incidental findings on routine abdominal imaging · incidental pancreatic cyst • incidence...
TRANSCRIPT
“To Follow or Not to Follow”Incidental Findings on Routine
Abdominal Imaging
Benjamin Holman, MDMemphis Radiological, PCAssistant Program Director
UTHSC/ Methodist Radiology Residency
Outline
• Background
• I. Liver Lesions
• II. Pancreatic Cysts
• III. Renal Lesions
• IV. Adrenal Nodules

https://www.acr.org/Clinical-Resources/Incidental-Findings

“Incidentaloma”
• “an incidentally discovered mass or lesion detected by CT, MR, or other imaging modality performed for an unrelated reason”
• Common (40% ) on routine CT abdomen and pelvis
• No known attributable symptoms, active malignancy, or other high risk factors
Purpose of ACR Incidental Findings Project
• 1. Consensus on patient characteristics and imaging features to characterize the finding
• 2. Guidance on how to manage incidental findings
• 3. Standardize reporting terminology
• 4. Enable future research

Incidental Findings Project
• “Guidance” or “Recommendation”. Not standard of care or formal guideline
• “Radiologists should feel comfortable deviating from the algorithm in circumstances not represented in algorithm on the basis of specific imaging appearance and patient characteristics”

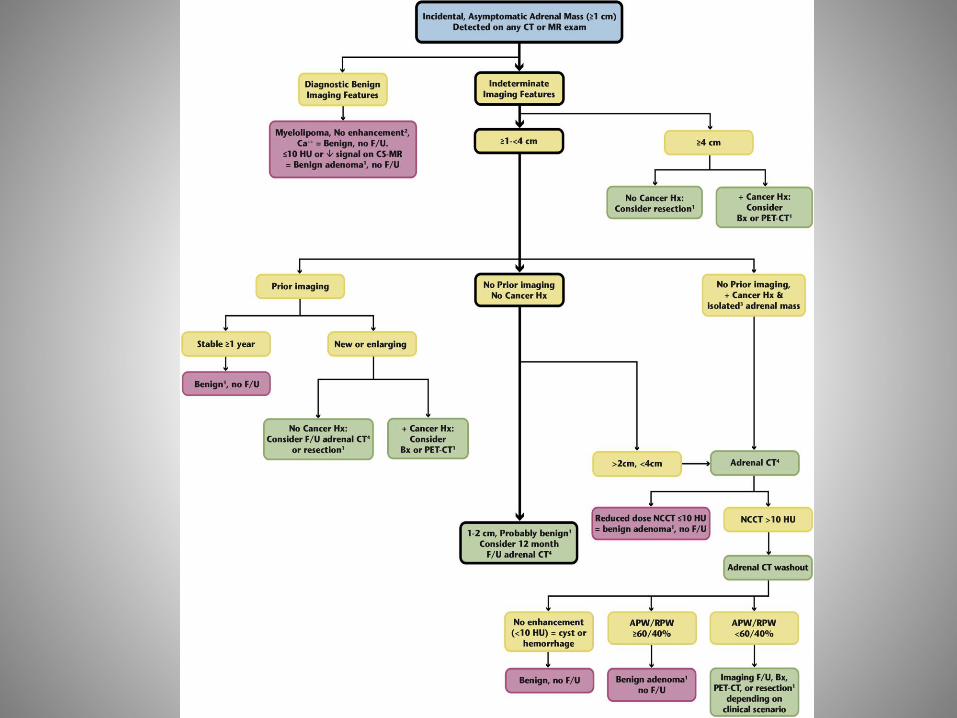
Principal of Flow Chart
• Yellow box: Use lesion or patient characteristics
• Green box: Action required
• Red box: Stop work up.
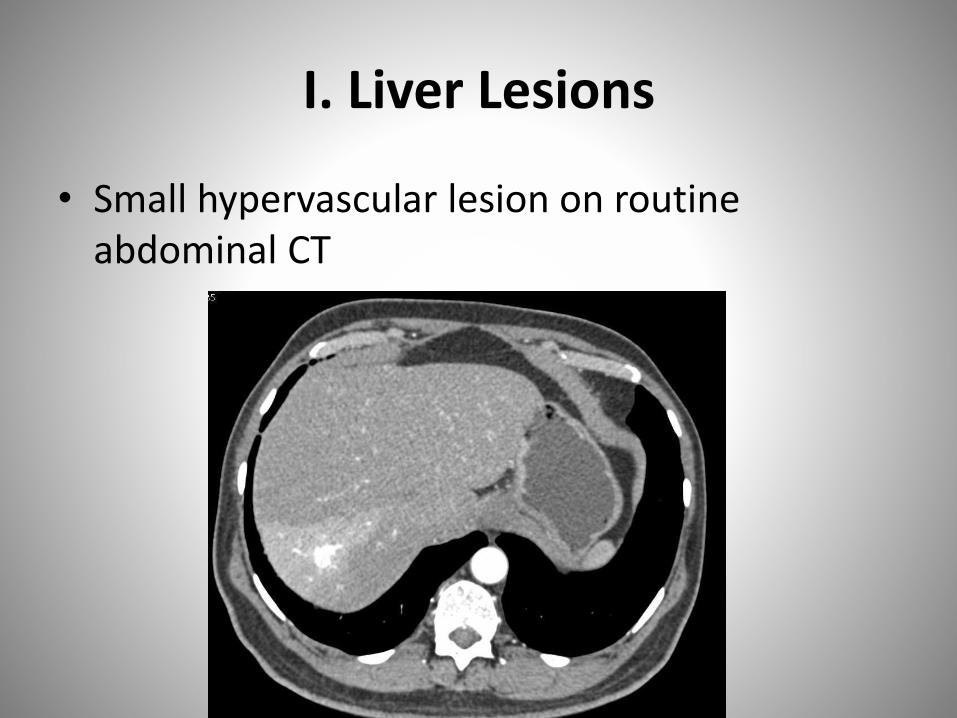
I. Liver Lesions
• Small hypervascular lesion on routine abdominal CT

Incidental Liver Lesion
• Very common, at least 30% of patients >40 yo
• Risk for any liver lesion dependent on imaging characteristics and patient risk factors
• Correlation with patient history is critical!

Common Liver Lesion DDX
• Common Benign– Cyst
– Hemangioma
– FNH
– Adenoma
• Primary– HCC
• Metastatic– Hypervascular vs hypovascular

Patient risk stratification
• Low Risk Patient
– No known malignancy
– No hepatic dysfunction
– No hepatic risk factors
• High Risk
– Known malignancy
– Cirrhosis
– Hepatic Risk factors


Incidental lesion < 1 cm:Low Risk: No follow up
High Risk: MRI in 3 to 6 mo

Hepatic Cyst: Benign, no work up

Classic Hemangioma: Benign, no work up

Transient Hepatic Attenuation Difference

Reporting Considerations
• Lesion size
• Lesion attenuation
• Lesion homogeneity vs complexity
• Lesion enhancement
• Lesion Margin
• Multiplicity
• Growth
• Location

5 Principals of Algorithm
• 1. Low Risk patient with lesion < 1cm: No work up
• 2. Incidental lesion > 1 cm with benign appearance: No work up
• 3. Incidental lesion > 1cm with suspicious features: Immediate MRI, biopsy if needed.
• 4. Flash Filling: benign in low risk, likely benign in high risk but need MRI
• 5. If indeterminate features, MRI hepatic protocol favored.
Low Risk Patient
• <1.5 cm
– <1 cm: No work up.
– 1 to 1.5 cm and benign features: No work up.
– 1 to 1.5 cm and suspicious: MRI
• >1.5 cm
– Distinctly benign features: No work up.
– Suspicious or Flash Filling/Indeterminate: MRI

“Flash Filling”, <1.5 cm
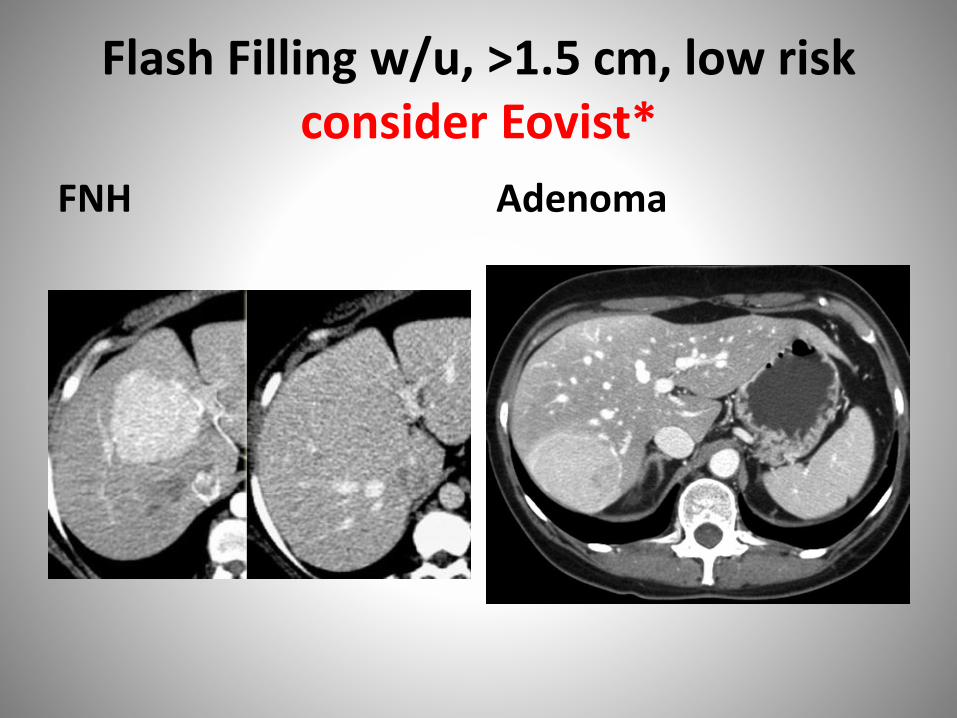
Flash Filling w/u, >1.5 cm, low risk consider Eovist*
FNH Adenoma
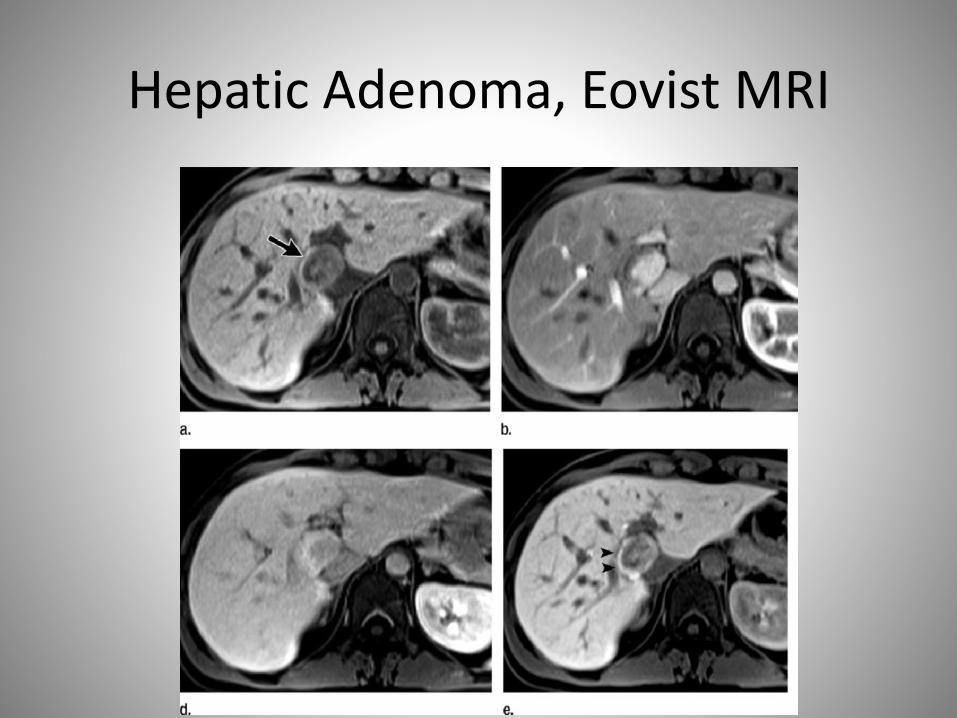
Hepatic Adenoma, Eovist MRI

High Risk Patient
• <1.5 cm
– < 1 cm: Follow up MRI in 3 to 6 months
– 1 to 1.5 cm with benign features: No work up.
– 1 to 1.5 cm suspicious/flash filling: MRI.
• >1.5 cm
– Distinctly benign: No work up.
– Flash Filling/ Indeterminate: MRI.
– Suspicious: +/- MRI, then biopsy.

High Risk Patient, flash filling, <1.5 cm: Regenerative Nodule

High Risk Patient, >1.5cm: HCC

Incidental Liver Lesion Summary
• Don’t follow or work up lesions <1 cm in low risk patients
• Don’t follow or work up incidental lesions with distinctly benign features regardless of risk level
• Work up (immediate MRI) all lesions >1cm without benign features in high risk patients

II. Pancreatic Cysts
• Incidental Pancreatic Cyst on Routine CT
Incidental Pancreatic Cyst
• Incidence increases with age– 2.4 to 13.5% rate on routine imaging– 40% rate on MRI in patients over 70 yo
• Risk of malignancy is unclear– Risk of any cyst harboring malignancy 0.25%– Risk of developing carcinoma in patient with IPMN 2.8%– However, 42% incidence of dysplasia or carcinoma in resected IPMN
• Resection carries 2.1% mortality rate and 30% morbidity rate
• Elta, GH. Enestvedt, BK. Et al. Diagnosis and Management of Pancreatic Cysts. American College of
Gastroenterology. February 2018.
Pancreatic Cyst DDX
• Post inflammatory: pseudocyst
• Simple cyst or lymphoepithelial cyst (rare)
• Serous cystadenoma (SCA)
• Solid Pseudopapillary Epithelial Neoplasm (SPEN)
• Side branch IPM
• Cystic Pancreatic Neuroendocrine Tumor
• Mucinous cystadenoma/carcinoma

Post inflammatory collections, no follow up necessary*
Pseudocyst Walled off necrosis
Role of Endoscopic FNA
• 1. Can characterize cyst as mucinous or post inflammatory (pseudocyst)
• 2. Can establish connection to duct (IPMN).
• 3. Can risk stratify cysts based on genetic assay
• Recommend for any cyst with suspicious features or enlarging cyst

Reporting Considerations
• 1. Cyst morphology and location
• 2. Size
• 3. Communication of MPD
• 4. Worrisome features and High Risk Stigmata
• 5. Growth
• 6. Multiplicity
Size/ Growth
• Single long axis measurement
• Growth
– Cyst size <0.5 cm: 100% increase in long axis
– >0.5 to <1.5 cm: 50% increase in long axis
– >1.5 cm: 20% increase in long axis

Suspicious Features
• Worrisome
– Cyst >3cm
– Thick or enhancing cyst wall
– Nonenhancing mural nodule
– MPD >7mm
• High Risk Stigmata
– Obstructive Jaundice with cyst in pancreatic head
– Enhancing solid component
– MPD >10 mm

5 Principals of Algorithm
• 1. All incidental cysts should be presumed mucinous, followed for 9-10 years, and EUS/FNA considered if growth
• 2. Cyst size determines f/u vs intervention.
• 3. Can shift between algorithm due to size change or patient aging
• 4. Cysts with Suspicious features should prompt EUS/FNA and surgical consultation
• 5. Careful review of prior studies


Pancreatic Cyst <1.5 cm


Branch Type IPMN <2.5 cm


Cyst 1.5-2.5 cm, cannot confirm IPMN


Serous Cystadenoma
• Classic appearance 60%
• Work up if symptomatic or > 4cm

Indeterminate Cyst > 2.5, No high risk features

Pancreatic Cyst, >2.5 cm, high risk features

Malignant Mixed IPMN


Pancreatic Cyst Summary
• Essentially all Pancreatic Cysts need follow up
• All cysts presumed mucinous until proven otherwise
• Growth or high risk features always triggers EUS

III. Renal Lesions
• “Complex” Cyst on Routine CT

Incidental Renal Lesions
• Very common
– 40% incidence on abdomen and pelvis in patient >50 yo
– 50% incidence on autopsy
• Simple cysts most common
• However, most RCC is detected incidentally and outcome is much better than symptomatic RCC

Incidental Renal Lesion DDX
• Cyst– Simple– Hemorrhagic/Proteinacious– Complex
• Abscess• Hematoma• Neoplasm
– Angiomyolipoma– Oncocytoma– Renal Cell Carcinoma– Metastasis, Urothelial CA (rare)

Incidental Renal Lesion W/U
• I. Incompletely Characterized: need renal protocol CT or MRI
• II. Completely Characterized– Benign: No further work up.
– Malignant: Urologic consult for treatment.
• III. Incompletely Characterized but benign features: further w/u unlikely to be beneficial

Complete Characterization
Reporting Considerations
• 1. Size
• 2. Attenuation
• 3. Homogeneity vs heterogeneity
• 4. Enhancement
• 5. Cyst complexity (Bosniak)
• 6. Growth or morphologic change
• 7. Biopsy

Size
• Too small to characterize (TSTC): lesion is less than 2 x reconstructed slice thickness
• <1 cm can use subject evidence of enhancement/heterogeneity
• Solid mass <1cm (40% benign): active surveillance
• “In a meta-analysis of over 200 renal masses less than 4.1 cm for 34 months, mean growth rate 0.28 cm/ year and only 1% developed metastasis”
Cyst Heterogeneity
• Wall thickening
• Septations
• Mural Nodule
• Varying degrees of attenuation
• Calcification
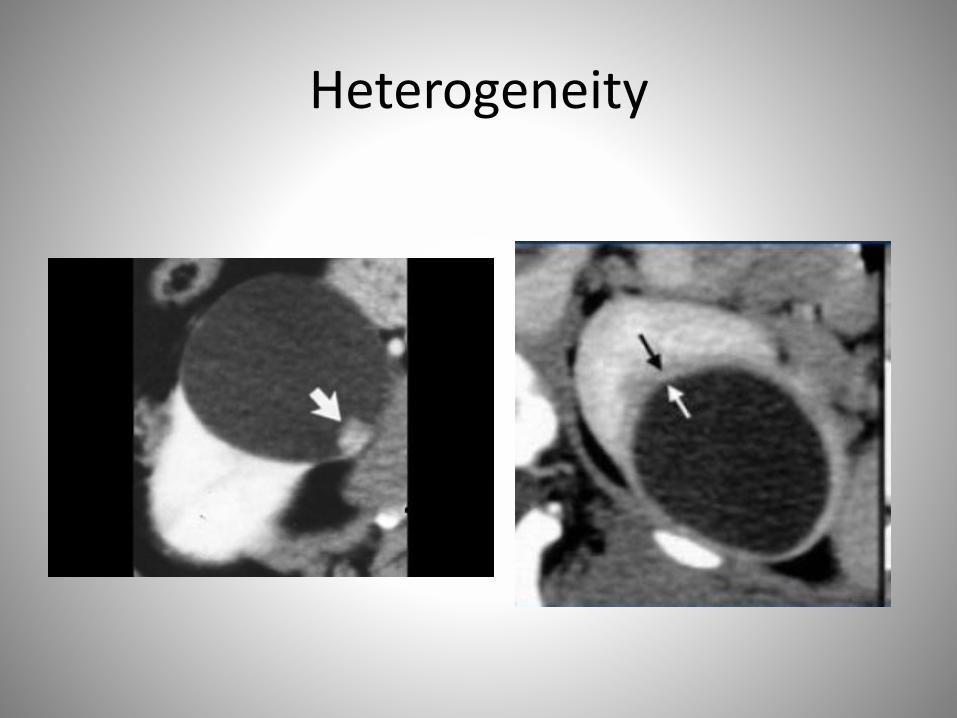
Heterogeneity
Enhancement
• CT
– <10 HU: No enhancement
– 10 to <20 HU Equivocal
– >20 HU Enhancement
• MRI
– 15% signal intensity increase
– Visible signal intensity on subtraction imaging

Bosniak Classification

Principals of Algorithm
• 1. Masses with macroscopic fat have separate algorithm
• 2. Other Flowcharts based on available imaging• 3. Renal protocol CT or MRI can be used based
on local expertise/ preference• 4. Majority of TSTC lesions are benign and can
be assessed subjectively• 5. Management may include biopsy, local
treatment, surgery, active surveillance, or nonimaging work up.
Incidental Renal Mass on Non Contrast CT
• Fat density: <-10 HU
• Cyst: -10 to 20 HU
• Indeterminate: 20 to 69 HU
• Hyperdense: >70 HU

Non Contrast CT

Simple Renal Cyst: Homogenous, -10 to 20 HU

Hemorrhagic Cyst: Homogenous, >70HU

Indeterminate, 20 to 69 HU: needs w/u
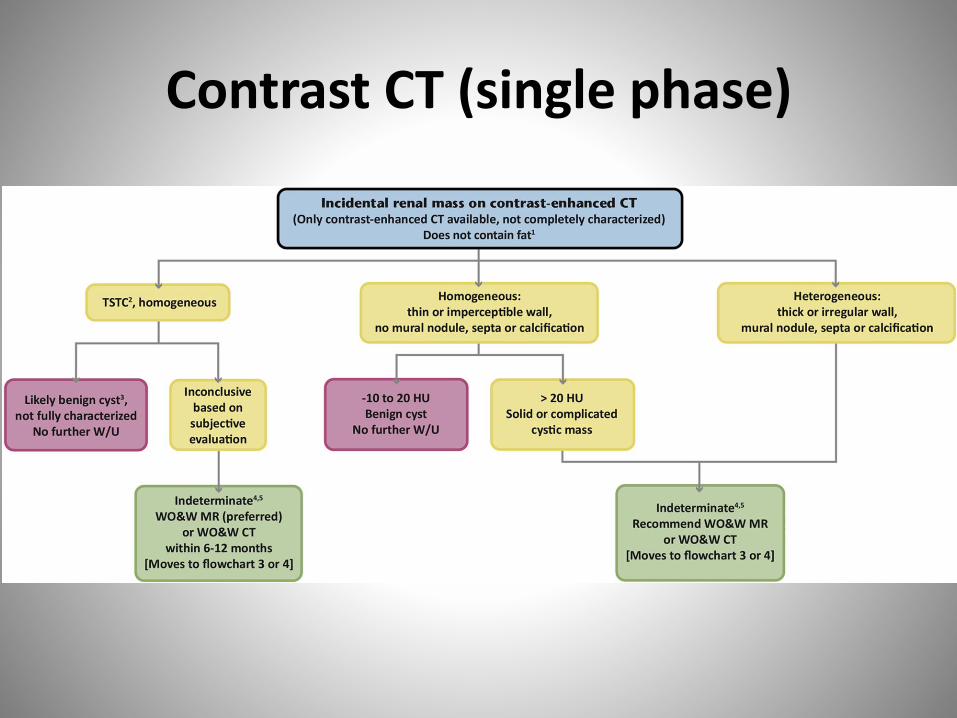
Contrast CT (single phase)
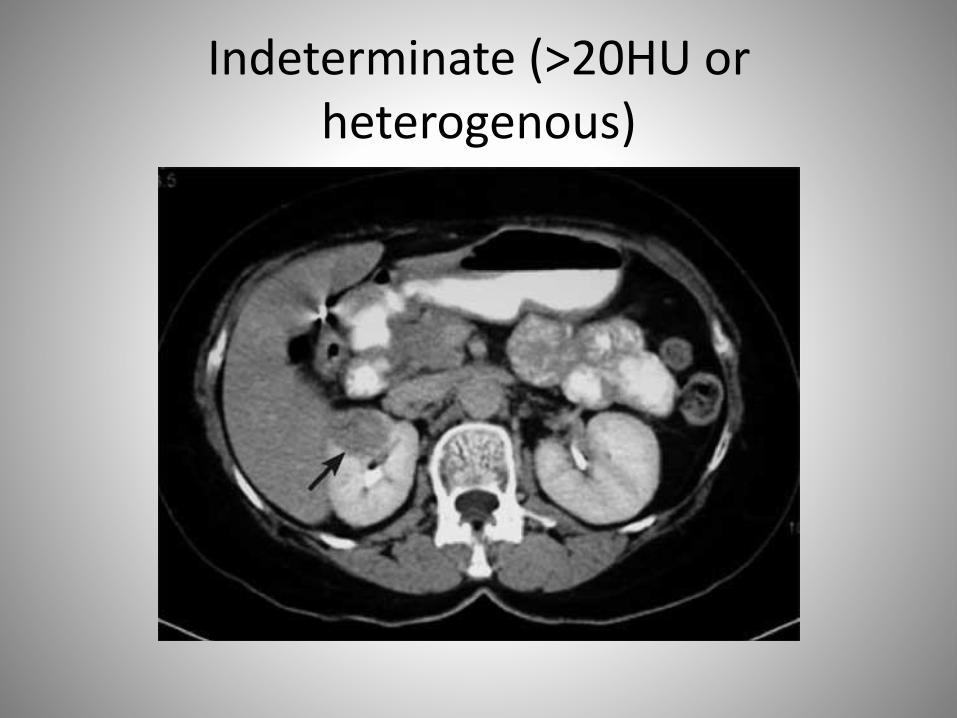
Indeterminate (>20HU or heterogenous)

Cystic Renal Mass (on renal CT/MR)

Bosniak IIF: 6 mo follow up
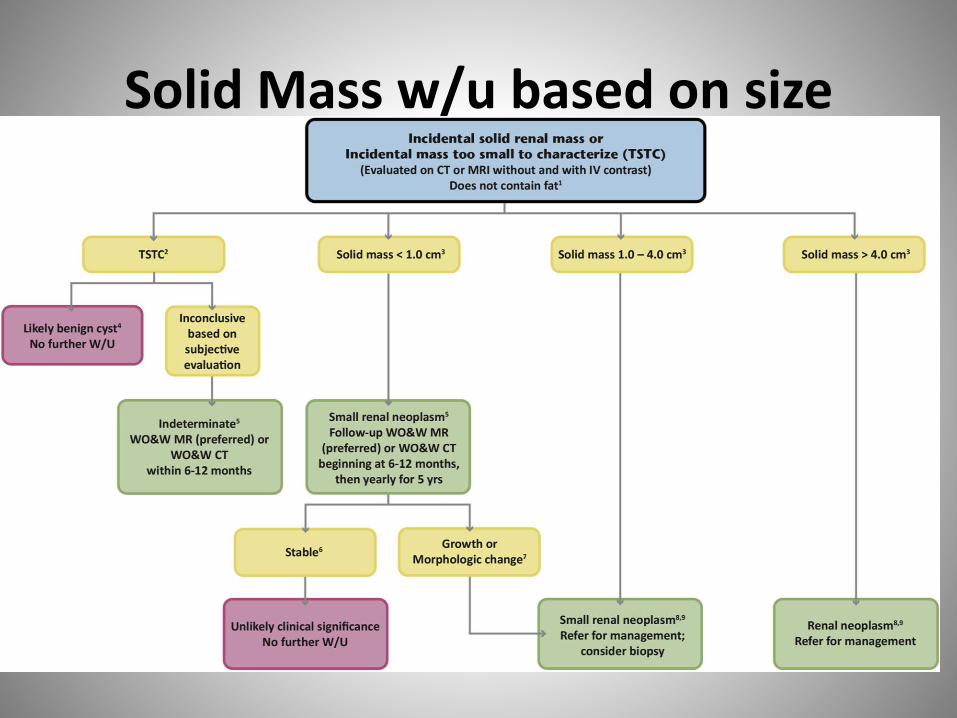
Solid Mass w/u based on size
Solid Mass < 1 cm
• Solid lesion with confirmed or subjective enhancement
• Active surveillance for 5 years
• If stable for 5 years, unlikely to be clinically significant
• If enlarges, biopsy or resect
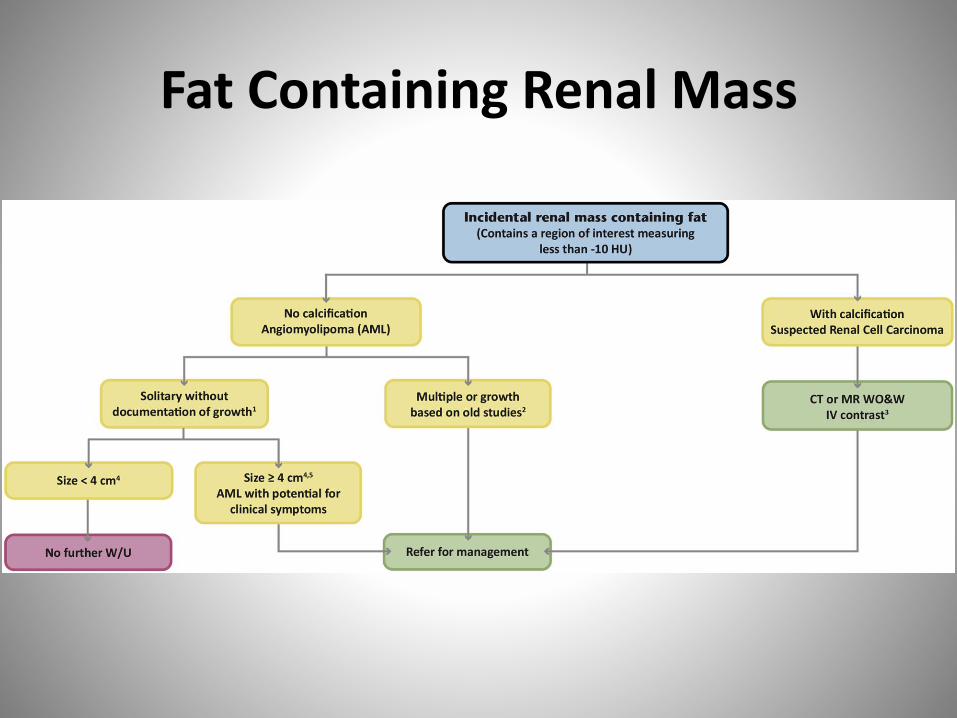
Fat Containing Renal Mass

Angiomyolipoma

Angiomyolipoma
> 4 cm, Urology ConsultMultiple, consider Tuberous Sclerosis
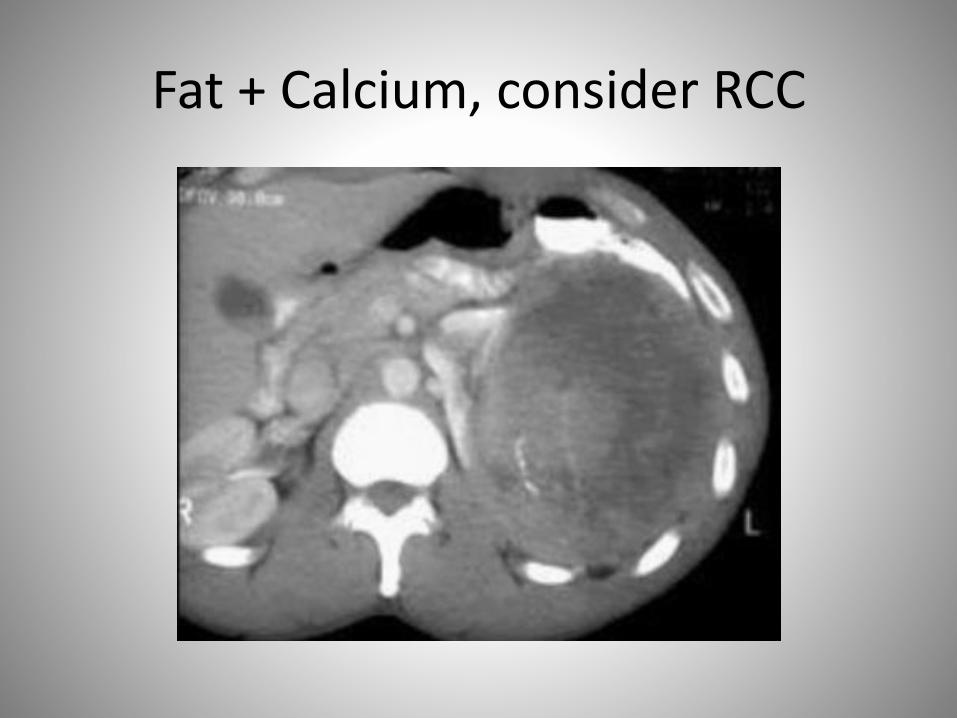
Fat + Calcium, consider RCC
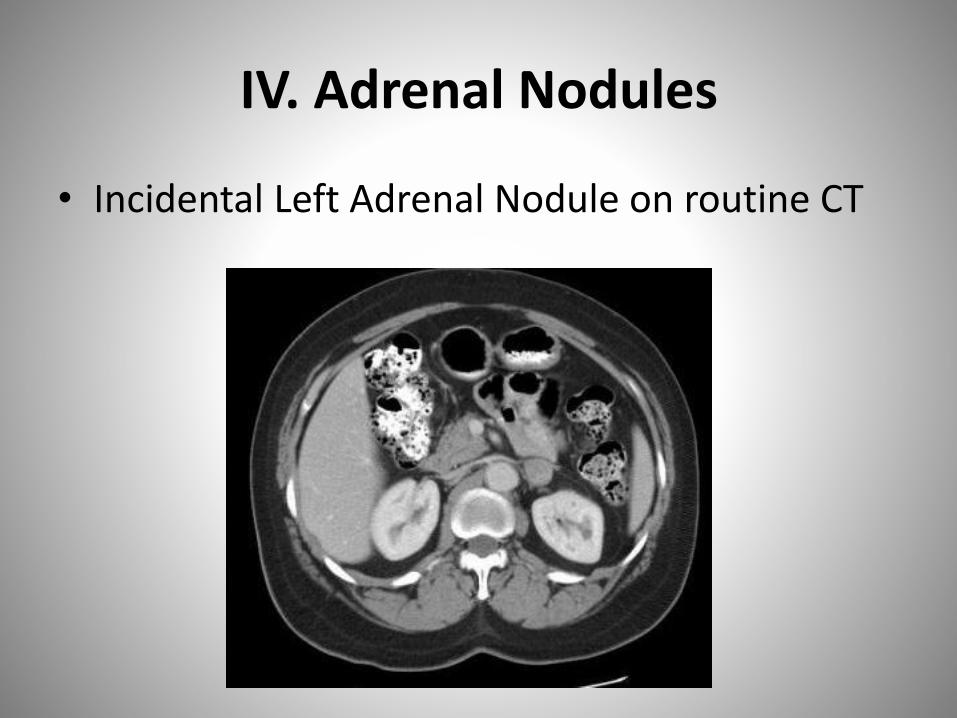
IV. Adrenal Nodules
• Incidental Left Adrenal Nodule on routine CT
Incidental Adrenal Nodules
• Very common, 7-15% of adults
• Nonfunctioning Adenoma most common
• Malignancy very rare– “1.2% rate of adrenal cortical carcinoma in 342 patients with
adrenal incidentaloma.” (all >5cm)– “0.3% incidence of metastasis if no known malignancy”– “25-36% incidence of metastasis if known malignancy”– Am Fam Physician. 2010 Jun 1;81(11):1361-1366.
• Algorithm based on imaging appearance, size, and cancer history

Common Adrenal Nodule DDX
• Benign
– Adenoma
– Myelolipoma
– Hemorrhage
• Primary
– Pheochromocytoma
– Adrenal Cortical Carcinoma
• Metastasis

Adrenal Nodule/Thickening <1cm:No work up*

Benign Features: No work up
• Adenoma, <4cm*:
– Non contrast CT: <10 HU
– CT adrenal protocol: 60% absolute washout
– MRI: SI drop out of >20% on out of phase
• Macroscopic Fat: Myelolipoma
• Calcification: Old hemorrhage, infection, granuloma
• No enhancement: Hemorrhage
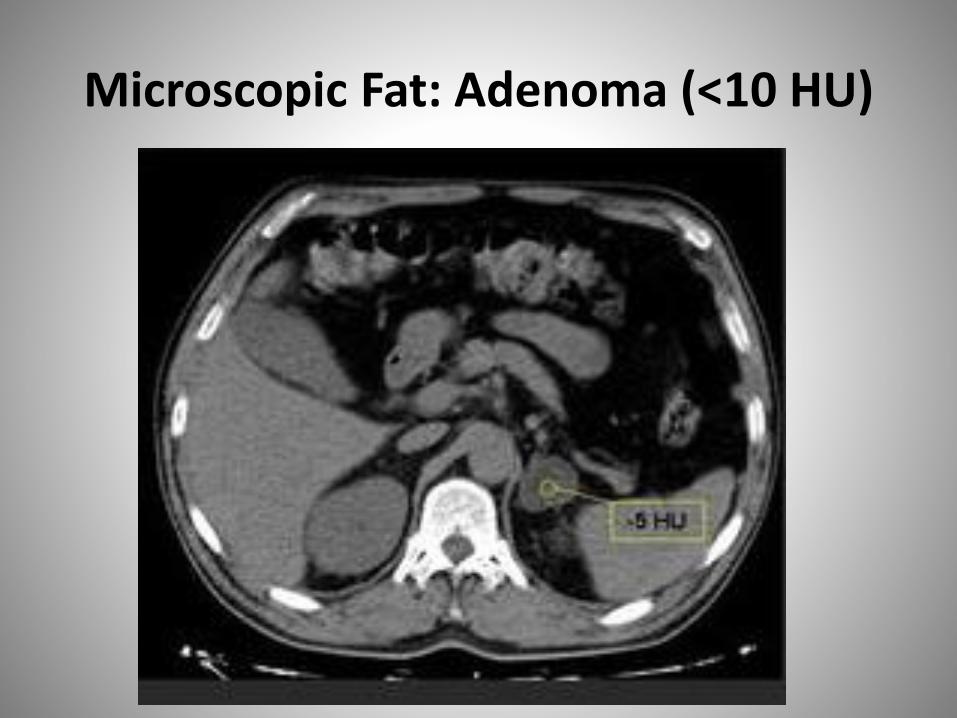
Microscopic Fat: Adenoma (<10 HU)

>20% SI Drop Out Opposed Phase MR: Adenoma

Macroscopic Fat: Myelolipoma

Adrenal Calcification: Benign

5 Principals of Algorithm
• 1. Incidental adrenal lesion < 1cm: No work up.
• 2. Risk determined by size, imaging features, growth, and cancer history
• 3. CT adrenal protocol study of choice for indeterminate lesion 1 to 4 cm.
• 4. Careful review of old studies for comparison
• 5. Work up of adrenal mass should consider clinical context: Life expectancy, change stage, co-morbidities, etc.
Incidental Adrenal Lesion >1 cm but <4cm, Indeterminate features
• No history of Cancer
– 1-2 cm: Follow up Adrenal CT in 12 mo
– 2 to <4cm: Adrenal Protocol CT now
• History of Cancer
– Adrenal Protocol CT now
– Biopsy or PET if indeterminate
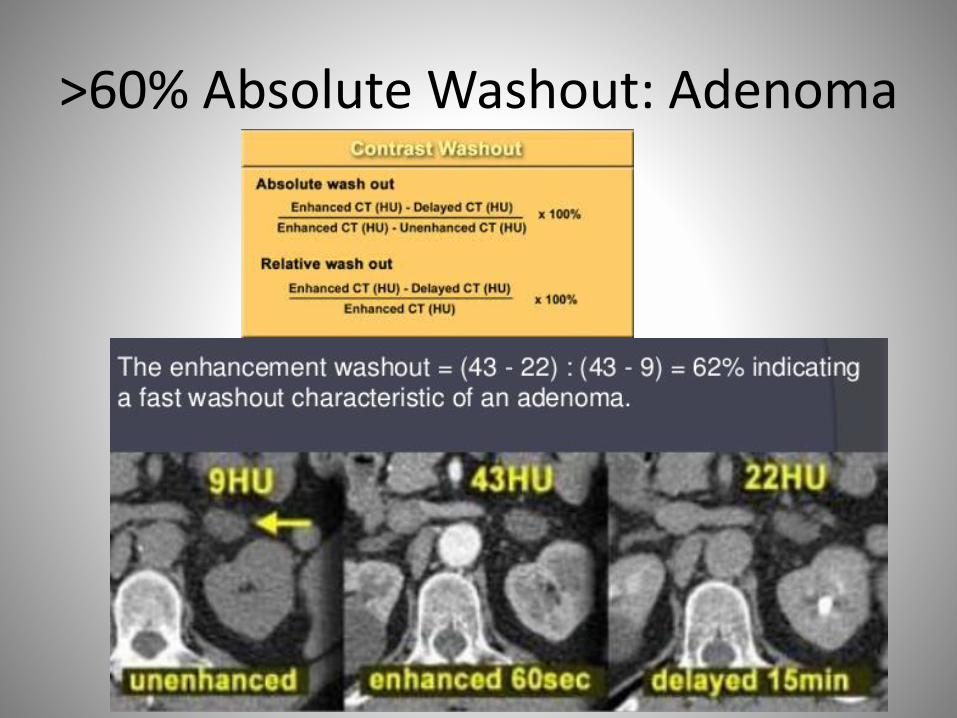
>60% Absolute Washout: Adenoma

>60% Washout, peak >120 HU:Consider Pheochromocytoma

Indeterminate 1 to <4cm, absolute washout less <60%

Adrenal Biopsy
Indeterminate 2-4cm lesion after adrenal protocol CT in patient with no history of cancer
New or enlarging indeterminate nodule 1-4 cm in patient with known cancer
Lesion >4cm in patient with known cancer
Incidental Adrenal Lesion > 4 cm, Indeterminate
• CT adrenal protocol immediately
• If indeterminate and no history of cancer, surgical resection recommended to exclude adrenal cortical carcinoma
• Biopsy indeterminate lesion in patient with history of cancer or if high risk surgical candidate
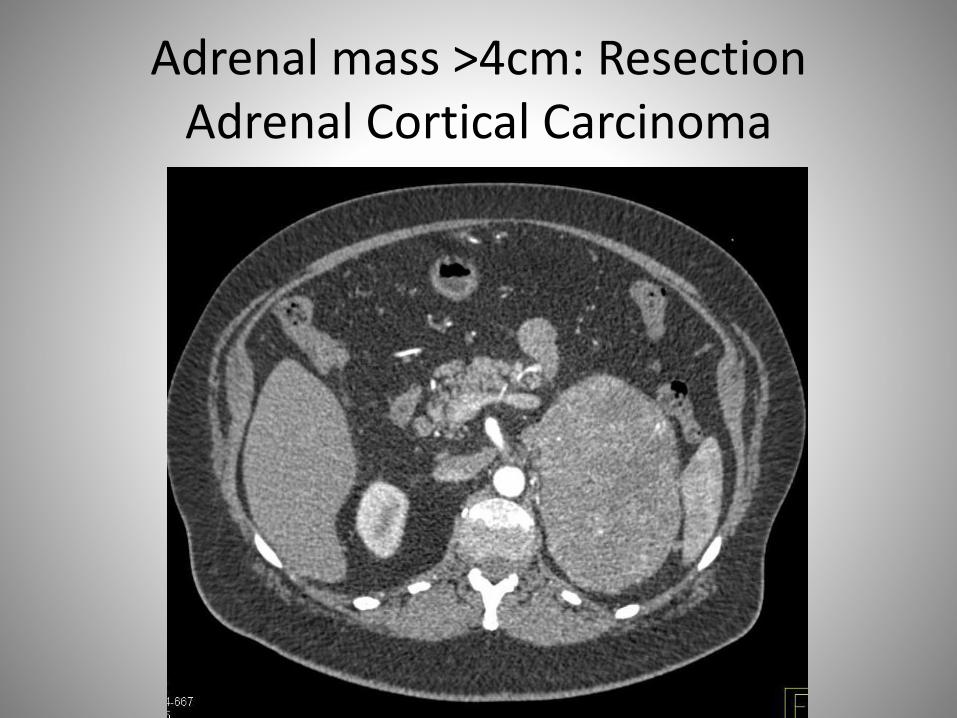
Adrenal mass >4cm: ResectionAdrenal Cortical Carcinoma

Summary
• Don’t Follow…– Liver Lesion
• <1cm in low risk patient• Benign appearance regardless of size (hemangioma/cyst)• Flash Filling <1.5 cm
– Renal lesion• Benign: Cyst, hemorrhagic
– Pancreatic Cyst• Pseudocyst• Serous Cystadenoma <4 cm (classic)
– Adrenal Nodule• <1 cm• Benign: Myelolipoma, Ca+, Hemorrhage, confirmed adenoma (<4cm) on
imaging• stable x 1 year (<4cm)

Questions?