increasing incidence of myelodysplastic syndromes: real or fictitious?
TRANSCRIPT

Pergamon Leukemia Research Vol. 22, No. I, 93- 100, 1998. pp.
0 1998 Published by Elsevier Science Ltd. All rights reserved Printed in Great Britain
0145-2126/98 $19.00 + 0.00
PII: SO1452126(97)00089-l
INCREASING INCIDENCE OF MYELODYSPLASTIC SYNDROMES: REAL OR FICTITIOUS?
Carlo Aul, Ulrich Germing, Norbert Gattermann and Horst Minning Department of Internal Medicine, Hematology and Oncology Division, Heimich Heine University,
MoorenstraRe 5, 40225 Dtisseldorf, Germany
(Received 15 May 1997. Accepted 14 June 1997)
Abstract-Over the past IO-20 years, there has been a growing interest in the myelodysplastic syndromes (MIX). Due to difficulties of diagnosis, classification and case recording, the epidemiological features of MDS are still poorly defined. Recently, a number of cancer registries have published data on the regional occurrence of MDS, suggesting that MDS are much more common than previously thought. The crude incidence of MDS in these studies was 3.5-12.6 per 100 000 population per year. In people over the age of 70 years, incidence rates varied between 15 and 50 per 100000 per year. Contrary to the assumption of most hematologists, cancer surveys usually failed to demonstrate a rising incidence of MDS. In those studies showing a significant increase in MDS, the rising number of cases was probably due to increased physician awareness and extended use of invasive diagnostic procedures in elderly people. Differences in incidence figures between regional studies may be attributed to several causes, including regional variations in disease incidence, small and ill-defined reference populations, bias due to patient referral patterns, varying intensity of diagnostic procedures and different observation periods. Because of the paucity of clinical symptoms and insignificance of morphological bone marrow changes particularly in early stage MDS, the currently available incidence figures are likely to underestimate the true incidence of MDS. Large-scale epidemiological studies are required for obtaining truly representative statistics on the incidence and prevalence of the MDS. In industrialized countries, a dramatic increase in these disorders can be expected over the next few decades due to the ‘greying’ of the population. 0 1998 Published by Elsevier Science Ltd. All rights reserved.
Key words: Myelodysplastic syndromes, epidemiology, incidence, causative factors, diagnostic accuracy, geriatric medical care.
Introduction
In 1991, Reizenstein and Dabrowski conducted an international opinion poll on the epidemiology of the myelodysplastic syndromes (MDS), in which 91% of 41 hematologists accepted a consensus statement that the prevalence and incidence of these disorders had increased by at least 100% during the past 10-20 years
Abbreviations: AML, acute myeloid leukemia; CMML, chronic myelomonocytic leukemia; FAB, French-American- British cooperative group; ZCD, International Classification of Diseases; LRF, Leukemia Research Fund Centre; MDS, myelodysplastic syndrome; RAEB, refractory anemia with excess of blasts; RAEB/I; refractory anemia with excess of blasts in transformation; RARS, refractory anemia with ring sideroblasts.
Correspondence to: Department of Internal Medicine, Hematology and Oncology Division, Heimich Heine Uni- versity, MoorenstraBe 5, 40225 Dusseldorf, Germany.
[l]. When asked for the causes of this development, most of the experts said that the increase in MDS was probably real and not due to improved diagnostics or demographical changes. More than 80% of the hematologists shared the impression that the rise in MDS resulted from increased exposure to leukemogenic agents at the workplace or during medical treatment.
However, these viewpoints should be interpreted cautiously, because an opinion poll is certainly not a reliable method for studying the incidence of MDS and its causative factors. Admittedly, there are no large-scale studies that provide reliable data on the descriptive and analytic epidemiology of MDS. Nevertheless, some progress has been made since the Delphi study was conducted by Reizenstein and Dabrowski. In this article, we shall review recent epidemiological studies that examined the incidence of these disorders. In addition, we shall discuss temporal trends in the disease
93
94 C. Au1 et al.
occurrence and try to answer the question whether the rising frequency of MDS is real or fictitious.
Diagnosis of Myelodysplastic Syndromes
MDS constitute a heterogenous group of acquired bone marrow disorders which are characterized by ineffective hematopoiesis, cellular dysfunction and an increased risk of transformation into acute myeloid leukemia (AML). Their diagnostic hallmark is periph- eral cytopenia with normal or increased bone marrow cellularity, although atypical variants with hypocellular bone marrow or pronounced myelofibrosis have also been described [2,3]. Morphological classification of the bone marrow changes is usually based on the diagnostic criteria of the French-American-British (FAB) Coop- erative Group [4]. It is generally agreed that MDS are caused by intrinsic defects of hematopoietic stem cells. The malignant character of MDS is suggested by the frequent increase in blast cells in the bone marrow, the occasional occurrence of Auer rods, the defective (‘leukemic’) in vitro growth pattern of hematopoietic progenitor cells and the detection of characteristic marker chromosomes. Cytogenetic abnormalities can be found in 40-60% of patients with primary MDS and are particularly common (up to 90%) in patients with secondary or therapy-related MDS [5]. Although it has not been possible to identify genetic lesions specific to MDS, certain anomalies (e.g. defects of chromosomes 5, 7 and 8) are clearly non-random changes. These genetic abnormalities reflect the multistep process of leukemo- genesis and clonal evolution in MDS.
Although MDS can occur in all age groups, they primarily affect elderly people. In larger series, the median age at diagnosis varied between 58 and 74 years [6]. Sixty to 90% of patients succumb to complications of their bone marrow disorder, with AML, infections or hemorrhages representing the main causes of death. The percentage of medullary blast cells and the karyotype at diagnosis appear to be the most important predictors of survival [7]. Patients with >lO% blast cells in the bone marrow or an unfavourable karyotype (chromosome 7 abnormalities or complex aberrations) usually sur- vive < 12 months [8].
Why are Epidemiological Data on MDS so Scarce?
Despite an increasing number of investigations into the MDS, precise data on the epidemiology and etiology of these disorders are largely lacking. The main reason for this appears to be that MDS has only recently been recognized as a specific hematological entity. MDS has been given at least 16 different names over the last 50 years. Therefore, it is not surprising that MDS was not an attractive disease for cancer epidemiologists.
Even today, 15 years after the publication of the FAB proposals [4], there are uncertainties concerning the diagnostic features of MDS, particularly for the early phases of the disease [9].
For many years, changing definitions and classifica- tions have impeded large-scale epidemiological studies that are required for obtaining truly representative data on the incidence and prevalence of MDS. MDS is not listed in the ninth version of the International Classifica- tion of Diseases (ICD) coding system for hematological malignancies [lo]. Therefore, cases must be assigned to various other diagnoses which are not always well defined. For example, chronic myelomonocytic leuke- mia (CMML) is grouped with the chronic myeloid leukemias rather than with MDS. A recent Swedish study found that cases of MDS were recorded under five different diagnoses in cancer registries [l]. Due to these shortcomings, current morbidity and mortality statistics are inadequate tools for characterizing the magnitude of the MDS problem. At present, accuracy of diagnosis and completeness of case registration seem to be confined to specialized registers such as regional cancer surveys or hospital-based statistics. It should be recognized that the usefulness of such registers is also restricted. Limiting factors include small and ill-defined reference popula- tions and bias due to patient referral patterns which are influenced by special diagnostic expertise of the participating institutions.
Crude and Age-specific Incidences of MDS
Up to now, only five studies have provided detailed data on the incidence of MDS. Except for one study, all investigations applied to relatively small patient samples and reference populations. All studies were performed in European countries. Crude and age-specific incidence figures calculated for these populations may not necessarily be valid for other countries in which people are exposed to different etiological agents. For example, Paydas and Kocak recently reported on a cohort of Turkish MDS patients who were on average 20 years younger than the typical MDS patient in Europe [ 1 I]. It was thought that this age discrepancy reflected differ- ences in ethnic, environmental, hygienic or infectious influences between the MDS populations.
The German study
Our study on the epidemiology of MDS in North- Rhine-Westfalia (Dusseldorf) covered a 16-year period from 1975 through 1990 [ 121. It was the first study to provide age-specific incidence figures of MDS. The Dusseldorf bone marrow register greatly benefits from the fact that bone marrow samples from virtually all cases of suspected hematological malignancy are sent to the University hematology department for cytological

Increasing incidence of myelodysplastic syndromes 95
Table 1. Minimal hematological criteria for diagnosis of MDS in the German study [12]
1. Peripheral blood: Single or multiple cytopenias Macrocytosis without anemia
2. Bone marrow: Normal or increased cellularity Signs of dyshematopoiesis No excessive myelofibrosis Myeloblast count < 30%
3. Absence of exclusion criteria: Vitamin B12 and folic acid deficiency Alcoholism Hypersplenism Paroxysmal nocturnal hemoglobinuria Antibody-mediated cytopenias Solid tumours Chronic inflammatory diseases Severe metabolic disorders Acute toxicity from myelotoxic substances or ionizing radiation
examination. For all potential MDS cases identified from the registry, the respective bone marrow slides were reevaluated. A morphological diagnosis of MDS was only accepted when the bone marrow showed normal or increased cellularity, signs of dyshematopoi- esis and a blast cell count ~30% (Table 1). The patients’ records were then traced in the University clinic and other hospitals, and reviewed for several clinical and laboratory features. Besides MDS patients, all cases of AML were retrieved from our database and used as a reference group for validation and comparison.
Among a total of 18 416 different bone marrow smears, 584 cases of MDS and 506 cases of AML were identified. Within the MDS group, 45% of patients had early stage MDS, 39% belonged to the refractory anemia with excess of blasts (RAEB) and refractory anemia with excess of blasts in transformation (RAEB/T) categories, and 16% of cases were classified as chronic myelomonocytic leukemia. Case registration over the study period differed considerably between MDS and AML. As regards AML, there was no consistent trend of increase or decline. On the other hand, the number of MDS patients rose substantially. This change was most pronounced during the last 8 years of study, with annual case numbers rising from 17 to 79. The relative frequency of MDS (percentage of MDS cases among other diagnoses in the registry) rose almost constantly from 1.3% during the first year of study to 4.5% in 1990, whereas a similar trend could not be recognized for the AML group.
For calculating MDS incidences, we had to restrict our analysis to the demographically well defined population of the town district of Dusseldorf (575 000 inhabitants). The steady increase in the number of MDS cases diagnosed produced a considerable rise in the age- related incidence figures over the 15-year collection
period. To compensate for annual variation, we calculated the incidences of MDS and AML by 5-year calendar periods, using average annual case numbers. Throughout the entire study period, the crude incidences remained almost constant for AML. They were 2.2 per 100 000 inhabitants per year. Looking at MDS, the crude annual incidences markedly increased from 1.3 in the first, to 4.1 in the last 5-year period. In the last quinquennium, MDS were about three times as frequent as AML in patients over 70. Crude annual incidence was also higher for MDS than for AML during the last 5-year observation period (Table 2).
The Swedish study
Radlund et al. [ 131 recently examined the incidence of MDS in the county of Jijnkiiping in Sweden. During the study period (1978-1992), 120 cases of MDS and 146
Table 2. Crude and age-specific incidences of MDS according to recently published regional studies [12,13,16] (incidence
figures per 100 000 population per annum)
Au1 et al. Radlund et al. Williamson [121 1131 et al. [16]
Geographic area Dusseldorf Jot&ping (Germany) (Sweden)
Study period 198690 1988-92
Age group ,<49 years 0.2 0.7
50-59years 60-69years > 4.9 > 1.6
70-79years >80years > 22.8 15.0
0.5 5.3
15.0 49.0 89.0
All ages 4.1 3.5 12.6
East Dorset (UK)
1981-90

96 C. Au1 et al.
Fig.
45
40
35 B z 8 30 E z .z 25
f 20
!t 3 15
10
5
O-24 25-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 >85
Agein5yearblocks 1. Age-specific incidence rates of MDS, separated according to sex, in the cancer registry of Cote d’Or (France) during the time
period of 198&1990. Incidence figures per 100 000 inhabitants per year. Reprinted with permission [14].
cases of AML were recorded. The numbers of newly diagnosed patients with MDS varied considerably from one year to another, but there was no obvious trend towards a rising frequency. Both the crude and age- specific incidences of MDS that they calculated for their reference population (3 10 000 inhabitants) were very similar to our own figures (Table 2). This is remarkable because the catchment area belongs to the rural parts of Sweden, without big cities, manufacturing industries or other obvious sources of toxic substances. During the last quinquennium (19881992), crude incidence was higher for MDS than for AML (4.3 vs 3.6 per 100 000 per year).
The French study Maynadie et al. [14] published data on the MDS
occurrence in the department of Cote d’Or which is located in Burgundy in France. About 480 000 inhabi- tants live in this region. Data on MDS and other hematopoietic malignancies were collected from public and private hospitals, general practitioners, biology and pathology laboratories as well as death certificates [ 151. All bone marrow smears were examined in a single cytology laboratory. During the study period (1980-
1990), a total of 167 cases of MDS were diagnosed. RAEB, refractory anemia with ring sideroblasts (RARS) and CMML were the most frequent morphological subtypes. The authors found that MDS cases represented about 10% of all hematological and lymphoid malig- nancy registrations. Noteworthy, 42% of MDS patients were diagnosed on the basis of an incidental blood count. People living in urban areas had a higher risk of MDS than those living in the countryside. The crude incidence of MDS was 3.2 per 100 000 per year. Age- specific incidence rates of MDS, separated according to sex, are shown in Fig. 1. No significant change in incidence was observed during the lo-year study period.
The British studies Williamson et ~2. [16] studied the incidence of MDS
in the East Dorset Health District in England. The East Dorset Health District serves a population which grew from 407 000 in 1980 to 452 000 in 1990. People living in the catchment area were not excessively exposed to toxic chemicals or ionizing radiation. Employment of residents was mainly in service industries such as tourism, banking or insurance. Epidemiological data of the study are summarized in Table 2. Over the lo-year
Increasing incidence of myelodysplastic syndromes 97
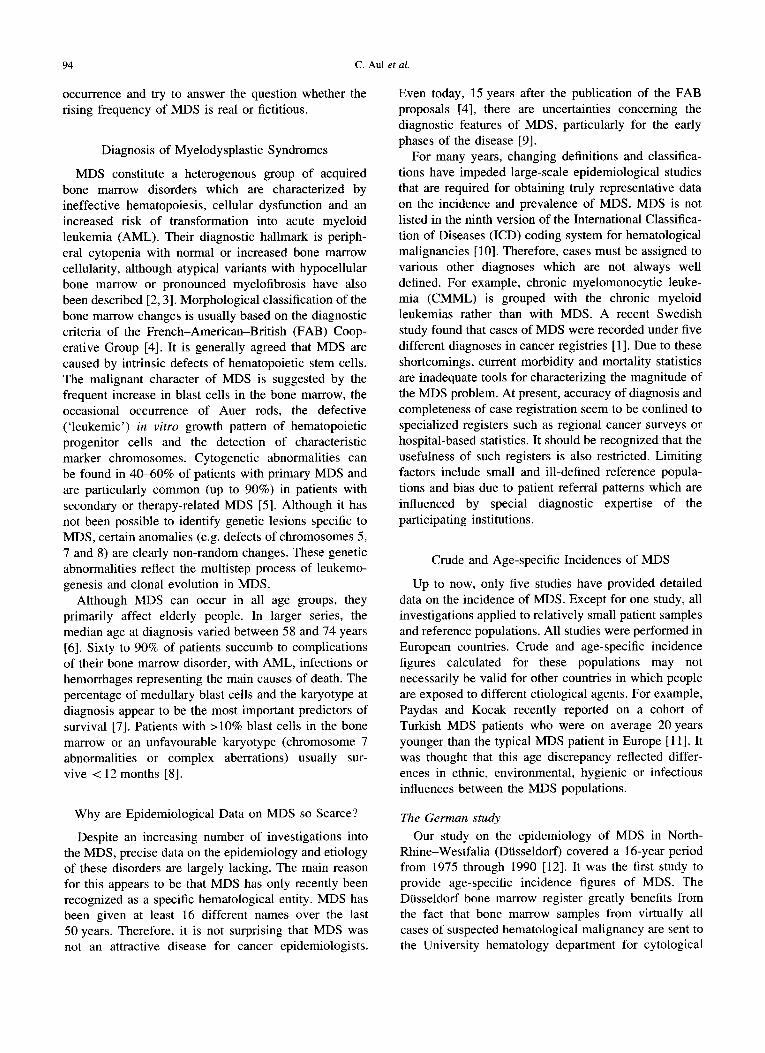
Table 3. Age-specific incidences of MDS and AML in the LRF Data Collection Survey during the time period of 1984-1986
[17] (incidence figures per 100 000 population per annum)
Age group (years) MDS AML
o-4 0.0 0.8 5-14 0.0 0.5
15-24 0.1 0.9 25-34 0.1 0.8 354 0.2 1.5 45-54 0.6 3.1 55-64 2.7 5.7 65-74 7.4 10.7 75-84 21.7 18.1
study period (1981-1990), a total of 279 new cases of MDS were diagnosed. Crude incidence of MDS was 12.6 per 100 000 per year, much higher than in the other studies. This difference extended to the age-specific incidence rates, which reached a maximum of 89 in patients >80 years of age. There was no increase in incidence rates over the study period. However, the authors emphasized that the average of 28 new cases per year in the period from 1981 to 1990 was substantially more than the four to six cases per year in the 1970s.
Subtypes of MDS in the British study were different from those in the other studies, with very few RAEB/T cases and nearly one third of patients belonging to the chronic myelomonocytic leukemia subgroup. Compared with the national average, the age distribution of the reference population was markedly skewed towards the old (22.7% of inhabitants >65 years), explaining the difference in crude incidences, but not in age-specific incidences between this study and the other epidemio- logical investigations. It should be emphasized, how- ever, that the authors performed hematological screening examinations in the elderly population and rigorously used bone marrow biopsies for documenting new cases of MDS. A cohort study of one large general practice revealed several previously unknown and asymptomatic cases, indicating that the observed indicence figures may still be an underestimate of the real incidence of MDS.
East Dorset is incorporated into the study area of the Leukemia Research Fund Centre for Clinical Epide- miology in England which also published data on the incidence of MDS [17]. This institution aims at complete registration of hematological neoplasias in- cluding aplastic anemias and MDS [ 181. The geogra- phical area of case collection extends over approximately half of England and Wales, and corre- sponds to a population of 16 million people, which is about one-third of the total population in Great Britain. The principal source of information is direct notifica- tions from collaborating local hematologists and histo-
pathologists via data clerks employed by the Leukemia Research Fund Centre (LRF). For the period of 1984 1986, the age-standardized incidence rate of MDS was 2.1 per 100 000 per year. Age-specific incidences were 2.7 for 55-64-year-old persons, 7.4 for 65-74-year-old persons, and >20 for the oldest age group (Table 3). Except for the patients >75, the incidences of MDS were lower than those of AML. The LRF has recently extended their analysis and incorporated the years 1987 and 1988. Incidence figures of MDS nearly doubled over the entire 5-year observation period [19]. Of interest, the LRF observed a marked variation in incidence rates among administrative counties, which was felt to reflect local hematological interests as well as differences in local population age structures. It should be emphasized that the LRF data are not exactly comparable to those of the other studies, because patients with RAEB/T were excluded. In large series, RAEB/T accounts for 4-27% of all MDS diagnoses rw.
Real or Apparent Increase of Myelodysplastic Syndromes?
Although not supported by all studies mentioned above, there is little doubt that the number of MDS cases diagnosed has risen substantially over the last two decades. Until 1973 there were only 143 patients with MDS reported worldwide [21]. Nowadays, referral centres are able to collect similar case numbers within a few years. What is behind this increase?
Principally, the rise in MDS cases may be attributed to several factors, including changes in the age structure of the population, better or more widely available laboratory facilities, expanded use of invasive diagnostic procedures, introduction of a practicable morphological classification (FAB classification system), increased exposure to known or new leukemogenic agents, and of course, a combination of these factors. We shall try to answer these questions by drawing on our own study material.
Demographical changes Changing demographics are unlikely to explain the
rising frequency of MDS in the Dusseldorf area, because the age structure of our reference population remained almost constant over the study period [ 111. However, in view of the ‘greying’ of the population in developed countries, we can be almost certain that there will be a substantial increase in MDS over the next few decades. According to Census Bureau projections, people over age 65 who now account for 12% of the population will increase to 21% by the year 2030 [22]. These dramatic changes in the age distribution of the population will

98 C. Au1 et al.
7-
6-
‘75 ‘76 ‘77 ‘78 ‘79 ‘80 ‘81 ‘82 ‘83 ‘84 ‘85 ‘86 ‘87 ‘88 ‘89 ‘90
Year Fig. 2. Annual case numbers of therapy-related MDS in the Dusseldorf bone marrow register between 1975 and 1990. Underlying malignant disorders in patients with secondary MDS were multiple myeloma (n = 6), breast cancer (n = 5), Hodgkin’s disease (n = 4), non-Hodgkin lymphoma (n = 4), thyroid carcinoma (n = 3) and other cancers (n = 5). Four patients had been treated for non- malignant disorders. Treatment consisted of cytotoxic chemotherapy (n = 13), radiotherapy (n = 10) and combined radio-
chemotherapy (n = 8).
lead to a marked increase in ail age-related disorders including the MDS.
Increased exposure to Eeukemogenic agents To examine the hypothesis of increased leukemogenic
exposure, we looked for known risk factors for the development of MDS. Reports in the literature have ascribed an etiological role to cytostatic treatment, ionizing radiation and prolonged occupational exposure to organic solvents or insecticides. However, there were only 31 patients in our series in whom a diagnosis of therapy-related secondary MDS could be made. Although we found a slight increase in frequency over the course of our study (Fig. 2), it is clear that this small patient group cannot account for the remarkable rise in the entire numbers of MDS cases.
We also screened our MDS population for potential occupational contact with myelotoxic substances. How- ever, by review of medical records or direct questioning of our patients, we found only 12 cases in which significant exposure to organic solvents could not be ruled out. Notwithstanding the limitations of a retro- spective study such as ours which cannot provide detailed information on occupational and environmental exposure, we do not think that leukemogenic toxins were responsible for the marked rise in MDS that we observed during the study period.
Changes in geriatric medical care Instead of invoking a change in etiological factors we
would rather ascribe the rising number of new MDS cases to improved geriatric medical care. We observed that in recent years physicians have become acquainted
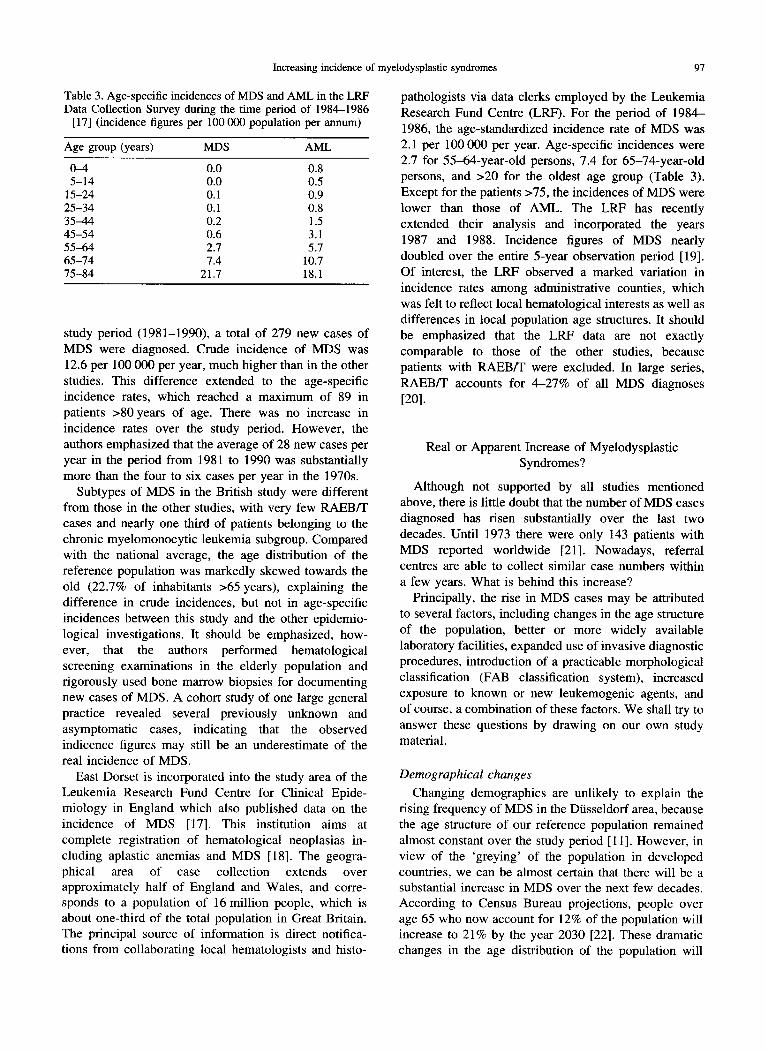
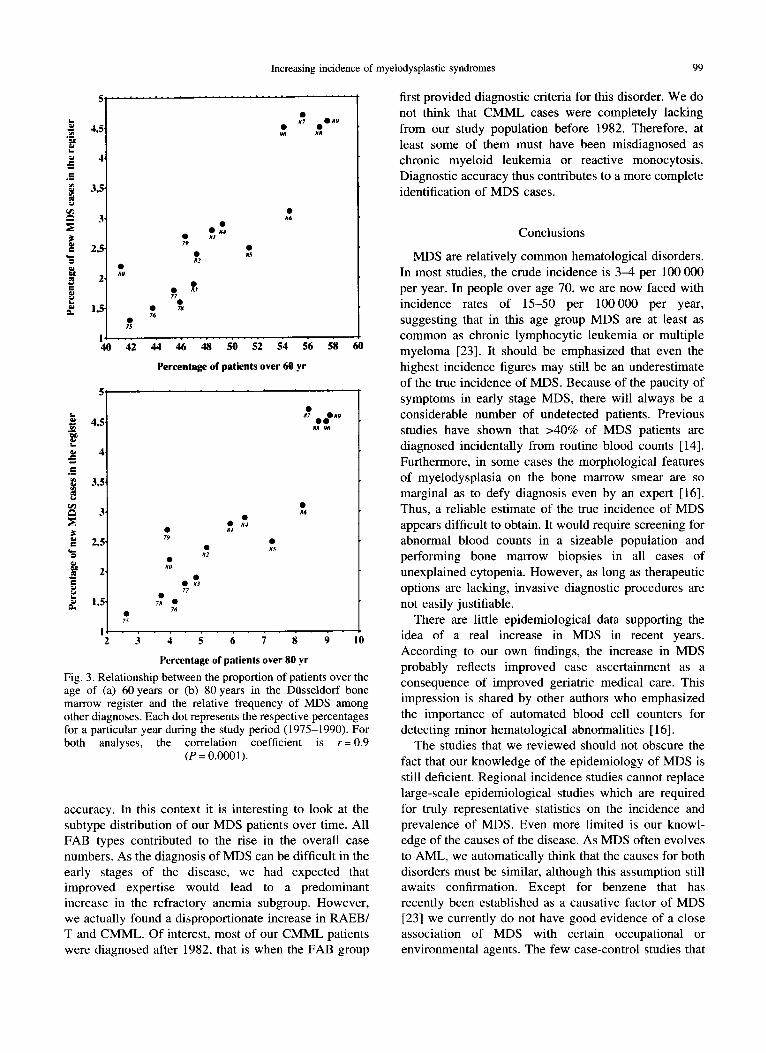
with MDS as a relatively common disease entity in elderly patients. This has been facilitated by the introduction of a practicable morphological classifica- tion, proposed by the FAB group in 1982 [4]. An increased index of suspicion has certainly helped to identify many new cases of MDS, even though the diagnosis can be masked in geriatric patients by multiple concurrent illnesses. Apparently, improved knowledge of MDS also increased the willingness of physicians to perform bone marrow biopsies in elderly people in order to arrive at a plausible explanation for abnormal hematological findings. This is suggested by data from the Dusseldorf bone marrow register, revealing a change in the age distribution of patients undergoing bone marrow biopsy (Fig. 3). The proportion of patients >60 years among new entries to the register increased from 42% in 1975 to 54% in 1990. During the same time period, the percentage of over 80-year-old patients climbed from 2.5 to 9%. Not surprisingly, there was a strong correlation between the proportion of elderly patients among new entries to the register and the relative frequency of MDS cases diagnosed. We there- fore think that the rising incidence of MDS at least partly reflects increased physician awareness and extended use of diagnostic procedures in the elderly. Considering the characteristic age distribution of MDS, careful hematological diagnostics in geriatric patients will inevitably increase the number of MDS patients identified.
Diagnostic accuracy In order to improve case ascertainment, an increased
level of suspicion must be coupled with diagnostic
Increasing incidence of myelodysplastic syndromes 99
0 85
k 4 4i 46 48 50 52 54 56 58 60
Percentage of patients over 60 yr
Percentage of patients over 80 yr
Fig. 3. Relationship between the proportion of patients over the age of (a) 60 years or (b) 80 years in the Diisseldorf bone marrow register and the relative frequency of MDS among other diagnoses. Each dot represents the respective percentages for a particular year during the study period (1975-1990). For both analyses, the correlation coefficient is r= 0.9
(P = 0.0001).
accuracy. In this context it is interesting to look at the subtype distribution of our MDS patients over time. All FAB types contributed to the rise in the overall case numbers. As the diagnosis of MDS can be difficult in the early stages of the disease, we had expected that improved expertise would lead to a predominant increase in the refractory anemia subgroup. However, we actually found a disproportionate increase in RAEB/ T and CMML. Of interest, most of our CMML patients were diagnosed after 1982, that is when the FAB group
first provided diagnostic criteria for this disorder. We do not think that CMML cases were completely lacking from our study population before 1982. Therefore, at least some of them must have been misdiagnosed as chronic myeloid leukemia or reactive monocytosis. Diagnostic accuracy thus contributes to a more complete identification of MDS cases.
Conclusions
MDS are relatively common hematological disorders. In most studies, the crude incidence is 3-4 per 100 000 per year. In people over age 70, we are now faced with incidence rates of 15-50 per 100000 per year, suggesting that in this age group MDS are at least as common as chronic lymphocytic leukemia or multiple myeloma [23]. It should be emphasized that even the highest incidence figures may still be an underestimate of the true incidence of MDS. Because of the paucity of symptoms in early stage MDS, there will always be a considerable number of undetected patients. Previous studies have shown that >40% of MDS patients are diagnosed incidentally from routine blood counts [14]. Furthermore, in some cases the morphological features of myelodysplasia on the bone marrow smear are so marginal as to defy diagnosis even by an expert [ 161. Thus, a reliable estimate of the true incidence of MDS appears difficult to obtain. It would require screening for abnormal blood counts in a sizeable population and performing bone marrow biopsies in all cases of unexplained cytopenia. However, as long as therapeutic options are lacking, invasive diagnostic procedures are not easily justifiable.
There are little epidemiological data supporting the idea of a real increase in MDS in recent years. According to our own findings, the increase in MDS probably reflects improved case ascertainment as a consequence of improved geriatric medical care. This impression is shared by other authors who emphasized the importance of automated blood cell counters for detecting minor hematological abnormalities [ 161.
The studies that we reviewed should not obscure the fact that our knowledge of the epidemiology of MDS is still deficient. Regional incidence studies cannot replace large-scale epidemiological studies which are required for truly representative statistics on the incidence and prevalence of MDS. Even more limited is our knowl- edge of the causes of the disease. As MDS often evolves to AML, we automatically think that the causes for both disorders must be similar, although this assumption still awaits confirmation. Except for benzene that has recently been established as a causative factor of MDS [23] we currently do not have good evidence of a close association of MDS with certain occupational or environmental agents. The few case-control studies that

100 C. Au1 et al.
have been published [24-261 are not conclusive because patient groups are too small and exposures to potential carcinogens have been difficult to measure retrospec- tively. Unfortunately, we cannot expect a rapid correc- tion of this deficiency, because the long period of latency, the likely involvement of several causal factors, and the demographic characteristics of the populations at risk will make it very difficult to conduct successful epidemiological studies.
Acknowledgement-This work was supported by the Leuk%mie-Liga e.V.
References
1. Reizenstein, P. and Dabrowski, L., Increasing prevalence of the myelodysplastic syndromes. An international Delphi study. Anticancer Research, 1991, 11, 1069.
2. Lambertenghi-Deliliers, G., Orazi, A., Luksch, R., Annaloro, C. and Soligo, D., Myelodysplastic syndrome with increased marrow fibrosis. A distinct clinico-patho- logical entity. British Journal of Haematology, 1991, 78, 161.
3. Maschek, H., Kaloutsi, V., Rodriguez-Kaiser, M., Werner, M., Choritz, H., Mainzer, K., Dietzfelbinger, M. and Georgii, A., Hypoplastic myelodysplastic syndrome. Incidence, morphology, cytogenetics, and prognosis. Annals in Hematology, 1993, 66, 117.
4. Bennett, J. M., Catovsky, D., Daniel, M. T., Flandrin, G., Galton, D. A. G., Gralnick, H. R. and Sultan, C., Proposals for the classification of the myelodysplastic syndromes. British Journal of Haematology, 1982, 51, 189.
5. Smith, M. A., McCaffrey, R. P. and Karp, J. E., The secondary leukemias: challenges and research directions. Journal of National Cancer Institute, 1996, 88, 407.
6. Aul, C., Gattermann, N. and Schneider, W., Epidemiolo- gical and etiological aspects of myelodysplastic syndromes. Leukemia Lymphoma, 1995, 16, 247.
7. Sanz, G. F. and Sanz, M. A., Prognostic factors in myelodysplastic syndromes. Leukemia Research, 1992,16, 77.
8. Greenberg, P., Cox, C., LeBeau., M. M., Fenaux, P., Morel, P., Sanz, G., Sanz, M., Vallespi, T., Hamblin, T., Oscier, D., Ohyashiki, K., Toyama, K., Aul, C., Mufti, G. and Bennett, J. International scoring system for evaluating prognosis in myelodysplastic syndromes. Blood, 1997, 89, 2079.
9. Reizenstein, P. and Gst, A., What is MDS? Leukemia Research, 1992, 16, 3.
10. World Health Organization, International Clussijication of Disease, 9th revision. World Health Organization, Geneva, 1977.
11. Paydas, S. and Kocak, R., Younger age observation in myelodysplastic syndromes (letter to the editor). Leukemia Research, 1996, 20, 367.
12. Aul, C., Gattermann, N. and Schneider, W., Age-related incidence and other epidemiological aspects of myelodys-
plastic syndromes. British Journal of Haematology, 1992, 82, 358.
13. Radlund, A., Thiede, T., Hansen, S., Carlsson, M. and Engquist, L., Incidence of myelodysplastic syndromes in a Swedish population. European Journal of Haematology, 1995, 54, 153.
14. Maynadie, M., Verret, C., Moskovtchenko, R., Mugneret, F., Petrella, T., Caillot, D. and Carli, P. M., Epidemiolo- gical characteristics of myelodysplastic syndromes in a well-defined French population. British Journal of Cancer, 1996, 74, 288.
15. Carli, P. M., Milan, C., Lange, A., Devilliers, E., Guy, H. and Faivre, J., Haematopoietic malignancies in Cote d’Or (France): a population based study. British Journal of Cancer, 1986, 53, 811.
16. Williamson, P. J., Kruger, A. R., Reynolds, P. J., Hamblin, T. J. and Oscier, D. G., Establishing the incidence of myelodysplastic syndrome. British Journal of Haematology, 1994, 87, 743.
17. Cartwright, R. A., Incidence and epidemiology of the myelodysplastic syndromes. In The Myelodysplastic Syn- dromes, eds G. J. Mufti and D. A. G. Galton, Churchill Livingstone, Edinburgh, 1992, p. 23.
18. Alexander, F., Ricketts, T. J., McKinney, P. A. and Cartwright, R. A., Cancer registration of leukaemias and lymphomas: results of a comparison with a specialist registry. Community Medicine, 1989, 11, 81.
19. Cartwright, R. A., Alexander, F. E., McKinney, P. A. and Ricketts, T. J., Leukaemias and Lymphoma: An Atlas of Distribution within Areas of England and Wales 1986 1988. Leukaemia Research Fund, London, 1990.
20. Pagliuca, A. and Mufti, G. J., Clinicomorphological features of myelodysplastic syndromes, In The Myelodys- plastic Syndromes, eds G. J. Mufti and D. A. G. Galton, Churchill Livingstone, Edinburgh, 1992, p. 1.
21. Saami, M. I. and Linman, J. W., Preleukemia: the hematologic syndrome preceding acute leukemia. Amer- ican Journal of Medicine, 1973, 55, 38.
22. Frank-Stromborg, M., Changing demographics in the United States. Implications for health professionals. Cancer, 1991, 67, 1772.
23. Travis, L. B., Li, C.-Y., Zhang, Z.-N., Li, D.-G., Yin, S.-N., Chow, W.-H., Li, G.-L., Dosemeci, M., Blot, W., Fraumeni, J. F., Hayes, R. B. and Linet, M. S., Hematopoietic malignancies and related disorders among benzene-exposed workers in China. Leukemia Lymphoma, 1994, 14, 91.
24. Mele, A., Szklo, M., Visani, G., Stazi, M. A., Castelli, G., Pasquini, P. and Mandelli, F., Hair dye use and other risk factors for leukemia and pre-leukemia: a case-control study. American Journal of Epidemiology, 1994, 139, 609.
25. West, R. R., Stafford, D. A., Farrow, A. and Jacobs, A., Occupational and environmental exposures and myelodys- plasia: a case-control study. Leukemia Research, 1995, 19, 127.
26. Nisse, C., Lorthois, C., Dorp, V., Eloy, E., Haguenoer, J. M. and Fenaux, P., Exposure to occupational and environmental factors in myelodysplastic syndromes. Preliminary results of a case-control study. Leukemia, 1995, 9, 693