ineos employee benefits 2011 open enrollment booklet ... o.e. plan changes booklet... · 2 this...
TRANSCRIPT

INEOS Employee Benefits
2011 Open EnrollmentBooklet
Explanation of Changes


2
This booklet contains detailed information regarding yourbenefit plans. Certain plan provisions are highlighted asan indication of change from a prior benefit plan. Someof these changes will pertain to USA plans, Heritageplans or, in some cases, both. In the event anydiscrepancies arise between this booklet and theSummary Plan Description, the information in theSummary Plan Description will prevail.
Table of Contents
MedicalPlan Design Summary Chart 1Other Important Information 3Expenses Covered 4Expenses Not Covered 4Prescription Drugs 7Patient Protection and Affordable Care Act (PPACA) 8Employee Eligibility 9Dependent Eligibility 9Wellness 9Opt-Out Credit 9
DentalPlan Design Summary Chart 10Expenses Not Covered 12Other Important Information 14Employee Eligibility 14Dependent Eligibility 14Opt-Out Credit 14
VisionPlan Design Summary Chart 15
Flexible Spending Accounts 16
Long-Term Disability 17
Benefits Website 19

1
Medical
Plan Design Summary ChartThe medical plan comparison chart details all plan provisions under the 80% PPO Plan and 90%PPO Plan. It includes a section of “Expenses Covered” and “Expenses Not Covered”. The“Other Important Information” section provides details on how copays, deductible and out-of-pocket maximums will be applied.
80% PPO Plan
(formerly USA PPO Choice)
90% PPO Plan
(formerly Heritage PPO Select)
In-Network Out-of-Network In-Network Only Out-of-Network
General Information
Deductible(excludes copays)
$450/person;
$1,350/family
$900/person;$2,700/family
$225/person;
$675/family
$450/person;
$1,350/family
Out-of-pocket maximum(includes copays,coinsurance and deductible)
$2,000/person;$4,000/family
$4,000/person;$8,000/family
$2,000/person;$4,000/family
$4,000/person;$8,000/family
Lifetime maximum benefit None None None None
For the following treatments and services, the medical plan options pay:
Physician Office Visits
Primary care office visit 100% after $20 copay 60% after deductible 100% after $20 copay 70% after deductible
Specialist office visit 100% after $30 copay 60% after deductible 100% after $30 copay 70% after deductible
Maternity services 80% after deductible 60% after deductible 90% after deductible 70% after deductible
Lab and X-ray 80% after deductible 60% after deductible 90% after deductible 70% after deductible
Preventative Care (Routine Services Only)
Annual physicals 100%; no copay ordeductible
60% after deductible100%; no copay ordeductible
70% after deductible
Gynecological Exam (1 examevery calendar year, inaddition to RoutinePhysical)
100%; no copay ordeductible
60% after deductible100%; no copay ordeductible
100%; no copay ordeductible
Routine Pap Smear 100%; no copay ordeductible
60% after deductible100%; no copay ordeductible
100%; no copay ordeductible
Routine Breast Exam 100%; no copay ordeductible
60% after deductible100%; no copay ordeductible
70% after deductible
Routine Mammograms 100%; no copay ordeductible
60% after deductible100%; no copay ordeductible
70% after deductible
Routine Digital Rectal Exam 100%; no copay ordeductible
60% after deductible100%; no copay ordeductible
70% after deductible
Routine Prostate SpecificAntigen (PSA) tests
100%; no copay ordeductible
60% after deductible100%; no copay ordeductible
70% after deductible
Routine Bone Density Test 100%; no copay ordeductible
60% after deductible100%; no copay ordeductible
100%; no copay ordeductible
Routine Colonoscopy 100%; no copay ordeductible
60% after deductible100%; no copay ordeductible
70% after deductible
Routine Colorectal CancerScreening
100%; no copay ordeductible
60% after deductible100%; no copay ordeductible
70% after deductible
Well-child care 100%; no copay ordeductible
60% after deductible100%; no copay ordeductible
70% after deductible

2
80% PPO Plan 90% PPO Plan
In-Network Out-of-Network In-Network Only Out-of-Network
Immunizations, HPVvaccine, Shingles vaccine
100%; no copay ordeductible
60% after deductible100%; no copay ordeductible
70% after deductible
Smoking Cessation 100%; no copay ordeductible
60% after deductible100%; no copay ordeductible
70% after deductible
Obesity Screening andCounseling
100%; no copay ordeductible
60% after deductible100%; no copay ordeductible
70% after deductible
Routine Lab Procedures 100%; no copay ordeductible
60% after deductible100%; no copay ordeductible
70% after deductible
Emergency ServicesHospital emergency room(applies to facility chargesonly) the copay is waived ifadmitted
80% after $100 copay 80% after $100 copay 90% after $100 copay 90% after $100 copay
Ambulance 80% after deductible 60% after deductible 90% after deductible 70% after deductible
Outpatient Services (services provided other than in a physician’s office)
Outpatient surgery facility 80% after deductible 60% after deductible90% after deductible
(no copay)70% after deductible
Physician/surgeon andrelated professional fees 80% after deductible 60% after deductible 90% after deductible 70% after deductible
Lab and X-ray 80% after deductible 60% after deductible 90% after deductible 70% after deductibleRadiation therapy/chemotherapy 80% after deductible 60% after deductible 90% after deductible 70% after deductible
Inpatient Hospital Services
Room and board (semi-private room), other facilityservices and supplies
80% after deductible;$100 copay peradmission applies
60% after deductible;$100 copay peradmission applies
90% after deductible;$100 copay peradmission applies
70% after deductible;$100 copay peradmission applies
Physician hospital visits,surgery and relatedprofessional fees (includingmaternity and newborncare)
80% after deductible 60% after deductible 90% after deductible 70% after deductible
Lab, X-ray and anesthesia 80% after deductible 60% after deductible 90% after deductible 70% after deductible
Alternatives to Inpatient Hospital Care
Skilled nursing facility(120 days per plan year) 80% after deductible 60% after deductible
90% after deductible(previously notcovered)
70% after deductible
(previously notcovered)
Home health care(120 visits per plan year) 80% after deductible 60% after deductible 90% after deductible 70% after deductible
Outpatient hospice care 80% after deductible 60% after deductible 90% after deductible 70% after deductible
Outpatient private dutynurse(120 visits per plan year)
80% after deductible 60% after deductible
90% after deductible
(previously notcovered)
70% after deductible
(previously notcovered)
Other Covered Services
Chiropractic care80% after deductible
(removed visit limits)
60% after deductible
(removed visit limits)90% after deductible 70% after deductible
Durable medical equipment;orthotics; consumablemedical supplies
80% after deductible 60% after deductible 90% after deductible 70% after deductible
Prosthetic appliances(including external breastprostheses); wigs
80% after deductible 60% after deductible 90% after deductible 70% after deductible
3
80% PPO Plan 90% PPO Plan
In-Network Out-of-Network In-Network Only Out-of-Network
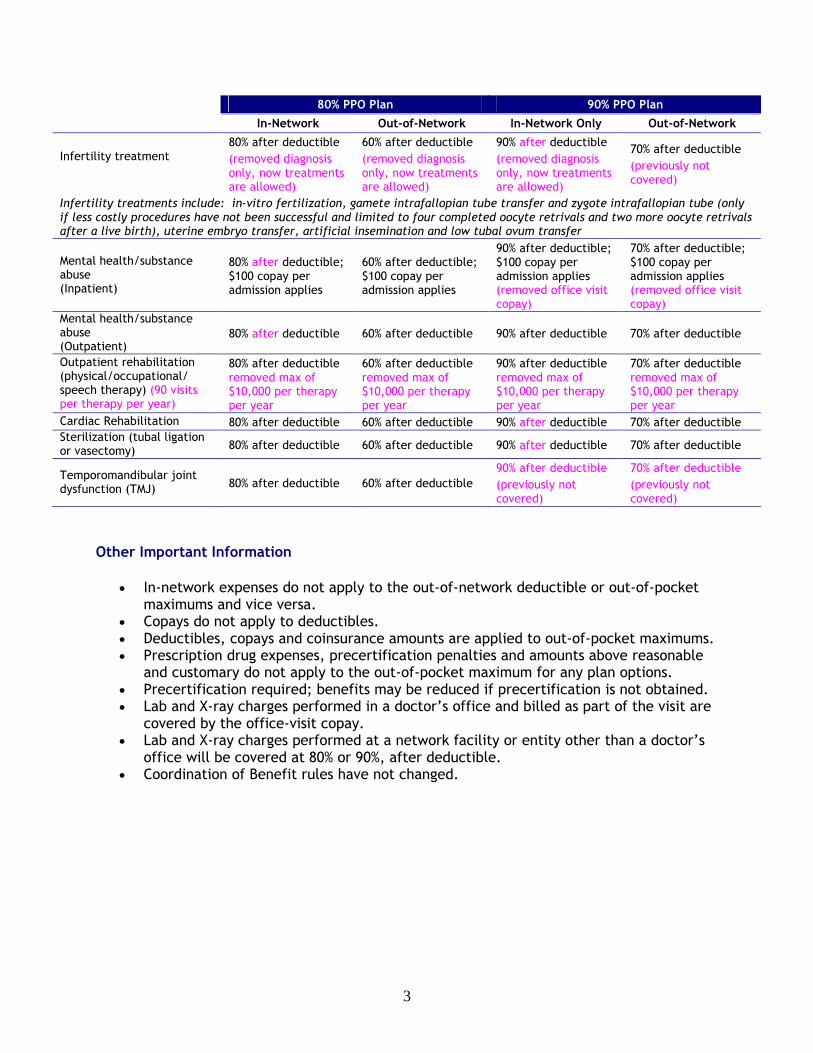
Infertility treatment80% after deductible
(removed diagnosisonly, now treatmentsare allowed)
60% after deductible
(removed diagnosisonly, now treatmentsare allowed)
90% after deductible
(removed diagnosisonly, now treatmentsare allowed)
70% after deductible
(previously notcovered)
Infertility treatments include: in-vitro fertilization, gamete intrafallopian tube transfer and zygote intrafallopian tube (onlyif less costly procedures have not been successful and limited to four completed oocyte retrivals and two more oocyte retrivalsafter a live birth), uterine embryo transfer, artificial insemination and low tubal ovum transfer
Mental health/substanceabuse(Inpatient)
80% after deductible;$100 copay peradmission applies
60% after deductible;$100 copay peradmission applies
90% after deductible;$100 copay peradmission applies(removed office visitcopay)
70% after deductible;$100 copay peradmission applies(removed office visitcopay)
Mental health/substanceabuse(Outpatient)
80% after deductible 60% after deductible 90% after deductible 70% after deductible
Outpatient rehabilitation(physical/occupational/speech therapy) (90 visitsper therapy per year)
80% after deductibleremoved max of$10,000 per therapyper year
60% after deductibleremoved max of$10,000 per therapyper year
90% after deductibleremoved max of$10,000 per therapyper year
70% after deductibleremoved max of$10,000 per therapyper year
Cardiac Rehabilitation 80% after deductible 60% after deductible 90% after deductible 70% after deductibleSterilization (tubal ligationor vasectomy) 80% after deductible 60% after deductible 90% after deductible 70% after deductible
Temporomandibular jointdysfunction (TMJ) 80% after deductible 60% after deductible
90% after deductible
(previously notcovered)
70% after deductible
(previously notcovered)
Other Important Information
In-network expenses do not apply to the out-of-network deductible or out-of-pocketmaximums and vice versa.
Copays do not apply to deductibles. Deductibles, copays and coinsurance amounts are applied to out-of-pocket maximums. Prescription drug expenses, precertification penalties and amounts above reasonable
and customary do not apply to the out-of-pocket maximum for any plan options. Precertification required; benefits may be reduced if precertification is not obtained. Lab and X-ray charges performed in a doctor’s office and billed as part of the visit are
covered by the office-visit copay. Lab and X-ray charges performed at a network facility or entity other than a doctor’s
office will be covered at 80% or 90%, after deductible. Coordination of Benefit rules have not changed.

4
Expenses Covered:
Speech therapy rendered for the treatment of psychological speech delay, behavioral problems, attention disorder,conceptual handicap or mental retardation.Hospital Admission in whole or in part when the patient primarily receives services to rehabilitate such as physicaltherapy, speech therapy or occupational therapy.Services and expenses provided to a hospital patient which could have been provided on an outpatient basis, giventhe patient's condition and the services provided. Benefits for these services will apply as though the services wereprovided on an outpatient basis. Examples are hospital stays primarily for diagnosis, diagnostic study, medicalobservation, rehabilitation, physical therapy and hydrotherapy.Services for or related to pregnancy, including the six week period after delivery, for any dependent children.Services or expenses for treatment of any condition including, but not limited to, obesity, diabetes, or heartdisease, which is based upon weight reduction or dietary control or services or expenses of any kind to treatobesity if medically necessary and in compliance with guidelines of the Claims Administrator. Benefits will only beprovided for one surgical procedure for obesity (morbid) in a lifetime.
Expenses Not Covered:
General
Services and supplies which are not medically necessary, as determined by BCBS
Services and supplies that do not meet accepted standards of medical/dental practice
Services and supplies which benefits are available under Workers Compensation Law
Services and supplies which are provided by or for which benefits are available from the government
Services and supplies for any illness or injury that occurs after the coverage date and is a result of war
Services or supplies not specifically mentioned in the benefit booklet
Services or supplies for which one would not have to pay in the absence of this coverage
Services or expenses for which a claim is not properly submitted to BlueCrossBlueShield
Services and supplies that are investigational
Diagnostic testing that is part of a survey or research study or that is investigational
Services or expenses for treatment of injury sustained in the commission of a crime or for treatment while confinedin a prison, jail or other penal institutionServices and supplies to the extent benefits are duplicated because more than one family member is a member ofthe group and covered separately
Reports, evaluation, examinations or hospitalizations not required for health reasons
Charges for failure to keep a visit or for completion of a claim form
Telephone consultations
Diet/Nutrition RelatedServices of a dietitian, foods required for special diets or nutritional supplements that do not require a prescription(except as an inpatient hospital expense)
Blood or Organ Related
Fees for directed blood donations i.e. when someone designates donation of blood to a specific person
Blood derivatives that are not officially classified as drugs
Blood and administration of blood and blood products when it is for the sole purpose of enhancing one's physicalstatus or when related to sports activities
Services and supplies for Human Organ Transplants other than those specifically mentioned in the benefit booklet
Foot Related
Treatment of flat feet and sublaxations of the foot

5
Routine foot care (except for persons diagnosed with diabetes)
Orthotics that are store-bought (not custom made)
Vision, Hearing and Dental RelatedEye glasses, contact lenses and cataract lenses and the examination for prescribing or fitting them or fordetermining the refractive state of the eye
Surgical correction of refractive errors, such as a radial keratotomy or LASIK surgery
Orthopic or visual training or visual therapy
Hearing aids or the examination for prescribing or fitting hearing aids
Most dental services (including anesthia), unless required to correct a condition caused by an injury that occurredwithin the last year (one-year limitation waived for a dependent child) or due to a concurrent hazardous medicalcondition that requires that oral surgery be done in a hospital/outpatient surgical facility (covered expenseslimited to facility fees).Services or expenses to cause for, treat, extract, remove or replace teeth or to increase the periodontium. Theperiodontium includes the gums, the membrane surrounding the root of a tooth and the upper and lower jaws andtheir borders, which contain the sockets for the teeth. Care to treat the periodontium, dental pulp or dead teeth,irregularities in the position of the teeth, artificial dental structures such as crowns, bridges or dentures, or anyother type of dental procedure is excluded. Hydroxyapatite or any other material to make the gums rigid isexcluded. It does not matter whether their purpose is to improve conditions inside or outside the mouth (oralcavity). These services, supplies or expenses are not covered even if they are used to prepare a patient forservices or procedures that plan benefits. Braces on the teeth are excluded for any purpose, even to prepare aperson with a cleft palate for surgery on the bones of the jaw. With the exception of braces, which are nevercovered under the medical plan, this exclusion does not apply to those services by a physician to treat or replacenatural teeth which are harmed by accidental injury covered under Other Covered Services.Dental implants into, across, or just above the bone and related appliances. Services or expenses to prepare themouth for dental implants such as those to increase the upper and lower jaws or their borders, sinus lift process,guided tissue or any other surgery, bone graft, hydroxyapatite and similar materials. These services, supplies orexpenses, even if medically or dentally necessary, are not covered under the medical plan even if they are neededto treat conditions existing at birth, while growing, or resulting from an accident.
Custodial Related
Respite care service, except as specifically mentioned under the Hospice Care Program
Long term care service
Inpatient private duty nursing service
Maintenance care
Custodial care service
Services received (including room and board) for custodial care that is given primarily to help a person withpersonal hygiene or to perform activities of daily living and that by generally accepted medical standards, can beadequately provided by someone other than a licensed medical professional or nurse, regardless of whorecommends, provides or directs the care.
Other Facilities and Practitioners Related
Treatment of mental disorders, custodial care, and other treatment in an institution that is not legally constituteda hospital, except as covered under the planServices provided by persons without nationally recognized licensure or which do not fall within the scope of thelicense.
Services rendered by a family member
Services or expenses any provider rendered to a member who is related to the provider by blood or marriage orwho regularly resides in the provider's household. Examples of a provider include a physician, a licensed registerednurse, a licensed practical nurse, or a licensed physical therapist.
Care provided by Christian Science Sanitariums and Practitioners
Prosthetics/Special Equipment Related
Prosthetic devices, special appliances and surgical implants which are for cosmetic purposes, the comfort andconvenience of the patient or unrelated to the treatment of an illness or injury
Any biochemical external prosthetic devise or replacement of external prosthetics due to loss theft or destruction.

6
Specialized equipment, special braces, splints, appliances, etc., except as specifically mentioned in the SPD
Amniocentesis, ultrasound or any other procedure requested solely to determine the gender of the fetus, unlessmedically necessary to determine the existence of a gender-linked genetic disorder
Mental Health/Self Help Related
Services or expenses for acupuncture, biofeedback and other forms of self-care or self-help training.Mental Health expenses related to: biofeedback, chronic pain treatment without a DSM-IV diagnosis, court-orderedmental health treatment, unless otherwise covered, financial counseling, light boxes, marriage and familycounseling, mental retardation, methadone maintenance, self-help programs, treatment of learning disabilities,treatment of nicotine addictions and treatment of sexual dysfunction not related to organic disease.Services and supplies received on an inpatient basis as the result of antisocial actions which are not the result ofmental illnessThose for or related to the following types of treatment: primal therapy, Rolfing, psychodrama, megavitamintherapy, bioenergetics therapy, vision perception training or carbon dioxide therapyServices for education or special education or job training whether or not given in a facility that also providesmedical psychiatric treatmentThose for treatment by covered health care providers who specialize in mental health care field and who receivetreatment as a part of their training in that field
Therapy Related
Maintenance Physical therapy, Maintenance Occupational therapy and Maintenance Speech therapy
Speech therapy that is custodial or educational or is not restorative in nature.
Speech therapy to maintain speech communication.
Services or expenses for speech, recreational, educational, or occupational therapy (except as stated previously)
Work hardening therapy or programsTesting or training for education purposes, including services associated with developmental delay or learningdisabilities
Travel/Transportation Related
Transportation services other than ambulance services to the nearest hospital where the needed medical care andtreatment can be provided
Travel, even if prescribed by your physician.
Life Style RelatedExpenses for in vitro fertilization, artificial insemination or other impregnation procedures for reversal ofsterilization.Services or expenses for or related to sexual dysfunctions or inadequacies not related to organic disease or whichare related to surgical sex transformations.Services for performance, athletic performance or lifestyle enhancement drugs or supplies, except to the extentcoverage for such drugs and supplies is specifically provided in the certificate bookletGender reassignmentPersonal hygiene or comfort or convenience items (air conditioner, physical fitness equipment, etc.)Cosmetic surgery except for the correction of congenital deformities or resulting from accidental injuries, scars,tumors or disease

7
Prescription Drugs
80% & 90% PPO Plans
Copay/Co-insuranceRetail(30 day supply)
Mail Service(90 day supply)
Generic $10 copay $20 copay
Brand name (Formulary) 20%; maximum of $30 per RX 15%; maximum of $60 per RX
Brand name (Non-Formulary)
30%; maximum of $60 per RX 25%; maximum of $100 per RX
Out-of-Network benefits are paid at the same level as In-Network Benefits.
Plan ChangesAll plans will experience a change to the brand name tiers wherein coinsurance has beenincorporated into the plan design. There is no deductible and you do not have to pay thedifference between brand and generic when a generic is available. (This was a former PPOChoice provision.) Also, three new programs will be added:
Prior AuthorizationUnder this part of the program, your physician will be required to obtain authorizationthrough Blue Cross Blue Shield of Illinois in order for you to receive benefits for certainmedications and drug categories.
Examples of drug categories and specific medications for which prior authorizationmay be needed are listed below. Please see the BCBS website for a complete list.
Drug categories may be added and the medications listed are only examples. Call thePharmacy Program number on the back of your ID card with questions about a specificmedication.
As always, cost is only one factor in choosing medication and treatment decisions arebetween you and your doctor.
Prior Authorization Category Prescription Drugs within the Category*Acne SolodynAndrogens/Anabolic Steroids Anadrol-50, Androderm, Androgel, Android, Androxy, danazol,
First-Testosterone, Methitest, Oxandrin, Striant, Testim,Testred
Antifungal Agents Lamisil, Noxafil, Penlac, Sporanox, VfendAttention Deficit HyperactivityDisorder (adults)
Adderall, Adderall XR, Concerta, Daytrana, Desoxyn, Dexedrine,Dextrostat, Focalin, Focalin XR, Intuniv, Liquadd, Methylin,Metadate CD, Metadate ER, Ritalin, Ritalin LA, Ritalin SR,Strattera, Vyvanse
Enzyme Deficiencies KuvanErectile Dysfunction Agents Caverject, Cialis, Edex, Levitra, Muse, ViagraGrowth Hormones Genotropin, Humatrope, Norditropin, Nutropin, Nutropin AQ,
Omnitrope, Saizen, Serostim, Tev-Tropin, ZorbtiveHepatitis C Infergen, Pegasys, PegIntronNarcolepsy Nuvigil, Provigil, XyremOral Fentanyl Actiq, Fentora, OnsolisRetinoids Atralin, Avita, Retin-A, Retin-A Micro, Tretin-X, Tazorac, Ziana
* Third-party brand names are the property of their respective owners.

8
Step TherapyThe Step Therapy program is designed to encourage the initial use of alternative medicationsgenerally recognized as safe and effective, which are also lower-cost. Under this program, inorder to receive coverage the member may need to first try a proven, cost-effectivemedication before progressing to a more costly treatment, if necessary. After the memberhas a prescription history for a lower-cost alternative medication, coverage will automaticallybe provided for a more costly medication included in the program. Employees that alreadyhave maintenance prescriptions will not be required to change medication. This only appliesto new employees or employees being prescribed medications for the first time where nohistory is available. (See the BCBS website for more information regarding this program.)
Specialty MedicationsSpecialty medications include those used in the treatment of complex medical conditions,such as hepatitis, hemophilia, multiple sclerosis, rheumatoid arthritis and other conditionsrequiring self-administered specialty medications. (See the BCBS website for a completelisting of specialty medications.) Any participant that has a specialty medication prescriptionmust order it through a separate vendor, Triessent. Through Triessent, you can have yourcovered specialty medication delivered directly to you, if it is a self-administered drug, or toyour doctor’s office. Since many specialty medications have unique shipping or handlingrequirements, all shipments are arranged with you through Triessent. Medications areshipped in plain, secure, tamper-resistant packaging.
When you purchase specialty medications through Triessent, you also receive at no additionalcharge the following services:
Coordination of coverage between you, your doctor and BCBS of Illinois Educational materials about your particular condition and information about managing
potential medication side effects Syringes, sharps containers and other supplies with every shipment for self-injectables 24/7/365 phone access to a pharmacist for urgent medication issues.
To order through Triessent:
Have your doctor call (888) 216-6710 or fax to (866) 203-6010. A Triessent coordinator will contact you to arrange delivery of your medication.
Patient Protection Affordable Care Act (PPACA)Health care reform required all medical plans to review and, where necessary, makeadjustments to plan design. The items from PPACA that most impacted our plans are: theelimination of lifetime maximums; increasing eligible child age to 26; broadening coverage foreligible dependents to include adult children; and requiring preventative care services (suchas annual physicals) to be offered at 100%. The medical plan comparison chart has beenupdated with the new provisions and is intended to be a summary of what preventativeservices are covered under the Plan. Once the Summary Plan Description is available, detailsof these plan provisions will be provided.

9
Employee EligibilityAll employees scheduled to work 20 hours or more per week will be eligible to participate inthe INEOS Health and Welfare benefits.
Dependent EligibilityUnder PPACA, a group health plan that offers dependent coverage must continue suchcoverage for an employee's adult child until the child turns 26 years old. The definition of an“eligible child” under our Plans include:
Your natural or adopted child (including a child placed for adoption); A child for whom you have legal guardianship; A child of your spouse or domestic partner; Your foster child who is a child placed with you by an authorized placement agency or
by judgment, decree, or other order of a court of competent jurisdiction; A child who is covered by the health care plans and is totally and permanently
disabled at the time he/she turns 26 can continue coverage if approved by BCBS.
“Eligible child” does not include:
Grandchildren of you and/or your spouse/domestic partner;
A child related to you by blood or marriage who does not meet the above eligible childdefinition (such as a niece, nephew)
WellnessThe deadline for the Wellness Program has been changed from September 30, 2010 toDecember 31, 2010. If you wish to participate, you now have until the end of the year withinwhich to complete the three criteria: (1) routine annual physical (2) age- and gender-appropriate blood screen, including lipid panel and blood glucose (3) online health riskassessment (HRA) at www.bcbsil.com. For future plan years, the deadline will continue to beDecember 31.
After January 1, 2011, the BCBS website (BAM) will reflect your credits accrued to date forthe plan year, in addition to any credits you accrue for the following plan year. As youcomplete each task during the year, BCBS will automatically update your Health CareAccount. Keep in mind that credits accrued during the plan year will not be available untilthe following year. However, you will be able to easily track your participation throughoutthe year, making sure you receive credit when you complete each task.
Opt-Out CreditThe medical plan “Opt-Out” provision has been extended to all employees. If you decide notto enroll in one of the INEOS Medical Plans, you will receive $100/month ($1,200/year). Thisamount will be paid to you over the course of the year through your normal payroll as long asyou are employed and not electing medical coverage. Opt-Out credits are taxable incomeand will be reported on your W2.

10
DentalThe dental plan comparison chart details all plan provisions under the Humana Dental DPOPlan. It includes a section of “Expenses Covered” and “Expenses Not Covered”.
General Information Humana Dental DPO Plan
Deductible In-Network Out-Of-Network
Individual $25 $25
Individual + One $50 $50
Family $75 $75
Plan Year Maximum $1,500 per person $1,500 per person
Lifetime Maximum Unlimited Unlimited
Orthodontia Maximum$1,750 per person (Paid at 50%, nodeductible for adults and children)
$1,750 per person (Paid at 50%, nodeductible for adults and children)
The following services will be covered in and out of network for the category indicated:Diagnostic and Preventative 100%, no deductible
Covered Services Include: Oral Exams – 2 times in one
calendar year Sealants – 1 per tooth per lifetime
Full Mouth X-rays or Panorex X-ray– 1 time within 36 months
Space Maintainer
Bitewing X-ray – 2 times in onecalendar year
Palliative (emergency) Treatment
Prophylaxis/Cleaning – 2 times inone calendar year
Oral Cancer Screening – over theage of 40
Fluoride – 1 time in one calendaryear (no age limit)
Pulp vitality testing andbacteriological studies fordetermination of bacteriologicagents
Basic Restoration 85% after deductible
Covered Services Include: Fillings (includes composite fillings
on anterior and bicuspids) Apexification/recalcification
Periodontal surgery, once perquadrant every 3 calendar years
Tissue Conditioning
Periodontal Scaling/Root Planning– 1 time per quadrant within 3years
Occlusal Adjustments (1 perquadrant every 3 years)
Periodontal Maintenance (2 timesper year)
Full mouth debridement’s, but notmore than once per lifetime
Pulp Capping (excluding finalrestoration)
Therapeutic pulpotomy (excludingfinal restoration)
Fixed and removable appliancesfor correction of harmful habits(no age limits)
Recementation of inlays/onlays,veneers, crowns and bridges
Appliances for treatment forbruxism (grinding teeth), includingbut not limited to occlusal guardsand night guards (reline and repairnot covered)
Application of desensitizing medicationswhere periodontal treatment (includingscaling, root planning, and periodontalsurgery, such as osseous surgery) hasbeen performed

11
Basic Restoration (cont.) 85% after deductible
Oral surgery Local chemotherapeutic agents(Site Therapy)
Administration of generalanesthesia when medicallynecessary, in conjunction withcovered oral surgical procedures
Drug injections done in conjunctionwith oral surgery
Stainless steel crowns Injections of therapeutic drugs,except oral surgery
Consultations Endodontics (root canals)
Extractions
Major Restoration 50% after deductible
Covered Services Include: Non-surgical treatment of TMJdisorders.
Labial veneers, but no more thanonce per tooth in a period of 60months
Core Buildup Repair of Implants
Cone beam imaging Diagnostic casts
Prosthodontic Posts and cores
Inlays and onlays, 1 time per 5years
Crowns, 1 time per 5 years
Implant services (including sinusaugmentation and bonereplacement and graft for ridgepreservation)
Crown repair
Removable or fixed bridgework Bridge, 1 time per 5 years
Complete Denture, 1 time per 5years
Partial denture, 1 time per 5 years
Relinings and rebasings of existingremovable dentures; if at least 6months have passed since theinstallation of the existingremovable denture
Partial or complete denturerepairs/adjustments
Addition of teeth to a partialremovable denture
Coverage Type Reasonable & Customary
Coordination of Benefits Birthday Rule, non-duplication of benefit applies

12
Expenses Not Covered:
General
Services which are not Dentally Necessary, those which do not meet generally accepted standards of care fortreating the particular dental condition, or which this Plan deems experimental in nature
Services not dentally necessary or services which do not have uniform professional endorsementServices covered under any workers' compensation or occupational disease law, covered under any employerliability law; for which the Employer of the person receiving such services is not required to pay; or received at afacility maintained by the Employer, labor union, mutual benefit association, or VA hospitalServices and supplies for which no charge is made, or for which you would not be required to pay if you did nothave coverage unless charges are received from and reimbursable to the United States Government or any of itsagencies as required by lawAny covered expense to the extent of any amount received from others for the accidental injuries or losses whichnecessitate such benefits. "Amounts received from others" specifically includes, without limitation, liabilityinsurance, workers' compensation, uninsured motorists, underinsured motorists, "no-fault" and automobile med-paypayments.Any accidental injury arising from or sustained in the course of any occupation or employment for compensation,profit or gain for which benefits are provided or payable under Worker's Comp or Occupational Disease Act or Law;coverage was available under any Worker's Comp or Occupational Disease Act or Law regardless of whether suchcoverage was actually purchasedServices and supplies furnished by or payable under any plan or law through any government or any politicalsubdivision. This does not include Medicare or Medicaid.
Services covered by a medical or Medicare planServices and supplies furnished for a military service connected accidental injury by or under an agreement with adepartment or agency of the United States Government, including the Department of Veterans Affairs
Any loss caused by or contributed to war or any act of war, whether declared or notAny loss caused by or contributed to any act of international armed conflict, or any conflict involving armed forcesor any international authority
Services for which you would not be required to pay in the absence of dental benefits
Services or supplies received by you or your dependent before the Dental Benefits start for that person
Services covered under other coverage provided by the Employer
Failure to keep an appointment with the dentist
Any service not specifically listed as a covered expenseThe extent the expense exceeds the maximum allowable fee or predetermined charge for the service, treatment orsupply in the locality where furnished
Any expense incurred prior to your enrollment in the Plan or after the date your coverage terminatesServices which neither performed nor prescribed by a Dentist, except for those services of a licensed dentalhygienist which are supervised and billed by a Dentist, and are for: scaling, teeth polishing or fluoride treatments
Services for which the submitted documentation indicates a poor prognosisFees for treatment by other than a dentist, except that scaling or cleaning of teeth and topical application offluoride may be performed by a licensed dental hygienist. The treatment must be rendered under the supervisionand guidance of the dentist in accordance with generally accepted dental standardsDental services arising out of accidental injury to the teeth and supporting structures, except for injuries to theteeth due to chewing or biting of foodThe following, when charged by the Dentist on a separate basis: claim form completion, infection control, such asgloves, masks, and sterilization of supplies or local anesthesia, non
Appliance Related
Temporary or provisional appliances
Restorations or appliances used for the purpose of periodontal splinting
Duplicate prosthetic devices or appliances
Replacement of a lost or stolen appliance, cast restoration or denture
Services or appliances which restore or alter occlusion or vertical dimension

13
Repair or replacement of an orthodontic device
Replacement of lost, broken or stolen appliances or duplicate appliances
Reline/repair of occlusal guards
Athletic mouth guards
StressbreakersAppliances and restorations for increasing vertical dimension, restoring occlusion, or replacing tooth structure lostby attrition, abrasion, or erosion
Denture Related
Initial installation of a denture to replace one or more teeth which were missing before such person was coveredfor dental benefits
Adjustment of a denture made within 6 months after installation by the same dentist who installed it
Temporary or provisional restorations
Prescription Drug/Anesthesia Related
Prescription drugs or pre-medications
Any hospital charges for services of any anesthesiologistGeneral anesthesia unless administered by a dentist in connection with oral and dental surgery and when dentallynecessary or necessary due to a medical condition that presents a high risk to the patient. This also excludesgeneral anesthesia administered in connection with routine extractions and the surgical removal of erupted teeth.
Maintenance and Repair Related
Overdentures and their maintenance/repairs
Gold crowns and their maintenance/repairs.
Gold fillings and their maintenance/repairs
Veneers and their maintenance/repairs on molar and bicuspid teeth
Miscellaneous Related
Biopsies of hard or soft oral tissue
Caries susceptibility testing, lab tests, anaerobic cultures, sensitivity testingAny splinting procedure, including but not limited to, multiple abutments or any service to stabilize periodontallyweakened teeth
Major restorative and Prosthodontic Services on other than permanent teeth
Restoration of tooth structure damaged by attrition, abrasion or erosion, unless caused by disease
Precision attachments associated with fixed and removable prostheses
Precision or semi-precision attachments
Intra and extraoral photographic images
Sterilization/infection control fees
Cosmetic/Life Style Related
Decoration or inscription of any tooth, device, appliance, crown or other dental workAny service which is considered cosmetic unless such service is necessary as a result of an accidental injury.Cosmetic dentistry includes: porcelain on crowns, abutments or pontics on molar teeth, personalization orcharacterization of prosthetic devices, composite restorations on molar teeth, and replacement of congenitallymissing teeth.
Counseling or instruction about oral hygiene, plaque control, nutrition and tobacco
Personal supplies or devices including but not limited to: water piks, toothbrushes, or dental floss
Preventive control programs including but not limited to, oral hygiene instruction, plaque control, take home itemson dietary planning

14
Other Important Information In-network expenses do not apply to the out-of-network deductible or out-of-pocket
maximums and vice versa. Remember, when changing vendors, we are always concerned with network access.
We want employees to have the best access regardless of location. To eliminateworries about providers not being in the Humana network, we designed the plan tocover out-of-network services at the same level as in-network. Although we stronglyencourage employees to use network providers due to the negotiated discounts (youwill pay less if you use a network provider), you have the choice to use any provideryou want and still have it covered under the dental plan. You may, however, end upusing your benefit quicker if Humana does not have negotiated discounts with them.
Employee EligibilityAll employees scheduled to work 20 hours or more per week will be eligible to participate inthe INEOS Health and Welfare benefits.
Dependent EligibilityUnder PPACA, a group health plan that offers dependent coverage must continue suchcoverage for an employee's adult child until the child turns 26 years old. Although PPACAdoes not impact dental plans, dependent eligibility under the dental plan will be changed toreflect the same as the medical plan definition. The definition of an “eligible child” underour Plans will include:
Your natural or adopted child (including a child placed for adoption); A child for whom you have legal guardianship; A child of your spouse or domestic partner; Your foster child who is a child placed with you by an authorized placement agency or
by judgment, decree, or other order of a court of competent jurisdiction; A child who is covered by the health care plans and is totally and permanently
disabled at the time he/she turns 26 can continue coverage if approved by BCBS.
Eligible child does not include:
Grandchildren of you and/or your spouse/domestic partner;
A child related to you by blood or marriage which does not meet the above eligiblechild definition (such as a niece, nephew)
Opt-Out CreditThe dental plan “Opt-Out” provision has been extended to all employees. If you decide notto enroll in the INEOS Dental Plan, you will receive $100/year ($8.33/month). This amountwill be paid to you over the course of the year through your normal payroll as long as you’reemployed and not electing dental coverage. Opt-Out credits are taxable income and will bereported on your W2.

15
Vision
Plan Design Summary ChartThe vision plan summary chart details plan provisions under the VSP Choice Plan.
Provisions Choice Vision Plan
Exam $10 copay, then 100% covered once every 12 months
Lenses $25 copay, then 100% covered once every 12 months
Frames $25 copay, then 100% covered once every 24 months
VSP Participating Provider
Frame Allowance $130Contact Lenses instead of Glasses 15% discount off the contact lens exam. Plus a $130.00
allowance for your contact lens exam and contacts.
Covered Lens Option: Polycarbonate lenses (dependent children) & Anti-reflective Coating
Additional Coverage: Diabetic Eye Care Program
$20 copay
Non-Participating Provider
Examination $45
Single Vision Lenses $30
Lined Bifocal Lenses $50
Lined Trifocal Lenses $65
Frame $70
Elective Contact Lens Allowance(Covers contact lenses and associatedprofessional services.)
$105
Plan Changes:For Heritage employees, you will see the addition of a new program—Diabetic Eye Care. TheDiabetic Eyecare Program enhances a Type 1 diabetic member’s routine vision coverage byoffering additional services that play an important role in the prevention, early detection,and management of related eye diseases, such as diabetic retinopathy. Early detection ofdiabetic retinopathy allows for more aggressive and effective treatment, reducing thechances of vision impairment or blindness.
For USA employees, you will notice a decrease in the Lens co-pay and higher reimbursementamounts for using Non-Participating providers. The network under the VSP Choice Plan isnearly the same as the former USA VSP Plan. Check the VSP website for participatingproviders.
Employee EligibilityAll employees scheduled to work 20 hours or more per week will be eligible to participate inthe INEOS Health and Welfare benefits.
Dependent EligibilityDependent eligibility will be changed to reflect the same as the medical and dental plandefinitions.

16
Flexible Spending Accounts
This year you will see changes in your Health Care Flexible Spending Accounts (FSAs) due toPPACA. The changes include the elimination of Over-The-Counter (OTC) items effectiveJanuary 1, 2011. The items in the list below will only be covered in the event that theemployee has a prescription for the item, but chooses to purchase the OTC product instead ofhaving the pharmacy fill the prescription. The member will no longer be able to use theirdebit card with the purchase of these types of products and services. In order for the OTCitems to be reimbursed under the FSA plan, the prescription and receipt will have to besubmitted to MedCom for reimbursement. This applies to expenses incurred January 1, 2011and later. These items will not be eligible for the FSA grace period.
Acid Controllers Allergy & Sinus Antibiotic Products Anti-Diarrheal Products Anti-Gas Anti-itch & Insect Bite Baby Rash Ointments/Creams Cold Sore Remedies Cough, Cold & Flu Medicines
Digestive Aids Feminine Anti-Fungal/Anti-Itch Hemorrhoidal Preps Laxatives Motion Sickness Pain Relievers Respiratory Treatments Sleep Aids & Sedatives Stomach Remedies
Items that will continue to be covered under FSA plans are items such as medical equipment(crutches, eyeglasses, contacts ect.), supplies (bandages, saline solution, etc.), anddiagnostic devices (blood sugar test kits, pregnancy tests, ect.). Some examples of theseitems are below:
Band Aids Birth Control Braces & Supports Contact Lens Supplies & Solutions Catheters Denture Adhesives Diagnostic Tests & Monitors
Elastic Bandages & Wraps First Aid Supplies Insulin & Diabetic Supplies Ostomy Products Reading Glasses Walkers & Canes Wheelchairs
The maximum amount you can contribute to the Health Care and Dependent Care FSAs willremain unchanged.
Dependent EligibilityFor the Health Care Spending Account (HCSA), “eligible dependents” include the samedependents as covered under the Medical Plan.

17
Long-Term Disability
This year INEOS had the opportunity to consolidate our Long-Term Disability (LTD)program with CIGNA. In prior years INEOS USA and INEOS Heritage employees haddifferent benefit levels. For 2011, the company provided LTD benefit will be 60% ofemployee’s monthly covered earnings, with a maximum monthly benefit of $15,000. Abuy-up option of up to 65% of your monthly covered earnings is available on a voluntarybasis, which is paid 100% by the employee.
If you wish to supplement the company-provided core benefit and purchase LTD buy-upinsurance, this can be done through Ceridian Self-Service during the Open Enrollmentwindow. You will be given a one-time opportunity to enroll without having to completean Evidence of Insurability (EOI) Form. However, in lieu of EOI, there will be a 12 monthpre-existing condition requirement prior to receiving any LTD benefits under the buy-upoption. If you decide to elect buy-up coverage at a future date outside of the openenrollment window, you will be required to complete an Evidence of Insurability (EOI)Form
If you are already enrolled in the LTD 65% Buy-Up option, your current election willremain in place and nothing further is required. If you have an election for a 60% buy-upoption, this election will expire at 12/31/2010 and a new election will be required for the65% buy-up option.
The new rates for the LTD Buy-Up plan are (per $100 of covered earnings):
Age Band Buy-Up RatesUnder 39 $0.08440-44 $0.12645-49 $0.18550-54 $0.21055-59 $0.16560-64 $0.12665-69 + $0.088
An example of how to calculate the LTD Buy-Up premium is below. Using assumptions ofan employee that is 52 years old and making $50,000 annually in base salary.
1. Calculate your monthly earnings (based on your annual salary):
Annual Salary = $50,000 / 12 = $4,166.67
2. Calculate the monthly covered earnings per $100 of coverage:
Covered Monthly Earnings = $4,166.67 / 100 = $41.67
3. Multiply this amount by the applicable Buy-Up Rate
Monthly Buy-Up Premium = $41.67 x $0.210 = $8.75

18
Please note, Ceridian Self-Service will reflect the annual “coverage” amount, which is 60%of your annual earnings. It does not display your annual earnings. You will also see thecorresponding payroll deduction, based on your payroll frequency.
Premiums will be deducted from your check on an after-tax basis for the additional 5% ofthe benefit. Since you will be paying for the buy-up coverage with after-tax money, thisamount will not be considered taxable income if you were to become disabled and startreceiving the benefit. The company provided benefit, however, would be taxable incomeat that time.
For INEOS Heritage employees, the Company premium paid was taxable to you as“imputed income”. Going forward into 2011, this benefit will no longer be taxable to you.

19
Benefits Website
Check out the INEOS Benefits Website at www.ineosbenefits.com for more informationregarding all benefit plans and for plan specific certificate booklets.
Since the website contains company-confidential information, you will need to register underyour INEOS email address to use the site.
Registration is an easy 2-step process:
1. After clicking on the "Register" link under the Login button on the website you willneed to complete a registration form that will be submitted to the BenefitsDepartment for authorization. You will receive 2 emails, one thanking you forregistering and another once your registration has been approved.
2. The second email will contain a link for you to set your personal access code(password). You will then be able to use the website from any computer connected tothe internet.
