induction of labor - a clinical case discussion
TRANSCRIPT
CASEA 24 year old Puan Nina was admitted to hospital on 8th August at 8.50 am for the induction of labour for post maturity, her pregnancy gestation is 40 weeks and 1 day.
Previous Obstetric history: Gravid 3, Para 2, two previous normal deliveries. No history of any medical problems and no problems identified in this pregnancy.
At 8.50am admitted to the Labour ward, no signs of labour on admission and the findings from the vaginal examination were that the cervix was 2 cm dilated. Decision was made to do an ARM (artificial rupture of membranes) and to commence Syntocinon.
CASEThe woman progressed well in labour and had a normal delivery of a female infant at 1.19pm, The infant's weight was 3.5kg, Apgar scores were 9 at 1 & 5 minutes.

INDUCTION OF
LABOR
CLINICAL CASE DISCUSIÓN
BY AFIQI
DEFINITIONSInduction of Labor (IOL) is defined as artificial initiation of uterine contractions before the spontaneous onset of labor.
Augmentation of labor refers to stimulation of spontaneous contractions that are considered inadequate because of failed cervical dilation and fetal descent.
INDICATIONFOR INDUCTION
11
1. pre-eclampsia, eclampsia, chronic hypertension > 37wks
2. Diabetes, renal disease, chronic pulmonary disease
3. Premature rupture of membranes
4. Chorioamnionitis
5. Fetal growth restriction
6. Rh isoimmunization
7. Postdated pregnancy
8. Fetal demise
9. Abruptio placentae
10.Fetal malformations incompatible with life
11.Logistic factors: Risk of rapid labor, distance from hospital, psychosocial indications
CONTRAINDICATIONOF INDUCTION
11
1. Placenta praevia or Vasa praevia
2. Cord presentation
3. Abnormal fetal lie/ presentation
4. Cephalopelvic disproportion because of malpresentation or abnormal pelvic bone structure
5. Active genital Herpes infection
6. Invasive cervical carcinoma
7. Hypersensitivity to cervical ripening agents
8. Previous uterine rupture

CONTRAINDICATIONOF INDUCTION
11
1. Multiple pregnancy
2. Polyhydramnios
3. Grand multiparity
4. Maternal heart disease.
5. Severe hypertension.
6. Breech presentation
7. One or more previous cesarean section
8. Abnormal fetal heart rate not requiring emergency cesarean section
CONDITIONS WHERE IOL IS NOT A TRUE CONTRAINDICATION BUT WHERE SPECIAL CAUTION IS REQUIRED :
1
RISK OF IOLMATERNAL RISKS
I. Failure leading to Cesarean section II. Uterine hyperstimulation III. Rupture uterus IV. Intrauterine infection, Chorioamnionitis V. Amniotic Fluid Embolism VI. Precipitate labor , Dysfunctional labor VII.Increased risk of operative vaginal delivery VIII.Increased risk of post partum hemorrhage IX. Abruptio Placentae X. APH from undiagnosed placenta praevia XI. Water intoxication

1
RISK OF IOLFETAL RISKS
I. Fetal distress . II. Fetal death III. Neonatal sepsis IV. Iatrogenic delivery of a preterm infant V. Cord prolapse VI. Neonatal jaundice VII.Increased risk of birth trauma

PRE- REQUISITES FOR IOLI. Evaluate the indication II. Explain the indication to the patient + details of the method to
be used and take a written informed consent III. Assess adequacy of the pelvis and fetal size IV. Confirm the gestational age, fetal lie, and assess the fetal lung
maturity # where ever indicated V. Uterine activity and FHR should be continuously monitored. In
case of clinical auscultation, FHR should be heard during and for 30 seconds after a contraction at least every 15 minutes during the active phase of labor and after every contraction in the second stage
VI. Partogram is to be maintained for active labour VII.Trained personnel and well equipped center

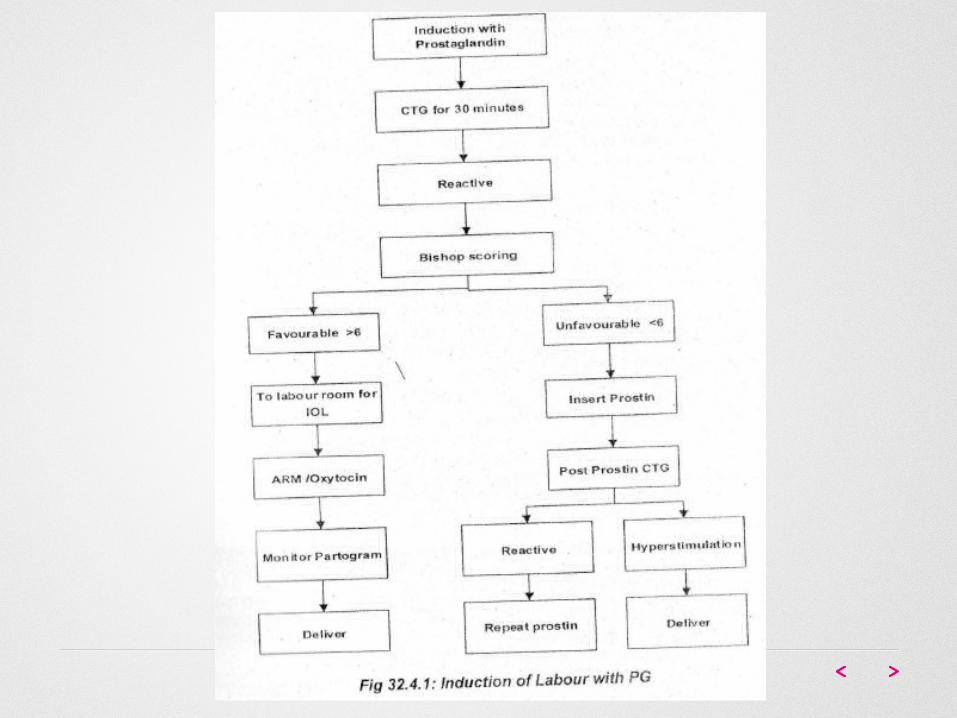
PRE INDUCTION CERVICAL ASSESSMENT:Modified Bishop’s Preinduction cervical scoring system: to determine the suitability of a patient for IOL in patients who were parous, at term , had an uncomplicated pregnancy and the fetus was in cephalic presentation.
FACTOR 0 1 2 3
Dilatation (cm) 0(closed)
1 – 2 3 – 4 5
Length (cm) >4 3 – 4 1 – 2 0
Position Posterior Midline Anterior -
Consistency Firm Medium Soft -
Head: station -3 -2 -1 , 0 +1 , +2
Score
Total Score =13Favourable Score= 6-13Unfavourable Score= 0-5
METHODS OF CERVICAL RIPENING AND IOL
Methods for cervical ripening and labor induction can be broadly classified as :
PHARMACEUTICAL MECANICAL SURGICAL

METHODS OF CERVICAL RIPENING AND IOLMECHANICAL
• Sweeping of membraneMembrane stripping at term shortens the interval of time to onset of spontaneous labor and reduces the need for formal induction.
• Foley's catheterThis uses the same mechanism as sweeping but the inflated bulb of Foley’sresults in release of endogenous prostaglandins and initiates labor.

METHODS OF CERVICAL RIPENING AND IOL• Exogenous ProstaglandinsProstaglandins (E2) are effective for both cervical ripening and- labor induction. Prostaglandin E2 are typically administered intravaginally for cervical ripening as the first step in labor induction. They are administered as gel, tablet or controlled release pessary.
The recommended regimens are:
One cycle of vaginal PGE2 tablets one dose 3mg in a nulliparous and 0.5 mg in a multipara, followed by second dose after 6 hours if labor is not established . Maximum of 2 doses in a cycle.
One cycle of vaginal PGE2 controlled release pessary one dose over 24 hours.
PHARMACEUTICAL
METHODS OF CERVICAL RIPENING AND IOL
intravaginal PGE2 are the preferred method of induction of labor, unless there are any specific indications for not using it like the risk of uterine hyperstimulation.
Prostaglandins PGEl – Misoprostol Although studies have demonstrated that misoprostol is an effective agent in induction of labor, there are concerns regarding its safety and until the best dosage regimen is determined, its use in labor induction is confined to clinical trials.
PHARMACEUTICAL
METHODS OF CERVICAL RIPENING AND IOL
Oxytocin
Increase in responsiveness with advancing gestational age. Once spontaneous labor begins the uterine sensitivity to endogenous oxytocin increases rapidly.
The dose is typically increased until there is normal progress of labor or strongcontractions occurring at 4 contractions per ten minutes and lasting for at least 45 seconds. There is no benefit to increasing the dose after one of theseendpoints has been achieved. Continuous monitoring of uterine activity and fetal heart rate are important once oxytocin is in use .
SURGICAL
METHODS OF CERVICAL RIPENING AND IOL Amniotomy
It is an effective method of labor induction but can only be performed in patients with partially dilated and effaced cervices.
The obstetrician should ensure that the fetal vertex is well-applied to the cervix and the umbilical cord or other fetal part is not the presenting part.
The fetal heart rate before and after the procedure has to be documented and the color of the amniotic fluid should be noted.
SURGICAL

CERVICAL RIPENING & SUCCESSFUL INDUCTION Oxytocin is less effective for labor induction when used in
women with uneffaced and undilated cervices. Therefore, a ripening process should be used prior to oxytocin induction when the cervix is unfavorable.
The two major methods are as follow:I. Mechanical (physical) interventions, such as disruption
of the fetal membranes or insertion of dilators or a balloon catheter.
II. Application of cervical ripening agents, such as prostaglandin compounds.
COMPLICATIONS Hyperstimulation Fetal hypoxemia Hyponatremia Hypotension Hyponatremia Failed induction Uterine rupture Hyperbilirunemia

XIE XIE