7.5. Surveillance • Requirements for routine surveillance of ALERT organisms have changed throughout the year in
response to amendments to data collection required by the Health Protection Agency and Department of Health. Predominantly it is still laboratory data which is required and this is returned via Worcestershire Acute Hospitals Trust. The Strategic Health Authority also requires data on MRSA bacteraemias via a weekly return. Health Protection Agency national publications relating to levels of Healthcare Associated Infections have been reviewed by the team throughout the year in addition to regular review at the HCAI forum. Targets have now been set for the health economy 2009/2010 which set a target of 424 cases, a significant reduction on the original target set in April 2008. A target of 15 MRSA bacteraemias is also in place for the health economy.
WPCT IC annual report – June 2009 13
• Within the county, an electronic computer package entitled ICNet Surveillance Programme has been implemented to enable accurate data to be transposed from the laboratory to the Infection Control Teams across the county. This package provides facilities to track positive isolates, record advice given on management and generate reports. The data collected from the system has led to changing of areas that the team are able to report on. It must therefore be noted that information pertaining to nursing homes and ESBL rates are no longer available. The package is used across the county by ICNs and Microbiologists. The team are represented on the countywide ICNet board and IT implementation group. Further information on the ICNet package can be viewed on http://www.icnet.org.uk/. During the course of the next year it is anticipated that a version upgrade will be implemented providing more options
• a) Post-operative targeted wound surveillance is now completed following up on Vasectomies undertaken at Moor Street Clinic. 511 Vasectomy operations have been performed during the study of which 477 patients consented to participate in the surgical site surveillance scheme. This equates to 93% uptake rate. Of these 477 patients, 471 have been followed up either through telephone conversations, letters, or via GP information. This equates to a 99% follow up rate of consented patients. Overall 92% of all vasectomy operations have been followed up on this scheme. 6 patients were sent letters requesting feedback on their post operative recovery. However, no response was received in readiness for this report. Of the 471 patients followed up, 30 patients have been treated as if they have an infection. This equates to a 6.4% infection rate, which is an appropriate outcome for clean/contaminated procedures. A presentation was made to the clinical team and recommendations for future review made.
• A surgical site surveillance scheme is now undertaken on Burlingham Ward at Evesham Community Hospital and at Tenbury Community Hospital. The scheme does not include Dental; Pain; Cystoscopy; D & C or Hysteroscopy patients. Patient feedback from both sites, has been extremely positive and comments have included ‘staff are helpful; friendly; supportive; informative and caring; hospitals are friendly and clean, received excellent care’.
• At Evesham Community Hospital, 1,492 operations (which result in a wound) have been carried out from commencement of the study in October 2006/April 2007. Of these, 927 have been included on the scheme. This equates to a 62% uptake. 20 letters have been sent out to patients who have been non contactable via a phone call. Information requested from patients includes general recovery rate and whether they required treating for an infection. 862 patients have been followed up to date and 75 of these were prescribed antibiotics. This gives an overall infection rate with current sample size of 8.7%. This can be compared to 9.4% which was identified in the initial main report completed in July 2008. It is important to take into account that a number of these cases were not wound infections and it is possible that symptoms could have been attributed to surgical procedure. With the exclusion of these procedures, 63 patients have presented with visible signs and symptoms of infection which equates to a 7.3% overall infection rate.
• At Tenbury Hospital, the scheme was established in January 2008 and 180 patients have been followed up with a 100% overall uptake rate. 3 responses are awaited from letters sent out for feedback. This equates to 98% follow up rate. Of these 180 patients, 4 have been treated with antibiotics which equates to 2.2% infection rate. Data is obviously limited due to the small sample size to date and statistical validity is therefore not achieved at this point of time.
• The surveillance package has been shared with General Practice on request as a way of providing follow up to minor surgery cases and reliable data relating to infection rates.
• b) Continuous monitoring of ‘ALERT’ organisms namely MRSA and Clostridium difficile This is available for each ward/unit and enables follow up on each patient and allows monitoring of whether patients were transferred into this setting with an infection. Surveillance of results

WPCT IC annual report – June 2009 14
obtained within GP practice is also collated in a database to enable identification of trends. Locally, the cases of Meticillin resistant Staphylococcus aureus (MRSA), Clostridium difficile, Extended Spectrum Beta Lactamase Resistant micro-organisms (ESBLs) and Noro/Rotaviruses form most of the follow up.
Clostridium difficile is an infection that causes diarrhoea by replacing some of the normal bacteria that are found in the gut. Symptoms are generally caused by the production of toxins in the large bowel. The main symptom is diarrhoea; however abdominal pain, fever and vomiting might also be present. Symptoms range from mild diarrhoea, which may resolve once antibiotic treatment is stopped, to severe colitis. Environmental cleaning, hand hygiene and the sensible use of antibiotics are the keys to the prevention and control of Clostridium difficile infection. Saving Lives guidance details 11 key controls for minimisation of Clostridium difficile within in patient units, under the headings of Prudent Antibiotic Prescribing, Correct Hand Hygiene, Appropriate Environmental Decontamination, Use of Personal Protective Clothing and Isolation/Cohort Nursing. The infection control service in following up all cases presenting within in patient areas can demonstrate a 99.6% compliance with these requirements in clinical areas. (Extended Spectrum Beta Lactamase) ESBLs are a group of Gram-negative bacteria (predominantly bowel organisms), such as Escherichia coli and Klebsiella species, which can produce enzymes that break down antibiotics, rendering them ineffective. Traditional first-line treatment drugs are no longer effective if the infection is caused by ESBL-producing bacteria. In the past these outbreaks have been seen in hospitals rather than the community however there have been some community outbreaks noted in England over the period of this report. Reporting on these micro-organism across GP practice cannot be undertaken at this time with ICNet but future provision is being investigated. Meticillin Resistant Staphylococcus aureus carriage is endemic amongst the population. It is estimated that 30% of people are colonised Staphylococcus aureus. ‘Colonised’ means that the bacteria lives harmlessly on a person’s skin or in the nose and does not cause any harm. If MRSA breaches the body’s natural defence mechanisms and causes an actual infection it becomes difficult to treat and is considered as one of the most serious Healthcare Associated Infections. It is recognised that several factors increase the likelihood of acquisition of MRSA infection in healthcare settings, these include poor levels of cleaning and hand hygiene. As part of DH (2008) and Lord Darzi’s recommendations, a programme for MRSA screening was implemented during March 2009. Screening occurs prior to certain elective procedures, on admission to all provider services non surgical beds and for identified risk groups in mental health settings. Noroviruses are a group of viruses that are the most common cause of gastroenteritis in England and Wales. In the past, noroviruses have also been called ‘winter vomiting viruses’, ‘small round structured viruses’ or ‘Norwalk-like viruses’. The virus is easily transmitted from one person to another and can be transmitted by contact with an infected person; by consuming contaminated food or water or by contact with contaminated surfaces or objects. Spread from person to person is via the faecal-oral route and by vomiting which leads to widespread aerosol dissemination of viral particles, environment contamination and subsequent indirect person to person spread, This variety of mechanisms for spread increases the virus’s transmissibility. The symptoms of norovirus infection generally begin around 12 to 48 hours after becoming infected and usually the illness is self-limiting with symptoms lasting for 12 to 60 hours, this can however be longer in babies and young children. Illness starts with a sudden onset of nausea followed by often a projectile vomit and watery diarrhoea. Some people may complain of abdominal pain, have a raised temperature, headaches and aching limbs. Most people make a full recovery within 1-2 days but in some cases, particularly in young children or the elderly, medical intervention may be required due to dehydration. It must be noted that there is no specific treatment for norovirus apart from letting the illness run its course. Due to the increased prevalence of norovirus across the health economy this year, in addition to the enteric precautions which are routinely put in place, including promotion of safe working practices,

WPCT IC annual report – June 2009 15
hand hygiene, use of personal protective clothing, minimising staff working in other areas and additional cleaning schedules including the use of hypochlorite solutions, a number of awareness raising initiatives were undertaken by the team. This was in addition to prolonged implementation of above recommendations and promotion of prompt recommendations to minimise any potential outbreaks. Some of the measures included bleach cleaning of toilet areas on hospital and inpatient sites (including staff, ward and general public toilet areas) on a daily basis, as opposed to the normal cleaning regime that would otherwise be followed. Information was circulated relating to the importance of checking with Agency/Bank Staff when they arrive on duty to ensure they have not worked in areas where viral gastroenteritis is confirmed or suspected in an outbreak situation in the 48 hours prior to their current shift. Outbreaks are detailed in Section 7. Rotavirus gastroenteritis is caused by the rotavirus, which is a virus that tends to spread easiest amongst children. It is the most common cause of viral gastroenteritis in children and most will have been infected by rotavirus by the age of five. After initial infection, usually some immunity is gained so future infections will be less severe. Rotavirus also affects adults although usually it is less severe as will have some immunity to the infection. Rotavirus can cause severe vomiting and diarrhoea and abdominal cramps, occasionally it may cause fever. During outbreaks enteric precautions are put into place; these include promotion of safe working practices, hand hygiene, use of personal protective clothing, minimising staff working in other areas and additional cleaning schedules including the use of hypochlorite solutions.
c) Data for inpatient areas total figures indicative of Primary Care
ALERT organisms – New Cases – In-patients DATE Mycobacterium
tuberculosis
Meticillin resistant Staphylococcus
aureus Clostridium difficile
Extended Spectrum Beta
Lactamase WPCT 2008 - 2009 1 97 43 27 April 2008 - 2009 1 105 45 31 WPCT 2007-2008 0 114 67 23 April 2007 – March 2008 0 128 72 26 WPCT 2006 - 2007 1 143 95 17 April 2006 – March 2007 1 165 101 20 WPCT 2005 - 2006 - 151 99 14 April 2005 – March 2006 - 176 102 17 The data above demonstrates that levels of positive isolates presenting, most noticeably for Clostridium difficile, have reduced significantly. This figure is not reportable as it includes all cases presenting within inpatient areas. The count for HPA purposes is detailed in the table below and details cases which were diagnosed within PCT areas, not cases which were diagnosed in other healthcare settings, relapses presenting within 28 days or patients on long term reducing treatment. There have been no MRSA bacteraemias presenting within the PCT for the period of this report.
Clostridium difficile POSITIVE ON ADMISSION
POSITIVE WITHIN 48 HRS
POSITIVE DURING ADMISSION
TOTAL NUMBER
07/8 08/09 07/08 08/09 07/08 08/09 07/08 08/09 PCT/MHPT 14 11 22 7 36 27 72 45 WPCT 13 11 20 7 34 25 67 43
Meticillin resistant Staphylococcus aureus POSITIVE ON ADMISSION
POSITIVE WITHIN SEVEN DAYS
POSITIVE DURING ADMISSION
TOTAL NUMBER
07/08 08/09 07/08 08/09 07/08 08/09 07/08 08/09 PCT/MHPT 55 61 40 27 33 17 128 105 WPCT 52 58 35 24 29 15 122 97

WPCT IC annual report – June 2009 16
• Other ALERT organisms recorded in in-patient areas over the last year have included Campylobacter (2), Chicken Pox (1), Head Lice (2), Salmonella (1), Scabies (4), Shingles (4), Stenotrophomonas (2), VRE (2).
. Table to detail figures returned on the MESS database for monitoring Clostridium difficile target.
MONTH April May June July Aug Sept Oct Nov Dec Jan Feb March Total PCT Provider 2 1 3 2 3 4 5 1 2 3 0 2 28
MHPT 0 0 0 0 0 1 0 0 0 0 1 0 2 GP 16 11 ** 6 *** 8 10 **** 8** 4 5 2 10 6 *** 6 **** 92
** One case relates to a GP practice in South Birmingham PCT *** One case relates to a GP practice in Shropshire PCT **** One case relates to a GP practice in Herefordshire PCT
d) Data for General Practice settings • Data is collated each quarter for positive isolates (infection/colonisation) relating to cases of
Meticillin Resistant Staphylococcus aureus, Clostridium difficile and for part year on Extended Spectrum Beta Lactamase infections from General Practice settings in Worcestershire. This relates to practices that utilise laboratory services at the Alexandra Hospital, Redditch or Worcestershire Royal Hospital.
A table to detail cases of ALERT organisms within Worcestershire GP practices based on laboratory data from
Worcestershire Acute Hospitals NHS Trust Number of Positive Isolates
YEAR Clostridium difficile ESBLs Meticillin Resistant Staphylococcus aureus
2006/2007 149 104 938 2007/2008 147 264 839 2008/2009 92 (6 non PCT) 46 * 598 * part year • e) All positive samples processed for Clostridium difficile associated diarrhoea in
community patients have been routinely followed up since August 2006 to identify potential predisposing factors. This has enabled targeted education, implementation of targeted measures to reduce occurrence and ongoing monitoring of the implementation.
During 2008-2009 the change-over to reporting directly from ICNet occurred. Therefore changes in data reported has had to occur. Since September 2008 it has not been possible to report on ESBL isolates or cases of ALERT organisms presenting within nursing homes. Discussions are currently in progress with ICNet as to how this information can now be collated. At this moment in time, there does not appear to be any noticeable change in trends which could indicate an increase in either of these categories.
Tables to detail positive isolates for year 2008/2009 in Worcestershire GP Practices by locality MRSA positive isolates (NOT MRSA BACTERAEMIAS)
Period Malvern, Pershore and Evesham
Redditch and Bromsgrove
Worcester, Droitwich and Ombersley
Wyre Forest and Tenbury Totals
Apr 08 –Mar 09 81 210 170 137 598
Clostridium difficile positive isolate
Period Malvern, Pershore and Evesham
Redditch and Bromsgrove
Worcester, Droitwich and Ombersley
Wyre Forest and Tenbury Totals
Apr 08 – Mar 09 17 15 36 18 86

WPCT IC annual report – June 2009 17
Extended Spectrum Beta Lactamase (ESBLs) positive isolate
Period Malvern, Pershore and Evesham
Redditch and Bromsgrove
Worcester, Droitwich and Ombersley
Wyre Forest and Tenbury Totals
Apr – Sept 08 9 29 5 3 46
Norovirus (only tested if clinical need e.g. outbreak)
Period Malvern, Pershore and Evesham
Redditch and Bromsgrove
Worcester, Droitwich and Ombersley
Wyre Forest and Tenbury Totals
Oct 08 - March 09 1 0 12 6 19
Rotavirus
Period Malvern, Pershore and Evesham
Redditch and Bromsgrove
Worcester, Droitwich and Ombersley
Wyre Forest and Tenbury Totals
Jan – Mar 09 11 16 38 10 75
8. The Strategic Health Authority has determined that a root cause analysis in compliance with Department of Health requirements should be undertaken for infections that fulfil the following criteria: • All MRSA bacteraemia. If diagnosed within the PCT or MHPT they are the responsibility of the
individual Trust to investigate. If they are identified within 48 hours of admission to another Trust, these are termed pre 48’s and are the responsibility of the previous healthcare provider to investigate.
• Any deaths that occur within the PCT/MHPT from Clostridium difficile associated diarrhoea where it was listed as the 1A cause of death were followed up prior to October 2007. Following this the team have followed up all deaths where Clostridium difficile is detailed on the death certificate. From December 2007 to March 2008 the service has participated in the Healthcare Commission Study to follow up all inpatients that have developed Clostridium difficile during their stay and subsequently died prior to discharge regardless of whether this is linked to their infection or status.
• Any deaths that occur within another NHS setting (predominantly this will be Worcestershire Acute Hospitals Trust) from Clostridium difficile associated diarrhoea that was diagnosed within 48 hours of admission, and listed as the 1A cause of death prior to October 2007 plus all deaths since where it is detailed on the death certificate as a contributory factor.
• When a patient has a serious confirmed infection which may be health care acquired and information is required.
• Investigations also occur when people die in the wider community eg. own home, nursing/residential home with the above criteria.
A synopsis of the above is presented at the Health Economy HCAI meetings as the need arises and lessons learnt are disseminated throughout the organisation. A total of 8 root cause analysis have been undertaken during this year for MRSA bacteraemias and 11 for Clostridium difficle associated diarrhoea (this includes completion of cases from previous year). There are two cases outstanding from current year (information awaited). With the exception of one case these do not relate to inpatients within provider services.
9. Outbreak Management Outbreak Management has been highlighted in the Infection Control Service Newsletter to promote the importance of prompt detection and appropriate management in addition to regular contact with key clinical areas during times of increased prevalence of viral gastroenteritis. Complete guidance is contained within section F of the Infection Control Policies and Procedures Binder. The number of outbreaks for the period of this report is 22, 18 of which relate to the PCT and these are detailed below. In comparison for the 2007/2008 period there were 11; in 2006/2007 period there were 11; for the 2005/2006 period there were 4. All outbreaks included in the period of this report, with the exception of one, relate to gastro-

WPCT IC annual report – June 2009 18
intestinal illness. The one outbreak not related to this is chicken pox within Noah’s Ark Day Nursery, where appropriate measures were put in place to minimise spread. It must be noted that although there has been a significant increase in Norovirus Outbreaks, appropriate management precautions were implemented in a timely manner on all occasions. Staff knowledge and management is to be commended and on the majority of occasions the small number of cases and reduced duration of ward closures can be attributed to high standards of infection control practice.
. Area and Month Number of people affected Causative organism
Tenbury Hospital February 2009
13 Patients 12 Staff 1 Relative
Viral Gatroenteritis with no microbiological confirmation to date,
further testing requested Cottage Ward, Princess of Wales Community Hospital February 2009
5 Patients 4 Staff 1 Confirmed Norovirus other cases
presented with no positive microbiology or epidemiological links
William Astley Ward, Evesham Community Hospital February 2009
5 Patients 3 Staff Norovirus Confirmed
Willows Ward, Evesham Community Hospital February 2009
7 Patients Unlikely to be connected cases, no
positive microbiology or epidemiological links
Bredon Ward, Evesham Community Hospital February 2009
3 Patients 4 Staff Norovirus Confirmed
Noah’s Ark Day Nursery, ECH February 2009 33 Children Chicken Pox
Cottage Ward, Princess of Wales Community Hospital 6 Patients
Unlikely to be connected cases, no positive microbiology or
epidemiological links Pershore Hospital January 2009 6 Patients 5 Staff Viral Gastroenteritis suspected
Houseman Unit, Princess of Wales Community Hospital January 2009
4 Patients 1 Staff Viral Gastroenteritis suspected
Lickey Ward, Princess of Wales Community Hospital December 2008
3 Patients 1 Staff 3 Relatives Norovirus confirmed
Noah’s Ark Day Nursey, ECH October 2008 9 Children/Babies 2 Staff Viral Gastroenteritis suspected
GP Unit, Kidderminster October 2008 7 Patients 3 Staff Viral Gastroenteritis suspected
Lickey Ward, Princess of Wales Community Hospital October 2008
19 Patients 6 Staff 1 Relative Norovirus Confirmed
Pershore Hospital September 2008 6 Patients
Unlikely to be connected cases, no positive microbiology or
epidemiological links. Houseman Unit, Princess of Wales Community Hospital September 2008
7 Patients 1 staff Norovirus confirmed
Izod Ward, Evesham Community Hospital May 2008
12 Patients 2 Staff Norovirus confirmed
Tenbury Hospital (Wards) May 2008 10 Patients 8 Staff Norovirus confirmed
Lickey Ward, Princess of Wales Community Hospital May 2008
6 Patients 14 Staff 1 Relative Norovirus confirmed

WPCT IC annual report – June 2009 19
10. Published literature reviewed The following publications were noted and discussed as appropriate at Infection Control Committee Meetings. Publications indicated with a * have also been the subject of a review and/or position statement on behalf of both client organisations: CAS (2009) Increase in Invasive Group A Streptococcal Infections In England https://www.cas.dh.gov.uk/ViewAndAcknowledgment/viewAlert.aspx?AlertID=101179 CQC (2008) Registering with the Care Quality Commission in relation to healthcare associated infection 2009/10* http://www.cqc.org.uk/pdf/CQC_registration_HCAI_guidance_27_10_2008.pdf CQC (2009) Press Release in relation Infection Prevention and Control DH (2008) Changes to arrangements for regulating NHS bodies in relation to healthcare associated infections for 2009/10: a consultation for the NHS http://www.dh.gov.uk/en/Consultations/Liveconsultations/DH_086926 DH (2008) MRSA Screening – Operational Guidance * http://www.dh.gov.uk/en/Publicationsandstatistics/Lettersandcirculars/Dearcolleagueletters/DH_086687 DH (2008) Pandemic influenza: Guidance for Dental Practices http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_087736 DH (2008) Letter - Measles - Protection of Health Professionals DH (2008) Vaccine Supply–Primary Immunisations http://www.immunisation.nhs.uk/files/vaccinesupply_letter160508.pdf DH (2008) Going Further Faster II: applying the learning to reduce HCAI and improve cleanliness http://www.clean-safe-care.nhs.uk/ArticleFiles/Files/82825-COI-Focus%20further%20faster(WEB)_FINAL_June%2013.pdf DH (2008) Decision Scorecards in Relation to Clostridium difficile associated diarrhoea * http://www.clean-safe-care.nhs.uk/ArticleFiles/Files/101.pdf and http://www.clean-safe-care.nhs.uk/ArticleFiles/Files/103.pdf DH (2008/2009) Flu News Publications - ongoing DH (2008)Pandemic influenza: guidance for primary care trusts and primary care professionals on the provision of healthcare in a community setting in England DH (2008) Travel safe: reducing the risk of getting a blood-borne infection when you're abroad. DH (2008) The Health Act (2006). Code of Practice (Revised and Updated Jan 2008). * DH (2008) Antimicrobial Resistance and HCAI Newsletter - ongoing DH (2009) MRSA Screening – Operational Guidance 2 * DH (2009) Information Relating to MRSA screening for Mental Health Settings * http://www.clean-safe-care.nhs.uk/ArticleFiles/Files/Screening-for-Mental-Health-patients_Final-Guidance.pdf DH (2009) MRSA Screening Frequently Asked Questions (version 4 – final) DH (2009) MRSA Screening Leaflet – What to Expect? DH (2009) MRSA Screening Leaflet – A Positive Result? DH (2009) Decontamination of Dental Instruments DH/HPA (2009) Clostridium difficile infection: How to deal with the problem. * http://www.hpa.org.uk/web/HPAwebFile/HPAweb_C/1232006607827 HPA (2008) Guidance on the Diagnosis and Management of PVL-associated Staphylococcus aureus infections (PVL-SA in England) HPA (2008) Guidance on Infection Control in Schools and other Child Care Settings. * HPA (2008) Pandemic Influenza Contingency Plan http://www.hpa.org.uk/webw/HPAweb&HPAwebStandard/HPAweb_C/1197382223603?p=1153846674367 HPA (2009) Clostridium difficile associated diarrhoea quarterly counts - ongoing Letter from Prime Minister to NHS Staff in relation to reduction in MRSA Bacteraemias (sept 08) http://www.clean-safe-care.nhs.uk/Documents/Open_letter_to_all_NHS_Staff.pdf NICE (2008) Guidelines for Surgical Site Infection http://www.nice.org.uk/Guidance/CG74 NICE (2009) Review of Guidance CG2 http://www.nice.org.uk/Guidance/CG2 NPSA (2008/09) cleanyourhands bulletins – ongoing http://npsacleanyourhands.createsend5.com/viewEmail.aspx?cID=C545EE0CCBB92267&sID=59F6F44BDEEB2530&dID=5CB9CB5A1CE688CE NPSA (2008) cleanyourhands Training Video http://www.npsa.nhs.uk/cleanyourhands/the-campaign/training-video/ NPSA (2008) Patient Safety Alert Clean Hands Save Lives 2 September 2008 PL CMO (2009 Influenza Immunisation Programme 2009/10 WHO (2009) Save Lives – Clean Hands Correspondence has been received from the Strategic Heath Authority relating to:
• Undertaking of MRSA Root Cause Analysis. • Undertaking MRSA screening.

WPCT IC annual report – June 2009 20
• Involvement in new build Malvern hospital project • Reporting of MRSA bacteraemias on a weekly basis • Planning and implementation of screening programme • Monitoring of Clostridium difficile associated diarrhoea • Prevalence of viral gastro-enteritis across the region • Information relating to Care Quality Commission requirements for the Decontamination of re-
usable medical devices 11. Issues identified and action taken • Provision of assistance on Contingency Planning for Pandemic Influenza including the purchase
of a stockpile of items as part of a countywide group. • Provision of position statements in relation to key documents published by the Department of
Health and Care Quality Commission. • Continued involvement in promotion of waste segregation practices across PCT and GP
practices including participation in internal audit review and waste management group. • Ongoing involvement in waste segregation and monitoring practices including an internal audit
undertaken at the request of the MHPT. • Involvement in a scoping exercise to establish volume of MRSA screens likely to be undertaken
in primary care following implementation of the Darzi guidance. Subsequent implementation of screening recommendations across the PCT and participation in development of patient group directions for suppression treatment in surgical patients.
• Guidance has been provided for new build and refurbishment projects to highlight key requirements from an infection prevention and control perspective. Advice has been provided for redevelopment and upgrade of wards at ECH, the new build Malvern Hospital, Farrier House, a number of GP practices, the community equipment service and a number of other PCT refurbishments/new developments.
• Provision of advice and updated leaflet on exclusion periods for use in client organisation child care facilities.
• Decontamination guidance relating to re-usable medical instruments within PCT directly managed services and GP settings in relation to the DH Decontamination Strategy; including assistance in option appraisal and scoping exercise to cease use of bench top steam sterilizers which was implemented for 1 April 2009.
• Provision of advice in relation to infection control implications associated with water systems in community hospitals and general practices.
• Provision of advice in relation to minor surgery requirements in General Practice settings. • At the request of the Child and Family Services Department based at Newtown a review of the
environment and practices to prevent and control infection was undertaken. • Maintenance of electronic links to the Service via www.worcestershirehealth.nhs.uk enabling
information and guidance on various aspects of the infection control service to be widely available.
• Involvement in discussions relating to the provision of drinking water through mains fed units rather than portable units.
• Undertaking of visits to shared health and county council buildings to review infection prevention and control in association with accommodation.
• Involvement in purchase of washer with capacity to provide thermal disinfection for use at the Community Equipment Service to process equipment.
12. Awareness Raising • Provision of “De-Bugged” Newsletter on a quarterly basis for onward dissemination and, in
addition to this, updates on waste management have also been provided. • Provision of an awareness raising fact sheet for non clinical staff to ensure they are aware of
infection prevention and control within NHS Trusts. • Update to leaflet advising on Infection Control Guidance for use in child care settings relating to

WPCT IC annual report – June 2009 21
management of childhood infections. • Continued provision of leaflets detailing a number of common infections that can be used as a
resource for staff or patients/visitors in addition to leaflets advising on ways in which the risk of Healthcare Associated Infections can be reduced.
• Celebration of Food Safety Week in June through the provision of quizzes, puzzles, posters, coasters and display board material.
• Although arrangements were made to enable infection control information to be displayed on computers across the Trusts during focus weeks, this was not successful.
• Response to increasing media interest and freedom of information requests on infection control, particularly in relation to Meticillin Resistant Staphylococcus aureus and Clostridium difficile associated diarrhoea.
12.1 Hand Hygiene • Hand Hygiene is routinely included in all study days, short courses and update sessions provided
by the Team. • Glow and Tell Box use is now promoted in all areas/departments within each organisation and in
the wider community (Sure Start Groups, Schools, Nursing Homes etc.) for encouraging effective hand hygiene.
• Clean Hands Save Lives NPSA Alert issued in September set out to provide guidance on best practice in hand hygiene at the point of care, to contribute to reducing healthcare associated infection (HCAI) in the NHS. Broad compliance with the Alert was reviewed at time of issue and it is planned to strengthen this process further by including key elements of the Alert in subsequent audit programmes.
• Replacement as required of floor stickers to promote hand hygiene at the entrance and exit of community hospital wards.
• Implementation of Hand Hygiene High Impact Intervention to increase compliance with Hand Hygiene requirements at ward level.
• Distribution of all materials for the cleanyourhands campaign. Prior to this, a three month preparation period occurred identifying leads within each area and formalising process with all GP practices.
• Staff remain able to access additional training on hand hygiene from the current supplier, infection control team or through web links; additionally posters are available from the Infection Control Team.
• Provision of a fact sheet on the importance of hand hygiene to increase awareness of non clinical staff.
13. PCT actions required The responsibilities placed on NHS organisations are set out in the guidance mentioned throughout this report. The following should be noted:- • Ongoing consideration and discussion of the implications posed by Department of Health
publications and targets in relation to provider and commissioned services. • Information relayed to the team in a timely manner when Trusts are requested by other bodies to
provide data on ALERT micro-organisms such as Clostridium difficile and MRSA or carry out Root Cause Analysis.
• Maintenance of communication links and accountability arrangements between individual organisations and Infection Control Service to ensure dissemination of information.
• Discussion of Infection Control Service annual report at Trust Board or equivalent. • Provision of designated outbreak funding within each organisation. • Promotion of Infection Control training to Medical Staff. • Support to ensure that an appropriate service level agreement and specific service objectives for
2009/2010 are formulated and signed off by customer organisations. • Provision of resources to ensure appropriate level of service can be provided.

WPCT IC annual report – June 2009 22
• In addition to the above, it must be recognised that there are a number of emerging challenges which need to be taken into account and will require addressing to ensure an appropriately resourced infection and prevention service for the health economy.
These include:
ο Monitoring of commissioned services. ο Need to consider from where advice for general dental practice, high street pharmacies
and opticians is currently sought. ο Need for provision of an infection control service to nursing and residential homes. ο Need for compliance with future registration requirements for Care Quality Commission
in non NHS Trust settings. ο Continued importance on infection prevention and control nationally and locally. ο Increased surveillance due to anticipated 10% increase in MRSA positive isolates. ο Ongoing increased prevalence of viral gastro-enteritis across the health economy.
Infection Control Team on behalf of
Worcestershire Primary Care Trust June 2009
References Department of Health. (1995). Hospital Infection Control-Guidance on the Control of Infection. PHLS. London. Chief Medical Officer. (2003). Winning Ways. Department of Health. December 2003. http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_4064689.pdf Department of Health. (2007). Saving Lives including High Impact Interventions http://www.dh.gov.uk/en/Publichealth/Healthprotection/Healthcareacquiredinfection/Healthcareacquiredgeneralinformation/ThedeliveryprogrammetoreducehealthcareassociatedinfectionsHCAIincludingMRSA/index.htm Department of Health. (2006). Essential Steps to Safe Clean Care http://www.dh.gov.uk/en/Publichealth/Healthprotection/Healthcareacquiredinfection/Healthcareacquiredgeneralinformation/ThedeliveryprogrammetoreducehealthcareassociatedinfectionsHCAIincludingMRSA/index.htm Department of Health. (2006). The Health Act 2006: Code of Practice for the Prevention and Control of Healthcare Associated Infections (Updated 2008). http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_081927 Healthcare Commission. 2007. Standards for Better Health. Health Service Circular. (2000). The Management and Control of Hospital Infection. HSC 2000/02. Pratt RJ; Pellowe CM; Wilson JA; Loveday HP; Harper P; Jones SRLJ; McDougall C; Wilcox MH. (2007). Epic 2: National Evidence-Based Guidelines for Preventing Healthcare-Associated Infections in NHS Hospitals in England. Hospital Infection Society. http://www.neli.org.uk/IntegratedCRD.nsf/e0babdca13c1cc428025705f003c19c8/74e975b7665fceaa802572170036d353?OpenDocument