indications of niv in pediatric orphan disorders 14h00 orateur n… · indications of niv in...
TRANSCRIPT

Indications of NIV in pediatric orphan disorders
Brigitte Fauroux, MD PhD Pediatric Noninvasive Ventilation and Sleep unit
& Inserm U 955, Necker Hospital Paris - France
Inserm Institut national de la santé et de la recherche médicale
Indications of NIV in pediatric orphan diseases
• Orphan diseases that may need NIV in childhood
• Indications of NIV in children with orphan diseases

McDougall et al. Arch Dis Childh 2013;98:660
Incidence 1995-2009 Prevalence 1995-2009
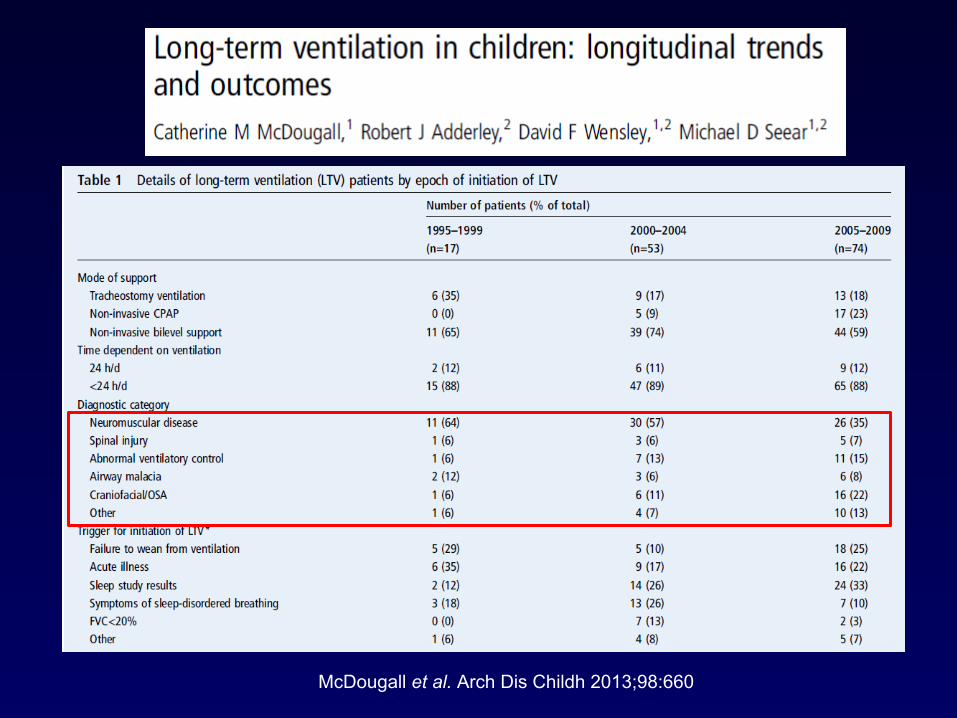
McDougall et al. Arch Dis Childh 2013;98:660
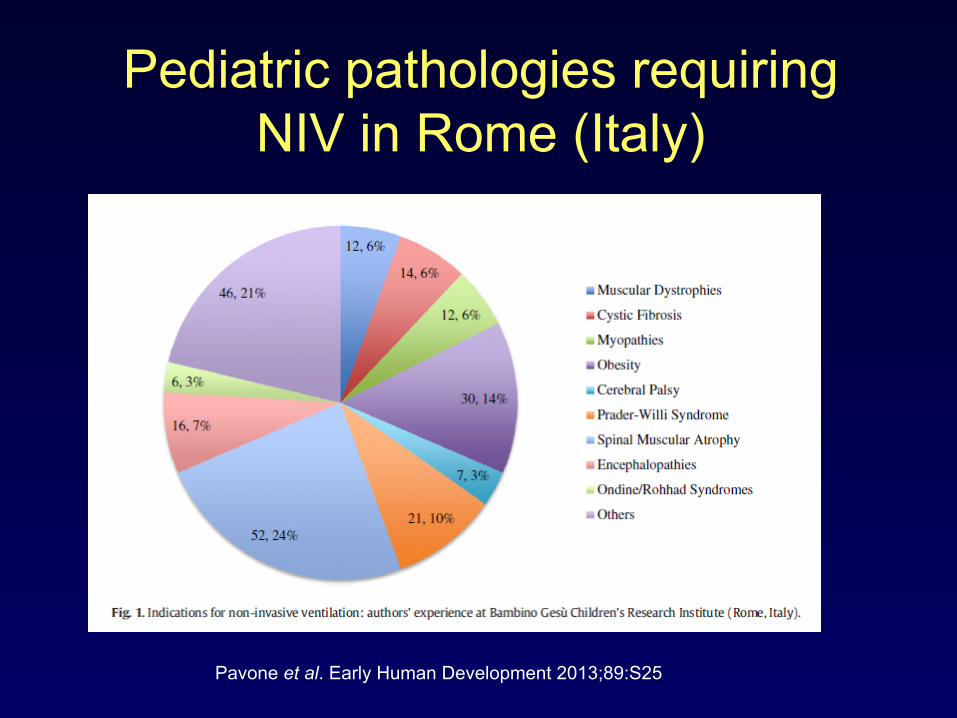
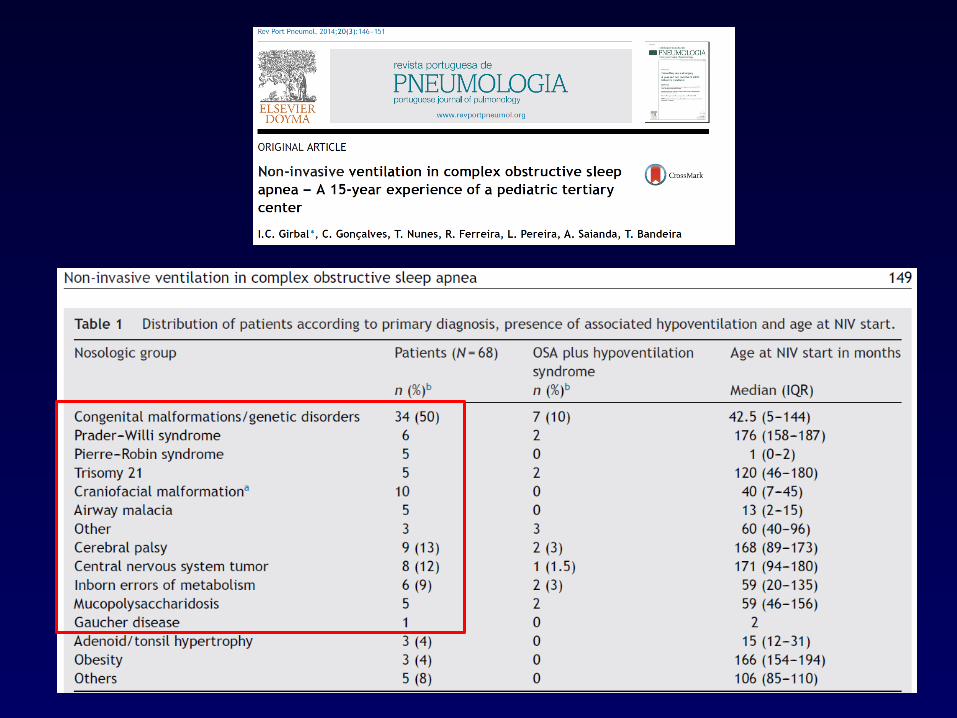
Pediatric pathologies requiring NIV in Rome (Italy)
Pavone et al. Early Human Development 2013;89:S25
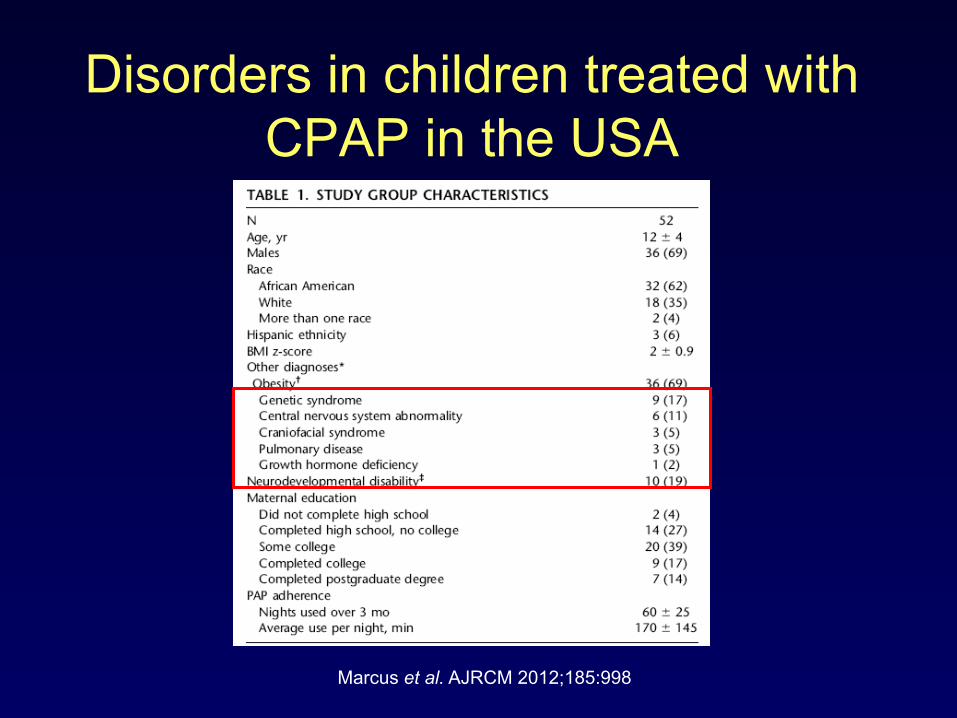
Disorders in children treated with CPAP in the USA
Marcus et al. AJRCM 2012;185:998
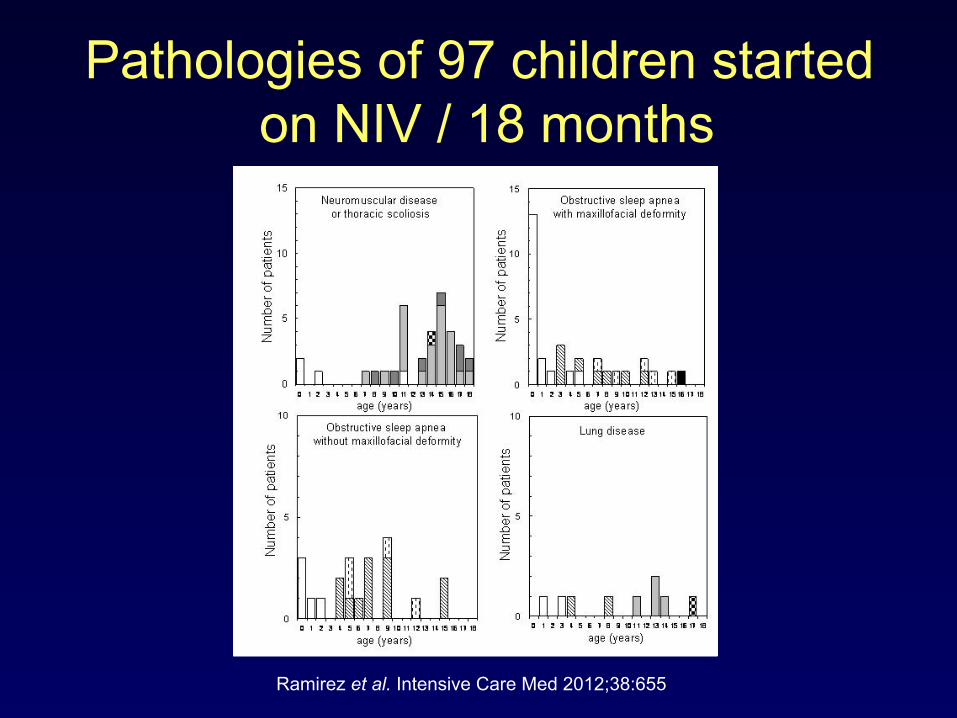
Pathologies of 97 children started on NIV / 18 months
Ramirez et al. Intensive Care Med 2012;38:655
Acute group n=15
Subacute group n=18
Chronic group n=43
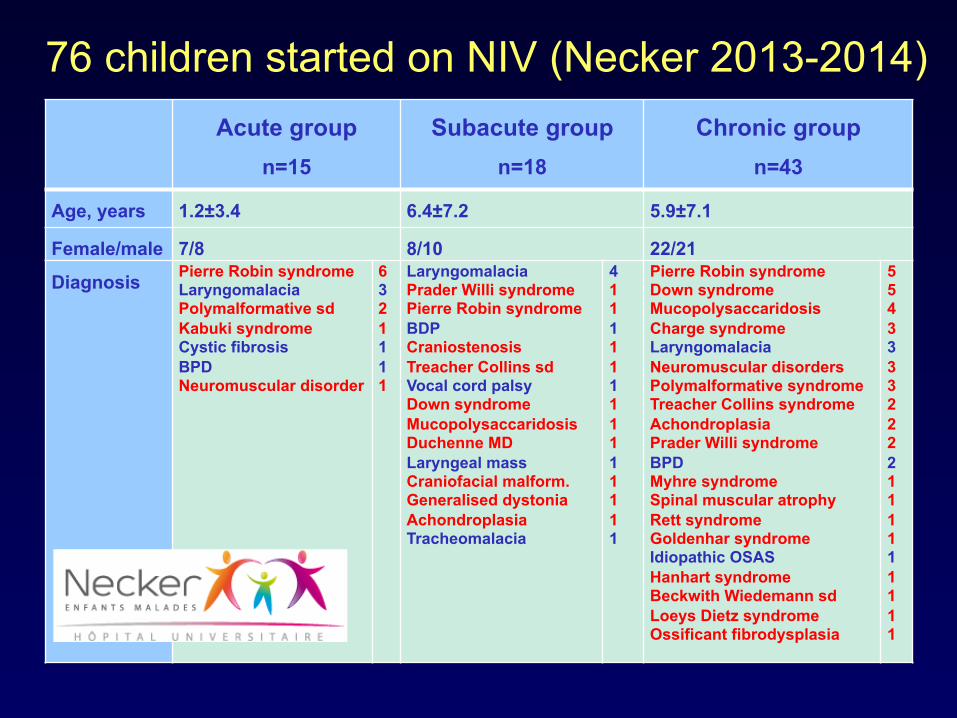
Age, years 1.2±3.4 6.4±7.2 5.9±7.1
Female/male 7/8 8/10 22/21
Diagnosis Pierre Robin syndrome Laryngomalacia Polymalformative sd Kabuki syndrome Cystic fibrosis BPD Neuromuscular disorder
6 3 2 1 1 1 1
Laryngomalacia Prader Willi syndrome Pierre Robin syndrome BDP Craniostenosis Treacher Collins sd Vocal cord palsy Down syndrome Mucopolysaccaridosis Duchenne MD Laryngeal mass Craniofacial malform. Generalised dystonia Achondroplasia Tracheomalacia
4 1 1 1 1 1 1 1 1 1 1 1 1 1 1
Pierre Robin syndrome Down syndrome Mucopolysaccaridosis Charge syndrome Laryngomalacia Neuromuscular disorders Polymalformative syndrome Treacher Collins syndrome Achondroplasia Prader Willi syndrome BPD Myhre syndrome Spinal muscular atrophy Rett syndrome Goldenhar syndrome Idiopathic OSAS Hanhart syndrome Beckwith Wiedemann sd Loeys Dietz syndrome Ossificant fibrodysplasia
5 5 4 3 3 3 3 2 2 2 2 1 1 1 1 1 1 1 1 1
76 children started on NIV (Necker 2013-2014)
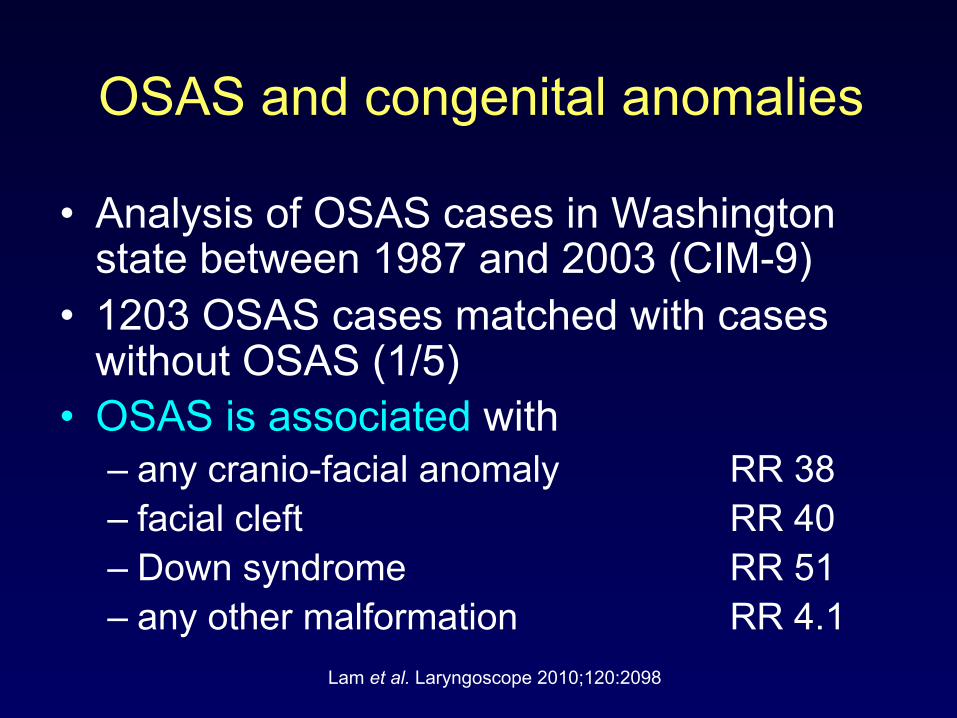
OSAS and congenital anomalies
• Analysis of OSAS cases in Washington state between 1987 and 2003 (CIM-9)
• 1203 OSAS cases matched with cases without OSAS (1/5)
• OSAS is associated with – any cranio-facial anomaly RR 38 – facial cleft RR 40 – Down syndrome RR 51 – any other malformation RR 4.1
Lam et al. Laryngoscope 2010;120:2098
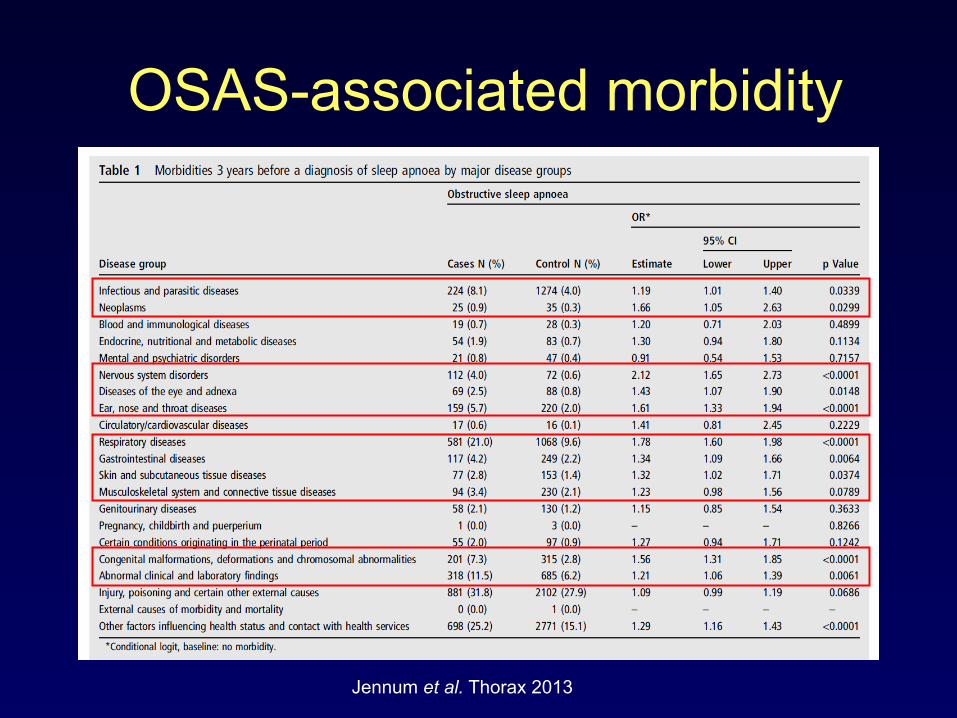
OSAS-associated morbidity
Jennum et al. Thorax 2013
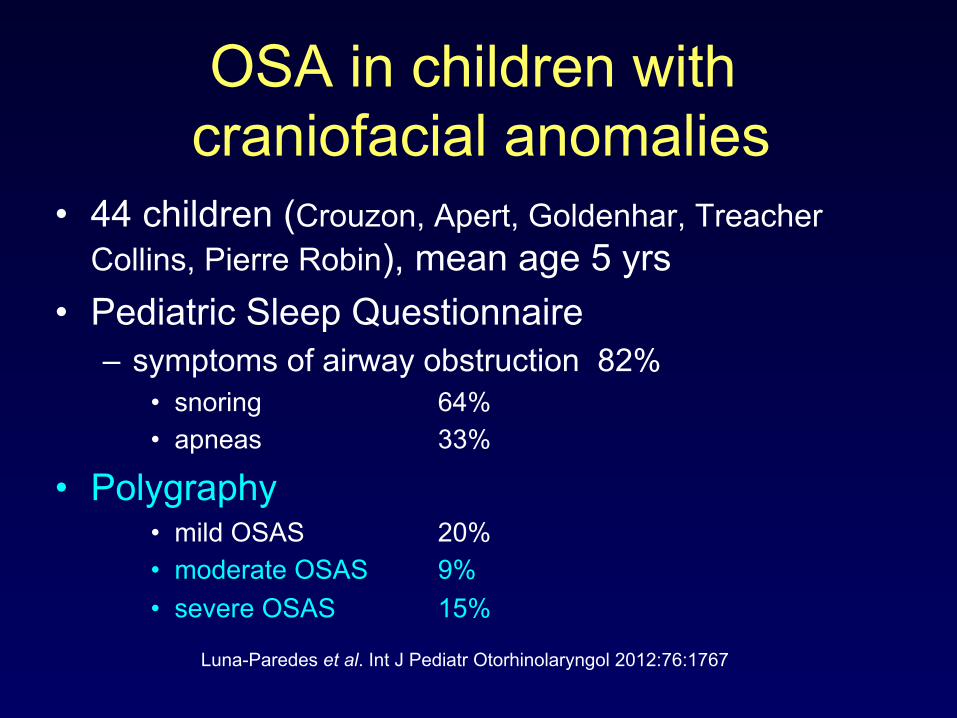
OSA in children with craniofacial anomalies
• 44 children (Crouzon, Apert, Goldenhar, Treacher Collins, Pierre Robin), mean age 5 yrs
• Pediatric Sleep Questionnaire – symptoms of airway obstruction 82%
• snoring 64% • apneas 33%
• Polygraphy • mild OSAS 20% • moderate OSAS 9% • severe OSAS 15%
Luna-Paredes et al. Int J Pediatr Otorhinolaryngol 2012:76:1767
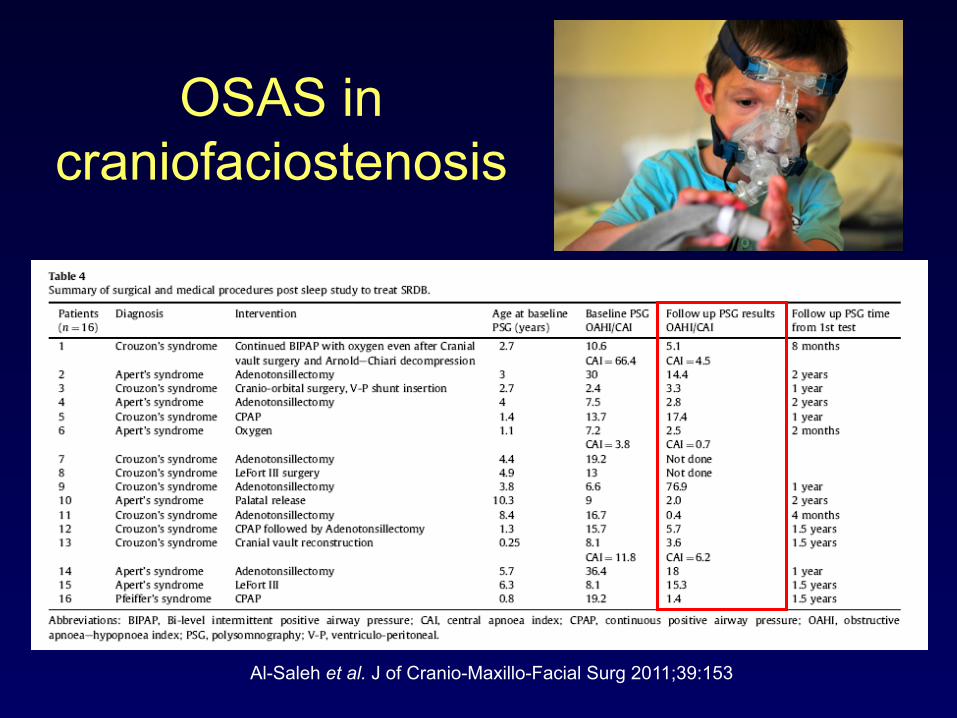
OSAS in craniofaciostenosis
Al-Saleh et al. J of Cranio-Maxillo-Facial Surg 2011;39:153
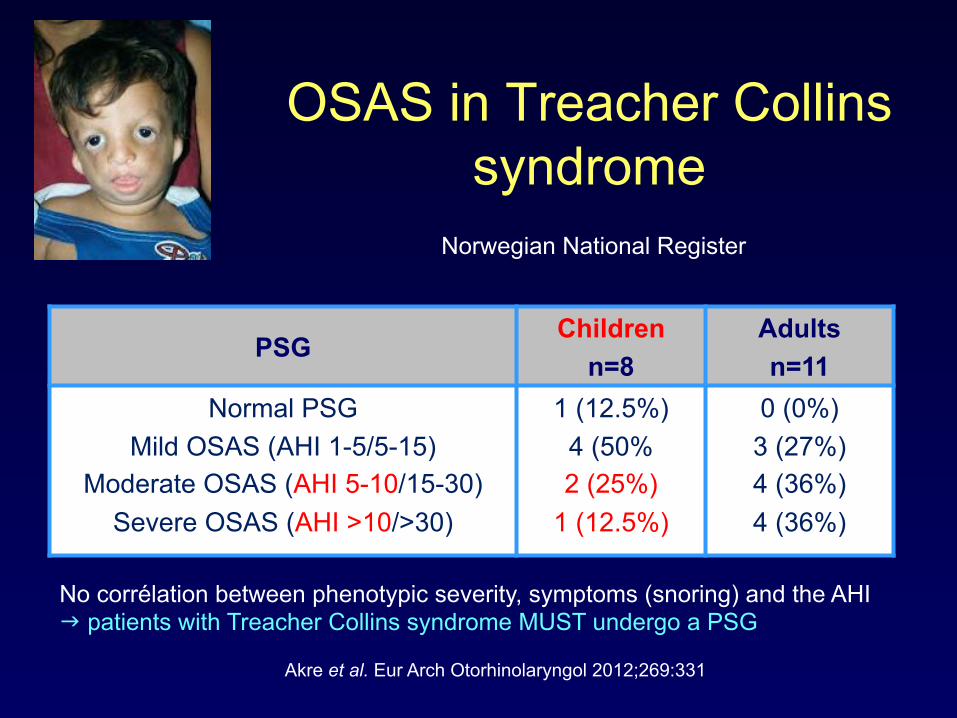
OSAS in Treacher Collins syndrome
Akre et al. Eur Arch Otorhinolaryngol 2012;269:331
PSG Children
n=8 Adults n=11
Normal PSG Mild OSAS (AHI 1-5/5-15)
Moderate OSAS (AHI 5-10/15-30) Severe OSAS (AHI >10/>30)
1 (12.5%) 4 (50% 2 (25%)
1 (12.5%)
0 (0%) 3 (27%) 4 (36%) 4 (36%)
No corrélation between phenotypic severity, symptoms (snoring) and the AHI g patients with Treacher Collins syndrome MUST undergo a PSG
Norwegian National Register
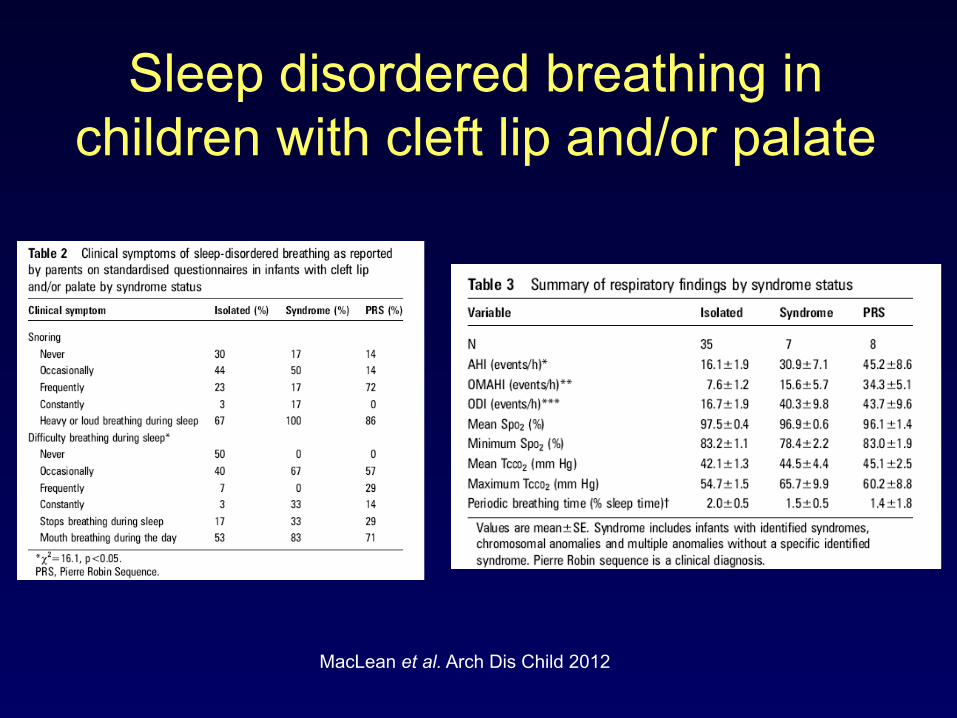
Sleep disordered breathing in children with cleft lip and/or palate
MacLean et al. Arch Dis Child 2012
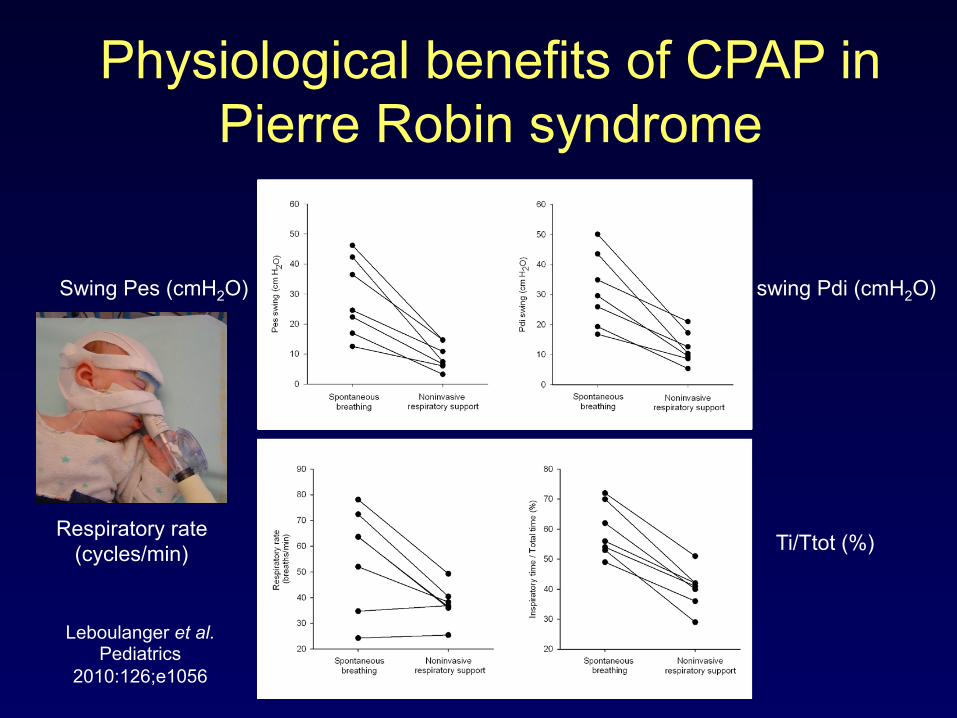
Physiological benefits of CPAP in Pierre Robin syndrome
Leboulanger et al. Pediatrics
2010:126;e1056
Swing Pes (cmH2O) swing Pdi (cmH2O)
Respiratory rate (cycles/min) Ti/Ttot (%)
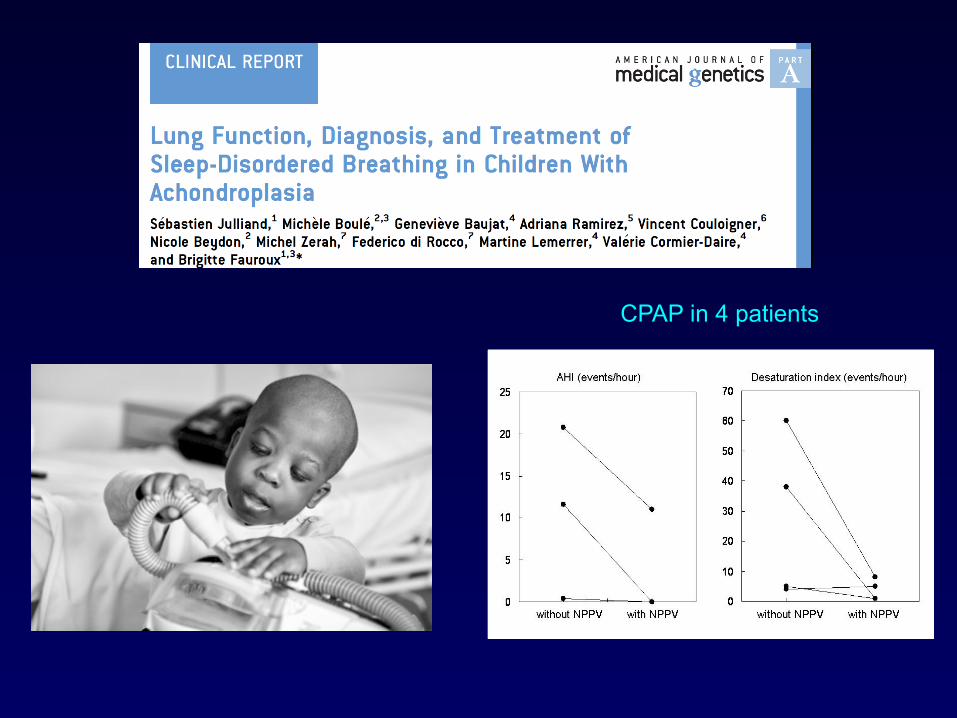
CPAP in 4 patients
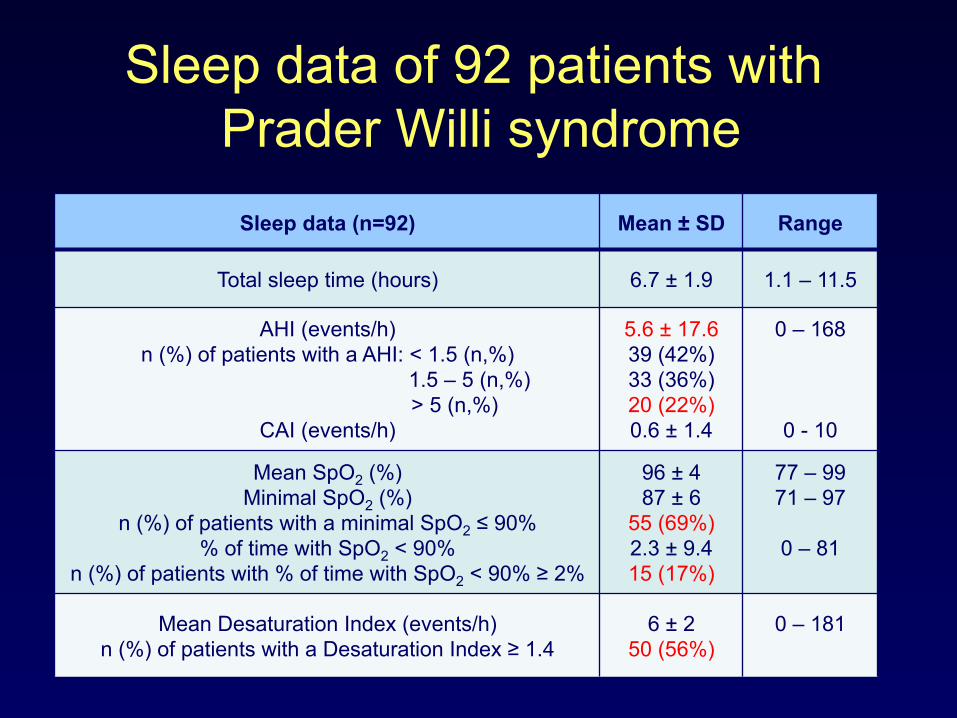
Sleep data of 92 patients with Prader Willi syndrome
Sleep data (n=92) Mean ± SD Range
Total sleep time (hours) 6.7 ± 1.9 1.1 – 11.5
AHI (events/h) n (%) of patients with a AHI: < 1.5 (n,%)
1.5 – 5 (n,%) > 5 (n,%)
CAI (events/h)
5.6 ± 17.6 39 (42%) 33 (36%) 20 (22%) 0.6 ± 1.4
0 – 168
0 - 10
Mean SpO2 (%) Minimal SpO2 (%)
n (%) of patients with a minimal SpO2 ≤ 90% % of time with SpO2 < 90%
n (%) of patients with % of time with SpO2 < 90% ≥ 2%
96 ± 4 87 ± 6
55 (69%) 2.3 ± 9.4 15 (17%)
77 – 99 71 – 97
0 – 81
Mean Desaturation Index (events/h) n (%) of patients with a Desaturation Index ≥ 1.4
6 ± 2 50 (56%)
0 – 181

Interventions after PG
Age (years) Growth
hormone therapy
ENT surgery Noninvasive ventilation
< 2 (n=37) 24 (65%) 5 (14%) 3 (8%)
2 – 4 (n=10) 8 (80%) 2 (20%) 2 (20%)
5 – 10 (n=17) 12 (70%) 3 (18%) 2 (12%)
11 – 20 (n=9) 3 (33%) 0 2 (22%)
> 20 (n=18) 1 (0.5%) 0 7 (39%)
Total population (n=92) 48 (52%) 10 (11%) 16 (17%)
Pavone et al. Pediatr Pulmonol, accepted
Conclusion - 1 • ~ 80% of children requiring CPAP/NIV
have an orphan disease • Association of complex disorders:
– obstructive (upper airway malformation) – restrictive (chest wall anomalies) – central (cervico-occipital compression)
• Challenging situations – choice of an adequate interface – ventilatory modes & settings
Indications of NIV in pediatric orphan diseases
• Orphan diseases that may need NIV in childhood
• Indications of NIV in children with orphan diseases
Aim of the study
• Analysis of criteria / situations that lead to the initiation of CPAP/NIV in children
• One year study (Sept 2013 – Oct 2014) in a single tertiary pediatric NIV center
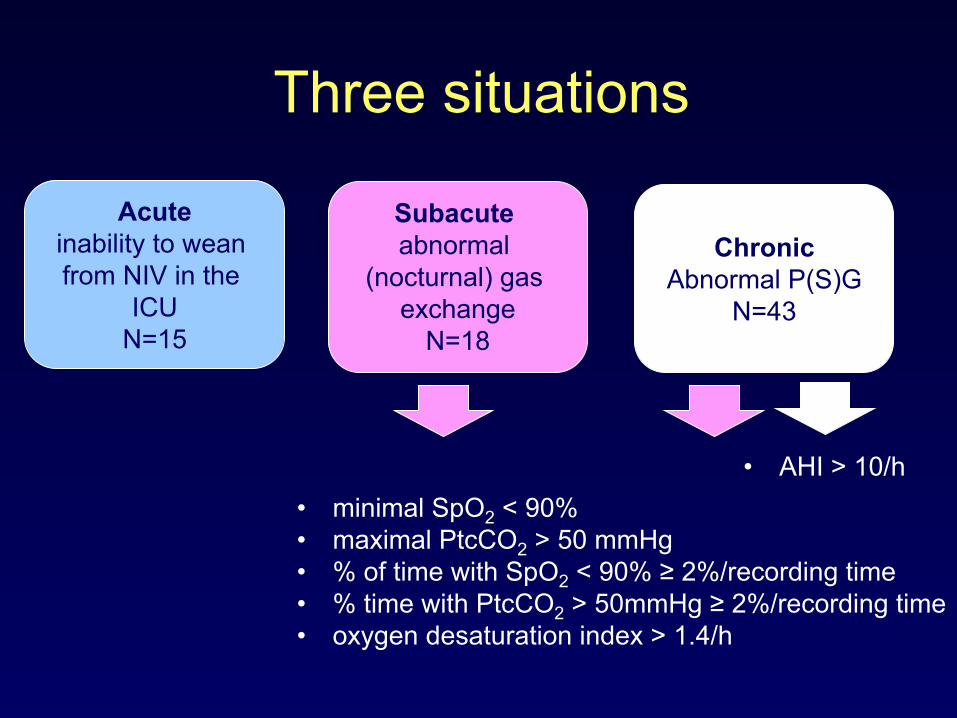
Three situations
Acute inability to wean from NIV in the
ICU N=15
Subacute abnormal
(nocturnal) gas exchange
N=18
Chronic
Abnormal P(S)G N=43
• minimal SpO2 < 90% • maximal PtcCO2 > 50 mmHg • % of time with SpO2 < 90% ≥ 2%/recording time • % time with PtcCO2 > 50mmHg ≥ 2%/recording time • oxygen desaturation index > 1.4/h
• AHI > 10/h
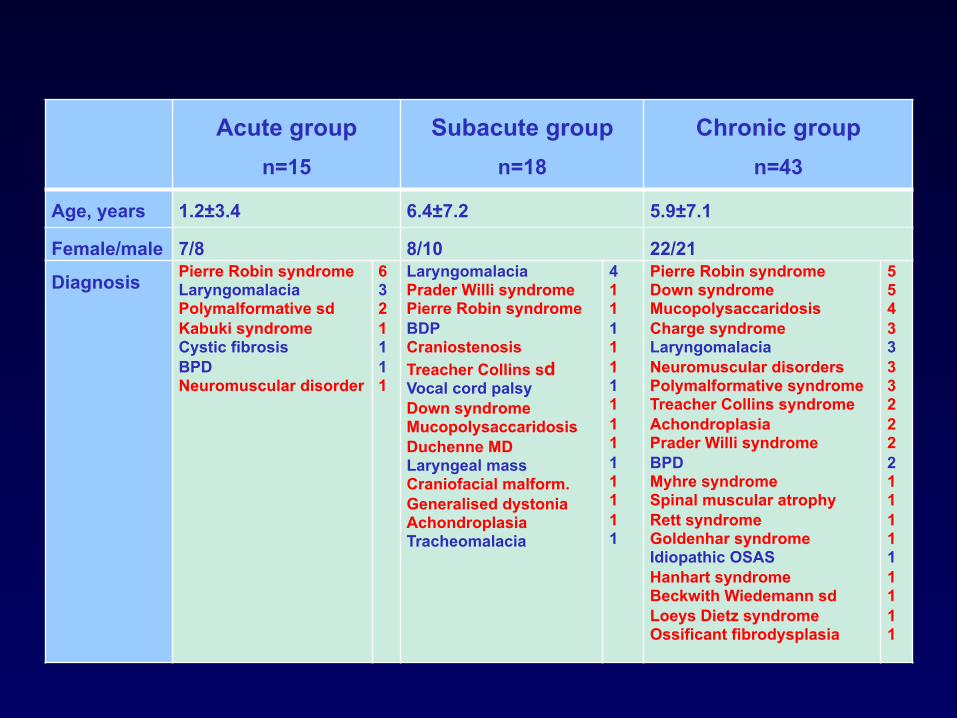
Acute group n=15
Subacute group n=18
Chronic group n=43
Age, years 1.2±3.4 6.4±7.2 5.9±7.1
Female/male 7/8 8/10 22/21
Diagnosis Pierre Robin syndrome Laryngomalacia Polymalformative sd Kabuki syndrome Cystic fibrosis BPD Neuromuscular disorder
6 3 2 1 1 1 1
Laryngomalacia Prader Willi syndrome Pierre Robin syndrome BDP Craniostenosis Treacher Collins sd Vocal cord palsy Down syndrome Mucopolysaccaridosis Duchenne MD Laryngeal mass Craniofacial malform. Generalised dystonia Achondroplasia Tracheomalacia
4 1 1 1 1 1 1 1 1 1 1 1 1 1 1
Pierre Robin syndrome Down syndrome Mucopolysaccaridosis Charge syndrome Laryngomalacia Neuromuscular disorders Polymalformative syndrome Treacher Collins syndrome Achondroplasia Prader Willi syndrome BPD Myhre syndrome Spinal muscular atrophy Rett syndrome Goldenhar syndrome Idiopathic OSAS Hanhart syndrome Beckwith Wiedemann sd Loeys Dietz syndrome Ossificant fibrodysplasia
5 5 4 3 3 3 3 2 2 2 2 1 1 1 1 1 1 1 1 1
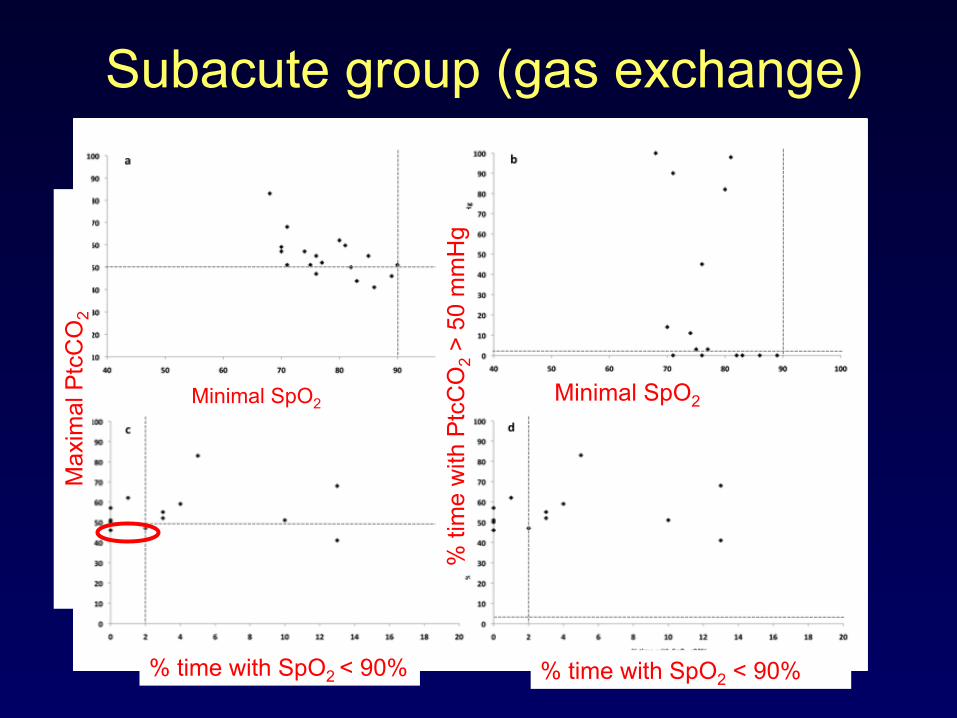
Subacute group (gas exchange)
Minimal SpO2 Minimal SpO2
% time with SpO2 < 90% % time with SpO2 < 90%
Max
imal
Ptc
CO
2
% ti
me
with
Ptc
CO
2 > 5
0 m
mH
g
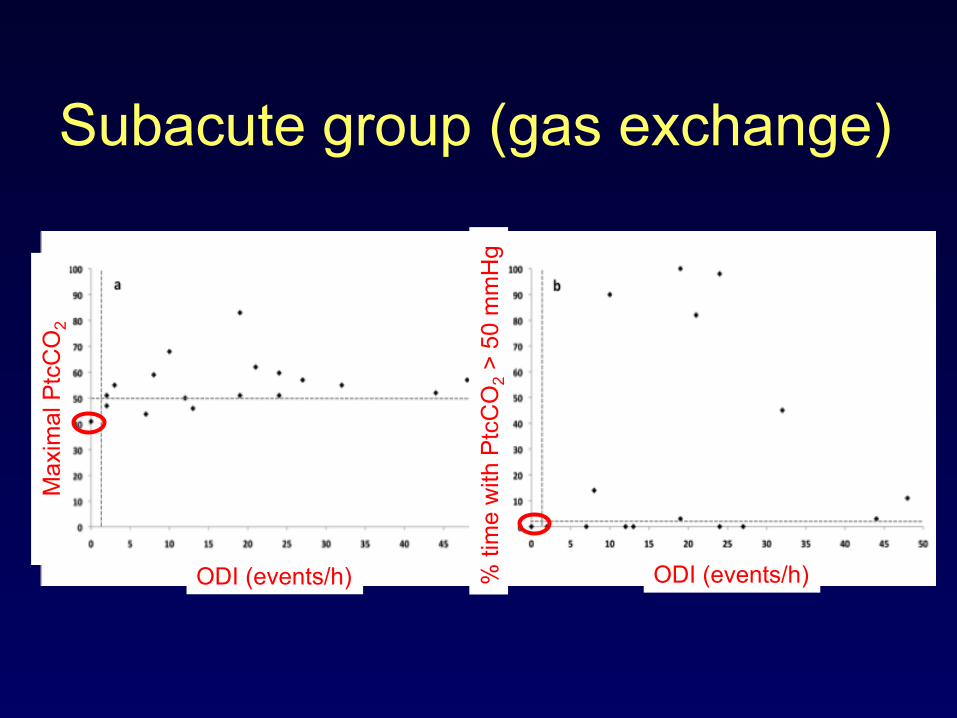
Subacute group (gas exchange)
ODI (events/h) ODI (events/h)
Max
imal
Ptc
CO
2
% ti
me
with
Ptc
CO
2 > 5
0 m
mH
g
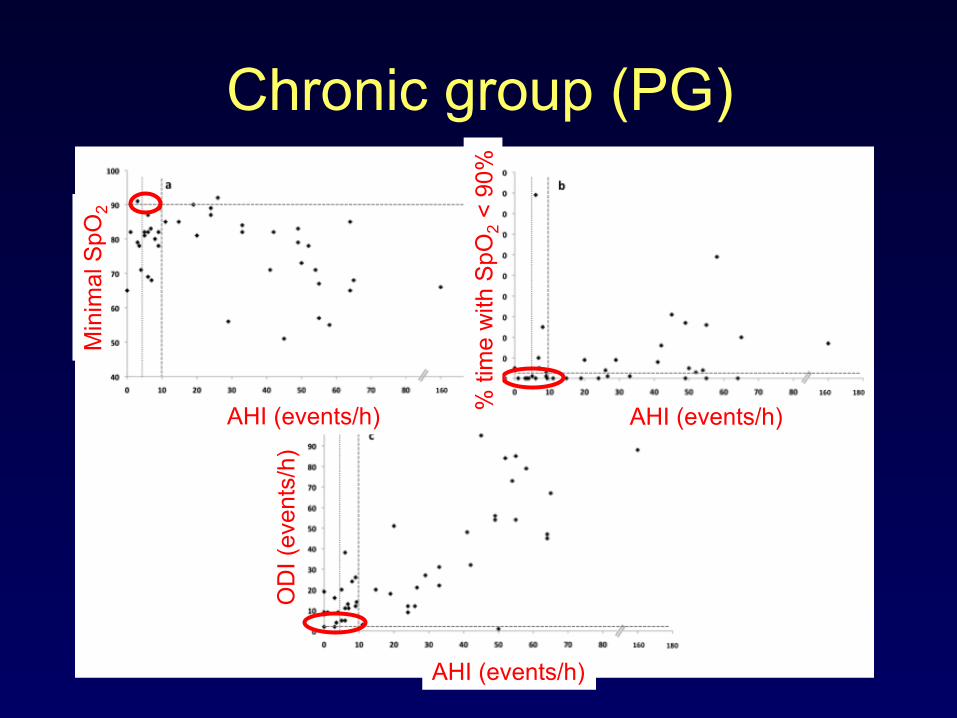
Chronic group (PG) M
inim
al S
pO2
% ti
me
with
SpO
2 < 9
0%
OD
I (ev
ents
/h)
AHI (events/h) AHI (events/h)
AHI (events/h)

Chronic group (PG)
AHI (events/h) AHI (events/h)
Max
imal
Ptc
CO
2
% ti
me
with
Ptc
CO
2 > 5
0 m
mH
g
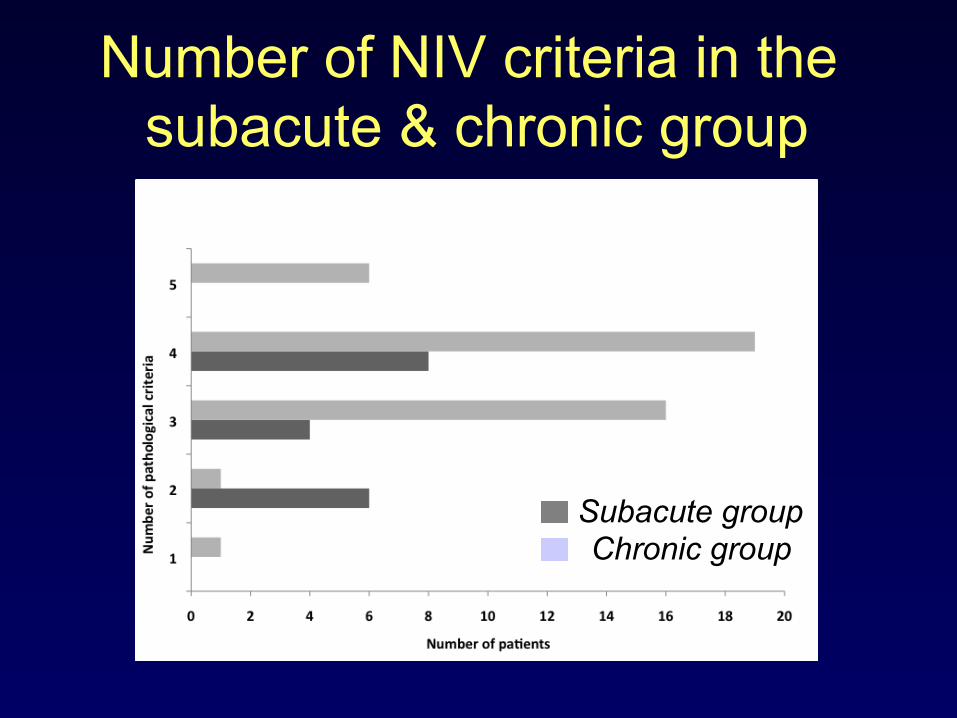
Number of NIV criteria in the subacute & chronic group
Subacute group Chronic group

Comparison of gas exchange in the subacute & chronic group
Subacute group n=18
Chronic group n=43
Nocturnal gas exchange
Mean SpO2 (%)
Minimal SpO2 (%)
Time spent with SpO2 < 90% (%)
Oxygen desaturation index (number/hr)
Mean PtcCO2 (mmHg)
Maximal PtcCO2 (mmHg)
Time spent with PtcCO2 > 50 mmHg (%)
94.2 ± 2.8
76.8 ± 9.8
7.9 ± 16.6
26.3 ± 24.4
45.8 ± 5.4
53.6 ± 9.4
21.5 ± 34
94.2 ± 2.7
77.3 ± 9.5
8.2 ± 16
27.6 ± 25.3
45.7 ± 5.5
53.3 ± 9.4
20.9 ± 32.9
AHI NA 27.2 ± 30
Conclusion - 2 • CPAP/NIV is initiated on > 1 criteria • No difference in gas exchange between
the subacute and chronic group • Limitations: single center • Prospectives:
– efficacy of & compliance with CPAP/NIV according to the initiation criteria
– comparison between centers and differents pathologies & ages
Conclusion
• A respiratory evaluation with sleep analysis should be performed on a routine basis in numerous orphan diseases in children
• Management of respiratory problem should be performed by an expert multi-disciplinary pediatric team
www.pediatric-niv-conference.com